
Abstract
Objective
To determine the significance of transient ischemic dilatation (TID) in patients with normal perfusion on adenosine stress/rest.
Methods
We analyzed 430 consecutive patients with normal perfusion on 2-day adenosine stress/rest 99mTc-sestamibi. A group of 70 patients with Framingham 10-year coronary heart disease risk < 10% was used to derive abnormal TID thresholds (derivation group). The significance of TID at these thresholds was validated in the remaining 360 patients (validation group) followed for cardiac events for 31.2 ± 9.7 (mean ± SD) months.
Results
Transient ischemic dilatation in the derivation group was 1.05 ± 0.13. Three definitions of an abnormal TID were used: > mean + 2SD (TID ≥ 1.32), > mean + 1SD (TID ≥ 1.19) and a TID in the group’s highest quartile (TID ≥ 1.15). Of the 360 validation group patients, 12 (3.3%), 48 (13.3%) and 70 (19.4%) had TID ≥ 1.32, 1.19 and 1.15, respectively. Age, gender, family history of coronary artery disease (CAD), known CAD, smoking, hypertension, diabetes, dyslipidemia, rest LVEF, post-stress LVEF, ΔLVEF, ≥ 5% or 10% decrease in LVEF did not predict TID ≥ 1.32. However, TID ≥ 1.19 was predicted by rest LVEF and ≥ 5% decrease in LVEF (P = 0.04 and 0.02, respectively) and TID ≥ 1.15 was predicted by ≥ 5% decrease in LVEF (P = 0.02). Cardiac event-free survivals were similar in patients with a TID ≥ and < 1.32 (P = 0.68), ≥ and < 1.19 (P = 0.40) and ≥ and < 1.15 (P = 0.79).
Conclusions
Transient ischemic dilatation does not confer adverse prognosis in patients with normal perfusion on adenosine stress/rest 99mTc-sestamibi irrespective of the threshold used for its definition.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The presence of stress-induced dilatation of left ventricular cavity, termed transient ischemic dilation (TID) on myocardial perfusion scans has been shown to provide incremental diagnostic and prognostic value [1,2,3,4,5,6]. However, its clinical significance in patients with normal perfusion scans remains controversial [2].
Transient ischemic dilatation is thought to be due to one or both of two mechanisms: a “true” dilatation due to post-stress myocardial stunning of areas with stress-induced ischemia resulting in an increased left ventricular end-systolic volume (LVESV) and/or global subendocardial ischemia [2, 7, 8].
When reporting on frequency or relevance of TID, an “optimal” abnormal threshold is employed which varies between studies depending on the perfusion tracer used (e.g., 201Tl, 99mTc-sestamibi or –tetrofosmin, 82Rb) [3,4,5,6, 9] and whether exercise [3, 4] or pharmacologic stress [6, 10, 11] was used to stress the patient [6, 10, 11].
There has only been limited reports on the abnormal TID threshold in patients undergoing adenosine stress/rest 99mTc-sestamibi. In addition, there is little data on the proportion of patients with normal perfusion on these studies who have an elevated TID nor on the prognostic value of such elevation.
The aim of this study is to determine the abnormal TID threshold based on a cohort of patients with normal perfusion who have Framingham 10-year coronary heart disease (CHD) risk < 10% and to subsequently validate the significance of this derived abnormal TID in a large cohort of consecutively enrolled patients followed for hard (cardiac death or nonfatal MI) and soft (coronary revascularization or congestive heart failure) cardiac events for a mean period of about 2.5 years.
Materials and methods
This retrospective study was approved by the Institutional Review Board (IRB) of Jordan University Hospital.
All patients with known or suspected CAD who underwent a 2-day adenosine gated stress/rest 99mTc-sestamibi imaging between March 2015 and December 2018 and had normal perfusion were analyzed, a total of 430 patients. Patients were divided into two groups: a derivation group and a validation group. The derivation group was used derive the abnormal TID threshold and consisted of 70 patients without history of diabetes or CAD, with a left ventricular ejection fraction (LVEF) of ≥ 50%, normal LV volume and Framingham 10-year CHD risk < 10% [12]. The validation group was used to validate the significance of abnormal TID and consisted of the remaining 360 patients.
The 2-day adenosine stress/rest gated SPECT 99mTc-sestamibi was the standard myocardial perfusion imaging approach used at our institution during the study period, because we intended to investigate the prevalence and prognostic significance of post-adenosine TID; the 2-day protocol was deemed more suitable for this purpose, since any stress-induced myocardial stunning resulting in TID would have completely recovered when patients are imaged at rest on a different day [13].
Gated-SPECT acquisition and interpretation
Gated adenosine stress SPECT images were obtained one hour after injection of 15 mCi (555 MBq) of 99mTc-sestamibi [20 mCi (740 MBq) in obese patients] given 3 minutes into a 6-min infusion of adenosine at a concentration of 140 µg/kg/min. Gated rest SPECT images were performed within 1 week thereafter, also 1 h after injection of 15 mCi (555 MBq) of 99mTc-sestamibi [20 mCi (740 MBq) in obese patients] with no intervening cardiac event or intervention between the stress and rest scans.
Single photon emission computerized tomography images were acquired using a dual-head gamma camera (E.CAM; Siemens Medical Solutions, Malvern, Pennsylvania, USA) equipped with a high-resolution parallel hole collimator with the peak energy set at 140 keV with a 20% window width, 180° rotation arc, 32 projections, 25 s/projection, 16 frames/heart cycle and 64 × 64 matrix. Processing was performed using filtered back projection to trans-axial tomographic images and these were reoriented to the short, vertical, and horizontal long axes. No attenuation correction was performed. We used beat-rejection software to acquire data with a stable R–R interval. A tolerance window of 20% was strictly enforced in all patients included in this study and all beats outside this window were rejected. Patients with atrial fibrillation and PVCs, who made up about 5% of our patients were only gated after applying this beat-rejection software.
We used the quantitative automated software programs QPS and QGS (Cedar Sinai Medical Center, Los Angeles, CA) to score the perfusion defects and wall motion abnormalities, respectively. Myocardial uptake in a 20-segment model was scored as pe QPS based on a 5-point scale ranging from 0 (normal uptake) to 4 (no detectable tracer uptake) with computation of the summed stress score (SSS) and summed rest score (SRS) for each patient by adding the scores of the 20 segments in the stress and rest images, respectively. The summed difference score (SDS) was computed as SSS-SRS. Scans with a SSS of ≤ 3 were considered negative (normal perfusion). Only patients with normal perfusion are included in the present study.
Quantitative automated software programs was used to calculate the TID as the ratio of the average stress to the average rest LV volume. QGS was used to measure the global LVEF, regional wall motion and thickness, LV end-systolic volume (LVESV) and LV end-diastolic volume (LVEDV) at rest and post stress.
Patient outcome
The 360 patients in the validation group were followed up for both hard (cardiac death or nonfatal MI) and soft (coronary revascularization and congestive heart failure requiring hospitalization) cardiac events by review of their hospital medical records as well as via telephone contact, either directly with the patients themselves, their relatives, or referring physician. The mean follow-up period was 31.2 ± 9.7 months. Cardiac death was defined as that due to MI or sudden cardiac death ascertained as such by trained board-certified emergency room physicians or cardiologists. Nonfatal MI was defined based on the third universal definition, the hallmark of which is the detection of a rise and/or fall of cardiac biomarker values, with at least one of the values being elevated (i.e., > 99th percentile upper reference limit, URL) [14]. High sensitivity troponin I is used in our laboratory in addition to one of the following conditions: symptoms suggestive of myocardial infarction, ECG changes, evidence of myocardial damage or identification of coronary thrombus. Coronary revascularization is defined as either percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG). Congestive heart failure hospitalization is defined as hospitalization due to pulmonary edema diagnosed by clinical criteria, laboratory data, and echocardiography.
Statistical analysis
Categorical variables, reported as frequencies and as percentages, were compared using Pearson’s Chi-squared test or Fisher Exact test, as appropriate. Mann Whitney U test was used to compare continuous variables. These were reported using means ± the standard deviations.
We examined the frequency, prognostic significance and predictors of abnormal TID, as previously reported in the literature [2]. Cardiac event-free survivals for normal and abnormal TID ratios were compared using Kaplan–Meier plots and log rank test. Hazard ratio for abnormal TID ratio was obtained through the Cox proportional hazard model.
Univariate analysis was first carried out to identify which variables among all possible variables known by published literature to potentially affect a certain outcome, such as abnormal TID or cardiac events were significant predictors in our patient population. The variables included were age, sex, family history of CAD, known history of CAD, diabetes, hypertension, dyslipidemia, rest LVEF, post-stress LVEF, ΔLVEF and TID.
Multivariate analyses for possible independent predictor variables of cardiac events and abnormal TID were carried out using the logistic regression model. Only significant variables (P ≤ 0.05) by univariate analysis were entered into the multivariate analysis. Statistical significance was determined at two-sided P-value ≤ 0.05. Analyses were performed in R version 3.5.0 and relevant packages [15].
Results
Definition of abnormal TID
The mean TID (± SD) of the derivation group was 1.05 ± 0.13. Three definitions of an abnormal TID were used: a value > mean + 2SD (TID ≥ 1.32), a value > mean + 1SD (TID ≥ 1.19) or as a value in the highest quartile of the derivation group (TID ≥ 1.15).
Validation group characteristics and TID
Table 1 shows the baseline characteristics of the 360 patients in the validation group. Two-hundred and three patients (56.4%) were diabetic and history of CAD was confirmed in 151 patients (41.9%) by the presence of documented prior myocardial infarction or the documentation of CAD by coronary angiography.
Coronary angiography (CAG) reports were available in106 of the 151 patients; the remaining patients had their CAG performed at outside institutions. Of the 106 patients, 81 had obstructive CAD. The extent of CAD in these patients and the percent diameter stenosis are shown in Fig. 1a–d. All these patients underwent revascularization (stent in 77 and CABG in 4) prior to the myocardial perfusion scan.

a Baseline extent of coronary artery disease (CAD) in patients with known obstructive CAD, b Percent diameter stenosis of left anterior descending artery (LAD) lesions, c Percent diameter stenosis of left circumflex artery (LCX) lesions, d Percent diameter stenosis of right coronary artery (RCA) lesions
The mean TID in the 360 patients was 1.05 ± 0.14 (median = 1.04, range 0.61–1.76). The TID values were not normally distributed in these patients (P < 0.001 based on Shapiro’s test indicting departure from normality). These TID values were not significantly different from those in the derivation group (P = 0.80) although the validation group had high percentages of patients with recognized risk factors, such as history of CAD (41.9%), diabetes (56.4%) and dyslipidemia (70%).
Only 12 of the 360 patients (3.3%) of the validation group had a TID ≥ 1.32 (> mean + 2D in the derivation group). The mean TID in these 12 patients was 1.44 ± 0.13 (range 1.32–1.76) vs. 1.04 ± 0.12 (range 0.60–1.31) in the 348 patients with a TID ratio of < 1.32 (P < 0.0001).
Forty-eight of the 360 patients (13.3%) had a TID ≥ 1.19 (> mean + 1SD in the derivation group). The mean TID in these 48 patients was 1.29 ± 0.11 (range 1.19–1.76) vs. 1.01 ± 0.09 (range 0.60–1.18) in the 312 patients with a TID < 1.19 (P < 0.0001). Seventy of the 360 patients (19.4%) had a TID ≥ 1.15 (highest quartile of the derivation group). The mean TID in these 70 patients was 1.25 ± 0.11 (range 1.15–1.76) vs. 1 ± 0.09 (range 0.60–1.14) in the 290 patients with a TID < 1.15 (P < 0.0001).
Predictors of abnormal TID
Table 2 shows the distribution of clinical and functional parameters in the 12 patients with a TID ≥ 1.32 as compared to the 348 patients with a TID < 1.32. Six of the 12 patients had known CAD and CAG was available in 4 of them. Three of the four patients had obstructive CAD manifested as single-vessel disease in two and double-vessel disease in one. % Diameter stenosis of LAD lesions in the patients were 50–69% in 2 patients and > 90% in one. One patient had 50–69% RCA stenosis. All three patients underwent revascularization prior to the myocardial perfusion scan.
Univariate analysis showed that none of the parameters in Table 2, including age, gender, family history of CAD, known CAD, smoking, hypertension, diabetes, dyslipidemia, rest LVEF, post-stress LVEF, ΔLVEF, ≥ 5% decrease in LVEF (ΔLVEF ≤ − 5%) and ≥ 10% decrease in LVEF (ΔLVEF ≤ − 10%) were significantly associated with a TID ≥ 1.32.
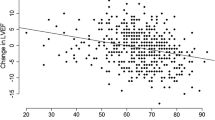
When a TID threshold of 1.19 was used to define an abnormal TID, univariate analysis showed that age (P = 0.02), rest LVEF (P = 0.003), ΔLVEF (P = 0.0008), and ΔLVEF ≤ − 5% (P ≤ 0.0001) were significantly associated with a TID ≥ 1.19. However, at multivariate analysis, only rest LVEF (P = 0.04) and ΔLVEF− 5% (P = 0.02) were significant predictors of a TID ≥ 1.19.
The TID threshold of 1.15 was associated with rest LVEF (P = 0.03), ΔLVEF (P = 0.001) and ΔLVEF ≤ − 5% (P = 0.003) in univariate analysis with ΔLVEF ≤ − 5% being a significant predictor of a TID ≥ 1.15 at multivariate analysis (P = 0.02).
Predictors of cardiac events
After a mean follow-up period of 31.2 ± 9.7 months (range 10–61 months), 42 patients (11.7%) had a cardiac event, including 9 (2.5%) hard (4 cardiac deaths and 5 nonfatal MI) and 33 (9.2%) soft events (25 revascularizations and 8 congestive heart failure requiring hospitalization). Early revascularization (< 60 days after the index SPECT scan) occurred in only two patients. SPECT result did not influence revascularization in these two patients, since it was normal showing relatively low TID of 1.09 and 1.26 that were not reported to the referring cardiologist.
At baseline, 30 of the 42 patients with cardiac events had known CAD with CAG reports available in 27 of them. Nineteen of those 27 patients had obstructive CAD manifested as single-vessel disease in 11, double-vessel disease in 3 and triple vessel disease in 5. % Diameter stenosis of LAD lesions in the patients were 50–69% in 3, 70–90% in 4 and > 90% in 6. The corresponding numbers for the LCX were 2, 2 and 1 patients, respectively and for the RCA, 2, 4 and 3 patients, respectively. The remaining 12 of the 42 patients did not have known CAD prior to myocardial perfusion scan and hence did not undergo CAG.
There was no apparent relationship between having multivessel disease and increased TID. Thus, based on the 81 patients who had obstructive CAD, abnormal TID was seen in 2 of the 43 patients (4.7%) with single-vessel disease, 1 of the 23 patients with double-vessel (4.3%) and 0 of the 15 patients (0%) with triple vessel disease.
At the time of event, 30 patients had CAG, 23 at our institution and 7 at an outside institution. Out of the 23 who had CAD at our institution, 4 had single-vessel disease, 11 double-vessel disease and 5 triple-vessel disease. % Diameter stenosis of LAD lesions in the patients were 50–69% in 4, 70–90% in 5 and > 90% in 6 patients. The corresponding numbers for the LCX were 7, 4 and 2 patients, respectively, and for the RCA, 3, 3 and 7 patients, respectively. The other 12 of the 42 patients had either fatal MI (n = 4) or congestive heart failure (n = 8), where CAG was not deemed necessary. One of the four patients with fatal MI had old MI prior to the scan, while the other three had known CAD with CAG performed at an outside institution. Seven of the 8 patients with congestive heart failure had known CAD of whom 4 had CAG at our institution showing single-vessel disease in 3 and triple-vessel disease in 1.
Among the variables of age, gender, family history of CAD, known CAD, smoking, hypertension, diabetes, dyslipidemia, TID as continuous variable, TID as cutoff values of ≥ 1.32, 1.19 and 1.15, rest LVEF, post-stress LVEF, ΔLVEF, ≥ 5% decrease in LVEF (ΔLVEF ≤ − 5%) and ≥ 10% decrease in LVEF (ΔLVEF ≤ − 10%), only known CAD (P < 0.001) and ≥ 10% decrease in LVEF (ΔLVEF ≤ − 10%) (P = 0.01) were significant predictors of future cardiovascular events. In contrast, TID as continuous variable or as cutoff values of ≥ 1.32 1.19 and 1.15 were not significant predictors (P = 0.25, 0.64, 0.63, and 0.73, respectively). Excluding the two patients with early revascularization did not affect the result of this analysis.
At multivariate analysis, known CAD (P < 0.0001) and ΔLVEF ≤ − 10% (P = 0.03) remained significant predictors of cardiac events.
TID and cardiac events
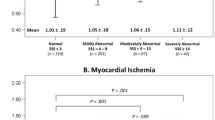
Figure 2a–c shows the hard, soft and total cardiac events in the patients with TID ≥ 1.32 vs. < 1.32, TID ≥ 1.19 vs. < 1.19 and TID ≥ 1.15 vs. < 1.15.

a Total, soft and hard cardiac event rates in the patients with and without a TID > mean + 2SD of the derivation group TID (≥ 1.32), b A TID > mean + SD of the derivation group TID (≥ 1.19) and c A TID ≥ 75th percentile of the derivation group TID (≥ 1.15)
No significant differences in the hard, soft or total cardiac event rates were found between the patients with and without a TID ≥ 1.32 (P = 0.27, 0.99 and 0.64, respectively; Fig. 2a), with and without a TID ≥ 1.19 (P = 0.34, 0.28 and 0.63, respectively; Fig. 2b) and with and without a TID ≥ 1.15 (P = 0.69, 0.82 and 0.73, respectively; Fig. 2c).
The positive predictive values (PPVs) of the TID thresholds of 1.32, 1.19 and 1.15 for predicting cardiac events were 16.7%, 8.3% and 12.9%, respectively. The sensitivities of these thresholds for cardiac events were 4.8%, 9.5%, and 21.4%, respectively.
Figure 3 shows the unadjusted and adjusted Kaplan–Meier survival curves in the patients with and without a TID ≥ 1.32, with and without a TID ≥ 1.19, and with and without a TID ≥ 1.15. Event-free survivals were similar in patients with a TID ≥ and < 1.32 (P = 0.68), in patients with a TID ≥ and < 1.19 (P = 0.4), and in patients with a TID ≥ and < 1.15 (P = 0.79). The unadjusted hazard ratio (95% confidence intervals) for cardiac events for TID ≥ 1.32 was 1.34 (0.32–5.60), P = 0.68, while the hazard ratio adjusted for the variables of known CAD and ≥ 10% decrease in LVEF was 1.49 (0.36–6.20), P = 0.58. The unadjusted hazard ratio (95% confidence intervals) for cardiac events for TID ≥ 1.19 was 0.64 (0.23–1.81), P = 0.40, while the hazard ratio adjusted for the variables of known CAD and ≥ 10% decrease in LVEF was 0.56 (0.20–1.59), P = 0.28. The unadjusted hazard ratio (95% confidence intervals) for cardiac events for TID ≥ 1.15 was 1.11 (0.53–2.31), P = 0.79, while the hazard ratio adjusted for the variables of known CAD and ≥ 10% decrease in LVEF was 1.02 (0.48–2.16), P = 0.95.


a, b Unadjusted and adjusted Kaplan–Meier survival curves in the patients with and without a TID > mean + 2SD of the derivation group TID (≥ 1.32), c, d A TID > mean + SD of the derivation group TID (≥ 1.19) and e, f A TID ≥ 75th percentile of the derivation group TID (≥ 1.15) showing similar event-free survivals in both groups of patients (see text)
Discussion
Our study is the first to address the significance of TID in patients with normal myocardial perfusion using a 2-day adenosine stress/rest 99mTc-sestamibi protocol [16,17,18,19,20,21,22].
The thresholds used to define an abnormal TID were: > derivation group’s mean TID + 2SD (TID ≥ 1.32) or 1SD (TID ≥ 1.19) or a TID ≥ the 75th percentile of the derivation group (TID ≥ 1.15). The > mean TID + 2SD approach has been employed in most previous studies [3, 4, 6, 11, 16, 17, 19]; however, other studies explored the use of the derivation group’s mean TID + 1SD as an abnormal TID cutoff [17, 20]. The highest quartile approach was previously based on the validation rather than the derivation group and represented a post hoc analysis rather than one based on a predefined threshold from a control population [10, 19].
Our derived abnormal threshold based on the derivation group’s mean + 2SD (1.32) is similar to the 1.31 threshold reported in patients undergoing rest/regadenoson stress 99mTc-tetrofosmin SPECT [17], the 1.39 threshold in patients undergoing rest 201Tl/regadenoson stress 99mTc-sestamibi dual-isotope SPECT [11] and the abnormal TID threshold of 1.37 for rest 201Tl/adenosine stress 99mTc-sestamibi dual-isotope SPECT [6]. However, lower abnormal TID thresholds ranging from 1.12 to 1.23 were found for rest 201Tl/exercise stress 99mTc-sestamibi dual-isotope SPECT (1.23) [4], rest/exercise 99mTc-sestamibi SPECT (1.19) [18], rest/exercise 99mTc-sestamibi SPECT (1.16) [16], rest/adenosine 99mTc-sestamibi SPECT (1.22) [16], rest/dipyridamole 82Rb PET (1.14) [5] and for the now obsolete exercise/redistribution 201Tl SPECT (1.12) [3], suggesting that the abnormal TID threshold may be radioisotope/radiotracer and protocol-specific, the latter including the modality and/or drug used to stress the patients [2,3,4,5,6, 11, 16,17,18].
It appears that the TID using adenosine stress is somewhat higher than with exercise even using the same radiotracers. Thus, the reported TID for rest 201Tl/adenosine stress 99mTc-sestamibi is 1.37 vs. 1.23 for rest 201Tl/exercise stress 99mTc-sestamibi [4, 6]. Doukky et al. also reported slightly higher TID values with rest/adenosine 99mTc-sestamibi compared with rest/exercise 99mTc-sestamibi (1.22 vs. 1.16) [16].
Factors affecting TID in patients with normal perfusion
Our study in patients with normal perfusion did not find that any of the clinical and functional parameters examined were predictive of an abnormal TID > mean + 2D. This could, in part be due to the small sample size of patients exceeding this threshold (n = 12). In fact, in multivariate analysis, TID ≥ 1.19 and ≥ 1.15 seen in 48 and 70 patients, respectively were predicted by ≥ 5% decrease in LVEF, a perhaps expected finding considering that the TID may be due to increased post-stress LVESV and LVEDV compared with rest. Interestingly, unlike Doukky et al. our study did not find association between TID and diabetes or known CAD [16].
TID and cardiac events
The most critical finding of our study is that, in patients with normal perfusion the TID as a continuous variables or as cutoff value was not significantly associated with increased cardiac events with similar cardiac event-free survivals in patients with TID at or above vs. below these cutoff values.
The PPVs of the three TID thresholds were very poor (8.3–16.7%). While a TID ≥ 1.32 had the highest PPV, 10 of 12 patients (83%) with such TID did not have any cardiac event over more than a 2.5-year follow up period. Moreover, the only 2 patients with TID ≥ 1.32 who experienced cardiac events represented only 4.8% of those who experienced a cardiac event subsequent to the stress/rest adenosine study.
Lack of association between TID and the presence of severe and/or extensive CAD or major adverse cardiac events (MACE) was reported in contemporary studies of patients with normal perfusion [21, 22]. For example, Valdiziezo et al. found an 11% incidence of left main or multivessel CAD in 28 patients with TID vs. a 16% incidence in 68 patients without TID with no significant increase in the incidence of any CAD in the TID patients [21]. Halligan et al. also not did find an increased incidence of multivessel disease or MACE in patients with TID and normal perfusion [22]. However, Doukky et al. found that TID is associated with a higher cardiac event rate in patients with diabetes and/or known CAD despite having normal perfusion on rest/stress 99mTc-sestamibi SPECT [16]. No such association was found in our study, where the cardiac event rates were similar between patients with TID who were diabetic and those who were not, those with and without known CAD and those with both diabetes and CAD vs. those without this combination (data not shown). Overall, the majority of studies support our finding of a lack of association between TID and cardiac events or severe/extensive CAD in patients with normal myocardial perfusion. The advantage of cardiac events analysis in our study is the potential for capturing adverse events that may occur despite insignificant CAD due to occult coronary microvascular dysfunction (CMD), which, similar to post-stress LVEF reduction may be responsible for the TID in some patients with normal perfusion who have multiple risk factors, including diabetes, hypertension, known CAD, and, potentially old age [23, 24]. It is important to emphasize, however, that the cause of abnormal TID in patients with normal perfusion remains unclear.
While agreeing with most contemporary studies on TID, our findings are different from those of older studies which found higher cardiac event rates in patients with normal (SSS = 0) or near normal (SSS ≤ 3) perfusion. Most notably, Abidov et al. showed that TID increased the risk of cardiac events threefold (2.4% vs. 0.8% year, P = 0.001) in 1560 patients with a SSS of 0 and no resting LV enlargement and about twofold (2.2% vs. 1.0%/year, P = 0.002) in 2037 patients with an SSS ≤ 3 and no resting LV enlargement [19]. The decreasing incidence of severe CAD or cardiac events in patients with TID and normal perfusion in contemporary compared to older studies is believed to be, in part related to the decreasing prevalence of ischemia on myocardial SPECT studies, declining from 29.6% in 1991 to 5.0% in 2009 [2, 17, 25]. In fact, Bourque argues that the decreasing presence and severity of CAD resulted in a decline in the PPV of TID for severe CAD with the abnormal TID now more likely representing another cause, such as the manifestation of cardiomyopathy or measurement variance [2, 20].
Limitations
One of the limitations of our study is its retrospective nature and that it was conducted at a single institution. We did not have a sufficient number of patients who underwent CAG to draw firm conclusions regarding the presence of severe and/or extensive CAD in patients with abnormal TID vs. those without, because patients with normal perfusion, even with abnormal TID typically do not undergo CAG unless other findings are present compelling the cardiologist to perform CAG. This was one of the main reasons for using cardiac events as the primary endpoint in our study.
Conclusion
The present study showed that TID does not confer an adverse prognosis and is not an independent prognosticator in patients with normal perfusion on adenosine stress/rest 99mTc-sestamibi SPECT. Our findings add to existing evidence that TID in these patients is typically benign and should not automatically expose patients to coronary angiography and, therefore, have implications in patient management. Notwithstanding all speculations, the cause of abnormal TID in patients with normal perfusion remains unclear.
References
Dorbala S, Ananthasubramaniam K, Armstrong IS, Chareonthaitawee P, DePuey EG, Einstein AJ, et al. Single photon emission computed tomography (SPECT) myocardial perfusion imaging guidelines: instrumentation, acquisition, processing, and interpretation. J Nucl Cardiol. 2018;25:1784–846.
Bourque JM. Contemporary relevance of TID: based on the company it keeps. J Nucl Cardiol. 2015;22:535–8.
Weiss AT, Berman DS, Lew AS, Nielsen J, Potkin B, Swan HJ, et al. Transient ischemic dilation of the left ventricle on stress thallium-201 scintigraphy: a marker of severe and extensive coronary artery disease. J Am Coll Cardiol. 1987;9:752–9.
Mazzanti M, Germano G, Kiat H, Kavanagh PB, Alexanderson E, Friedman JD, et al. Identification of severe and extensive coronary artery disease by automatic measurement of transient ischemic dilation of the left ventricle in dual-isotope myocardial perfusion SPECT. J Am Coll Cardiol. 1996;27:1612–20.
Rischpler C, Higuchi T, Fukushima K, Javadi MS, Merrill J, Nekolla SG, et al. Transient ischemic dilation ratio in 82Rb PET myocardial perfusion imaging: normal values and significance as a diagnostic and prognostic marker. J Nucl Med. 2012;53:723–30.
Abidov A, Bax JJ, Hayes SW, Cohen I, Nishina H, Yoda S, et al. Integration of automatically measured transient ischemic dilation ratio into interpretation of adenosine stress myocardial perfusion SPECT for detection of severe and extensive CAD. J Nucl Med. 2004;45:1999–2007.
Marcassa C, Galli M, Baroffio C, Campini R, Giannuzzi P. Transient left ventricular dilation at quantitative stress-rest sestamibi tomography: clinical, electrocardiographic, and angiographic correlates. J Nucl Cardiol. 1999;6:397–405.
Bestetti A, Di Leo C, Alessi A, Triulzi A, Tagliabue L, Tarolo GL. Post-stress end-systolic left ventricular dilation: a marker of endocardial post-ischemic stunning. Nucl Med Commun. 2001;22:685–93.
Peace RA, McKiddie FI, Staff RT, Gemmell HG. Comparison of methods for quantification of transient ischaemic dilation in myocardial perfusion SPET. Nucl Med Commun. 2000;21:971–6.
Hung GU, Lee KW, Chen CP, Lin WY, Yang KT. Relationship of transient ischemic dilation in dipyridamole myocardial perfusion imaging and stress-induced changes of functional parameters evaluated by Tl-201 gated SPECT. J Nucl Cardiol. 2005;12:268–75.
Katz JS, Ruisi M, Giedd KN, Rachko M. Assessment of transient ischemic dilation (TID) ratio in gated SPECT myocardial perfusion imaging (MPI) using regadenoson, a new agent for pharmacologic stress testing. J Nucl Cardiol. 2012;19:727–34.
D’Agostino RB Sr, Vasan RS, Pencina MJ, Wolf PA, Cobain M, Massaro JM, et al. General cardiovascular risk profile for use in primary care: the Framingham heart study. Circulation. 2008;117:743–53.
Benz DC, Gaemperli O. The right timing for post-ischemic stunning. J Nucl Cardiol. 2017;24:1302–4.
Thygesen K, Alpert JS, Jaffe AS, Simoons ML, Chaitman BR, White HD. Third universal definition of myocardial infarction. Global Heart. 2012;7:275–95.
Mente S, Kuhn M. The use of the R language for medicinal chemistry applications. Curr Top Med Chem. 2012;12:1957–64.
Doukky R, Frogge N, Bayissa YA, Balakrishnan G, Skelton JM, Confer K, et al. The prognostic value of transient ischemic dilatation with otherwise normal SPECT myocardial perfusion imaging: a cautionary note in patients with diabetes and coronary artery disease. J Nucl Cardiol. 2013;20:774–84.
Golzar Y, Olusanya A, Pe N, Dua SG, Golzar J, Gidea C, et al. The significance of automatically measured transient ischemic dilation in identifying severe and extensive coronary artery disease in regadenoson, single-isotope technetium-99m myocardial perfusion SPECT. J Nucl Cardiol. 2015;22:526–34.
Xu Y, Arsanjani R, Clond M, Hyun M, Lemley M Jr, Fish M, et al. Transient ischemic dilation for coronary artery disease in quantitative analysis of same-day sestamibi myocardial perfusion SPECT. J Nucl Cardiol. 2012;19:465–73.
Abidov A, Bax JJ, Hayes SW, Hachamovitch R, Cohen I, Gerlach J, et al. Transient ischemic dilation ratio of the left ventricle is a significant predictor of future cardiac events in patients with otherwise normal myocardial perfusion SPECT. J Am Coll Cardiol. 2003;42:1818–25.
Mandour Ali MA, Bourque JM, Allam AH, Beller GA, Watson DD. The prevalence and predictive accuracy of quantitatively defined transient ischemic dilation of the left ventricle on otherwise normal SPECT myocardial perfusion imaging studies. J Nucl Cardiol. 2011;18:1036–43.
Valdiviezo C, Motivala AA, Hachamovitch R, Chamarthy M, Navarro PC, Ostfeld RJ, et al. The significance of transient ischemic dilation in the setting of otherwise normal SPECT radionuclide myocardial perfusion images. J Nucl Cardiol. 2011;18:220–9.
Halligan WT, Morris PB, Schoepf UJ, Mischen BT, Spearman JV, Spears JR, et al. Transient ischemic dilation of the left ventricle on SPECT: correlation with findings at coronary CT angiography. J Nucl Med. 2014;55:917–22.
Marciano C, Galderisi M, Gargiulo P, Acampa W, D’Amore C, Esposito R, et al. Effects of type 2 diabetes mellitus on coronary microvascular function and myocardial perfusion in patients without obstructive coronary artery disease. Eur J Nucl Med Mol Imaging. 2012;39:1199–206.
Obeidat OS, Alhouri A, Baniissa B, Alqaisi O, Akkawi M, Zyad H, et al. Prognostic significance of post-stress reduction in left ventricular ejection fraction with adenosine stress in Jordanian patients with normal myocardial perfusion. J Nucl Cardiol. 2020;27:1596–606.
Rozanski A, Gransar H, Hayes SW, Min J, Friedman JD, Thomson LE, et al. Temporal trends in the frequency of inducible myocardial ischemia during cardiac stress testing: 1991 to 2009. J Am Coll Cardiol. 2013;61:1054–65.
Acknowledgements
No potential conflicts of interest were disclosed.
Funding
No funding source was used to support this work.
Author information
Authors and Affiliations
Contributions
MEJ and AA were responsible for the conception and design of the study, analysis and interpretation of data, drafting and final approval of the manuscript. OSO has contributed to the analysis and interpretation of data and approved the final manuscript. BB, ZFA-R, NR, MS, MA, ABI, AA and SA were actively involved in collecting and analyzing data and approved the final manuscript. DR was actively involved in statistical analysis and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval
The study was approved by the Institutional Review Board (IRB) of Jordan University Hospital.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Juweid, M.E., Alhouri, A., Baniissa, B. et al. Transient ischemic dilatation with adenosine 99mTc-sestamibi stress: prognostic significance in patients with normal myocardial perfusion. Ann Nucl Med 35, 569–579 (2021). https://doi.org/10.1007/s12149-021-01599-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12149-021-01599-3