
Abstract
This meta-analysis examines the impact of parent interventions on outcomes for parents of children with ASD. A systematic review of the literature produced 37 studies that met inclusion criteria. Random-effects models revealed small but significant impacts of intervention on parental outcomes, primarily in parenting confidence and mental health. No improvements were observed in caregiving burden, family adjustment, physical health, or stress. Significant heterogeneity was observed; however, no moderation effects were detected for intervention or sample characteristics. These findings suggest parent interventions improve parenting confidence and, to a lesser degree, mental health. More work is needed to develop interventions that address a wider range of outcomes for parents of children with ASD. Limitations and implications for future research are discussed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Caring for an individual with autism spectrum disorder (ASD) is a unique experience, with both joys and challenges for parents across the lifespan. It has been widely supported that some of the specific challenges involved in this unique parenting experience can lead to a range of poor psychological, emotional, and family outcomes for parents. Parents of children with ASD tend to experience poorer outcomes than parents of typically developing children, and also, notably, than parents of children with other developmental disabilities such as cerebral palsy or Down syndrome (Hayes & Watson, 2013; Padden & James, 2017). They also report significant stress and psychiatric problems, with high rates of depression and anxiety (Estes et al., 2009; Padden & James, 2017; Snow & Donnelly, 2016). Additionally, high rates of caregiving burden and low parenting self-efficacy are common (Olsson & Hwang, 2002; Picardi et al., 2018; Sivberg, 2002; Snow & Donnelly, 2016). The experience of poor outcomes for these parents has been attributed to a wide range of challenges related to parenting an individual with ASD, such as management of symptoms and behaviors, financial burden, social stigma, and navigation of care systems and services (Bonis & Sawin, 2016).
Of the factors that influence poor outcomes for parents, connections between parental outcomes and child characteristics such as ASD symptoms and challenging behaviors are perhaps the most widely studied. Greater ASD symptom severity has been associated with higher stress and psychological distress among parents, as well as lower family wellbeing (Davis & Carter, 2008; Falk et al., 2014; García-López et al., 2016; Kissel & Nelson, 2016; Miller et al., 2016; Tomeny, 2017; Wang et al., 2013; Zablotsky et al., 2013). Challenging behavior refers to behaviors that threaten the safety of the individual with ASD or others, most commonly aggression, self-injury, property destruction, impulsivity, and emotion dysregulation (Matson et al., 2011). Challenging behaviors are common in ASD (Brobst et al., 2009; Estes et al., 2009) and can be significant sources of strain on parents. For example, more severe challenging behavior in children with ASD has been linked to higher rates of parental stress, depression, and anxiety (Athari et al., 2013; Beer et al., 2013; Davis & Carter, 2008; Estes et al., 2009; Falk et al., 2014; Hou et al., 2018; Jellett et al., 2015; MacHado Junior et al., 2016; Rezendes & Scarpa, 2011; Warfield et al., 2014). The strong links established between ASD characteristics and parent outcomes have provided the impetus for developing interventions that help parents understand and manage their child’s symptoms and behaviors.
Many interventions have been developed to try to ease the burden on parents of children with ASD. Given the connections identified between ASD characteristics and parent outcomes, interventions often consist of skills training and/or knowledge building treatments that prioritize didactic and/or hands-on training designed to teach parents about ASD symptomatology, train them to support their child’s adaptive growth in communication or social interaction, and/or help them learn to manage and shape maladaptive behavior (Ginn et al., 2017; Gulsrud et al., 2016; Howard et al., 2018; Iadarola et al., 2018; Karst et al., 2015; Kuravackel et al., 2018; Liao et al., 2014; Minjarez et al., 2013; Reitzel et al., 2013; Rivard et al., 2017; Tellegen & Sanders, 2014; Zand et al., 2017; Zlomke et al., 2017). A growing number of interventions extend beyond skills training and knowledge building to include direct strategies for general stress reduction, coping, and improvements in general mindfulness (Blackledge & Hayes, 2008; Dun et al., 2012; Ferraioli & Harris, 2013; Hwang et al., 2015; Lunsky et al., 2017; Nguyen et al., 2016; Rayan & Ahmad, 2017). While some studies examine the impacts of interventions that are well established in the literature, (e.g. Parent–Child Interaction Therapy; Joint Attention, Symbolic Play, Engagement & Regulation), many studies investigate new interventions with wide variation in purpose, content, and format.
In response to noted heterogeneity across parent interventions, Bearss et al. (2015) propose a helpful heuristic that organizes interventions into two categories representing their overall purpose: (1) “parent support” interventions that support parents with knowledge, and (2) “parent implementation” interventions that teach parents skills to implement an intervention (Bearss et al., 2015). Interventions classified as “parent support” provide parents with information on a wide range of topics relevant to caring for a child with ASD. Those classified as “parent implementation” instead teach parents how to facilitate development of their child’s social and communication skills or provide them with specific skills training to help them respond to challenging behaviors. This superstructure provides a useful approach to broadly organize the wide range of parent interventions that have been tested in the literature.
Given the well-documented caregiving impact of parenting an individual with autism combined with the great heterogeneity of existing parent interventions, a better understanding of the efficacy of such interventions for improving parent outcomes is needed. While the benefits of such parent interventions have been supported for improving child outcomes such as irritability, adaptive functioning, externalizing behaviors, disruptive behaviors, language, and communication (Ginn et al., 2017; Hansen et al., 2017; Howard et al., 2018; Iadarola et al., 2018; Postorino et al., 2017; Tellegen & Sanders, 2014; Zhou et al., 2018), the extent to which parent outcomes are improved by these interventions is less known. This is perhaps due in part to the fact that a substantial number of interventions designed for parents include only measures of child outcomes (Lecavalier, 2017; Mandelberg et al., 2014; Scahill, 2016; Tonge Brereton et al., 2014). Others may include only measures of intervention fidelity, acquisition of parenting skills (e.g. reciprocity, etc.), or social validity (i.e. parent satisfaction and intervention acceptability) (Oosterling, 2010; Siller Hutman & Sigman, 2012; Venker et al., 2011; Radley et al., 2014; Shire et al., 2015). A smaller, albeit growing, number of studies of parent interventions include measures of parent outcomes that are psychological, emotional, or related to family functioning, which has limited the conclusions that can be drawn about the ability for parent interventions to improve outcomes for parents. Consequently, selection of parent outcomes for the present analysis was limited to (1) outcomes that were available in the literature and (2) outcomes that were psychological, emotional or related to family functioning (i.e. beyond parenting behaviors, fidelity, and satisfaction). Thus, the present analysis looked at the following parent outcomes: caregiving burden, confidence in the parenting role, family adjustment, mental health, physical health, and stress.
Tarver et al. (2019) conducted a more recent systematic and meta-analytic review examining the impact specifically of interventions that teach parents behavioral management strategies on parental efficacy and stress outcomes. The present meta-analysis expands on work from Tarver et al. (2019) in that it includes a wider range of interventions (i.e. behavioral management interventions in addition to interactional/play-based interventions and psychoeducational/informational interventions) as well as examines a wider range of parent outcomes than prior meta-analytic work. Thus this analysis provides a broader understanding of whether different types of parent interventions may benefit parents across a range of domains. The purpose of this study was to conduct a meta-analytic review of existing interventions for parents of children with ASD in an effort to examine the degree to which parent interventions in any form may improve parental outcomes for parents of children with ASD.
Method
Data Sources and Literature Search
A systematic literature search was conducted to identify empirical tests of interventions for parents of children with ASD following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2009). The present review has not been registered, but a detailed description of the review protocol is described below. Keyword database searches were conducted in PubMed and PsycINFO from January 1967 to January 2020. The following sets of keywords were systematically combined: (1) autism, Asperger*, PDD, or pervasive developmental; and (2) parent, caregiver, mother, or father; and (3) parent mediated, parent intervention, parent education, psychoeducation, parent training, parent implemented, instruction, therapy, or program. The keyword search was limited to article titles and abstracts and duplicates between databases were automatically removed.
Inclusion and Exclusion Criteria
Included articles: (1) were written in English, (2) were published in peer-reviewed journals, (3) utilized a randomized controlled trial design, (4) provided a treatment or intervention to parents of children with ASD, (5) measured at least one parent outcome that was psychological, emotional, or related to family functioning (e.g. stress, depression, family adjustment, etc.), and (6) provided quantitative results on the effects of the parent intervention compared to a control. Studies were excluded if the parents of the sample had children who were at-risk for ASD without a formal diagnosis. Risk of bias was minimized by only selecting randomized controlled trials. Beyond that, no further risk of bias assessment was conducted. Comparative efficacy studies were excluded, which were small in number (k = 9), to reduce heterogeneity and ensure that experimental interventions were compared to a routine care control condition. One article (Kuravackel et al., 2018) examined two experimental treatments compared to treatment as usual, which was included as two separate studies. One article (Factor et al., 2019) utilized the same sample and study data from an older, smaller pilot RCT of the same intervention (Scarpa & Reyes, 2011). Because Factor and colleagues used parent data from the pilot RCT in addition to recruiting additional participants, study information was abstracted only from Factor et al., (2019) to avoid double counting identical data.
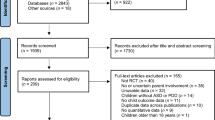
The initial search yielded 2, articles. The majority of these (2151) were excluded after abstract review, leaving 223 articles for full-text review. A total of 36 articles met inclusion criteria, representing 37 studies, and were included in the final meta-analysis (see Fig. 1 for PRISMA flow diagram).

PRISMA 2009 Flow Diagram
Data Extraction/Coding Procedures
The final 37 studies were reviewed and data were abstracted on the effects of experimental interventions compared to control on parent outcomes. Methodological characteristics that may moderate the efficacy of these interventions were also recorded. Raw pre- and post-intervention means and standard deviations for both the experimental and control groups were prioritized for outcome data abstraction. In the absence of raw means and standard deviations, F-statistics, p-values, or Cohen’s d were recorded.
Sample characteristics were coded, including sample size, average child IQ, and average parent and child age, proportion female, and proportion of the sample who were racial and/or ethic minorities. Studies were also coded for treatment setting (in-home, clinic/medical center, combined in-home/clinic, or other), total study duration, number and frequency of sessions, and total time of individual sessions (in minutes). Intervention durations were recorded in weeks, where 1 month was equal to 4.33 weeks. For studies that reported variable numbers of sessions, the maximum number of sessions was used.
Outcomes were categorized into five broad domains: caregiving burden, confidence in the parenting role, family adjustment, mental health, physical health, and stress. The caregiving burden category included outcomes related to the demands of child rearing and the available support in meeting such demands. Measures of caregiver strain, caregiver burden, the strains and stresses of child rearing, participation in social life, and social support were included in this category [e.g. Caregiver Strain Questionnaire (Brannan et al., 1997), Zarit Caregiver Burden Interview (Zarit et al., 1980), etc.]. Confidence in the parenting role included measures of parenting efficacy, parenting confidence, satisfaction with parenting, parent advocacy skills, empowerment in parenting, and parenting sense of competence [e.g. Parent Sense of Competence (Johnston & Mash, 1989), Family Empowerment Scale (Koren et al., 1992), etc.]. The family adjustment category included outcomes related to family life and adaptation, including family strengths and challenges and the structure and harmony of the home environment [Family Assessment Measure (Skinner et al., 1983) and Confusion, Hubbub, and Order Scale (CHAOS; Matheny et al., 1995), etc.]. The mental health category included measures of global mental health, depression, anxiety, and happiness [e.g. CES-D (Radloff, 1977), Beck Depression Inventory (Beck et al., 1961), State and Trait Anxiety Inventory (Spielberger et al., 1983), etc.]. Physical health was measured in one study using RAND’s Medical Outcomes Study (MOS) 36-Item Short-Form Health Survey (SF-36) (Ware & Sherbourne, 1992). The stress category included various measures of parenting stress [e.g., Parenting Stress Index (Abidin, 1995), Stress-Arousal Checklist (MacKay et al., 1978), etc.]. Outcome measures were reverse coded so that higher scores indicated more favorable outcomes.
Intervention Classification
A wide range of interventions with varying theoretical frameworks, modalities, and learning objectives were included in this meta-analysis. To conduct analyses on the relative impact of different types of interventions, additional classification of each intervention was conducted using the superstructure put forth by Bearss et al. (2015). Two independent raters categorized each intervention using the superstructure of the parent training classification system in Bearss, Burrell, Stewart, & Scahill & 2015. Coders for the superstructure had acceptable levels of reliability (kappa = 0.78), and discrepancies were resolved by consensus. Coding of the sub-components of the categorization system put forth by Bearss and colleagues (e.g., parent training for core symptoms; parent training for maladaptive behaviors, parent support via psychoeducation) proved to be unreliable, likely due to the wide variability of different sub-targets of each intervention.
Data Analysis
After sample and intervention characteristics where extracted, effect sizes were calculated, represented as Cohen’s d, to reflect the impact of the experimental intervention on parent outcomes relative to control. Outcome measures were reverse coded such that higher scores indicated more favorable outcomes. Statistical analysis was conducted using R version 3.4.3 software using the Metafor package (Viechtbauer, 2010). When within-group Cohen’s d statistics were reported, they were extracted and entered into the study database, along with sample size and other study characteristics. For studies that reported raw means and standard deviations of pre- and post-intervention outcomes, within-group Cohen’s d statistics were calculated for each parent outcome measured based on the formula:
Subsequently, between-group Cohen’s d statistics were calculated by subtracting the control group Cohen’s d from the treatment group Cohen’s d.
One study reported outcomes in terms of betas. Betas were transformed to r with the formula used by Peterson & Brown (2005):
Then, Cohen’s d was calculated from r using the formula:
When F statistics were reported for parent outcomes (k = 2, NES = 3), Cohen’s d was calculated by first taking the square root of F and then transforming from t to Cohen’s d using established methods (Cohen, 1988). Studies that did not provide any statistical information regarding parent outcomes, yet explicitly stated in the manuscript that parent outcomes were not significantly different between the experimental group and control (k = 2, NES = 7) were assigned a p-value of 0.50 (Rosenthal, 1995). For these studies, as well as any study that reported outcomes in terms of p-values (k = 2, NES = 3), p-values were first transformed to r using the formula:
where Z is the standard normal deviate that corresponds to the p-value (Rosenthal, 1995, p. 33). Cohen’s d was then calculated from r using the formula reported above.
Random-effects meta-analytic models were conducted on extracted and converted effect sizes to examine the average pooled effect of parental intervention versus control on parent outcomes. Since a single study could examine multiple outcome domains and therefore contribute multiple effect sizes, study was used as a nesting factor in these random-effects models to account for dependency among effect sizes. All meta-analytic results were estimated using the inverse variance weight of the effect size, to provide greater weight to studies with better precision and larger sample sizes. Separate meta-analytic models were constructed across the entire pool of effect sizes, and within each outcome domain examined.
Heterogeneity was assessed by estimating Q and I2 statistics, which provided overall estimates of between-study heterogeneity (Q) as well as a quantification of the extent to which heterogeneity may impact meta-analytic results (I2) (Cochran, 1954; Higgins & Thompson, 2002; Higgins et al., 2003). In traditional meta-analytic methods, Cochran’s Q is used to compute I2, as I2 reflects a percentage of variance that is due to heterogeneity (Q) (Higgins et al., 2003). However, in multilevel models, where individual studies may report more than one effect size, this approach is not sufficient, as it only provides a between-study variance estimate. Recent efforts have been made to develop approaches to calculate within-study I2 statistics for multilevel meta-analyses. We used the method outlined in Nakagawa and Santos (2012) and Sutton et al. (2011) to calculate both between- (\(I_{s}^{2}\)) and within-study (\(I_{u}^{2}\)) estimates of heterogeneity.
Meta-regression analyses were used to investigate potential moderators of intervention efficacy on parent outcomes. Rosenthal fail safe N analyses were conducted to examine the potential impact of publication bias (i.e. the greater likelihood that interventions with positive effects are published) on the estimated effect sizes on parent outcomes.
Results
Systematic Literature Search
Figure 1 depicts the literature search, screening, and analysis process. A total of 37 studies met inclusion criteria and examined the effect of interventions on psychological, emotional, and/or family outcomes of parents for children with ASD. Across these studies, 124 total effect sizes were extracted. Included interventions and key intervention characteristics are shown in Table 1.
Sample Characteristics
A total of 1657 parents with a mean age of 38.74 years were included across the 37 studies (SD = 4.99, range = 33.64–49.99 years). Mean age for children across the studies was 5.32 years (SD = 3.64, range = 1.77–18.19). Most parents were female (94.40%) and most of the parents’ children (80.50%) were male. A total of 19 (51%) studies reported participant racial or ethnic identification. In regards to ethnicity, 8 studies were completed internationally among various ethnic groups: 2 studies were completed with Indian parents, 2 studies with Japanese parents, 2 with Hispanic/Latinx parents, 1 with Korean parents, and 1 with Saudi Arabian parents. Of the 7 studies that measured parent race, 77.24% of participants identified as white. Of the 4 studies that did not provide measures of parent race, but provided measures of child race, 72.78% of participants identified as white. Total sample sizes ranged from 11 to 112 participants (M = 45.05; SD = 26.41). About half of the interventions (k = 19, 51.35%) had total sample sizes greater than 40.
Outcomes Assessed
The most frequently measured parent outcome was stress (NES = 47), followed by confidence in the parenting role (NES = 35), mental health (NES = 27), caregiving burden (NES = 6), family adjustment (NES = 4), and physical health (NES = 4),
Intervention Characteristics
Purpose of the Intervention
Over half of the included studies (k = 21, NES = 81) were parent support interventions, while the remaining studies (k = 16; NES = 43) were investigations of parent implementation interventions. Parent support interventions included those that provided information on topics relevant to caring for an individual with ASD. For example, parent support interventions included information on at least one of the following topics: psychoeducation, including information about ASD, associated characteristics, navigation of care systems, and available resources, psychological support for the parent, such as education on coping and stress management strategies, information on enhancing the development of adaptive skills, such as communication, social skills, or feeding, and behavioral management strategies. Parent implementation interventions included those interventions that provided skills training to help parents facilitate development in social behavior or communication or reduce maladaptive behaviors. For example, several included parent implementation studies investigated Parent–Child Interaction Therapy, an intervention that aims to teach parents child-directed play skills as well as effective discipline techniques in an effort to reduce conflict and improve the parent–child relationship (Ginn et al., 2017; Scudder et al., 2019; M. Solomon et al., 2008). Other parent implementation interventions, such as Play and Language for Autistic Youngsters (PLAY) project and Hanen’s More Than Words (HMTW) taught parents how to identify initiation and social cues from their children during play and other daily routines and then respond in ways that encourage the development of communication skills (Lieberman-betz et al., 2014; Solomon et al., 2014). Other included parent implementation interventions taught behavioral strategies. For example, the Autism MEAL (Manage Eating Aversions and Low intake) Plan taught parents selective ignoring, reinforcing, prompting, and task chaining in order to reduce feeding problems and the Functional Behavior Skills Training (FBST), taught parents behavioral strategies adopted from Applied Behavioral Analysis (ABA) such as prompting, reinforcement, and task analysis to teach their children functional behavior skills, such as making requests and eating at the table (Reitzel et al., 2013; Sharp et al., 2014).
Setting, Duration, Frequency and Session Time
Total intervention duration ranged from 2 weeks to 51.96 weeks (approximately one year) with a mean of 12.00 (SD = 11.66) weeks. Less than one third of included studies (k = 11) reported total number of sessions. These interventions ranged from 2 to 24 sessions, with a mean of 9.7 sessions (SD = 5.47). Over half (k = 23) of the included interventions reported treatment frequency. Of those, 15 interventions were delivered weekly, three interventions were delivered every other week, two interventions were delivered monthly and three interventions were delivered with a variable frequency across participants. Of the studies that reported treatment setting (k = 27), most interventions (k = 12) were conducted in a clinic or university, seven were conducted in the homes of participants, four included a combination of in-home and clinic settings, and four interventions were conducted at a variety of different settings, including in-home, clinic, and other community settings (e.g. daycare, conference centers, etc.).
Effects on Parental Outcomes
We began our meta-analysis by first examining the effect of interventions on parent outcomes overall. Table 2 shows that there was a small, but significant impact of existing interventions on parent outcomes (d = 0.29, p < 0.001). Cochran’s Q indicated significant heterogeneity between studies (Q = 401.08, p < 0.001). I2 statistics indicated that the percentage of variance attributable to heterogeneity was low between studies and low-to-moderate within studies, according to cutoffs suggested by Higgins et al. (2003). We then examined the effect of interventions across the six different outcome domains (caregiving burden, confidence in the parenting role, family adjustment, mental health, physical health, and stress) and the two types of interventions (parent implementation and parent support). As shown in Table 2, the overall effect was driven primarily by improvements in confidence in the parenting role (d = 0.49, p < 0.001) and mental health (d = 0.37, p = 0.002). There were no significant observed effects of parent interventions on caregiving burden, family adjustment, physical health, or stress. Effects on outcomes were modest for both parent implementation (d = 0.24) and parent support interventions (d = 0.33). Significant heterogeneity was observed in the confidence, mental health, and stress domains. Examination of I2 statistics indicated that confidence in the parenting role and mental health outcomes were characterized by low and moderate-to-high within-study heterogeneity respectively (confidence: \(I_{W}^{2}\) = 37.87%; mental health: \(I_{W}^{2}\) = 71.69%). Additionally stress outcomes were characterized by moderate-to-high between-study heterogeneity (\(I_{B}^{2}\) = 71.07%). Neither parent support nor parent implementation interventions were characterized by concerning levels of between- or within-study heterogeneity, according to I2 statistics.
To further examine the impact of the different types of parent interventions on parent outcomes, the three outcome variables with the most effect sizes (i.e. confidence in the parenting role, mental health, and stress) were separately analyzed by intervention type (parent support and parent implementation). Results showed no significant observed effects of parent support or parent implementation interventions on mental health (z = − 0.57, p = 0.570) or stress (z = − 0.73, p = 0.176). However, there was a significant effect of intervention type on confidence, such that parent support interventions had a significantly larger impact on confidence in the parenting role than parent implementation interventions (z = 2.12, p = 0.034).
Of the 37 studies included, four studies used follow-up measures of parent outcomes post-intervention, which were analyzed for preliminary evidence of intervention durability (Ibañez et al., 2018; Lieberman et al., 2014; Suzuki et al., 2014, Tellegen & Sanders, 2014). One study investigated a parent implementation intervention (Lieberman et al., 2014) and the remaining 3 studies investigated parent support interventions. Outcomes measured were stress (k = 1), mental health (k = 1), and confidence in the parenting role (k = 2). Sample sizes in these studies ranged from 56 to 104. The impact of interventions from pre-intervention to treatment completion was calculated to determine the treatment effect of these four studies on parent outcomes. Results showed an overall positive impact on parent outcomes from pre-intervention to treatment completion (d = 0.41, p = 0.001). However, the overall effect size observed on parent outcomes was not significant at follow-up (d = − 0.10, p = 0.482), suggesting that treatment effects were not maintained among the four studies with follow-up measures. It should be noted that due to the small number of studies analyzed for follow-up, results on intervention durability are highly tentative and should be interpreted with caution.
Significant heterogeneity was found in the overall meta-analysis and in estimated effects by outcome domain and treatment type necessitating further investigation into potential moderators of parental outcomes. We proceeded to examine whether estimated effects were consistent across intervention and sample characteristics by conducting a series of meta-regressions. No significant moderation effects were found for any intervention characteristics (i.e. intervention type, delivery format, duration, and setting) or sample characteristics (sample size, parent age, and child age).
A Rosenthal fail safe N analysis was conducted to investigate the potential impact of unpublished studies of negative findings on the observed effect size estimate on parent outcomes (Rosenthal, 1991). Results revealed that in order to reduce the overall observed effect size on parental outcomes to non-significant levels, there would need to be an additional 6561 unpublished studies of null findings regarding intervention efficacy on parental outcomes. Fail safe N analyses were also conducted for both intervention categories: parent support and parent implementation. The fail-safe N was 3306 for parent support interventions. Comparatively, the fail safe N for parent implementation interventions was 513, indicating that there would need to be a relatively small number of additional unpublished studies of null findings in order to reduce observed effect sizes on parental outcomes to non-significant levels. Such findings suggest that the effect size for parent support interventions is less susceptible to publication bias than parent implementation interventions.
Discussion
The impact of parent interventions on child outcomes is well established (Ginn et al., 2017; Hansen et al., 2017; Howard et al., 2018; Iadarola et al., 2018; Postorino et al., 2017; Tellegen & Sanders, 2014; Zhou et al., 2018). Yet, less is known about the benefits of these interventions for parent outcomes. To examine this issue, we conducted a meta-analytic review of existing interventions for parents of children with ASD in order to examine the extent to which they improved psychological, emotional, and familial outcomes.
Results revealed a small but significant overall effect of interventions on parent outcomes, which was primarily driven by marked improvements in measures of parenting confidence and, to a lesser degree, mental health. There were no significant improvements observed in caregiving burden, family adjustment, physical health, or stress. Effects were small and significant across both parent implementation and parent support interventions; although the effects observed for parent implementation interventions were susceptible to publication bias and should be interpreted with caution. Significant heterogeneity was found in both the overall meta-analysis and in examinations of effects across outcome domains and intervention purpose. However, despite considerable heterogeneity, no systematic moderators were detected.
These findings suggest that existing interventions are effective at teaching caregivers how to better parent their children with ASD, but are not as effective for addressing other poor psychological and emotional outcomes. This is perhaps not surprising, as the majority of interventions in this analysis aimed to transmit skills and/or information that directly relates to the unique challenges involved in parenting a child with ASD. In terms of the known factors that influence parent outcomes, this is certainly justified by the well-established link between child characteristics and poorer outcomes for parents (Hou et al., 2018; Jellett et al., 2015; MacHado Junior et al., 2016). However, it appears that these approaches may not be adequate to provide substantial improvements in stress and family functioning or to reduce mental health problems, physical health symptoms or caregiving burden. This may be due in part to the presence of a wider range of influences of poor parent outcomes that are not adequately addressed in current interventions and approaches. For example, the experience of poorer outcomes among parents has been attributed to a host of factors beyond ASD symptomatology and challenging behavior, such as the lengthy and complex diagnostic process, socioeconomic status and financial burden, identifying, securing, and maintaining appropriate support services, professional and social support, worry about the future, and public stigma (Bones et al., 2019; Bonis, 2016; Prata et al., 2019). Thus, it is possible that the primary targets of existing efforts to improve parent outcomes may be too narrow in scope to confer meaningful benefits to parents beyond parenting confidence. Furthermore, although parent interventions are designed to be delivered to parents of children with ASD, they are typically designed to provide ultimate benefit, whether behaviorally, functionally, to their children with ASD. This is especially true for parent implementation interventions. The findings of the present analysis showed that parent support interventions had a significantly larger positive impact on parenting confidence than parent implementation interventions, which may suggest that the burden of implementing skills-based interventions could potentially outweigh some of the intended benefits for parents. It is important for researchers to consider and further investigate the impact of implementation interventions on what may already be a considerable burden for caregivers of individuals with ASD.
The present analysis also revealed that a more systematic approach to developing and testing parent interventions is needed. The variation in design and content of the interventions was striking. In addition, the content of many included interventions appeared eclectic, covering a wide range of topics and targets. Although some interventions did have strong theoretical roots (e.g. PCIT, Triple P), many of the interventions lacked a clear conceptual model. The Bearss (2015) framework was helpful for categorizing interventions at a broader level, but the ability to further sort interventions into the framework’s sub-categories was unreliable. The Bearss (2015) model was developed in an effort to more clearly define and classify the wide range of available parent interventions and to establish a common language for researchers and clinicians. However, the findings of the present analysis suggest that currently available parent interventions may not cohesively fit within the existing Bearss taxonomy. This may be due to the fact that parent interventions are part of a growing field that is changing consistently, perhaps so much so that the Bearss (2015) taxonomy should be revisited and updated. It is also possible that the Bearss (2015) framework is being underutilized in the parent intervention literature as a theoretical model from which new interventions are developed. Nevertheless, the lack of conceptual coherence across interventions in the present analysis may have contributed to the observed heterogeneity and small observed impact on parent outcomes across studies. The successful development of interventions for parents requires development of and adherence to a fundamental, parent-centered conceptual model to help researchers focus the content and targets of interventions in a way that effectively improves parent outcomes such as stress, mental health, and burden. This may be accomplished by developing new parent interventions that fit within the established Bearss (2015) taxonomy or perhaps by a establishing a new, parent-centered theoretical model that more comprehensively accommodates the wide range of currently available parent interventions. The development of this central conceptual model may also require researchers to consider theoretical frameworks separate from those traditionally used in the development of interventions that provide benefit children with ASD. In developing such parent-centered frameworks, researchers may also consider adopting a strengths-based perspective, emphasizing the positive aspects of parenting a child with ASD and helping parents to identify elements of personal and family growth. Additionally, while the development of more parent-focused interventions is a growing area of study for ASD researchers, more rigorous testing of such interventions is greatly needed.
There are several limitations to note. First, we could not evaluate all potential moderators because many of them were not reported. Sociodemographic factors, such as race/ethnicity, gender, income, child symptom severity and functioning, and child and parent age, as well as intervention characteristics, such as the length of the intervention, number of sessions, and delivery location, were inconsistently reported across studies. In order to meaningfully examine systematic moderators, more consistent reporting of these variables is needed. It is also important to note that the sample was made up predominantly of women, which potentially limits findings to the experiences of mothers. This is particularly important to note given there is evidence to suggest that parenting experiences, mental health, and stress outcomes may be different for fathers of children with autism (see: Davis & Carter, 2008; Hastings et al., 2005; Seymour, 2018); however, the proportion of women in the sample largely reflects the fact that mothers have historically been the predominant caretakers of children with ASD. Additionally, the inability to detect systematic moderators indicates that the substantial amount of observed heterogeneity is driven by variance in methodology. For example, total sample sizes ranged from 11 to 112. Measurement varied considerably, with interventions using a wide range of different instruments within each category. Of note, there was little variance in parental stress measures, with the majority of the 37 studies that included stress measures (k = 15; 60.00%) utilizing the Parenting Stress Index—Short Form (PSI-SF), yet beneficial effects in this area were still not observed. Finally, the findings of this meta-analysis make it difficult to confidently recommend a treatment or approach for improving psychological, emotional, and family outcomes for parents. This is primarily due to the fact that the number of eligible studies was limited with a diverse set of outcomes, further limiting our ability to conduct analyses by both intervention type and outcome type. As a result, the review has instead highlighted the need to conduct more studies of parent interventions with diverse outcomes so that researchers can examine the effects of different intervention types on specific parent outcomes.
Decades of empirical study have produced a wide range of interventions that demonstrate great benefit for behavioral and functional outcomes for children of ASD, including parent interventions. However, parents of children with ASD tend to experience poor outcomes across a wide range of psychological, emotional, and family domains, making them important targets of intervention as well. A growing body of literature investigating the impact of parent interventions on parent outcomes demonstrates that researchers have recognized this need. Yet, findings indicate that the benefit of parent interventions on parent outcomes is modest and more work is needed to develop interventions with more substantial impacts. Future research should focus on developing a conceptual framework for improving parent outcomes and testing interventions that systematically target such factors in order to identify interventions that provide more direct benefit to parents of children with ASD.
References
Abidin, R. R. (1995). Parenting stress index, third edition: Professional manual. Psychological Assessment Resources Inc.
Athari, P., Ghaedi, L., Kosnin, A., & Binti, M. (2013). Mothers’ depression and stress, severity of autism among children and family income. International Journal of Psychological Research, 6(2), 98–106.
Bearss, K., Burrell, T. L., Stewart, L., & Scahill, L. (2015). Parent training in autism spectrum disorder: What’s in a name? Clinical Child and Family Psychology Review, 18(2), 170–182. https://doi.org/10.1007/s10567-015-0179-5
Beck, A. T., Ward, C. H., Mendelson, M., Mock, J., & Erbaugh, J. (1961). An inventory for measuring depression. Archives of General Psychiatry, 4, 561–571.
Beer, M., Ward, L., & Moar, K. (2013). The relationship between mindful parenting and distress in parents of children with an autism spectrum disorder. Mindfulness, 4(2), 102–112. https://doi.org/10.1007/s12671-012-0192-4
Blackledge, J. T., & Hayes, S. C. (2008). Using acceptance and commitment training in the support of parents of children diagnosed with autism. Child & Family Behavior Therapy, 28, 37–41. https://doi.org/10.1300/J019v28n01
Bones, S., Norris, K., & Quinn, M. (2019). Empirical validation of a model predicting depression, anxiety, and stress in parents of children with autism. Clinical Psychologist, 23(3), 249–260. https://doi.org/10.1111/cp.12190
Bonis, S. (2016). Stress and parents of children with autism: A review of literature. Issues in Mental Health Nursing, 37(3), 153–163. https://doi.org/10.3109/01612840.2015.1116030
Bonis, S. A., & Sawin, K. J. (2016). Risks and protective factors for stress self-management in parents of children with autism spectrum disorder: An integrated review of the literature. Journal of Pediatric Nursing. https://doi.org/10.1016/j.pedn.2016.08.006
Brannan, A. M., Heflinger, C. A., & Bickman, L. (1997). The caregiver strain questionnaire: Measuring the impact on the family of living with a child with serious emotional disturbance. Journal of Emotional and Behavioral Disorders, 5(4), 212–222.
Brobst, J. B., Clopton, J. R., & Hendrick, S. S. (2009). The couple’ s relationship. Focus on Autism and Other Developmental Disabilities, 24(1), 38–50. https://doi.org/10.1177/1088357608323699
Cochran, W. G. (1954). The combination of estimates from different experiments. Biometrics, 10(1), 101–129. https://doi.org/10.2307/3001666
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Lawrence Erlbaum Associates Inc.
Davis, N. O., & Carter, A. S. (2008). Parenting stress in mothers and fathers of toddlers with autism spectrum disorders: Associations with child characteristics. Journal of Autism and Developmental Disorders, 38(7), 1278–1291. https://doi.org/10.1007/s10803-007-0512-z
Divan, G., Vajaratkar, V., Cardozo, P., Huzurbazar, S., Verma, M., Howarth, E., Emsley, E., Taylor, R., Patel, C., & Green, J. (2018). The feasibility and effectiveness of PASS plus, a lay health worker delivered comprehensive intervention for autism spectrum disorders: Pilot RCT in a rural low and middle income country setting. Autism Research. https://doi.org/10.1002/aur.1978
Drew, A., Baird, G., Baron-Cohen, S., Slonims, V., Wheelwright, S., Swettenham, J., Berry, B., & Charman, T. (2002). A pilot randomised control trial of a parent training intervention for pre-school children with autism. European Child & Adolescent Psychiatry, 11, 266–272. https://doi.org/10.1007/s00787-002-0299-6
Dun, W., Cox, J., Foster, L., Mische-Lawson, L., & Tanquary, J. (2012). Impact of a contextual intervention on child participation and parent competence among children with autism spectrum disorders: A pretest-posttest repeated-measures design. The American Journal of Occupational Therapy, 66(5), 520–528.
Estes, A., Munson, J., Dawson, G., Koehler, E., Zhou, X.-H., & Abbott, R. (2009). Parenting stress and psychological functioning among mothers of preschool children with autism and developmental delay. Autism, 13(4), 375–387. https://doi.org/10.1177/1362361309105658
Factor, R. S., Swain, D. M., Antezana, L., Muskett, A., Gatto, A. J., Radtke, S. R., & Scarpa, A. (2019). Teaching emotion regulation to children with autism spectrum disorder: Outcomes of the stress and anger management program (STAMP). Bulletin of the Menninger Clinic, 83(3), 235–258. https://doi.org/10.1521/bumc.2019.83.3.235
Falk, N. H., Norris, K., & Quinn, M. G. (2014). The factors predicting stress, anxiety and depression in the parents of children with autism. Journal of Autism and Developmental Disorders, 44(12), 3185–3203. https://doi.org/10.1007/s10803-014-2189-4
Ferraioli, S. J., & Harris, S. L. (2013). Comparative effects of mindfulness and skills-based parent training programs for parents of children with autism: Feasibility and preliminary outcome data. Mindfulness, 4(2), 89–101. https://doi.org/10.1007/s12671-012-0099-0
García-López, C., Sarriá, E., & Pozo, P. (2016). Multilevel approach to gender differences in adaptation in father-mother dyads parenting individuals with autism spectrum disorder. Research in Autism Spectrum Disorders, 28, 7–16. https://doi.org/10.1016/j.rasd.2016.04.003
Ginn, N. C., Clionsky, L. N., Eyberg, S. M., Warner-Metzger, C., & Abner, J.-P. (2017). Child-directed interaction training for young children with autism spectrum disorders: Parent and child outcomes. Journal of Clinical Child and Adolescent Psychology, 46(1), 101–109. https://doi.org/10.1080/15374416.2015.1015135
Gulsrud, A. C., Hellemann, G., Shire, S., & Kasari, C. (2016). Isolating active ingredients in a parent-mediated social communication intervention for toddlers with autism spectrum disorder. Journal of Child Psychology and Psychiatry, 57(5), 606–613. https://doi.org/10.1111/jcpp.12481
Haakonsen Smith, C., Turbitt, E., Muschelli, J., Leonard, L., Lewis, K. L., Freedman, B., Muratori, M., & Biesecker, B. B. (2018). Feasibility of coping effectiveness training for caregivers of children with autism spectrum disorder: A genetic counseling intervention. Journal of Genetic Counseling, 27(1), 252–262. https://doi.org/10.1007/s10897-017-0144-1
Hahs, A. D., Dixon, M. R., & Paliliunas, D. (2019). Randomized controlled trial of a brief acceptance and commitment training for parents of individuals diagnosed with autism spectrum disorders. Journal of Contextual Behavioral Science, 12, 154–159.
Hansen, B. D., Orton, E. L., Adams, C., Knecht, L., Rindlisbaker, S., Jurtoski, F., & Trajkovski, V. (2017). A pilot study of a behavioral parent training in the republic of Macedonia. Journal of Autism and Developmental Disorders, 47(6), 1878–1889.
Hastings, R. P., Kovshoff, H., Brown, T., Ward, N. J., Degli Espinosa, F., & Remington, B. (2005). Coping strategies in mothers and fathers of preschool and school-age children with autism. Autism : THe International Journal of Research and Practice, 9(4), 377–391. https://doi.org/10.1177/1362361305056078
Hayes, S. A., & Watson, S. L. (2013). The impact of parenting stress: A meta-analysis of studies comparing the experience of parenting stress in parents of children with and without autism spectrum disorder. Journal of Autism and Developmental Disorders, 43(3), 629–642. https://doi.org/10.1007/s10803-012-1604-y
Hemdi, A., & Daley, D. (2017). The Effectiveness of a Psychoeducation Intervention delivered via WhatsApp for mothers of children with Autism Spectrum Disorder (ASD) in the Kingdom of Saudi Arabia: A randomized controlled trial. Child: Care, Health and Development 43(6): 933–941
Higgins, J. P. T., & Thompson, S. G. (2002). Quantifying heterogeneity in a meta-analysis. Statistics in Medicine, 21, 1539–1558. https://doi.org/10.1002/sim.1186
Higgins, J. P. T., Thompson, S. G., Deeks, J. J., & Altman, D. G. (2003). Measuring inconsistency in meta-analyses need for consistency. British Medical Journal, 327, 557–560.
Hou, Y. M., Stewart, L., Iao, L. S., & Wu, C. C. (2018). Parenting stress and depressive symptoms in Taiwanese mothers of young children with autism spectrum disorder: Association with children’s behavioural problems. Journal of Applied Research in Intellectual Disabilities, 31(6), 1–9. https://doi.org/10.1111/jar.12471
Howard, A. R. H., Copeland, R., Lindaman, S., & Cross, D. R. (2018). Theraplay impact on parents and children with autism spectrum disorder: Improvements in Affect, Joint Attention, and Social cooperation. International Journal of Play Therapy, 27(1), 56–68. https://doi.org/10.1037/pla0000056
Hwang, Y. S., Kearney, P., Klieve, H., Lang, W., & Roberts, J. (2015). Cultivating mind: Mindfulness interventions for children with autism spectrum disorder and problem behaviours, and their mothers. Journal of Child and Family Studies, 24(10), 3093–3106. https://doi.org/10.1007/s10826-015-0114-x
Iadarola, S., Levato, L., Harrison, B., Smith, T., Lecavalier, L., Johnson, C., Swiezy, N., Bearss, K., & Scahill, L. (2018). Teaching parents behavioral strategies for autism spectrum disorder (ASD): Effects on stress, strain, and competence. Journal of Autism and Developmental Disorders, 48(4), 1031–1040. https://doi.org/10.1007/s10803-017-3339-2
Ibañez, L. V., Kobak, K., Swanson, A., Wallace, L., Warren, Z., & Stone, W. L. (2018). Enhancing interactions during daily routines: A randomized controlled trial of a web-based tutorial for parents of young children with ASD. Autism Research, 111(4), 667–678. https://doi.org/10.1002/aur.1919
Ichikawa, K., Takahashi, Y., Ando, M., Anme, T., Ishizaki, T., Yamaguchi, H., & Nakayama, T. (2013). TEACCH-based group social skills training for children with high-functioning autism: A pilot randomized controlled trial. BioPsychoSocial Medicine, 7(1), 1–8. https://doi.org/10.1186/1751-0759-7-14
Jamison, J. M., Fourie, E., Siper, P. M., Trelles, M. P., George-Jones, J., Buxbaum Grice, A., Krata, J., Holl, E., Shaoul, J., Hernandez, B., Mitchell, L., McKay, M. M., Buxbaum, J. D., & Kolevzon, A. (2017). Examining the efficacy of a family peer advocate model for black and hispanic caregivers of children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 47(5), 1314–1322. https://doi.org/10.1007/s10803-017-3045-0
Jellett, R., Wood, C. E., Giallo, R., & Seymour, M. (2015). Family functioning and behaviour problems in children with autism spectrum disorders: The mediating role of parent mental health. Clinical Psychologist, 19(1), 39–48. https://doi.org/10.1111/cp.12047
Jocelyn, L. J., Casiro, O. G., Beattie, D., Bow, J., & Kneisz, J. (1998). Treatment of children with autism: A randomized controlled trial to evaluate a caregiver-based intervention program in community day-care centers. Developmental and Behavioral Pediatrics, 19(5), 326–334.
Johnson, C. R., Brown, K., Hyman, S. L., Brooks, M. M., Aponte, C., Levato, L., Schmidt, B., Evans, V., Huo, Z., Bendixen, R., Eng, H., Sax, T., & Smith, T. (2019). Parent training for feeding problems in children with autism spectrum disorder: Initial randomized trial. Journal of Pediatric Psychology, 44(2), 164–175. https://doi.org/10.1093/jpepsy/jsy063
Johnston, C., & Mash, E. J. (1989). A measure of parenting satisfaction and efficacy. Journal of Clinical Child Psychology, 18(2), 167–175.
Karst, J. S., Van Hecke, A. V., Carson, A. M., Stevens, S., Schohl, K., & Dolan, B. (2015). Parent and family outcomes of PEERS : A social skills intervention for adolescents with autism spectrum disorder. Journal of Autism and Developmental Disorders, 45, 752–765. https://doi.org/10.1007/s10803-014-2231-6
Kissel, S. D., & Nelson, W. M. (2016). Parents’ perceptions of the severity of their child’s autistic behaviors and differences in parental stress, family functioning, and social support. Focus on Autism and Other Developmental Disabilities, 31(2), 152–160. https://doi.org/10.1177/1088357614537352
Koren, P. E., DeChillo, N., & Friesen, B. J. (1992). Measuring empowerment in families whose children have emotional dis- abilities: A brief questionnaire. Rehabilitation Psychology, 37, 305–321.
Kuravackel, G. M., Ruble, L. A., Reese, R. J., Ables, A. P., Rodgers, A. D., & Toland, M. D. (2018). COMPASS for hope: Evaluating the effectiveness of a parent training and support program for children with ASD. Journal of Autism and Developmental Disorders, 48(2), 404–416. https://doi.org/10.1007/s10803-017-3333-8
Lecavalier, L., et al. (2017). Moderators of parent training for disruptive behaviors in young children with autism spectrum disorder. Journal of Abnormal Child Psychology, 45(6), 1235–1245. https://doi.org/10.1007/s10802-016-0233-x
Lecavalier, L., Pan, X., Smith, T., Handen, B. L., Arnold, L. E., Silverman, L., Tumuluru, R. V., Hollway, J., & Aman, M. (2018). Parent stress in a randomized clinical trial of atomoxetine and parent training for children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 48(4), 980–987. https://doi.org/10.1007/s10803-017-3345-4
Liao, S.-T., Hwang, Y.-S., Chen, Y.-J., Lee, P., Chen, S.-J., & Lin, L.-Y. (2014). Home-based DIR/FloortimeTM intervention program for preschool children with autism spectrum disorders: Preliminary findings. Physical & Occupational Therapy in Pediatrics, 34(4), 356–367. https://doi.org/10.3109/01942638.2014.918074
Lieberman-betz, R. G., Yoder, P., Stone, W. L., Nahmias, A. S., Carter, A. S., Celimli-aksoy, S., & Messinger, D. S. (2014). An illustration of using multiple imputation versus listwise deletion analyses : The effect of Hanen’s ‘“ more than words ”’ on parenting stress. American Journal on Intellectual and Developmental Disabilities, 119(5), 472–486. https://doi.org/10.1352/1944-7558-119.5.472
Lopez, K., Magaña, S., Morales, M., & Iland, E. (2019). Parents taking action: reducing disparities through a culturally informed intervention for latinx parents of children with autism. Journal of Ethnic and Cultural Diversity in Social Work, 28(1), 31–49. https://doi.org/10.1080/15313204.2019.1570890
Lunsky, Y., Fung, K., Lake, J., Steel, L., & Bryce, K. (2017). Evaluation of acceptance and commitment therapy (ACT) for mothers of children and youth with autism spectrum disorder. Mindfulness, 9(4), 1110–1116. https://doi.org/10.1007/s12671-017-0846-3
MacHado Junior, S. B., Celestino, M. I. O., Serra, J. P. C., Caron, J., & Pondé, M. P. (2016). Risk and protective factors for symptoms of anxiety and depression in parents of children with autism spectrum disorder. Developmental Neurorehabilitation, 19(3), 146–153. https://doi.org/10.3109/17518423.2014.925519
MacKay, C., Cox, T., Burrows, G., & Lazzerini, T. (1978). An inventory for the measurement of self-reported stress and arousal. British Journal of Social and Clinical Psychology, 17, 283–284.
Magaña, S., Lopez, K., Salkas, K., Iland, E., Morales, M. A., Garcia Torres, M., Zeng, M. G., & Machalicek, W. (2020). A randomized waitlist-control group study of a culturally tailored parent education intervention for latino parents of children with ASD. Journal of Autism and Developmental Disorders, 50(1), 250–262. https://doi.org/10.1007/s10803-019-04252-1
Mandelberg, F., Cunningham, T., Gorospe, C., & Laugeson, E. A. (2014). Long-term outcomes of parent-assisted social skills intervention for high-functioning children with autism spectrum disorders. Autism : THe International Journal of Research and Practice, 18(3), 255–263. https://doi.org/10.1177/1362361312472403
Manohar, H., Kandasamy, P., Chandrasekaran, V., & Rajkumar, R. P. (2019). Brief parent-mediated intervention for children with autism spectrum disorder: A feasibility study from South India. Journal of Autism and Developmental Disorders, 49(8), 3146–3158. https://doi.org/10.1007/s10803-019-04032-x
Matheny, A., Wachs, T., Ludwig, J., & Phillips, K. (1995). Bringing order out of chaos: Psychometric characteristics of the confusion, hubbub, and order scale. Journal of Applied Developmental Psychology, 16(3), 429–444. https://doi.org/10.1016/0193-3973(95)90028-4
Matson, J. L., Sipes, M., Fodstad, J. C., & Fitzgerald, M. E. (2011). Issues in the management of challenging behaviours of adults with autism spectrum disorder. CNS Drugs, 25(7), 597–606. https://doi.org/10.2165/11591700-000000000-00000
Miller, A., Shen, J., & Mâsse, L. C. (2016). Child functional characteristics explain child and family outcomes better than diagnosis: Population-based study of children with autism or other neurodevelopmental disorders/disabilities. Health Reports, 27(6), 9–18.
Minjarez, M. B., Mercier, E. M., Williams, S. E., & Hardan, A. Y. (2013). Impact of pivotal response training group therapy on stress and empowerment in parents of children with autism. Journal of Positive Behavior Interventions, 15(2), 71–78. https://doi.org/10.1177/1098300712449055
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., & Altman, . (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Medicine, 6(7), e1000097. https://doi.org/10.1371/journal.pmed.1000097
Moody, E. J., Kaiser, K., Sharp, D., Kubicek, L. F., Rigles, B., Davis, J., McSwegin, S., D’Abreu, L. C., & Rosenberg, C. R. (2019). Improving family functioning following diagnosis of ASD: A randomized trial of a parent mentorship program. Journal of Child and Family Studies, 28(2), 424–435. https://doi.org/10.1007/s10826-018-1293-z
Nakagawa, S., & Santos, E. S. A. (2012). Methodological issues and advances in biological meta-analysis. Evolutionary Ecology, 26, 1253–1274. https://doi.org/10.1007/s10682-012-9555-5
Nguyen, C. T., Fairclough, D. L., & Noll, R. B. (2016). Problem-solving skills training for mothers of children recently diagnosed with autism spectrum disorder: A pilot feasibility study. Autism, 20(1), 55–64. https://doi.org/10.1177/1362361314567134
Olsson, M. B., & Hwang, C. P. (2002). Sense of coherence in parents of children with different developmental disabilities. Journal of Intellectual Disability Research, 46(7), 548–559. https://doi.org/10.1046/j.1365-2788.2002.00414.x
Oosterling, I., Visser, J., Swinkels, S., Rommelse, N., Donders, R., Woudenberg, T., Roos, S., van derGaag, R. J., & Buitelaar, J. (2010). Randomized controlled trial of the focus parent training for toddlers with autism: 1-year outcome. Journal of Autism and Developmental Disorders, 40(12), 1447–1458. https://doi.org/10.1007/s10803-010-1004-0
Padden, C., & James, J. E. (2017). Stress among parents of children with and without autism spectrum disorder: A comparison involving physiological indicators and parent self-reports. Journal of Developmental and Physical Disabilities, 29(4), 567–586. https://doi.org/10.1007/s10882-017-9547-z
Picardi, A., Gigantesco, A., Tarolla, E., Stoppioni, V., Cerbo, R., Cremonte, M., Alessandri, G., Lega, I., & Nardocci, F. (2018). Parental burden and its correlates in families of children with autism spectrum disorder: A multicentre study with two comparison groups. Clinical Practice & Epidemiology in Mental Health, 14(1), 143–176. https://doi.org/10.2174/1745017901814010143
Poslawsky, I. E., Naber, F. B., Bakermans-Kranenburg, M. J., Daalen, E., Engeland, H., & Ijzendoorn, M. H. (2015). Video-feedback intervention to promote positive parenting adapted to autism (VIPP-AUTI): A randomized controlled trial. Autism, 19(5), 588–603. https://doi.org/10.1177/1362361314537124
Postorino, V., Sharp, W. G., McCracken, C. E., Bearss, K., Burrell, T. L., Evans, A. N., & Scahill, L. (2017). A systematic review and meta-analysis of parent training for disruptive behavior in children with autism spectrum disorder. Clinical Child and Family Psychology Review. https://doi.org/10.1007/s10567-017-0237-2
Prata, J., Lawson, W., & Coelho, R. (2019). Stress factors in parents of children on the autism spectrum: An integrative model approach. International Journal of Clinical Neurosciences and Mental Health. https://doi.org/10.21035/ijcnmh.2019.6.2
Pugliese, C. E., Ratto, A. B., Granader, Y., Dudley, K. M., Bowen, A., Baker, C., & Anthony, L. G. (2020). Feasibility and preliminary efficacy of a parent-mediated sexual education curriculum for youth with autism spectrum disorders. Autism, 24(1), 64–79. https://doi.org/10.1177/1362361319842978
Radley, K. C., Jenson, W. R., Clark, E., & O’Neill, R. E. (2014). The feasibility and effects of a parent-facilitated social skills training program on social engagement of children with autism spectrum disorders. Psychology in the Schools, 51(3), 241–255. https://doi.org/10.1002/pits.21749
Radloff, L. S. (1977). The CES-D scale: A self report depression scale for research in the general population. Applied Psychological Measurement, 1, 385–401.
Rayan, A., & Ahmad, M. (2017). Effectiveness of mindfulness-based intervention on perceived stress, anxiety, and depression among parents of children with autism spectrum disorder. Mindfulness, 8(3), 677–690. https://doi.org/10.1007/s12671-016-0595-8
Reitzel, J., Summers, J., Lorv, B., Szatmari, P., Zwaigenbaum, L., Georgiades, S., & Duku, E. (2013). Pilot randomized controlled trial of a functional behavior skills training program for young children with autism spectrum disorder who have significant early learning skill impairments and their families. Research in Autism Spectrum Disorders, 7(11), 1418–1432. https://doi.org/10.1016/j.rasd.2013.07.025
Rezendes, D. L., & Scarpa, A. (2011). Associations between parental anxiety/depression and child behavior problems related to autism spectrum disorders: The roles of parenting stress and parenting self-efficacy. Autism Research and Treatment, 2011, 1–10. https://doi.org/10.1155/2011/395190
Rivard, M., Morin, M., Mercier, C., Terroux, A., Mello, C., & Lépine, A. (2017). Social validity of a training and coaching program for parents of children with autism spectrum disorder on a waiting list for early behavioral intervention. Journal of Child and Family Studies, 26(3), 877–887. https://doi.org/10.1007/s10826-016-0604-5
Rollins, P. R., John, S., Jones, A., & De Froy, A. (2019). Pathways early ASD intervention as a moderator of parenting stress on parenting behaviors: A randomized control trial. Journal of Autism and Developmental Disorders, 49(10), 4280–4293. https://doi.org/10.1007/s10803-019-04144-4
Rosenthal, R. (1991). Meta-analytic procedures for social research. Sage. https://doi.org/10.4135/9781412984997
Rosenthal, R. (1995). Writing meta-analytic reviews. Psychological Bulletin, 118(2), 183–192. https://doi.org/10.1037/0033-2909.118.2.183
Scahill, B., et al. (2016). Effect of parent training on adaptive behavior in children with autism spectrum disorder and disruptive behavior: Results of a randomized trial. Journal of the American Academy of Child and Adolescent Psychiatry, 55(7), 602-609.e3. https://doi.org/10.1016/j.jaac.2016.05.001
Scarpa, A., & Reyes, N. M. (2011). Improving emotion regulation with CBT in young children with high functioning autism spectrum disorders: A pilot study. Behavioural and Cognitive Psychotherapy, 39(4), 495–500. https://doi.org/10.1017/S1352465811000063
Scudder, A., Wong, C., Ober, N., Hoffman, M., Toscolani, J., & Handen, B. L. (2019). Parent–child interaction therapy (PCIT) in young children with autism spectrum disorder. Child and Family Behavior Therapy, 41(4), 201–220. https://doi.org/10.1080/07317107.2019.1659542
Seymour, M., Giallo, R., & Wood, C. E. (2018). Bio-ecological factors associated with the psychological distress of fathers of children with autism spectrum disorder: A population-based study of Australian families. Autism : THe International Journal of Research and Practice, 22(7), 825–836. https://doi.org/10.1177/1362361317709971
Sharp, W. G., Burrell, T. L., & Jaquess, D. L. (2014). The Autism MEAL Plan: A parent-training curriculum to manage eating aversions and low intake among children with autism. Autism, 18(6), 712–722. https://doi.org/10.1177/1362361313489190
Shire, S. Y., Goods, K., Shih, W., Distefano, C., Kaiser, A., Wright, C., Mathy, P., Landa, R., & Kasari, C. (2015). Parents’ adoption of social communication intervention strategies: Families including children with autism spectrum disorder who are minimally verbal. Journal of Autism Developmental Disorders, 45, 1712–1724. https://doi.org/10.1007/s10803-014-2329-x
Siller, M., Hutman, T., & Sigman, M. (2012). A parent-mediated intervention to increase responsive parental behaviors and child communication in children with ASD: A randomized clinical trial. Journal of Autism and Developmental Disorders, 43(3), 540–555. https://doi.org/10.1007/s10803-012-1584-y
Sivberg, B. (2002). Coping strategies and parental attitudes, a comparison of parents with children with autistic spectrum disorders and aprents with non-autistic children. International Journal of Circumpolar Health, 61(sup2), 36–50.
Skinner, H. A., Steinhauer, P. D., & Santa-Barbara, J. (1983). The family assessment measure. Canadian Journal of Community Mental Health, 2(2), 91–105. https://doi.org/10.7870/cjcmh-1983-0018
Snow, M., & Donnelly, J. (2016). Factors mediating dysphoric moods and help seeking behaviour among Australian parents of children with autism. Journal of Autism and Developmental Disorders, 46(6), 1941–1952. https://doi.org/10.1007/s10803-016-2725-5
Solomon, M., Ono, M., Timmer, S., & Goodlin-Jones, B. (2008). The effectiveness of parent—child interaction therapy for families of children on the autism spectrum. Journal of Autism and Developmental Disorders, 38, 1767–1776. https://doi.org/10.1007/s10803-008-0567-5
Solomon, R., Van Egeren, L. A., Mahoney, G., Quon Huber, M. S., & Zimmerman, P. (2014). PLAY project home consultation intervention program for young children with autism spectrum disorders : A randomized controlled trial. Journal of Developmental and Behavioral Pediatrics, 35(8), 475–485.
Spielberger, C. D., Gorsuch, R. L., Lushene, R., Vagg, P. R., & Jacobs, G. A. (1983). Manual for the state-trait anxiety inventory. Consulting Psychologists Press.
Sutton, J. T., Nakagawa, S., Robertson, B. C., & Jamieson, I. G. (2011). Disentangling the roles of natural selection and genetic drift in shaping variation at MHC immunity genes. Molecular Ecology, 20, 4408–4420. https://doi.org/10.1111/j.1365-294X.2011.05292.x
Suzuki, M., Yamada, A., Watanabe, N., Akechi, T., Katsuki, F., Nishiyama, T., Imaeda, M., Miyachi, T., Otaki, K., Mitsuda, Y., Ota, A., & Furukawa, T. A. (2014). A failure to confirm the effectiveness of a brief group psychoeducational program for mothers of children with high-functioning pervasive developmental disorders : A randomized controlled pilot trial. Neuropsychiatric Disease and Treatment, 10(1), 1141–1153.
Tarver, J., Palmer, M., Webb, S., Scott, S., Slonims, V., Simonoff, E., & Charman, T. (2019). Child and parent outcomes following parent interventions for child emotional and behavioral problems in autism spectrum disorders: A systematic review and meta-analysis. Autism : THe International Journal of Research and Practice, 23(7), 136236131983004–1644. https://doi.org/10.1177/1362361319830042
Taylor, J. L., Hodapp, R. M., Burke, M. M., Waitz-Kudla, S. N., & Rabideau, C. (2017). Training parents of youth with autism spectrum disorder to advocate for adult disability services : Results from a pilot randomized controlled trial. Journal of Autism and Developmental Disorders, 47(3), 846–857. https://doi.org/10.1007/s10803-016-2994-z
Tellegen, C. L., & Sanders, M. R. (2014). A randomized controlled trial evaluating a brief parenting program with children with autism spectrum disorders. Journal of Consulting and Clinical Psychology, 82(6), 1193–1200.
Tomeny, T. S. (2017). Parenting stress as an indirect pathway to mental health concerns among mothers of children with autism spectrum disorder. Autism: The International Journal of Research and Practice, 21(7), 907–911. https://doi.org/10.1177/1362361316655322
Tonge, B., Brereton, A., Kiomall, M., Mackinnon, A., & Rinehart, N. J. (2014). A randomised group comparison controlled trial of “preschoolers with autism”: A parent education and skills training intervention for young children with autistic disorder. Autism : THe International Journal of Research and Practice, 18(2), 166–177. https://doi.org/10.1177/1362361312458186
Turner-Brown, L., Hume, K., Boyd, B. A., & Kainz, K. (2019). Preliminary efficacy of family implemented TEACCH for toddlers: Effects on parents and their toddlers with autism spectrum disorder. Journal of Autism and Developmental Disorders, 49(7), 2685–2698. https://doi.org/10.1007/s10803-016-2812-7
Venker, M., McDuffie, A., Weismer, S. E., & Abbeduto, L. (2011). Increasing verbal responsiveness in parents of children with autism: A pilot study. Autism, 16(6), 568–585. https://doi.org/10.1177/1362361311413396
Wang, J., Hu, Y., Wang, Y., Qin, X., Xia, W., Sun, C., Wu, L., & Wang, J. (2013). Parenting stress in Chinese mothers of children with autism spectrum disorders. Social Psychiatry and Psychiatric Epidemiology, 48(4), 575–582. https://doi.org/10.1007/s00127-012-0569-7
Ware, J. E., Jr., & Sherbourne, C. D. (1992). The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Medical Care, 30(6), 473–483.
Warfield, M. E., Chiri, G., Leutz, W. N., & Timberlake, M. (2014). Family well-being in a participant-directed autism waiver program: The role of relational coordination. Journal of Intellectual Disability Research, 58(12), 1091–1104. https://doi.org/10.1111/jir.12102
Welterlin, A., Turner-Brown, L. M., Harris, S., Mesibov, G., & Delmolino, L. (2012). The home TEACCHing program for toddlers with autism. Journal of Autism and Developmental Disorders, 42, 1827–1835. https://doi.org/10.1007/s10803-011-1419-2
Whittingham, K., Sofronoff, K., Sheffield, J., & Sanders, M. R. (2009). Stepping stones triple P: An RCT of a parenting program with parents of a child diagnosed with an autism spectrum disorder. Journal of Abnormal Child Psychology, 37(4), 469–480.
Yoo, H. J., Bahn, G., Cho, I. H., Kim, E. K., Kim, J. H., Min, J. W., Lee, W. H., Seo, J. S., Jun, S. S., Bong, G., Cho, S., Shin, M. S., Kim, B. N., Kim, J. W., Park, S., & Laugeson, E. A. (2014). A randomized controlled trial of the Korean version of the PEERS® parent-assisted social skills training program for teens with ASD. Autism Research, 7, 145–161. https://doi.org/10.1002/aur.1354
Zablotsky, B., Anderson, C., & Law, P. (2013). The association between child autism symptomatology, maternal quality of life, and risk for depression. Journal of Autism and Developmental Disorders, 43(8), 1946–1955. https://doi.org/10.1007/s10803-012-1745-z
Zand, D. H., Bultas, M. W., Mcmillin, S. E., Halloran, D., White, T., Mcnamara, D., & Pierce, K. J. (2017). A pilot of a brief positive parenting program on children newly diagnosed with autism spectrum disorder. Family Process, 57(4), 901–914. https://doi.org/10.1111/famp.12334
Zarit, S. H., Reever, K. E., & Back-Peterson, J. (1980). Relatives of the impaired elderly: Correlates of feelings of burden. The Gerontologist, 20, 649–655.
Zhou, B., Xu, Q., Li, H., Zhang, Y., Wang, Y., Rogers, S. J., & Xu, X. (2018). Effects of parent-implemented early start denver model intervention on chinese toddlers with autism spectrum disorder: A non-randomized controlled trial. Autism Research, 11(4), 654–666.
Zlomke, K. R., Jeter, K., & Murphy, J. (2017). Open-trial pilot of parent-child interaction therapy for children with autism spectrum disorder. Child & Family Behavior Therapy, 39(1), 1–18. https://doi.org/10.1080/07317107.2016.1267999
Funding
The authors received no specific funding for this work. The study was conducted without grant or financial support.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Author contributions
KTM had the idea for the review and both authors contributed to its design. The literature search was performed by KTM. Data analysis was performed by KTM and SME. The first draft of the manuscript was written by KTM and both authors critically revised the manuscript. Both authors read and approved the final manuscript.
Conflict of interest
The authors declare that they have no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
MacKenzie, K.T., Eack, S.M. Interventions to Improve Outcomes for Parents of Children with Autism Spectrum Disorder: A Meta-Analysis. J Autism Dev Disord 52, 2859–2883 (2022). https://doi.org/10.1007/s10803-021-05164-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-021-05164-9