
Abstract
Impulsivity-characterized executive function impairments have been hypothesized to represent mechanisms underlying the symptomology associated with gambling disorder (GD). Despite this, a clear profile of executive function within GD has yet to be established. Furthermore, it remains unclear whether executive function deficits represent a vulnerability marker for the disorder. This study assessed executive function performance within a GD sample compared to a sample of familial relatives and community controls. Using a family study methodology, a broad assessment of executive function was administered to analyze performance differences and their potential characterization by impulsivity between a sample of individuals meeting criteria for GD, their first-degree familial relatives, and a community control sample. Performance differences emerged regarding the capacity to delay gratification and inhibit automatic task-irrelevant responses between the GD and control samples. Results support the presence of impulsive choice and impulsive cognitive bias as components of the GD executive functioning profile. Similar difficulties inhibiting automatic attentional shifting were observed within the first-degree relative sample. Executive functioning within GD appears to be characterized by an impulsive pattern of behaviours/decisions but impacts processes differently. Evidence suggests that individuals diagnosed with GD demonstrate a statistically different capacity to delay gratification (e.g. a propensity towards smaller, more immediate rewards as opposed to larger delayed rewards) and inhibit cognitive biases (e.g. difficulty shifting attention away from task-irrelevant stimuli). This latter difference may represent a vulnerability marker of GD as preliminary evidence was provided for similar difficulties in a first-degree relative sample. Further research must replicate these findings and assess the impact of task modality, symptom severity, and comorbidity on the observation of executive functioning impairment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Gambling disorder (GD) is characterized by persistent and habitual patterns of problematic behaviours despite their negative consequences leading to clinically significant impairment (American Psychiatric Association, 2013). The presence and severity of gambling symptoms have been shown to predict functional outcomes for the individual (Petry & Armentano, 1999) and their familial relatives (Kourgiantakis et al., 2013). Research has demonstrated that problematic gambling behaviours are associated with familial conflict (Shaw et al., 2007), as well as legal (May-Chahal et al., 2017), psychiatric (Lorains et al., 2011), and financial difficulties (Grant et al., 2010). To improve our capacity to treat GD, there is a need for further research aimed at understanding both its maintenance and etiological factors.
Broadly, deficits in executive function, a hierarchical category of high-order cognitive processes (e.g. working memory, response inhibition, mental flexibility), may underlie and maintain addictive disorders, including GD (Noël et al., 2013; Pallanti et al., 2021). Such models of GD are supported by evidence of impairments related to cognitive flexibility (Ellis et al., 2018; Leppink et al., 2016), planning (Ellis et al., 2018; Kräplin et al., 2014), response inhibition (Brevers et al., 2012a, 2012b; Mestre-Bach et al., 2020), working memory (Brevers et al., 2012a, 2012b; Leiserson & Pihl, 2007), and decision-making (Ciccarelli et al., 2017; Fauth-Bühler et al., 2017; Perandrés-Gómez et al., 2021). While such findings have not consistently been replicated (Albein-Urios et al., 2012; Boog et al., 2014; Brevers et al., 2012a, 2012b; Hur et al., 2012; Ledgerwood et al., 2012, 2012; Manning et al., 2013; Sharif-Razi et al., 2019; Yan et al., 2014), it is widely accepted that disrupted executive function reflects a core component of the GD presentation.
More recently, executive functioning impairment within GD has been recognized to reflect a pattern of impulsivity (Mestre-Bach et al., 2020; Tiego et al., 2018; Yücel et al., 2019). Impulsivity refers to risky, hastily initiated, and inappropriate behaviours frequently leading to adverse outcomes (Evenden, 1999). Importantly, impulsivity is a complex multifactorial construct. Models of impulsivity have identified several separable domains, including but not limited to impulsive cognitive bias (i.e. difficulty suppressing inappropriate attentional bias), impulsive choice (i.e. propensity towards smaller, more immediate rewards as opposed to larger delayed rewards), impulsive behaviour (i.e. difficulty inhibiting inappropriate motor responses), and impulsive decision-making (i.e. tendency to make risky choices, specifically within situations of ambiguity) (MacKillop et al., 2016; Tiego et al., 2018, 2019). Applying this model, a recent meta-analysis provided evidence of deficits within GD across all domains of impulsivity, suggesting generalized impulsivity characterizes the cognitive profile of GD (Ioannidis et al., 2019). Despite such findings, results remain inconsistent, and further research using novel and broad neuropsychological measures is necessary to clarify the manifestation of impulsive behaviours/traits within GD samples.
Of note, previous research has highlighted the presence of impulsivity in the form of personality traits, cognitive control issues, and decision-making deficits in individuals with GD and their familial relatives. This suggests that impulsivity may represent a vulnerability marker of the disorder (Black et al., 2015a, 2015b). In further support of this finding, results from the Ioannidis et al. (2019) meta-analysis suggest that evidence of impulsive decision-making is present within samples characterized by problem gambling (i.e. individuals engaging in disordered gambling behaviour that does not meet GD diagnostic criteria). Despite this, it remains unclear whether broad executive functioning impairment characterized by impulsivity represents a vulnerability marker of GD or a product of chronic gambling behaviour. In light of this, there is clinical utility in the identification of methodology which supports the assessment of vulnerability markers for developing GD. One such method is comparisons of individuals with GD and unaffected first-degree familial relatives (i.e. parents, siblings, or children) (Ersche et al., 2010; Gottesman & Gould, 2003; Robbins et al., 2012). Research using a twin study methodology has suggested genetic factors account for approximately 50% of the risk of developing GD (Ibanez et al., 2003; Lobo, 2016; Slutske, 2000). Family studies, therefore, offer a unique opportunity to assess the manifestation of possible vulnerability markers in a sample that shares genetic and environmental factors (Hodgins et al., 2011). Despite this, research to date assessing first-degree relatives of individuals with GD has been limited, with even fewer studies assessing possible neurocognitive mechanisms. Additional research characterizing cognitive performance in GD samples and samples of their familial relatives could provide evidence supporting the identification of vulnerability markers and underlying mechanisms.
Current Study
This study characterizes the manifestation of a broad range of executive functioning processes within a sample of GD, their first-degree biological relatives, and a community control sample. The objective is to offer further evidence characterizing GD's executive functioning impairment as impulsive and providing characterizations of the cognitive profile of first-degree biological relatives of individuals with GD. To facilitate this, this study administered tasks validated in their assessment of domains of executive functioning, which have been previously identified as measures of impulsive attentional bias (i.e. the Colour-Word Interference Task; Hierarchy Paper), impulsive choice (i.e. the Delayed Discounting Task), impulsive decision-making (i.e. the Balloon-Analogue Risk Task, the Tower of London Task), impulsive behaviours (i.e. Stop-Signal Anticipation Task (Bonini et al., 2018, p. 201; Ioannidis et al., 2019; MacKillop et al., 2016; Tiego et al., 2018), and working memory (i.e. the Spatial Working Memory Task).
Based on the previously discussed literature, several hypotheses were proposed. We hypothesized that the GD sample would demonstrate broad executive functioning impairments reflective of an impulsive response pattern. Specifically, we anticipated that the GD sample would demonstrate a reduced capacity for response inhibition and delayed gratification compared to the control sample. Results reflecting decision-making, attention, and working memory have been more inconsistent within the literature, yet impulsive performance patterns have been observed. Therefore, we hypothesized that performances on measures of these domains would demonstrate a pattern of impulsivity within the GD sample compared to the control sample. Finally, given previous research, which has suggested that impulsivity may reflect a vulnerability marker of GD, we hypothesized that performances observed within the first-degree relative sample would demonstrate a similar pattern of impulsivity to that observed within the GD sample.
Methods
Participants
The study sample consisted of 40 participants meeting lifetime criteria for GD (DSM-5; American Psychiatric Association, 2013), 19 of their first-degree biological relatives, and 50 community controls (see Table 1). Using a convenience sampling methodology, the GD and the control samples were recruited using community announcements (e.g. online ads, posters), advertisements at local treatment facilities, and an existing research registry. Control participants were excluded if they met lifetime criteria for GD or had a family history of GD. Relatives were contacted using information provided by the GD sample and included parents (n = 7), children (n = 5), and siblings (n = 7). The following exclusion criteria were applied to all participants and subgroups: (1) age less than 18 years; (2) IQ less than 80; (3) diagnosis with a neurological condition (e.g. multiple sclerosis, epilepsy, stroke, AIDS, traumatic brain injury); or (4) diagnosis with a psychotic disorder that could confound measurement of cognitive function. Participants were also excluded if they reported any condition(s), medical or otherwise, that would make participation in the study difficult or confound the study's analysis.
Procedure
All procedures were approved by the University of Calgary Conjoint Facilities Research Ethics Board and aligned with the 1964 Helsinki Declaration (World Medical Association, 2013). All participants were screened during a phone interview. Diagnosis was verified in person using the Structured Clinical Interview for the DSM-5 (First et al., 2016). The presence of mood, psychotic, substance use, anxiety, eating, adult attention-deficit hyperactivity, obsessive–compulsive, and trauma/stress-related disorders were assessed. Diagnosis of GD was further verified using the Composite International Diagnostic Interview (CIDI; Kessler et al., 2008). All diagnoses were verified using case discussions attended by at least one of the principal investigators (MASKED). Before any study procedures were completed, informed written consent was obtained. The measures analyzed were administered over 2 days as part of a larger test battery. Gift cards were provided as a reimbursement.
Clinical Measures
Clinical constructs were assessed using validated clinical measures to assist in characterizing the participants. Gambling symptomology and severity were indexed using the Problem Gambling Severity Index (PGSI). This is a nine-item self-report questionnaire (α = 0.943) demonstrating satisfactory psychometrics (Currie et al., 2013; Holtgraves, 2009). The PGSI queries potential problems resulting from gambling, coded from 0 (“never”) to 4 (“almost always”), with responses summed for a total score. Recent psychological symptomology was similarly assessed. Depressive mood experiences and symptoms were assessed using the widely used and psychometrically acceptable (Aben et al., 2002) 17-item version (α = 0.848) of the Hamilton Depression Rating Scale (HAMD; Hamilton, 1960). Manic symptomology was assessed using the valid and reliable Young Mania Rating Scale (YMRS; Young et al., 1978). The YMRS is an 11-item measure (α = 0.462, Inter-Item Correlation = 0.074) which assesses manic experiences over the past 48 h. Premorbid intelligence was estimated using the validated (Green et al., 2008) Wechsler Test of Adult Reading measure (WTAR; Wechsler, 2001). Based on case discussion, psychosocial and occupational functioning was measured using the validated and reliable Social and Occupational Functioning Assessment Scale (SOFAS; Morosini et al., 2000).
Cognitive Tasks
Color-Word Interference Test (CWIT)
The CWIT is a valid and reliable (Shunk et al., 2006) paper and pencil-based assessment of inhibitory control from the Delis-Kaplan Executive Function System (Delis et al., 2004). This measure has moderate reliability, high internal consistency, and satisfactory validity (Delis et al., 2004). It consists of four distinct conditions (i.e. colour naming, word reading, inhibition, and inhibition/switching). Performances within each condition are scaled based on normative age-appropriate data. This assessment allows for examining performance on a factor-by-factor basis through contrasting performance within each of the four conditions, comparing speed scores, and scoring accuracy.
Tower of London Task (ToLT)
The ToLT is an executive function assessment with demonstrated construct validity (Debelak et al., 2016), criterion validity, and reliability (Köstering et al., 2015) which provides a measurement of planning, decision-making, and problem-solving (Shallice, 1982). Participants are asked to recreate a presented tower with a similar tower consisting of coloured rings. Two rules are applied while completing this task (1: The number of rings staked cannot exceed the bar’s capacity; 2: Only one ring can be moved at a time). Participants complete this task over ten trials.
Spatial Working Memory Task (SWMT)
The SWMT is a computer-based assessment with demonstrated reliability and validity previously used to assess visuospatial working memory (Almeida et al., 2015; Glahn et al., 2002). Participants are exposed to two conditions, maintenance and manipulation. During the maintenance condition, participants must remember the spatial location of a set of three circles presented for 1500 ms. After a 6000 ms delay, the second set of three circles is presented. Participants are asked to verify whether the new set of circles is presented in the exact spatial location and orientation as the initial set. Participants are presented with similar stimuli for the manipulation condition and asked if they represent a mirror flip of the first set of circles.
Stop-Signal Anticipation Task (SSAT)
The SSAT is a widely used (Clark et al., 2020) measure of response inhibition and, more specifically, the processes of reactive and proactive inhibition (Zandbelt & Vink, 2010). Three horizontal lines are displayed in this task, one above the other. On every trial, a bar is presented, which rises towards the middle-presented line. The time between the line beginning to move and reaching the middle line is set at a constant duration of 800 ms. Trials are presented within three blocks, which consisted of stop trials pseudo-randomly interspersed between go trials. In go trials, the participant is tasked with stopping the bar as close as possible to the middle line by pressing the spacebar. On stop trials, representing the minority of trials, the bar would stop automatically before reaching the second line. The sudden stopping of the line represents a stop signal and signals to the participant that a button depress response should be inhibited. The likelihood of a stop signal being presented is manipulated across each trial. It is cued based upon the colour of the lines presented (i.e. green: 0%, yellow: 17%, amber: 20%, orange: 25%, and red: 33%). The presentation of the stop signal is adjusted throughout the task based on the participants responding accuracy. The task’s difficulty is increased and decreased as necessary, manipulated by stop-signal presentation, so that accuracy was maintained at 50%.
Balloon Analogue Risk Task (BART)
Openness to risky behaviours was measured using the demonstrated reliable and valid (Lejuez et al., 2007; Weafer et al., 2013; White et al., 2008) computerized BART (Lejuez et al., 2002). With this measure, participants inflate a balloon, earning a single point for each pump. If the balloon pops, the participant loses all the collected points. This procedure is repeated over 30 trials. Unfortunately, participants are not provided with an opportunity to test the propensity for popping (i.e. evaluate risk) as there are no practice trials in this measure.
Delayed Discounting Task (DDT)
The capacity to delay gratification was assessed using the DDT, a valid and reliable computer-based assessment of the subjective value of a delayed reward (Bailey et al., 2021; Reynolds & Schiffbauer, 2004; Weafer et al., 2013). The DDT comprises 100 questions, which query whether the participant would prefer a reward now or a larger award later. Questions are presented using an adjusted-amount procedure (Richards et al., 1999). The amount of immediate reward is adjusted across successive trials until an amount is reached that the participant judges to be equivalent to the delayed reward. This amount represents the participant’s subjective valuation of the delayed reward. This point of subjective equality is referred to as the indifference point. Indifference points were assessed at seven different delays: 1 week, 2 weeks, 1 month, 6 months, 1 year, 5 years, and 25 years. After each question, the amount of the immediate reward is adjusted. If the smaller-sooner reward was selected, the amount of that reward is decreased by $25 in the subsequent choice trial. Alternatively, if the larger-latter reward was selected, the amount of the sooner reward was increased by $25. Subsequent adjustments to the immediate reward were 50% of the preceding adjustment. The amount of immediate reward following the tenth-choice trial was used as the indifference point for that delay. At each subsequent delay, the amounts of the smaller-immediate reward and the larger-delayed reward were returned to $50 and $100, respectively, and the titration procedure was repeated.
Statistical Analysis
All tests were performed using SPSS for Windows, version 26.0 (IBM, 2019) and were two-tailed. Outliers, normality, and test assumptions for each analysis were assessed and corrected if necessary. Demographic information for the three groups was compared using univariate ANOVA, Chi-Square test, and Fisher’s exact test when appropriate analyses of variance (ANOVA) models were conducted for each administered tasks to observe for statistical between-group performance differences. Effect sizes, p values, and 95% confidence intervals are reported and interpreted based on accepted guidelines. To test the proposed hypotheses, planned comparisons were conducted regardless of the presence of a significant main effect. Preliminary analyses included family ID as a nested variable to assess for variance related to familial relationships. Familial relationships failed to demonstrate a significant interaction with the group condition in any of the analyses conducted and, therefore, was excluded from the analysis to preserve power.
Cognitive Task Analysis
Separate multivariate ANOVAs (MANOVA) were conducted to test for performance differences on the CWIT. Performance on each primary condition (DV: 4 levels: colour naming, word reading, inhibition, and inhibition/switching) was compared using a MANOVA with group (IV: 3 levels; GD, relatives, controls) as the between-subjects factor. Contrast differences were assessed using a MANOVA with inhibition vs. colour naming, inhibition/switching vs. colour reading + word reading, inhibition/switching vs. inhibition, inhibition/switching vs. colour naming, and inhibition/switching vs. word reading as the dependent variables and group (3 levels: GD, relative, controls) as the independent variable. Finally, the frequency of errors was compared between the groups using a MANOVA with group (3 levels: GD, relative, control) as the independent variable and colour naming errors, word reading errors, inhibition errors, and inhibition/switching errors as the dependent variables.
A univariate ANOVA (group: 3 levels: GD, relative, control) was used to assess differences in relation to overall achievement scores (DV) on the ToLT. An additional MANOVA was conducted to further query between-group performance differences with group as the between-subject factor and total rule violations percentile, scaled mean time until the first move, scaled time-per-move ratio, move accuracy ratio, and rule violations per item ratio as the dependent variables.
To assess for between-group differences regarding accuracy (IV: total score) and reaction time (IV: mean reaction time) on the SWMT, separate ANOVAs were conducted. Both ANOVAs followed a 2 (group: GD, relative, control) × 2 (condition: maintenance, manipulation) mixed model design.
Performance on the SSAT was assessed for differences in the respective processes of reactive and proactive inhibition. Reactive inhibition was assessed using average stop-signal reaction time (SSRT), calculated using the integration method (Verbruggen & Logan, 2008). This method facilitates the calculation of stop-signal reaction time by subtracting the nth reaction time from the mean stop-signal delay. The nth reaction time is identified by multiplying the number of trials by the probability of the participant responding on the stop-signal trial. Outliers for the analysis were identified as reaction times that exceeded 1.5 × the inter-quartile range away from the 25th and 75th percentiles of the reaction time distribution. The remaining reaction times were averaged per task condition (4 stop-signal probability levels) and compared between groups. A mixed model ANOVA was used to assess for differences regarding proactive inhibition with group (3 levels: GD, relatives, controls) as the between-subject variable and stop-signal probability (4 levels: 17%, 20%, 25%, 30%) as the within-subject variable.
Performance on the BART was assessed using a MANOVA, with group (3 levels: GD, relative, controls) as the independent variable and each of the outcome scores of interests (3 levels: adjusted total score, total number of pumps, average reaction time) as the dependent variables. Cutoff was applied to the reaction time data to reduce the confounding impact of poor effort. Per group cutoffs were specified as average reaction times greater than the mean + 2 SDs.
Differences regarding performance on the DDT were assessed using model fit estimates and a follow-up univariate ANOVA. Median indifference points, reflecting the point where the amount of the smaller-sooner outcome is regarded as equal to the present value of the larger-later outcome, for each group were fit to the Mazur hyperbola (Mazur, 1987) and the Myerson and Green (Myerson & Green, 1995) hyperboloid models. Indifference points were calculated in alignment with the process outlined above in the measures section. Akaike information criterion (AIC), a weighted index of variance accounted for by the model as a factor of its number of parameters, was utilized to select the most appropriate analysis model. Based upon the model of best fit, between-group comparisons were carried out using a one-way (group; 3 levels; GD, relative, control) ANOVA using the average area under the curve (AUC), the sum of the trapezoidal area between each set of adjacent indifference points for each group as the dependent variable. Since it was demonstrated that the Myerson and Green hyperboloid ((Myerson & Green, 1995) provided the best fit for the data, the free-parameter k, indicating a measure of the degree of discounting, was not used. In the Myerson and Green model, k interacts with the value of s, an exponential scaling parameter, and therefore is not an independent index of delayed discounting. Finally, non-systematic delayed discounting data were excluded from the analysis based on the criteria and algorithm developed by Johnson and Bickel (2008).
Results
Demographics
The samples were shown to be not statistically different regarding age, handedness, marital status, level of employment, annual income, mania symptom ratings (i.e. YMRS), and estimated intelligence (i.e. word reading; WTAR). However, samples differed on gender, the number of years of education, gambling symptoms, depression symptom ratings, and psychosocial/occupational functioning. See Table 1 for a list of statistics and significance values. Comorbid mental health disorders for each sample are displayed in Table 2.
Neuropsychological Measures
The results for each impulsivity domain assessed are outlined below. See Table 3 for means, standard deviations, and contrast statistics.
Inhibitory Control
A non-significant main group effect was observed regarding performance on the primary four conditions of the CWIT (Pillai’s Trace = 0.11, F(8, 96) = 1.34, p = 0.227, np2 = 0.056). Planned comparisons in alignment with the study’s goals were carried out. Non-significant differences were observed between the samples regarding colour naming, word reading, and inhibition/switching performance. In contrast, a significant effect was observed regarding inhibition performance (F(2, 93) = 4.28, p = 0.017, np2 = 0.084). The relative (Mean Δ = 1.80, p = 0.008, 95% CI [0.48, 3.11]) and the GD samples (Mean Δ = 1.06, p = 0.043, 95% CI [0.03, 2.09]) both demonstrated cognitive inhibitory performances significantly below that demonstrated by the control sample. Performance analysis regarding the primary contrasts returned a similar non-significant main effect of group (Pillai’s Trace = 0.053, F(8, 176) = 0.60, p = 0.779, np2 = 0.026). Non-significant between-group differences were supported based on planned comparisons. Similar non-significant differences were observed from the MANOVA assessing between-group differences regarding error rates on each condition (Pillai's Trace = 0.072, F(8, 172) = 0.799, p = 0.604, np2 = 0.036) and the conducted planned comparisons.
Decision-Making/Planning
Total achievement scores derived from the TolT were shown to be statistically similar between the samples (F(2, 98) = 0.642, p = 0.528, np2 = 0.013). The main effect of group derived from a MANOVA analyzing the optional performance measures was non-significant (Pillai’s Trace = 0.156, F(10, 188) = 11.59, p = 0.113, np2 = 0.078). Planned comparisons generally provided further evidence of similar performances between the study samples regarding mean first move time, mean time-per-move ratio, move accuracy ratio, and rule-violations per item ratio. Total rule violations, represented as a scaled percentile rank, reflected a significant between-group difference (F(2, 81) = 4.70, p = 0.012, np2 = 0.104) reflective of the relative sample performing significantly worse than the GD sample (Mean Δ = − 31.097, p = 0.004, 95% CI [− 51.84, − 10.36]).
Working Memory
The repeated measures ANOVA analyzing working memory performance returned an expected significant effect of condition (F(1, 95) = 28.28, p < 0.001, np2 = 0.229). In contrast, the between-group effect (F(2, 95) = 1.13, p = 0.327, np2 = 0.023) and interaction (F(2, 95) = 0.793, p = 0.455, np2 = 0.016) were non-significant. A similar pattern of effects was observed with the repeated measures ANOVA assessing reaction time with an expected significant effect of condition (F(1, 95) = 54.01, p < 0.001, np2 = 0.046), a non-significant between-group effect (F(2, 95) = 0.61, p = 0.544, np2 = 0.013), and non-significant interaction (F(2, 95) = 2.29, p = 0.107, np2 = 0.362). All planned comparisons between the study samples regarding differences in working memory performance and reaction times on the separate conditions were non-significant.
Reactive and Proactive Inhibition
Despite slower average performance within our proband sample (see Table 3) compared to both the relative and control sample, measured by SSRT and reflective of poorer reactive inhibition, the overall effect of group failed to reach significance (F(2, 52) = 1.93, p = 0.153, np2 = 0.074). Planned comparisons between the study samples corroborated this performance pattern with no significant differences. Regarding proactive inhibition, a significant main effect of trial probability was demonstrated (Wilks Lambda = 0.81, F(3, 57) = 4.35, p = 0.008, np2 = 0.19), while neither the between-group comparison (F(1, 59) = 0.093, p = 0.911, np2 = 0.003) nor the interaction (Wilks Lambda = 0.87, F(6, 114) = 1.39, p = 0.226, np2 = 0.068) reached significance. Planned comparisons were carried out, which supported the lack of significant between-group differences.
Risky Behaviour Propensity
The main effect of group was observed to be significant (Pillai’s Trace = 0.140, F(6, 186) = 0.2.33, p = 0.034 np2 = 0.070). Univariate comparisons revealed non-significant differences regarding adjusted total score (i.e. risky behaviour propensity) (F(2, 97) = 0.07, p = 0.936, np2 = 0.001) and total number pumps (F(2, 94) = 0.31, p = 0.736, np2 = 0.007), but indicated a significant between-group difference associated with average reaction time (F(2, 94) = 3.61, p = 0.031, np2 = 0.071). Follow-up planned comparisons revealed significantly slower reaction times within the relative sample compared to the control sample (Mean Δ = 86.73, p = 0.014, 95% CI [18.29, 155.18]). No other significant differences were observed.
Delayed Discounting
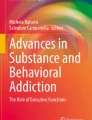
Model fit analysis results, utilizing proportional median indifference points derived from the DDT, are presented in Table 4 below. Figure 1 below displays median indifference points, expressed as a proportion of the delayed reward amount, organized by study group. Model parameters (e.g. k, s, R2) for each model are displayed in Table 4. This analysis returned a significant main effect of group (F(2, 60) = 3.22, p = 0.047, np2 = 0.097). Planned comparisons revealed significant differences between the GD and control sample, with the GD sample having a significantly steeper discounting curve than the control sample (Mean Δ = − 0.17, p = 0.015, 95% CI [− 0.30, − 0.04]).

Discounting models are organized by study group. Points on the figure represent median indifference points with lines indicating the best fitting discounting function (Myerson & Green, 1995). The inset figure represents the same data. The X-axis has been scaled to better represent the median indifference points at the shorter delays (i.e. 1 week, 2 weeks, 1 month, and 6 months)
Discussion
The first objective of this study was to provide further evidence characterizing GD’s executive functioning profile. The results offer mixed support for the hypotheses posed related to this aim. In alignment with the hypotheses, performances observed with our GD sample reflecting cognitive control and capacity to delay gratification were impulsive compared to those observed with the community control sample. In contrast, motor response inhibition, planning, visuospatial working memory, and propensity for risky behaviours were statistically similar between the GD and control samples. This overall pattern of results suggests that while patterns of impulsivity can characterize the executive functioning profile of GD, these impairments impact specific domains of executive functioning and are not broadly observed.
In comparison to the control sample, the GD sample was characterized by a reduced capacity to delay gratification. This performance pattern has been observed in previous studies revealing similarly elevated tendencies of choice impulsivity in GD samples compared to controls (Albein-Urios et al., 2014; Amlung et al., 2017; Dixon et al., 2003; Ioannidis et al., 2019; Petry, 2001). It has been hypothesized that GD is associated with a hypoactive reward system, biasing reward representation and valuation and, as a result, biasing motivations leading to dysfunctional behaviours (Brevers et al., 2012a, 2012b; Lorains et al., 2014; Madden & Bickel, 2010). In other words, individuals diagnosed with GD appear to pay greater attention to potential gains as opposed to potential losses during tasks tapping decision-making processes. This attentional or motivational bias has been proposed to explain this consistently observed performance pattern, reflecting impulsive choice, associated with delay discounting tasks (Ioannidis et al., 2019; O’Connor et al., 2014).
Response inhibition impairments are a relatively well-established observation associated with GD samples (Brevers & Noël, 2013; Chowdhury et al., 2017; Goudriaan et al., 2005, 2006; Smith et al., 2014). However, this effect has not consistently been replicated, with some researchers suggesting that motor response inhibition is not a central expression of GD impulsivity (Brevers et al., 2012a, 2012b; Leppink et al., 2016; Sharif-Razi et al., 2019). In support of this latter conclusion, and inconsistent with our hypotheses, this study failed to replicate previous findings suggesting individuals with GD demonstrate impaired proactive or reactive response inhibition.
In contrast, compared to the community controls, impairments were observed in the ability to inhibit highly automatic behaviours such as reading, specifically the capacity to inhibit the more salient and automatic behaviour of reading a word instead of naming the dissonant ink colours. Models of impulsivity suggest that this performance pattern reflects an impulsive cognitive bias, in which individuals are less able to inhibit attentional shifting towards task-irrelevant stimuli or highly automatic behaviours. Notably, the GD and control samples were shown to have comparable error rates across all conditions, testing various inhibitory processes on the CWIT. This suggests that impairment reflects the speed at which the inhibitory process is elicited, not explicitly a lack of capacity to inhibit overlearned responses which would manifest as elevated error rates. Therefore, the pattern of results observed here suggests that while individuals with GD can inhibit and shift their attention away from task-irrelevant responses, the speed at which this process is elicited, specifically for overlearned and highly automatic behaviours, is slower than that observed within the non-GD population.
Finally, this study failed to provide evidence supporting the existence of impulsive planning, working memory, or a propensity for risk-taking behaviours within the analyzed GD sample. This suggests that these domains of cognition are preserved within the GD cognitive profile. These results align with literature which has supported the normal functioning of verbal and spatial working memory (Albein-Urios et al., 2012; Brevers et al., 2012a, 2012b; Ledgerwood et al., 2012; Manning et al., 2013; Yan et al., 2014) and planning (Manning et al., 2013) within GD samples. On the other hand, these results contradict other efforts at characterizing executive functioning within the GD population (Kertzman et al., 2017; Ledgerwood et al., 2012; Mallorquí-Bagué et al., 2018; Zhou et al., 2016), including the recent meta-analysis that supported broad impulsivity-characterized executive functioning impairment within GD (Ioannidis et al., 2019). Our failure to detect between-group differences regarding the noted cognitive domains may reflect cognitive profile heterogeneity within the GD population. Alternatively, cognitive task variance regarding psychometrics and specificity may impact the observation of performance differences and explain our lack of between-group findings. Replicating such findings will be necessary to clarify.
The second aim of this study was to assess whether executive functioning deficits observed within the GD sample were similarly observed with the biological relative sample, providing evidence of potential vulnerability markers of GD. The impairment that reflected impulsive attentional bias was the only domain in which similar performance patterns were observed in the relative and GD samples. This offers preliminary evidence supporting the specific inhibitory processes underlying attentional biases as a possible vulnerability marker in non-diagnosed first-degree relatives of individuals with GD. Additionally, while not significant, the overall pattern of performance on the DDT, reflecting choice impulsivity, suggested individuals with GD perform significantly more impulsively compared to controls, with the relative sample demonstrating an intermediary performance. Studies to date assessing cognitive performance patterns within familial relatives of individuals with GD have been mixed but have generally suggested that impulsivity and impaired reward-based decision-making represent candidate markers of GD vulnerability (Black et al., 2014, 2015a, 2015b; Limbrick-Oldfield et al., 2020). Although the results of this study regarding the relative sample should be reviewed cautiously, given the small sample size, they do support impulsive cognitive biases as a potential vulnerability marker in need of further assessment and replication.
Several explanations for the pattern of results observed are worth discussing. First, the contradiction between the results observed from the CWIT and the SSAT suggests that inhibitory processes may be impaired in both individuals with GD and their first-degree biological relatives but that this impairment may not be generalized and may be moderated by task-specific factors. For example, inter-task demand variation between inhibition paradigms may impact the specific inhibition process being tapped, resulting in variation in the observed results. The CWIT largely indexes verbal inhibition, while the SSAT reflects a motor inhibitory process, potentially explaining the difference in observed results. Alternatively, the subjective evaluation of the inhibited response may interact with performance, biased by underlying motivational dysfunctions and symptom severity. This explanation has been supported by evidence suggesting motor impulsivity is more consistently disrupted in severe cases of GD (Chowdhury et al., 2017; Michalczuk et al., 2011). Additionally, other studies have demonstrated that behavioural impulsivity, in the form of an increased propensity for risky behaviours, may be moderated by previous experiences. Specifically, a study by Bonini et al. (2018) reported no differences between a control, pathological, and problematic gambling sample regarding risk-taking behaviours measured by the BART. Of note, some differences did emerge within the problematic gambling group following a predetermined series of losses, interpreted as reduced sensitivity to negative feedback and a loss-chasing tendency. These results highlight the importance of considering task-specific characteristics in observing impulsivity-characterized executive function impairment.
It has also been suggested that GD is best characterized by distinct subtypes, differentiated by course of illness (e.g. age, age of onset), symptomology (e.g. severity, comorbidity), and personality (e.g. harm avoidance, self-directedness, impulsive personality traits), which are predictive of neurocognitive functioning (Heiskanen & Toikka, 2016; Jiménez-Murcia et al., 2017; Mallorquí-Bagué et al., 2018; Moon et al., 2017, p. 201; Nower et al., 2022; Suomi et al., 2014). For example, one GD cluster has been proposed, which presents more significant executive functioning impairment in addition to higher rates of unemployment, later age of GD onset, greater endorsed negative/positive urgency, and broadly elevated comorbid psychological symptoms (Mallorquí-Bagué et al., 2018). Considering this, the results reviewed here should be interpreted with caution as, due to our modest sample size, we were unable to analyze within sample subsets. Greater than half (55%) of our GD sample met the criteria for lifetime substance-use disorder, while only 2 (5%) met the criteria for adult attention deficit hyperactivity disorder (ADHD). This is relevant as previous research has supported the importance of comorbid substance use disorder in attenuating impulsive behaviours, potentially due to the neurotoxic effects of alcohol and drugs (Chowdhury et al., 2017; Lawrence et al., 2009; Potenza, 2006). On the other hand, ADHD is consistently associated with poorer inhibition performance and greater impulsivity (Brunault et al., 2020; Lijffijt et al., 2005; Senderecka et al., 2012; Verbruggen & Logan, 2008). This highlights the need for additional studies analyzing the potential clustering of individuals with GD based on salient factors such as symptom severity and comorbidity, which may elucidate the mixed results to date.
Finally, a hypothesis has been proposed which suggests that cognitive deficits may be driven by an underlying motivational mechanism. In a study by Boog et al. (2014), mental flexibility performance was compared between a GD and a control sample. Uniquely, this study compared the capacity for mental flexibility when the rules were arbitrary versus rules that were previously reinforced with rewards. Between-group differences were non-significant when the rules were arbitrary but were significant when the rules were reward-based. This result was interpreted as evidence of a motivational impairment rather than a more generalized mental flexibility impairment. It has been hypothesized that these reward-motivation biases may explain inconsistencies within the GD neurocognitive literature (Stevens et al., 2015). While the impact of a motivational bias was not directly assessed within this study, it may offer a further explanation for the discrepancies observed and warrants further investigation.
Limitations
Several limitations of this study are acknowledged. The GD sample was recruited based on the presence or absence of GD. The presence of other psychological disorders, though assessed, did not act as an exclusion criterion. While this increases the generalizability of these observed results, it also introduces the confounding influence of comorbidity. Additionally, while the sample sizes of the GD and control samples were adequate, the relative sample was modest due to recruitment difficulties. Effect sizes are reported to reduce the impact of this issue. Future studies may wish to assess variance in neuropsychological impairment manifestation as a factor of symptom variation (i.e. remission vs. worsening). With limitations noted, several strengths are also worth mentioning. Including a first-degree biological relative sample allowed for assessing executive functioning vulnerability markers of GD. Additionally, while differing on some characteristics (see Table 1), our samples were largely well-matched regarding demographics, except for fewer female participants within the gambling sample. Finally, this study applied a comprehensive neuropsychological assessment tapping many executive functioning domains critical to the cognitive profile of GD. This allowed for a thorough assessment of the manifestation of cognitive impairments.
Conclusions
The results of this study provide evidence of impulsive choice (i.e. a reduced capacity to delay gratification) and impulsive cognitive biases (i.e. reduced capacity for inhibiting overlearned verbal behaviours) within a sample of GD. These results contribute to the growing literature characterizing the cognitive profile of GD as impulsive while highlighting areas of interest for future studies. Specifically, the importance of the unique contributions of disorder onset, task demands, and comorbidity was reviewed and emphasized as essential areas for future research. Additionally, while preliminary and in need of replication, this study provided evidence of the characterization of impulsive cognitive biases as a potential familial vulnerability marker for GD development, as similar performance patterns were observed within the analyzed first-degree relative sample. Further research is needed to directly explore the manifestation of impulsivity as a function of task modality while considering the possible utility of symptom, cognition, and demographic-based cluster analyses.
References
Aben, I., Verhey, F., Lousberg, R., Lodder, J., & Honig, A. (2002). Validity of the Beck Depression Inventory, Hospital Anxiety and Depression Scale, SCL-90, and Hamilton Depression Rating Scale as screening instruments for depression in stroke patients. Psychosomatics, 43(5), 386–393. https://doi.org/10.1176/appi.psy.43.5.386
Albein-Urios, N., Martinez-González, J. M., Lozano, Ó., Clark, L., & Verdejo-García, A. (2012). Comparison of impulsivity and working memory in cocaine addiction and pathological gambling: Implications for cocaine-induced neurotoxicity. Drug and Alcohol Dependence, 126(1–2), 1–6. https://doi.org/10.1016/j.drugalcdep.2012.03.008
Albein-Urios, N., Martinez-González, J. M., Lozano, Ó., & Verdejo-Garcia, A. (2014). Monetary delay discounting in gambling and cocaine dependence with personality comorbidities. Addictive Behaviors, 39(11), 1658–1662. https://doi.org/10.1016/j.addbeh.2014.06.001
Almeida, R., Barbosa, J., & Compte, A. (2015). Neural circuit basis of visuo-spatial working memory precision: A computational and behavioral study. Journal of Neurophysiology, 114(3), 1806–1818. https://doi.org/10.1152/jn.00362.2015
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
Amlung, M., Vedelago, L., Acker, J., Balodis, I., & MacKillop, J. (2017). Steep delay discounting and addictive behavior: A meta-analysis of continuous associations. Addiction, 112(1), 51–62. https://doi.org/10.1111/add.13535
Bailey, A. J., Romeu, R. J., & Finn, P. R. (2021). The problems with delay discounting: A critical review of current practices and clinical applications. Psychological Medicine, 51(11), 1799–1806. https://doi.org/10.1017/S0033291721002282
Black, D. W., Coryell, W. H., Crowe, R. R., Shaw, M., McCormick, B., & Allen, J. (2014). Personality disorders, impulsiveness, and novelty seeking in persons with DSM-IV pathological gambling and their first-degree relatives. Journal of Gambling Studies, 31(4), 1201–1214. https://doi.org/10.1007/s10899-014-9505-y
Black, D. W., Coryell, W., Crowe, R., Shaw, M., McCormick, B., & Allen, J. (2015). The relationship of DSM-IV pathological gambling to compulsive buying and other possible spectrum disorders: Results from the Iowa PG family study. Psychiatry Research, 226(1), 273–276. https://doi.org/10.1016/j.psychres.2014.12.061
Black, D. W., Coryell, W. H., Crowe, R. R., Shaw, M., McCormick, B., & Allen, J. (2015). Personality disorders, impulsiveness, and novelty seeking in persons with DSM-IV pathological gambling and their first-degree relatives. Journal of Gambling Studies, 31(4), 1201–1214. https://doi.org/10.1007/s10899-014-9505-y
Bonini, N., Grecucci, A., Nicolè, M., & Savadori, L. (2018). Reduced risk-taking after prior losses in pathological gamblers under treatment and healthy control group but not in problem gamblers. Journal of Gambling Studies, 34(2), 429–447. https://doi.org/10.1007/s10899-017-9709-z
Boog, M., Höppener, P., Ben, B. J. M., Goudriaan, A. E., Boog, M. C., & Franken, I. H. A. (2014). Cognitive inflexibility in gamblers is primarily present in reward-related decision making. Frontiers in Human Neuroscience, 8(AUG), 1–6. https://doi.org/10.3389/fnhum.2014.00569
Brevers, D., & Noël, X. (2013). Pathological gambling and the loss of willpower: A neurocognitive perspective. Socioaffective Neuroscience & Psychology, 3(1), 21592. https://doi.org/10.3402/snp.v3i0.21592
Brevers, D., Cleeremans, A., Goudriaan, A. E., Bechara, A., Kornreich, C., Verbanck, P., & Noël, X. (2012). Decision making under ambiguity but not under risk is related to problem gambling severity. Psychiatry Research, 200(2–3), 568–574. https://doi.org/10.1016/j.psychres.2012.03.053
Brevers, D., Cleeremans, A., Verbruggen, F., Bechara, A., Kornreich, C., Verbanck, P., & Noël, X. (2012). Impulsive action but not impulsive choice determines problem gambling severity. PLoS ONE, 7(11), 5–12. https://doi.org/10.1371/journal.pone.0050647
Brunault, P., Mathieu, S., Faussat, C., Barrault, S., & Varescon, I. (2020). Impulsivity facets and cognitive distortions associated with problem gambling: Differences between ADHD and non-ADHD gamblers. European Review of Applied Psychology, 70(4), 100559. https://doi.org/10.1016/j.erap.2020.100559
Chowdhury, N. S., Livesey, E. J., Blaszczynski, A., & Harris, J. A. (2017). Pathological gambling and motor impulsivity: A systematic review with meta-analysis. Journal of Gambling Studies, 33(4), 1213–1239. https://doi.org/10.1007/s10899-017-9683-5
Ciccarelli, M., Griffiths, M. D., Nigro, G., & Cosenza, M. (2017). Decision making, cognitive distortions and emotional distress: A comparison between pathological gamblers and healthy controls. Journal of Behavior Therapy and Experimental Psychiatry, 54(September), 204–210. https://doi.org/10.1016/j.jbtep.2016.08.012
Clark, S. V., King, T. Z., & Turner, J. A. (2020). Cerebellar contributions to proactive and reactive control in the stop signal task: A systematic review and meta-analysis of functional magnetic resonance imaging studies. Neuropsychology Review, 30(3), 362–385. https://doi.org/10.1007/s11065-020-09432-w
Currie, S. R., Hodgins, D. C., & Casey, D. M. (2013). Validity of the problem gambling severity index interpretive categories. Journal of Gambling Studies, 29(2), 311–327. https://doi.org/10.1007/s10899-012-9300-6
Debelak, R., Egle, J., Köstering, L., & Kaller, C. P. (2016). Assessment of planning ability: Psychometric analyses on the unidimensionality and construct validity of the Tower of London Task (TOL-F). Neuropsychology, 30(3), 346–360. https://doi.org/10.1037/neu0000238
Delis, D. C., Kramer, J. H., Kaplan, E., & Holdnack, J. (2004). Reliability and validity of the Delis-Kaplan Executive Function System: An update. Journal of the International Neuropsychological Society, 10(2), 301–303. https://doi.org/10.1017/S1355617704102191
Dixon, M. R., Marley, J., & Jacobs, E. A. (2003). Delay discounting by pathological gamblers. Journal of Applied Behavior Analysis, 36(4), 449–458. https://doi.org/10.1901/jaba.2003.36-449
Ellis, J. D., Carr, M. M., & Ledgerwood, D. M. (2018). Executive function in problem gamblers with and without history of depression. International Journal of Mental Health and Addiction, 16(5), 1085–1094. https://doi.org/10.1007/s11469-017-9804-5
Ersche, K. D., Turton, A. J., Pradhan, S., Bullmore, E. T., & Robbins, T. W. (2010). Drug addiction endophenotypes: Impulsive versus sensation-seeking personality traits. Biological Psychiatry, 68(8), 770–773. https://doi.org/10.1016/j.biopsych.2010.06.015
Evenden, J. L. (1999). Varieties of impulsivity. Psychopharmacology, 146(4), 348–361. https://doi.org/10.1007/PL00005481
Fauth-Bühler, M., Mann, K., & Potenza, M. N. (2017). Pathological gambling: A review of the neurobiological evidence relevant for its classification as an addictive disorder. Addiction Biology, 22(4), 885–897. https://doi.org/10.1111/adb.12378
First, M., Williams, J., Karg, R., & Spitzer, R. (2016). Structured Clinical Interview for DSM-5 Disorders, Clinician Version (SCID-5-CV). In American Psychiatric Association. https://doi.org/10.1002/9781118625392.wbecp351
Glahn, D. C., Kim, J., Cohen, M. S., Poutanen, V.-P., Therman, S., Bava, S., Van Erp, T. G. M., Manninen, M., Huttunen, M., & Lönnqvist, J. (2002). Maintenance and manipulation in spatial working memory: Dissociations in the prefrontal cortex. NeuroImage, 17(1), 201–213. https://doi.org/10.1006/nimg.2002.1161
Gottesman, I. I., & Gould, T. D. (2003). The Endophenotype Concept in Psychiatry: Etymology and Strategic Intentions. American Journal of Psychiatry, 160(April), 636–645. https://doi.org/10.1176/appi.ajp.160.4.636
Goudriaan, A. E., Oosterlaan, J., De Beurs, E., & Van Den Brink, W. (2005). Decision making in pathological gambling: A comparison between pathological gamblers, alcohol dependents, persons with Tourette syndrome, and normal controls. Cognitive Brain Research, 23(1), 137–151. https://doi.org/10.1016/j.cogbrainres.2005.01.017
Goudriaan, A. E., Oosterlaan, J., De Beurs, E., & Van Den Brink, W. (2006). Neurocognitive functions in pathological gambling: A comparison with alcohol dependence, Tourette syndrome and normal controls. Addiction, 101(4), 534–547. https://doi.org/10.1111/j.1360-0443.2006.01380.x
Grant, J. E., Schreiber, L., Odlaug, B. L., & Kim, S. W. (2010). Pathologic gambling and bankruptcy. Comprehensive Psychiatry, 51(2), 115–120. https://doi.org/10.1016/j.comppsych.2009.04.002
Green, R. E. A., Melo, B., Christensen, B., Ngo, L.-A., Monette, G., & Bradbury, C. (2008). Measuring premorbid IQ in traumatic brain injury: An examination of the validity of the Wechsler Test of Adult Reading (WTAR). Journal of Clinical and Experimental Neuropsychology, 30(2), 163–172. https://doi.org/10.1080/13803390701300524
Hamilton, M. (1960). A rating scale for depression. Journal of Neurology, Neurosurgery & Psychiatry, 23(1), 56–62. https://doi.org/10.1136/jnnp.23.1.56
Heiskanen, M., & Toikka, A. (2016). Clustering Finnish gambler profiles based on the money and time consumed in gambling activities. Journal of Gambling Studies, 32(2), 363–377. https://doi.org/10.1007/s10899-015-9556-8
Hodgins, D. C., Stea, J. N., & Grant, J. E. (2011). Gambling disorders. The Lancet, 378(9806), 1874–1884. https://doi.org/10.1016/S0140-6736(10)62185-X
Holtgraves, T. (2009). Evaluating the problem gambling severity index. Journal of Gambling Studies, 25(1), 105–120. https://doi.org/10.1007/s10899-008-9107-7
Hur, J. W., Shin, N. Y., Kim, S. N., Hwanjang, J., Choi, J. S., Shin, Y. C., & Kwon, J. S. (2012). Do pathological gambling and obsessive-compulsive disorder overlap? A neurocognitive perspective. CNS Spectrums, 17(4), 207–213. https://doi.org/10.1017/S1092852912000545
Ibáñez, A., Blanco, C., Perez de Castro, I., Fernandez-Piqueras, J., & Sáiz-Ruiz, J. (2003). Genetics of pathological gambling. Journal of Gambling Studies, 19, 11–22.
IBM Corp. (2019). IBM SPSS Statistics for Windows, Version 26.0. Armonk, NY: IBM Corp.
Ioannidis, K., Hook, R., Wickham, K., Grant, J. E., & Chamberlain, S. R. (2019). Impulsivity in gambling disorder and problem gambling: A meta-analysis. Neuropsychopharmacology, 44(8), 1354–1361. https://doi.org/10.1038/s41386-019-0393-9
Jiménez-Murcia, S., Fernández-Aranda, F., Mestre-Bach, G., Granero, R., Tárrega, S., Torrubia, R., Aymamí, N., Gómez-Peña, M., Soriano-Mas, C., Steward, T., Moragas, L., Baño, M., del Pino-Gutiérrez, A., & Menchón, J. M. (2017). Exploring the relationship between reward and punishment sensitivity and gambling disorder in a clinical sample: A path modeling analysis. Journal of Gambling Studies, 33(2), 579–597. https://doi.org/10.1007/s10899-016-9631-9
Johnson, M. W., & Bickel, W. K. (2008). An algorithm for identifying nonsystematic delay-discounting data. Experimental and Clinical Psychopharmacology, 16(3), 264–274. https://doi.org/10.1037/1064-1297.16.3.264
Kertzman, S., Vainder, M., Aizer, A., Kotler, M., & Dannon, P. N. (2017). Pathological gambling and impulsivity: Comparison of the different measures in the behavior inhibition tasks. Personality and Individual Differences, 107, 212–218. https://doi.org/10.1016/j.paid.2016.11.042
Kessler, R. C., Hwang, I., Labrie, R., Petukhova, M., Sampson, N. A., Winters, K. C., & Shaffer, H. J. (2008). The prevalence and correlates of DSM-IV Pathological Gambling in the National Comorbidity Survey Replication. Psychological Medicine, 38(9), 1351–1360. https://doi.org/10.1017/S0033291708002900.The
Köstering, L., Schmidt, C. S. M., Egger, K., Amtage, F., Peter, J., Klöppel, S., Beume, L.-A., Hoeren, M., Weiller, C., & Kaller, C. P. (2015). Assessment of planning performance in clinical samples: Reliability and validity of the Tower of London task (TOL-F). Neuropsychologia, 75, 646–655. https://doi.org/10.1016/j.neuropsychologia.2015.07.017
Kourgiantakis, T., Saint-Jacques, M. C., & Tremblay, J. (2013). Problem gambling and families: A systematic review. Journal of Social Work Practice in the Addictions, 13(4), 353–372. https://doi.org/10.1080/1533256X.2013.838130
Kräplin, A., Bühringer, G., Oosterlaan, J., van den Brink, W., Goschke, T., & Goudriaan, A. E. (2014). Dimensions and disorder specificity of impulsivity in pathological gambling. Addictive Behaviors, 39(11), 1646–1651. https://doi.org/10.1016/j.addbeh.2014.05.021
Lawrence, A. J., Luty, J., Bogdan, N. A., Sahakian, B. J., & Clark, L. (2009). Problem gamblers share deficits in impulsive decision-making with alcohol-dependent individuals. Addiction, 104(6), 1006–1015. https://doi.org/10.1111/j.1360-0443.2009.02533.x
Ledgerwood, D. M., Orr, E. S., Kaploun, K. A., Milosevic, A., Frisch, G. R., Rupcich, N., & Lundahl, L. H. (2012). Executive function in pathological gamblers and healthy controls. Journal of Gambling Studies, 28(1), 89–103. https://doi.org/10.1007/s10899-010-9237-6
Leiserson, V., & Pihl, R. O. (2007). Reward-sensitivity, inhibition of reward-seeking, and dorsolateral prefrontal working memory function in problem gamblers not in treatment. Journal of Gambling Studies, 23(4), 435–455. https://doi.org/10.1007/s10899-007-9065-5
Lejuez, C. W., Richards, J. B., Read, J. P., Kahler, C. W., Ramsey, S. E., Stuart, G. L., Strong, D. R., & Brown, R. A. (2002). Evaluation of a behavioral measure of risk taking: The balloon analogue risk task (BART). Journal of Experimental Psychology: Applied, 8(2), 75–84. https://doi.org/10.1037/1076-898X.8.2.75
Lejuez, C. W., Aklin, W., Daughters, S., Zvolensky, M., Kahler, C., & Gwadz, M. (2007). Reliability and validity of the youth version of the Balloon Analogue Risk Task (BART–Y) in the assessment of risk-taking behavior among inner-city adolescents. Journal of Clinical Child & Adolescent Psychology, 36(1), 106–111. https://doi.org/10.1080/15374410709336573
Leppink, E. W., Redden, S. A., & Grant, J. E. (2016). Impulsivity and gambling: A complex clinical association across three measures. American Journal on Addictions, 25(2), 138–144. https://doi.org/10.1111/ajad.12341
Lijffijt, M., Kenemans, J. L., Verbaten, M. N., & van Engeland, H. (2005). A meta-analytic review of stopping performance in attention-deficit/hyperactivity disorder: Deficient inhibitory motor control? Journal of Abnormal Psychology, 114(2), 216–222. https://doi.org/10.1037/0021-843X.114.2.216
Limbrick-Oldfield, E. H., Mick, I., Cocks, R. E., Flechais, R. S. A., Turton, S., Lingford-Hughes, A., Bowden-Jones, H., & Clark, L. (2020). Neural and neurocognitive markers of vulnerability to gambling disorder: A study of unaffected siblings. Neuropsychopharmacology, 45(2), 292–300. https://doi.org/10.1038/s41386-019-0534-1
Lobo, D. S. S. (2016). Genetic aspects of gambling disorders: Recent developments and future directions. Current Behavioral Neuroscience Reports, 3(1), 58–66. https://doi.org/10.1007/s40473-016-0064-7
Lorains, F. K., Cowlishaw, S., & Thomas, S. A. (2011). Prevalence of comorbid disorders in problem and pathological gambling: Systematic review and meta-analysis of population surveys: Comorbid disorders in pathological gambling. Addiction, 106(3), 490–498. https://doi.org/10.1111/j.1360-0443.2010.03300.x
Lorains, F. K., Dowling, N. A., Enticott, P. G., Bradshaw, J. L., Trueblood, J. S., & Stout, J. C. (2014). Strategic and non-strategic problem gamblers differ on decision-making under risk and ambiguity. Addiction, 109(7), 1128–1137. https://doi.org/10.1111/add.12494
MacKillop, J., Weafer, J., Gray, J. C., Oshri, A., Palmer, A., & de Wit, H. (2016). The latent structure of impulsivity: Impulsive choice, impulsive action, and impulsive personality traits. Psychopharmacology, 233(18), 3361–3370. https://doi.org/10.1007/s00213-016-4372-0
Madden, G. J., & Bickel, W. K. (2010). Impulsivity: The behavioral and neurological science of discounting. American Psychological Association, 12069. https://doi.org/10.1037/12069-000
Mallorquí-Bagué, N., Tolosa-Sola, I., Fernández-Aranda, F., Granero, R., Fagundo, A. B., Lozano-Madrid, M., Mestre-Bach, G., Gómez-Peña, M., Aymamí, N., Borrás-González, I., Sánchez-González, J., Baño, M., Del Pino-Gutiérrez, A., Menchón, J. M., & Jiménez-Murcia, S. (2018). Cognitive deficits in executive functions and decision-making impairments cluster gambling disorder sub-types. Journal of Gambling Studies, 34(1), 209–223. https://doi.org/10.1007/s10899-017-9724-0
Manning, V., Teoh, H. C., Guo, S., Wong, K. E., & Li, T. K. (2013). Executive functioning in Asian pathological gamblers. International Gambling Studies, 13(3), 403–416. https://doi.org/10.1080/14459795.2013.829516
May-Chahal, C., Humphreys, L., Clifton, A., Francis, B., & Reith, G. (2017). Gambling harm and crime careers. Journal of Gambling Studies, 33(1), 65–84. https://doi.org/10.1007/s10899-016-9612-z
Mazur, J. E. (1987). An adjusting procedure for studying delayed reinforcement. Quantitative Analyses of Behavior, 5, 55–73.
Mestre-Bach, G., Steward, T., Granero, R., Fernández-Aranda, F., Mena-Moreno, T., Vintró-Alcaraz, C., Lozano-Madrid, M., Menchón, J. M., Potenza, M. N., & Jiménez-Murcia, S. (2020). Dimensions of impulsivity in gambling disorder. Scientific Reports, 10(1), 1–11. https://doi.org/10.1038/s41598-019-57117-z
Michalczuk, R., Bowden-Jones, H., Verdejo-Garcia, A., & Clark, L. (2011). Impulsivity and cognitive distortions in pathological gamblers attending the UK National Problem Gambling Clinic: A preliminary report. Psychological Medicine, 41(12), 2625–2635. https://doi.org/10.1017/S003329171100095X
Moon, M., Lister, J. J., Milosevic, A., & Ledgerwood, D. M. (2017). Subtyping non-treatment-seeking problem gamblers using the pathways model. Journal of Gambling Studies, 33(3), 841–853. https://doi.org/10.1007/s10899-016-9658-y
Morosini, P. L., Magliano, L., Brambilla, L., Ugolini, S., & Pioli, R. (2000). Development, reliability and acceptability of a new version of the DSM- IV Social Occupational Functioning Assessment Scale (SOFAS) to assess routine social functioning. Acta Psychiatrica Scandinavica, 101(4), 323–329. https://doi.org/10.1034/j.1600-0447.2000.101004323.x
Myerson, J., & Green, L. (1995). Discounting of delayed rewards: Models of individual choice. Journal of the Experimental Analysis of Behavior, 64(3), 263–276. https://doi.org/10.1901/jeab.1995.64-263
Noël, X., Brevers, D., & Bechara, A. (2013). A neurocognitive approach to understanding the neurobiology of addiction. Current Opinion in Neurobiology, 23(4), 632–638. https://doi.org/10.1016/j.conb.2013.01.018
Nower, L., Blaszczynski, A., & Anthony, W. L. (2022). Clarifying gambling subtypes: The revised pathways model of problem gambling. Addiction, 117(7), 2000–2008. https://doi.org/10.1111/add.15745
O’Connor, D. A., Meade, B., Carter, O., Rossiter, S., & Hester, R. (2014). Behavioral sensitivity to reward is reduced for far objects. Psychological Science, 25(1), 271–277. https://doi.org/10.1177/0956797613503663
Pallanti, S., Marras, A., & Makris, N. (2021). A research domain criteria approach to gambling disorder and behavioral addictions: Decision-making, response inhibition, and the role of cannabidiol. Frontiers in Psychiatry, 12, 634418. https://doi.org/10.3389/fpsyt.2021.634418
Perandrés-Gómez, A., Navas, J. F., van Timmeren, T., & Perales, J. C. (2021). Decision-making (in)flexibility in gambling disorder. Addictive Behaviors, 112, 106534. https://doi.org/10.1016/j.addbeh.2020.106534
Petry, N. M. (2001). Pathological gamblers, with and without substance use disorders, discount delayed rewards at high rates. Journal of Abnormal Psychology, 110(3), 482–487. https://doi.org/10.1037/0021-843X.110.3.482
Petry, N. M., & Armentano, C. (1999). Prevalence, assessment, and treatment of pathological gambling: A review. Psychiatric Services, 50(8), 1021–1027.
Potenza, M. N. (2006). Should addictive disorders include non-substance-related conditions? Addiction, 101, 142–151. https://doi.org/10.1111/j.1360-0443.2006.01591.x
Reynolds, B., & Schiffbauer, R. (2004). Measuring state changes in human delay discounting: An experiential discounting task. Behavioural Processes, 67(3), 343–356. https://doi.org/10.1016/S0376-6357(04)00140-8
Richards, J. B., Zhang, L., Mitchell, S. H., & de Wit, H. (1999). Delay or probability discounting in a model of impulsive behavior: Effect of alcohol. Journal of the Experimental Analysis of Behavior, 71(2), 121–143. https://doi.org/10.1901/jeab.1999.71-121
Robbins, T. W., Gillan, C. M., Smith, D. G., de Wit, S., & Ersche, K. D. (2012). Neurocognitive endophenotypes of impulsivity and compulsivity: Towards dimensional psychiatry. Trends in Cognitive Sciences, 16(1), 81–91. https://doi.org/10.1016/j.tics.2011.11.009
Senderecka, M., Grabowska, A., Szewczyk, J., Gerc, K., & Chmylak, R. (2012). Response inhibition of children with ADHD in the stop-signal task: An event-related potential study. International Journal of Psychophysiology, 85(1), 93–105. https://doi.org/10.1016/j.ijpsycho.2011.05.007
Shallice, T. (1982). Specific impairments of planning. Philosophical Transactions of the Royal Society of London B, Biological Sciences, 298(1089), 199–209. https://doi.org/10.1098/rstb.1982.0082
Sharif-Razi, M., Hodgins, D. C., & Goghari, V. M. (2019). Reactive and proactive control mechanisms of response inhibition in gambling disorder. Psychiatry Research, 272(May 2018), 114–121. https://doi.org/10.1016/j.psychres.2018.12.049
Shaw, M. C., Forbush, K. T., Schlinder, J., Rosenman, E., & Black, D. W. (2007). The effect of pathological gambling on families, marriages, and children. CNS Spectrums, 12(8), 615–622. https://doi.org/10.1017/S1092852900021416
Shunk, A. W., Davis, A. S., & Dean, R. S. (2006). TEST REVIEW: Dean C. Delis, Edith Kaplan & Joel H. Kramer, Delis Kaplan Executive Function System (D-KEFS), The Psychological Corporation, San Antonio, TX, 2001. $415.00 (complete kit). Applied Neuropsychology, 13(4), 275–27. https://doi.org/10.1207/s15324826an1304_9
Slutske, W. S. (2000). Common genetic vulnerability for pathological gambling and alcohol dependence in men. Archives of General Psychiatry, 57(7), 666–673. https://doi.org/10.1001/archpsyc.57.7.666
Smith, J. L., Mattick, R. P., Jamadar, S. D., & Iredale, J. M. (2014). Deficits in behavioural inhibition in substance abuse and addiction: A meta-analysis. Drug and Alcohol Dependence, 145, 1–33. https://doi.org/10.1016/j.drugalcdep.2014.08.009
Stevens, T., Brevers, D., Chambers, C. D., Lavric, A., McLaren, I. P. L., Mertens, M., Noël, X., & Verbruggen, F. (2015). How does response inhibition influence decision making when gambling? Journal of Experimental Psychology: Applied, 21(1), 15–36. https://doi.org/10.1037/xap0000039
Suomi, A., Dowling, N. A., & Jackson, A. C. (2014). Problem gambling subtypes based on psychological distress, alcohol abuse and impulsivity. Addictive Behaviors, 39(12), 1741–1745. https://doi.org/10.1016/j.addbeh.2014.07.023
Tiego, J., Testa, R., Bellgrove, M. A., Pantelis, C., & Whittle, S. (2018). A hierarchical model of inhibitory control. Frontiers in Psychology, 9, 1339. https://doi.org/10.3389/fpsyg.2018.01339
Tiego, J., Oostermeijer, S., Prochazkova, L., Parkes, L., Dawson, A., Youssef, G., Oldenhof, E., Carter, A., Segrave, R. A., Fontenelle, L. F., & Yücel, M. (2019). Overlapping dimensional phenotypes of impulsivity and compulsivity explain co-occurrence of addictive and related behaviors. CNS Spectrums, 24(4), 426–440. https://doi.org/10.1017/S1092852918001244
Verbruggen, F., & Logan, G. D. (2008). Response inhibition in the stop-signal paradigm Successful stopping: Inhibition and performance monitoring. Trends in Cognitive Science, 12(11), 418–424. https://doi.org/10.1016/j.tics.2008.07.005
Weafer, J., Baggott, M. J., & de Wit, H. (2013). Test–retest reliability of behavioral measures of impulsive choice, impulsive action, and inattention. Experimental and Clinical Psychopharmacology, 21(6), 475–481. https://doi.org/10.1037/a0033659
World Medical Association. (2013). World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA, 310(20), 2191–4. https://doi.org/10.1001/jama.2013.281053
Wechsler, D. (2001). Wechsler Test of Adult Reading: WTAR. Psychological Corporation.
White, T. L., Lejuez, C. W., & de Wit, H. (2008). Test-retest characteristics of the Balloon Analogue Risk Task (BART). Experimental and Clinical Psychopharmacology, 16(6), 565–570. https://doi.org/10.1037/a0014083
Yan, W. S., Li, Y. H., Xiao, L., Zhu, N., Bechara, A., & Sui, N. (2014). Working memory and affective decision-making in addiction: A neurocognitive comparison between heroin addicts, pathological gamblers and healthy controls. Drug and Alcohol Dependence, 134(1), 194–200. https://doi.org/10.1016/j.drugalcdep.2013.09.027
Young, R. C., Biggs, J. T., Ziegler, V. E., & Meyer, D. A. (1978). A rating scale for mania: Reliability, validity and sensitivity. British Journal of Psychiatry, 133(11), 429–435. https://doi.org/10.1192/bjp.133.5.429
Yücel, M., Oldenhof, E., Ahmed, S. H., Belin, D., Billieux, J., Bowden-Jones, H., Carter, A., Chamberlain, S. R., Clark, L., Connor, J., Daglish, M., Dom, G., Dannon, P., Duka, T., Fernandez-Serrano, M. J., Field, M., Franken, I., Goldstein, R. Z., Gonzalez, R., & Verdejo-Garcia, A. (2019). A transdiagnostic dimensional approach towards a neuropsychological assessment for addiction: An international Delphi consensus study: Transdiagnostic neuropsychological approaches to addiction. Addiction, 114(6), 1095–1109. https://doi.org/10.1111/add.14424
Zandbelt, B. B., & Vink, M. (2010). On the role of the striatum in response inhibition. PloS one, 5(11), e13848. https://doi.org/10.1371/journal.pone.0013848
Zhou, Z., Zhou, H., & Zhu, H. (2016). Working memory, executive function and impulsivity in Internet-addictive disorders: A comparison with pathological gambling. Acta Neuropsychiatrica, 28(2), 92–100. https://doi.org/10.1017/neu.2015.54
Funding
This study was funded by the Gambling Family Study of Clinical and Cognitive Functioning (Alberta Gambling Research Institute Grant 68). Dr. Goghari was supported by a Canadian Institutes of Health Research New Investigator Award. The funding agencies had no role in the study design, interpretation, or manuscript preparation and submission.
Author information
Authors and Affiliations
Contributions
Each of the authors of this paper contributed to it in a significant way, whether that be through initial conceptualization, development of the methodology, the investigation, the formal analysis, or the writing/review/editing of the final draft.
Corresponding author
Ethics declarations
Ethics Approval and Consent to Participate
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its amendments or comparable ethical standards.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Aidelbaum, R., Hodgins, D.C. & Goghari, V.M. A Family Study of Executive Function in Gambling Disorder. Int J Ment Health Addiction 22, 1876–1899 (2024). https://doi.org/10.1007/s11469-022-00963-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11469-022-00963-2