
Abstract
We previously reported a 2 × 2 randomized clinical trial of atomoxetine (ATX) and parent training (PT) for attention deficit hyperactivity disorder (ADHD) symptoms and behavioral noncompliance in 128 children with autism spectrum disorder, ages 5–14 years. Children were randomized to one of four conditions: ATX alone, placebo alone, ATX + PT, or PT + placebo. Both ATX and PT improved some indices of ADHD and behavioral compliance. In this report, we describe parent stress over time and across conditions. All four treatments improved parent self-rated stress from baseline to week 10. However, there were no statistically significant differences between treatment groups. Significantly more improvement in parent stress scores was observed for clinical responders than non-responders.
ClinicalTrials.gov Title: Atomoxetine, Placebo and Parent Management Training in Autism (Strattera) ClinicalTrials.gov Identifier: NCT00844753.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
A significant proportion of children with autism spectrum disorder (ASD) present with behavior and emotional problems (Kanne and Mazurek 2011; Lecavalier 2006). Disruptive behavior disorders are especially common. Approximately 25% of children with ASD meet diagnostic criteria for either oppositional defiant disorder (ODD) or conduct disorder (CD) (Kaat and Lecavalier 2013). Rates of ADHD appear to be higher (Gadow et al. 2005; Leyfer et al. 2006; Simonoff et al. 2008).
Parents of children with ASD report high levels of stress (Karst and Van Hecke 2012; Hayes and Watson 2013). The stress seems exacerbated by the presence of comorbid externalizing behavior problems (Baker et al. 2003; Lecavalier et al. 2006). This is not unique to ASD. In their meta-analysis on parent stress in children with ADHD, Theule et al. (2012) found that severity of ADHD and symptoms of externalizing behaviors such as non-compliance and aggression were significant predictors of parent stress.
It is widely believed that interventions targeting core features of ASD or behavior problems will have the added advantage of reducing parent stress. Despite this belief, there are few data on this topic in children with ASD, and these data are difficult to interpret because of limitations in study design or small sample sizes. In one of the few larger controlled trials, Tonge et al. (2006) reported that parents of young children newly diagnosed with ASD (n = 105) improved on the General Health Questionnaire with 20 weeks of parent education and either counseling or behavior management training, relative to a nonintervention control group. Recently, Iadarola et al. (2017) reported improvements in parental competence and reductions in parent stress and strain in a randomized clinical trial (RCT) with 180 young children with ASD and disruptive behaviors. Benefits were seen in both the parent training (PT) condition and an active comparator, but were significantly greater in PT.
Several studies have reported on the impact of interventions to reduce parent stress in children with ADHD and other disruptive behaviors (Lundahl et al. 2006). In the largest study of its kind (n = 579 randomized to one of four conditions and followed over 14 months), the Multimodal Treatment Study of ADHD (MTA) failed to find differences between groups on the Parenting Stress Index (PSI) (Wells et al. 2000). Similarly, Abikoff et al. (2007) examined PSI scores in a 4-week trial of methylphenidate in 114 preschoolers with ADHD. There was no significant difference in the PSI ratings of parents of children in the methylphenidate and placebo groups, with mean total scores decreasing in both groups from baseline to end of study. Van Den Hoofdakker et al. (2007) reported on parent stress in a 5-month effectiveness study of PT in 94 children with ADHD. Although the PT enhanced the effectiveness of routine treatment of children on some variables, it did not reduce ADHD symptoms or parent stress on the PSI. Reductions in parenting stress were comparable in both treatment groups, with only trivial-to-small effect sizes.
We recently reported a 10-week 2 × 2 RCT of individual and combined treatment with atomoxetine (ATX) versus placebo and PT vs no PT for ADHD symptoms and behavioral noncompliance in 128 children with ASD. This study represented an opportunity to examine the differential impact of PT, medicine, and their combination on parent stress. Aiming to add to the limited literature on PT and parent stress in ASD, our first research question addressed whether we would observe changes in parent stress in this large sample and, if so, whether the changes would differ among the four treatment groups. We hypothesized that scores would decline across all groups but that the decline would be smaller in the placebo group compared to the active treatment groups (ATX, PT, or both). Our second research question asked whether clinical responder status at the end of the study would be associated with change in parent stress. With the supposition that decreases in parent stress would accompany decreases in disruptive behavior, we hypothesized positive clinical responders would have bigger reductions than nonresponders in parent stress from baseline to study end point.
Method
Procedures
We previously described the background, methods, and week 10 results of this clinical trial (Handen et al. 2015). Briefly, the study was a three-site, randomized, parallel-groups, placebo-controlled trial of 128 children with ASD and ADHD, age 5–14 years. Randomization was stratified by site in equal numbers to one of four conditions (32 in each condition): ATX + PT, ATX-alone, PT + Placebo, or Placebo-alone, and balanced by mental age (MA < 6 years vs. > 6 years). During the acute trial, ATX assignment was double-blind and PT assignment was single-blind: known by only the family, behavior therapist, and study coordinator, while other study personnel, including staff raters, remained blinded. Visits initially occurred weekly to assess medication response, monitor adverse events and adjust doses. Final dose adjustments were made at week 6, with subsequent monitoring at weeks 8 and 10. Families assigned to PT met weekly for up to nine one-to-one sessions with a clinician for 60 to 90 min. Variations of the PT manual, which three of the authors of this article helped develop, were used in two prior RCTs of children with ASD and behavioral problems. The PSI (described below) was completed at baseline and at the end of the 10 weeks. For patients who terminated early, the PSI was completed at the last visit.
At Week 10, participants were considered ADHD Responders (having a favorable ADHD outcome) if they received a Clinical Global Impressions—Improvement (CGI—I) rating of 1 or 2 (much or very much improved) for ADHD symptoms by a blinded evaluator and ≥ 30% decrease on the ADHD subscale of the parent-rated Swanson, Nolan, and Pelham Scale Fourth Edition (SNAP-IV). Participants were classified as Noncompliance Responders (achieving a favorable noncompliance outcome) if they received a CGI-I Improvement rating of 1 or 2 for Noncompliance by the blinded evaluator and ≥ 30% decrease on the mean severity score on the Home Situations Questionnaire—PDD version (described below). All procedures were approved by each institution’s IRB.
Participants
Participants were 128 children, age 5.0 to 14.11 years, with a mental age > 24 months, based upon either the Stanford-Binet—5th Edition (Roid 2003) or Mullen Scales of Early Learning (Mullen 1995). All participants had an ASD diagnosis based upon the Autism Diagnostic Interview—Revised (Rutter et al. 2003) and expert clinical evaluation that included interview, observation, and DSM-IV-TR checklist (APA 2000). ASD included autistic disorder (n = 57, 44.5% of sample), pervasive developmental disorder not otherwise specified (n = 50, 39.1% of sample), and Asperger’s disorder (n = 21, 16.4% of sample). Participants had to exhibit problematic overactivity and/or inattention at both home and school, defined as mean item score ≥ 1.5 on both the parent- and teacher-completed SNAP-IV as well as CGI-severity score ≥ 4. Participants were enrolled in the study regardless of severity of noncompliance scores. Consequently, not all participants displayed clinically significant noncompliance. Participants had to be free of all psychotropic medications for two weeks prior to randomization. We excluded children with significant psychiatric disorders other than ASD, ADHD, and DBD, medical conditions, or abnormalities on routine laboratory tests and ECG. Table 1 shows participant characteristics. There were no significant differences on demographic variables except for the percentage of children in regular education classrooms, where the placebo group had significantly fewer participants in special education. Importantly, there were no differences across conditions in ASD subtype (p = 0.85). There were also no differences across groups on parent-rated symptoms of ADHD and ODD symptoms (p > 0.84) or on categorical diagnoses (116 of the 128 children met criteria for ADHD combined subtype).
In approximately 90% of cases, the mother provided the ratings. The average age was 39.4 years (SD = 7.0) for mothers and 41.2 years (SD = 8.2) for fathers. There was no association between parental age and PSI change score.
Measures
Parenting Stress Index-Short Form (PSI-SF; Abidin 1995). The PSI was designed to identify potentially dysfunctional parent–child systems. It was derived from the full length PSI and contains 36 items distributed among three subscales with 12 items each: parental distress, parent–child dysfunctional interaction, and difficult child. Items are rated on a 5-point scale ranging from Strongly agree to Strongly disagree. The PSI-SF has good test re-retest reliability and internal consistency. The correlation between the 101- item PSI and the PSI-SF is 0.94 (Abidin 1995).
Clinical Global Impressions (CGI; Guy 1976). The CGI includes scales for severity and improvement. The CGI-Severity (CGI-S) is scored from “1” (normal) to “7” (extremely ill). The CGI-Improvement (CGI-I) score ranges from “1” (very much improved), through “4” (no change), to “7” (very much worse). The CGI was completed by a blinded evaluator based on parent/child interviews, observation, and review of parent and teacher ratings. Separate CGI ratings were obtained for ADHD and noncompliance.
Swanson, Nolan, and Pelham Scale (SNAP-IV; Bussing et al. 2008). The SNAP-IV parent and teacher scales were used to measure ADHD and oppositional symptoms at home and school. The SNAP-IV, ADHD, and ODD sections include the 18 DSM-IV symptoms of ADHD (9 inattention and 9 hyperactive/impulsive items) and 8 symptoms of ODD rated on a 0–3 scale. A mean item score of 1.5 on the parent and teacher SNAP-IV 18-symptom combined ADHD items, or the 9-symptom hyperactive-impulsive items, or the 9-symptom inattentive items served as a study inclusion criterion.
Home Situations Questionnaire-PDD (HSQ-PDD; Chowdhury et al. 2010). The HSQ-PDD was completed by parents to assess noncompliance. Originally developed to assess noncompliance in typically developing children with disruptive behavior, the HSQ was adapted to evaluate behavioral noncompliance in children with ASD. Items are rated on 10-point Likert scales, ranging from 0 to 9. The HSQ has good psychometric properties and is sensitive to treatment effects (Chowdhury et al. 2016; Handen et al. 2015).
Aberrant Behavior Checklist (ABC; Aman et al. 1985a, b) is a 58-item parent-rated measure of behavior problems. Each item is rated on a Likert scale from 0 (not a problem) to 3 (severe in degree). The ABC contains five subscales: (I) irritability (15 items), (II) social withdrawal (16 items), (III) stereotypic behavior (7 items), (IV) hyperactivity/noncompliance (16 items), and (V) inappropriate speech (4 items). The ABC has good psychometric properties in children with ASD (Kaat et al. 2014).
Developmental/Cognitive Functioning. The Stanford-Binet Fifth Edition (SB-V; Roid 2003) or the Mullen Scales of Early Learning (MSEL; Mullen 1995) were used to assess cognitive functioning. The Mullen was administered to children who did not achieve a basal score on the abbreviated SB-V.
Data Analysis
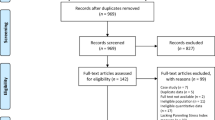
Changes in PSI score over time were analysed using the MIXED procedure in SAS, v9.4 (SAS Institute, Inc., Cary, NC). Model fit and normality assumptions were assessed by examination of residuals. Linear mixed models for repeated measures were used with site (3 levels), treatment group (4 levels), and time x treatment interaction as fixed factors, while subjects were a random factor. Missing data due to early termination of the trial were handled using last observation carried forward. One participant withdrew consent at baseline (no PSI survey collected) and an additional five participants exited the study either before the start of treatment or right after the first visit and did not complete the end-of-study PSI. In all, 99 participants had PSI collected at the end of 10-week treatment. The remaining 23 were collected at weeks 1 (n = 1), 2 (n = 3), 3 (n = 1), 4 (n = 4), 5 (n = 5), 6 (n = 3), and 8 (n = 6). Sensitivity analyses using the missing-at-random assumption for missing data were implemented in the mixed procedure to ensure that conclusions were robust.
We reported the relationship between percent change on the PSI and other clinical measures with Spearman Rank correlations because data were not normally distributed. Percent change was calculated by subtracting the score at baseline from the score at study endpoint and dividing it by the baseline score. Sensitivity analyses were conducted by examining absolute change and percentage change to control for baseline scores. There were no differences in results. Here, we report scores based on percentage change.
Results
Table 2 shows PSI total and subscale scores from baseline to study endpoint for each of the four experimental groups. Overall, the total stress score declined significantly from 98.4 to 91.2 (p < 0.001). Changes in stress scores among the four groups were not significantly different (p = 0.624). Additionally, we looked at the effects of PT alone and in combination with drug versus no PT (ATX + PT and PT + placebo treatment groups vs the ATX alone and placebo alone groups), as well as the effect of ATX alone and in combination with PT versus placebo (ATX + PT and ATX alone versus PT + placebo and placebo alone). There was no statistically significant effect for PT or ATX on parent PSI total score (p = 0.754 and 0.542 respectively). Similar patterns were observed for all three PSI subscales.
Table 3 shows the difference in total and subscale PSI scores from baseline to study endpoint by clinical responder status (i.e., the combination of CGI-Improvement of 1 or 2 + 30% score reduction) for each of the four experimental groups. Both the ADHD and non-compliance response status at the end of the acute phase were associated with significant stress reductions. The 44 ADHD positive responders had a total stress score reduction of 13.6 ± 14.6 points, which was significantly more than the 78 non-responders who saw their total stress score increase slightly (− 3.9 ± 14.0; p = 0.004). Once again, the differences among the four treatment groups were not statistically significant (p = 0.726). Similarly, the 38 non-compliance positive responders saw their total stress scores decline by 15.1 ± 13.0 points, which was significantly more than the 84 non-responders (3.9 ± 14.5; p = 0.001). The differences among the four groups were not statistically significant (p = 0.525) although ATX + PT always had the largest change for noncompliance responders. Finally, we examined the effects of PT alone and in combination with drug (ATX + PT and PT + placebo treatment groups vs the ATX alone and placebo groups), as well as the effect of ATX alone and in combination with PT (ATX + PT and ATX alone vs PT + placebo and Placebo alone). There was no PT effect (p = 0.631) or ATX effect on parent stress (p = 0.950).
Next, we posed the question whether changes in ADHD symptoms, behavioral noncompliance, irritability, or social withdrawal accounted for some or most of the changes observed in parent stress. Table 4 shows Spearman Rank correlations between percent change on PSI total score and percent change on other behavior problem measures (n = 122). All the associations were statistically significant and of similar magnitude, with the ABC Irritability being the most correlated (r = .42) and ABC-Lethargy the least correlated (r = .30).
Finally, we conducted a series of exploratory multiple regressions with stepwise variable selection in an attempt to quantify how much of the change in total parent stress could be accounted for by reported changes in child outcomes. The mother’s education level, treatment group, and percent changes of the child outcomes (HSQ-PDD, ABC subscales, SNAP subscales), were included as dependent variables in the models. Sensitivity analyses were also conducted using the square root transformation of the PSI percent change as a dependent variable. Depending on the combination of variables, R2 was between 0.20 and 0.25. For example, when only the HSQ-PDD was entered in the model, 20% of the variance was accounted for. Adding the remaining variables did not significantly increase R2.
Discussion
Many professionals believe that interventions effective in ameliorating behavior problems may have the added advantage of reducing parent stress. This study provided a good opportunity to examine this question in a large sample of children with ASD and comorbid ADHD receiving PT, ATX, and their combination. Our data showed that PSI scores declined in all four experimental groups. The average total PSI score reduction across conditions was 7.4 points. This corresponds to about one-third SD and a drop of 7% when comparing to the baseline values. This suggests a modest added benefit of the study interventions to parent well-being. Interestingly, there was no statistically significant differentiation among groups, although changes in the placebo group were smaller than the three other groups (PSI total score of − 4.8 for placebo versus − 7.4, for ATX + PT, − 9.0 for ATX alone, and − 8.2 for PT + placebo). Declines in PSI score in all experimental conditions have been reported in a number of trials in children with ADHD without ASD (Wells et al. 2000; Abikoff et al. 2007), as well as in the Iadarola et al. (2017) study of children with ASD. This rather small differentiation between treatment groups and placebo may indicate that treatment effects on parent stress are modest, requiring much larger samples to demonstrate differential effect. It is also a testament to the placebo response, suggesting that meeting regularly with research staff may contribute to lower overall parent stress, independent of treatment or placebo group assignment. If so, it raises the possibility of using regular meetings with paraprofessional volunteers as a support for parents. The lack of specialized effect for PT might also be because symptoms of ADHD might be more challenging to decrease with our current intervention compared to other trials focusing more on disruptive behaviors such as tantrums or aggression. In fact, moderator analyses of a PT trial in preschoolers with ASD and disruptive behaviors revealed that children with significant ADHD symptoms improved much less than their counterparts with fewer ADHD symptoms (Lecavalier et al. 2017).
The duration of the study is of importance when interpreting these results. It is possible that 10 weeks is too brief to allow significant changes to manifest themselves. This might be especially true in the case of PT where more time is needed to learn intervention techniques and make them habitual. In the Iadarola (2017) preschool PT study, the average total PSI score reduction was 8 points after 12 weeks of treatment, and 12 points after 24 weeks of treatment. In addition to the short duration of the trial, attrition likely influenced our findings. Fourteen families dropped out before week 6. One would not expect large effects on parent well-being if little treatment (PT or medicine) was received.
Our hypothesis that positive clinical responders would have important reductions in parent stress was supported. In fact, it is the clinical status at study endpoint that was associated with the largest changes in PSI scores (14 total PSI points for the ADHD responders and 15 total PSI points for the Noncompliance responders). In other words, parents who reported child improvement also reported improvement in their own stress. We can only speculate on causal mechanisms without proper mediation analyses. It could be that reduction in stress increases parent availability to help their child or that improvement in the child’s behavior alleviates parent stress. As with previous analyses, the differences across conditions were not significant, although parent stress scores of ATX + PT noncompliance responders declined twice as much as their counterparts in the Placebo group. The absence of statistical significance is likely due to the large variances and small sample sizes (n = 7 responders in the ATX + PT group and n = 5 responders in the Placebo group).
In an attempt to explore factors associated with stress reduction, we examined reduction in ADHD, behavioral compliance, irritability, and social withdrawal in relation to parent stress reductions. Our measures of child behavior change explained about 20–25% of the changes in parent stress scores. Although this is instructive, it leaves most of the change unexplained.
The two main limitations of our study included our narrow definition of stress and the sample size. The PSI only measures one aspect of parent stress. Nevertheless, it is the most frequently used measure of parent stress, thereby facilitating comparisons across studies. This was one of the largest intervention studies in the ASD field thus far and one of only two to examine a combination of treatments. Nevertheless, only 32 children were randomized to each experimental condition, and lack of statistical power may have undermined detection of treatment effects on parent stress.
In sum, the experience of being in a research study was associated with a reduction in parent stress. Reduction in parent stress was significantly associated with child improvement, but the type of treatment was not critical to the amount of stress reduction. Larger samples are needed for a better understanding of moderating and mediating variables.
References
Abidin, R. R. (1995). Parenting stress index (3rd ed). Odessa, FL: Psychological Assessment Resource.
Abikoff, H. B., Vitiello, B., Riddle, M. A., Cunningham, C., Greenhill, L. L., & …Wigal, T. (2007). Methylphenidate effects on functional outcomes in the preschoolers with attention-deficit/hyperactivity disorder treatment study (PATS). Journal of Child and Adolescent Psychopharmacology, 17, 581–592.
Aman, M. G., Singh, N. N., Stewart, A. W., & Field, C. J. (1985a). Psychometric characteristics of the aberrant behavior checklist. American Journal of Mental Deficiency, 89, 492–502.
Aman, M. G., Singh, N. N., Stewart, A. W., & Field, C. J. (1985b). The Aberrant behavior checklist: A behavior rating scale for the assessment of treatment effects. American Journal of Mental Deficiency, 89, 485–491.
American Psychiatric Association (2000). Diagnostic and Statistical Manual of Mental Disorders-Text Revised, 4th ed.Washington, DC,American Psychiatric Publishing.
Baker, B. L., McIntyre, L. L., Blacher, J., Crnic, K., Edlebrock, C., & Low, C. (2003). Pre-school children with and without developmental delay: Behavior problems and parenting stress over time. Journal of Intellectual Disability Research, 47, 217–230.
Bussing, R., Fernandez, M., Harwood, M., Hou, W., Garvan, C. W., Eyberg, S. M., et al. (2008). Parent and teacher SNAP-IV ratings of attention deficit hyperactivity disorder symptoms: Psychometric properties and normative ratings from a school district sample. Assessment, 15, 317–328.
Chowdhury, M., Aman, M. G., Lecavalier, L., Smith, T., Johnson, C., Swiezy, N., et al. (2016). Factor structure and psychometric properties of the Home Situations Questionnaire for autism spectrum disorder: The Home Situations Questionnaire—Autism Spectrum Disorder. Autism, 20, 528–537.
Chowdhury, M., Aman, M. G., Scahill, L., Sweizi, N., Arnold, L. E., Lecavalier, L., et al. (2010). The Home Situations Questionnaire-PDD Version: Factor structure and psychometric properties. Journal of Intellectual and Disability Research, 54, 281–291.
Gadow, K. D., DeVincent, C. J., Pomeroy, J., & Azizian, A. (2005). Comparison of DSM-IV symptoms in elementary school-aged children with PDD versus clinic and community samples. Autism, 9, 392–415.
Guy, W. (1976). ECDEU assessment manual of psychopharmacology (pp. 218–222). Rockville, MD: National Institute of Mental Health, U.S. Department of Health, Education, and Welfare publication (ADM), Psychopharmacology Research Branch.
Handen, B. L., Aman, M. G., Arnold, L. E., Hyman, S. L., Tumuluru, R. V., Lecavalier, L., et al. (2015). Effects of atomoxetine, parent training, and their combination in children with autism spectrum disorder and ADHD symptoms. Journal of the American Academy of Child and Adolescent Psychiatry, 54, 905–915.
Hayes, S. A., & Watson, S. L. (2013). The impact of parenting stress: A Meta-analysis of studies comparing the experience of parenting stress in parents of children with and without autism spectrum disorder. Journal of Autism and Developmental Disorders, 43, 629–642.
Iadarola, S., Levato, L., Harrison, B., Smith, T., Lecavalier, L., et al. (2017). Teaching parents behavioral strategies for autism spectrum disorder (ASD): Effects on stress, strain, and competence. Journal of Autism and Developmental Disorders. doi:10.1007/s10803-017-3339-2.
Kaat, A. J., & Lecavalier, L. (2013). Disruptive behavior disorders in children and adolescents with autism spectrum disorders: A review of the prevalence, presentation, and treatment. Research in Autism Spectrum Disorders, 7, 1579–1594.
Kaat, A. J., Lecavalier, L., & Aman, M. G. (2014). Validity of the aberrant behavior checklist in children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 44, 1103–1116.
Kanne, S. M., & Mazurek, M. O. (2011). Aggression in children and adolescents with ASD: Prevalence and risk factors. Journal of Autism and Developmental Disorders, 41, 926–937.
Karst, J. S., & Van Hecke, A. V. (2012). Parent and family impact of autism spectrum disorders: A review and proposed model for intervention evaluation. Clinical Child and Family Psychology Review, 15, 247–277.
Lecavalier, L. (2006). Behavior and emotional problems in young people with pervasive developmental disorders: Relative prevalence, effects of subject characteristics, and empirical classification. Journal of Autism and Developmental Disorders, 36, 1101–1114.
Lecavalier, L., Leone, S., & Wiltz, J. (2006). The impact of behavior problems on caregiver stress in young people with autism spectrum disorders. Journal of Intellectual Disability Research, 50, 172–183.
Lecavalier, L., Smith, T., Johnson, C., Bearss, K., Swiezy, N., et al. (2017). Moderators of parent training for disruptive behaviors in young children with autism spectrum disorder. Journal of Abnormal Child Psychology, 45, 1235–1245.
Leyfer, O. T., Folstein, S. E., Bacalman, S., Davis, N. O., Dinh, E., Morgan, J., et al. (2006). Comorbid psychiatric disorders in children with autism: Interview development and rates of disorders. Journal of Autism and Developmental Disorders, 36, 849–861.
Lundahl, B., Risser, H. J., & Lovejoy, M. C. (2006). A meta-analysis of parent training: Moderators and follow-up effects. Clinical Psychology Review, 26(1), 86–104.
Mullen, E. J. (1995). Mullen scales of early learning. Bloomington, MN: Pearson Assessments.
Roid, G. H. (2003). Stanford-Binet intelligence scales (5th ed.). Itasca, IL: Riverside Publishing.
Rutter, M., Le Couteur, A., & Lord, C. (2003). Autism diagnostic interview revised. Torrance, CA: Western Psychological Services.
Simonoff, E., Pickles, A., Charman, T., Chandler, S., Loucas, T., & Baird, G. (2008). Psychiatric disorders in children with autism spectrum disorders: Prevalence, comorbidity, and associated factors in a population-derived sample. Journal of the American Academy of Child and Adolescent Psychiatry, 47, 921–929.
Theule, J., & Wiener, J., Tannock, R., & Jenkins, J. M. (2012). Parenting stress in families of children with ADHD: A meta-analysis. Journal of Emotional and Behavioral Disorders, 21, 3–17.
Tonge, B., Brereton, A., Kiomall, M., Mackinnin, A., King, N., & Rineheart, N. (2006). Effects on parental mental health of an education and skills training program for parents of young children with autism: A randomized controlled trial. Journal of the American Academy of Child and Adolescent Psychiatry, 45, 561–569.
Van Den Hoofdakker, B. J., Van der Veen-Mulder, L., Sytema, S., Emmelkamp, P. M. G., Minderaa, R. B., & Nauta, M. H. (2007). Effectiveness of behavioral parent training for children with ADHD in routine clinical practice: a randomized controlled study. Journal of the American Academy of Child and Adolescent Psychiatry, 46, 1263–1271.
Wells, K. C., Epstein, J. N., Hinshaw, S. P., Conners, C. K., Klaric, J., Abikoff, L. E., et al. (2000). Parenting and family stress treatment outcomes in attention deficit hyperactivity disorder (ADHD): An empirical analysis in the MTA study 1. Journal of Abnormal Child Psychology, 28, 543–553.
Funding
This work was supported by grants from the National Institute of Mental Health to Ohio State University (5R01MH079080), University of Pittsburgh (5R01MH079082-05), and University of Rochester (5R01 MH083247), by Eli Lilly and Co., who provided atomoxetine and placebo, and by the University of Rochester CTSA (UL1 RR024160) and Ohio State University CTSA (UL1TR001070) from the National Center for Research Resources and the National Center for Advancing Translational Sciences of the National Institutes of Health.
Author Contributions
LL participated in design and coordination of current study, participated in analysis, and drafted the manuscript; XP performed the statistical analyses and assisted in drafting the manuscript; TS conceived the original study, participated in its design and coordination, assisted with data interpretation, helped to draft the manuscript; BLH conceived the original study, participated in its design and coordination, assisted with data interpretation, helped to draft the manuscript; LEA conceived the original study, participated in its design and coordination, assisted with data interpretation, helped to draft the manuscript; LS participated in original study, assisted to draft the manuscript; RVT participated in original study, assisted to draft the manuscript; JH participated in original study, assisted to draft the manuscript; MGA conceived the original study, participated in its design and coordination, assisted with data interpretation and helped to draft the manuscript. All authors read and approved the final manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Dr. Aman has received research contracts, consulted with, served on advisory boards, or done investigator training for AMO Pharma, CogState, Inc.; Confluence Pharmaceutica; CogState Clinical Trials, Ltd.; Coronado Biosciences; Forest Research; Hoffman-La Roche; Johnson & Johnson, Lumos Pharma, MedAvante, Inc.; Novartis; Ovid Therapeutics, ProPhase LLC; and Supernus Pharmaceuticals. Dr. Handen has received research support from Lilly, Roche, Curemark, Autism Speaks, NIMH, and NIA. Dr. Arnold has received research funding from Curemark, Forest, Lilly, Neuropharm, Novartis, Noven, Shire, Supernus, Roche, YoungLiving, NIH and Autism Speaks. He has consulted with Gowlings, Neuropharm, Organon, Pfizer, Sigma Tau, Shire, Tris Pharma, and Waypoint. He has been on advisory boards for Arbor, Ironshore, Novartis, Noven, Otsuka, Pfizer, Roche, Seaside Therapeutics, Sigma Tau, Shire, and received travel support from Noven. Dr. Hollway has received research funding from Forest Research Institute, Sunovion Pharmaceuticals, Supernus Pharmaceuticals, Young Living, F. Hoffman-La Roche AG, and Autism Speaks. Drs. Lecavalier, Pan, Smith, Tumuluru, and Silverman, have no conflicts of interest to report.
Informed Consent
Informed consent was obtained from all individual participants who were included in this article.
Research Involving Human Participants
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committees and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Rights and permissions
About this article

Cite this article
Lecavalier, L., Pan, X., Smith, T. et al. Parent Stress in a Randomized Clinical Trial of Atomoxetine and Parent Training for Children with Autism Spectrum Disorder. J Autism Dev Disord 48, 980–987 (2018). https://doi.org/10.1007/s10803-017-3345-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-017-3345-4