
Abstract
In the past 30 years there have been major improvements in the care of children with chronic kidney disease (CKD). The incidence and prevalence of CKD are fairly similar among published studies in spite of marked differences in case definition, suggesting inconsistencies in ascertainment and measurement so that children with moderate CKD are not yet well identified and/or included. Congenital disorders, including congenital anomalies of the kidney and urinary tract (CAKUT) and hereditary nephropathies, are responsible for about two third of all cases of CKD in developed countries while acquired causes predominate in developing countries. Most young children commenced on dialysis, begin on peritoneal dialysis, while older children start with hemodialysis. The predominant form of renal replacement therapy, particularly in high-income countries, is renal transplantation.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
Irreversible kidney damage or so-called chronic kidney disease (CKD) has become a major public health problem worldwide. The adult population has been the subject of extensive epidemiological research [1, 2] but fewer data are available about CKD and end stage kidney disease (ESKD) in children [3]. Despite major scientific advances resulting in substantial improvement in the care of children with CKD, some will still progress and require renal replacement therapy (RRT). ESKD is a devastating disorder causing substantial mortality and morbidity (most notably cardiovascular, cancer and infection), but this is compounded by specific problems which occur in children such as impaired growth and psychosocial adjustment [4], all of which severely impact upon quality of life [5]. Understanding of the epidemiology of CKD in children is required in order to make a precise and early diagnosis, identify preventable or reversible causes of progression, predict prognosis, and aid the counseling of children and their families.
Part I: CKD (Stages I–4)
Definition of CKD
One of the problems when collecting data on the epidemiology of CKD in the pediatric population results from the historical absence of a common definition and well-defined classification of CKD. For example, the ItalKid Project and North American Pediatric Renal Trials and Collaborative Studies (NAPRTCS) defined CKD as having a glomerular filtration rate (GFR) of below 75 ml/min/1.73 m2 [6, 7]. Others based their definition on serum creatinine levels themselves or on other thresholds of GFR [8–10].
In 2002, the National Kidney Foundation’s Kidney Disease Outcomes Quality Initiative (NKF-K/DOQI) published a guideline on CKD, which included a classification system for CKD severity, independent of cause, and applicable to children [11]. The K/DOQI classification system identified five stages of CKD from mild disease (stage 1) to ESKD (stage 6) based primarily on the level of GFR (Table 52.1), and has been revised in 2013. CKD is defined by a presence of kidney damageFootnote 1 (e.g., any structural or functional abnormality involving pathologic, laboratory or imaging findings) for ≥3 months or a GFR <90 ml/min/1.73 m2 for ≥3 months. For children, the same criteria generally apply as for adults with the following exceptions or allowances: (a) the criteria for duration >3 months does not apply to newborns or infants <3 months of age. (b) the criteria of a GFR <90 ml/min/1.73 m2 does not apply to children <2 years of age as neonates are born with a GFR of around 60, which increases to normal values in the first 2 years of life, (c) a urinary total protein or albumin excretion rate above the normal value for age may be substituted for albuminuria ≥30 mg/24 h. (d) all electrolyte abnormalities are to be defined in light of age normative values. For children below 2 years of age, it has been recommended by (NKF-K/DOQI) to closely monitor children with values of GFR more than 1 SD below the mean.
The new classification was widely adopted after its introduction; however, its limitations and possible modifications have been a matter of extensive discussions. Recently the revised (bedside) Schwartz formula was developed [12] and since then many papers have been published on the accuracy and optimal methods to define GFR particularly in early stages of kidney injury [13–15].
Screening for Early CKD
CKD screening and surveillance in adults, either population-based or targeted at risk populations, has become widely advocated and implemented in many countries worldwide, in an attempt to prevent ESKD and the progression of CKD. However, the benefit of screening for early-stage CKD is uncertain [16]. The benefit of such programs in children is even more uncertain [17]. Tests used for CKD screening in children are usually limited to urinary dipstick protein instead of urine albumin/creatinine ratio or on creatinine-based calculation of estimated GFR as recommended for adults. There is also a large variation in the methods used and approaches taken by the different countries, and the findings have shown poor reproducibility [17].
The main studies about screening for CKD in children are summarized in Table 52.2 [25–36]. Mass screening programs to detect CKD in children have been undertaken for many years in several Asian countries such as Japan, Taiwan and Korea [25, 26]. Conversely, screening programs have not been adopted in Europe or Australasia but screening using urine dipsticks have routinely been performed in healthy children for decades in the United States [37]. In 2000, the recommendations from the American Academy of Pediatrics were to screen the urine of preschool children and adolescents [38]. This policy has been revised in 2007 and this practice is no longer recommended [39]. Although a decrease in the incidence of ESKD has been observed in Japan and Taiwan, there is only limited evidence that early detection of kidney injury in children may lead to effective interventions to slow progression of CKD and further reduce the risk of developing ESKD [17]. Furthermore, some studies suggest that a urine dipstick is not a cost-effective strategy for screening in children [40].
Data on detection of early-stage CKD based on estimated GFR derived from serum creatinine concentration in the pediatric population are scarce. In a population-based study from Turkey, the prevalence of children aged 5–18 years with CKD stage 2 and higher was 3 % and the prevalence of CKD as defined by estimated GFR <75 ml/min/1.73 m2 was 0.9 % [41]. In a cross sectional study from Iran, the prevalence of CKD stage 3 and higher among school age children (7–17 years) was 1.7 % according to the updated Schwartz formula [42]. These data simply indicate that a certain proportion of asymptomatic children have CKD, which can be detected by mass screening, and do not constitute reliable evidence that early detection and treatment improves the outcomes for early CKD. Trial data are required showing early intervention is better than intervention when there is clinically evident disease.
Demographics of CKD
There is limited information on the epidemiology of early stages of CKD in children. As CKD is usually asymptomatic in its early stages, providing precise epidemiological data are difficult so CKD in children is likely to be underestimated and underreported. Although some pediatric CKD registries using K/DOQI classification are beginning to emerge, only a few reports on the epidemiology of CKD stages 2–5 in children are available. Due to lack of resources and national renal registries, we know even less about the incidence and prevalence in low income countries. For these countries, data are mostly obtained from reports of major tertiary care referral centers, but the validity of this data is variable.
Europe
The largest population-based study in Europe on the epidemiology of pediatric CKD is the ItalKid project. This study in Italy has been collecting data since 1990 on the epidemiology of childhood CKD, describing the natural history of the disease, and identifying factors that influence its course [6]. So far, nearly 1198 patients have been registered. Other nation-wide European studies are the Serbian CKD registry [21], collecting data on over 336 patients since 2000, the Belgium CKD registry which started in 2001 and has over 143 patients [19], and the data from the Swedish Pediatric Nephrology Association [43]. Also regional studies have taken place in Spain [44], the South-East of the UK [23] and Lorraine in France [8].
Several pediatric nephrology societies from European countries have provided data on the early stages of CKD (Table 52.3). Even though age categories and definition of CKD differed between countries, incidence in Europe was fairly consistent, ranging from 8 to 14 per million age-related population (pmarp) for CKD stages 2–5, and being around 8 pmarp for CKD stage 4–5 (Fig. 52.1). The incidence was highest (17.5 pmarp) in a report from the United Kingdom but the study was hospital-based leading to potential referral filter bias and there may be some uncertainty about the covered geographical area [23].

Reported incidence (pmarp) of CKD in children in Europe
While an increase in incidence since the 1970s was seen in France [8], this was not seen when comparing two time periods in Sweden [9, 43]. Two very recent studies from Serbia and the UK also suggested an increase in incidence in the past 10 years [21, 23]. Prevalence ranged from about 55–60 to 90–95 pmarp in Spain, Italy, UK and Serbia, depending on the clinical definition of CKD that was used in each study.
North America
In Northern America most of the information on CKD derives from two large sources of information namely the North American Pediatric Renal Trials and Collaborative Studies (NAPRTCS) [7] and the Chronic Kidney Disease in Children Prospective Cohort Study (CKiD) [45]. Both studies are collecting data on a voluntary basis and are not population based. Therefore it is not possible to determine the incidence and prevalence of CKD in this region.
Latin America and the Caribbean
In Chile, a national survey of pediatric nephrologists estimated an incidence of CKD (GFR <30 ml/min/1.73 m2) in children aged less than 18 years of 5.7 pmarp and a prevalence of 42.5 pmarp in 1996 [46]. Among these patients, half were on conservative treatment and the others were on RRT. Very similar results were found in Argentina, with an incidence of 6.5 pmarp, but with a lower prevalence (15.4 pmarp) [47]. Fifty-eight percent of this population had ESKD and started with dialysis. In Jamaica, the estimated incidence of CKD was 4.6 pmarp and 28 % of them were already in ESKD, without having access to RRT [48].
A study on the epidemiology of CKD conducted in several Latin American countries (Argentina, Brazil, Chile, Colombia, Mexico, Uruguay, and Venezuela) has shown a wide variation in incidence that ranged from 2.8 to 15.8 new cases pmarp [49]. Also an indirect estimation of the incidence of CKD in Mexico suggested a very high incidence, between 24 and 39 per million inhabitants, for which the differences within Mexico were explained by the level of social deprivation [50]. New projects to collect data in Nicaragua [51] and Guatamala [52] are in progress.
Asia
The estimated prevalence of CKD stage 3–5 among Japanese children in 2010 was 29.8 pmarp [24]. This lower prevalence of pre-dialysis CKD in Japan than in Europe was consistent with the lower prevalence of pediatric ESKD in Japan. Two reports from Vietnam and one from Thailand have suggested an annual incidence of hospitalization for CKD around 5 pmarp, most of patients had already reached ESKD [53–55]. Very little is known about pediatric CKD epidemiology in India and China. A survey conducted in 91 Chinese hospitals found a total of 1658 children aged <15 years with CKD stage 3–5 between 1990 and 2002 which suggests a very low incidence of treated CKD <0.5 pmarp [56]. Patients were referred late with advanced CKD or ESKD in 80 % and in-hospital mortality was as high as 72 % [56]. Additional related information concerning dialysis in India and China can be found in Chap. 62.
Middle East
The referral center for pediatric kidney diseases in Kuwait provided data on children aged 0–15 years with a GFR <50 ml/min/1.73 m2 [10]. The mean incidence was found to be as high as 38 pmarp whereas the prevalence increased from 188 in 1996 to a rate as high as 329 pmarp in 2003. The marked difference in incidence between Kuwaiti children and non-Kuwaiti residents suggested the role of genetic factors [10]. An incidence of 12 pmarp was found in a Turkish survey including children with a GFR <75 ml/min/1.73 m2 [22]. An incidence of 11 pmarp and a prevalence of 51 pmarp have been reported in Jordanian children [57].
Africa
Single center studies from sub-Saharan Africa showed very low incidence of CKD estimated at 1–4 pmarp in Nigeria, Sudan, and South Africa [20, 58–60]. Another single center report from Nigeria, however, found an annual incidence of CKD stage 1–5 of 11 pmarp and a prevalence of 48 pmarp [61], which was much higher than the 1.7 pmarp reported in 2004 [62]. Additional related information concerning dialysis in Africa can be found in Chap. 62.
Causes of CKD
Among adults, the leading causes of CKD are diabetes and hypertension. However, in children the causes of CKD are very different. In the ItalKiD study, congenital causes including congenital anomalies of the kidney and urinary tract (CAKUT) (53.6 %) and hereditary nephropathies (15 %) were the most common (Table 52.4). Glomerulonephritis accounted for 5 % of cases [6]. A fairly similar distribution of causes of CKD was reported in other European countries like the Belgian and Serbian registries [19, 21], in a UK tertiary center [23] (Table 52.2), and in the non-populations based studies like NAPRTCs and CKiD. In Japan, distributions were similar, with the primary causes of CKD among children aged <15 years were CAKUT in 62 %, hereditary nephropathy in 14 % and glomerulonephritis in 5 % [24].
Whereas CAKUT predominated in younger patients, glomerulonephritis was the leading cause in children older than 12 years of age. Causes of CKD vary across races, for example, focal segmental glomerulosclerosis, the main cause of glomerular disease, was three times more common in blacks than in whites (19 compared with 6 %) and especially among black adolescents (35 %) [18].
Because of a dearth of national registries and surveys, estimating the causes of CKD in children in low and middle income countries is difficult. In Turkey and countries in the Middle East, CAKUT is the leading cause of CKD (47–62 %) with a clear predominance of uropathies over hypodysplasia, followed by hereditary nephropathies (17–30 %) [10, 22, 57, 63]. Of note, neuropathic bladder remained an important cause of CKD in Turkey (15 %) while it accounted for about 4 % in Italy and Belgium. These figures may reflect a delay in appropriate urological diagnosis and treatment. In addition, the higher proportion of genetic diseases found in Middle East than in Europe may be explained by a higher prevalence of consanguinity. In contrast, chronic glomerulonephritis is the main reported cause of CKD in various studies from India, Southeast Asia, Latin America and Caribbean area and sub-Saharan Africa with a prevalence ranging from 30 to 60 % [48, 49, 53–55, 58–60, 64]. Studies from a tertiary hospital in Nigeria reported proportions of glomerular disease as high as 90 % [61], but this was not consistant across Nigeria as in other locations rates of 57 % were reported [20]. The high prevalence of glomerulonephritis may be related to a high prevalence of bacterial, viral, and parasitic infections that commonly affect the kidneys in developing countries [65], the lack of kidney biopsy, as well as a different age distribution in the population of these reports.
In general there is a predominance of male gender (male/female ratio ranging from 1.3 to 3.0). This partly reflects the higher incidence of CAKUT in boys than in girls, but has also been reported in the regions with a high rate of glomerulonephritis.
Part II: RRT (CKD Stage 5D and 5T)
Data on RRT for ESKD are typically more robust than for CKD, with the most reliable data from national/international dialysis and transplant registries. Unfortunately not every country has such a registry, not all children are reported to the relevant registry, and some countries with registries do not regularly publish reports. Also, as RRT is expensive not all countries are able to offer RRT to children with ESKD. Approximately 80 % of the children on RRT live in Europe, Japan or the United States.
Dialysis and transplant registries only collect data on treated ESKD; untreated children with ESKD are not captured. However, at least in the developed world, the proportion of children with ESKD who do not receive RRT is likely to be very low [1].
Incidence
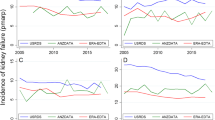
The incidence of RRT, in countries other than the United States, has a mean of around six to nine patients per million age related population ranging from 0 (Malta) to 17 pmarp (Kuwait) [66] (Fig. 52.2). However, given that pediatric RRT is extremely rare, numbers in smaller countries are subject to random error, and even 3-year estimates can give extreme values. In the larger countries, the US incidence is consistently high at around 15.6 per million population (11 in those aged 0–14). In Japan, incidence of pediatric RRT (4.3 pmarp) was consistently much lower than in other high income countries. Variations in incidence may reflect variations in the incidence of CKD, differences in pre-ESKD care or differences in the propensity to treat patients with ESKD.

Incidence of RRT in children aged 0–14 between 2008 and 2011
Among lower income countries the incidence is typically lower, as was shown for the Eastern European countries in the ESPN/ERA-EDTA registry [67, 68], and in previous reports on RRT. In developing countries where RRT is unaffordable for all but the very wealthy, incidence rates are either not available or were extremely low (<1 pmarp in Bangladesh and Nepal). RRT rates vary by the level of funding for healthcare in a country rather than with geographical regions. For example, in other Asian countries, such as Malaysia the incidence is comparable to that of Europe [50]. In South-West Nigeria, a recent study showed that the incidence among children under the age of 14 was 4 pmarp [69], although the median survival was 45 days. Finally Taiwan had an incidence of even 10 pmarp [70]. Some of the variation in incidence may be due to differences in timing that RRT is commenced. In Europe, RRT was generally started at a median GFR of 10.4 ml/min/1.73 m2 whereas mean GFR ranged from 11.3 to 13.6 ml/min/1.73 m2 in the United States [71, 72].
Within-country variations occur by racial group; for example African American and Australian and New Zealand indigenous children have a significantly higher incidence of ESKD than their white counterparts [73]. In the UK, the prevalence and the incidence of RRT in children from the South Asian population in 2008 were 2.5 and 1.5 times greater to that of the Caucasian population aged 0–15 years [74].
There are also large differences between age groups. The incidence has a typical U-shape distribution, with the highest incidence in the preschool children and in adolescents. Consequently registries that include patients up to 20 years of age report higher incidence and prevalence data compared with registries excluding those over the age of 15.
Around 20 % of patients commence RRT with a pre-emptive kidney transplant, a proportion that has been slowly rising. Of the remaining patients, around half commence hemodialysis (HD) and half peritoneal dialysis (PD). The relative proportion of HD and PD is quite variable, presumably reflecting differences in clinician preference and funding models. Treatment at start is also strongly dependent on age; while peritoneal dialysis is the treatment of choice in the majority in young children, this pattern decreases with age, with typically higher rates of HD from the age of 10 onwards [75].
Prevalence
The prevalence of children receiving RRT varies from 56.7 per million population in Australia/New Zealand and the UK, to 89.2 per million in the US (Fig. 52.3). In Malaysia the prevalence was 63 pmarp. A survey conducted in the largest Brazilian State showed a prevalence of 23 pmarp in children less than 18 years [76]. Within Europe there are also large differences, with high income countries reporting prevalence rates or over 55 pmarp and the middle income countries of around 40 pmarp.

Prevalence of RRT in children on 31st of December 2011 (2012 for Australia and New Zealand and Malaysia). The light bar corresponds to the prevalence in children aged 0–14 years, the sum of the light and the dark bars corresponds to the prevalence in children aged 0–19 years. For countries marked with an asterix they might be an underestimation in the oldest 15–19 year olds as they cover pediatric centers only
In many countries the prevalence is rising due to the combination of a fairly steady incidence and improved patient survival on RRT. In the United States, the adjusted annual incidence of ESRD in the pediatric population rose slowly during the 1980s then increased marginally from 14 to 15 pmarp between 1990 and 2011 [33]. In contrast, the adjusted prevalence increased from 60 to 85 in between 1990 and 2011. Similar trends were observed in Australia and New Zealand, where the incidence has remained constant at about 8 pmarp over the past 25 years, while the prevalence of RRT increased from approximately 30–50 pmarp [38]. A report from the ERA-EDTA registry on patients aged 0–19 years starting RRT between 1980 and 2000 in 12 Western European countries showed that the incidence of RRT rose from 7 pmarp in 1980–1984 to 10 pmarp in 1985–1989 and remained stable thereafter [77], while the prevalence increased from 22.9 pmarp in 1980 to 62 pmarp in 2000. The increases in prevalence were explained by improved survival and treatment of younger children, while the prevalence was relatively constant for the pubertal age groups.
Transplantation is by far the most common treatment modality in most countries, accounting for 60–80 % of patients receiving RRT (Fig. 52.4). Here again, differences among countries are substantial. For example, fewer than 10 % of children on RRT are maintained with a kidney transplant in Belarus, compared with over 90 % in Japan and Finland [78]. Recent data show that differences among countries were explained by factors such as the deceased donor rate, the pediatric priority from deceased donor programs, the living donation rate, and healthcare funding models [79]. Compared to adults, children are much more likely to be treated by transplantation due to a combination of fewer comorbidities, higher availability of living donors and, in some cases, preferential allocation of deceased donor kidneys.

Percentage of prevalent children living with a transplant on the 31st of December 2011 (2012 for Australia and New Zealand and Malaysia)
Primary Renal Disease
The causes of ESKD are shown in Table 52.4, and are broadly similar across developed countries. Classification is difficult as each registry categorizes primary renal disease differently, and disease definitions have evolved over time. In most of high income countries congenital anomalies of the urinary tract are the most important cause of ESKD. Usually this accounts for about 50 % of the patients. In low-middle income countries, high proportions of CKD due to glomerulonephritis have been reported, and it is likely that this finding would also apply to the ESKD population [3, 69]. There are also very specific local factors. For example, congenital nephrotic syndrome of the Finnish type, explains the very high prevalence of childhood RRT in Finland.
Conclusion
Although there has been a large increase in the amount of available data about CKD in children, most data are about ESKD and not the earlier stages. As numbers of children are small, more research is needed to improve the understanding for the differences in risk of CKD among countries, and the causes and progression of CKD, in order to prevent ESKD, and to improve the quality of care. A standardized, universally used and reported staging system for CKD, such as the one proposed by KDOQI, and using a standardized approach to age categorization are required. The incidence and prevalence of ESKD is not decreasing and so more research on the complex causal pathways for ESKD is still required.
Notes
- 1.
Kidney damage is defined as pathologic abnormalities or markers of damage including blood or urine tests or imaging studies abnormalities
References
Remuzzi G, Benigni A, Finkelstein FO, Grunfeld J-P, Joly D, Katz I, et al. Kidney failure: aims for the next 10 years and barriers to success. Lancet. 2013;382(9889):353–62.
Eckardt K-U, Coresh J, Devuyst O, Johnson RJ, Kottgen A, Levey AS, et al. Evolving importance of kidney disease: from subspecialty to global health burden. Lancet. 2013;382(9887):158–69.
Harambat J, van Stralen KJ, Kim JJ, Tizard EJ. Epidemiology of chronic kidney disease in children. Pediatr Nephrol. 2012;27(3):363–73.
Shroff R, Weaver DJ, Mitsnefes MM. Cardiovascular complications in children with chronic kidney disease. Nat Rev Nephrol. 2011;7(11):642–9.
Al-Uzri A, Matheson M, Gipson DS, Mendley SR, Hooper SR, Yadin O, et al. The impact of short stature on health-related quality of life in children with chronic kidney disease. J Pediatr. 2013;163(3):736–41.
Ardissino G, Dacco V, Testa S, Bonaudo R, Claris-Appiani A, Taioli E, et al. Epidemiology of chronic renal failure in children: data from the ItalKid project. Pediatrics. 2003;111(4 Pt 1):382–7.
Fivush BA, Jabs K, Neu AM, Sullivan EK, Feld L, Kohaut E, et al. Chronic renal insufficiency in children and adolescents: the 1996 annual report of NAPRTCS. North American Pediatric Renal Transplant Cooperative Study. Pediatr Nephrol. 1998;12(4):328–37.
Deleau J, Andre JL, Briancon S, Musse JP. Chronic renal failure in children: an epidemiological survey in Lorraine (France) 1975–1990. Pediatr Nephrol. 1994;8(4):472–6.
Esbjorner E, Aronson S, Berg U, Jodal U, Linne T. Children with chronic renal failure in Sweden 1978–1985. Pediatr Nephrol. 1990;4(3):249–52.
Al-Eisa A, Naseef M, Al-Hamad N, Pinto R, Al-Shimeri N, Tahmaz M. Chronic renal failure in Kuwaiti children: an eight-year experience. Pediatr Nephrol. 2005;20(12):1781–5.
Eckardt K-U, Berns JS, Rocco MV, Kasiske BL. Definition and classification of CKD: the debate should be about patient prognosis – a position statement from KDOQI and KDIGO. Am J Kidney Dis. 2009;53(6):915–20.
Schwartz GJ, Munoz A, Schneider MF, Mak RH, Kaskel F, Warady BA, et al. New equations to estimate GFR in children with CKD. J Am Soc Nephrol. 2009;20(3):629–37.
Pottel H, Hoste L, Martens F. A simple height-independent equation for estimating glomerular filtration rate in children. Pediatr Nephrol. 2012;27(6):973–9.
Schwartz GJ, Schneider MF, Maier PS, Moxey-Mims M, Dharnidharka VR, Warady BA, et al. Improved equations estimating GFR in children with chronic kidney disease using an immunonephelometric determination of cystatin C. Kidney Int. 2012;82(4):445–53.
Sharma AP, Yasin A, Garg AX, Filler G. Diagnostic accuracy of cystatin C-based eGFR equations at different GFR levels in children. Clin J Am Soc Nephrol. 2011;6(7):1599–608.
Qaseem A, Hopkins RH, Sweet DE, Starkey M, Shekelle P. Screening, monitoring, and treatment of stage 1–3 chronic kidney disease: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2013;159(12):835–47.
Hogg RJ. Screening for CKD in children: a global controversy. Clin J Am Soc Nephrol. 2009;4(2):509–15.
The North American Pediatric Renal Trials and Collaborative Studies 2010 Annual Report. www.naprtcs.org2010.
Mong Hiep TT, Ismaili K, Collart F, Van Damme-Lombaerts R, Godefroid N, Ghuysen M-S, et al. Clinical characteristics and outcomes of children with stage 3–5 chronic kidney disease. Pediatr Nephrol. 2010;25(5):935–40.
Odetunde OI, Okafor HU, Uwaezuoke SN, Ezeonwu BU, Adiele KD, Ukoha OM. Chronic kidney disease in children as seen in a tertiary hospital in Enugu, South-East, Nigeria. Niger J Clin Pract. 2014;17(2):196–200.
Peco-Antic A, Bogdanovic R, Paripovic D, Paripovic A, Kocev N, Golubovic E, et al. Epidemiology of chronic kidney disease in children in Serbia. Nephrol Dial Transplant. 2012;27(5):1978–84.
Bek K, Akman S, Bilge I, Topaloglu R, Caliskan S, Peru H, et al. Chronic kidney disease in children in Turkey. Pediatr Nephrol. 2009;24(4):797–806.
Kim JJ, Booth CJ, Waller S, Rasmussen P, Reid CJD, Sinha MD. The demographic characteristics of children with chronic kidney disease stages 3–5 in South East England over a 5-year period. Arch Dis Child. 2013;98(3):189–94.
Ishikura K, Uemura O, Ito S, Wada N, Hattori M, Ohashi Y, et al. Pre-dialysis chronic kidney disease in children: results of a nationwide survey in Japan. Nephrol Dial Transplant. 2013;28(9):2345–55.
Murakami M, Hayakawa M, Yanagihara T, Hukunaga Y. Proteinuria screening for children. Kidney Int Suppl. 2005;94:23–7.
Lin CY, Sheng CC, Chen CH, Lin CC, Chou P. The prevalence of heavy proteinuria and progression risk factors in children undergoing urinary screening. Pediatr Nephrol. 2000;14(10–11):953–9.
Haysom L, Williams R, Hodson E, Lopez-Vargas P, Roy LP, Lyle D, et al. Risk of CKD in Australian indigenous and nonindigenous children: a population-based cohort study. Am J Kidney Dis. 2009;53(2):229–37.
Silverberg DS, Smith ES, Juchli B, VanDorsser E. Use of shopping centres in screening for hypertension. Can Med Assoc J. 1974;111(8):769–74.
Zhai Y-H, Xu H, Zhu G-H, Wei M-J, Hua B-C, Shen Q, et al. Efficacy of urine screening at school: experience in Shanghai, China. Pediatr Nephrol. 2007;22(12):2073–9.
Vehaskari VM, Rapola J. Isolated proteinuria: analysis of a school-age population. J Pediatr. 1982;101(5):661–8.
Shajari A, Shajari H, Zade MHF, Kamali K, Kadivar MR, Nourani F. Benefit of urinalysis. Indian J Pediatr. 2009;76(6):639–41.
Koshy SM, Garcia-Garcia G, Pamplona JS, Renoirte-Lopez K, Perez-Cortes G, Gutierrez MLS, et al. Screening for kidney disease in children on World Kidney Day in Jalisco, Mexico. Pediatr Nephrol. 2009;24(6):1219–25.
Jafar TH, Stark PC, Schmid CH, Landa M, Maschio G, de Jong PE, et al. Progression of chronic kidney disease: the role of blood pressure control, proteinuria, and angiotensin-converting enzyme inhibition: a patient-level meta-analysis. Ann Intern Med. 2003;139(4):244–52.
Ramirez SP, Hsu SI, McClellan W. Low body weight is a risk factor for proteinuria in multiracial Southeast Asian pediatric population. Am J Kidney Dis. 2001;38(5):1045–54.
Meadow SR, White RH, Johnston NM. Prevalence of symptomless urinary tract disease in Birmingham schoolchildren. I. Pyuria and bacteriuria. Br Med J. 1969;3(5662):81–4.
Mueller PW, Caudill SP. Urinary albumin excretion in children: factors related to elevated excretion in the United States population. Ren Fail. 1999;21(3–4):293–302.
Sox CM, Christakis DA. Pediatricians’ screening urinalysis practices. J Pediatr. 2005;147(3):362–5.
Committee on P, Ambulatory M. Recommendations for preventive pediatric health care. Pediatrics. 2000;105(3):645–6.
Committee on P, Ambulatory M, Bright Futures Steering C. Recommendations for preventive pediatric health care. Pediatrics. 2007;120(6):1376.
Sekhar DL, Wang L, Hollenbeak CS, Widome MD, Paul IM. A cost-effectiveness analysis of screening urine dipsticks in well-child care. Pediatrics. 2010;125(4):660–3.
Soylemezoglu O, Duzova A, Yalcinkaya F, Arinsoy T, Suleymanlar G. Chronic renal disease in children aged 5–18 years: a population-based survey in Turkey, the CREDIT-C study. Nephrol Dial Transplant. 2012;27 Suppl 3:146–51.
Gheissari A, Kelishadi R, Roomizadeh P, Abedini A, Haghjooy-Javanmard S, Abtahi S-H, et al. Chronic kidney disease stages 3–5 in Iranian children: need for a school-based screening strategy: the CASPIAN-III study. Int J Prev Med. 2013;4(1):95–9101.
Esbjorner E, Berg U, Hansson S. Epidemiology of chronic renal failure in children: a report from Sweden 1986–1994. Swed Pediatr Nephrol Assoc Pediatr Nephrol. 1997;11(4):438–42.
Areses Trapote R, Sanahuja Ibanez MJ, Navarro M, Investigadores Centros Participantes en el R, II. Epidemiology of chronic kidney disease in Spanish pediatric population. REPIR II Project. Nefrol Publ Off Soc Esp Nefrol. 2010;30(5):508–17.
Furth SL, Cole SR, Moxey-Mims M, Kaskel F, Mak R, Schwartz G, et al. Design and methods of the Chronic Kidney Disease in Children (CKiD) prospective cohort study. Clin J Am Soc Nephrol. 2006;1(5):1006–15.
Lagomarsimo E, Valenzuela A, Cavagnaro F, Solar E. Chronic renal failure in pediatrics 1996. Chilean survey. Pediatr Nephrol. 1999;13(4):288–91.
Grimoldi IA, Briones LM, Ferraris JR, Rodriguez Rilo L, Sojo E, Turconi A, et al. Chronic renal failure, dialysis and transplant: multicentric study: 1996–2003. Arch Argent Pediatr. 2008;106(6):552–9.
Miller ME, Williams JA. Chronic renal failure in Jamaican children – an update (2001–2006). West Indian Med J. 2009;58(3):231–4.
Orta-Sibu N, Lopez M, Moriyon JC, Chavez JB. Renal diseases in children in Venezuela, South America. Pediatr Nephrol. 2002;17(7):566–9.
Franco-Marina F, Tirado-Gomez LL, Estrada AV, Moreno-Lopez JA, Pacheco-Dominguez RL, Duran-Arenas L, et al. An indirect estimation of current and future inequalities in the frequency of end stage renal disease in Mexico. Salud Publica Mex. 2011;53 Suppl 4:506–15.
Marra G, Edefonti A, Galan YS, Sandoval M, Sereni F. Relevance of a database for monitoring a cooperative paediatric nephrology project in Nicaragua. Pediatr Nephrol. 2011;26(4):641–2.
Lou-Meda R. ESRD in Guatemala and a model for preventive strategies: outlook of the Guatemalan Foundation for Children with Kidney Diseases. Ren Fail. 2006;28(8):689–91.
Huong NTQ, Long TD, Bouissou F, Liem NT, Truong DM, Nga DK, et al. Chronic kidney disease in children: the National Paediatric Hospital experience in Hanoi, Vietnam. Nephrology (Carlton). 2009;14(8):722–7.
Mong Hiep TT, Janssen F, Ismaili K, Khai Minh D, Vuong Kiet D, Robert A. Etiology and outcome of chronic renal failure in hospitalized children in Ho Chi Minh City. Vietnam Pediatr Nephrol. 2008;23(6):965–70.
Vachvanichsanong P, Dissaneewate P, McNeil E. Childhood chronic kidney disease in a developing country. Pediatr Nephrol. 2008;23(7):1143–7.
Yang JY, Yao Y, Chinese Society of Pediatric N. Analysis of 1268 patients with chronic renal failure in childhood: a report from 91 hospitals in China from 1990 to 2002. Zhonghua er ke za zhi Chinese Journal of Pediatrics. 2004;42(10):724–30.
Hamed RMA. The spectrum of chronic renal failure among Jordanian children. J Nephrol. 2002;15(2):130–5.
Anochie I, Eke F. Chronic renal failure in children: a report from Port Harcourt, Nigeria (1985–2000). Pediatr Nephrol. 2003;18(7):692–5.
Bhimma R, Adhikari M, Asharam K, Connolly C. The spectrum of chronic kidney disease (stages 2–5) in KwaZulu-Natal, South Africa. Pediatr Nephrol. 2008;23(10):1841–6.
Ali E-TMA, Abdelraheem MB, Mohamed RM, Hassan EG, Watson AR. Chronic renal failure in Sudanese children: aetiology and outcomes. Pediatr Nephrol. 2009;24(2):349–53.
Olowu WA, Adefehinti O, Aladekomo TA. Epidemiology and clinicopathologic outcome of pediatric chronic kidney disease in Nigeria, a single center study. Arab J Nephrol Transplant. 2013;6(2):105–13.
Michael IO, Gabreil OE. Chronic renal failure in children of benin, Nigeria. Saudi J Kidney Dis Transplant: Off Publ Saudi Cent Organ Transplant Saudi Arabia. 2004;15(1):79–83.
Madani K, Otoukesh H, Rastegar A, Van Why S. Chronic renal failure in Iranian children. Pediatr Nephrol. 2001;16(2):140–4.
Gulati S, Mittal S, Sharma RK, Gupta A. Etiology and outcome of chronic renal failure in Indian children. Pediatr Nephrol. 1999;13(7):594–6.
Barsoum RS. Chronic kidney disease in the developing world. N Engl J Med. 2006;354(10):997–9.
Al-Eisa AA, Samhan M, Naseef M. End-stage renal disease in Kuwaiti children: an 8-year experience. Transplant Proc. 2004;36(6):1788–91.
van Stralen KJ, Tizard EJ, Verrina E, Schaefer F, Jager KJ. Demographics of paediatric renal replacement therapy in Europe: 2007 annual report of the ESPN/ERA-EDTA registry. Pediatr Nephrol. 2010;25(7):1379–82.
Chesnaye NC, Groothoff JW, Verrina E, Heaf JG, Jankauskiene A, Lukosiene V, Molchanova EA, Conceicao M, Amira P-A, Ilse-Maria R, Reisæter AV, Roussinov D, Sukalo A, Topaloglu R, Van Hoeck K, Zurowska AM, Jager KJ, Van Stralen KJ, On behalf of the ESPN/ERA-EDTA registry. Demographics of children with renal replacement therapy in Europe: triannual report of the ESPN/ERA-EDTA registry. Paediatr Nephrol. 2014;29(12):2403–10.
Asinobi AO, Ademola AD, Ogunkunle OO, Mott SA. Paediatric end-stage renal disease in a tertiary hospital in South West Nigeria. BMC Nephrol. 2014;15(1):25.
Tsai TC, Chen YC, Lo CW, Wang WS, Lo SS, Tang GJ, et al. Incidence and renal survival of ESRD in the young Taiwanese population. Clin J Am Soc Nephrol. 2014;9(2):302–9.
van Stralen KJ, Tizard EJ, Jager KJ, Schaefer F, Vondrak K, Groothoff JW, et al. Determinants of eGFR at start of renal replacement therapy in paediatric patients. Nephrol Dial Transplant. 2010;25(10):3325–32.
System USRD. USRDS 2009 Annual data report: atlas of chronic kidney disease and end-stage renal disease in the United States. Bethesda, MD: 2009.
White A, Wong W, Sureshkumur P, Singh G. The burden of kidney disease in indigenous children of Australia and New Zealand, epidemiology, antecedent factors and progression to chronic kidney disease. J Paediatr Child Health. 2010;46(9):504–9.
Lewis MA, Shaw J, Sinha MD, Adalat S, Hussain F, Castledine C, et al. UK Renal Registry 12th Annual Report (December 2009): chapter 14: demography of the UK paediatric renal replacement therapy population in 2008. Nephron Clin Pract. 2010;115 Suppl 1:c279–88. Epub;%2010 Mar 31.:c279–c88.
Registry E-E. ERA-EDTA registry annual report 2011: academic medical center. Amsterdam: Department of Medical Inofrmatic; 2013.
Nogueira PC, Feltran Lde S, Camargo MF, Leao ER, Benninghoven JR, Goncalves NZ, et al. Estimated prevalence of childhood end-stage renal disease in the state of Sao Paulo. Rev Assoc Med Bras. 2011;57(4):436–41.
van der Heijden BJ, van Dijk PC, Verrier-Jones K, Jager KJ, Briggs JD. Renal replacement therapy in children: data from 12 registries in Europe. Pediatr Nephrol. 2004;19(2):213–21.
Harambat J, van Stralen KJ, Schaefer F, Grenda R, Jankauskiene A, Kostic M, et al. Disparities in policies, practices and rates of pediatric kidney transplantation in Europe. Am J Transplant: Off J Am Soc Transplant Am Soc Transplant Surg. 2013;13(8):2066–74.
Harambat J, van Stralen KJ, Verrina E, Groothoff JW, Schaefer F, Jager KJ, et al. Likelihood of children with end-stage kidney disease in Europe to live with a functioning kidney transplant is mainly explained by nonmedical factors. Pediatr Nephrol. 2014;29(3):453–9.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
van Stralen, K.J., Harambat, J., Clayton, P., Craig, J.C. (2016). Demographics of CKD and ESRD in Children. In: Geary, D., Schaefer, F. (eds) Pediatric Kidney Disease. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-662-52972-0_52
Download citation
DOI: https://doi.org/10.1007/978-3-662-52972-0_52
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-662-52970-6
Online ISBN: 978-3-662-52972-0
eBook Packages: MedicineMedicine (R0)