
Abstract
Background
We have established a standard procedure for Roux-en-Y (RY) reconstruction in laparoscopic total gastrectomy (LTG) using esophagojejunostomy by the overlap method (OL). We report on our RY reconstruction technique and special approaches, and evaluate the usefulness of our reconstruction method based on the surgical results of 100 patients we have experienced to date.
Methods
We performed LTG in 100 patients with gastric cancer. After total gastrectomy using five ports, the resected stomach was extracted through a small laparotomy. Through that, we performed sacrifice of the jejunum, Y limb anastomosis, creation of the lifted jejunum. As the OL, a side-to-side anastomosis of the lifted jejunum to the esophageal stump was laparoscopically performed using a linear stapler in an isoperistaltic direction, and the entry hole was closed with full-thickness suturing. The lifted jejunum was fixed with suture to the duodenal stump at a location where the esophagojejunostomy site was made linear, and the duodenal stump was buried. The mesenteric gap was laparoscopically closed with suture.
Results
The median operative time in 100 patients undergoing LTG was 385 min, the median blood loss was 65 mL, and the median time required for the OL was 32 min. The mean hospitalization period was 10 days, and postoperative complications included bleeding requiring reoperation in one patient; other complications such as pancreatic fistula in five patients (5 %) were treated conservatively. No complication associated with anastomosis occurred.
Conclusion
In RY reconstruction using the OL, there were no complications associated with the anastomosis site in 100 consecutive patients, such as anastomotic leak or stenosis, indicating that it is a very useful and safe reconstruction method.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Laparoscopic total gastrectomy (LTG) requires a high degree of skill in gastrectomy with systematic lymphadenectomy as well as for postresection reconstruction, and is difficult even for expert laparoscopic surgeons. Therefore, it is not as widely used as laparoscopic distal gastrectomy (LDG) [1–3]. Similar to laparotomy, Roux-en-Y (RY) reconstruction is generally performed following LTG, and various methods and approaches have been reported for esophagojejunostomy [2, 4]. Esophagojejunostomy is largely performed by a circular stapler (CS) or a linear stapler (LS) method. For the CS method, various approaches have been employed for laparoscopic insertion of an anvil and the main unit, and new tools such as OrVil™ (Covidien, Mansfield, MA, USA) have been developed based on experience with laparotomy [5–7]. Meanwhile, the LS method is a unique procedure developed for laparoscopic surgery [1, 8–11]. We selected the LS method as appropriate for LTG because it can be used regardless of the diameters of the esophagus and jejunum. Furthermore, it can easily be inserted through a port for laparoscopy, and it is slender and can easily secure a visual field. However, despite advantages of using LS for laparoscopic surgery, serious complications such as esophagojejunostomy leak, stenosis, internal hernia, and duodenal stump fistula have been reported for RY reconstruction using LS, similar to those for CS; therefore, special approaches are required [2, 3]. We established a standard method for RY reconstruction using the overlap method (OL) with isoperistaltic side-to-side esophagojejunostomy by adding special approaches to prevent complications, such as linear anastomosis, prevention of excessive mobility of the lifted jejunum, duodenal stump covering, and mesenteric gap closure. Herein, we report the short-term results for 100 patients who underwent RY reconstruction using the OL, and demonstrate the details of the new anastomosis technique, which is an advancement over the conventional OL.
Methods
Patients
The subjects were 100 patients who had undergone LTG and RY reconstruction using the overlap method for the diagnosis of gastric cancer at Kariya Toyota General Hospital between April 2011 and April 2015. One surgeon (HK) participated as an operator or a supervisory assistant. The Japanese classification of gastric carcinoma, 14th edition [12], was used for all patients; total gastrectomy was indicated in all patients according to the Japanese gastric cancer treatment guidelines [13].
Operative methods
Setting
Patients underwent surgery in an open-leg position under general anesthesia. The same port arrangement, forceps, and energy device (ultrasound incision device, electric scalpel) were used in all surgeries. ECHELON FLEX™ ENDOPATH® Stapler 45 mm (Ethicon Endo-Surgery, LLC Guaynabo, Puerto Rico, USA) was used as the LS for gastric resection and reconstruction. PDS®II and PROLENE® (Ethicon, Inc., Somerville, New Jersey, USA) were used as absorbable and non-absorbable suture threads, respectively.
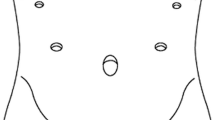
A 12 mm video port was inserted into the subumbilical area. Two operator ports were placed: a 5 mm port in the right hypochondrium, and a 12 mm lower right port medial and caudal to the 5 mm port, with a fist-size distance between them. One 5 mm assistant port was placed in the left hypochondrium and another 5 mm port was placed at the height of the umbilicus, caudal and medial to the first port. A liver retractor was inserted from the right side immediately below the manubrium to elevate the round ligament and the lateral segment of the liver. Surgery with CO2 pneumoperitoneum (8 mmHg) was performed (Fig. 1).

Arrangement of port sites. LR Liver retractor, black circle 12 mm trocar for the scope, gray circle 12-mm trocar for insert of linear stapler, triangle 5 mm trocar
Gastrectomy
D1+ or D2 lymphadenectomy was performed with the addition of splenectomy or pancreatic tail resection when required. The LS used for cutting and reconstruction was inserted through the lower right port, and was operated by the surgeon’s right hand. The duodenum was resected immediately below the pylorus, from the caudal side to the cranial side with the LS (1.5 mm closed staple height cartridge). The esophagus was transected from the right to the left side with the LS (1.8 mm cartridge). The resected stomach was collected in a bag and removed through the small laparotomy (the extended umbilical port wound).
Reconstruction
Creation of the lifted jejunum, Y limb anastomosis
The jejunum was guided outside the abdominal cavity through the small laparotomy, and transected 25 cm from the ligament of Treitz with the LS (1.0 mm cartridge). From there, the mesentery was transected along the jejunum to the anal side, and the distal side of the jejunum (approximately 15 cm) to be sacrificed was prepared. The prepared jejunum was resected with the LS (1.0 mm cartridge), and the jejunum of the anal side was lifted. The staple line on the stump was buried with interrupted 4-0 absorbable suture. A 1 cm hole was made on the antimesenteric side of the lifted jejunum, approximately 45 cm to the anal side. Another 1 cm hole was made by resecting the stapled site on the antimesenteric side of the oral side jejunal stump. The forks of the LS (1.0 mm cartridge) were inserted through each hole and fired side-to-side. The entry hole, through which the LS was inserted, was opened toward the direction where a V-shaped staple line was created in the inner cavity, and closed with continuous 4-0 absorbable suture. The exposed staple line was buried and sutured. To insert the anvil fork of the LS, a 1 cm hole was made on the antimesenteric side, 5 cm to the anal side from the apex of the lifted jejunum. The extracorporeally operated small intestine was returned to the abdominal cavity, and a port was inserted through the small laparotomy, which was sutured.
Overlap method of esophagojejunostomy
The left end of the stapled line on the cut-off stump of the esophagus was transected by 1 cm, and a small hole was made at the esophagus. The lifted jejunum was guided to the left side of the esophagus via the antecolic route, and the anvil fork was inserted through the small hole. A transnasal gastric tube was inserted into the abdominal cavity through the small hole made at the esophagus; using this as a guide, the cartridge fork of the LS (1.5 mm cartridge) was inserted into the esophagus (Fig. 2A). The LS was fired in an isoperistaltic direction with the esophagus stump on the right side and the lifted jejunal stump on the left side (Fig. 2B). A supporting thread was placed on both ends of the entry hole to create a V-shaped staple line between the esophagus and jejunum. Using 3-0 absorbable suture, single-ligation full thickness suture with 11–13 stitches was performed using the extracorporeal slip knot technique for closure (Fig. 2C).

Schematic outline of the overlap anastomosis. A An anvil fork is inserted into a small hole at the lifted jejunum, and using a transnasal gastric tube as a guide, the cartridge fork of the LS is inserted into the esophagus. B The LS is fired in an isoperistaltic direction with the esophageal stump on the right side and the lifted jejunal stump on the left side. C The entry hole is closed by single-ligation full thickness suture to make a V-shaped staple line in the inner cavity. D The lifted jejunum is fixed with suture to the duodenal stump at a location where the esophagojejunostomy site is made linear, and the duodenal stump is covered (black arrow). The mesenteric gap and Petersen’s defect are closed with suture (white arrow)
Fixation of the lifted jejunum, mesenteric gap closure
The lifted jejunum was fixed to the duodenal stump at a position where the esophagojejunostomy site was made linear with 3 stitches and single ligation using 3-0 absorbable suture, and the staple line on the duodenum was covered with the jejunal wall. The mesenteric gap created between the lifted jejunum and the Y limb anastomosis site and Petersen’s defect were respectively closed laparoscopically using 3-0 non-absorbable suture (Fig. 2D). A closed-type drain was placed dorsal to the esophagojejunostomy site through the lower right port wound.
Postoperative management
All patients received the same postoperative management according to a critical pathway. On the first postoperative day, the transnasal gastric tube was removed and patients started ambulation. Water was started on postoperative day (POD) 1. On POD 3, all patients started a liquid diet after undergoing gastrointestinal contrast-enhanced imaging to check for leakage and passage at the anastomosis site. Drains were removed on POD 5, with discharge on a soft diet on POD 8–10. Patients were followed regularly in the outpatient department.
Results
To date, RY reconstruction using the OL has been conducted in 100 patients by 7 surgeons. In these continuous 100 cases of LTG indication, there were no cases of using anastomosis method other than OL.There were 76 men and 24 women, with a median age of 69 years and body mass index (BMI) 22.0 kg/m2. The median tumor diameter was 45 mm, and the clinical stages were Ia in 45 patients, Ib in 15, IIa in 6, IIIa in 13, IIIb in 4, IIIc in 7, and IV in 4 (Table 1). The types of surgery were total gastrectomy in 98 patients and total resection of the gastric remnant in 2 patients. The median operative time was 379 min, blood loss was 65 mL, and the time required for the OL was 32 min. Concurrent resections included spleen resection in 10 patients, pancreatic tail/spleen resection in 5, and cholecystectomy for concurrent gallstone in 5; descending colon resection in 1, and transverse colon resection in 1 were performed for early-stage colorectal cancer. Postoperative complications were noted in 6 patients, including postoperative bleeding (bleeding from short gastric artery stump) in 1 patient, Grade B pancreatic fistula (based on the criteria of the international study group on pancreatic fistula [14]) in 3, and pseudomembranous enterocolitis in 2. One patient with postoperative bleeding underwent reoperation, and others received conservative treatment. No patients had complications associated with anastomosis or reconstruction, such as anastomotic leak, stenosis, or stasis. The median first day of food intake was day 3, and the median hospitalization period was 10 days (Table 2). The patients have been followed for up to 4 years in the outpatient department; 1 patient had Petersen’s hernia 2 years after surgery and 1 had strangulating intestinal obstruction caused by band formation resulting from greater omentum adhesion to the staple of the Y limb anastomosis site 9 months after surgery; both underwent surgery.
Discussion
Many techniques have been reported for RY reconstruction after LTG, but it is not clear which anastomosis technique is most useful, and no standard method has been established [2, 4].
The OL was first reported by Inaba et al. [8] as a new method for esophagojejunostomy in RY reconstruction after LTG. Various approaches were recently added to the OL, and surgical results with a few complications have been reported [9, 10]. In order to stabilize the results of LTG, we selected RY reconstruction using OL, and standardized the method by adding special approaches. These include: (1) doing as much as possible through the small laparotomy, through which the stomach is removed; (2) operating the LS with the surgeon’s right hand through the lower right port; (3) suturing the lifted jejunum to the duodenum; thereby making the anastomosis site linear, and covering the duodenal stump. The following were subsequently added: (4) burial and suturing of the staple line, and (5) suturing and closing the mesenteric gap laparoscopically using non-absorbable suture after the completion of anastomosis. We were able to adapt this reconstruction method in all LTG cases.
Operation through a small laparotomy interferes with a good visual field and a wide operative field, which are the advantages of laparoscopic surgery. However, using a small laparotomy is advantageous for operations on the small intestine, which can easily be guided outside the abdominal cavity. We prepared the distal part of the jejunum to be sacrificed, created the lifted jejunum, performed Y limb anastomosis, and buried and sutured the staple line through an approximately 4 cm longitudinal laparotomy crossing the umbilicus, which was created for the removal of the resected stomach. In all of our patients, these procedures could be performed through the small laparotomy without difficulty; a procedure under direct vision could reduce the total operative time.
Yamamoto et al. [10] reported the superiority of operating the LS with the surgeon’s right hand through a lower right port in the OL. Similarly, in our patients, the right hand operated the LS through the lower right port. The esophagus was vertically transected, and esophagojejunostomy was performed on the left side of the esophagus. The esophageal stump was pulled to the right side with forceps inserted through the upper right port, which made the LS inserted through the lower right port and the axis of the esophagus parallel, enabling easy insertion of the LS fork into the inner cavity of the esophagus. In addition, the entry hole was opened by placing a supporting thread on both ends, making the entry hole linear and turned to the right (surgeon’s) side, which made closure with suture easy. Although the entry hole was closed with suture using Roeder’s knots, as reported by Inaba et al. [8], the use of continuous suture has also been reported, and should be considered to further reduce operative time.
The incidence of post-LTG complications is high at 10–40 % [3]. Esophagojejunostomy leak is a complication related to reconstruction, and accounts for 0.9–8.5 % of the overall LTG complications; it is a serious complication with a mortality rate of 50 % [5]. Excessive tension at the anastomosis site causes bleeding and perforation by a rupture of the esophageal mucosa, which is considered to be a cause of anastomotic leak [6, 7]. We sutured the lifted jejunum to the duodenal stump to make the esophagojejunal anastomosis site linear. This limits excessive mobility of the lifted jejunum, resulting in decreased tension at the anastomosis site. In addition, linear fixation should prevent torsion of the lifted jejunum, which will prevent passage disorders. Duodenal stump leakage was also noted in 1.0–3.4 % of the overall LTG complications [3]. Covering with adequate tissue should be effective for prevention of duodenal stump leakage; therefore, we performed suturing to the lifted jejunum along with covering of the duodenal stump in our technique.
Internal hernia is a complication unrelated to the anastomosis site, and has been reported in LTG [3, 15]. One of our patients developed Petersen’s hernia 2 years after surgery; since we considered this partly associated with gap closure with absorbable suture, we now use non-absorbable suture. Additionally, laparoscopic suturing for the mesojejunum defect after completion of anastomosis achieves appropriate closure with no tension at the anastomosis or fixation site. One of our patients had a strangulated ileus due to greater omentum adhesion to exposed staples at the Y limb anastomosis site; therefore, staples should be buried and sutured as much as possible.
We added special approaches to the OL to prevent complications and to enable procedures through a small laparotomy, thereby simplifying RY as much as possible and establishing a standard method for RY reconstruction. We have performed the procedure in 100 patients to date, and none have had complications related to the anastomosis site.
Limitations of this paper are in these. These include: (1) the OL has not been compared to other anastomotic methods; (2) this is a study of a single hospital of about 25 LTG cases per year; (3) one expert surgeon is involved as operator or assistant in all operations. However, our series demonstrated that a number of practicing surgeons was able to perform this reconstruction for various state of gastric cancer safely without complications under the proper guidance of an expert surgeon.
Conclusion
The OL, which is known as safe and firm method, could be the effective option for the reconstruction in RY.
References
Morimoto M, Kitagami H, Hayakawa T, Tanaka M, Matsuo Y, Takeyama H (2014) The overlap method is a safe and feasible for esophagojejunostomy after laparoscopic-assisted total gastrectomy. World J Surg Oncol 12:392–402
Okabe H, Tsunoda S, Tanaka E, Hisamori A, Kawada H, Sakai Y (2015) Is laparoscopic total gastrectomy a safe operation? A review of various anastomotic techniques and their outcomes. Surg Today 45:549–558
Kunisaki C, Makino H, Takagawa R, Kimura J, Ota M, Ichikawa Y, Kosaka T, Akiyama H, Endo I (2015) A systematic review of laparoscopic total gastrectomy for gastric cancer. Gastric Cancer 18:218–226
Shim JH, Yoo HM, Oh SI, Nam MJ, Jeon HM, Park CH, Song KY (2013) Various type of intracorporeal esophagojejunostomy after laparoscopic total gastrectomy for gastric cancer. Gastric Cancer 16:420–427
LaFemina J, Vinuela EF, Schattner MA, Gerdes H, Strong VE (2013) Esophagojejunal reconstruction after total gastrectomy for gastric cancer using a transsorally inserted anvil delivery system. Ann Surg Oncol 20:2975–2983
Chong-Wei K, Dan-Lei C, Dan D (2013) A modified thechnique for esophagojejunostomy or esophagogastrostomy after laparoscopic gastrectomy. Surg Laparosc Endosc Percutan Tech 23:e109–e115
Liao G-Q, Ou X-W, Lui S-Q, Zhang S-R, Huang W (2013) Laparoscopy-assisted total gastrectomy with trans-orally inseted anvil (Orvil™): a single institution experience. World J Gastroenterol 19:755–760
Inaba K, Satoh S, Ishida Y, Taniguchi K, Isogaki J, Kanaya S, Uyama I (2010) Overlap method: novel intracorporeal esophagojejunostomy after laparoscopic total gastrectomy. J Am Coll Surg 211:e25–e29
Tsujimoto H, Uyama I, Yaguchi Y, Kumano I, Takahata R, Matsumoto Y, Yoshida K, Horiguchi H, Aosasa S, Ono S, Yamamoto J, Hase K (2012) Outcome of overlap anastomosis using a linear stapler after laparoscopic total and proximal gastectomy. Langenbecks Arch Surg 397:833–840
Yamamoto M, Zaima M, Yamamoto H, Harada H, Kawamura J, Yamaguchi T (2014) A modified overlap methodo using a linear stapler for intracorporeal esophagojejunostomy after laparoscopic total gastrectomy. Hepatogastroenterology 61:543–548
Nagai E, Ohuchida K, Nakata K, Miyasaka Y, Maeyama R, Toma H, Shimizu S, Tanaka M (2013) Feasibility and safety of intracorporeal esophagojejunostomy after laparoscopic total gastrectomy: inverted T-shaped anastomosis using linear staplers. Surgery 153:732–738
Japanese Gastric Cancer Association (2011) Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer 14:101–112
Japanese Gastric Cancer Association (2011) Japanese gastriccancer treatment guidelines 2010 (ver. 3). Gastric Cancer 14:113–123
Bassi C, Dervenis C, Butturini G et al (2005) Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery 138:8–13
Ichikawa D, Komatsu S, Kubota T, Okamoto K, Konishi H, Shiozaki A, Fujiwara H, Otsuji E (2015) Evaluation of the safety and feasibility of laparoscopic total gastrectomy in clinical stage I gastric cancer patients. World J Surg 39:1782–1788
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Hidehiko Kitagami, Mamoru Morimoto, Kenichi Nakamura, Takahiro Watanabe, Yo Kurashima, Keisuke Nonoyama, Kaori Watanabe, Shiro Fujihata, Akira Yasuda, Minoru Yamamoto, Yasunobu Shimizu and Moritsugu Tanaka have no conflicts of interest or financial ties to disclose.
Rights and permissions
About this article

Cite this article
Kitagami, H., Morimoto, M., Nakamura, K. et al. Technique of Roux-en-Y reconstruction using overlap method after laparoscopic total gastrectomy for gastric cancer: 100 consecutively successful cases. Surg Endosc 30, 4086–4091 (2016). https://doi.org/10.1007/s00464-015-4724-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-015-4724-6