
Abstract
Summary
The present cross-sectional study investigated the prevalence of sarcopenia and clarified its associated factors in 1,000 elderly participants of Japanese population-based cohorts. Exercise habit in middle age was associated with low prevalence of sarcopenia in older age, suggesting that it is a protective factor against sarcopenia in older age.
Introduction
The present study investigated the prevalence of sarcopenia using the European Working Group on Sarcopenia in Older People (EWGSOP) definition, and clarified the association of sarcopenia with physical performance in the elderly participants of Japanese population-based cohorts of the Research on Osteoarthritis/osteoporosis Against Disability (ROAD) study.
Methods
We enrolled 1,000 participants (aged ≥65 years) from the second visit of the ROAD study who had completed assessment of handgrip strength, gait speed, and skeletal muscle mass measured by bioimpedance analysis. Presence of sarcopenia was determined according to the EWGSOP algorithm. Information collected included exercise habits in middle age.
Results
Prevalence of sarcopenia was 13.8 % in men and 12.4 % in women, and tended to be significantly higher according to increasing age in both sexes. Factors associated with sarcopenia, as determined by logistic regression analysis, were chair stand time (odds ratio [OR], 1.09; 95 % confidence interval [CI], 1.04–1.14), one-leg standing time (OR, 0.97; 95 % CI, 0.96–0.99), and exercise habit in middle age (OR, 0.53; 95 % CI, 0.31–0.90). Exercise habit in middle age was associated with low prevalence of sarcopenia in older age. Furthermore, linear regression analysis revealed that exercise habits in middle age were significantly associated with grip strength (P < .001), gait speed (P < .001), and one-leg standing time (P = .005) in older age.
Conclusions
This cross-sectional study suggests that exercise habit in middle age is a protective factor against sarcopenia in older age and effective in maintaining muscle strength and physical performance in older age.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Sarcopenia is characterized by generalized loss of skeletal muscle mass and muscle strength and/or function in the elderly, causing multiple adverse health outcomes, including physical disability, poor quality of life, and death [1–6]. Although cross-sectional studies have investigated prevalence of sarcopenia [7–13], epidemiologic evidence using population-based samples is insufficient despite the urgent need for strategies to prevent and treat this condition.
Japan is a super-aged society, and the proportion of the aged population is increasing. The percentage of individuals aged ≥65 years was 23 % in 2010 and is expected to reach 30.1 % in 2024 and 39 % in 2051 [14]. The government of Japan reported that musculoskeletal disorders were present in 22.9 % of the entire population of those who were certified as requiring assistance or long-term care elderly in 2010 and were ranked first among its causes, together with joint diseases, falls, fractures, and spinal cord disorders [15]. For preventing and treating musculoskeletal disorders, there is an urgent need to develop and establish a prevention strategy and treatment programs that are effective in reducing the risk of disability among the elderly, which leads to requirement of assistance or long-term care. Although sarcopenia is a common musculoskeletal disease in the elderly, it is not clearly categorized [15]. There appears to be insufficient recognition of sarcopenia in daily clinical practice and society, leading to the disease being undiagnosed and untreated. One of the reasons may be the lack of a broadly accepted definition of sarcopenia until the European Working Group on Sarcopenia in Older People (EWGSOP) developed a practical clinical definition and consensus diagnostic criteria for this disease in 2010 [4]. There is a growing consensus that sarcopenia should not be defined merely on the basis of muscle mass but also with regard to muscle strength and function [4]. However, few epidemiologic studies have been based on the EWGSOP definition of sarcopenia using population-based samples, and no epidemiologic study has investigated the relationship between exercise habits in middle age and sarcopenia in older age.
The Research on Osteoarthritis/osteoporosis Against Disability (ROAD) study is a prospective cohort study aimed at elucidating the environmental and genetic background of musculoskeletal diseases [16, 17]. The present study investigated the prevalence of sarcopenia using the EWGSOP definition, and clarified the association of sarcopenia with exercise habits in middle age and physical performance in the elderly participants of Japanese population-based cohorts of the ROAD study.
Methods
Participants
From 2005–2007, we began a large-scale population-based cohort study entitled Research on Osteoarthritis/osteoporosis Against Disability consisting of 3,040 participants in three regions (baseline study) [16, 17]. The ROAD study is a prospective cohort study with the aim of elucidating the environmental and genetic backgrounds of musculoskeletal diseases. It is designed to examine the extent to which risk factors for these diseases are related to clinical features of the diseases, laboratory and radiographic findings, bone mass, bone geometry, lifestyle, nutritional factors, anthropometric and neuromuscular measures, and fall propensity. It also aims to determine how these diseases affect activities of daily living and quality of life of Japanese men and women. The subjects were residents of any one of three communities: an urban region in Itabashi, Tokyo; a mountainous region in Hidakagawa, Wakayama; and a coastal region in Taiji, Wakayama. The inclusion criteria were as follows: ability to (1) walk to the clinic where the survey was performed, (2) provide self-reported data, and (3) understand and sign an informed consent form. Participants from the urban region were aged ≥60 years and were recruited from those enrolled in a randomly selected cohort study from the previously established Itabashi Ward residential registration database [18]. Invitation letters were distributed only to inhabitants whose names were listed on this database. Participants from Hidakagawa and Taiji were aged ≥40 years and were recruited from residential registration listings. Residents aged <60 years from Itabashi and <40 years from Hidakagawa and Taiji who were interested in participating in the study were also invited. A total of 99.8, 84.3, and 54.7 % of the participants were aged ≥60 years in Itabashi, Hidakagawa, and Taiji, respectively. The response rates in the groups aged ≥60 years were 75.6 % in Itabashi, 68.4 % in Hidakagawa, and 29.3 % in Taiji. Two-thirds of the 3,040 participants in the baseline survey were women, and their mean age was 1 year less than that of the male participants. No significant difference was observed in body mass index (BMI) between the sexes.
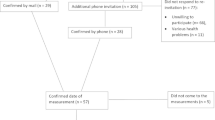
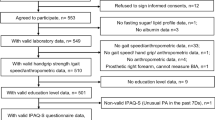
After the baseline study, a second survey was performed in the same communities from 2008 to 2010, in which 2,674 inhabitants (892 men, 1,782 women) aged 21–97 years participated (second visit) [19]. Invitation letters were distributed to the inhabitants whose names were listed on the baseline database of the ROAD study. In addition to the former participants, inhabitants aged ≥60 years from Itabashi and those aged ≥40 years from Hidakagawa and Taiji who were willing to participate in the ROAD survey performed in 2008–2010 were also included in the second visit. In addition, residents aged <60 years from Itabashi and <40 years from Hidakagawa and Taiji who were interested in participating in the study were invited to be examined as well at the baseline. The inclusion criteria were as follows: ability to (1) walk to the clinic where the survey was performed, (2) provide self-reported data, and (3) understand and sign an informed consent form. No other exclusion criteria were used. Thus, 2,674 residents (892 men and 1,782 women) aged 21–97 years participated in the second visit. Of the 2,674 participants, 1,846 individuals aged ≥65 years visited the clinic and underwent an examination at the survey site located in Hidakagawa (504 individuals), Taiji (391 individuals), the University of Tokyo Hospital (132 individuals), or Tokyo Metropolitan Geriatric Hospital (819 individuals). For participants from Itabashi, the survey site was randomly assigned to either the University of Tokyo Hospital or Tokyo Metropolitan Geriatric Hospital. Since gait speed was not measured at Tokyo Metropolitan Geriatric Hospital, 819 individuals who visited this hospital were removed from the present study. Of 1,846 participants, the remaining 1,019 individuals aged ≥65 years who visited the survey site located in Hidakagawa, Taiji, or at the University of Tokyo Hospital and underwent an examination including gait speed assessment were recruited for the present study. Of the 1,019 individuals, 19 were removed because 1 did not undergo handgrip strength measurement and 18 did not undergo skeletal muscle mass measurement. For the present study, we enrolled 1,000 participants (349 men and 651 women aged ≥65 years) from the second visit who completed assessment of handgrip strength, gait speed, and skeletal muscle mass. The mean age of the participants was 75.7 (SD, 5.9) years in men and 74.4 (SD, 6.1) years in women. All participants provided written informed consent, and the study was conducted with approval from the Ethics Committee of the University of Tokyo.
Participants completed an interviewer-administered questionnaire comprising 400 items regarding lifestyle information such as smoking habits, alcohol consumption, and physical activity. An interviewer asked the following question regarding past physical activity: “During the time you were aged 25–50 years, did you ever practice sports or physical exercise sufficient to produce sweating or shortness of breath?” Possible responses were as follows: never, occasionally, <2 hours per week, and ≥2 hours per week. Those who answered “occasionally, <2 hours per week, or ≥2 hours per week” were defined as having exercise habits in middle age. The following question was asked regarding current physical activity: “Do you practice walking more than 30 minutes every day?” Those who answered “yes” were defined as having a current walking habit.
Anthropometric and physical performance measurements
Anthropometric measurements, including height and weight, were obtained, and body mass index (weight [kg]/height [m2]) was estimated based on the measured height and weight. Grip strength was measured on the right and left sides using a TOEI LIGHT handgrip dynamometer (TOEI LIGHT CO. LTD, Saitama, Japan), and the highest measurement was used to characterize maximum muscle strength. Subjects were defined as having low grip strength if grip strength was <30 kg in men and <20 kg in women, as reported by Lauretani and colleagues [20].
Skeletal muscle mass was measured by bioimpedance analysis [21–25] using the Body Composition Analyzer MC-190 (Tanita Corp., Tokyo, Japan). The protocol was described by Tanimoto and colleagues [10, 12], and the method has been validated [26]. Appendicular skeletal muscle mass (ASM) was derived as the sum of the muscle mass of the arms and the legs. Absolute ASM was converted to an appendicular muscle mass index (SMI) by dividing by height in meters squared (kg/m2). Subjects were defined as having low skeletal muscle mass if the SMI was <2 SDs of the young adult mean. We used an SMI of <7.0 kg/m2 in men and <5.8 kg/m2 in women as cut-off points for low skeletal muscle mass based on the reference data of SMI measured by the MC-190 in 1,719 healthy young Japanese volunteers aged 18–39 years [10].
To measure physical performance, the time taken to walk 6 m at normal walking speed in a hallway was recorded, and usual gait speed was calculated. Subjects were defined as having low gait speed if usual gait speed was ≤0.8 m/s. The time taken for five consecutive chair rises without the use of hands was also recorded. Timing began with the command “Go” and ended when the buttocks contacted the chair on the fifth landing. One-leg standing time with eyes open was measured on both sides, and the best measurement was used. Participants were asked to stand on one leg while continuing to elevate their contralateral limb. Timing commenced when the participant assumed the correct posture and ended when any body part touched a supporting surface.
Statistical analysis
All statistical analyses were performed using STATA statistical software (STATA, College Station, TX). Differences in the values of the parameters between two groups were tested for significance using the nonpaired Student’s t test and chi-square test. Trends in values were tested using the Jonckheere-Terpstra trend test. Factors associated with sarcopenia were determined using multivariate logistic regression analysis with sarcopenia as the dependent variable; the odds ratio (OR) and 95 % confidence interval were determined after adjusting for age, sex, and BMI. Factors associated with exercise habits in middle age were determined using multivariate linear regression analysis with exercise habits in middle age as the independent variable; the regression coefficient and 95 % CI were determined after adjusting for age, sex, and BMI.
Results
Table 1 shows the characteristics of the participants according to EWGSOP sarcopenia status. Age was significantly greater, while BMI, ASM, and SMI were significantly lesser in those with sarcopenia than in those without sarcopenia in both men and women. In physical performance, chair stand time was significantly greater and one-leg standing time was significantly lesser in those with sarcopenia than in those without sarcopenia in both men and women. The percentage of individuals with exercise habits in middle age was significantly lower in those with sarcopenia than in those without sarcopenia in both men and women.
Figure 1 shows sex- and age-wise distributions of prevalence of sarcopenia (Fig. 1a), low SMI (Fig. 1b), low grip strength (Fig. 1c), and low gait speed (Fig. 1d). The total prevalence of sarcopenia was 13.8 % in men and 12.4 % in women. Prevalence of sarcopenia (number of cases/subjects) in the age strata of 65–69, 70–74, 75–79, 80–84, and ≥85 years was 1.6 % (1/63), 5.7 % (5/88), 17.8 % (19/107), 23.2 % (16/69), and 31.8 % (7/22) in men and 0.6 % (1/163), 5.5 % (10/182), 13.8 % (22/160), 22.9 % (25/109), and 62.2 % (23/37) in women. Prevalence of sarcopenia tended to be significantly higher according to increasing age (P < .001 for trend) in both men and women. Prevalence of low grip strength and low gait speed also tended to be significantly higher according to increasing age (P < .001 for trend) in both men and women. However, the increasing tendency of prevalence of low SMI (P < .001 for trend) was milder compared with that of sarcopenia, low grip strength, and low gait speed.

Percentage of sarcopenia (a), low skeletal muscle mass index (SMI) (b), low grip strength (c), and low gait speed (d) in men and women in each age stratum (65–69, 70–74, 75–79, 80–85, and ≥85 years). Low SMI was defined as a value of <7.0 kg/m2 in men and <5.8 kg/m2 in women. Low grip strength was defined as a value of <30 kg in men and <20 kg in women. Low gait speed was defined as a value of ≤0.8 m/s
Then, we determined the factors associated with sarcopenia by logistic regression analysis; the upper part of Table 2 shows the results using sarcopenia as the dependent variable. In the overall population, age (OR, 1.20; 95 % CI, 1.15–1.24) and BMI (OR, 0.68; 95 % CI, 0.63–0.75) were significantly associated with sarcopenia, whereas sex was not. In physical performance, chair stand time (OR, 1.09; 95 % CI, 1.04–1.14) and one-leg standing time (OR, 0.94; 95 % CI, 0.96–0.99) were significantly associated with sarcopenia in the overall population after adjusting for age, sex, and BMI. Current walking habit (OR, 0.69; 95 % CI, 0.42–1.12) was not significantly associated with sarcopenia. However, exercise habit in middle age (OR, 0.53; 95 % CI, 0.31–0.90) was associated with sarcopenia in the overall population after adjusting for age, sex, and BMI, indicating that exercise habit in middle age was significantly associated with low prevalence of sarcopenia in older age. The significance of the association did not change when current walking habit was added as an explanatory variable in this logistic regression model (OR, 0.53; 95 % CI, 0.32–0.90). In addition, we investigated the association of each category—occasionally, <2 h per week, and ≥2 h per week—with sarcopenia using “never” as a reference, in addition to the association of the presence of exercise habits in middle age with sarcopenia. The associated ORs for the three categories were comparable, but they did not reach significance level (occasionally: OR, 0.63; 95 % CI, 0.34–1.17; <2 h per week: OR, 0.30; 95 % CI, 0.09–1.01; ≥2 h per week: OR, 0.49; 95 % CI, 0.22–1.09).
The lower part of Table 2 shows the results of linear regression analysis using SMI, grip strength, gait speed, chair stand time, or one-leg standing time as the dependent variable and exercise habit in middle age as the independent variable. Exercise habit in middle age was significantly associated with grip strength in older age (P < .001), gait speed in older age (P < .001), and one-leg standing time in older age (P = .005) after adjusting for age, sex, and BMI in the overall population. We conducted the same analyses in men and women separately (Tables 3 and 4) and found results similar to those in the overall population. Some sex differences were observed in the present results. Exercise habit in middle age was significantly associated with grip strength and gait speed in older age in both men and women, whereas it was significantly associated with chair stand time and one-leg standing time only in men; however, the sample size of men was smaller than that of women. In the overall population, exercise habit in middle age was not associated with chair stand time.
Discussion
The present study investigated the prevalence of sarcopenia using the EWGSOP definition in the elderly participants of Japanese population-based cohorts. We determined that age was positively associated with sarcopenia and that BMI was inversely associated, but sex was not. Exercise habit in middle age was associated with increased muscle strength and physical performance and low prevalence of sarcopenia in older age. To the best of our knowledge, this is the first study to show the relationship between exercise habits in middle age and sarcopenia in older age in the elderly participants of population-based cohorts.
Previous studies have reported the prevalence of sarcopenia and its associated factors. For example, Tanimoto and colleagues reported the prevalence of sarcopenia in Japanese community-dwelling elderly individuals based on the EWGSOP definition using bioimpedance analysis (MC-190) [12]. They reported a prevalence of 11.3 % in men and 10.7 % in women [12], which is similar to our results. Although the cut-off value for low SMI was the same in these two studies, the cut-off value used for handgrip strength was different; we used cutoff values of <30 kg in men and <20 kg in women, in accordance with Lauretani and colleagues [20], while they used values of <30.3 kg in men and <19.3 kg in women, based on the lowest quartile of handgrip strength in their study population [12]. In the population of the present study, the lowest quartile of grip strength was 30.5 kg in men and 20.0 kg in women. Considering that these two studies showed similar results, cut-off values of 30 kg in men and 20 kg in women for handgrip strength [20] also may be appropriate for the practical case definition of the EWGSOP algorithm in the Japanese population.
Patel and colleagues reported the prevalence of sarcopenia in Caucasians using the EWGSOP definition, in which low muscle mass is defined as the lowest tertile of lean or fat-free mass [11]. They recommended use of the lowest tertile of muscle mass as a cut-off value if the reference value of muscle mass in a young healthy population is unavailable. In the population of the present study, the lowest tertile of SMI was 6.92 kg/m2 in men and 5.80 kg/m2 in women, which is similar to the cut-off value of <2 SDs of the young adult mean (7.0 kg/m2 in men and 5.8 kg/m2 in women) [10]. For evaluating low muscle mass, use of the lowest tertile may be an appropriate alternative method if the reference value of a young healthy population is unavailable.
The present study showed an association between sarcopenia and physical performance, including chair stand time and one-leg standing time, which is consistent with results of previous reports using the EWGSOP definition [11, 13]. However, these were comparisons between sarcopenia and current status of physical performance or exercise habit. Therefore, causal association was unclear whether sarcopenia was caused by decreased physical performance or activity or whether low physical performance or activity was due to sarcopenia. We also revealed that exercise habit in middle age was associated with increased muscle strength and physical performance and low prevalence of sarcopenia in older age. These results suggest that exercise habit in middle age is a protective factor against sarcopenia in older age and effective in maintaining muscle strength and physical performance in older age.
Some sex differences were observed in the present results. Exercise habit in middle age was significantly associated with grip strength and gait speed in older age in both men and women, whereas it was significantly associated with chair stand time and one-leg standing time only in men; however, the sample size of men was smaller than that of women. In the overall population, exercise habit in middle age was not associated with chair stand time; this finding may have been influenced by the fact that the sample size of women was almost twice that of men. The present results suggest that the impact of exercise habit in middle age on physical ability in older age is greater in men than in women.
Since exercise is a modifiable factor, it is a promising finding that exercise habit may be effective in preventing sarcopenia. In the present study, exercise habit was defined as physical activity in the period when the individual was aged 25–50 years, in which subjects practiced sports or physical exercise sufficient to produce sweating or shortness of breath, occasionally or more frequently. Although exercise habit was associated with low prevalence of sarcopenia at the age of ≥65 years, some details remain unclear, including exercise type, intensity, time, and other factors appropriate for prevention of sarcopenia. In addition to the association of the presence of exercise habit in middle age with sarcopenia, we further investigated the association of each category—occasionally, <2 h per week, and ≥2 h per week—with sarcopenia using “never” as a reference. Among the three categories, the analysis could not determine the best frequency and amount of exercise for protection from sarcopenia. The associated ORs for the three categories were comparable, and no dose–response tendency was seen in the relationship between frequency and amount of exercise and prevalence of sarcopenia; the associations also did not reach significance level. The present results suggest that abstaining from exercise during middle age is a risk factor for sarcopenia in older age. Furthermore, the presence of exercise habit in middle age might be much more important than the frequency and amount of exercise. Further studies are necessary to develop intervention programs and to test their effectiveness, along with accumulation of epidemiologic evidence including longitudinal studies.
The present study has several limitations. First, since this was a cross-sectional design, a causal relationship could not be determined. Second, information regarding exercise habits in middle age was obtained by self-report, and there is a possibility of recall bias. Third, the present study included participants who could walk to the survey site and could understand and sign an informed consent form. Since those who did not meet these inclusion criteria were not included in the analyses, the study participants do not truly represent the general population because of health bias. This should be considered when generalizing the results of the present study. Fourth, the results may have been affected by the characteristics of the population, including age and BMI. In the present study, age was positively associated with sarcopenia, whereas BMI was inversely associated with sarcopenia. Therefore, care should be taken when extrapolating the data to other populations with different characteristics, including age and BMI, which may confound the results.
In conclusion, the present study revealed prevalence of sarcopenia in the elderly participants of Japanese population-based cohorts. Exercise habit in middle age was associated with increased muscle strength and physical performance and low prevalence of sarcopenia in older age. These results suggest that exercise habit in middle age is a protective factor against sarcopenia in older age and is effective in maintaining muscle strength and physical performance in older age. Further long-term longitudinal epidemiological studies are necessary to develop effective intervention programs for the prevention and treatment of sarcopenia.
References
Rosenberg I (1989) Summary comments: epidemiological and methodological problems in determining nutritional status of older persons. Am J Clin Nutr 50:1231–1233
Rosenberg IH (1997) Sarcopenia: origins and clinical relevance. J Nutr 127(5 Suppl):990S–991S
Morley JE, Baumgartner RN, Roubenoff R, Mayer J, Nair KS (2001) Sarcopenia. J Lab Clin Med 137(4):231–243
Cruz-Jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, Landi F, Martin FC, Michel JP, Rolland Y, Schneider SM, Topinkova E, Vandewoude M, Zamboni M (2010) European Working Group on Sarcopenia in Older People. Sarcopenia: European consensus on definition and diagnosis: report of the European Working Group on Sarcopenia in Older People. Age Ageing 39(4):412–423
Delmonico MJ, Harris TB, Lee JS, Visser M, Nevitt M, Kritchevsky SB, Tylavsky FA, Newman AB, Health, Aging and Body Composition Study (2007) Health, Aging and Body Composition Study. Alternative definitions of sarcopenia, lower extremity performance, and functional impairment with aging in older men and women. J Am Geriatr Soc 55(5):769–774
Goodpaster BH, Park SW, Harris TB, Kritchevsky SB, Nevitt M, Schwartz AV, Simonsick EM, Tylavsky FA, Visser M, Newman AB (2006) The loss of skeletal muscle strength, mass, and quality in older adults: the health, aging and body composition study. J Gerontol A Biol Sci Med Sci 61(10):1059–1064
Baumgartner RN, Koehler KM, Gallagher D, Romero L, Heymsfield SB, Ross RR, Garry PJ, Lindeman RD (1998) Epidemiology of sarcopenia among the elderly in New Mexico. Am J Epidemiol 147(8):755–763
Melton LJ 3rd, Khosla S, Crowson CS, O'Connor MK, O'Fallon WM, Riggs BL (2000) Epidemiology of sarcopenia. J Am Geriatr Soc 48(6):625–630
Iannuzzi-Sucich M, Prestwood KM, Kenny AM (2002) Prevalence of sarcopenia and predictors of skeletal muscle mass in healthy, older men and women. J Gerontol A Biol Sci Med Sci 57(12):M772–M777
Tanimoto Y, Watanabe M, Sun W, Sugiura Y, Tsuda Y, Kimura M, Hayashida I, Kusabiraki T, Kono K (2012) Association between sarcopenia and higher-level functional capacity in daily living in community-dwelling elderly subjects in Japan. Arch Gerontol Geriatr 55(2):e9–e13
Patel HP, Syddall HE, Jameson K, Robinson S, Denison H, Roberts HC, Edwards M, Dennison E, Cooper C, Aihie Sayer A (2013) Prevalence of sarcopenia in community-dwelling older people in the UK using the European Working Group on Sarcopenia in Older People (EWGSOP) definition: findings from the Hertfordshire Cohort Study (HCS). Age Ageing 42(3):378–384
Tanimoto Y, Watanabe M, Sun W, Tanimoto K, Shishikura K, Sugiura Y, Kusabiraki T, Kono K (2013) Association of sarcopenia with functional decline in community-dwelling elderly subjects in Japan. Geriatr Gerontol Int. doi:10.1111/ggi.12037
Lin CC, Lin WY, Meng NH, Li CI, Liu CS, Lin CH, Chang CK, Lee YD, Lee CC, Li TC (2013) Sarcopenia prevalence and associated factors in an elderly Taiwanese metropolitan population. J Am Geriatr Soc 61(3):459–462
National Institute of Population and Society Research. Population projections for Japan (January 2012): 2011 to 2060. http://www.ipss.go.jp/site-ad/index_english/esuikei/gh2401e.asp. Accessed 30 May 2013
Ministry of Health, Labour and Welfare. The outline of the results of National Livelihood Survey 2010. http://www.mhlw.go.jp/toukei/saikin/hw/k-tyosa/k-tyosa10/4-2.html. Accessed 30 May 2013
Yoshimura N, Muraki S, Oka H, Kawaguchi H, Nakamura K, Akune T (2010) Cohort profile: research on Osteoarthritis/Osteoporosis Against Disability study. Int J Epidemiol 39(4):988–995
Yoshimura N, Muraki S, Oka H, Mabuchi A, En-Yo Y, Yoshida M, Saika A, Yoshida H, Suzuki T, Yamamoto S, Ishibashi H, Kawaguchi H, Nakamura K, Akune T (2009) Prevalence of knee osteoarthritis, lumbar spondylosis, and osteoporosis in Japanese men and women: the research on osteoarthritis/osteoporosis against disability study. J Bone Miner Metab 27(5):620–628
Shimada H, Lord SR, Yoshida H, Kim H, Suzuki T (2007) Predictors of cessation of regular leisure-time physical activity in community-dwelling elderly people. Gerontology 53(5):293–297
Yoshimura N, Oka H, Muraki S, Akune T, Hirabayashi N, Matsuda S, Nojiri T, Hatanaka K, Ishimoto Y, Nagata K, Yoshida M, Tokimura F, Kawaguchi H, Nakamura K (2011) Reference values for hand grip strength, muscle mass, walking time, and one-leg standing time as indices for locomotive syndrome and associated disability: the second survey of the ROAD study. J Orthop Sci 16(6):768–777
Lauretani F, Russo CR, Bandinelli S, Bartali B, Cavazzini C, Di Iorio A, Corsi AM, Rantanen T, Guralnik JM, Ferrucci L (2003) Age-associated changes in skeletal muscles and their effect on mobility: an operational diagnosis of sarcopenia. J Appl Physiol 95(5):1851–1860
No authors listed (1996) Bioelectrical impedance analysis in body composition measurement: National Institutes of Health Technology Assessment Conference Statement. Am J Clin Nutr 64(3 Suppl):524S-532S
Janssen I, Heymsfield SB, Baumgartner RN, Ross R (2000) Estimation of skeletal muscle mass by bioelectrical impedance analysis. J Appl Physiol 89(2):465–471
Kyle UG, Genton L, Slosman DO, Pichard C (2001) Fat-free and fat mass percentiles in 5225 healthy subjects aged 15 to 98 years. Nutrition 17(7–8):534–541
Kyle UG, Genton L, Karsegard L, Slosman DO, Pichard C (2001) Single prediction equation for bioelectrical impedance analysis in adults aged 20–94 years. Nutrition 17(3):248–253
Roubenoff R, Baumgartner RN, Harris TB, Dallal GE, Hannan MT, Economos CD, Stauber PM, Wilson PW, Kiel DP (1997) Application of bioelectrical impedance analysis to elderly populations. J Gerontol A Biol Sci Med Sci 52(3):M129–M136
Nemoto M, Yasbushita N, Kim M, Tomoaki M, Satoshi S, Jung S, Hiroyuki S, Kiyoji T (2012) Validity of the bioelectrical impedance method for assessing body composition in non-frail and pre-frail older adults. Int J Body Comps Res 10:225–262
Acknowledgments
This study was supported by Grants-in-Aid for Scientific Research (S19109007, B20390182, B23390172, B23390356, and B23390357) from the Japanese Ministry of Education, Culture, Sports, Science and Technology; H17-Men-eki-009, H18-Choujyu-037, H20-Choujyu-009, H21-Chouju-Wakate-011, H22-Chouju-Wakate-007, and H23-Chouju-002 from the Ministry of Health, Labour and Welfare; and Research Aid from the Japanese Orthopaedic Association (JOA-Subsidized Science Project Research 2006–1 and 2010–2).
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Akune, T., Muraki, S., Oka, H. et al. Exercise habits during middle age are associated with lower prevalence of sarcopenia: the ROAD study. Osteoporos Int 25, 1081–1088 (2014). https://doi.org/10.1007/s00198-013-2550-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-013-2550-z