
Abstract
The Problem Gambling Severity Index (PGSI) is a widely used nine item scale for measuring the severity of gambling problems in the general population. Of the four gambler types defined by the PGSI, non-problem, low-risk, moderate-risk and problem gamblers, only the latter category underwent any validity testing during the scale’s development, despite the fact that over 95% of gamblers fall into one of the remaining three categories. Using Canadian population data on over 25,000 gamblers, we conducted a comprehensive validity and reliability analysis of the four PGSI gambler types. The temporal stability of PGSI subtype over a 14-month interval was modest but adequate (intraclass correlation coefficient = 0.63). There was strong evidence for the validity of the non-problem and problem gambler categories however the low-risk and moderate-risk categories showed poor discriminant validity using the existing scoring rules. The validity of these categories was improved with a simple modification to the scoring system.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The Canadian Problem Gambling Index (CPGI) has become the standard in Canada for collecting population level data on gambling habits and problem gambling symptoms (Stinchfield et al. 2007). It is also used in Australia, Norway, Great Britain, and Iceland. The CPGI has two components: a section assessing gambling habits for all major games types, and a nine item scale assessing gambling problems. The latter forms a quantitative index called the Problem Gambling Severity Index (PGSI). Whereas the gambling habits section is often modified (e.g., variations in the questions on gambling expenditures are common) to meet the data needs of local jurisdictions, the PGSI is considered a standardized scale that should not be altered from the original wording and response choices. Most of the research on the CPGI has focused on the PGSI (Stinchfield et al. 2007).
The PGSI items were chosen from a larger pool of symptoms based on superior test–retest reliability, ability to discriminate recreational gamblers from problem gamblers, and contributing to high internal consistency of the total score (Ferris and Wynne 2001). Although PGSI scores correlate highly (r = 0.83) with DSM-based scales such as the National Opinion Research Center DSM Screen for Gambling Problems (NODS) (Ferris and Wynne 2001), the PGSI is not intended as an index of pathological gambling. Rather, the PGSI is considered a continuous scale of problem gambling severity. The response choices for each PGSI item are ‘never,’ ‘sometimes,’ ‘most of the time,’ or ‘almost always,’ with a total score ranging from 0 to 27. Cut-offs are used to assign gamblers to categories consisting of ‘non-problem gamblers’ (PGSI = 0), ‘low-risk’ (PGSI = 1–2), ‘moderate-risk’ (PGSI = 3–7), or ‘problem-gambler’ (PGSI > 7) (Ferris and Wynne 2001). These PGSI categories are purported to represent distinct types of gamblers within the continuum of problem gambling severity.
Criticism of the PGSI has emerged as researchers have become more familiar with the scale and its limitations. Reviews of the PGSI using both qualitative (McCready and Adlaf 2006) and quantitative (Orford et al. 2010) methods have revealed several notable weaknesses. Of the four PGSI gambler types, only the problem gambler category underwent any extensive validity testing. The names and cut-offs for the remaining categories (non-problem, low-risk, and moderate-risk gamblers) were established without validity testing. The scale developers argued that issues of sensitivity and specificity do not apply because these groups do not represent problem gambling (Ferris and Wynne 2001). Nonetheless, the PGSI is intended to be a continuous measure of problem gambling severity hence the non-problem, low-risk and moderate-risk gambler categories should represent a meaningful progression in level of risk for all gamblers who are below the threshold of problem gambling. The validity of these categories has never been evaluated despite the fact that over 95% of the gambling population falls in the range covered by these groups.
Because the prevalence of individuals who score eight or higher on the PGSI is typically very small (<2% in many studies) even in large survey samples, researchers often merge the moderate-risk and problem gamblers categories into a single category of problematic gambling to increase statistical power (Afifi et al. 2010; Crockford et al. 2008). Concerns of false positives have been raised when the lower cut-off of 3 is used to define problematic gambling (McCready and Adlaf 2006). False negatives may also be an issue with the PGSI. Measures of gambling intensity (e.g., frequency of gambling, monthly expenditure on gambling), although collected by the CPGI, are not used in the determination of problem gambling. Heavy gamblers may escape detection as problem gamblers if they endorse few PGSI symptoms. Another concern is the numerical scoring system of PGSI. The range of scores for each PGSI category varies considerably: non-problem (1-point range), low-risk (2-point range), moderate-risk (5-point), and problem gambling (19-point range), which could impact the temporal stability of the PGSI classifications. Finally, the total score although appearing to be a ratio scale has properties that are more consistent with an ordinal scale. Foremost, equivalency between scale points is not assumed. The significance of a score difference is much greater at the lower end of the scale (PGSI scores between 0 and 8) compared to the higher end (scores between 20 and 27).
Despite these concerns, many authors have concluded that the PGSI is psychometrically stronger than similar screening tools including the South Oaks Gambling Screen (SOGS), the Victorian Gambling Screen and DSM-IV based scales (McCready and Adlaf 2006; Mcmillen and Wenzel 2006; Orford et al. 2010). Orford et al. (2010) conducted the most rigorous psychometric evaluation of the PGSI to date. They compared the performance of the PGSI and a DSM-IV-based scale using data from the 2007 British Gambling Prevalence Survey. The DSM-IV scale employed a 4-point Likert scale similar to the PGSI. Focusing on the sample of 6,161 adult past-year gamblers, the investigators examined internal reliability, item response patterns, factor structure, and inter-scale agreement. The PGSI was found to have better internal reliability than the DSM-IV scale and fewer problems with differential item endorsement along gender, age, and socioeconomic divisions. The correlation between the PGSI and DSM scale was high, but the rate of agreement in identifying problem gamblers was only modest. There was even less agreement between the scales for the remaining gambler categories (non-problem, low-risk and moderate-risk).
There has been no analysis of the PGSI comparable to the work of Orford et al. with data from Canada where the instrument was developed. Moreover, the statistical approach of Orford and colleagues to assess the validity of the PGSI gambler types was largely descriptive. The DSM-IV based scale of pathological gambling was the only scale used to determine PGSI validity. Comparisons between DSM-IV scales and the PGSI are limited because the former assesses pathological gambling and the latter is intended as a broader measure of gambling problems. The DSM-IV items do not form a continuous scale although it is often used as a quantitative index of severity (Strong and Kahler 2007).
In the present study, we conducted a comprehensive assessment of the validity of the PGSI gambler types using the largest sample of CPGI population data compiled to date (over 25,000 cases). Multiple measures of external validity, including socioeconomic indicators, opinions of professionals familiar with the PGSI, concurrent mental health measures, indices of gambling intensity and game preferences were used to examine the distinctiveness of the four PGSI gambler types. The specific aims of the present study were to (1) assess the opinions of professionals involved in gambling research, treatment and policy on the current PGSI scoring system; (2) using Canadian population data assess the discriminant validity of the present PGSI severity classifications and cut-off scores for the non-problem gamblers, low-risk, moderate-risk and problem gamblers groups using cross-sectional and longitudinal population data, and; (3) assess the impact of re-calibrating the PGSI scoring rules on the reliability and external validity of PGSI severity categories.
Method
Data Sources
Survey of Professionals Involved in Gambling Research, Treatment, and Policy
A web-based survey on assessing problem gambling severity was completed by 142 professionals who were based in Canada (78%), United States (14%), and other countries (8%). Respondents were recruited from several sources: a mailing list used in a prior gambling survey (Currie et al. 2008b), lists of attendees at major gambling conferences in the past 5 years, researchers who received funding for gambling from provincial, Canadian and American granting agencies, and members of the Gambling Issues International Listserv. We attempted to recruit from three main professional groups: gambling researchers, clinicians who work with gamblers in treatment, and government and industry persons involved in the administration and oversight of gambling venues. An email invitation was sent to 422 individuals making the response rate 34%. For the present study we report on respondents’ overall opinions (items used a 5-point Likert scale: strongly disagree, disagree, neutral, agree and strongly agree) on the PGSI and its scoring system.
CPGI Integrated Dataset
The CPGI integrated dataset includes data from prevalence surveys conducted in Alberta, British Columbia, Ontario (two cycles 2001 and 2005), Manitoba, Newfoundland and the National CPGI validation study for a combined sample size of 14,833 past year gamblers. We have used this dataset in previous research (Currie et al. 2008c). Each survey employed a similar methodology. Namely, the data were collected via a computer-assisted telephone interviewing system. Samples were stratified by regional boundaries, age, and gender. Random digit dialing was used to select cases at the household level and the adult resident (≥18 years) with the most recent birthday was selected to be interviewed. The prevalence of problem gambling (PGSI ≥ 8) ranged from 0.4% in BC to 1.3% in AB. The CPGI integrated dataset was the study’s source of data for dollars spent on gambling in a typical month and percent of gross family income spent on gambling (range 0–100%). In previous research, percent of income spent on all gambling activities has shown a strong relationship with level of risk as measured by the PGSI (Currie et al. 2008c; Currie and Casey 2007) and related instruments like the SOGS (Weinstock et al. 2007).
Canadian Community Health Survey: Mental Health Well-being (CCHS-1.2)
Detailed descriptions of the CCHS-1.2 in terms of target population, sampling procedures, response rate and psychiatric assessment are in other sources (Currie et al. 2006; Statistics Canada 2002; Gravel and Beland 2005). Briefly, the CCHS-1.2 was a 2002 cross-sectional survey of a nationally representative sample of individuals aged 15 and older. Valid PGSI data for past year adult gamblers is available for 18,913 cases. The CCHS-1.2 remains the largest national sample of persons administered the CPGI. Gambling data used from the CCHS-1.2 included frequency of gambling (CPGI categories: daily; 2–6 times a week; once a week; 2–3 times a month; once a month; 6–11 times year; 1–5 times a year), number of game types played at least once in the last 12 months (to a maximum of 8), and types of games played. For the latter, we collapsed game type into two categories: (1) gaming machine or casino gamblers were persons who reported playing electronic gaming machines (EGMs; video lottery terminals and slot machines) or casino games in the past 12 months, and; (2) other gamblers consisting of individuals who reported types of gambling other than EGMs or casino games. Research has shown that EGM and casino gambling have a greater risk of harm and addiction compared to other forms of gambling (Breen and Zimmerman 2002; Welte et al. 2004). Moreover, the general public ranks EGMs and casino games as having the most potential for harm (Smith 2010). We have used this definition of game type in prior studies (Currie et al. 2006, 2008d; Miller and Currie 2008).
The CCHS-1.2 also provided data on 12-month prevalence of mood disorders (major depression, bipolar disorder, and dysthymia), anxiety disorders (panic disorder, obsessive–compulsive disorder, social anxiety, phobias), and substance use disorders (alcohol and drug). All disorders were based on a Canadian adaptation of the world mental health version of the Composite International Diagnostic Interview (WMH-CIDI). The CCHS-1.2 also assessed self-reported stress (1 = no stress to 5 = extreme stress), and psychological well-being (0–100 with higher values indicating better psychological well-being). The psychological well-being scale is a composite score based on the sum of participants’ responses to 25 items (Masse et al. 1998).
Leisure, Lifestyle, and Lifecycle Project (LLLP)
This longitudinal study is described in detail in other sources (el-Guebaly et al. 2008; Currie et al. 2012). Briefly, the LLLP is a prospective 5 year panel study of five age cohorts (13–65 years) of 1,808 adolescents and adults living in rural and urban Alberta. The data collected at each wave includes psychological, behavioural, medical, and social variables used to examine the etiology and natural progression of all levels of gambling. Random digit dialing (RDD) recruited participants from the general population. A second wave of RDD sampling was used to recruit ‘at-risk’ gamblers (n = 524) who were above the 70th percentile in gambling expenditure or gambling frequency. Sample weights were developed in consideration of: age-sex-geography variability, the number of individuals in the same age-sex grouping residing in the household, and oversampling of at-risk gamblers. The present study uses data on adults from times 1 (February 2006–October 2006) and 2 (November 2007–June 2008), with an interval of 14 months between assessments.
Table 1 compares the demographics of these three datasets. The LLLP data were limited to the assessment of PGSI temporal reliability and were not merged with the other datasets. Participants in this dataset have a different demographic and gambling profile than the other datasets due to oversampling of at-risk gamblers and the restriction of recruitment to a single province. Participants in the CPGI integrated and CCHS-1.2, datasets used in most analyses, were largely comparable in demographic and gambling profile. The CCHS-1.2 contained a higher proportion of males (χ2 = 10.43, p < .01), older adults (65+ years; χ2 = 233.64, p < .001), and individuals earning less than $30,000CAN annual income (χ2 = 283.24, p < .001). These differences, although significant because of the very large sample sizes, were not large in magnitude. There were no differences in education, proportion of EGM/casino players, or mean PGSI scores between the groups (all ps > .05).
Analyses
General Analytic Approach
Analyses of the PGSI data were restricted to individuals who (a) were 18 years and older; (b) reported gambling in the past year, and; (c) were administered all the PGSI items. The CPGI Integrated dataset and CCHS-1.2 were merged into one file for some analyses. Both the CPGI integrated datasets contain sampling weights, to adjust for age and gender biases. However, the methods used to weight cases were different hence it was not possible to utilize the sampling weights in analyses of the merged dataset. For some analyses, the use of the individual datasets was a better choice to ensure the results were clear and interpretable. The LLLP dataset was reserved for analyses involving longitudinal data. In consideration of the number of statistical tests performed we adopted more conservative criteria for significance (p < .01) to guard against Type I error.
Validity and Reliability of PGSI Gambler Types Derived from Original Scoring
We first tested the validity of the current PGSI scoring rules to determine if the four types of gamblers represent meaningfully distinct subpopulations of gamblers. We reasoned that the categories of non-problem, low-risk, moderate-risk, and problem gambler should demonstrate differences reflecting the gradient of risk assessed by the PGSI continuous score. Specifically, we compared the PGSI category groupings on the following key variables: (1) age, gender (proportion of males), marital status (single, married/common-law, widowed/divorced), and gross household income; (2) intensity of gambling involvement (frequency, total expenditures, percent of income spent on gambling, total number of different games played); (3) preference for EMG or casino games, and: (4) frequency of other addictive behaviours and mental health concerns. These particular measures were selected because prior research has shown each to be a well established or probable risk factor associated with pathological gambling, problem gambling or negative consequences from gambling (Currie et al. 2006, 2008a; Raylu and Oei 2002; el-Guebaly et al. 2006; Johansson et al. 2009).
Both the CPGI integrated and CCHS-1.2 datasets were used in this set of analyses. The merged data file was used to examine demographic variations across PGSI categories. The remaining analyses were conducted using the CPGI integrated or CCHS-1.2 datasets. The merged dataset could not be used in many analyses because of differences in the coding for key variables such as dollars spent on gambling, which was more precise in the CPGI integrated dataset (the CCHS-1.2 used broad categories to solicit amount spent on gambling), and frequency of playing different game types, which had large variations in the number response choices provided participants across the individual provincial surveys.
Each PGSI category was statistically compared with the other categories. For continuous variables, an ANOVA was conducted followed by Scheffe post hoc pairwise comparisons to identify the source of significance. Because the distributions for total monthly expenditures on gambling and percent of income spent on gambling were highly skewed, these variables were transformed using the natural log function. Statistical tests were conducted on the transformed data; however for ease of interpretation we report the untransformed means and medians in the tables. For categorical variables, the 99% confidence interval for the proportion estimate was calculated. Significant differences were identified by non-overlapping confidence intervals. In light of the large sample size and tendency for relatively small differences to be statistically significant, we also examined the magnitude of group mean and proportional differences.
The intraclass correlation coefficient (ICC), an index of the agreement of ratings, was used to assess the temporal stability of the original PGSI categories using the time 1 and 2 data from the LLLP. The type A ICC was used which assesses absolute agreement of categories rather than consistency. Interpretative guidelines for the ICC are: 0.6–0.7 indicates good agreement, 0.7–0.8 indicates strong agreement; and values >0.8 indicates near perfect agreement. Partial correlations were also computed to control for the influence of change in gambling behavior, specifically change in percentage of income spent on gambling between time 1 and 2, on PGSI total score. Finally, a reliable change index (RCI) was calculated (Jacobson et al. 1999) as a way of capturing the natural change in the PGSI total scores over time. Using the PGSI’s published test–retest reliability coefficient of 0.78, the reliable change index (Jacobson et al. 1999) provided a statistical method of determining if the observed change is beyond the limits of chance variation, given the reliability of the assessment instrument.
Validity and Reliability of PGSI Severity Categories Based on Revised Scoring Rules
Using the original 0–27 scoring range (each item scored on a 4-point scale), four novel categories were created that corresponded to scores of 0, 1–4, 5–7, and 8+). This scoring maintained the non-problem (zero-symptom) gambler and problem gamblers categories as unchanged from the original scoring, while having nearly equal intervals (3 and 4 points each) for the two middle categories. We hypothesized these revised categories would facilitate greater separation between the low-risk and moderate-risk groups. Although we originally sought to create categories that would have the same score range, the results from the analysis of the existing PGSI categories suggested the non-problem and problem gambler categories did not need revisions. Moreover, a change to the cut-off for the problem gambler subtype (9 instead of 8), would make comparisons with previous research using the old cut-off problematic. To assess the strength of the revised scoring, we repeated the validity and reliability analyses.
Results
Professionals’ Opinions on the PGSI
Three quarters of professionals who responded to our survey rated their knowledge of the PGSI as good to excellent. High proportions of respondents gave neutral responses to the opinion items on the PGSI and its scoring system. In response to the item, “The PGSI is an effective tool for identifying problem gamblers,” 59% of respondents strongly agreed or agreed. A high proportion (52%) also agreed that the PGSI is an effective tool to identify persons at risk for problem gambling. Only 21% believed false positives were a concern with the PGSI, but 38% were neutral on this issue. Similarly, 27% were neutral on whether false negatives are a concern on the PGSI while 31% agreed with this statement. In response to the item “The total score on the PGSI is a useful way of assessing severity of problem gambling,” 48% strongly agreed or agreed with this statement. Similarly, 48% agreed that the scoring categories for the PGSI are a useful way of classifying level of problem gambling risk. Nonetheless, 35% of responders felt the PGSI could be improved by revising the scoring system, although 38% were neutral on this item.
Validity and Reliability of PGSI Severity Categories Based on Original Scoring
Demographics
Table 2 compares the four PGSI groups on demographic variables. Using both the CCHS-1.2 and CPGI Integrated dataset (N = 25,584). No differences in age across the PGSI categories were detected at the p < .01 level. In terms of gender, the low-risk and moderate-risk group contained a significantly higher proportion of males compared to the non-problem group, but the difference between the low-risk and moderate-risk groups was not significant. As expected the proportion of males in the problem gambling group was significantly different from the proportion in the non-problem gambling group but not different from the remaining categories. The proportion of low income gamblers (<$30,000 per year) was significantly higher in the low-risk, moderate-risk, and problem gambling groups compared to the non problem group. The proportion in the problem gambling group was not significantly different from the low-risk and moderate-risk groups.
Gambling Intensity Measures
There were large and significant differences among the PGSI categories for total monthly expenditures on gambling and percent of gross household income spent on gambling. Results of the Scheffe test were significant for all pairwise comparisons. As shown in Table 3, both average expenditure on gambling and percent of income spent on gambling increase from the non-problem to the problem gambling groups. For adjacent categories, the percent of income spent on gambling was 2–2.5 times greater in the more severe PGSI grouping. A similar pattern was observed for total gambling expenditure.
In light of the large variability associated with the untransformed data (as evidenced by the large standard deviations), the median value is a better representation of the midpoints for each PGSI grouping. The actual difference in median percent of income among the non-problem, low-risk, and moderate-risk groups is relatively small. In contrast, there is a large increase in median percent of income between the moderate-risk and problem gambling group. The percentile ranks provide an indication of how the typical percent of income, monthly expenditures, and number of games played in the past year within each group compares to the full distribution of values in the population of Canadian gamblers. For example, the median monthly expenditure for non-problem gamblers, which represents about 85% of Canadian population, corresponds roughly to the 50th percentile for total expenditure and percent of income spent on gambling. The median proportion of income spent on gambling within the low-risk, moderate-risk, and problem gambling groups corresponded to percentiles 73th, 79th, and 96th, respectively in the general population.
For number of games played in the last year, the difference among the four PGSI gambler types was also highly significant. With this indicator, the source of variability was the difference between the non-problem group and the low-risk and moderate-risk types (p < .01 for Scheffe pairwise comparisons). There was little difference in number of games played in the last year among the low-risk, moderate-risk, and problem gambling groups.
Game Preferences
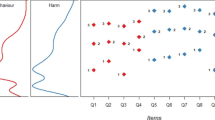
Figure 1 shows the proportion of gamblers in each PGSI subtype who play various game types at least 2–3 times per month. We examined differences among the PGSI types in high frequency game play (at least >2–3 times per month) to minimize group differences due to one-time game experimentation. Furthermore, 2–3 times per month is the low-risk gambling limit for frequency validated in previous research (Currie et al. 2008a, b). The results show large differences in high frequency playing of many game types across the four PGSI types. Non-problem gamblers are distinct from the other gambler types on all game types. For example, the proportion who played instant win tickets also increased substantially from 19% in the non-problem group to 41% in the low-risk group. Examining the differences using two categories of game type (EGMs and casino games versus other game types) provides a more succinct picture of the association between PGSI subtype and game preference (shown in right half of Fig. 1). Preference for EGMs or casino games was significantly lower among non-problem gamblers compared to the other three types (all ps < .01). The proportion of problem gamblers who play EGMs and casino games was significantly higher than moderate-risk gamblers (p < .01). There was no difference in game preference between low and moderate-risk gamblers for either EGMs/casino games or other game types.

Proportion of non-problem, low-risk, moderate-risk, and problem gamblers who play different game types 2–3 times per month or more
Mental Health Indicators
Table 3 shows the results of statistical comparisons of self-reported stress, and psychological well-being. The non-problem gambling group reported significantly less stress and greater well-being than the remaining PGSI groups. The low-risk group also reported less stress than the problem gambling group. Problem gamblers reported significantly lower psychological well-being compared to the other groups.
In terms of CIDI-diagnosed mental disorders, mood and anxiety disorders were more prevalent in the problem gambling group compared to the other PGSI groups. The differences in prevalence for these disorders among the non-problem, low-risk and moderate-risk gambling groups were not significant. Substance use disorders were significantly more common in the low-risk, moderate-risk and problem gambling groups compared to the non-problem gambling group. The prevalence of substance use disorders among the low-risk, moderate-risk and problem gambling groups was not significant.
Reliability of Current PGSI Gambler Types
The intraclass correlation coefficient for absolute agreement of PGSI subtype between time 1 and 2 in the LLLP sample was 0.63 (F = 4.51, p < .001). There were 239 gamblers (30%) who changed PGSI subtype from time 1–2. Among those gamblers that changed PGSI subtype, 21% shifted from low to moderate risk gamblers or vice versa. A partial correlation was also completed that allowed for the statistical control of any change in gambling involvement (i.e., percent of income spent on all gambling activities) between waves. Without controlling for the change in gambling involvement, the correlation between the PGSI score at time 1 and 2 was r = 0.64, p < .001, whereas when the change in gambling involvement was controlled, the correlation only dropped slightly to r = 0.62, p < .001.
The reliable change index was calculated for all participants with a non-zero PGSI score at time 1 or 2 (n = 303). This analysis revealed 62 individuals (8% of original 808) showing a reliable change in their PGSI score from time 1–2. This included 15 individuals (2%) who showed a significant decrease in PGSI and 47 individuals (6%) who showed a significant increase in PGSI score. The remaining individuals in the sample (92%, including 506 persons with a PGSI of zero at both time points) did not show a statistically significant change in their score.
Validity and Reliability of PGSI Gambler Types Using Revised Cut-offs
An emergent theme from the preceding analysis was the absence of many differences between the low-risk and moderate-risk groups. Our revised scoring proposal seeks to improve the distinctiveness of these groups. As shown in Table 4, the revised low-risk and moderate-risk categories are more distinct on measures of gambling intensity and game preference. The median proportion of income spent on gambling within the low-risk, moderate-risk, and problem gambling groups corresponded to the percentiles 74th, 88th, and 96th, respectively, in the general population of gamblers. The difference between these groups in preference for EMG or casino games is significant (14% for low-risk gamblers vs. 27% for moderate-risk gamblers). The revised categories had no appreciable impact on the mental health indicators.
Although the intraclass correlation coefficient for the revised categories did not increase (ICC = 0.63; F = 4.40, p < .001), the proportion of the sample that changed PGSI subtype between time 1 to time 2 decreased to 20% (n = 168). Furthermore, the proportion within this group who shifted from low to moderate risk gamblers or vice versa decreased to 11% from 21% using the original scoring. The partial correlations and RCI calculations were not repeated because the revised scoring changed the participant’s PGSI category not their score on the continuous scale.
Discussion
Among the four original PGSI types, the non-problem and problem gambler categories have the greatest validity as distinct subgroups of gamblers in the population. Non-problem gamblers were distinct from the low-risk, moderate-risk, and problem gambler types on most dimensions. For example, differences between non-problem gamblers and the remaining categories were statistically different for measures of gambling intensity and game preferences. Expenditures for gamblers in this category were at the 50th percentile for the population. Non-problem gamblers, according to current PGSI scoring rules, comprise about 85% of the Canadian population of past-year gamblers. Hence, this group represents the typical, normative gambler. This group contained the lowest proportion of males and highest proportion of married or common-law individuals. Non-problem gamblers reported greater mental health and had the lowest proportion of mood, anxiety, and substance use disorders compared to the other three groups.
The problem gambler category also appears to be a distinct group of gamblers on all dimensions. Differences between this category and the remaining PGSI types were statistically significant at the p = .01 level on nearly every dimension examined including demographics, game type preferences, indicators of gambling intensity and prevalence of other mental health concerns. Gambling expenditures for gamblers in this group exceed 96% of the general population of gamblers. Moreover, the differences between this category and closest adjacent category, moderate-risk gamblers, were large enough to be considered clinically meaningful on many key dimensions.
The most problematic PGSI categories are the low-risk and moderate-risk categories. Differences between these gambler types were not statistically significant for many dimensions. For example, these groups are demographically similar and play many game types at the same level of frequency. There was no difference in the proportion who play EGMs or casino games at least 2–3 times per week. There was no difference between these groups in measures of stress, well-being, or prevalence of mental health problems. The groups did show statistically significant differences in gambling expenditures. For example, the median proportion of income spent on gambling by moderate-risk gamblers is double the median amount spent by low-risk gamblers. However, the difference between these categories in terms of percentile rank within the population was relatively small: the spending habits of low-risk gamblers exceed 73% of the population while the spending habits of moderate-risk gamblers exceed 79% of the population.
The difference between moderate-risk and problem gamblers is very large on nearly all dimensions, most notably in gambling expenditures and preference for EGMs or casino games (21 vs. 47%). Our data suggest these are distinct types of gamblers and that the merging of these categories creates a very heterogeneous group with a wide range of risk. It would be inaccurate to label such a group problem gamblers or even moderate-risk gamblers given the similarity in profile between the latter group and gamblers labelled as low-risk.
The stability of the PGSI types over time was modest. The ICC on consistency in PGSI category resulted in good agreement between the time 1 and 2 assessments. In nominal terms, 70% of gamblers do not change PGSI group over an 14 month interval. Some change in PGSI score would be expected over such a long retest interval. The RCI, which accounts for change in score due to an instrument’s measurement error, revealed that only 8% of the sample showed a reliable change in total PGSI score over time.
We incorporated a survey of professionals who are familiar with the PGSI to provide an additional validity check by the instrument’s main users. We felt strongly any proposed changes to the instrument should not be driven by statistics alone. Given some of the criticism of the PGSI that has emerged in recent years, we were surprised the scale is still very well-regarded by researchers and clinicians in the field. The majority of professionals who participated in our survey felt the PGSI is useful in identifying both at risk and problem gamblers. About one-third of the sample felt the scoring system could be improved however a large proportion of respondents were neutral on this issue. It is possible that many users are unaware of any concerns with the scoring system.
It is inevitable that after an instrument is used many times in research and surveillance activities notions of improving the scoring or items will surface. The PGSI has undergone no revision since it was first introduced in 2001. There are many options for improving the instrument. Given the positive opinion on PGSI voiced by professionals familiar with scale, a major overhaul does not seem warranted. Nonetheless, it has been noted by some authors that the PSGI has a limited number of items and that existing items are overrepresented by symptoms associated with pathological gamblers (McCready and Adlaf 2006). New items could increase the range of scores for gamblers classified as low-risk or moderate-risk. Moreover, the Likert scale for each item has two response choices very similar in wording (‘most of the time’ and ‘almost always’). Australia has proposed five response choices for each item (Australian Government Productivity Commission 2010) although two choices are assigned the same score (never = 0, sometimes = 1, rarely = 1, often = 2, always = 3). The addition of new scored items that better reflect the mid-level degree of problem gambling risk, or a change the Likert scale for every item would represent a major overhaul of the measure. This would invalidate the previous cut-offs and necessitate the collection of a new normative sample.
Although a major revision to the PGSI may eventually be necessary, there are simpler ways to improve the instrument without requiring a new validation sample. The absence of meaningful differences between the low-risk and moderate-risk gambler types could be eliminated by simply merging these categories into a single PGSI subtype of ‘low-risk gamblers.’ The PGSI score could be used as a quantitative index of degree of risk that ranges from 1 to 7. However, the resulting category may be too inclusive of a wide range of gambling risk. A gambler with a PGSI score 1 is clearly distinguishable from a gambler with a score of 7. A more defendable option is to re-calibrate these categories. Our proposed re-scoring of the low-risk (1–4) to moderate-risk (5–7) cut-off did improve the distinctiveness of these categories on many dimensions. Most notably, the preference for high risk games was not significantly different between these groups with the original scoring but became significant using the revised scoring. The percentile ranks of gambling expenditures showed greater separation (74% for low-risk gamblers vs. 88% for moderate-risk gamblers). The revised categories showed greater stability over time. The overall proportion of the LLLP sample that changed PGSI subtype over time decreased to 20%, which is closer to the proportion of gamblers that showed a reliable change on the continuous PGSI score (8%). The change did not impact all the risk factors examined. For example, the proportion with mood, anxiety or substance use disorders was not affected. Additional research using the re-calibrated scoring rules is required to confirm the new categories represent an improvement in the subtyping of risk for gamblers with scores in the mid-range on the PGSI.
A limitation of any study using secondary data sources is that the role of non-measured variables cannot be determined. We acknowledge there are many other risk factors that could be used to delineate low-risk, moderate-risk, and problem gamblers. For example, antisocial behaviour and academic achievement were identified by Johansson et al. (2009) as probable risk factors for problem gambling. Although we examined the presence of alcohol and drug dependence, we were unable to assess the role of alcohol or drug use while gambling, or the role of non-dependent levels of alcohol and drug misuse because of limitations of the CCHS-1.2 data. Being mostly cross-sectional in nature, our study provides no evidence of the progression gambling problems over time. For example, we cannot conclude that gamblers who progress from moderate-risk to problem gamblers would experience an increase in mood and anxiety disorders. Our team used the LLLP data to show that an increase in gambling participation does result in an increase in problem gambling severity over time (Currie et al. 2012).
In conclusion, scale validation is an ongoing and iterative process. Although a major modification of the scale might also lead to enhanced validity, it appears that relatively minor changes in the scoring of categories are worthwhile to consider. Secondary analysis of existing data sets in countries other than Canada will be an important further step in establishing revised scoring cut-offs.
References
Afifi, T. O., Cox, B. J., Martens, P. J., Sareen, J., & Enns, M. W. (2010). The relation between types and frequency of gambling activities and problem gambling among women in Canada. The Canadian Journal of Psychiatry (La Revue canadienne de psychiatrie), 55, 21–28.
Australian Government Productivity Commission (2010). Gambling: Productivity Commission Report (Rep. No. Volume 2). Melbourne: Commonwealth of Australia Productivity Commission.
Breen, R., & Zimmerman, M. (2002). Rapid onset of pathological gambling in machine gamblers. Journal of Gambling Studies, 18, 31–43.
Crockford, D., Quickfall, J., Currie, S., Furtado, S., Suchowersky, O., & El-Guebaly, N. (2008). Prevalence of problem and pathological gambling in Parkinson’s disease. Journal of Gambling Studies, 24, 411–422.
Currie, S. R., & Casey, D. M. (2007). Quantification and dimensionalization of gambling behaviour. In G. Smith, D. C. Hodgins, & R. J. Williams (Eds.), Research and measurement issues in gambling studies (pp. 156–173). Burlington: Academic Press.
Currie, S. R. et al. (2012). Examining the predictive validity of low risk gambling limits with longitudinal data. Addiction, 107, 400–406.
Currie, S., Hodgins, D. C., & Wang, J. L. (2008a). Canadian low-risk gambling limits: New evidence and limitations. Guelph, ON: Ontario Problem Research Centre.
Currie, S. R., Hodgins, D. C., Wang, J., el-Guebaly, N., & Wynne, H. (2008b). In pursuit of empirically based responsible gambling limits. International Gambling Studies, 8, 209–229.
Currie, S. R., Hodgins, D. C., Wang, J., el-Guebaly, N., Wynne, H., & Chen, S. (2006). Risk of harm from gambling in the general population as a function of level of participation in gambling activities. Addiction, 101, 570–580.
Currie, S. R., Hodgins, D. C., Wang, J., el-Guebaly, N., Wynne, H., & Miller, N. V. (2008c). Replication of low-risk gambling limits using Canadian provincial gambling prevalence data. Journal of Gambling Studies, 24, 321–335.
Currie, S. R., Miller, N. V., Hodgins, D. C., & Wang, J. (2008d). Defining a threshold of harm from gambling for population health surveillance research. International Gambling Studies, 9, 19–38.
el-Guebaly, N., Casey, D., Hodgins, D. C., Smith, G., Williams, R. J., Schopflocher, D. P., et al. (2008). Designing a longitudinal cohort study of gambling in Alberta: Rationale, methods, and challenges. Journal of Gambling Studies, 4, 479–504.
el-Guebaly, N., Patten, S. B., Currie, S. R., Williams, J. M., Beck, C., & Maxwell, C. (2006). Epidemiological associations between gambling behavior, substance use and mood and anxiety disorders. Journal of Gambling Studies, 22, 275–287.
Ferris, J., & Wynne, H. J. (2001). The Canadian Problem Gambling Index final report Ottawa. ON: Canadian Centre on Substance Abuse.
Gravel, R., & Beland, Y. (2005). The Canadian Community Health Survey: Mental health and well-being. Canadian Journal of Psychiatry (Revue Canadienne de Psychiatrie), 50, 573–579.
Jacobson, N. S., Roberts, L. J., Berns, S. B., & McGlinchey, J. B. (1999). Methods for defining and determining the clinical significance of treatment effects: Description, application, and alternatives. Journal of Consulting and Clinical Psychology, 67, 300–307.
Johansson, A., Grant, J. E., Won Kim, S., Odlaug, B. L., & Gotestam, K. G. (2009). Risk factors for problematic gambling: A critical literature review. Journal of Gambling Studies, 25, 67–92.
Masse, R., Poulin, C., Dasa, C., Lambert, J., Belair, S., & Battaglini, A. (1998). Elaboration et validation d’un outil de mesure du bien-etre psychologique: L’emmbep. Canadian Journal of Public Health, 89, 357.
McCready, J., & Adlaf, E. (2006). Performance and enhancement of the Canadian Problem Gambling Index: Report and recommendations Guelph. ON: Ontario Problem Gambling Research Centre.
Mcmillen, J., & Wenzel, M. (2006). Measuring problem gambling: Assessment of three prevalence screens. International Gambling Studies, 6, 147–174.
Miller, N. V., & Currie, S. R. (2008). A Canadian population level analysis of the roles of irrational gambling cognitions and risky gambling practices as correlates of gambling intensity and pathological gambling. Journal of Gambling Studies, 24, 257–274.
Orford, J., Wardle, H., Griffith, M., Sproston, K., & Erens, B. (2010). PGSI and DSM-IV in the 2007 British Gambling Prevalence Survey: Reliability, item response, factor structure and inter-scale agreement. International Gambling Studies, 10, 31–44.
Raylu, N., & Oei, T. P. S. (2002). Pathological gambling: A comprehensive review. Clinical Psychology Review, 22, 1009–1062.
Smith, G. J. (2010). Gambling policy and public opinion. Presentation at the Alberta Gaming Research Institute’s 9th Annual Conference (On-line).
Statistics Canada. (2002). Canadian Community Health Survey (Cycle 1.2)—Mental health and well-being user’s guide. Ottawa, ON: Statistics Canada.
Stinchfield, R., Govoni, R., & Frisch, G. R. (2007). A review of screening and assessment instruments for problem and pathological gambling. In G. Smith, D. C. Hodgins, & R. J. Williams (Eds.), Research and measurement issues in gambling studies (pp. 179–213). Burlington, MA: Academic Press.
Strong, D. R., & Kahler, C. W. (2007). Evaluation of the continuum of gambling problems using the DSM-IV. Addiction, 102, 713–721.
Weinstock, J., Ledgerwood, D. M., & Petry, N. M. (2007). Association between posttreatment gambling behavior and harm in pathological gamblers. Psychology of Addictive Behaviors, 21(2), 185–193.
Welte, J., Barnes, G., Wieczorek, W., Tidwell, M.-C., & Parker, J. (2004). Risk factors for pathological gambling. Addictive Behaviors, 29, 323–335.
Acknowledgments
This research was funded by research grants from the Alberta Gaming Research Institute and the Canadian Consortium for Gambling Research (consisting of Alberta Gaming Research Institute, Canadian Centre on Substance Abuse, Canadian Partnership for responsible Gambling, Manitoba Gaming Control Commission, Nova Scotia Gaming Foundation, Ontario Problem Gambling Research Centre, Saskatchewan Health). The authors thank the other investigators on the Leisure, Lifestyle, and Lifecycle Project (Drs. Nady el-Guebaly, Gary Smith, Robert Williams, and Donald Schopflocher) for permission to use the LLLP data in this study. The authors also thank Lynda Edwards who helped in manuscript preparation.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Currie, S.R., Hodgins, D.C. & Casey, D.M. Validity of the Problem Gambling Severity Index Interpretive Categories. J Gambl Stud 29, 311–327 (2013). https://doi.org/10.1007/s10899-012-9300-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10899-012-9300-6