
Abstract
Purpose
To evaluate patellofemoral congruity after opening wedge high tibial osteotomy (OWHTO) and hybrid HTO.
Methods
Twenty-four knees with hybrid HTO and 24 with OWHTO were evaluated in this study. The Caton–Deschamps and modified Miura–Kawamura indices were used to evaluate pre- and post-operative patellar heights for both types of surgery. Tibial tuberosity–trochlear groove (TT–TG) distance, patellar tilt, and medial and lateral joint space at the patellofemoral joint were compared. Anterior knee pain was assessed using the Kujala anterior knee pain scale.
Results
There was no significant difference between the correction angles of the hybrid HTO and OWHTO. Pre- and post-operative values for the Caton–Deschamps and modified Miura–Kawamura indices in patients who underwent hybrid HTO changed from 0.90 to 0.94 and from 0.95 to 1.03, respectively, with no significant differences noted. Following OWHTO, these values decreased significantly from 0.91 to 0.73 and from 1.06 to 0.84, respectively (p < 0.01). The post-operative patellar height after OWHTO was significantly lower than that after hybrid HTO (p < 0.01). After hybrid HTO, the TT–TG distance decreased significantly from 11.4 to 7.4 (p < 0.01), but it did not change significantly after OWHTO. Although pre- and post-operative patellar tilt were not altered significantly in either group, the medial joint space of the patellofemoral joint was significantly increased post-operatively following hybrid HTO (p = 0.035). The pre-operative Kujala scores were significantly lower in the hybrid HTO group, but post-operative scores improved in both groups.
Conclusions
Hybrid HTO provides a better post-operative patellofemoral joint than does OWHTO with regard to patellar position and reduction of the TT–TG distance, as well as improved clinical outcomes. Hybrid HTO, rather than OWHTO, is the preferred technique for the treatment of varus knees combined with patellofemoral osteoarthritis.
Level of evidence
Retrospective comparative study, Level III.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
High tibial osteotomy (HTO) is recognised as a successful joint preservation surgery for knee osteoarthritis (OA) [14, 25]. The purpose of the HTO procedure is to realign the lower limb to shift the load distribution from the medial to the lateral compartment, thereby decreasing OA symptoms in the medial compartment of the knee [1, 4, 24]. However, opening wedge HTO (OWHTO) has been reported to induce unfavourable changes in patellofemoral mechanics [8, 28] due to a decrease in patellar height after OWHTO [3]. Consequently, the progression of patellofemoral OA after OWHTO has been widely discussed [9, 26]. Recently, HTO with a descending cut at the tibial tuberosity has been introduced for patellofemoral OA, because this procedure does not alter patellar height [16, 20]. While it might be true that this surgical technique does not reduce patellar height, patellofemoral joint congruity might not be improved in cases of symptomatic patellofemoral OA. Closing wedge HTO (CWHTO) is another procedure to address varus knee OA. Patellar height after CWHTO is elevated relative to the tibia [30], which creates a better patellofemoral joint congruity than OWHTO. However, CWHTO is known to result in several issues, such as leg shortening and step-off at the lateral cortex [31]. To reduce these issues, hybrid HTO, which was a novel surgical procedure that combines OWHTO and CWHTO, was established [29]. The hinge point is set at approximately two-thirds of the lateral distance along the proximal osteotomy line to combine the lateral closing and medial opening wedge osteotomy techniques. This is thought to maintain the appropriate positioning of the tibial tuberosity relative to the patellofemoral joint [29].
Although patellofemoral joint congruity is an important point to consider in improving clinical outcomes with HTO, it has not been assessed in any studies, including changes in the tibial tuberosity–trochlear groove (TT–TG) distance and joint space narrowing after hybrid HTO and OWHTO. Therefore, the purpose of this study was to compare changes in patellar height after hybrid HTO and OWHTO based on the hypothesis that hybrid HTO is preferable to OWHTO for the treatment of varus knees combined with patellofemoral osteoarthritis.
Materials and methods
One hundred and four knees that had undergone HTO from 2012 to 2016 were initially enrolled in this study. Pre-operative digital planning software (TraumaCaD, BRAINLAB, Feldkirchen, Germany) was used. First, it was planned to pass the post-operative mechanical axis through the lateral eminence of the proximal tibia in the picture archiving and communication system (PACS) [13]. Double-level osteotomy was selected when the planning indicated that the post-operative medial proximal tibial angle (MPTA) would have been greater than 95°. When the projected MPTA was less than 95°, OWHTO was indicated when the severity of patellofemoral OA was less than stage III, and hybrid HTO was selected when the severity was > stage III [22] or if patients complained of patellofemoral pain and crepitus with OA. As a result, 77 knees (43 males and 34 females) that had undergone OWHTO and 24 knees (13 males and 11 females) that had undergone hybrid HTO were identified. Three knees (1 male and 2 females) had undergone double-level HTO. In our final analysis, 24 knees that had undergone OWHTO were matched by age and gender with 24 knees that had undergone hybrid HTO. Patellofemoral joint congruity between the two groups was compared. Both groups consisted of 13 males and 11 females, while the average patient age was 66.9 (range 44–78) years in the hybrid HTO group and 66.0 (range 44–76) years in the OWHTO group.
Diagnostic and radiographic measurements
Coronal knee alignment after hybrid HTO and OWHTO was evaluated by the percent of mechanical axis (%MA); femorotibial angle (FTA), which is the lateral angle between the centreline of the femur and the tibia on the coronal radiograph in the standing position [15]; and MPTA, whereas sagittal alignment was assessed by the posterior tibial slope [18]. Patellar height was evaluated radiographically using the Caton–Deschamps index [5, 6] and modified Miura–Kawamura index [16]. These measurements are depicted in lateral radiographs in 30° of knee flexion, as shown in Fig. 1a–d. The TT–TG distance was assessed using three-dimensional CT (Fig. 2a–d). Patellar tilt and joint space narrowing, which were measured from the centre of the medial and lateral facets to the patella by drawing a perpendicular line, were also evaluated (Fig. 3a–d) [21]. Clinical outcomes, including anterior knee pain, were assessed using the Kujala anterior knee pain scale [10, 17]. All parameters were measured on radiographs which were taken pre-operatively and at the end of the follow-up period, and were evaluated by two orthopedic surgeons who were blinded to the patients’ information. The mean follow-up duration was 31.0 (range 21–48) months.

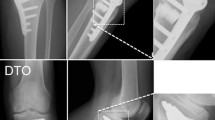
Patellar height measurement with hybrid and opening wedge HTO. Pre- and post-operative patellar heights are evaluated with the Caton–Deschamps index (B/A) (a, b), and modified Miura–Kawamura index (C/A) (c, d)

Tibial tuberosity–trochlear groove (TT–TG) distance measurement with hybrid and opening wedge HTO. Pre- and post-operative patellar height are shown in hybrid HTO (a, b) and OWHTO (c, d)

Patellofemoral joint space measurement. a–d Medial and lateral joint space was measured from the centre of the joint surface to the patella by drawing a perpendicular line. Pre- and post-operative joint space width for hybrid HTO (a, b) and OWHTO (c, d) is shown
Surgical procedure
Biplane OWHTO was performed to correct the mechanical axis based on pre-operative planning [19] and the osteotomy was fixed with a locking plate. The surgical procedure for hybrid HTO was performed as previously reported [29]. Briefly, an approximately 10-mm length of the distal third of the fibula was removed and the proximal lateral tibia was exposed by separation of the attachment of the tibialis anterior muscle. Under fluoroscopy, hybrid HTO, a 33% medial opening combined with a 67% lateral closed wedge, was performed. A locking plate was used for fixation of the osteotomy site. Rehabilitation was initiated on post-operative day 1 with 50% weight-bearing allowed initially and full weight-bearing permitted starting on day 14 for both osteotomy procedures.
This study was performed in accordance with a protocol and was approved by the Institutional Review Board of Osaka Medical College (No. Rin-217).
Statistical analysis
A power analysis was performed for the primary comparison of interest (post-operative TT–TG distance and the Caton–Deschamps index between hybrid HTO and OWHTO). The power analysis was set up as follows: α = 0.05 and power = 0.9. As a result, a minimum of 32 knees for TT–TG distance and 24 knees for the Caton–Deschamps index were required for the total sample size based on G*power (version 3.1.9.2) [7]. On the basis of the power analysis, a sample size of 48 was considered adequate. A paired t test was performed to compare the pre- and post-operative radiographic results using JMP Pro (version 11.2.0, SAS, Cary, NC, USA). P values < 0.05 were considered statistically significant.
Results
The mean (± standard deviation) body mass index was 24.5 ± 4.4 kg/m2 for those who underwent hybrid HTO and 24.0 ± 2.4 kg/m2 for those who underwent OWHTO. Four patients had Kellgren–Lawrence grade II OA, 10 had grade III OA, and 10 had grade IV OA in the hybrid HTO group, while 3 had grade II OA, 12 had grade III OA, and 9 had grade IV OA in the OWHTO group. There were no significant differences in baseline characteristics between the two groups (Table 1). However, patellofemoral OA was more severe in those that underwent hybrid HTO than OWHTO (Table 1, p = 0.003). The average correction angle for hybrid HTO was 11.0 ± 2.9°, which was not significantly different than the average correction angle for OWHTO (10.6 ± 2.6°, Table 2). Regarding the intra- and inter-observer reliability of these parameters, pre- and post-operative %MA, FTA, MPTA, and posterior tibial slope were not significantly different between the hybrid HTO and OWHTO groups (Table 2). The Caton–Deschamps and modified Miura–Kawamura indices decreased significantly from 0.91 ± 0.12 to 0.73 ± 0.15 and from 1.06 ± 0.09 to 0.84 ± 0.07 after OWHTO, respectively (Table 3, p < 0.01), whereas no difference was seen after hybrid HTO (Table 3). Post-operatively, these indices were significantly different between the two groups (Table 3, p < 0.001). TT–TG distance after hybrid HTO decreased significantly from 11.4 ± 2.2 to 7.4 ± 3.0 (p < 0.01), whereas no difference was noted following OWHTO (Table 4). Although pre- and post-operative patellar tilt were not altered in either group, post-operative medial joint space at the patellofemoral joint was significantly increased with hybrid HTO compared to OWHTO (Table 5, p = 0.035). The pre-operative Kujala scores were significantly lower in the hybrid HTO group than in the OWHTO group (Table 5, p = 0.007); however, outcomes improved in both groups after HTO, and there were no significant differences between the groups post-operatively (Table 5). All radiographic parameters demonstrated good (0.5–0.75)-to-excellent (> 0.75) intra- and inter-observer reliability (Table 6).
Discussion
The most important finding of this study is that hybrid HTO is the better surgical procedure for improving patellofemoral joint congruity with regards to patellar height and reduction of the TT–TG distance as compared with OWHTO. Hybrid HTO has the potential to improve the pre-operative medial and patellofemoral OA symptoms.
The advantages of hybrid HTO, which are first reported by Takeuchi et al. [29], are the removal of a smaller wedge of bone from the lateral osteotomy site and the preservation of pre-operative leg length compared with CWHTO. Patellar height might be diminished after hybrid HTO, because the insertion of the patellar tendon is elevated anteriorly and repositioned proximally during the hybrid HTO procedure.
Several reports have described changes in post-operative patellar height after HTO procedures [12, 18, 23] and the degree of change is correlated with the magnitude of the correction angle [2, 30]. Gaasbeek et al. compared patellar height before and after OWHTO and CWHTO and reported that the patella descended after OWHTO and ascended after CWHTO. Moreover, they reported that a larger correction angle resulted in greater alterations in patellar height after both [8]. The current study was able to compare the correction angle between two types of procedures, because the two procedure groups were matched based on patient characteristics. Consequently, it was clear that patellar height was significantly decreased after OWHTO, whereas no change occurred after hybrid HTO.
A descending cut of the tibial tuberosity with OWHTO might be another option for maintaining patellar height [16, 20]. Descending OWHTO preserves, whereas ascending OWHTO decreases patellar height according to the Caton–Deschamps index [16]. This has been described in both coronal and sagittal alignments as evaluated by several parameters; however, TT–TG distance has not been evaluated after HTO. TT–TG distance has already been described in varus OA and correlated with the severity of patellofemoral OA [22]. Earlier findings indicated that lateralization of the tibial tuberosity resulted in the deterioration of patellofemoral OA and that hybrid HTO is able to transfer the tibial tuberosity in a direction of medialisation, reducing patellofemoral contact pressures [27], unlike descending OWHTO. Modifications of the OWHTO technique might be necessary in patients with symptomatic patellofemoral OA. Hybrid HTO can correct the medialisation of the tibial tuberosity and this indicates that hybrid HTO is the better surgical option for varus knees with symptomatic patellofemoral OA.
Several parameters have been used to evaluate patellar height after HTO [12, 18]. The method that we chose, the Caton–Deschamps index, was the first used to assess patellar height after HTO by Tigani et al. [30]. In addition, Amzallag et al. reported patellar heights after HTO and determined that the Caton–Deschamps index was more reproducible [2]. The modified Miura–Kawamura index has been recently used to focus on evaluating patellar height after HTO, because it is not affected by tibial factors [18]. In the current study, the Caton–Deschamps and modified Miura–Kawamura indices showed similar changes, because alteration of the posterior tibial slope was similar between hybrid HTO and OWHTO. Both parameters might be useful if the pre- and post-operative posterior tibial slope is well controlled.
The grade of patellofemoral OA in the hybrid HTO group was more severe than that in the OWHTO group, and the pre-operative Kujala score was lower in the hybrid HTO group than in the OWHTO group. However, post-operative scores between the groups were not different. These findings indicate that hybrid HTO might be a potential therapy for patellofemoral OA rather than OWHTO.
Femoral anteversion is associated with trochlear morphology and tibiofemoral contact pressures [11, 32]. Although hybrid HTO has the potential to address symptomatic patellofemoral OA in varus knees, hybrid HTO should not be considered for symptomatic patellofemoral OA in varus knees that are possibly affected by femoral anteversion.
Conclusion
Improved patellofemoral joint congruity is considered an advantage of hybrid HTO over OWHTO. Hybrid high tibial osteotomy is superior to medial opening high tibial osteotomy in patients with symptomatic varus knee combined with patellofemoral OA.
Abbreviations
- CWHTO:
-
Closing wedge high tibial osteotomy
- FTA:
-
Femorotibial angle
- HTO:
-
High tibial osteotomy
- MPTA:
-
Medial proximal tibial angle
- OA:
-
Osteoarthritis
- OWHTO:
-
Opening wedge high tibial osteotomy
- PACS:
-
Picture archiving and communication system
- %MA:
-
Percent of mechanical axis
- TT–TG:
-
Tibial tuberosity–trochlear groove
References
Akizuki S, Shibakawa A, Takizawa T, Yamazaki I, Horiuchi H (2008) The long-term outcome of high tibial osteotomy. J Bone Joint Surg Br 90:592–596
Amzallag J, Pujol N, Maqdes A, Beaufils P, Judet T, Catonne Y (2013) Patellar height modification after high tibial osteotomy by either medial opening-wedge or lateral closing-wedge osteotomies. Knee Surg Sports Traumatol Arthrosc 21:255–259
Bin S-I, Kim H-J, Ahn H-S, Rim DS, Lee D-H (2016) Changes in patellar height after opening wedge and closing wedge high tibial osteotomy: a meta-analysis. Arthroscopy 32:2393–2400
Bode G, Heyden von J, Pestka J, Schmal H, Salzmann G, Südkamp N, Niemeyer P (2015) Prospective 5-year survival rate data following open-wedge valgus high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc 23:1949–1955
Caton J, Deschamps G, Chambat P, Lerat JL, Dejour H (1982) Patella infera. Apropos of 128 cases. Rev Chir Orthop Reparatrice Appar Mot 68:317–325
Dejour H, Walch G, Nove-Josserand L, Guier C (1994) Factors of patellar instability: an anatomic radiographic study. Knee Surg Sports Traumatol Arthrosc 2:19–26
Faul F, Erdfelder E, Buchner A, Lang A-G (2009) Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav Res Methods 41:1149–1160
Gaasbeek R, Welsing R, Barink M, Verdonschot N, van Kampen A (2007) The influence of open and closed high tibial osteotomy on dynamic patellar tracking: a biomechanical study. Knee Surg Sports Traumatol Arthrosc 15:978–984
Gaasbeek RDA, Sonneveld H, van Heerwaarden RJ, Jacobs WCH, Wymenga AB (2004) Distal tuberosity osteotomy in open wedge high tibial osteotomy can prevent patella infera: a new technique. Knee 11:457–461
Ittenbach RF, Huang G, Barber Foss KD, Hewett TE, Myer GD (2016) Reliability and validity of the anterior knee pain scale: applications for use as an epidemiologic screener. PLoS One 11:e0159204
Kenawey M, Liodakis E, Krettek C, Ostermeier S, Horn T, Hankemeier S (2011) Effect of the lower limb rotational alignment on tibiofemoral contact pressure. Knee Surg Sports Traumatol Arthrosc 19:1851–1859
Kesmezacar H, Erginer R, Ogut T, Seyahi A, Babacan M, Tenekecioglu Y (2005) Evaluation of patellar height and measurement methods after valgus high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc 13:539–544
Kim H-J, Lee H-J, Shin J-Y, Park K-H, Min S-G, Kyung HS (2017) Preoperative planning using the picture archiving and communication system technique in high tibial osteotomy. J Orthop Surg (Hong Kong) 25:2309499016684701
Kohn L, Sauerschnig M, Iskansar S, Lorenz S, Meidinger G, Imhoff AB, Hinterwimmer S (2013) Age does not influence the clinical outcome after high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc 21:146–151
Koshino T (1982) The treatment of spontaneous osteonecrosis of the knee by high tibial osteotomy with and without bone-grafting or drilling of the lesion. J Bone Joint Surg Am 64:47–58
Krause M, Drenck TC, Korthaus A, Preiss A, Frosch K-H, Akoto R (2018) Patella height is not altered by descending medial open-wedge high tibial osteotomy (HTO) compared to ascending HTO. Knee Surg Sports Traumatol Arthrosc 26:1859–1866
Kujala UM, Jaakkola LH, Koskinen SK, Taimela S, Hurme M, Nelimarkka O (1993) Scoring of patellofemoral disorders. Arthroscopy 9:159–163
LaPrade RF, Oro FB, Ziegler CG, Wijdicks CA, Walsh MP (2010) Patellar height and tibial slope after opening-wedge proximal tibial osteotomy: a prospective study. Am J Sports Med 38:160–170
Lobenhoffer P, Agneskirchner JD (2003) Improvements in surgical technique of valgus high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc 11:132–138
Monllau JC, Erquicia JI, Ibañez F, Ibañez M, Gelber PE, Masferrer-Pino A, Pelfort X (2017) Open-wedge valgus high tibial osteotomy technique with inverted L-shaped configuration. Arthroscopy Techniques 6:e2161–e2167
Otsuki S, Nakajima M, Oda S, Hoshiyama Y, Fujiwara K, Jotoku T, Neo M (2013) Three-dimensional transfer of the tibial tuberosity for patellar instability with patella alta. J Orthop Sci 18:437–442
Otsuki S, Nakajima M, Okamoto Y, Oda S, Hoshiyama Y, Iida G, Neo M (2014) Correlation between varus knee malalignment and patellofemoral osteoarthritis. Knee Surg Sports Traumatol Arthrosc 24:176–181
Portner O (2014) High tibial valgus osteotomy: closing, opening or combined? Patellar height as a determining factor. Clin Orthop Relat Res 472:3432–3440
Saier T, Minzlaff P, Feucht MJ, Lämmle L, Burghoff M, Ihle C, Imhoff AB, Hinterwimmer S (2017) Health-related quality of life after open-wedge high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc 25:934–942
Schallberger A, Jacobi M, Wahl P, Maestretti G, Jakob RP (2011) High tibial valgus osteotomy in unicompartmental medial osteoarthritis of the knee: a retrospective follow-up study over 13–21 years. Knee Surg Sports Traumatol Arthrosc 19:122–127
Scuderi GR, Windsor RE, Insall JN (1989) Observations on patellar height after proximal tibial osteotomy. J Bone Joint Surg Am 71:245–248
Stephen JM, Kittl C, Williams A, Zaffagnini S, Marcheggiani Muccioli GM, Fink C, Amis AA (2016) Effect of medial patellofemoral ligament reconstruction method on patellofemoral contact pressures and kinematics. Am J Sports Med 44:1736–1194
Stoffel K, Willers C, Korshid O, Kuster M (2007) Patellofemoral contact pressure following high tibial osteotomy: a cadaveric study. Knee Surg Sports Traumatol Arthrosc 15:1094–1100
Takeuchi R, Ishikawa H, Miyasaka Y, Sasaki Y, Kuniya T, Tsukahara S (2014) A novel closed-wedge high tibial osteotomy procedure to treat osteoarthritis of the knee: hybrid technique and rehabilitation measures. Arthroscopy Techniques 3:e431–e437
Tigani D, Ferrari D, Trentani P, Barbanti-Brodano G, Trentani F (2001) Patellar height after high tibial osteotomy. Int Orthop 24:331–334
Tunggal JAW, Higgins GA, Waddell JP (2010) Complications of closing wedge high tibial osteotomy. Int Orthop 34:255–261
Wright SJ, Boymans TAEJ, Grimm B, Miles AW, Kessler O (2014) Strong correlation between the morphology of the proximal femur and the geometry of the distal femoral trochlea. Knee Surg Sports Traumatol Arthrosc 22:2900–2910
Acknowledgements
We thank Maki Miyaki for her expert technical assistance with the statistical analysis.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Contributions
Designed the study: SO, TM, KN, and YO. Analysed the data: SO, TM, KN, YO, NO, and HW. Wrote the manuscript: SO, TM, KN, YO, NO, HW, and MN. Supervised the study: TM, YO, and MN. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The author(s) declare no potential conflicts of interest with respect to research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Rights and permissions
About this article

Cite this article
Otsuki, S., Murakami, T., Okamoto, Y. et al. Hybrid high tibial osteotomy is superior to medial opening high tibial osteotomy for the treatment of varus knee with patellofemoral osteoarthritis. Knee Surg Sports Traumatol Arthrosc 27, 1332–1338 (2019). https://doi.org/10.1007/s00167-018-5015-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-018-5015-2