
Abstract
Summary
This study evaluates the prevalence of sarcopenia among older people admitted to a rehabilitation unit after hip fracture and the association between sarcopenia and functional outcomes. The results show that sarcopenia had a negative impact on functional recovery. The assessment of sarcopenia among older adults receiving rehabilitation programs is crucial.
Introduction
Sarcopenia is a highly prevalent geriatric syndrome associated with adverse outcomes, including falls, disability, institutionalization, and mortality. Few studies assessed sarcopenia among older adults receiving rehabilitation programs.
Methods
Patients aged 70 years or more consecutively admitted to in-hospital rehabilitation programs that had suffered from hip fracture entered the study. Sarcopenia was defined according to the Foundation for National Institutes of Health (FNIH) criteria. Multivariable linear regression models were used to analyze the association between the sarcopenia and functional recovery.
Results
The recruited population was composed of 127 patients, with a mean age of 81.3 ± 4.8 years, predominantly females (64.6%). Using the criteria proposed by the FNIH, patients with a diagnosis of sarcopenia were 43 (33.9%). After adjustment for potential confounders, participants with sarcopenia had a significant increased risk of incomplete functional recovery compared with non-sarcopenic patients (OR 3.07, 95% CI 1.07–8.75). Compared with participants without sarcopenia, those with sarcopenia showed lower Barthel index scores at the time of discharge from the rehabilitation unit (69.2 versus 58.9, respectively; p < 0.001) and after 3 months of follow-up (90.9 versus 80.5, respectively; p = 0.02).
Conclusions
These findings support the systematic assessment of sarcopenia among older adults receiving rehabilitation programs to assist in the development of personalized treatment plans aimed at improving functional outcomes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The concept of sarcopenia is encountered with increasing frequency in research and clinical practice, not only in geriatric medicine but also in other specialties [1]. Sarcopenia is considered a geriatric syndrome defined as a progressive impairment of muscle function due to the loss of skeletal muscle mass, which occurs with advancing age [2]. In older people, sarcopenia is one of the most important risk factor for mobility impairment, falls, disability, loss of independence, hospitalization, and death [3, 4]. The clinical implications of this geriatric syndrome have been consistently described across different settings including community-dwelling samples, nursing homes, and acute care units [5, 6].
According to a recent systematic review, the prevalence of sarcopenia is significantly high in most of the geriatric settings, but estimations impressively vary across studies because of different population characteristics, diagnostic criteria, and methods used to assess muscle mass and physical performance. When assessed according to the European Working Groups on Sarcopenia in Older People (EWGSOP) criteria [7], prevalence rates range from 1 to 29% among community-dwelling populations and from 17.4 to 32.8 among institutionalized older people [1, 8].
Previous study has reported that sarcopenia is independently associated with worse functional outcome at rehabilitation discharge, even though subjects with sarcopenia responded to rehabilitation and recovered their relatively poor pre-hospital functioning [9]. Nevertheless, data on the prevalence of sarcopenia and the association between sarcopenia and functional outcomes among patients admitted to in-hospital rehabilitation programs are scarce and limited to few and small studies.
The reports by the Foundation for National Institutes of Health (FNIH) Sarcopenia Project have recently motivated a reevaluation of existing operational definitions of sarcopenia that were mainly based on expert consensuses [10]. Indeed, the cut points for appendicular lean mass (ALM) proposed by the FNIH were identified through ad hoc analyses of multiple cohort studies of older persons. The FNIH project indicates two alternative gender-specific measures to define low muscle mass (ALM-to-body mass index and crude ALM). Given the rigorous approach followed by the FNIH consortium, these definitions may be considered the current “best practice” for defining low muscle mass in the older persons [11].
We therefore conducted a prospective study to evaluate the prevalence of sarcopenia—as defined by FNIH criteria [10]—and functional outcomes at discharge and after a 3-month follow-up in a cohort of older patients with hip fracture admitted to an in-hospital rehabilitation setting.
Materials and methods
Setting and sample
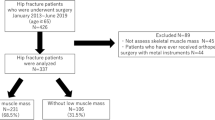
All patients aged 70 years or more (n = 135) consecutively admitted to the in-hospital Geriatric Rehabilitation Unit of the “A. Gemelli” Hospital—Catholic University of Sacred Heart, Rome—from October 2015 to September 2016, who suffered from a hip fracture, entered the study protocol. Seven patients who required interruption of the rehabilitation program for transfer back to acute care because of acute illness (four for sepsis, two for pulmonary embolism, and one for acute myocardial infarct) and one patient who died during the stay in the rehabilitation unit were excluded. Thus, 127 subjects were considered eligible for the study. The Catholic University of Sacred Heart ethics committee ratified the entire study protocol. Informed consent was obtained from all patients or, in the case of cognitive impairment, from authorized carers.
All patients were given an intensive rehabilitation program of physical therapy and occupational therapy. The rehabilitation program involved the patients for 3 h per day (6 days per week). This program included all purposeful activities to achieve maximal functional independence in mobility, prevent or correct disability, and maintain health. The treatment areas utilized were strengthening and range of motion exercise, musculoskeletal control, trunk and upper extremity positioning, transfer training, postural and gait training, functional and self-care retraining, and adaptive equipment training.
Participants were assessed within 48 h of admission to the in-hospital rehabilitation unit and followed until discharge. Participants’ data were collected through a standardized dedicated questionnaire including demographic characteristics, self-report functional status, cognitive assessment, medication use, admission and discharge diagnoses, and the results of some biochemical tests. The questionnaire was filled using a variety of information sources, such as direct observation, interviews with the patients, family or formal service providers, and a review of clinical records, both medical and nursing.
Assessment of sarcopenia
Body composition was estimated through whole-body supine DXA scans (Hologic QDR 4500A, Waltham, MA). Baseline DXA scan was used to identify sarcopenia based on the following procedure. First, ALM was calculated as the sum of lean soft tissue mass of upper and lower extremities, which were defined by computer-generated and manually adjusted regions of interest separating the appendages from the trunk and head. Second, the presence of sarcopenia was defined according to the FNIH recommendations [10]. The first criterion—ALM-to-body mass index [BMI] ratio (ALMBMI)—is recommended by the FNIH project, while the second—crude ALM—is proposed as an alternative. Thus, a participant was considered “sarcopenic” only if presenting with an ALMBMI below the gender-specific cut points indicated in the FNIH reports (<0.789 and <0.512 kg for men and women, respectively). If this first criterion was not fulfilled, the participant was tested with the alternative criterion to verify the true absence of a sarcopenic phenotype (<19.75 and <15.02 kg for men and women, respectively). Given the relevance of the FNIH initiative and the adopted approach [10], these definitions may be considered the current “best practice” for defining sarcopenia in older persons [11].
Functional outcome measure
Functional status was assessed using the Barthel index total score [12] through patient and surrogate interviews referring to the week before hospital admission for hip fracture, at the in-hospital rehabilitation unit admission, and at discharge. Furthermore, 3 months after discharge, a new Barthel index assessment was taken by telephone interview with the patient and/or a surrogate. Barthel index scores range from 0 (total functional dependency) to 100 (total functional independency). Shah and colleagues [13] suggested that scores of 0–20 indicate “total” dependency, 21–60 indicate “severe” dependency, 61–90 indicate “moderate” dependency, and 91–99 indicate “slight” dependency.
The full functional recovery at the time of discharge from the in-hospital rehabilitation unit was defined as the restoration of the Barthel index score to the pre-fracture value.
Covariates
Sociodemographic variables (age, gender, smoking habit, education) were recorded through clinical interview at in-hospital rehabilitation unit admission. Standardized assessments administered by research personnel (during the first 2 days) included the global Mini-Nutritional Assessment [14] and cognitive status upon admission as measured by the Mini-Mental State Examination (MMSE) test, which ranges from 0 (severely cognitively impaired) to 30 (cognitively intact) [15]. The BMI, based on admission weight, was then calculated as the weight (kg) divided by the square of height (m). Participants reporting light-intensity exercise for at least 2–4 h per week in the year prior to the hip fracture were defined as physically active.
Diagnoses of medical conditions and specific geriatric syndromes (pressure ulcer, urinary incontinence, daily pain) were gathered from the patient, attending physicians, and by a careful review of medical charts; comorbidity was assessed using the Charlson comorbidity index by adding scores assigned to specific diagnoses [16]. Assessors recorded all drugs taken by the participants at admission. All drugs were coded according to Anatomical Therapeutic Chemical codes and the number of drugs taken was calculated.
The number of days before admission was calculated as the day of surgery until the day of entry to the in-hospital rehabilitation unit. The total stay (in days) at the in-hospital rehabilitation unit was also calculated.
Standard determinations of serum albumin and hemoglobin were performed by commercially available kits (Olympus, Italy), suitable on Olympus 2700 instrumentation.
Statistical analysis
For descriptive purpose, baseline characteristics of the study population were compared according to presence or absence of sarcopenia, using a chi-squared test for categorical variables and the t-test or the non-parametric Mann-Whitney test for continuous variables.
Logistic regression analysis was used to assess the association between potential clinical and functional characteristics and functional recovery. Candidate variables to be included in the logistic regression model were selected on the basis of biological and clinical plausibility as risk factors for poor functional recovery (Table 1). To identify factors independently associated with negative outcomes, we first estimated a crude prevalence rate ratio (PRR) at a 95% CI and then controlled for age and gender. A logistic regression analysis was computed including all the variables that were associated with the outcome at an α level of 0.05 (education, BMI, pressure ulcer, urinary incontinence, daily pain, comorbidity index, total hip replacement, days before to be admitted in-hospital rehabilitation unit). Analysis of covariance (ANCOVA) was also used to compare the age- and gender-adjusted means of Barthel index scores between subjects with and without sarcopenia pre-fracture, at admission to the in-hospital rehabilitation unit, at discharge, and after 3 months of follow-up.
All analyses were performed using SPSS software (version 11.0, SPSS Inc., Chicago, IL).
Results
The recruited population was composed of 127 patients, with a mean age of 81.3 ± 4.8 years (range 71–100), predominantly females (64.6%). Using the criteria proposed by the FNIH [10], patients with a diagnosis of sarcopenia were 43 (33.9%).
The general characteristics of participants, stratified for the presence of sarcopenia, are presented in Table 1. Overall, men had a significantly higher rate of sarcopenia than women (72% versus 28%, respectively; p < 0.001). Compared with participants without sarcopenia, those diagnosed with sarcopenia were not significantly older, had a lower BMI, and a higher prevalence of pressure ulcers, urinary incontinence, and daily pain. Patients with sarcopenia were significantly more likely to have a higher Charlson comorbidity index (6.4 versus 5.2, respectively, p = 0.01). No significant differences were observed between sarcopenic and non-sarcopenic participants regarding the pre-fracture Barthel index scores and those obtained at the in-hospital rehabilitation unit admission. No differences were observed for the remaining variables.
In the unadjusted model, there was a direct association between sarcopenia and incomplete functional recovery (OR 3.44, 95% CI 1.08–11.74) (Table 2). After adjusting for potential confounders, this association remained statistically significant. In the adjusted model, participants with sarcopenia had a significant increased risk of not achieving a full recovery compared with non-sarcopenic patients (OR 3.07, 95% CI 1.07–8.75) (Table 2).
Figure 1 shows the trend of Barthel index scores, adjusted for age and gender (ANCOVA analysis), from pre-fracture to the 3-month follow-up. No significant difference was observed between sarcopenic and non-sarcopenic participants regarding the pre-fracture Barthel index scores and scores obtained at admission to the rehabilitation unit. Compared with those without sarcopenia, participants with sarcopenia show significant lower scores at the time of discharge from rehabilitation unit (69.2 versus 58.9, respectively; p < 0.001) and after the 3-month follow-up (90.9 versus 80.5, respectively; p = 0.02).

Trend of Barthel index scores adjusted for age and gender (ANCOVA analysis) from pre-fracture to 3-month follow-up after rehabilitation unit (RU) discharge according to sarcopenia. No significant difference was observed between sarcopenic and non-sarcopenic participants for pre-fracture Barthel index score and at admission to RU. Patients with sarcopenia showed lower scores at discharge from RU and after 3 months compared with those without sarcopenia
Discussion
In the present study, we estimated the effect of sarcopenia on functional recovery in a population of older persons admitted to an in-hospital rehabilitation unit following hip fracture repair. According to our findings, sarcopenia—assessed using the FNIH criteria [10]—is highly prevalent. Sarcopenia was significantly associated with worse overall functional status, as evaluated using the Barthel index total score, both at the time of discharge from the rehabilitation unit and after the 3-month follow-up.
Despite growing scientific interest around this condition, information regarding sarcopenia among older patients with hip fractures and its possible relation to functional recovery after intensive rehabilitation program is limited. Previous research conducted in various outpatient settings has reported a prevalence of sarcopenia ranging from 5 to 50% [1]. Only a limited number of studies evaluated the prevalence of sarcopenia and associated outcomes among patients admitted to in-hospital rehabilitation units. One study found a prevalence of sarcopenia around 46% in a group of 99 older adults (aged 75 years and older) admitted to a sub-acute geriatric care unit for rehabilitation [17]. More recently, Morandi and colleagues [9] observed a prevalence of sarcopenia of 60% in older adults admitted to an in-hospital rehabilitation setting and demonstrated that sarcopenia per se was independently associated with worse functional outcome at discharge. Thus, the relatively high prevalence of sarcopenia among participants in the current study is consistent with previous findings in outpatient settings [18, 19] and with prior studies in rehabilitation units [9].
Sarcopenia plays a central role in the frailty process as well as in its latent phase, contributing to many aspects of the frailty status [20]. The consequences of sarcopenia are detrimental as sarcopenic persons have important problems with mobility, frailty, fractures, and falls, and have an increased mortality [21]. In a study carried out in a community population, sarcopenic participants were over three times more likely to have fallen after a follow-up of 2 years compared with those without sarcopenia, regardless of age, gender, and other possible confounding factors [22]. However, few studies have described the presence of sarcopenia, as measured by means of validated methods, to be associated with worse functional outcomes in older adults. Furthermore, no research paper that relies on the accepted sarcopenia criteria has been published addressing its role in determining functional recovery after falls and hip fractures. The present study is the first attempt to estimate the relationship between sarcopenia and rehabilitation outcomes in older individuals using the FNIH criteria [10]. In this respect, it is important to highlight that the recent reports by the FNIH initiative have caused a re-evaluation of previously existing operational definitions (including the on proposed by the EWGSOP) that were largely based on experts’ consensuses. Findings of the FNIH were generated through ad hoc analyses of multiple cohort studies of older persons. Through the adoption of Classification and Regression Tree (CaRT) model, a wide range of muscle-related variables were tested and those that best predicted mobility disability identified. This statistical model not only supported the identification of the best predictors of the studied outcome but also proposed the optimal cut point for them. In this way, the FNIH reports have provided the variables that best capture the muscle mass decline and also proposed the gender-specific cut points to be used [10].
There is an urgent need to identify sarcopenia at an early stage—for example at hospital admission—to initiate prevention and specific interventions to avoid the debilitating consequences of this condition. For the construction of a practical conceptual model, sarcopenia may be considered the central element of the physical frailty syndrome [23]. By establishing a specific biological basis (i.e., skeletal muscle decline) of physical frailty, new approaches may be determined for the development of interventions designed to reduce or reverse this disorder. In this respect, it is noteworthy that all of the factors describing physical frailty and sarcopenia are quantifiable and measurable [24]. Hence, the implementation of this theoretical model is more likely to encourage important advancements than traditional approaches to this syndrome by enabling the accurate operationalization of the disorder, a clear identification of the affected population, and the rapid translation of findings into a clinical setting [25]. It is worth noting that such a conceptualization renders sarcopenia comparable to other common geriatric conditions, with the significant benefit of making the syndrome more easily identifiable by healthcare professionals, public health authorities, and regulatory bodies.
The relationship between sarcopenia and functional recovery after hip fracture has important implications regarding multifactorial interventions aimed at reducing the risk of declines in physical performance. Many studies have hypothesized that specific programs of physical activity represent the most important approach to slowing the decline of muscle mass and strength associated with aging and in the treatment of sarcopenia [26, 27]. At the same time, adequate nutrition, with respect to total calorie intake, protein, and micronutrients, such as vitamin D, has to be considered as an essential requisite for any successful therapeutic approach, in terms of prevention and treatment of sarcopenia [28, 29].
In interpreting the present findings, some limitations should be considered. As in all studies of this kind, selective survival before entry to the cohort has to be taken into account. Furthermore, in this observational study, results may be confounded by unmeasured factors. However, our homogeneous population of old people with a recent history of falls and hip fracture minimizes the possibility that patients without sarcopenia had substantially better health care or health knowledge than those with sarcopenia. In addition, we cannot completely exclude that a reverse causation may play an important role in the relationship between sarcopenia and poor functional recovery observed in our sample. However, because of the use of an extensive multidimensional assessment approach, the present study could comprehensively investigate the different domains influencing sarcopenia and rehabilitation outcomes. This made it possible to control for a large number of potential confounders. Despite this effort, it is possible that significant, not considered, differences between study groups may have biased the results and conclusions. For example, biomarkers that potentially correlated with sarcopenia and negative outcomes (i.e., vitamin D and inflammatory markers) have not been considered. Finally, this was a single-center study, potentially limiting the generalizability of the results.
In summary, in this sample of geriatric patients admitted to an in-hospital rehabilitation unit after hip fracture repair, the FNIH criteria identify sarcopenia as a common condition strongly related to functional recovery [10]. The potential relevance of these findings to clinical practice needs to be considered. In fact, it is important to highlight that worse functional outcomes were observed not only at the time of rehabilitation discharge but also at the 3-month follow-up. The measurement of muscle mass—as suggested by FNIH assessment criteria [10]—may contribute to the risk stratification process for rehabilitation outcomes. A deeper understanding of the mechanisms underlying the association between sarcopenia and functional recovery after hip fracture may also facilitate the development of interventions across the life course to preserve muscle function, prevent falls, and improve functional outcomes [30]. However, whether a prompt diagnosis and adequate nutritional and pharmacological interventions would modify the prognosis of these patients remains to be determined [31], [32], [33].
References
Cruz-Jentoft AJ, Landi F, Schneider SM, Zúñiga C, Arai H, Boirie Y, Chen L-K, Fielding RA, Martin FC, Michel J-P, Sieber C, Stout JR, Studenski SA, Vellas B, Woo J, Zamboni M, Cederholm T (2014) Prevalence of and interventions for sarcopenia in ageing adults: a systematic review. Report of the International Sarcopenia Initiative (EWGSOP and IWGS). Age Ageing 43:748–759
Landi F, Calvani R, Cesari M, Tosato M, Martone AM, Bernabei R, Onder G, Marzetti E (2015) Sarcopenia as the biological substrate of physical frailty. Clin Geriatr Med 31:367–374
Clynes MA, Edwards MH, Buehring B, Dennison EM, Binkley N, Cooper C (2015) Definitions of sarcopenia: associations with previous falls and fracture in a population sample. Calcif Tissue Int 97:445–452
Cruz-Jentoft AJ, Landi F, Topinková E Michel J-P 2010 Understanding sarcopenia as a geriatric syndrome. Curr. Opin. Clin. Nutr. Metab. Care 13
Beaudart C, McCloskey E, Bruyère O, Cesari M, Rolland Y, Rizzoli R, Araujo de Carvalho I, Amuthavalli Thiyagarajan J, Bautmans I, Bertière M-C, Brandi ML, Al-Daghri NM, Burlet N, Cavalier E, Cerreta F, Cherubini A, Fielding R, Gielen E, Landi F, Petermans J, Reginster J-Y, Visser M, Kanis J, Cooper C (2016) Sarcopenia in daily practice: assessment and management. BMC Geriatr 16:170
He H, Liu Y, Tian Q, Papasian CJ, Hu T, Deng H-W (2016) Relationship of sarcopenia and body composition with osteoporosis. Osteoporos Int 27:473–482
Cruz-Jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, Landi F, Martin FC, Michel J-P, Rolland Y, Schneider SM, Topinková E, Vandewoude M, Zamboni M, European Working Group on Sarcopenia in Older People (2010) Sarcopenia: European consensus on definition and diagnosis: report of the European Working Group on Sarcopenia in Older People. Age Ageing 39:412–423
Bischoff-Ferrari HA, Orav JE, Kanis JA, Rizzoli R, Schlögl M, Staehelin HB, Willett WC, Dawson-Hughes B (2015) Comparative performance of current definitions of sarcopenia against the prospective incidence of falls among community-dwelling seniors age 65 and older. Osteoporos Int 26:2793–2802
Morandi A, Onder G, Fodri L, Sanniti A, Schnelle J, Simmons S, Landi F, Gentile S, Trabucchi M, Bellelli G (2015) The association between the probability of sarcopenia and functional outcomes in older patients undergoing in-hospital rehabilitation. J Am Med Dir Assoc 16:951–956
Studenski SA, Peters KW, Alley DE, Cawthon PM, McLean RR, Harris TB, Ferrucci L, Guralnik JM, Fragala MS, Kenny AM, Kiel DP, Kritchevsky SB, Shardell MD, Dam T-TL, Vassileva MT (2014) The FNIH sarcopenia project: rationale, study description, conference recommendations, and final estimates. Journals Gerontol Ser A Biol Sci Med Sci 69:547–558
Dawson-Hughes B, Bischoff-Ferrari H (2016) Considerations concerning the definition of sarcopenia. Osteoporos Int 27:3139–3144
Mahoney FI, BARTHEL DW (1965) Functional evaluation: the Barthel index. Md State Med J 14:61–65
Shah S, Vanclay F, Cooper B (1989) Improving the sensitivity of the Barthel index for stroke rehabilitation. J Clin Epidemiol 42:703–709
Vellas B, Villars H, Abellan G, Soto ME, Rolland Y, Guigoz Y, Morley JE, Chumlea W, Salva A, Rubenstein LZ, Garry P Overview of the MNA—its history and challenges. J Nutr Health Aging 10:456–463 discussion 463–5
Folstein MF, Folstein SE, McHugh PR (1975) “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12:189–198
Deyo RA, Cherkin DC, Ciol MA (1992) Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol 45:613–619
Sánchez-Rodríguez D, Marco E, Miralles R, Fayos M, Mojal S, Alvarado M, Vázquez-Ibar O, Escalada F, Muniesa JM Sarcopenia, physical rehabilitation and functional outcomes of patients in a subacute geriatric care unit. Arch Gerontol Geriatr 59:39–43
Frost M, Nielsen TL, Brixen K, Andersen M (2015) Peak muscle mass in young men and sarcopenia in the ageing male. Osteoporos Int 26:749–756
Figueiredo CP, Domiciano DS, Lopes JB, Caparbo VF, Scazufca M, Bonfá E, Pereira RMR (2014) Prevalence of sarcopenia and associated risk factors by two diagnostic criteria in community-dwelling older men: the São Paulo Ageing & Health Study (SPAH). Osteoporos Int 25:589–596
Landi F, Calvani R, Tosato M, Martone AM, Bernabei R, Onder G, Marzetti E (2016) Impact of physical function impairment and multimorbidity on mortality among community-living older persons with sarcopaenia: results from the ilSIRENTE prospective cohort study. BMJ Open 6:e008281
Landi F, Cruz-Jentoft AJ, Liperoti R, Russo A, Giovannini S, Tosato M, Capoluongo E, Bernabei R, Onder G (2013) Sarcopenia and mortality risk in frail older persons aged 80 years and older: results from ilSIRENTE study. Age Ageing 42:203–209
Landi F, Liperoti R, Russo A, Giovannini S, Tosato M, Capoluongo E, Bernabei ROG (2012) Sarcopenia as a risk factor for falls in elderly individuals: results from the ilSIRENTE study. Clin Nutr 31:652–658
Cesari M, Landi F, Vellas B, Bernabei R, Marzetti E (2014) Sarcopenia and physical frailty: two sides of the same coin. Front Aging Neurosci 6:192
Scott D, Hayes A, Sanders KM, Aitken D, Ebeling PR, Jones G (2014) Operational definitions of sarcopenia and their associations with 5-year changes in falls risk in community-dwelling middle-aged and older adults. Osteoporos Int 25:187–193
Menant JC, Weber F, Lo J, Sturnieks DL, Close JC, Sachdev PS, Brodaty H, Lord SR 2016 Strength measures are better than muscle mass measures in predicting health-related outcomes in older people: time to abandon the term sarcopenia? Osteoporos. Int
Kemmler W, von Stengel S, Engelke K, Sieber C, Freiberger E (2016) Prevalence of sarcopenic obesity in Germany using established definitions: baseline data of the FORMOsA study. Osteoporos Int 27:275–281
Landi F, Marzetti E, Martone AM, Bernabei R, Onder G (2014) Exercise as a remedy for sarcopenia. Curr Opin Clin Nutr Metab Care 17:25–31
Landi F, Calvani R, Tosato M, Martone AM, Ortolani E, Savera G, D’Angelo E, Sisto A, Marzetti E (2016) Protein intake and muscle health in old age: from biological plausibility to clinical evidence. Nutrients 8
Gianoudis J, Bailey CA, Daly RM (2015) Associations between sedentary behaviour and body composition, muscle function and sarcopenia in community-dwelling older adults. Osteoporos Int 26:571–579
Morley JE (2016) Pharmacologic options for the treatment of sarcopenia. Calcif Tissue Int 98:319–333
Kelaiditi E, Jennings A, Steves CJ, Skinner J, Cassidy A, MacGregor AJ, Welch AA (2016) Measurements of skeletal muscle mass and power are positively related to a Mediterranean dietary pattern in women. Osteoporos Int 27:3251–3260
Cangussu LM, Nahas-Neto J, Orsatti CL, Bueloni-Dias FN, Nahas EAP (2015) Effect of vitamin D supplementation alone on muscle function in postmenopausal women: a randomized, double-blind, placebo-controlled clinical trial. Osteoporos Int 26:2413–2421
Akune T, Muraki S, Oka H, Tanaka S, Kawaguchi H, Nakamura K, Yoshimura N (2014) Exercise habits during middle age are associated with lower prevalence of sarcopenia: the ROAD study. Osteoporos Int 25:1081–1088
Acknowledgments
The study was partly supported by intramural research grants from the Catholic University of the Sacred Heart (D3.2 2013 and D3.2 2015), IMI-JU (# 115621), Fondazione Roma (NCDs Call for Proposals 2013, and the “Centro Studi Achille e Linda Lorenzon”.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
Emanuele Marzetti, Francesco Landi, and Riccardo Calvani are partners of the SPRINTT Consortium, which is partly funded by the European Federation of Pharmaceutical Industries and Associations (EFPIA). The other authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Landi, F., Calvani, R., Ortolani, E. et al. The association between sarcopenia and functional outcomes among older patients with hip fracture undergoing in-hospital rehabilitation. Osteoporos Int 28, 1569–1576 (2017). https://doi.org/10.1007/s00198-017-3929-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-017-3929-z