
Abstract
Background
Self-expanding metal stents can be used as bridge to elective surgery for acute malignant colonic obstruction. However, the impact on long-term oncological outcome and the optimal timing of surgery are still unknown.
Method
This was a retrospective multicenter study performed at four colorectal centers. Patients undergoing stent placement as bridge to surgery, between January 2010 and December 2013, were included in the study. Primary outcomes were survival and recurrence rates along with location of the metastases. Additionally, we recorded time from stent placement to elective surgery. Secondary outcomes were postoperative complication rates. Complications were classified according to the Clavien-Dindo classification score. A logistic regression model was used to describe impact of delayed stent removal on risk of recurrence.
Results
This study included 112 patients, with a median follow-up of 43 months. Survival rate was 70%. We found a recurrence rate of 37%, primarily local recurrences (17%). Procedure-related complications at the stent placement were seen in 18%, and complications after subsequent elective surgery were seen in 39%. A significantly higher risk of recurrence with increased time from stent placement to elective surgery (OR 5.1 [1.6–15.8], p = 0.005) was found.
Conclusion
Delay of elective surgery after stent placement may have a negative influence on long-term oncologic outcomes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Colorectal carcinoma is the third most common type of cancer. It has been reported that 8–40% of all patients with colorectal carcinoma present with acute malignant obstruction [1–3]. Self-expanding metal stent (SEMS) was introduced in the 1990s as an alternative to emergency surgery [2]. SEMS can restore luminal patency as a definitive palliative treatment or as a bridge to elective surgery. The expected benefit of SEMS as a bridge to surgery is the opportunity to optimize the patient’s clinical condition before surgery, with less morbidity, mortality, and need for a stoma [2, 4].
However, a meta-analysis of randomized controlled trials failed to show beneficial effects of SEMS compared with emergency surgery, regarding morbidity and mortality [4]. Furthermore, a recent study found SEMS to be related to worse overall and disease-free survival compared with emergency surgery [5]. In addition, a higher rate of local recurrence after SEMS compared with emergency surgery has also been shown [6]. Although SEMS is frequently implemented as an alternative to emergency surgery in the management of colonic obstruction, little is known about the impact on long-term oncological outcomes and the optimal time for the elective procedure with resection of the obstructed colon. Longer duration of stent placement may result in an increased risk of microperforation or induce a local response that may result in poorer oncological outcome.
We aimed to investigate the long-term oncological outcome after stent placement as bridge to surgery. Additionally, we planned to investigate if time from stent placement until tumor resection was related to recurrence rate.
Method
A retrospective multicenter study was conducted according to the STROBE statement for observational studies [7]. This study included four Danish colorectal centers. Medical records, from January 2010 to December 2013, of patients undergoing SEMS placement for acute malignant obstruction were reviewed. Only patients with potentially curable colorectal cancer at time of stent placement were included in the analysis. Patients undergoing SEMS placement, as a palliative treatment, were excluded. Bridge to surgery was defined as scheduled elective surgery at the primary stent treatment or in the immediate period hereafter, independent of time between SEMS insertion and surgery.
Stent placement
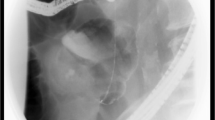
SEMS insertions were performed by a combined endoscopic and fluoroscopic approach. All procedures were carried out under general anesthesia or conscious sedation. SEMS insertion across the obstruction was performed according to the standard technique as previously described [8–10]. A guidewire was introduced over the stenosis and beyond the obstruction, and a stent was deployed over the guidewire. Correct positioning of the stent was confirmed by fluoroscopy. Stents used were WallFlex (colonic stent; Boston Scientific), Hanarostent (M.I. Tech., Seoul, Korea), and Evolution (Cook Medical, IN, USA). After SEMS placement, patients were offered an elective resection.
Data recorded
Following demographical data were retrieved: gender, age, TNM stage, adjuvant chemotherapy, American Society of Anesthesiologist (ASA) score, tumor location, and type of stent. Furthermore, time from SEMS placement to elective surgery, 30-day survival rate, 1-year survival rate, and complications were recorded. Complications were classified according to Clavien-Dindo classification [11]. Finally, we registered recurrence rate and the location of the metastasis. Local recurrence was defined as cancer in the same place to the original cancer or very close to it. Local recurrence could be solid tumors or diffusely peritoneal. In systemic metastasis, the cancer had spread to organs or tissues far away from the original cancer. Patients were followed until death or May 2015.
Statistical analysis
Demographic data were presented as absolute numbers with percentages, unless indicated otherwise. The unadjusted relationship between outcome and delayed stent removal was assessed using an independent χ 2 test. A multiple logistic regression model was used to describe the independent effect of delayed stent removal on the risk for metastasis controlled for potential confounders (gender, age, tumor grade, and chemotherapy). Outcomes were presented as odds ratios (OR) with 95% confidence limits. Statistical significance was considered for p ≤ 0.05.
All data analyses were performed using SPSS statistics, version 23.0 (SPSS, Inc.).
The current study was approved by the Danish Data Protection Agency (REG-74-2015).
Results
From January 2010 to December 2013, a total of 112 patients underwent stent placement as bridge to surgery at the four included colorectal centers. There were 56 (50%) females and 56 males, with a mean age of 71 years. Patients’ demographical data are summarized in Table 1. Time from stent placement to tumor resection ranged from 0 to 165 days with a median of 18 days. Of the 112 patients, 20 (18%) had an emergency surgery due to a stent-related complication, primarily migration and perforation (Table 2). Complications after tumor resection were seen in 44 (39%) patients. A 30-day survival rate at 106 (95%) was found, and at 1-year follow-up, the survival rate was 101 (90%). At the final follow-up (median 43 months), the survival rate was 78 (70%). Results are summarized and complications are classified according to Clavien-Dindo in Table 2.
Oncological outcomes
An overall recurrence rate of 41 (37%) was recorded. Of these, 19 patients had local recurrence of which 11 were solid tumors and eight were diffuse peritoneal metastases. Liver metastasis was found in 17 patients, and metastasis located in the lungs was found in 13 patients. In four cases, the metastasis was found in other locations. In one case, the metastasis was found in the columna, in another case in the kidney, and additionally, a case with metastasis in the esophagus. Finally, one patient had metastasis in her breast and retroperitoneum and cutaneous metastasis. Results are summarized in Table 2.
We investigated time from stent placement to elective surgery related to the risk of recurrence, controlled for gender, age, tumor grade, and postoperative chemotherapy. Median time from SEMS insertion to surgery was 18 days. We divided the patients in two groups: patients who underwent surgery within 18 days and patients who underwent surgery later than 18 days after SEMS placement. Of the 112 patients, 20 patients underwent emergency surgery due to failure of the stent placement. These patients were excluded from the analysis. A logistic regression analysis was performed. We found a significant increased risk of recurrence in the group with more than 18 days from stent placement to elective surgery (OR 5.1 [1.6–15.8], p = 0.005). See Table 3. Furthermore, we performed the analysis as an “intention-to-treat” model including patients undergoing emergency surgery because of complications due to stent placement. In this analysis, we also found a significant increased risk of recurrence in the group with more than 18 days from stent placement to surgery (OR 2.6 [1.1–6.5], p = 0.037). Additionally, we found a significantly lower risk of recurrence related to increasing age at stent placement (OR 0.96 [0.91–1.00], p = 0.049). See Table 4.
Discussion
This study found a relatively high recurrence rate of 37%, primarily local recurrences followed by metastases in the lungs and liver, in patients undergoing SEMS placement as bridge to surgery. Our analysis showed a significantly higher recurrence rate related to increasing time from SEMS placement to surgery. Larger studies are needed to verify the results found in this study. Furthermore, it is relevant to note that 18% needed an emergency surgery due to a stent-related complication, primarily perforation or migration.
Recent studies have failed to show beneficial effects of stenting as bridge to surgery over emergency surgery [12–14]. A number of meta-analyses support these findings [4, 15, 16]. In the past few years, long-term oncologic outcomes have been discussed. In 2014, a study ended prematurely, as they found a risk of recurrence associated with stent placement for malignant colonic obstruction [17]. Additionally, in 2013, one study reported increased local recurrence rate after SEMS placement compared with emergency surgery [6]. A number of reasons for these findings have been suggested. Several studies have demonstrated increased histopathological changes in patients undergoing SEMS placement compared with emergency surgery [18–20]. These studies reported higher rates of perineural invasion, inflammation, lymph node invasion, ulceration at or near the tumor, and necrosis. Additionally, tumor cell dissemination following SEMS placement has been reported [21].
The high recurrence rate in our study supports the findings of other studies. Efforts were made to minimize the limitations of this study, primarily due to the retrospective design. However, selection bias among others cannot be ruled out. Our study should be interpreted with caution. Larger prospective studies are needed to confirm our findings.
In conclusion, our study found a relatively high recurrence rate after SEMS placement as bridge to surgery for malignant colonic obstruction. Furthermore, we found a higher risk of recurrence associated with increased time from SEMS placement to elective surgery.
References
Chen HS, Sheen-Chen SM (2000) Obstruction and perforation in colorectal adenocarcinoma: an analysis of prognosis and current trends. Surgery 127:370–376
Deans GT, Krukowski ZH, Irwin ST (1994) Malignant obstruction of the left colon. Br J Surg. 81:1270–1276
Stower MJ, Hardcastle JD (1985) The results of 1115 patients with colorectal cancer treated over an 8-year period in a single hospital. Eur J Surg Oncol 11:119–123
Liu Z, Kang L, Li C et al (2014) Meta-analysis of complications of colonic stenting versus emergency surgery for acute left-sided malignant colonic obstruction. SLEPT 24:73–79
Sabbagh C, Browet F, Diouf M et al (2013) Is stenting as “a bridge to surgery” an oncologically safe strategy for the management of acute, left-sided, malignant, colonic obstruction? A comparative study with a propensity score analysis. Ann Surg 258:107–115
Gorissen KJ, Tuynman JB, Fryer E et al (2013) Local recurrence after stenting for obstructing left-sided colonic cancer. Br J Surg. 100:1805–1809
von Elm E, Altman DG, Egger M et al (2007) The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet 370:1453–1457
Baron TH, Harewood GC (2003) Enteral self-expandable stents. Gastrointest Endosc 58:421–433
Baron TH (2007) Minimizing endoscopic complications: endoluminal stents. Gastrointest Endosc Clin North Am 17:83–104
Fernandez-Esparrach G, Bordas JM, Giraldez MD et al (2010) Severe complications limit long-term clinical success of self-expanding metal stents in patients with obstructive colorectal cancer. Am J Gastroenterol 105:1087–1093
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–213
Knight AL, Trompetas V, Saunders MP et al (2012) Does stenting of left-sided colorectal cancer as a “bridge to surgery” adversely affect oncological outcomes? A comparison with non-obstructing elective left-sided colonic resections. Int J Color Dis 27:1509–1514
Choi JM, Lee C, Han YM et al (2014) Long-term oncologic outcomes of endoscopic stenting as a bridge to surgery for malignant colonic obstruction: comparison with emergency surgery. Surg Endosc 28:2649–2655
Pirlet IA, Slim K, Kwiatkowski F et al (2011) Emergency preoperative stenting versus surgery for acute left-sided malignant colonic obstruction: a multicenter randomized controlled trial. Surg Endosc 25:1814–1821
Ye GY, Cui Z, Chen L et al (2012) Colonic stenting vs emergent surgery for acute left-sided malignant colonic obstruction: a systematic review and meta-analysis. World J Gastroenterol 18:5608–5615
Tan CJ, Dasari BV, Gardiner K (2012) Systematic review and meta-analysis of randomized clinical trials of self-expanding metallic stents as a bridge to surgery versus emergency surgery for malignant left-sided large bowel obstruction. Br J Surg. 99:469–476
Sloothaak DA, van den Berg MW, Dijkgraaf MG et al (2014) Oncological outcome of malignant colonic obstruction in the Dutch Stent-In 2 trial. Br J Surg. 101:1751–1757
Kim HJ, Choi GS, Park JS et al (2013) Higher rate of perineural invasion in stent-laparoscopic approach in comparison to emergent open resection for obstructing left-sided colon cancer. Int J Color Dis 28:407–414
Fryer E, Gorissen KJ, Wang LM et al (2015) Spectrum of histopathological changes encountered in stented colorectal carcinomas. Histopathology 66:480–484
Sabbagh C, Chatelain D, Trouillet N et al (2013) Does use of a metallic colon stent as a bridge to surgery modify the pathology data in patients with colonic obstruction? A case-matched study. Surg Endosc 27:3622–3631
Maruthachalam K, Lash GE, Shenton BK et al (2007) Tumour cell dissemination following endoscopic stent insertion. Br J Surg 94:1151–1154
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The current study was approved by the Danish Data Protection Agency (REG-74-2015).
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Broholm, M., Kobborg, M., Frostberg, E. et al. Delay of surgery after stent placement for resectable malignant colorectal obstruction is associated with higher risk of recurrence. Int J Colorectal Dis 32, 513–516 (2017). https://doi.org/10.1007/s00384-016-2705-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-016-2705-4