
Abstract
The topic of return to sport (RTS) after anterior cruciate ligament (ACL) reconstruction has become the subject of increased scrutiny as a result of publications citing high reinjury rates upon return to high-risk sports postoperatively, as well as disappointing percentages of athletes who are able to RTS. Because the majority of patients who undergo ACL reconstruction are young athletes, the ability to return these individuals to their desired sports levels is paramount and is highly correlated with overall satisfaction and quality of life. This chapter discusses long-term data from ACL reconstruction studies, including reinjury rates and the factors that are most likely related to increased risk of developing arthritis. Reinjury rates (to the ACL in either knee) differ among studies, and it is unclear whether reinjuries are due to younger patient age or participation in high-risk activities per se; failure to restore normal neuromuscular indices (to both knees) may be one major source of this problem. The majority of ACL reconstruction studies show favorable results in terms of improved knee stability and function, and the rates of osteoarthritis (OA) vary widely. Whether RTS after ACL reconstruction correlates with eventual symptomatic OA is unknown at present.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
The majority of patients who undergo anterior cruciate ligament (ACL) reconstruction are athletes <25 years of age [1]. While there are several major goals of surgery, returning these individuals to their desired sport is paramount for patient satisfaction [2,3,4,5,6,7,8] and is the main motivating factor for patients to undergo surgery and months of rehabilitation. Physicians and others involved with patient care often believe return to sports (RTS) is one of the most important outcome criteria after ACL reconstruction [9]. The ultimate RTS goals vary widely and include returning professional athletes back to their careers, allowing collegiate athletes to receive scholarships, providing high school athletes a chance to play additional seasons, and returning recreational athletes back to their desired active lifestyle. Although historic rates of RTS have been acceptable, this topic has come under increased scrutiny due to high reinjury rates recently reported (to the ACL in either knee) upon return to athletics after surgery [10].
In addition to reinjury rates, several barriers that prevent or delay full RTS have recently come under rigorous investigation. These include fear, anxiety, depression, preoperative stress, motivation, self-esteem, locus of control, and self-efficacy [3, 7, 11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26]. Persistent knee symptoms of pain, swelling, stiffness, and instability may also hamper the expected progress of rehabilitation and negatively affect the time to RTS [18, 27,28,29].
Even though many studies have reported significant correlations of return to high-risk sports with ACL reinjuries, few have documented the results of rehabilitation in terms of restoration of normal muscle strength, balance, proprioception, and other neuromuscular indices required for return to high-risk activities that require pivoting, cutting, and jumping/landing. In addition, several studies have shown that changes in neurocognitive function and cortical activity occur after ACL injury and reconstruction [30,31,32,33,34,35,36,37]. The question of whether modern rehabilitation programs effectively resolve these impairments remains to be answered [38, 39]. Therefore, reinjuries may not be due simply to participation in high-risk activities; failure to restore multiple indices to normal (in both knees) may be one major source of this problem, and this will be explored later in this textbook.
The question of what factors play a role in the development of knee osteoarthritis (OA) after ACL reconstruction remains under study, with the exception of meniscectomy. Nearly every long-term study has reported a statistically significant correlation between meniscectomy (performed either concurrently or after the ACL reconstruction) and moderate-to-severe radiographic evidence of OA [40,41,42,43,44,45,46,47,48]. Other factors that may influence the development of knee joint OA include preexisting chondral damage, severe bone bruising, biochemical alterations after the injury, older patient age, elevated body mass index (BMI), excessive uncorrected varus or valgus lower limb malalignment, damage of other knee ligaments, failure of the reconstruction to restore knee stability, serious complications (such as infection, arthrofibrosis), and poor quadriceps strength [47, 49,50,51,52,53,54]. Whether return to high-impact sports after ACL reconstruction increases the rate of development of knee OA is unknown at present. Regardless of the cause, the development of symptomatic OA is especially concerning in young athletic individuals, in whom rates of total knee arthroplasty (TKA) continue to rise rapidly. In 2013, Weinstein et al. [55] estimated that over 1.5 million individuals aged 50–69 years had undergone TKA in the USA, tripling the number compared with the proceeding decade. With TKA survival rates of 20 years, many younger individuals may require a revision arthroplasty.
2 Quality of Life and Patient Satisfaction: Correlation with Return to Sport
One major goal of ACL reconstruction is to return patients to their desired sports activity level. Interestingly, a review published in 2015 found that, in 119 ACL-reconstruction studies, only 24% provided return to preinjury sports activity data [56]. The authors recommended enhanced reporting of these data due to the high level of relevance of RTS for both patients and clinicians. In the same year, a survey of 1779 orthopedic medical professionals reported a consensus of six measures believed important for successful outcome 2 years after ACL reconstruction [9]. These measures included no giving-way (indicated by 96.4% of respondents), RTS as indicated by playing 2 seasons at the preinjury level (92.4%), quadriceps strength symmetry >90% (90.3%), absence of joint effusion (84.1%), patient-reported outcomes (83.2%), and hamstrings strength symmetry >90% (83.1%).
Ardern et al. [2] questioned whether satisfaction of knee function according to the patient was associated with different measures, including psychological factors and personal opinion of knee function. These authors followed 177 ACL-reconstructed patients a mean of 3 years postoperatively, of whom 44% were satisfied with their outcome, 28% mostly satisfied, and 28% dissatisfied. There was a significantly greater percentage of patients in the satisfied group that returned to their preinjury sports level compared with the other groups (61%, 29%, and 22%, respectively, P < 0.0001). Participants who had returned to their preinjury activity level had 3 times increased odds of being satisfied (versus mostly satisfied or dissatisfied). The other two significant associations with satisfaction were knee-related self-efficacy and quality of life (QOL).
Another study performed a cross-sectional comparison of patients who underwent either operative or conservative treatment for acute ACL ruptures [57]. At 1 year post-injury or postoperative, 350 ACL-deficient knees and 350 ACL-reconstructed knees completed the Knee Injury and Osteoarthritis Outcome Score (KOOS). The ACL-reconstructed group had higher scores for pain, activities of daily living, sports, and quality of life 1 year postoperatively (Table 1.1). The authors concluded that patients who elected ACL reconstruction had superior outcomes for knee symptoms, function, and quality of life that remained for at least 5 years postoperatively.
Filbay et al. [4] studied QOL and psychological health outcomes in 162 patients who had residual knee pain, symptoms, or functional limitations a mean of 9 years (range, 5–20) postoperative. These investigators found that RTS was related to better knee-related KOOS and general health-related QOL (AQoL-8D) scores. In this study, 39% returned to competitive sports, 28% returned at a lower level of competition, and 32% did not return. When asked what activities they would consider most important to participate in (in the absence of knee pain), 80% of the patients indicated sports or exercise; 14%, family duties; 4%, social activities; and 2%, work duties. This high rate of patients that preferred sports/exercise over all other activities indicates the high priority athletics had in this cohort many years following their ACL injury and surgery.
Nwachukwu et al. [7] surveyed 231 patients a mean of 3.7 years following ACL reconstruction and reported that 87% had RTS and 85.4% were very satisfied with the outcome of the operation. A significantly greater number of patients who RTS were very satisfied with their outcome compared with those who did not return (P < 0.001). It is important to note that only 43.6% of the athletes played with unlimited effort and performance and no pain. The use of a patellar tendon autograft was associated with a significantly increased odds of returning to play compared with use of an allograft (odds ratio [OR] = 5.6; P = 0.02).
Faltstrom et al. [17] conducted a short-term study (mean follow-up, 1.5 years) in 182 female soccer players who underwent ACL STG autograft reconstruction. The survey study found that 52% were currently playing soccer, 80% at the same or higher preinjury level and 20% at a lower level. Players that returned had significantly higher scores compared with those who had not returned on all KOOS subscales and the ACL-Quality of Life scale. In addition, psychological readiness and motivation to return to sport correlated with return to preinjury levels. The negative effects of fear of reinjury and poor motivation on RTS are further discussed in Chap. 2.
Kocher et al. [5] followed a cohort of 201 patients whose mean age was 28.6 years (range, 14.4–60) an average of 3 years after primary ACL reconstruction. Patients were found to be significantly less satisfied with the outcome of surgery if they had a lower level of sports activity (P < 0.001) and if they had difficulty with specific athletic functions such as running, jumping, cutting, and twisting (P < 0.001). In this study, 75 patients (37%) were participating in sports with no limitations.
3 Reinjury Rates After ACL Reconstruction
The published rates of either reinjuring an ACL-reconstructed knee or sustaining an ACL rupture on the contralateral knee vary widely (Table 1.2) [58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83]. One problem is the definition of ACL failure; some studies consider only those knees that required ACL revision reconstruction (or reconstruction of the contralateral ACL) as failures, while others include knees in which a pivot shift grade 2–3 and/or Lachman grade 2–3 is detected clinically. Large registry studies or those that involved meta-analyzed data typically only used the number of ACL revision cases to calculate failure rates [65, 69, 76, 79, 81, 84]. There are many potential causes of ACL graft failure other than reinjuries that have been discussed in detail elsewhere [85,86,87,88,89,90]. The reinjury and failure rate data in Table 1.2 should therefore be interpreted cautiously.
Many studies have cited that the most frequent factors that appear to cause graft failure or injury to the contralateral ACL are younger patient age, return to cutting/pivoting sports, and use of an allograft. In a meta-analysis of data from 19 studies, Wiggins et al. [62] reported, in athletes <25 years of age who returned to high-risk sports, a pooled secondary ACL injury rate (to either knee) of 23%. In a group of 1415 patients who underwent ACL autograft reconstruction, Shelbourne et al. [60] reported the risk of subsequent injury to either knee was 17% for patients <18 years of age compared with 7% for patients 18–25 years and 4% for patients >25 years. These authors attributed the reinjuries to the high-risk sports patients had returned to, with basketball and soccer accounting for 67% of the reinjuries. Andernord et al. [84] reported data on 16,930 patients from the Swedish National Knee Ligament Register and found in both males and females a significantly increased twofold risk of revision surgery with ages 13–19 years (P < 0.001). In a separate study, Andernord et al. [91] reported a significantly increased twofold to threefold risk of contralateral ACL reconstruction in patients less than 20 years of age (P < 0.001).
Dekker et al. [83] followed 85 patients who were <18 years of age at the time of ACL autograft reconstruction a mean of 4 years postoperatively. A majority (91%) returned to sports activities; however, 32% suffered a subsequent ACL tear (19% ipsilateral graft tear, 13% contralateral ACL tear, and 1% both knees) a mean of 2.2 years postoperatively. The only significant risk factor associated with reinjury was earlier return to sport (P < 0.05). Longer times before returning to athletics were protective against a second ACL injury (hazard ratio per month, 0.87 for each 1-month increase).
Faltstrom et al. [92] followed 117 female soccer players (mean age, 19.9 ± 2.5 years) a mean of 2 years after primary ACL reconstruction and compared reinjury rates, proportion of players who stopped playing soccer, and patient satisfaction with a matched group of uninjured players. The ACL-reconstructed group had nearly a fivefold higher rate of new ACL injuries (29 versus 8, rate ratio 4.82, P < 0.001), a higher rate of players who stopped playing soccer (62% versus 36%, P = 0.001), and a lower satisfaction rate (47% versus 87%).
Several investigations have reported discouraging percentages of athletes who RTS even though muscle strength and neuromuscular function appeared to be restored to normal levels [28, 29, 93,94,95,96]. A meta-analysis of 69 articles involving 7556 athletes reported that only 65% returned to their preinjury sports level and 55% returned to competitive sports [94]. Factors associated with RTS included symmetrical hopping performance, younger age, male gender, playing elite sports, and having a positive attitude. A study of 205 soccer players reported that only 54% returned to the sport a mean of 3.2 years postoperatively [29]. Of those that returned, 39% experienced pain, 43% had stiffness, and 42% reported instability during or after physical activity. Male gender, no cartilage injury, and no pain during physical activity were associated with greater odds of RTS. An investigation of 99 athletes reported that although 92% returned to sports, only 51% returned to their preinjury level [23]. Factors associated with RTS in this study included female gender and higher scores on the International Knee Documentation Committee (IKDC) Subjective Knee scale and the Lysholm scale. Rosso et al. [28] reported that, although 90% of 161 patients RTS after primary ACL reconstruction, only 58% did so at the preinjury level. The main reasons for not returning were knee symptoms (37%), personal reasons (30%), or both (29%).
A meta-analysis that assessed RTS and reinjury rates of 1008 children and adolescents (aged 6–19) from 19 studies reported a pooled return to preinjury activity level in 79% (range, 41–100%) [97]. ACL reinjury rates were provided for 717 patients, 13% of whom sustained ACL graft ruptures. Contralateral ACL rupture rates were provided for 652 knees, 14% of whom sustained injuries. Ten of the studies reported that the majority of injuries occurred during sports activities.
Critical Points
-
Long-term failure rates vary widely (2–32%).
-
Factors correlated with ACL graft failure: younger age, high sports activity level, vertical graft angle, and use of a small STG autograft or allograft.
-
Contralateral ACL at risk for rupture, higher than ACL graft in some studies.
4 Factors Involved in the Development of Knee Osteoarthritis After ACL Surgery
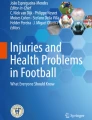
Long-term clinical studies documenting radiographic OA after ACL reconstruction show high variability in the percent of knees that develop moderate or severe joint damage (Table 1.3) [40, 41, 45,46,47,48, 75, 99,100,101, 103,104,105,106, 108, 110,111,112,113,114]. These studies most frequently used weight-bearing anteroposterior (AP) and posteroanterior radiographs (Fig. 1.1), as well as lateral and Merchant, to determine the presence and severity of OA, although a few used MRI [110, 111, 114, 116, 117] or computed tomography [118]. The two most commonly used radiographic rating systems to classify OA are the Kellgren-Lawrence (K-L) [119] and the IKDC system [120]. It is also important to note that few investigators have determined if OA is accompanied by pain, swelling, and impaired knee function. The longest clinical studies published to date have followed patients for 16–24.5 years postoperatively [102, 121,122,123]. As investigations obtain longer follow-up periods, one may speculate that the OA findings will become more severe and correlate with clinical symptoms such as loss of extension and swelling with daily activities.

Standing radiographs of a patient 14 years after a right ACL reconstruction and subsequent medial meniscectomy. The pivot-shift test was negative, indicating a stable reconstruction. However, narrowing to the medial tibiofemoral compartment is evident and the patient demonstrated 2° of varus alignment (Reprinted from Noyes and Barber-Westin [115])
Studies have shown that, regardless of the outcome of ACL reconstruction in terms of restoration of knee stability, meniscectomy accelerates degenerative joint changes [40, 41, 45,46,47,48, 124, 125]. Claes et al. [43] systematically reviewed 16 long-term ACL reconstruction studies (follow-up range, 10–24.5 years) involving 1554 subjects. The investigators reported that the estimate for the prevalence of moderate to severe OA (IKDC ratings of C or D) for all patients was 27.9%. The prevalence of OA was 16.4% in patients with isolated ACL injuries and 50.4% in patients with concurrent meniscectomy (OR 3.54).
Barenius et al. [41] followed 164 patients a mean of 14 years after ACL reconstruction and reported symptomatic OA (K-L grade ≥2) in 57% of ACL-reconstructed knees compared with 18% of contralateral knees. Statistically significant risk factors for medial tibiofemoral OA were BMI ≥25 kg/m2 at follow-up (OR 3.3), manual labor (OR 3.2), positive pivot shift at 2-year follow-up (OR 2.5), and medial meniscectomy (OR 4.2). Statistically significant risk factors for lateral tibiofemoral OA were lateral meniscectomy (OR 5.1) and use of a B-PT-B autograft (OR 2.3). Statistically significant risk factors for patellofemoral OA were BMI ≥25 kg/m2 at follow-up (OR 3.5) and medial meniscectomy (OR 2.3). There was no significant difference in the prevalence of OA between the two graft types.
We conducted a systematic review of the treatment of meniscus tears during ACL reconstruction of studies published from 2001 to 2011 [126]. Data on 11,711 meniscus tears (in 19,531 patients) from 159 studies showed that 65% were treated by meniscectomy; 26%, by repair; and 9%, by no treatment. This was concerning because many meniscus tears can be successfully treated by repair, thereby salvaging this important structure.
It is important to note that there are many factors other than meniscectomy that may influence the development of knee joint OA, including preexisting chondral damage, severe bone bruising, biochemical alterations in the knee joint after the injury, older patient age, elevated BMI, failure of the reconstruction to restore normal AP displacement, complications (such as infection, arthrofibrosis), and poor quadriceps strength [47, 49,50,51,52,53,54]. In many studies, these variables are not controlled for, making reaching conclusions on these factors difficult.
Occult injuries to the bone, commonly referred to as bone bruises , occur with ACL ruptures in 80–100% of knees (Fig. 1.2) [127,128,129,130,131,132,133]. Occult osteochondral lesions vary, and therefore, the relationship between the presence of these injuries with ACL ruptures and subsequent OA remains unclear. Several studies have reported that bone bruises resolve with time [110, 132, 134]. Conversely, Frobell [134] followed 61 consecutive patients who had acute ACL injuries with MRI within 4 weeks of the injury and then 2 years later. Subjects were treated either with early ACL reconstruction (34 subjects), delayed ACL reconstruction (11 subjects), or rehabilitation alone (16 subjects). Posttraumatic bone marrow lesions noted in the lateral tibiofemoral compartment resolved in 57 of 61 knees by 2 years after the ACL injury. However, new lesions developed in the lateral tibiofemoral joint for unknown reasons in one-third of the population, and significant thinning of the cartilage in the trochlea was noted that was not detected during the baseline MRI. Evidence does exist that the most severe injuries are associated with future cartilage degeneration, and they therefore should be considered part of the sequela of post-traumatic OA.

Bone bruise on MRI following rupture of the ACL
A few studies that longitudinally followed patients with acute ACL ruptures for several years demonstrated a strong potential for joint deterioration [54, 131, 134]. For instance Potter et al. prospectively followed 40 patients who underwent baseline MRI within 8 weeks of the injury and again 7–11 years later [131]. The MRI evaluation used a cartilage-sensitive, pulse sequence evaluation with T2 techniques which have shown increased ability to detect traumatic chondral injuries. None of the patients had concurrent damage to the menisci or other knee ligaments or an articular cartilage lesion rated as Outerbridge grade 3 or higher. ACL reconstruction was performed in 28 patients, while no surgery was done in 14. At baseline, all knees had an MRI-detectable cartilage injury, most severely over the lateral tibial plateau. Regardless of surgical intervention, by 7–11 years after injury, the risk of cartilage damage as viewed on MRI for the lateral femoral condyle was 50 times that of baseline, 30 times for the patella, and 18 times for the medial femoral condyle. The nonsurgical group had a significantly higher OR effect of cartilage loss over the medial tibial plateau compared with the surgical group.
ACL ruptures create biochemical alterations in the knee joint which many investigators hypothesize play a major role in the development of OA [135,136,137,138,139,140,141,142,143,144,145,146,147,148,149,150]. The sequence of events begins immediately after the injury and continues for years thereafter (Table 1.4) [135, 136, 149]. The injury causes collagen rupture, joint hemarthrosis, subchondral bone edema, elevated glycosaminoglycan (GAG) levels, and cell necrosis. In the ensuing months, the inflammatory process (indicated by elevated levels of several cytokine mediators such as IL-1β, IL-6, and tumor necrosis factor α [TNFα]), decrease in lubricin concentrations, release of enzymes, production of metalloproteinase (MMP), degradation of the extracellular matrix and proteoglycans, chondrocyte apoptosis, and cell death all contribute to articular cartilage deterioration.
Our analysis of current long-term studies provided no answer regarding the potential deleterious effect of returning to high athletic activity levels on subsequent risk of symptomatic OA. One may hypothesize that knees with intact menisci and no other ligament damage (that do not sustain reinjuries) will have no statistically significant increased risk for symptomatic OA compared with matched controls. The need to preserve meniscal function remains paramount for the long-term welfare of the joint, and we have long advocated meniscal repair for tears in the red/red (periphery) and red/white (central) regions (Fig. 1.3) [152,153,154,155,156]. Complex tears are evaluated on an individual basis for repair potential (Fig. 1.4). The indications and contraindications for meniscus repair procedures have been discussed in detail elsewhere [153]. Our long-term study (10–22 years) of single longitudinal meniscus repairs that extended into the central region in patients ≤20 years of age showed the potential longevity of this procedure [155]. Twenty-nine repairs were evaluated; 18 by follow-up arthroscopy, 19 by clinical evaluation, 17 by MRI, and 22 by weight-bearing posteroanterior radiographs. A 3 T MRI scanner with cartilage-sensitive pulse sequences was used and T2 mapping was performed (Fig. 1.5). We found that 18 (62%) of the meniscus repairs had normal or nearly normal characteristics. Six repairs (21%) required arthroscopic resection, two had loss of joint space on radiographs, and three that were asymptomatic failed according to MRI criteria. There was no significant difference in the mean T2 scores in the menisci that had not failed between the involved and contralateral tibiofemoral compartments. There were no significant differences between the initial and long-term evaluations for pain, swelling, jumping, patient knee condition rating, or the Cincinnati rating score. The majority of patients were participating in sports without problems, which did not affect the failure rate. The outcomes support the recommendation in younger active patients to spend as much time and attention to a meniscus repair as a concurrent ACL reconstruction, as the eventual function of the knee joint is equally dependent on the success of the both structures

Meniscus repair instead of meniscectomy to preserve knee joint function. A longitudinal meniscal tear site demonstrates some fragmentation inferiorly. This tear required multiple superior and inferior vertical divergent sutures to achieve anatomic reduction (Reprinted from Noyes and Barber-Westin [152])

Arthroscopic visualization of a lateral meniscus root tear. (a) A double locking loop stitch (NovoStitch, Ceterix) is placed through the meniscus at the tear site (b). Three loop stitches were used to achieve a high strength fixation (c). Final configuration of the lateral meniscus repair with the meniscus pulled flush to the repair site (d) (Reprinted from Noyes and Barber-Westin [115])

T2 MRI of a 37-year-old male 17 years post-ACL reconstruction and lateral meniscus repair. The patient was asymptomatic with light sports activities. The lateral meniscus repair healed and the ACL reconstruction restored normal stability. Prolongation of T2 values is noted over the posterior margin with adjacent subchondral sclerosis (arrow) (Reprinted from Noyes et al. [155])
Critical Points
-
Majority OA mild or moderate; presence of associated symptoms not reported in most studies.
-
Meniscectomy correlates with radiographic evidence of osteoarthritis (OA) in nearly all long-term studies in which cohorts are sorted according to intact versus meniscectomized knees.
-
Other risk factors associated with OA after ACL reconstruction include preexisting chondral damage, severe bone bruising, biochemical alterations, patient age, body mass index, failure of the reconstruction to restore normal anteroposterior displacement, complications, and poor quadriceps strength.
-
ACL injury causes collagen rupture, joint hemarthrosis, subchondral bone edema, elevated glycosaminoglycan levels, and cell necrosis.
-
Bone bruises 80–100% acute ACL rupture, natural history unclear.
-
Large severe bone bruises associated with subchondral or osteochondral injuries may persist for years after injury.
-
Consider most severe bone injuries part of sequela of post-traumatic OA.
-
We have long advocated repair of meniscus tears when appropriate indications met to preserve this vital structure.
References
Sanders TL, Maradit Kremers H, Bryan AJ, Larson DR, Dahm DL, Levy BA, Stuart MJ, Krych AJ. Incidence of anterior cruciate ligament tears and reconstruction: a 21-year population-based study. Am J Sports Med. 2016;44(6):1502–7. https://doi.org/10.1177/0363546516629944.
Ardern CL, Osterberg A, Sonesson S, Gauffin H, Webster KE, Kvist J. Satisfaction with knee function after primary anterior cruciate ligament reconstruction is associated with self-efficacy, quality of life, and returning to the preinjury physical activity. Arthroscopy. 2016;32(8):1631–1638 e1633. https://doi.org/10.1016/j.arthro.2016.01.035.
Ardern CL, Osterberg A, Tagesson S, Gauffin H, Webster KE, Kvist J. The impact of psychological readiness to return to sport and recreational activities after anterior cruciate ligament reconstruction. Br J Sports Med. 2014;48(22):1613–9. https://doi.org/10.1136/bjsports-2014-093842.
Filbay SR, Ackerman IN, Russell TG, Crossley KM. Return to sport matters-longer-term quality of life after ACL reconstruction in people with knee difficulties. Scand J Med Sci Sports. 2017;27(5):514–24. https://doi.org/10.1111/sms.12698.
Kocher MS, Steadman JR, Briggs K, Zurakowski D, Sterett WI, Hawkins RJ. Determinants of patient satisfaction with outcome after anterior cruciate ligament reconstruction. J Bone Joint Surg. 2002;84-A(9):1560–72.
Novaretti JV, Franciozi CE, Forgas A, Sasaki PH, Ingham SJM, Abdalla RJ. Quadriceps strength deficit at 6 months after ACL reconstruction does not predict return to preinjury sports level. Sports Health. 2018;10(3):266–71. https://doi.org/10.1177/1941738118759911.
Nwachukwu BU, Voleti PB, Berkanish P, Chang B, Cohn MR, Williams RJ, Allen AA. Return to play and patient satisfaction after ACL reconstruction: study with minimum 2-year follow-up. J Bone Joint Surg. 2017;99(9):720–5. https://doi.org/10.2106/JBJS.16.00958.
Sonesson S, Kvist J, Ardern C, Osterberg A, Silbernagel KG. Psychological factors are important to return to pre-injury sport activity after anterior cruciate ligament reconstruction: expect and motivate to satisfy. Knee Surg Sports Traumatol Arthrosc. 2017;25(5):1375–84. https://doi.org/10.1007/s00167-016-4294-8.
Lynch AD, Logerstedt DS, Grindem H, Eitzen I, Hicks GE, Axe MJ, Engebretsen L, Risberg MA, Snyder-Mackler L. Consensus criteria for defining ‘successful outcome’ after ACL injury and reconstruction: a Delaware-Oslo ACL cohort investigation. Br J Sports Med. 2015;49(5):335–42. https://doi.org/10.1136/bjsports-2013-092299.
Dingenen B, Gokeler A. Optimization of the return-to-sport paradigm after anterior cruciate ligament reconstruction: a critical step back to move forward. Sports Med. 2017;47(8):1487–500. https://doi.org/10.1007/s40279-017-0674-6.
Ardern CL, Taylor NF, Feller JA, Webster KE. Fear of re-injury in people who have returned to sport following anterior cruciate ligament reconstruction surgery. J Sci Med Sport. 2012;15(6):488–95. https://doi.org/10.1016/j.jsams.2012.03.015.
Ardern CL, Taylor NF, Feller JA, Whitehead TS, Webster KE. Psychological responses matter in returning to preinjury level of sport after anterior cruciate ligament reconstruction surgery. Am J Sports Med. 2013;41(7):1549–58. https://doi.org/10.1177/0363546513489284.
Ardern CL. Anterior cruciate ligament reconstruction-not exactly a one-way ticket back to the preinjury level: a review of contextual factors affecting return to sport after surgery. Sports Health. 2015;7(3):224–30. https://doi.org/10.1177/1941738115578131.
Christino MA, Fantry AJ, Vopat BG. Psychological aspects of recovery following anterior cruciate ligament reconstruction. J Am Acad Orthop Surg. 2015;23(8):501–9. https://doi.org/10.5435/JAAOS-D-14-00173.
Ellman MB, Sherman SL, Forsythe B, LaPrade RF, Cole BJ, Bach BR Jr. Return to play following anterior cruciate ligament reconstruction. J Am Acad Orthop Surg. 2015;23(5):283–96. https://doi.org/10.5435/JAAOS-D-13-00183.
Everhart JS, Best TM, Flanigan DC. Psychological predictors of anterior cruciate ligament reconstruction outcomes: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2015;23(3):752–62. https://doi.org/10.1007/s00167-013-2699-1.
Faltstrom A, Hagglund M, Kvist J. Factors associated with playing football after anterior cruciate ligament reconstruction in female football players. Scand J Med Sci Sports. 2016;26(11):1343–52. https://doi.org/10.1111/sms.12588.
Flanigan DC, Everhart JS, Pedroza A, Smith T, Kaeding CC. Fear of reinjury (kinesiophobia) and persistent knee symptoms are common factors for lack of return to sport after anterior cruciate ligament reconstruction. Arthroscopy. 2013;29(8):1322–9. https://doi.org/10.1016/j.arthro.2013.05.015.
Garcia GH, Wu HH, Park MJ, Tjoumakaris FP, Tucker BS, Kelly JD, Sennett BJ. Depression symptomatology and anterior cruciate ligament injury: incidence and effect on functional outcome--a prospective cohort study. Am J Sports Med. 2016;44(3):572–9. https://doi.org/10.1177/0363546515612466.
Hsu CJ, Meierbachtol A, George SZ, Chmielewski TL. Fear of reinjury in athletes. Sports Health. 2017;9(2):162–7. https://doi.org/10.1177/1941738116666813.
Lentz TA, Zeppieri G Jr, George SZ, Tillman SM, Moser MW, Farmer KW, Chmielewski TL. Comparison of physical impairment, functional, and psychosocial measures based on fear of reinjury/lack of confidence and return-to-sport status after ACL reconstruction. Am J Sports Med. 2015;43(2):345–53. https://doi.org/10.1177/0363546514559707.
Podlog L, Heil J, Schulte S. Psychosocial factors in sports injury rehabilitation and return to play. Phys Med Rehabil Clin N Am. 2014;25(4):915–30. https://doi.org/10.1016/j.pmr.2014.06.011.
Rodriguez-Roiz JM, Caballero M, Ares O, Sastre S, Lozano L, Popescu D. Return to recreational sports activity after anterior cruciate ligament reconstruction: a one- to six-year follow-up study. Arch Orthop Trauma Surg. 2015;135(8):1117–22. https://doi.org/10.1007/s00402-015-2240-8.
Tjong VK, Murnaghan ML, Nyhof-Young JM, Ogilvie-Harris DJ. A qualitative investigation of the decision to return to sport after anterior cruciate ligament reconstruction: to play or not to play. Am J Sports Med. 2014;42(2):336–42. https://doi.org/10.1177/0363546513508762.
Webster KE, Nagelli CV, Hewett TE, Feller JA. Factors associated with psychological readiness to return to sport after anterior cruciate ligament reconstruction surgery. Am J Sports Med. 2018;46(7):1545–50. https://doi.org/10.1177/0363546518773757.
Webster KE, Feller JA, Kimp AJ, Whitehead TS. Low rates of return to preinjury sport after bilateral anterior cruciate ligament reconstruction. Am J Sports Med. 2018;47(2):334–8. https://doi.org/10.1177/0363546518813901.
Lentz TA, Zeppieri G Jr, Tillman SM, Indelicato PA, Moser MW, George SZ, Chmielewski TL. Return to preinjury sports participation following anterior cruciate ligament reconstruction: contributions of demographic, knee impairment, and self-report measures. J Orthop Sports Phys Ther. 2012;42(11):893–901. https://doi.org/10.2519/jospt.2012.4077.
Rosso F, Bonasia DE, Cottino U, Cambursano S, Dettoni F, Rossi R. Factors affecting subjective and objective outcomes and return to play in anterior cruciate ligament reconstruction: a retrospective cohort study. Joints. 2018;6(1):23–32. https://doi.org/10.1055/s-0038-1636931.
Sandon A, Werner S, Forssblad M. Factors associated with returning to football after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2015;23(9):2514–21. https://doi.org/10.1007/s00167-014-3023-4.
Baumeister J, Reinecke K, Weiss M. Changed cortical activity after anterior cruciate ligament reconstruction in a joint position paradigm: an EEG study. Scand J Med Sci Sports. 2008;18(4):473–84. https://doi.org/10.1111/j.1600-0838.2007.00702.x.
Baumeister J, Reinecke K, Schubert M, Weiss M. Altered electrocortical brain activity after ACL reconstruction during force control. J Orthop Res. 2011;29(9):1383–9. https://doi.org/10.1002/jor.21380.
Grooms DR, Page SJ, Nichols-Larsen DS, Chaudhari AM, White SE, Onate JA. Neuroplasticity associated with anterior cruciate ligament reconstruction. J Orthop Sports Phys Ther. 2017;47(3):180–9. https://doi.org/10.2519/jospt.2017.7003.
Kapreli E, Athanasopoulos S, Gliatis J, Papathanasiou M, Peeters R, Strimpakos N, Van Hecke P, Gouliamos A, Sunaert S. Anterior cruciate ligament deficiency causes brain plasticity: a functional MRI study. Am J Sports Med. 2009;37(12):2419–26. https://doi.org/10.1177/0363546509343201.
Lepley AS, Gribble PA, Thomas AC, Tevald MA, Sohn DH, Pietrosimone BG. Quadriceps neural alterations in anterior cruciate ligament reconstructed patients: a 6-month longitudinal investigation. Scand J Med Sci Sports. 2015;25(6):828–39. https://doi.org/10.1111/sms.12435.
Luc-Harkey BA, Harkey MS, Pamukoff DN, Kim RH, Royal TK, Blackburn JT, Spang JT, Pietrosimone B. Greater intracortical inhibition associates with lower quadriceps voluntary activation in individuals with ACL reconstruction. Exp Brain Res. 2017;235(4):1129–37. https://doi.org/10.1007/s00221-017-4877-8.
Miao X, Huang H, Hu X, Li D, Yu Y, Ao Y. The characteristics of EEG power spectra changes after ACL rupture. PLoS One. 2017;12(2):e0170455. https://doi.org/10.1371/journal.pone.0170455.
Swanik CB. Brains and sprains: the brain’s role in noncontact anterior cruciate ligament injuries. J Athl Train. 2015;50(10):1100–2. https://doi.org/10.4085/1062-6050-50.10.08.
Bien DP, Dubuque TJ. Considerations for late stage ACL rehabilitation and return to sport to limit re-injury risk and maximize athletic performance. Int J Sports Phys Ther. 2015;10(2):256–71.
Grooms D, Appelbaum G, Onate J. Neuroplasticity following anterior cruciate ligament injury: a framework for visual-motor training approaches in rehabilitation. J Orthop Sports Phys Ther. 2015;45(5):381–93. https://doi.org/10.2519/jospt.2015.5549.
Ahn JH, Kim JG, Wang JH, Jung CH, Lim HC. Long-term results of anterior cruciate ligament reconstruction using bone-patellar tendon-bone: an analysis of the factors affecting the development of osteoarthritis. Arthroscopy. 2012;28(8):1114–23. https://doi.org/10.1016/j.arthro.2011.12.019.
Barenius B, Ponzer S, Shalabi A, Bujak R, Norlen L, Eriksson K. Increased risk of osteoarthritis after anterior cruciate ligament reconstruction: a 14-year follow-up study of a randomized controlled trial. Am J Sports Med. 2014;42(5):1049–57. https://doi.org/10.1177/0363546514526139.
Cantin O, Lustig S, Rongieras F, Saragaglia D, Lefevre N, Graveleau N, Hulet C. Outcome of cartilage at 12 years of follow-up after anterior cruciate ligament reconstruction. OTSR. 2016;102(7):857–61. https://doi.org/10.1016/j.otsr.2016.06.011.
Claes S, Hermie L, Verdonk R, Bellemans J, Verdonk P. Is osteoarthritis an inevitable consequence of anterior cruciate ligament reconstruction? A meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2013;21(9):1967–76. https://doi.org/10.1007/s00167-012-2251-8.
Devitt BM, Bell SW, Webster KE, Feller JA, Whitehead TS. Surgical treatments of cartilage defects of the knee: systematic review of randomised controlled trials. Knee. 2017;24(3):508–17. https://doi.org/10.1016/j.knee.2016.12.002.
Gerhard P, Bolt R, Duck K, Mayer R, Friederich NF, Hirschmann MT. Long-term results of arthroscopically assisted anatomical single-bundle anterior cruciate ligament reconstruction using patellar tendon autograft: are there any predictors for the development of osteoarthritis? Knee Surg Sports Traumatol Arthrosc. 2013;21(4):957–64. https://doi.org/10.1007/s00167-012-2001-y.
Keays SL, Newcombe PA, Bullock-Saxton JE, Bullock MI, Keays AC. Factors involved in the development of osteoarthritis after anterior cruciate ligament surgery. Am J Sports Med. 2010;38(3):455–63. https://doi.org/10.1177/0363546509350914.
Li RT, Lorenz S, Xu Y, Harner CD, Fu FH, Irrgang JJ. Predictors of radiographic knee osteoarthritis after anterior cruciate ligament reconstruction. Am J Sports Med. 2011;39(12):2595–603. https://doi.org/10.1177/0363546511424720.
Shelbourne KD, Gray T. Minimum 10-year results after anterior cruciate ligament reconstruction: how the loss of normal knee motion compounds other factors related to the development of osteoarthritis after surgery. Am J Sports Med. 2009;37(3):471–80. https://doi.org/10.1177/0363546508326709.
Beynnon BD, Uh BS, Johnson RJ, Abate JA, Nichols CE, Fleming BC, Poole AR, Roos H. Rehabilitation after anterior cruciate ligament reconstruction. A prospective, randomized, double-blind comparison of programs administered over 2 different time periods. Am J Sports Med. 2005;33(3):347–59.
Beynnon BD, Johnson RJ, Abate JA, Fleming BC, Nichols CE. Treatment of anterior cruciate ligament injuries, part I. Am J Sports Med. 2005;33(10):1579–602.
Hui C, Salmon LJ, Kok A, Maeno S, Linklater J, Pinczewski LA. Fifteen-year outcome of endoscopic anterior cruciate ligament reconstruction with patellar tendon autograft for “isolated” anterior cruciate ligament tear. Am J Sports Med. 2011;39(1):89–98. https://doi.org/10.1177/0363546510379975.
Myklebust G, Bahr R. Return to play guidelines after anterior cruciate ligament surgery. Br J Sports Med. 2005;39(3):127–31. https://doi.org/10.1136/bjsm.2004.010900.
Smith MV, Nepple JJ, Wright RW, Matava MJ, Brophy RH. Knee osteoarthritis is associated with previous meniscus and anterior cruciate ligament surgery among elite college American football athletes. Sports Health. 2017;9(3):247–51. https://doi.org/10.1177/1941738116683146.
Theologis AA, Kuo D, Cheng J, Bolbos RI, Carballido-Gamio J, Ma CB, Li X. Evaluation of bone bruises and associated cartilage in anterior cruciate ligament-injured and -reconstructed knees using quantitative t(1rho) magnetic resonance imaging: 1-year cohort study. Arthroscopy. 2011;27(1):65–76. https://doi.org/10.1016/j.arthro.2010.06.026.
Weinstein AM, Rome BN, Reichmann WM, Collins JE, Burbine SA, Thornhill TS, Wright J, Katz JN, Losina E. Estimating the burden of total knee replacement in the United States. J Bone Joint Surg. 2013;95(5):385–92. https://doi.org/10.2106/JBJS.L.00206.
Makhni EC, Padaki AS, Petridis PD, Steinhaus ME, Ahmad CS, Cole BJ, Bach BR Jr. High variability in outcome reporting patterns in high-impact ACL literature. J Bone Joint Surg. 2015;97(18):1529–42. https://doi.org/10.2106/JBJS.O.00155.
Ardern CL, Sonesson S, Forssblad M, Kvist J. Comparison of patient-reported outcomes among those who chose ACL reconstruction or non-surgical treatment. Scand J Med Sci Sports. 2017;27(5):535–44. https://doi.org/10.1111/sms.12707.
Salmon LJ, Heath E, Akrawi H, Roe JP, Linklater J, Pinczewski LA. 20-year outcomes of anterior cruciate ligament reconstruction with hamstring tendon autograft: the catastrophic effect of age and posterior tibial slope. Am J Sports Med. 2018;46(3):531–43. https://doi.org/10.1177/0363546517741497.
Morgan MD, Salmon LJ, Waller A, Roe JP, Pinczewski LA. Fifteen-year survival of endoscopic anterior cruciate ligament reconstruction in patients aged 18 years and younger. Am J Sports Med. 2016;44(2):384–92. https://doi.org/10.1177/0363546515623032.
Shelbourne KD, Gray T, Haro M. Incidence of subsequent injury to either knee within 5 years after anterior cruciate ligament reconstruction with patellar tendon autograft. Am J Sports Med. 2009;37(2):246–51.
Takazawa Y, Ikeda H, Saita Y, Kawasaki T, Ishijima M, Nagayama M, Kaneko H, Kaneko K. Return to play of rugby players after anterior cruciate ligament reconstruction using hamstring autograft: return to sports and graft failure according to age. Arthroscopy. 2017;33(1):181–9. https://doi.org/10.1016/j.arthro.2016.06.009.
Wiggins AJ, Grandhi RK, Schneider DK, Stanfield D, Webster KE, Myer GD. Risk of secondary injury in younger athletes after anterior cruciate ligament reconstruction: a systematic review and meta-analysis. Am J Sports Med. 2016;44(7):1861–76. https://doi.org/10.1177/0363546515621554.
Grindem H, Snyder-Mackler L, Moksnes H, Engebretsen L, Risberg MA. Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction: the Delaware-Oslo ACL cohort study. Br J Sports Med. 2016;50(13):804–8. https://doi.org/10.1136/bjsports-2016-096031.
Webster KE, Feller JA, Leigh WB, Richmond AK. Younger patients are at increased risk for graft rupture and contralateral injury after anterior cruciate ligament reconstruction. Am J Sports Med. 2014;42(3):641–7. https://doi.org/10.1177/0363546513517540.
Kaeding CC, Pedroza AD, Reinke EK, Huston LJ, Consortium M, Spindler KP. Risk factors and predictors of subsequent ACL injury in either knee after ACL reconstruction: prospective analysis of 2488 primary ACL reconstructions from the moon cohort. Am J Sports Med. 2015;43(7):1583–90. https://doi.org/10.1177/0363546515578836.
Kyritsis P, Bahr R, Landreau P, Miladi R, Witvrouw E. Likelihood of ACL graft rupture: not meeting six clinical discharge criteria before return to sport is associated with a four times greater risk of rupture. Br J Sports Med. 2016;50(15):946–51. https://doi.org/10.1136/bjsports-2015-095908.
Kamath GV, Murphy T, Creighton RA, Viradia N, Taft TN, Spang JT. Anterior cruciate ligament injury, return to play, and reinjury in the elite collegiate athlete: analysis of an NCAA Division I Cohort. Am J Sports Med. 2014;42(7):1638–43. https://doi.org/10.1177/0363546514524164.
Lefevre N, Klouche S, Mirouse G, Herman S, Gerometta A, Bohu Y. Return to sport after primary and revision anterior cruciate ligament reconstruction: a prospective comparative study of 552 patients from the FAST Cohort. Am J Sports Med. 2017;45(1):34–41. https://doi.org/10.1177/0363546516660075.
Faltstrom A, Hagglund M, Magnusson H, Forssblad M, Kvist J. Predictors for additional anterior cruciate ligament reconstruction: data from the Swedish national ACL register. Knee Surg Sports Traumatol Arthrosc. 2016;24(3):885–94. https://doi.org/10.1007/s00167-014-3406-6.
Ardern CL, Taylor NF, Feller JA, Whitehead TS, Webster KE. Sports participation 2 years after anterior cruciate ligament reconstruction in athletes who had not returned to sport at 1 year: a prospective follow-up of physical function and psychological factors in 122 athletes. Am J Sports Med. 2015;43(4):848–56. https://doi.org/10.1177/0363546514563282.
Myklebust G, Holm I, Maehlum S, Engebretsen L, Bahr R. Clinical, functional, and radiologic outcome in team handball players 6 to 11 years after anterior cruciate ligament injury: a follow-up study. Am J Sports Med. 2003;31(6):981–9.
Mohtadi N, Chan D, Barber R, Paolucci EO. Reruptures, reinjuries, and revisions at a minimum 2-year follow-up: a randomized clinical trial comparing 3 graft types for ACL reconstruction. Clin J Sport Med. 2016;26(2):96–107. https://doi.org/10.1097/JSM.0000000000000209.
Park SY, Oh H, Park S, Lee JH, Lee SH, Yoon KH. Factors predicting hamstring tendon autograft diameters and resulting failure rates after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2013;21(5):1111–8. https://doi.org/10.1007/s00167-012-2085-4.
Thompson SM, Salmon LJ, Waller A, Linklater J, Roe JP, Pinczewski LA. Twenty-year outcome of a longitudinal prospective evaluation of isolated endoscopic anterior cruciate ligament reconstruction with patellar tendon or hamstring autograft. Am J Sports Med. 2016;44(12):3083–94. https://doi.org/10.1177/0363546516658041.
Pinczewski LA, Lyman J, Salmon LJ, Russell VJ, Roe J, Linklater J. A 10-year comparison of anterior cruciate ligament reconstructions with hamstring tendon and patellar tendon autograft: a controlled, prospective trial. Am J Sports Med. 2007;35(4):564–74.
Hettrich CM, Dunn WR, Reinke EK, Group M, Spindler KP. The rate of subsequent surgery and predictors after anterior cruciate ligament reconstruction: two- and 6-year follow-up results from a multicenter cohort. Am J Sports Med. 2013;41(7):1534–40. https://doi.org/10.1177/0363546513490277.
Schlumberger M, Schuster P, Schulz M, Immendorfer M, Mayer P, Bartholoma J, Richter J. Traumatic graft rupture after primary and revision anterior cruciate ligament reconstruction: retrospective analysis of incidence and risk factors in 2915 cases. Knee Surg Sports Traumatol Arthrosc. 2015;25(5):1535–41. https://doi.org/10.1007/s00167-015-3699-0.
Webster KE, Feller JA. Exploring the high reinjury rate in younger patients undergoing anterior cruciate ligament reconstruction. Am J Sports Med. 2016;44(11):2827–32. https://doi.org/10.1177/0363546516651845.
Persson A, Fjeldsgaard K, Gjertsen JE, Kjellsen AB, Engebretsen L, Hole RM, Fevang JM. Increased risk of revision with hamstring tendon grafts compared with patellar tendon grafts after anterior cruciate ligament reconstruction: a study of 12,643 patients from the Norwegian Cruciate Ligament Registry, 2004-2012. Am J Sports Med. 2014;42(2):285–91. https://doi.org/10.1177/0363546513511419.
Kamien PM, Hydrick JM, Replogle WH, Go LT, Barrett GR. Age, graft size, and Tegner activity level as predictors of failure in anterior cruciate ligament reconstruction with hamstring autograft. Am J Sports Med. 2013;41(8):1808–12. https://doi.org/10.1177/0363546513493896.
Maletis GB, Inacio MC, Funahashi TT. Risk factors associated with revision and contralateral anterior cruciate ligament reconstructions in the Kaiser Permanente ACLR registry. Am J Sports Med. 2015;43(3):641–7. https://doi.org/10.1177/0363546514561745.
Leys T, Salmon L, Waller A, Linklater J, Pinczewski L. Clinical results and risk factors for reinjury 15 years after anterior cruciate ligament reconstruction: a prospective study of hamstring and patellar tendon grafts. Am J Sports Med. 2012;40(3):595–605. https://doi.org/10.1177/0363546511430375.
Dekker TJ, Godin JA, Dale KM, Garrett WE, Taylor DC, Riboh JC. Return to sport after pediatric anterior cruciate ligament reconstruction and its effect on subsequent anterior cruciate ligament injury. J Bone Joint Surg. 2017;99(11):897–904. https://doi.org/10.2106/JBJS.16.00758.
Andernord D, Desai N, Bjornsson H, Ylander M, Karlsson J, Samuelsson K. Patient predictors of early revision surgery after anterior cruciate ligament reconstruction: a cohort study of 16,930 patients with 2-year follow-up. Am J Sports Med. 2015;43(1):121–7. https://doi.org/10.1177/0363546514552788.
Anand BS, Feller JA, Richmond AK, Webster KE. Return-to-sport outcomes after revision anterior cruciate ligament reconstruction surgery. Am J Sports Med. 2016;44(3):580–4. https://doi.org/10.1177/0363546515618381.
Kamath GV, Redfern JC, Greis PE, Burks RT. Revision anterior cruciate ligament reconstruction. Am J Sports Med. 2011;39(1):199–217. https://doi.org/10.1177/0363546510370929.
Marchant BG, Noyes FR, Barber-Westin SD, Fleckenstein C. Prevalence of nonanatomical graft placement in a series of failed anterior cruciate ligament reconstructions. Am J Sports Med. 2010;38(10):1987–96. https://doi.org/10.1177/0363546510372797.
MARS. Effect of graft choice on the outcome of revision anterior cruciate ligament reconstruction in the multicenter ACL Revision Study (MARS) Cohort. Am J Sports Med. 2014;42(10):2301–10. https://doi.org/10.1177/0363546514549005.
Noyes FR, Barber-Westin SD. Revision anterior cruciate ligament reconstruction: report of 11-year experience and results in 114 consecutive patients. Instr Course Lect. 2001;50:451–61.
Trojani C, Sbihi A, Djian P, Potel JF, Hulet C, Jouve F, Bussiere C, Ehkirch FP, Burdin G, Dubrana F, Beaufils P, Franceschi JP, Chassaing V, Colombet P, Neyret P. Causes for failure of ACL reconstruction and influence of meniscectomies after revision. Knee Surg Sports Traumatol Arthrosc. 2011;19(2):196–201. https://doi.org/10.1007/s00167-010-1201-6.
Andernord D, Desai N, Bjornsson H, Gillen S, Karlsson J, Samuelsson K. Predictors of contralateral anterior cruciate ligament reconstruction: a cohort study of 9061 patients with 5-year follow-up. Am J Sports Med. 2015;43(2):295–302. https://doi.org/10.1177/0363546514557245.
Faltstrom A, Kvist J, Gauffin H, Hagglund M. Female soccer players with anterior cruciate ligament reconstruction have a higher risk of new knee injuries and quit soccer to a higher degree than knee-healthy controls. Am J Sports Med. 2019;47(1):31–40. https://doi.org/10.1177/0363546518808006.
Ardern CL, Webster KE, Taylor NF, Feller JA. Return to the preinjury level of competitive sport after anterior cruciate ligament reconstruction surgery: two-thirds of patients have not returned by 12 months after surgery. Am J Sports Med. 2011;39(3):538–43. https://doi.org/10.1177/0363546510384798.
Ardern CL, Taylor NF, Feller JA, Webster KE. Fifty-five per cent return to competitive sport following anterior cruciate ligament reconstruction surgery: an updated systematic review and meta-analysis including aspects of physical functioning and contextual factors. Br J Sports Med. 2014;48(21):1543–52. https://doi.org/10.1136/bjsports-2013-093398.
Hamrin Senorski E, Samuelsson K, Thomee C, Beischer S, Karlsson J, Thomee R. Return to knee-strenuous sport after anterior cruciate ligament reconstruction: a report from a rehabilitation outcome registry of patient characteristics. Knee Surg Sports Traumatol Arthrosc. 2017;25(5):1364–74. https://doi.org/10.1007/s00167-016-4280-1.
Nawasreh Z, Logerstedt D, Cummer K, Axe MJ, Risberg MA, Snyder-Mackler L. Do patients failing return-to-activity criteria at 6 months after anterior cruciate ligament reconstruction continue demonstrating deficits at 2 years? Am J Sports Med. 2017;45(5):1037–48. https://doi.org/10.1177/0363546516680619.
Kay J, Memon M, Marx RG, Peterson D, Simunovic N, Ayeni OR. Over 90 % of children and adolescents return to sport after anterior cruciate ligament reconstruction: a systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2018;26(4):1019–36. https://doi.org/10.1007/s00167-018-4830-9.
Shelbourne KD, Benner RW, Gray T. Results of anterior cruciate ligament reconstruction with patellar tendon autografts: objective factors associated with the development of osteoarthritis at 20 to 33 years after surgery. Am J Sports Med. 2017;45(12):2730–8. https://doi.org/10.1177/0363546517718827.
Oiestad BE, Holm I, Engebretsen L, Aune AK, Gunderson R, Risberg MA. The prevalence of patellofemoral osteoarthritis 12 years after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2013;21(4):942–9. https://doi.org/10.1007/s00167-012-2161-9.
Holm I, Oiestad BE, Risberg MA, Gunderson R, Aune AK. No differences in prevalence of osteoarthritis or function after open versus endoscopic technique for anterior cruciate ligament reconstruction: 12-year follow-up report of a randomized controlled trial. Am J Sports Med. 2012;40(11):2492–8. https://doi.org/10.1177/0363546512458766.
Murray JR, Lindh AM, Hogan NA, Trezies AJ, Hutchinson JW, Parish E, Read JW, Cross MV. Does anterior cruciate ligament reconstruction lead to degenerative disease? Thirteen-year results after bone-patellar tendon-bone autograft. Am J Sports Med. 2012;40(2):404–13. https://doi.org/10.1177/0363546511428580.
Pernin J, Verdonk P, Si Selmi TA, Massin P, Neyret P. Long-term follow-up of 24.5 years after intra-articular anterior cruciate ligament reconstruction with lateral extra-articular augmentation. Am J Sports Med. 2010;38(6):1094–102. https://doi.org/10.1177/0363546509361018.
Inderhaug E, Strand T, Fischer-Bredenbeck C, Solheim E. Long-term results after reconstruction of the ACL with hamstrings autograft and transtibial femoral drilling. Knee Surg Sports Traumatol Arthrosc. 2013;21(9):2004–10. https://doi.org/10.1007/s00167-012-2330-x.
Struewer J, Ziring E, Frangen TM, Efe T, Meissner S, Buecking B, Bliemel C, Ishaque B. Clinical outcome and prevalence of osteoarthritis after isolated anterior cruciate ligament reconstruction using hamstring graft: follow-up after two and ten years. Int Orthop. 2013;37(2):271–7. https://doi.org/10.1007/s00264-012-1653-z.
Streich NA, Reichenbacher S, Barie A, Buchner M, Schmitt H. Long-term outcome of anterior cruciate ligament reconstruction with an autologous four-strand semitendinosus tendon autograft. Int Orthop. 2013;37(2):279–84. https://doi.org/10.1007/s00264-012-1757-5.
Janssen RP, du Mee AW, van Valkenburg J, Sala HA, Tseng CM. Anterior cruciate ligament reconstruction with 4-strand hamstring autograft and accelerated rehabilitation: a 10-year prospective study on clinical results, knee osteoarthritis and its predictors. Knee Surg Sports Traumatol Arthrosc. 2013;21(9):1977–88. https://doi.org/10.1007/s00167-012-2234-9.
Bjornsson H, Samuelsson K, Sundemo D, Desai N, Sernert N, Rostgard-Christensen L, Karlsson J, Kartus J. A randomized controlled trial with mean 16-year follow-up comparing hamstring and patellar tendon autografts in anterior cruciate ligament reconstruction. Am J Sports Med. 2016;44(9):2304–13. https://doi.org/10.1177/0363546516646378.
Sanders TL, Kremers HM, Bryan AJ, Fruth KM, Larson DR, Pareek A, Levy BA, Stuart MJ, Dahm DL, Krych AJ. Is anterior cruciate ligament reconstruction effective in preventing secondary meniscal tears and osteoarthritis? Am J Sports Med. 2016;44(7):1699–707. https://doi.org/10.1177/0363546516634325.
Ferretti A, Monaco E, Ponzo A, Basiglini L, Iorio R, Caperna L, Conteduca F. Combined intra-articular and extra-articular reconstruction in anterior cruciate ligament-deficient knee: 25 years later. Arthroscopy. 2016;32(10):2039–47. https://doi.org/10.1016/j.arthro.2016.02.006.
Hanypsiak BT, Spindler KP, Rothrock CR, Calabrese GJ, Richmond B, Herrenbruck TM, Parker RD. Twelve-year follow-up on anterior cruciate ligament reconstruction: long-term outcomes of prospectively studied osseous and articular injuries. Am J Sports Med. 2008;36(4):671–7.
Hoffelner T, Resch H, Moroder P, Atzwanger J, Wiplinger M, Hitzl W, Tauber M. No increased occurrence of osteoarthritis after anterior cruciate ligament reconstruction after isolated anterior cruciate ligament injury in athletes. Arthroscopy. 2012;28(4):517–25. https://doi.org/10.1016/j.arthro.2011.09.014.
Kessler MA, Behrend H, Henz S, Stutz G, Rukavina A, Kuster MS. Function, osteoarthritis and activity after ACL-rupture: 11 years follow-up results of conservative versus reconstructive treatment. Knee Surg Sports Traumatol Arthrosc. 2008;16(5):442–8.
Thompson S, Salmon L, Waller A, Linklater J, Roe J, Pinczewski L. Twenty-year outcomes of a longitudinal prospective evaluation of isolated endoscopic anterior cruciate ligament reconstruction with patellar tendon autografts. Am J Sports Med. 2015;43(9):2164–74. https://doi.org/10.1177/0363546515591263.
Wipfler B, Donner S, Zechmann CM, Springer J, Siebold R, Paessler HH. Anterior cruciate ligament reconstruction using patellar tendon versus hamstring tendon: a prospective comparative study with 9-year follow-up. Arthroscopy. 2011;27(5):653–65. https://doi.org/10.1016/j.arthro.2011.01.015.
Noyes FR, Barber-Westin SD. Meniscus tears: diagnosis, surgical techniques, and clinical outcomes. In: Noyes FR, Barber-Westin SD, editors. Noyes’ knee disorders: surgery, rehabilitation, clinical outcomes. 2nd ed. Philadelphia: Elsevier; 2017. p. 677–718.
Andreisek G, White LM, Sussman MS, Kunz M, Hurtig M, Weller I, Essue J, Marks P, Eckstein F. Quantitative MR imaging evaluation of the cartilage thickness and subchondral bone area in patients with ACL-reconstructions 7 years after surgery. Osteoarthr Cartil. 2009;17(7):871–8. https://doi.org/10.1016/j.joca.2008.05.024.
Culvenor AG, Collins NJ, Guermazi A, Cook JL, Vicenzino B, Khan KM, Beck N, van Leeuwen J, Crossley KM. Early knee osteoarthritis is evident one year following anterior cruciate ligament reconstruction: a magnetic resonance imaging evaluation. Arthritis Rheumatol. 2015;67(4):946–55. https://doi.org/10.1002/art.39005.
Hart AJ, Buscombe J, Malone A, Dowd GS. Assessment of osteoarthritis after reconstruction of the anterior cruciate ligament: a study using single-photon emission computed tomography at ten years. J Bone Joint Surg. 2005;87(11):1483–7.
Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957;16(4):494–502.
Irrgang JJ, Snyder-Mackler L, Wainner RS, Fu FH, Harner CD. Development of a patient-reported measure of function of the knee. J Bone Joint Surg. 1998;80(8):1132–45.
Ait Si Selmi T, Fithian D, Neyret P. The evolution of osteoarthritis in 103 patients with ACL reconstruction at 17 years follow-up. Knee. 2006;13(5):353–8. https://doi.org/10.1016/j.knee.2006.02.014.
Drogset JO, Grontvedt T, Robak OR, Molster A, Viset AT, Engebretsen L. A sixteen-year follow-up of three operative techniques for the treatment of acute ruptures of the anterior cruciate ligament. J Bone Joint Surg Am. 2006;88(5):944–52.
Mihelic R, Jurdana H, Jotanovic Z, Madjarevic T, Tudor A. Long-term results of anterior cruciate ligament reconstruction: a comparison with non-operative treatment with a follow-up of 17-20 years. Int Orthop. 2011;35(7):1093–7. https://doi.org/10.1007/s00264-011-1206-x.
Nakata K, Shino K, Horibe S, Tanaka Y, Toritsuka Y, Nakamura N, Koyanagi M, Yoshikawa H. Arthroscopic anterior cruciate ligament reconstruction using fresh-frozen bone plug-free allogeneic tendons: 10-year follow-up. Arthroscopy. 2008;24(3):285–91.
Salmon LJ, Russell VJ, Refshauge K, Kader D, Connolly C, Linklater J, Pinczewski LA. Long-term outcome of endoscopic anterior cruciate ligament reconstruction with patellar tendon autograft: minimum 13-year review. Am J Sports Med. 2006;34(5):721–32.
Noyes FR, Barber-Westin SD. Treatment of meniscus tears during anterior cruciate ligament reconstruction. Arthroscopy. 2012;28(1):123–30. https://doi.org/10.1016/j.arthro.2011.08.292.
Bisson LJ, Kluczynski MA, Hagstrom LS, Marzo JM. A prospective study of the association between bone contusion and intra-articular injuries associated with acute anterior cruciate ligament tear. Am J Sports Med. 2013;41(8):1801–7. https://doi.org/10.1177/0363546513490649.
Dunn WR, Spindler KP, Amendola A, Andrish JT, Kaeding CC, Marx RG, McCarty EC, Parker RD, Harrell FE Jr, An AQ, Wright RW, Brophy RH, Matava MJ, Flanigan DC, Huston LJ, Jones MH, Wolcott ML, Vidal AF, Wolf BR. Which preoperative factors, including bone bruise, are associated with knee pain/symptoms at index anterior cruciate ligament reconstruction (ACLR)? A Multicenter Orthopaedic Outcomes Network (MOON) ACLR Cohort Study. Am J Sports Med. 2010;38(9):1778–87. https://doi.org/10.1177/0363546510370279.
Nishimori M, Deie M, Adachi N, Kanaya A, Nakamae A, Motoyama M, Ochi M. Articular cartilage injury of the posterior lateral tibial plateau associated with acute anterior cruciate ligament injury. Knee Surg Sports Traumatol Arthrosc. 2008;16(3):270–4. https://doi.org/10.1007/s00167-007-0458-x.
Papalia R, Torre G, Vasta S, Zampogna B, Pedersen DR, Denaro V, Amendola A. Bone bruises in anterior cruciate ligament injured knee and long-term outcomes. A review of the evidence. Open Access J Sports Med. 2015;6:37–48. https://doi.org/10.2147/OAJSM.S75345.
Potter HG, Jain SK, Ma Y, Black BR, Fung S, Lyman S. Cartilage injury after acute, isolated anterior cruciate ligament tear: immediate and longitudinal effect with clinical/MRI follow-up. Am J Sports Med. 2012;40(2):276–85. https://doi.org/10.1177/0363546511423380.
Yoon JP, Chang CB, Yoo JH, Kim SJ, Choi JY, Choi JA, Seong SC, Kim TK. Correlation of magnetic resonance imaging findings with the chronicity of an anterior cruciate ligament tear. J Bone Joint Surg. 2010;92(2):353–60. https://doi.org/10.2106/JBJS.I.00031.
Yoon KH, Yoo JH, Kim KI. Bone contusion and associated meniscal and medial collateral ligament injury in patients with anterior cruciate ligament rupture. J Bone Joint Surg. 2011;93(16):1510–8. https://doi.org/10.2106/JBJS.J.01320.
Frobell RB. Change in cartilage thickness, posttraumatic bone marrow lesions, and joint fluid volumes after acute ACL disruption: a two-year prospective MRI study of sixty-one subjects. J Bone Joint Surg. 2011;93(12):1096–103. https://doi.org/10.2106/JBJS.J.00929.
Amano K, Huebner JL, Stabler TV, Tanaka M, McCulloch CE, Lobach I, Lane NE, Kraus VB, Ma CB, Li X. Synovial fluid profile at the time of anterior cruciate ligament reconstruction and its association with cartilage matrix composition 3 years after surgery. Am J Sports Med. 2018;46(4):890–9. https://doi.org/10.1177/0363546517749834.
Bigoni M, Sacerdote P, Turati M, Franchi S, Gandolla M, Gaddi D, Moretti S, Munegato D, Augusti CA, Bresciani E, Omeljaniuk RJ, Locatelli V, Torsello A. Acute and late changes in intraarticular cytokine levels following anterior cruciate ligament injury. J Orthop Res. 2013;31(2):315–21. https://doi.org/10.1002/jor.22208.
Cuellar VG, Cuellar JM, Golish SR, Yeomans DC, Scuderi GJ. Cytokine profiling in acute anterior cruciate ligament injury. Arthroscopy. 2010;26(10):1296–301. https://doi.org/10.1016/j.arthro.2010.02.011.
Elsaid KA, Fleming BC, Oksendahl HL, Machan JT, Fadale PD, Hulstyn MJ, Shalvoy R, Jay GD. Decreased lubricin concentrations and markers of joint inflammation in the synovial fluid of patients with anterior cruciate ligament injury. Arthritis Rheum. 2008;58(6):1707–15. https://doi.org/10.1002/art.23495.
Fang C, Johnson D, Leslie MP, Carlson CS, Robbins M, Di Cesare PE. Tissue distribution and measurement of cartilage oligomeric matrix protein in patients with magnetic resonance imaging-detected bone bruises after acute anterior cruciate ligament tears. J Orthop Res. 2001;19(4):634–41. https://doi.org/10.1016/S0736-0266(00)00039-5.
Higuchi H, Shirakura K, Kimura M, Terauchi M, Shinozaki T, Watanabe H, Takagishi K. Changes in biochemical parameters after anterior cruciate ligament injury. Int Orthop. 2006;30(1):43–7. https://doi.org/10.1007/s00264-005-0023-5.
Irie K, Tomatsu T. Atrophy of semitendinosus and gracilis and flexor mechanism function after hamstring tendon harvest for anterior cruciate ligament reconstruction. Orthopedics. 2002;25(5):491–5.
Lee JH, Ort T, Ma K, Picha K, Carton J, Marsters PA, Lohmander LS, Baribaud F, Song XY, Blake S. Resistin is elevated following traumatic joint injury and causes matrix degradation and release of inflammatory cytokines from articular cartilage in vitro. Osteoarthr Cartil. 2009;17(5):613–20. https://doi.org/10.1016/j.joca.2008.08.007.
Li H, Chen C, Chen S. Posttraumatic knee osteoarthritis following anterior cruciate ligament injury: potential biochemical mediators of degenerative alteration and specific biochemical markers. Biomed Rep. 2015;3(2):147–51. https://doi.org/10.3892/br.2014.404.
Lohmander LS, Atley LM, Pietka TA, Eyre DR. The release of crosslinked peptides from type II collagen into human synovial fluid is increased soon after joint injury and in osteoarthritis. Arthritis Rheum. 2003;48(11):3130–9. https://doi.org/10.1002/art.11326.
Lotz MK, Kraus VB. New developments in osteoarthritis. Posttraumatic osteoarthritis: pathogenesis and pharmacological treatment options. Arthritis Res Ther. 2010;12(3):211. https://doi.org/10.1186/ar3046.
Marks PH, Donaldson ML. Inflammatory cytokine profiles associated with chondral damage in the anterior cruciate ligament-deficient knee. Arthroscopy. 2005;21(11):1342–7. https://doi.org/10.1016/j.arthro.2005.08.034.
Mutsuzaki H, Sakane M, Honda K, Ikeda K, Hattori S, Ochiai N. Cell death and cell proliferation in cartilage layers in human anterior cruciate ligament tibial insertions after rupture. Connect Tissue Res. 2010;51(4):282–8. https://doi.org/10.3109/03008200903318303.
Papathanasiou I, Michalitsis S, Hantes ME, Vlychou M, Anastasopoulou L, Malizos KN, Tsezou A. Molecular changes indicative of cartilage degeneration and osteoarthritis development in patients with anterior cruciate ligament injury. BMC Musculoskelet Disord. 2016;17:21. https://doi.org/10.1186/s12891-016-0871-8.
Struglics A, Larsson S, Kumahashi N, Frobell R, Lohmander LS. Changes in cytokines and aggrecan ARGS neoepitope in synovial fluid and serum and in c-terminal crosslinking telopeptide of type II collagen and n-terminal crosslinking telopeptide of type I collagen in urine over five years after anterior cruciate ligament rupture: an exploratory analysis in the knee anterior cruciate ligament, nonsurgical versus surgical treatment trial. Arthritis Rheumatol. 2015;67(7):1816–25. https://doi.org/10.1002/art.39146.
Tiderius CJ, Olsson LE, Nyquist F, Dahlberg L. Cartilage glycosaminoglycan loss in the acute phase after an anterior cruciate ligament injury: delayed gadolinium-enhanced magnetic resonance imaging of cartilage and synovial fluid analysis. Arthritis Rheum. 2005;52(1):120–7. https://doi.org/10.1002/art.20795.
Noyes FR, Barber-Westin SD. Risks of future joint arthritis and reinjury after ACL reconstruction. In: Noyes FR, Barber-Westin SD, editors. ACL injuries in the female athlete: causes, impacts, and conditioning programs. 2nd ed; 2018. p. 67–93.
Noyes FR, Barber-Westin SD. Arthroscopic repair of meniscal tears extending into the avascular zone in patients younger than twenty years of age. Am J Sports Med. 2002;30(4):589–600.
Noyes FR, Barber-Westin SD. Meniscus tears: diagnosis, repair techniques, and clinical outcomes. In: Noyes FR, Barber-Westin SD, editors. Noyes’ knee disorders: surgery, rehabilitation, clinical outcomes. 2nd ed. Philadelphia: Elsevier; 2017. p. 677–718. https://doi.org/10.1016/b978-0-323-32903-3.00023-8.
Noyes FR, Barber-Westin SD. Arthroscopic repair of meniscus tears extending into the avascular zone with or without anterior cruciate ligament reconstruction in patients 40 years of age and older. Arthroscopy. 2000;16(8):822–9. https://doi.org/10.1053/jars.2000.19434.
Noyes FR, Chen RC, Barber-Westin SD, Potter HG. Greater than 10-year results of red-white longitudinal meniscal repairs in patients 20 years of age or younger. Am J Sports Med. 2011;39(5):1008–17. https://doi.org/10.1177/0363546510392014.
Rubman MH, Noyes FR, Barber-Westin SD. Arthroscopic repair of meniscal tears that extend into the avascular zone. A review of 198 single and complex tears. Am J Sports Med. 1998;26(1):87–95.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Noyes, F.R., Barber-Westin, S. (2019). Advantages and Potential Consequences of Return to Sport After ACL Reconstruction: Quality of Life, Reinjury Rates, and Knee Osteoarthritis. In: Noyes, F., Barber-Westin, S. (eds) Return to Sport after ACL Reconstruction and Other Knee Operations. Springer, Cham. https://doi.org/10.1007/978-3-030-22361-8_1
Download citation
DOI: https://doi.org/10.1007/978-3-030-22361-8_1
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-22360-1
Online ISBN: 978-3-030-22361-8
eBook Packages: MedicineMedicine (R0)