
Abstract
Introduction
Resection for hilar cholangiocarcinoma is the single hope for long-term survival.
Methods
Ninety patients underwent curative intent surgery for hilar cholangiocarcinoma between 1996 and 2012. The potential prognostic factors were assessed by univariate (Kaplan–Meier curves and log-rank test) and multivariate analyses (Cox proportional hazards model).
Results
The median overall and disease-free survivals were 26 and 17 months, respectively. The multivariate analysis identified R0 resection (HR = 0.03, 95 % CI 0–0.19, p < 0.001), caudate lobe invasion (HR = 6.33, 95 % CI 1.31–30.46, p = 0.021), adjuvant gemcitabine-based chemotherapy (HR = 0.38, 95 % CI 0.15–0.94, p = 0.037), and the neutrophil-to-lymphocyte ratio (HR = 0.78, 95 % CI 0.62–0.98, p = 0.036) as independent prognostic factors for disease-free survival. The independent prognostic factors for overall survival were R0 resection (HR = 0.03, 95 % CI 0–0.22, p < 0.001), caudate lobe invasion (HR = 11.75, 95 % CI 1.65–83.33, p = 0.014), and adjuvant gemcitabine-based chemotherapy (HR = 0.19, 95 % CI 0.06–0.56, p = 0.003).
Conclusions
The negative resection margin represents the most important prognostic factor. Adjuvant gemcitabine-based chemotherapy appears to benefit survival. The neutrophil-to-lymphocyte ratio may potentially be used to stratify patients for future clinical trials.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hilar cholangiocarcinoma is the most frequently identified cholangiocarcinoma1 and refers to malignant tumors that arise from the biliary confluence and may extend to the left and/or the right hepatic ducts. These tumors are widely considered to have a worse prognosis than intrahepatic or distal cholangiocarcinomas2 because the disease is often advanced at presentation and requires demanding surgical techniques of resection and there is a lack of effective adjuvant therapies.3 Surgery represents the single hope for a long-term survival.4, 5 The surgery for hilar cholangiocarcinomas has evolved significantly over the years1, 6 and includes the resection of the extrahepatic bile duct, regional lymphadenectomy, caudate lobectomy and, most frequently, hepatectomy.7 Liver transplant has been associated with very good outcome in highly selected patients.8
The role of the systemic inflammatory response as a predictor of the long-term outcome for patients resected for cancer has been previously demonstrated for colorectal cancer, liver metastases, and gastro-esophageal cancer,9 but a limited number of studies have investigated the biliary malignancies and the available studies have mainly focused on intrahepatic cholangiocarcinoma10 and ampullary tumors.11
The aim of the present study was to identify the prognostic factors for overall and disease-free survival after curative intent resection for Klatskin tumors in a large, single-center study. Moreover, the impact of systemic inflammation on long-term outcome was assessed with well-established preoperative markers.
Materials and Methods
One hundred ninety-seven patients were surgically treated for a presumed diagnosis of hilar cholangiocarcinoma at our institution between 1996 and March 1, 2012. Patients with gallbladder or intrahepatic cholangiocarcinoma invading the hilum were excluded. Sixty-three patients (32 %) were preoperatively assessed as unresectable and underwent palliative surgery, while 134 patients (68 %) were surgically explored with a curative intent. Furthermore, 41 patients (31 %) were intraoperatively assessed as unresectable and underwent palliative surgery, while 93 patients (69 %) underwent resection. Benign hilar lesions were identified in three of the patients in the resected group (3.3 %). The final pathological diagnosis of hilar cholangiocarcinoma was established in 90 patients who were further analyzed (Fig. 1). The criteria for unresectability that were used in the present series are shown in Table 1. The data for the 90 resected hilar cholangiocarcinomas were retrospectively assessed from a prospectively gathered electronic database that included demographic and pre-, intra-, and postoperative parameters. The study was approved by the Ethics Committee at our institution.

Flow chart of patients surgically treated for hilar cholangiocarcinoma at Fundeni Clinical Institute (1996–2012)
The clinical and anatomical assessment of these tumors was made using the Bismuth–Corlette classification, while The American Joint Committee on Cancer TNM Staging System (seventh edition) was used for tumor staging.12 Preoperative biliary drainage was selectively used only for patients with cholangitis and impaired renal function.
Postoperative complications were assessed with the Dindo–Clavien classification13 and the International Study Group of Liver Surgery definitions and severity grading for post-hepatectomy liver failure,14 bile leakage,15 and post-hepatectomy hemorrhage.16 In patients with more than one postoperative complication, the highest grade of severity was considered. Postoperative mortality was defined as the 60-day mortality rate.
Statistical Analysis
The data are expressed as number (percentage) and median (range). The univariate analysis for potential prognostic factors utilized Kaplan–Meier curves and the log-rank test. For continuous variables, the median was used as the cut-off point for dividing the patients into subgroups. The multivariate analysis used a Cox proportional hazards model to analyze variables with p values less than 0.10 in the univariate analysis, after elimination of intercorrelated factors. Pearson’s correlation coefficient was used for continuous variables, while Spearman’s rho correlation coefficient was used for categorical variables. A p value less than 0.05 was considered statistically significant. The statistical analysis was performed with SPSS version 17.0 software (SPSS Inc., Chicago, IL, USA).
Results
Demographic and Preoperative Data
The median age was 57.5 years (range, 24–77), with the male gender predominating (52 patients—58 %). Most of the patients presented with jaundice (85 patients—94 %), and 24 patients (27 %) showed signs of cholangitis. The cholangitis was due to the disease in 14 patients (16 %) and related to biliary drainage in 10 patients (11 %).
Preoperative biliary drainage was performed for 26 patients (29 %); drainage was performed percutaneously (eight patients—9 %), endoscopically (five patients—6 %), or by previous surgery (13 patients—14 %). Only eight patients (9 %) were considered for preoperative biliary drainage in our unit (due to cholangitis with impaired renal function); 10 other patients had already received biliary drainage during previous surgical exploration (11 %) and eight patients (9 %) were referred from gastroentereologists with previous palliation of jaundice. Nineteen patients (21 %) had previously received exploratory surgery in another unit.
The preoperative median serum bilirubin level was 10.4 mg/dl (range, 0.6–35 mg/dl), hemoglobin level was 12.5 g/dl (range, 7.1–16 g/dl), and the CA 19-9 serum level was 200 UI/ml (range, 3–5,000 UI/ml). The markers of systemic inflammation were assessed no more than 7 days prior to resection and included the white blood cell count (median, 8,000/μl; range, 5,100–37,000), neutrophil count (5,550/μl; range, 3,400–33,300), lymphocyte count (1,700/μl; range, 800–2,800), platelet count (312,000/μl; range, 170,000–700,000), serum albumin level (4 g/dl; range, 2–5.4), neutrophil-to-lymphocyte ratio (3.3; range, 1.3–23.2), and thrombocyte-to-lymphocyte ratio (183.9; range, 63.1–700).9
Operative Data
The Bismuth classification of the tumors and the surgical procedures are shown in Table 2. The standard lymphadenectomy (performed in 87 patients—97 %) included the lymph nodes from the hepato-duodenal ligament, the common hepatic artery, the posterior surface of the pancreatic head, and right side of the celiac trunk.
Vascular resection was performed in 15 patients (17 %) for presumed invasion into the portal vein (12 patients—13 %) or hepatic artery (three patients—3 %). Caudate lobectomy was performed in 45 patients (50 %). The median intraoperative blood loss was 600 ml (range, 100–12,000 ml) and 56 patients (62 %) required peroperative blood transfusions. The median operating time was 270 min (range, 120–620 min).
Pathology Data
Most of the tumors had an infiltrative phenotype (53 patients—59 %) but the nodular type was encountered in 30 patients (33 %). The papillary phenotype was only noticed in seven patients (8 %). The median tumor diameter was 2.5 cm (range, 0.4–5 cm). While most of the tumors were adenocarcinomas (87 patients—97 %), three of the patients (3 %) had squamous cell carcinoma. Most of the tumors were well-differentiated G1 (53 patients—59 %), while moderately differentiated G2 were 27 patients (30 %) and poorly differentiated G3 10 patients (11 %). Perineural invasion was observed in 39 patients (43 %).
Eighteen patients were assessed as T1 (20 %), 32 patients as T2 (36 %), 35 patients as T3 (39 %), and five patients as T4 (5 %). Lymph node metastases were present in 37 patients (41 %) and the status of loco-regional lymph nodes could not be assessed in three patients (3 %). The median number of harvested lymph nodes was 4 (range, 1–22), and the median lymph node ratio was 0.25 (range, 0–1).
Six patients (7 %) from the present study had one to three metastases that were removed with the operative specimen. The TNM staging system classified 16 patients as stage I (19 %), 20 patients as stage II (22 %), 13 patients as stage IIIa (14 %), 28 patients as stage IIIb (31 %), four patients as stage IVa (4 %), and six patients as stage IVb (7 %). The stage could not be assessed in three patients (3 %) due to missing lymph node data.
A curative resection (i.e., R0—no microscopic residual tumor) was achieved in 68 patients (75 %), while 22 patients (25 %) were assessed as R1 (microscopic residual tumor). The residual microscopic tumor was mainly observed in the liver (17 patients—19 %), while five patients (5 %) had an R1 on the biliary side.
Ten of the 15 patients with associated vascular resections (67 %) had microscopically confirmed tumor invasion (PV1—eight patients, PV0—four patients, HA1—two patients, HA0—one patient). Caudate lobe invasion was histologically confirmed in 11 of the 45 patients with caudate lobectomy (22.2 %).
Postoperative Morbidity and Mortality
Complications occurred in 48 patients (53 %). The Dindo–Clavien classification classified nine patients as grade I (10 %), 12 patients as grade II (13 %), six patients as grade IIIa (7 %), seven patients as grade IIIb (8 %), six patients as grade IVa (7 %), and one patient as grade IVb (1 %). The median postoperative hospital stay was 15 days (range, 1–65 days). Re-laparotomy was necessary in 17 patients (19 %) due to complications.
A postoperative bile leak was the most frequent complication (27 patients—30 %): grade A—three patients (3 %), grade B—19 patients (21 %), and grade C—five patients (5 %). Postoperative hemorrhage was observed in five patients (5 %) (grade C), and postoperative liver failure was observed in 16 patients (18 %) (grade A—five patients, grade B—seven patients, and grade C—four patients). The 60-day mortality rate was 8 % (seven patients) due to postoperative liver failure (four patients), sepsis with multi-organ failure (two patients), and hemorrhagic shock (one patient).
Postoperative Long-term Follow-up
The median follow-up time was 68 months (range, 6–143 months). A total of 82 patients were included in the survival analyses (the seven postoperative deaths were excluded and one patient was lost to follow-up). Forty-three patients (52 %) received adjuvant treatment: chemotherapy (36 patients—44 %), radiochemotherapy (six patients—7 %), or radiotherapy (one patient—1 %). Gemcitabine was used the most frequently for adjuvant chemotherapy (26 patients—32 %). The follow-up protocol included a clinical examination, CA 19-9 serum level, and computer tomography/magnetic resonance imaging every 3 months during the first year, every 6 months in the second year, and yearly thereafter.
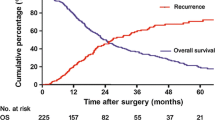
Twenty-six patients (32 %) were still alive (22 patients without recurrence of the disease—27 %) at the last follow-up (September 1, 2012). Fifty-one patients (92 %) died from disease-related causes, while five patients died from other causes (56 total deaths—68 %). The disease recurred in 54 patients (66 %) during the follow-up period: only locally (four patients—7 %), only distant (29 patients—54 %), and locally and distant (21 patients—39 %).
Survival Analysis
After resection, the median overall survival time was 26 months and the 1-, 3-, 5-, and 10-year survival rates were 74, 45, 27, and 24 %, respectively. The median disease-free survival time was 17 months and the 1-, 3-, 5-, and 10-year survival rates were 64, 34, 25, and 24 %, respectively.
Univariate Analysis
The potential prognostic factors for disease-free and overall survival are shown in Table 3.
Multivariate Analysis
In the multivariate analysis, the neutrophil-to-lymphocyte ratio (p = 0.036), type of resection (R0 vs. R1) (p < 0.001), caudate lobe invasion (p = 0.021), and adjuvant chemotherapy with gemcitabine (p = 0.037) were found to be independent risk factors for disease-free survival, as shown in Table 4. For overall survival, the type of resection (R0 vs. R1) (p < 0.001), caudate lobe invasion (p = 0.014), and adjuvant chemotherapy with gemcitabine (p = 0.037) were found to be independent risk factors, as shown in Table 5. The neutrophil-to-lymphocyte ratio was not found to be an independent risk factor for overall survival, although the p value was close to statistical significance (p = 0.053).
Discussion
Resection has significantly improved the prognosis of patients with Klatskin tumors compared to unresected patients.4, 5, 17, 18 The resectability rate has increased through the years from 10 %5 to more than 50 %,2, 19 with the leading hilar cholangiocarcinoma treatment centers even achieving rates of 70 to 100 %.18, 20–22 The resectability rate in the present series was 69 %.
Although rarely performed in the past,5, 23 major liver resection is now widely used for curative intent surgery of Klatskin tumors7, 21, 24 and has been proven to significantly improve the prognosis for even advanced tumors (i.e., type III and IV Bismuth).4, 19, 25
Portal vein invasion is no longer a contraindication for resection in Klatskin tumors.18, 25 While the routine en bloc resection of the portal vein has been proposed by some groups24 in order to increase R0 resection rates, this procedure has a high mortality rate. Therefore, most surgical teams perform a portal vein resection only when there is a clinical suspicion of invasion.18, 21, 26 The reported percentages of portal vein resection in Klatskin tumors vary from 9.8 to 37 %,7, 17, 18, 21, 26 while hepatic artery resections range from 1.7 to 18 %.7, 18, 21 Nevertheless, the need for portal vein resection has been associated with decreased survival in some studies.3, 17, 27 Other studies have not shown an impaired prognosis,21, 26, 28–33 as is the case in the present series.
Caudate lobectomy was proposed as a routine procedure18, 21, 34, 35 due to frequent reports of tumor invasion to the caudate lobe bile ducts.36 However, the real impact of caudate lobectomy on long-term outcome remains debatable. Some studies have shown that caudate lobectomy appears to have no impact on survival after the resection of Klatskin tumors,7, 23 while other studies have shown an improvement in prognosis, which mainly occurs due to an increased rate of negative resection margins.34, 35 A recent study identified the absence of caudate lobectomy as an independent risk factor for an impaired disease-free survival after Klatskin tumors resection, but not overall survival.31 Conversely, caudate lobe invasion appears to be correlated with a poor prognosis.7 However, the incidence of histologically proven caudate lobe invasion has been lower in recent series than historically reported (12.6 vs. 98 % of patients with associated caudate lobectomy).7, 36 The present study identified caudate lobe invasion as an independent prognostic factor for both disease-free and overall survival. The incidence of histological caudate lobe invasion was 22 % (Fig. 2c, d). Although caudate lobectomy has not emerged as a prognostic factor in the present series, we do believe that this procedure should be routinely performed because of the relatively high incidence of tumor invasion into the caudate lobe and the lack of an accurate pre- or intraoperative assessment of this feature. Dissection of the tumor from the caudate lobe to assess tumor invasion may potentially jeopardize the oncological safety of the resection.

Kaplan–Meier curves stratified according to R status for disease-free (a) and overall survival (b) and to caudate lobe invasion for disease-free (c) and overall survival (d)
Preoperative biliary drainage of the future remnant liver has been proposed as a routine by some surgical teams,3, 18, 21, 37 while others recommend using this approach selectively.38 The proponents of routine preoperative biliary drainage argue for the increased safety of liver resection despite the increased risk of cholangitis,39 while opponents emphasize the potential risks, such as ascending cholangitis (up to 48 %)40 or tumor seeding.41 Cholangitis has been identified as a risk factor for morbidity and mortality in some studies42 but not others.37 Preoperative biliary drainage appears to have no impact on long-term outcome,43, 44 as confirmed in the present study.
In the present study, cholangitis was associated with a significant decrease in both disease-free and overall survival, as determined by univariate analysis. These data suggest that reducing the incidence of preoperative cholangitis may potentially lead not only to decreased postoperative morbidity and mortality but also to a better long-term prognosis. The selective use of preoperative biliary drainage is most likely the best approach, for patients with cholangitis and a future remnant liver volume of less than 30–40 %.30, 41
The postoperative mortality rate after Klatskin tumor resection decreased from 15.35 to 5–10.1 % in a recent large series.4, 7, 19, 25 In-hospital mortality rates of 1.7–2 %18, 21 and even no mortality20 were also reported in highly specialized centers. The most common cause of death was liver failure.21
The morbidity rate after curative intent surgery for Klatskin tumors is reported to be approximately 42–75 %;4, 7, 18, 19, 21, 33, 45 the high rates were reported when the Dindo–Clavien classification was used.38, 43 Morbidity has been recently demonstrated as an independent risk factor for an impaired long-term outcome after curative intent surgery for Klatskin tumors.43 In the present series, the 60-day mortality rate was 8 %. The overall morbidity rate was 53 %, with major complications (grade III–IV Dindo) occurring in 23 % of the patients and with no impact on long-term prognosis, as shown in previous studies.4
The current median overall survival after curative intent surgery for Klatskin tumors is 19.9–39 months,3–5, 7, 19, 20, 26, 31, 46 with 1-year survival rates of 66.8–82 %,3, 4, 21, 26 5-year survival rates of 20–42 %,3, 4, 7, 18, 21, 26, 46 and 10-year survival rates of 12–19.9 %.7, 23 The median disease-free survival rates vary from 12 to 20 months.3, 4, 7, 19, 29, 47, 48
Cancer-free margins (R0 resection) are widely accepted as the most important independent prognostic factor for both disease-free and overall survival after Klatskin tumor resection,2–4, 7, 19, 21, 25–30, 32, 46 with the incidence of cancer-free margins ranging from to 9 to 90 %.2–4, 7, 19, 21, 26, 37, 38 In the present series, R0 resection was obtained in 75 % of the cases (Table 6) and emerged as an independent prognostic factor for both disease-free and overall survival (Fig. 2a, b).
Loco-regional lymph node metastases are also an important independent prognostic factor for both disease-free7, 33, 47, 48 and overall survival.2, 7, 17, 19, 21, 26, 27, 29, 31, 32, 46 However, some studies have only identified the presence of metastatic lymph nodes at the celiac trunk as an independent prognostic factor for disease-free4, 31 and overall survival,4 while others have failed to demonstrate any prognostic value of loco-regional lymph node metastasis.25, 26, 33 Metastases to loco-regional lymph nodes have been reported in 26.1–51 % of cases.2–4, 7, 19, 21, 26 In the present series, metastases to loco-regional lymph nodes were detected in 41 % of the patients.
The prognostic value of the lymph node ratio and number of harvested lymph nodes for Klastskin tumors was previously investigated in only one study, which identified the lymph node ratio as an independent risk factor for overall survival.28 The number of harvested lymph nodes was not identified as a prognostic factor in the present study, but an increased lymph node ratio appears to impair prognosis as determined by univariate analysis, with a similar cut-off (0.25) to the cut-off value used in the multivariate analysis of Guglielmi and co-workers.28
The use of adjuvant treatment after Klatskin tumor resection is controversial6 and has not been strongly proven to be of any benefit.1 The reasons for both postoperative radio- and chemotherapy are related to the high local and distant recurrence rates that occur after the so-called curative intent surgery for Klatskin tumors. Cheng and co-workers identified adjuvant radiotherapy but not chemotherapy as an independent prognostic factor after curative intent surgery for Klatskin tumors,49 but other studies have failed to demonstrate any benefit.26
In the present study, adjuvant gemcitabine-based chemotherapy was identified as an independent prognostic factor for both disease-free and overall survival (Fig. 3c, d), as previously shown.44 Nevertheless, some studies deny any benefit of adjuvant chemotherapy.4, 26

Kaplan–Meier curves stratified according to neutrophil-to-lymphocyte ratio for disease-free (a) and overall survival (b) and to adjuvant gemcitabine-based chemotherapy disease-free (c) and overall survival (d)
Recurrence after curative intent surgery for Klatskin tumors primarily occurs at the liver hilum,3 but other studies have shown a predominantly distant pattern of recurrence after R0 resection.29, 47, 48 Associated liver resection has been demonstrated to reduce liver recurrence.47 In the present series, the distant pattern of recurrence was predominant (50 of 54 patients with recurrent disease—92.5 %, with local recurrence in 21 patients—39 %).
The systemic inflammatory response has been largely investigated as a prognostic factor for primary operable cancer and was proven to have prognostic value.9, 50 The cause of this inflammatory response in cancer patients is still being researched, but disease progression appears to depend on the interaction of tumor with the host inflammatory response.9 In patients with jaundice, as is the case for the largest portion of Klatskin tumor patients, the systemic inflammatory response may also result from local infection (i.e., cholangitis).
Inflammation pathways have been demonstrated to be implicated in cholangiocarcinogenesis51 and were associated with poor prognosis.52 Interleukin-6 appears to have a key role in biliary inflammation and carcinogenesis.53 Nevertheless, anti-inflammatory drugs have been demonstrated to prevent carcinogen-induced cholangiocarcinoma formation in animal models.54
For Klatskin tumors, there is only one study investigating the prognostic value of systemic inflammatory markers in Klatskin tumors.55 Although this study identified C-reactive protein as an independent risk factor for overall survival, most of the patients in the study did not undergo resection.55
The present study identified preoperative markers of systemic inflammation as prognostic factors for both disease-free and overall survival, in a univariate analysis, as shown in Table 3. Moreover, the neutrophil-to-lymphocyte ratio has been identified as an independent prognostic factor for disease-free survival (Fig. 3a, b). An increased neutrophil-to-lymphocyte ratio approached statistical significance as a negative prognostic factor for overall survival in the present study (p = 0.053). The neutrophil-to-lymphocyte ratio was recently demonstrated to be superior to other inflammatory markers in other neoplasms as a prognostic factor.56
Previous studies have shown that an increased neutrophil-to-lymphocyte ratio is associated with a reduced disease-free or overall survival after resection for solid cancers such as colo-rectal cancer, colo-rectal liver metastases, or pancreatic adenocarcinoma.9, 57, 58 However, the clinical usefulness of this finding remains unclear, as is the case in the present study. Nevertheless, preoperative markers of the systemic inflammatory response are widely available, inexpensive, and part of the routine preoperative work-up.
The present study could not identify the cause of the systemic inflammatory response in patients with Klatskin tumors; however, we speculate that the cause is most likely due to local infection (i.e., cholangitis) rather than to the host inflammatory response to cancer.
Conclusion
Negative resection margins represent the most important prognostic factor after curative intent surgery for Klatskin tumors. The long-term postoperative outcome is more likely to be influenced by the presence of caudate lobe invasion rather than caudate lobe resection. However, caudate lobectomy should be routinely performed. The use of gemcitabine-based adjuvant chemotherapy appears to benefit survival. Several preoperative parameters, such as hypoalbuminemia and cholangitis, may have a negative impact on survival and are potentially correctable prior to resection. The neutrophil-to-lymphocyte ratio, which was identified as a novel and promising independent prognostic factor, may potentially be used to stratify patients for future clinical trials, but its impact on clinical practice remains unclear.
References
Lafemina J, Jarnagin WR: Surgical management of proximal bile duct cancers. Langenbecks Arch Surg 2012;397:869-879.
DeOliveira ML, Cunningham SC, Cameron JL, Kamangar F, Winter JM, Lillemoe KD, Choti MA, Yeo CJ, Schulick RD: Cholangiocarcinoma: thirty-one-year experience with 564 patients at a single institution. Ann Surg 2007;245:755-762.
Saxena A, Chua TC, Chu FC, Morris DL: Improved outcomes after aggressive surgical resection of hilar cholangiocarcinoma: a critical analysis of recurrence and survival. Am J Surg 2011;202:310-320.
Baton O, Azoulay D, Adam DV, Castaing D: Major hepatectomy for hilar cholangiocarcinoma type 3 and 4: prognostic factors and longterm outcomes. J Am Coll Surg 2007;204:250-260.
Launois B, Reding R, Lebeau G, Buard JL: Surgery for hilar cholangiocarcinoma: French experience in a collective survey of 552 extrahepatic bile duct cancers. J Hepatobiliary Pancreat Surg 2000;7:128-134.
van Gulik TM, Kloek JJ, Ruys AT, Busch OR, van Tienhoven GJ, Lameris JS, Rauws EA, Gouma DJ: Multidisciplinary management of hilar cholangiocarcinoma (Klatskin tumor): extended resection is associated with improved survival. Eur J Surg Oncol 2011;37:65-71.
Nuzzo G, Giuliante F, Ardito F, Giovannini I, Aldrighetti L, Belli G, Bresadola F, Calise F, Dalla VR, D'Amico DF, Gennari L, Giulini SM, Guglielmi A, Jovine E, Pellicci R, Pernthaler H, Pinna AD, Puleo S, Torzilli G, Capussotti L, Cillo U, Ercolani G, Ferrucci M, Mastrangelo L, Portolani N, Pulitano C, Ribero D, Ruzzenente A, Scuderi V, Federico B: Improvement in perioperative and long-term outcome after surgical treatment of hilar cholangiocarcinoma: results of an Italian multicenter analysis of 440 patients. Arch Surg 2012;147:26-34.
Rosen CB, Murad SD, Heimbach JK, Nyberg SL, Nagorney DM, Gores GJ: Neoadjuvant therapy and liver transplantation for hilar cholangiocarcinoma: is pretreatment pathological confirmation of diagnosis necessary? J Am Coll Surg 2012;215:31-38.
Roxburgh CS, McMillan DC: Role of systemic inflammatory response in predicting survival in patients with primary operable cancer. Future Oncol 2010;6:149-163.
Gomez D, Morris-Stiff G, Toogood GJ, Lodge JP, Prasad KR: Impact of systemic inflammation on outcome following resection for intrahepatic cholangiocarcinoma. J Surg Oncol 2008;97:513-518.
Smith RA, Ghaneh P, Sutton R, Raraty M, Campbell F, Neoptolemos JP: Prognosis of resected ampullary adenocarcinoma by preoperative serum CA19-9 levels and platelet–lymphocyte ratio. J Gastrointest Surg 2008;12:1422-1428.
Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A: AJCC Cancer Staging Manual, Seventh Edition. New York, Springer, 2010.
Dindo D, Demartines N, Clavien PA: Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 2004;240:205-213.
Rahbari NN, Garden OJ, Padbury R, Brooke-Smith M, Crawford M, Adam R, Koch M, Makuuchi M, Dematteo RP, Christophi C, Banting S, Usatoff V, Nagino M, Maddern G, Hugh TJ, Vauthey JN, Greig P, Rees M, Yokoyama Y, Fan ST, Nimura Y, Figueras J, Capussotti L, Buchler MW, Weitz J: Posthepatectomy liver failure: a definition and grading by the International Study Group of Liver Surgery (ISGLS). Surgery 2011;149:713-724.
Koch M, Garden OJ, Padbury R, Rahbari NN, Adam R, Capussotti L, Fan ST, Yokoyama Y, Crawford M, Makuuchi M, Christophi C, Banting S, Brooke-Smith M, Usatoff V, Nagino M, Maddern G, Hugh TJ, Vauthey JN, Greig P, Rees M, Nimura Y, Figueras J, Dematteo RP, Buchler MW, Weitz J: Bile leakage after hepatobiliary and pancreatic surgery: a definition and grading of severity by the International Study Group of Liver Surgery. Surgery 2011;149:680-688.
Rahbari NN, Garden OJ, Padbury R, Maddern G, Koch M, Hugh TJ, Fan ST, Nimura Y, Figueras J, Vauthey JN, Rees M, Adam R, Dematteo RP, Greig P, Usatoff V, Banting S, Nagino M, Capussotti L, Yokoyama Y, Brooke-Smith M, Crawford M, Christophi C, Makuuchi M, Buchler MW, Weitz J: Post-hepatectomy haemorrhage: a definition and grading by the International Study Group of Liver Surgery (ISGLS). HPB (Oxford) 2011;13:528-535.
Ebata T, Nagino M, Kamiya J, Uesaka K, Nagasaka T, Nimura Y: Hepatectomy with portal vein resection for hilar cholangiocarcinoma: audit of 52 consecutive cases. Ann Surg 2003;238:720-727.
Igami T, Nishio H, Ebata T, Yokoyama Y, Sugawara G, Nimura Y, Nagino M: Surgical treatment of hilar cholangiocarcinoma in the "new era": the Nagoya University experience. J Hepatobiliary Pancreat Sci 2010;17:449-454.
Matsuo K, Rocha FG, Ito K, D'Angelica MI, Allen PJ, Fong Y, Dematteo RP, Gonen M, Endo I, Jarnagin WR: The blumgart preoperative staging system for hilar cholangiocarcinoma: analysis of resectability and outcomes in 380 patients. J Am Coll Surg 2012;215:343-355.
Kondo S, Hirano S, Ambo Y, Tanaka E, Okushiba S, Morikawa T, Katoh H: Forty consecutive resections of hilar cholangiocarcinoma with no postoperative mortality and no positive ductal margins: results of a prospective study. Ann Surg 2004;240:95-101.
Lee SG, Song GW, Hwang S, Ha TY, Moon DB, Jung DH, Kim KH, Ahn CS, Kim MH, Lee SK, Sung KB, Ko GY: Surgical treatment of hilar cholangiocarcinoma in the new era: the Asan experience. J Hepatobiliary Pancreat Sci 2010;17:476-489.
van Gulik TM, Ruys AT, Busch OR, Rauws EA, Gouma DJ: Extent of liver resection for hilar cholangiocarcinoma (Klatskin tumor): how much is enough? Dig Surg 2011;28:141-147.
Dinant S, Gerhards MF, Rauws EA, Busch OR, Gouma DJ, van Gulik TM: Improved outcome of resection of hilar cholangiocarcinoma (Klatskin tumor). Ann Surg Oncol 2006;13:872-880.
Neuhaus P, Jonas S, Settmacher U, Thelen A, Benckert C, Lopez-Hanninen E, Hintze RE: Surgical management of proximal bile duct cancer: extended right lobe resection increases resectability and radicality. Langenbecks Arch Surg 2003;388:194-200.
Neuhaus P, Thelen A, Jonas S, Puhl G, Denecke T, Veltzke-Schlieker W, Seehofer D: Oncological superiority of hilar en bloc resection for the treatment of hilar cholangiocarcinoma. Ann Surg Oncol 2012;19:1602-1608.
de Jong MC, Marques H, Clary BM, Bauer TW, Marsh JW, Ribero D, Majno P, Hatzaras I, Walters DM, Barbas AS, Mega R, Schulick RD, Choti MA, Geller DA, Barroso E, Mentha G, Capussotti L, Pawlik TM: The impact of portal vein resection on outcomes for hilar cholangiocarcinoma: A multi-institutional analysis of 305 cases. Cancer 2012.
Miyazaki M, Kato A, Ito H, Kimura F, Shimizu H, Ohtsuka M, Yoshidome H, Yoshitomi H, Furukawa K, Nozawa S: Combined vascular resection in operative resection for hilar cholangiocarcinoma: does it work or not? Surgery 2007;141:581-588.
Guglielmi A, Ruzzenente A, Campagnaro T, Pachera S, Conci S, Valdegamberi A, Sandri M, Iacono C: Prognostic significance of lymph node ratio after resection of peri-hilar cholangiocarcinoma. HPB (Oxford) 2011;13:240-245.
Hasegawa S, Ikai I, Fujii H, Hatano E, Shimahara Y: Surgical resection of hilar cholangiocarcinoma: analysis of survival and postoperative complications. World J Surg 2007;31:1256-1263.
Jarnagin WR, Bowne W, Klimstra DS, Ben-Porat L, Roggin K, Cymes K, Fong Y, Dematteo RP, D'Angelica M, Koea J, Blumgart LH: Papillary phenotype confers improved survival after resection of hilar cholangiocarcinoma. Ann Surg 2005;241:703-712.
Kow AW, Wook CD, Song SC, Kim WS, Kim MJ, Park HJ, Heo JS, Choi SH: Role of caudate lobectomy in type III A and III B hilar cholangiocarcinoma: a 15-year experience in a tertiary institution. World J Surg 2012;36:1112-1121.
Li H, Qin Y, Cui Y, Chen H, Hao X, Li Q: Analysis of the surgical outcome and prognostic factors for hilar cholangiocarcinoma: a Chinese experience. Dig Surg 2011;28:226-231.
Young AL, Prasad KR, Toogood GJ, Lodge JP: Surgical treatment of hilar cholangiocarcinoma in a new era: comparison among leading Eastern and Western centers, Leeds. J Hepatobiliary Pancreat Sci 2010;17:497-504.
Tsao JI, Nimura Y, Kamiya J, Hayakawa N, Kondo S, Nagino M, Miyachi M, Kanai M, Uesaka K, Oda K, Rossi RL, Braasch JW, Dugan JM: Management of hilar cholangiocarcinoma: comparison of an American and a Japanese experience. Ann Surg 2000;232:166-174.
Wahab MA, Sultan AM, Salah T, Fathy O, Elebidy G, Elshobary M, Shiha O, Rauf AA, Elhemaly M, El-Ghawalby N: Caudate Lobe Resection with Major Hepatectomy for Central Cholangiocarcinoma: Is it of Value? Hepatogastroenterology 2012;59:321-324.
Nimura Y, Hayakawa N, Kamiya J, Kondo S, Shionoya S: Hepatic segmentectomy with caudate lobe resection for bile duct carcinoma of the hepatic hilus. World J Surg 1990;14:535-543.
Hirano S, Kondo S, Tanaka E, Shichinohe T, Tsuchikawa T, Kato K, Matsumoto J, Kawasaki R: Outcome of surgical treatment of hilar cholangiocarcinoma: a special reference to postoperative morbidity and mortality. J Hepatobiliary Pancreat Sci 2010;17:455-462.
Regimbeau JM, Fuks D, Le Treut YP, Bachellier P, Belghiti J, Boudjema K, Baulieux J, Pruvot FR, Cherqui D, Farges O: Surgery for hilar cholangiocarcinoma: a multi-institutional update on practice and outcome by the AFC-HC study group. J Gastrointest Surg 2011;15:480-488.
Nimura Y: Preoperative biliary drainage before resection for cholangiocarcinoma (Pro). HPB (Oxford) 2008;10:130-133.
Kloek JJ, van der Gaag NA, Aziz Y, Rauws EA, van Delden OM, Lameris JS, Busch OR, Gouma DJ, van Gulik TM: Endoscopic and percutaneous preoperative biliary drainage in patients with suspected hilar cholangiocarcinoma. J Gastrointest Surg 2010;14:119-125.
Laurent A, Tayar C, Cherqui D: Cholangiocarcinoma: preoperative biliary drainage (Con). HPB (Oxford) 2008;10:126-129.
Sakata J, Shirai Y, Tsuchiya Y, Wakai T, Nomura T, Hatakeyama K: Preoperative cholangitis independently increases in-hospital mortality after combined major hepatic and bile duct resection for hilar cholangiocarcinoma. Langenbecks Arch Surg 2009;394:1065-1072.
Chauhan A, House MG, Pitt HA, Nakeeb A, Howard TJ, Zyromski NJ, Schmidt CM, Ball CG, Lillemoe KD: Post-operative morbidity results in decreased long-term survival after resection for hilar cholangiocarcinoma. HPB (Oxford) 2011;13:139-147.
Murakami Y, Uemura K, Sudo T, Hayashidani Y, Hashimoto Y, Nakamura H, Nakashima A, Sueda T: Gemcitabine-based adjuvant chemotherapy improves survival after aggressive surgery for hilar cholangiocarcinoma. J Gastrointest Surg 2009;13:1470-1479.
Nagino M, Kamiya J, Arai T, Nishio H, Ebata T, Nimura Y: One hundred consecutive hepatobiliary resections for biliary hilar malignancy: preoperative blood donation, blood loss, transfusion, and outcome. Surgery 2005;137:148-155.
Klempnauer J, Ridder GJ, von WR, Werner M, Weimann A, Pichlmayr R: Resectional surgery of hilar cholangiocarcinoma: a multivariate analysis of prognostic factors. J Clin Oncol 1997;15:947-954.
Ito F, Agni R, Rettammel RJ, Been MJ, Cho CS, Mahvi DM, Rikkers LF, Weber SM: Resection of hilar cholangiocarcinoma: concomitant liver resection decreases hepatic recurrence. Ann Surg 2008;248:273-279.
Kobayashi A, Miwa S, Nakata T, Miyagawa S: Disease recurrence patterns after R0 resection of hilar cholangiocarcinoma. Br J Surg 2010;97:56-64.
Cheng Q, Luo X, Zhang B, Jiang X, Yi B, Wu M: Predictive factors for prognosis of hilar cholangiocarcinoma: postresection radiotherapy improves survival. Eur J Surg Oncol 2007;33:202-207.
Proctor MJ, McMillan DC, Morrison DS, Fletcher CD, Horgan PG, Clarke SJ: A derived neutrophil to lymphocyte ratio predicts survival in patients with cancer. Br J Cancer 2012;107:695-699.
Fava G, Lorenzini I: Molecular pathogenesis of cholangiocarcinoma. Int J Hepatol 2012;2012:630543.
Thanan R, Oikawa S, Yongvanit P, Hiraku Y, Ma N, Pinlaor S, Pairojkul C, Wongkham C, Sripa B, Khuntikeo N, Kawanishi S, Murata M: Inflammation-induced protein carbonylation contributes to poor prognosis for cholangiocarcinoma. Free Radic Biol Med 2012;52:1465-1472.
Johnson C, Han Y, Hughart N, McCarra J, Alpini G, Meng F: Interleukin-6 and its receptor, key players in hepatobiliary inflammation and cancer. Transl Gastrointest Cancer 2012;1:58-70.
Wentz SC, Yip-Schneider MT, Gage EA, Saxena R, Badve S, Schmidt CM: Sulindac prevents carcinogen-induced intrahepatic cholangiocarcinoma formation in vivo. J Surg Res 2009;157:e87-e95.
Gerhardt T, Milz S, Schepke M, Feldmann G, Wolff M, Sauerbruch T, Dumoulin FL: C-reactive protein is a prognostic indicator in patients with perihilar cholangiocarcinoma. World J Gastroenterol 2006;12:5495-5500.
Wang DS, Luo HY, Qiu MZ, Wang ZQ, Zhang DS, Wang FH, Li YH, Xu RH: Comparison of the prognostic values of various inflammation based factors in patients with pancreatic cancer. Med Oncol 2012.
Aliustaoglu M, Bilici A, Seker M, Dane F, Gocun M, Konya V, Ustaalioglu BB, Gumus M: The association of pre-treatment peripheral blood markers with survival in patients with pancreatic cancer. Hepatogastroenterology 2010;57:640-645.
Garcea G, Ladwa N, Neal CP, Metcalfe MS, Dennison AR, Berry DP: Preoperative neutrophil-to-lymphocyte ratio (NLR) is associated with reduced disease-free survival following curative resection of pancreatic adenocarcinoma. World J Surg 2011;35:868-872.
Launois B, Terblanche J, Lakehal M, Catheline JM, Bardaxoglou E, Landen S, Campion JP, Sutherland F, Meunier B: Proximal bile duct cancer: high resectability rate and 5-year survival. Ann Surg 1999;230:266-275.
Acknowledgments
The authors express their gratitude to Cristian Baicus, MD (Carol Davila University of Medicine and Pharmacy) and Raluca Purnichescu-Purtan, PhD (Department of Mathematics, Politehnica University of Bucharest, Romania) for their valuable assistance with the statistical analyses.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Dumitrascu, T., Chirita, D., Ionescu, M. et al. Resection for Hilar Cholangiocarcinoma: Analysis of Prognostic Factors and the Impact of Systemic Inflammation on Long-term Outcome. J Gastrointest Surg 17, 913–924 (2013). https://doi.org/10.1007/s11605-013-2144-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-013-2144-2