
Abstract
Purpose of Review
Personalized medicine is a challenge to improve survival and quality of life of patients suffering from primary malignant brain tumor. Molecular biology is integrated in initial diagnosis and relapse, and, in the nearest future, over treatment schedule and monitoring. Liquid biopsy is a minimally invasive way to obtain tumor material.
Recent Findings
Over the past years, three fluids have been explored to provide tumor information in primary malignant brain tumor: blood, cerebrospinal fluid, and vitreous liquid. Different tumor components were identified: (1) circulating tumor cells, (2) circulating tumor DNA, (3) RNA and non-coding miRNA, and (4) extracellular vesicles. The performance of the liquid biopsy depends on the tumor type and on the method of detection.
Summary
Liquid biopsy could be a valuable tool to improve patient care in primary malignant brain tumor. Improvement of its sensitivity is the major challenge to generalize its use in daily practice.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The worldwide prevalence of primary malignant brain tumors (PMBTs) is around 11 persons per 100,000 per year [1]. In 2016, the World Health Organization (WHO) classification has integrated molecular biology for diagnosis purposes for several PMBT subtypes [2]. Three major genetic somatic alterations with clinical relevance have been implemented in clinical routine: IDH1/IDH2 mutations, 1p/19q codeletion, and H3.1/H3.3 mutation. Additional alterations will undoubtedly be integrated soon, expanding the number of molecular biomarkers to be tested in the management of PMBT patients. Innovative drugs, including molecular targeted therapies, need specific corresponding alterations in tumor to be effective and safe. As an example, temozolomide and radiotherapy change the tumor cells’ mutational load and induce DNA mutations in the mismatch repair (MMR) system in 3.5% of glioblastomas (GBM) [3]. Alterations in the MMR system induce a highly mutational burden in tumor, conferring sensitivity to immune checkpoints inhibitors (anti-PD-1/PDL-1) [4, 5]. Epidermal growth factor receptor (EGFR) amplification is present in around 40% of GBM. An antibody–drug conjugate is currently evaluated in clinical trials dedicated to GBM patients [6, 7]. Amplification of EGFR is required for the drug to be fully effective. Indeed, EGFR antibody acts as a Trojan horse. Other gene point mutations are theranostic biomarkers for drugs under development. Ibrutinib, a tyrosine kinase inhibitor targeting B-cell receptor, seems to be more efficient in MYD88 or CD79B mutated primary central nervous system lymphoma (PCNSL) [8, 9]. In gliomas, IDH1 inhibitor is a promising drug in IDH-mutated tumors. Mohammad et al. have suggested that EZH2 inhibitor might be of interest in histone-mutant glioma [10]. In this context, molecular analysis of tumor DNA will constitute a routine test for treatment decision-making and for treatment monitoring in PMBT patients. Indeed, tumor DNA is currently obtained from surgical resection or biopsies, mostly at initial diagnosis or at lesser extent at relapse. Postoperative complications (e.g., hemorrhages, infection, and/or neurological deficits) may occur. A minimally invasive tool that may help with molecular diagnosis and with identification of druggable alterations is of major interest in neuro-oncology. This review will present and discuss recent advances in the field of liquid biopsy in PMBT.
Blood
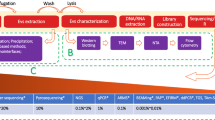
In the field of liquid biopsy in oncology, peripheral blood obtained with blood puncture represents advantages: (1) quick availability, (2) minimally invasive procedure, and (3) wealth of information. Blood-based biomarkers have been widely described in extra-cerebral cancers such as non-small cell lung cancer (NSCLC) [11], breast cancer [12], or colorectal cancer [13]. Three components of blood-based biomarkers have been described in PMBT patients: circulating tumor cells, nucleic acids, and exosomes (Fig. 1).

Representation of sources and components of the liquid biopsy concept in primary malignant brain tumor (PMBT). The components of the figure are from Servier Medical Art by Servier®. The license is available at https://creativecommons.org/licenses/by/3.0/legalcode. Some components have been modified
Circulating Tumor Cells
Circulating tumor cells (CTCs) are cells released by tumor bulk into body fluids, including blood. CTCs reflect the ability of epithelial cancer cells to metastasize. The phenotype of CTCs changes after epithelial-to-mesenchymal transition, to stem cell or mesenchymal phenotypes. Identification of CTCs is based on detection of cell-surface epithelial markers. Immunocytology is the most common detection method [14]. Antibodies targeting epithelial cell adhesion molecule (EpCAM) and cytokines are used in the Cellsearch System (Veridex, Warren, NJ, USA) [15]. Glioma cells do not express epithelial biomarkers and therefore are not detectable using these conventional methods. Sullivan et al. performed a custom immunocytology method to detect circulating brain tumor cells (CBTCs) in blood from GBM patients. Five specific GBM markers were identified. The authors developed a detection assay using antibodies targeting these specific GBM markers including anti-CD14, CD16, and CD45 antibodies. Thirteen out of 33 patients with GBM (39%) had CBTCs in blood at different times in treatment schedule. Detection of CBCTs was not correlated with tumor location, extent of initial resection, or tumor genotype. The number of CBTCs was higher in the blood of patients with progressive disease compared to patients with stable disease (respectively median 11.8 cells/mL vs. 2.1 cells/mL). Interestingly, CBTCs express mesenchymal phenotype while tumor cells express neural phenotype within the tumor bulk [16•] (Table 1). The evidence of CBTCs in GBM patients was confirmed by two other studies. Mac Arthur et al. developed a CBTC detection method using telomerase activity. CBTCs were detectable in 8/11 patients (72%) before the radiotherapy and in 1/8 patient post-radiotherapy. In pre-radiotherapy period, three patients had a CBTC concentration lower than the threshold identified in healthy subjects. Interestingly, the number of CBTCs was correlated with clinical outcome. Indeed, in one patient, the CBTC number increased before ulterior progressive disease (5 CBTC/mL pre-radiotherapy vs. 15 CBTC/mL after radiotherapy) [17•]. Muller et al. used an anti-glial fibrillary acidic protein (GFAP) antibody to detect CBTC in GBM patients. Overall, 30 patients out of 147 (20.4%) had detectable GFAP-positive circulating cells in peripheral blood. In two patients, both genome-wide chromosomal and array CGH were performed in PMBT and GFAP-positive cells. Similar chromosomal aberrations were found in both samples, but heterogeneities were observed in the same patient between several circulating cells and initial tumor sample, especially regarding EGFR and chromosome 3 amplifications [27].
Nucleic Acids
Cell-Free Circulating Tumor DNA
Cell-free DNA (cfDNA) are DNA fragments circulating in body fluids. In non-cancer patients, blood cfDNA comes mainly from genomic DNA released during cell apoptosis or inflammation process [28]. Genomic cfDNA are long DNA fragments (> 500 bp). In physiological conditions, blood cfDNA concentration is low due to its clearance by phagocytes. DNA fragments released by tumor, called circulating tumor DNA (ctDNA), are also a part of cancer patients’ cfDNA. ctDNA are released by necrotic and apoptotic cells [29]. In contrast to genomic cfDNA, ctDNA are small fragments (< 100 bp) and exhibit somatic genetic alterations [30]. Indeed, single nucleotide variants, chromosomal rearrangements, or gene copy number variations could be detected in ctDNA. ctDNA is extracted from peripheral blood sample (5 to 10 mL of whole blood). As the mean half-life duration of ctDNA is short (~ 1.5–2 h) [31], plasma must be quickly separated and frozen within 3 h after collection. Recently, specific DNA tube collectors have been developed to guarantee DNA stability for 24 h [32, 33]. Once extracted, detection of somatic alterations on ctDNA depends on the quantity of ctDNA and the sensitivity of the sequencing method. The ctDNA proportion among whole cfDNA is correlated with tumor burden in advanced solid tumors. The overall cfDNA concentration and the variant allele frequency (VAF) are two quantitative biomarkers. At diagnosis, the cfDNA level is inversely correlated to overall survival in lung, colorectal, ovarian, and breast cancer patients [34,35,36,37]. The VAF represents the proportion of one specific somatic alteration among wild-type allele and varies from 0.01% to > 80% in cfDNA. The clinical significance of a VAF lower than 5% remains questioned as prognostic and/or theranostic marker. Two methods are currently used to detect somatic alteration in ctDNA: next-generation sequencing (NGS) and digital PCR (dPCR). NGS has the advantage of massive parallel sequencing, such as whole-exome sequencing in one-time experiment. Required DNA amount is proportional to the size and the number of sequenced areas. Targeted panels are usually used to increase the coverage depth. Schwaederle et al. have explored the usefulness of a custom targeted panel to detect actionable mutations in several cancers. One hundred fifty-two patients suffering from PMBT were included. Interestingly, 31.5% (49/152) had at least one detectable somatic alteration in blood ctDNA: 4% associated to FDA approved drugs, 11% to experimental drugs, and 16.5% had non-actionable alterations [18•] (Table 1). De Mattos-Arruda et al. also explored targeted panel on plasma ctDNA, CSF ctDNA, and matched tumor DNA in a cohort of 12 patients (7 patients with CNS restricted tumors and 5 patients with both brain metastases and extra-neuronal tumors). In the CNS-restricted tumor cohort (four GBM, two patients with breast cancer brain metastasis, and one patient with lung cancer brain metastasis), no alterations were found in plasma ctDNA. The coverage depth of plasma cfDNA was mostly lower than 1000 reads [38•]. Rothe et al. have highlighted the need of a coverage depth higher than 25,000 reads for plasma cfDNA [39]. Fontanilles et al. performed a two-time approach in a cohort of PCNSL: somatic mutations were firstly identified in tumor using a targeted panel and secondly a restricted patient-specific panel was performed on matched plasma cfDNA. A total of 32% patients (8/25) had detectable somatic mutations in cfDNA with a mean sequencing depth of 12,550 reads versus 185 reads in tumor [19]. Hattori et al. have recently investigated the sensitivity of two methods, droplet dPCR (ddPCR) or targeted NGS, for detection of MYD88 c.T778C (p.L265P) in plasmatic ctDNA of PCNSL patients. At initial diagnosis, ddPCR detected MYD88 c.T778C in 93% (13/14) of patients whereas targeted NGS did not (0/14) [20]. The superiority of PCR to detect somatic alteration in plasma has already been shown in glioma patients for IDH1 mutation [40] and MGMT promoter methylation [41, 42].
miRNA
MicroRNA (miRNA) are small nucleotide fragments (< 25 bp). miRNA act as translational regulators by binding RNA and a silencer of gene expression. miRNA play an important role in cancer cell by modulating growth, apoptosis, and differentiation processes [43], especially in GBM [21, 44] (Table 1). miRNA are stable in body fluids and could be detected by PCR. Recently, several studies have explored serum miRNA signature in human glioma as diagnostic or prognostic markers. As an example, a low serum miRNA-125b level seems to be associated with glioma diagnosis in several studies [45, 46]. Wang et al. have also shown that low serum level of miR-485-3p seemed to be an independent poor prognostic factor in GBM patients [47].
Extracellular Vesicles (EVs)
EVs are a group of membrane-limited vesicles released by cells. EVs play an important role in intercellular communication by carrying cell components such as nucleic acids (DNA, coding and non-coding RNA, miRNA), lipids, and proteins. EVs are isolated from serum by centrifugation and purification or precipitation. Exosomes and microvesicles are two different types of EVs issued from endosomal and plasma membrane, respectively [48]. Exosomes are 40- to 150-nm-diameter EVs of endocytic origin and can be released by tumor cells. Cancer exosomes are a key component of tumor progression through interactions with the microenvironment (i.e., immune cells, vascular cells, tissue specific cells, and extracellular matrix) [49]. Kucharzewska et al. have highlighted that GBM exosomes are enriched in hypoxic components that promote tumor growth and stimulate neoangiogenesis [50]. Cancer exosomes circulate in blood, thus their component could be detected as circulating biomarkers. EGFRvIII was detected from serum exosome in 96 high-grade glioma patients with a sensitivity of 81.6% and a specificity of 79.3% using reverse transcription PCR (RT-PCR) [22•] (Table 1). The expression of one non-coding RNA (RNU6-1) and two miRNAs (miR-320 and miR-574-3p) in serum exosomes was significantly associated with diagnosis in 25 GBM patients compared to healthy controls [51].
Cerebrospinal Fluid
Cerebrospinal fluid (CSF) is an important source of molecular biomarkers in the setting of PMBT. CSF is collected during lumbar puncture or surgical operation. CSF contains ctDNA, miRNA, exosomes, and protein derivative from the brain tumor. IDH1 mRNA expression was found significantly higher in CSF compared to serum of 24 glioma patients. IDH1 c.G395A mutation, which encodes IDH1 R132H, was identified in CSF by ddPCR in half of the IDH-mutant glioma patients (n = 4/8) [52]. Pan et al. have performed a two-step approach on CSF ctDNA. First, an exome sequencing was made on tumor DNA to identify somatic mutations. Then, two sequencing runs were performed: one using ddPCR and one using targeted NGS. In a cohort of seven patients suffering from PMBT (one vestibular schwannoma and one atypical meningioma) or brain metastasis (two lung carcinoma cancers, two melanomas, and two colorectal cancers), CSF contains gene mutational hotspots in six patients (86%). The mutation allele frequency (MAF) seemed to be lower in ctDNA CSF compared to tumor bulk: AKT1 mutation p.E71K MAF was at 45.2% in tumor, 4% in CSF, and 0% in plasma in the meningioma samples [53]. ctDNA detection in CSF is more sensitive than plasma as highlighted by De Mattos-Arruda et al. CSF provides more qualitative and quantitative information than plasma in a cohort of 12 patients with PMBT (4 GBM) or metastasis restricted to the brain (6 breast cancers and 2 lung cancers): no alteration was identified in plasma while all CSF samples harbored at least one somatic alteration. In GBM patients, mutational profiles detected in CSF differed from the ones obtained in primary tumors: less alteration was identified in CSF [38•]. Recently, in a cohort of 71 GBM, RNA EGFR expression was significantly higher in CSF of patients with EGFRvIII-positive tumor. EGFRvIII was identified by PCR in CSF of 61% of EGFRvIII-positive GBM (n = 14/23) [23•] (Table 1). Histone H3 mutations were identified in ctDNA CSF in a cohort of children with diffuse midline glioma. Eleven patients were analyzed with agreement between tumor tissue and CSF for H3.3K27M in seven patients [24•].
miRNA detection and quantification in CSF could also serve as diagnostic tool in PMBT. Baraniskin et al. proposed a diagnostic tree of PCNSL based on relative expression of three miRNAs (miR-21, miR-19b, and miR-92a) in the CSF, compared to control subjects [54, 55]. Overall, their algorithm permitted to distinguish 22 PCNSL from 30 controls. Drusco et al. also highlighted that candidate miRNA expression varied depending on brain subtype in a cohort of 34 patients with CNS benign or malignant tumor and 14 healthy subjects. For example, expression of mirR-125b was higher in CSF of all malignant tumors, especially medulloblastoma, GBM, and metastasis [56]. Akers et al. identified a nine-miRNA signature in CSF to diagnose GBM. In a validation set, their signature correctly distinguishes GBM from non-malignant lesions in 13/28 patients and 27/32 subjects, respectively [25].
Others
Intraocular Liquid Biopsy
Vitreous biopsy is a reservoir of biomarkers in vitreoretinal B-cell lymphoma (VRL), a subgroup of CNS lymphoma. It has been widely described that vitreous liquid contains tumor cells, monoclonal rearrangement of immunoglobulin heavy chains, and IL10/IL6 ratio higher than 1 [57]. Presence of ctDNA in vitrectomy material has been explored. Bonzheim et al. identified MYD88 mutations in 20/29 patients (69%) suffering from VRL [58]. Recently, Cani et al. performed targeted NGS including 16 genes in vitreous aspirate from four VRL patients. All cases harbored at least one point mutation affecting MYD88 and copy number losses of PTEN or CDKN2A [26] (Table 1).
Urine and Saliva ctDNA
Urinary ctDNA was initially described in patients suffering from urothelial tract cancers. TP53 and FGFR3 mutations were identified in urine of patients with bladder cancer [59]. TERT promoter mutations were also identified in a preliminary study in various urothelial cancers [60]. ctDNA in urine are directly released by apoptotic or necrotic tumor cells. Urinary ctDNA is also issued from the bloodstream after filtration through glomerular system [61]. EGFR mutations were described in urine from patients with NSCLC [62, 63]. The acquired p.T790M resistance mutation to EGFR tyrosine kinase inhibitor was found in urine for 53% patients during follow-up in a cohort of 150 NSCLC.
Saliva cfDNA has been described to contain genomic DNA. As urine, saliva may also contain ctDNA from the bloodstream. Pu et al. explored an original approach based on electric field (EFIRM). Exon 19 deletion and p.L858R mutations of EGFR gene were detected with good agreement between saliva, plasma, and tumor tissue (n = 6/17 patients with NSCLC) [64].
To date, and despite easy availability of urine and saliva in patients with PMBT, no study was published in this specific topic.
Challenges and Perspectives
What Is Influencing the ctDNA Release from the PMBT?
ctDNA is detected in blood and CSF of patients suffering from glioma, medulloblastoma, PCNSL, and brain metastasis. The detection rate is low in blood. The mechanisms of ctDNA release from the PMBT are not fully understood. The first explanation could be the low tumor burden, which has been described to influence the sensitivity of plasma ctDNA detection in NSCLC [65]. Boisselier et al. have highlighted that cfDNA concentration was correlated with contrast-enhancement tumor volume in glioma [40]. Conversely to those results, tumor volume was not correlated to plasmatic cfDNA concentration in PCNSL [19, 20]. The release of ctDNA through the blood–brain barrier and its elimination from the bloodstream is not fully understood. To identify the parameters potentially impacting ctDNA release into CSF and blood is of major interest. Necrosis and macrophage activity are correlated with ctDNA release in Hodgkin lymphoma [66]. Once released, ctDNA distribution and elimination from body fluids should also be studied during the nycthemeron to explore influence of corticosteroid therapy, chemotherapy, and/or radiotherapy.
How to Improve the Sensitivity of ctDNA Detection?
One major limitation of liquid biopsy in daily practice for PMBT is its low sensitivity. The fragment length of ctDNA seems to be shorter in rat models bearing GBM xenograft (134–144 bp) [67•]. Consequently, detection of ctDNA can fail because of non-amplification of small DNA fragments, especially for NGS. cfDNA integrity is estimated by the ratio of short (< 200 bp) versus long DNA fragments (> 500 bp). A high ratio means the presence of ctDNA over genomic cfDNA and correlates with cancer diagnosis in NSCLC and breast cancer [68, 69]. To date, no study investigated this specific topic in glioma patients. The sensitivity should also be improved by using tumor-educated platelets (TEPs). TEPs contain RNA and allow early lung cancer diagnosis by identifying a specific RNA signature [70]. Recently, the combination of RNA from exosome and plasmatic ctDNA increases EGFR mutation detection in NSCLC patients [71]. Beyond detection of somatic alterations, epigenetic modification in cancer is a promising tool for liquid biopsy. The cfDNA methylation status in plasma is a valuable biomarker in cancer diagnosis. Uehiro et al. have performed a genome-wide methylation analysis on plasmatic cfDNA. Twelve methylated regions have been identified to correlate with breast cancer diagnosis compared to healthy subjects [72]. Moreover, temozolomide induces DNA methylation. It could be interesting to evaluate the methylation profile over treatment course and to correlate it to treatment response and toxicity.
Conclusion
Liquid biopsy in PMBT covers three types of body fluids (blood, CSF, and vitreous liquid) and multiple biomarkers. Despite recent improvement in detection methods, the low sensitivity in glioma or PCNSL does not allow its use in daily practice. Further studies are warranted to better understand the release of molecular biomarkers in blood or CSF to identify patients for whom liquid biopsy could improve their cancer management. To find biomarkers that could be easily and minimally invasively collected at initial diagnosis and during treatment course remains a challenging question in PMBT. Epigenetic, transcriptomic, and deep-sequencing methods are the keys of this challenge in the future.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
de Robles P, Fiest KM, Frolkis AD, Pringsheim T, Atta C, St Germaine-Smith C, et al. The worldwide incidence and prevalence of primary brain tumors: a systematic review and meta-analysis. Neuro-Oncology. 2015;17(6):776–83. https://doi.org/10.1093/neuonc/nou283.
Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, et al. The 2016 World Health Organization classification of tumors of the central nervous system: a summary. Acta Neuropathol. 2016;131(6):803–20. https://doi.org/10.1007/s00401-016-1545-1.
Hodges TR, Ott M, Xiu J, Gatalica Z, Swensen J, Zhou S, et al. Mutational burden, immune checkpoint expression, and mismatch repair in glioma: implications for immune checkpoint immunotherapy. Neuro-Oncology. 2017;19(8):1047–57. https://doi.org/10.1093/neuonc/nox026.
Goodman AM, Kato S, Bazhenova L, Patel SP, Frampton GM, Miller V, et al. Tumor mutational burden as an independent predictor of response to immunotherapy in diverse cancers. Mol Cancer Ther. 2017;16(11):2598–608. https://doi.org/10.1158/1535-7163.MCT-17-0386.
Le DT UJN, Wang H, Bartlett BR, Kemberling H, Eyring AD, et al. PD-1 blockade in tumors with mismatch-repair deficiency. N Engl J Med. 2015;372(26):2509–20. https://doi.org/10.1056/NEJMoa1500596.
Reardon DA, Lassman AB, van den Bent M, Kumthekar P, Merrell R, Scott AM, et al. Efficacy and safety results of ABT-414 in combination with radiation and temozolomide in newly diagnosed glioblastoma. Neuro-Oncology. 2017;19(7):965–75. https://doi.org/10.1093/neuonc/now257.
Gan HK, Reardon DA, Lassman AB, Merrell R, van den Bent M, Butowski N, et al. Safety, pharmacokinetics and antitumor response of depatuxizumab mafodotin as monotherapy or in combination with temozolomide in patients with glioblastoma. Neuro-Oncology. 2017; https://doi.org/10.1093/neuonc/nox202.
Wilson WH, Young RM, Schmitz R, Yang Y, Pittaluga S, Wright G, et al. Targeting B cell receptor signaling with ibrutinib in diffuse large B cell lymphoma. Nat Med. 2015;21(8):922–6. https://doi.org/10.1038/nm.3884.
Grommes C, Pastore A, Palaskas N, Tang SS, Campos C, Schartz D, et al. Ibrutinib unmasks critical role of Bruton tyrosine kinase in primary CNS lymphoma. Cancer Discov. 2017;7(9):1018–29. https://doi.org/10.1158/2159-8290.CD-17-0613.
Mohammad F, Weissmann S, Leblanc B, Pandey DP, Højfeldt JW, Comet I, et al. EZH2 is a potential therapeutic target for H3K27M-mutant pediatric gliomas. Nat Med. 2017;23(4):483–92. https://doi.org/10.1038/nm.4293.
Pi C, Zhang M-F, Peng X-X, Zhang Y-C, Xu C-R, Zhou Q. Liquid biopsy in non-small cell lung cancer: a key role in the future of personalized medicine? Expert Rev Mol Diagn. 2017;17(12):1089–96. https://doi.org/10.1080/14737159.2017.1395701.
De Mattos-Arruda L, Caldas C. Cell-free circulating tumour DNA as a liquid biopsy in breast cancer. Mol Oncol. 2016;10(3):464–74. https://doi.org/10.1016/j.molonc.2015.12.001.
Jia S, Zhang R, Li Z, Li J. Clinical and biological significance of circulating tumor cells, circulating tumor DNA, and exosomes as biomarkers in colorectal cancer. Oncotarget. 2017;8(33):55632–45. https://doi.org/10.18632/oncotarget.17184.
Masuda T, Hayashi N, Iguchi T, Ito S, Eguchi H, Mimori K. Clinical and biological significance of circulating tumor cells in cancer. Mol Oncol. 2016;10(3):408–17. https://doi.org/10.1016/j.molonc.2016.01.010.
Allard WJ, Matera J, Miller MC, Repollet M, Connelly MC, Rao C, et al. Tumor cells circulate in the peripheral blood of all major carcinomas but not in healthy subjects or patients with nonmalignant diseases. Clin Cancer Res. 2004;10(20):6897–904. https://doi.org/10.1158/1078-0432.CCR-04-0378.
• Sullivan JP, Nahed BV, Madden MW, Oliveira SM, Springer S, Bhere D, et al. Brain tumor cells in circulation are enriched for mesenchymal gene expression. Cancer Discov. 2014;4:1299–309. This study provides evidence of release of tumor cells in blood in GBM and highlights that the release mechanism is dependent on a phenotype modification.
• Macarthur KM, Kao GD, Chandrasekaran S, Alonso-Basanta M, Chapman C, Lustig RA, et al. Detection of brain tumor cells in the peripheral blood by a telomerase promoter-based assay. Cancer Res. 2014;74:2152–9. This study develops an original method to detect circulating tumor cells in plasma.
• Schwaederle M, Chattopadhyay R, Kato S, Fanta PT, Banks KC, Choi IS, et al. Genomic alterations in circulating tumor DNA from diverse cancer patients identified by next-generation sequencing. Cancer Res. 2017;77:5419–27. This study highlights that a targeted NGS panel permits to detect somatic mutations and among them, targetable alterations, in plasma in PMBT.
Fontanilles M, Marguet F, Bohers É, Viailly P-J, Dubois S, Bertrand P, et al. Non-invasive detection of somatic mutations using next-generation sequencing in primary central nervous system lymphoma. Oncotarget. 2017;8(29):48157–68. https://doi.org/10.18632/oncotarget.18325.
Hattori K, Sakata-Yanagimoto M, Suehara Y, Yokoyama Y, Kato T, Kurita N, et al. Clinical significance of disease-specific MYD88 mutations in circulating DNA in primary central nervous system lymphoma. Cancer Sci. 2017;
Odjélé A, Charest D, Morin P. miRNAs as important drivers of glioblastomas: a no-brainer? Cancer Biomark. 2012;11(6):245–52. https://doi.org/10.3233/CBM-2012-0271.
• Manda SV, Kataria Y, Tatireddy BR, Ramakrishnan B, Ratnam BG, Lath R, et al. Exosomes as a biomarker platform for detecting epidermal growth factor receptor-positive high-grade gliomas. J. Neurosurg. 2017;1–11. This study highlights the use of exosomes in blood to identify high grade glioma using EGFR amplification.
• Figueroa JM, Skog J, Akers J, Li H, Komotar R, Jensen R, et al. Detection of wild-type EGFR amplification and EGFRvIII mutation in CSF-derived extracellular vesicles of glioblastoma patients. Neuro-Oncol. 2017;19:1494–502. This study is the first to report the two most common EGFR alterations in CSF.
• Huang TY, Piunti A, Lulla RR, Qi J, Horbinski CM, Tomita T, et al. Detection of Histone H3 mutations in cerebrospinal fluid-derived tumor DNA from children with diffuse midline glioma. Acta Neuropathol Commun. 2017;5:28. This study describes for the first time the detection of histone mutations H3 in CSF in children and opens the possibility to perform this method in midline gliomas in adults, which are particularly difficult to access surgically.
Akers JC, Hua W, Li H, Ramakrishnan V, Yang Z, Quan K, et al. A cerebrospinal fluid microRNA signature as biomarker for glioblastoma. Oncotarget. 2017;8(40):68769–79. https://doi.org/10.18632/oncotarget.18332.
Cani AK, Hovelson DH, Demirci H, Johnson MW, Tomlins SA, Rao RC. Next generation sequencing of vitreoretinal lymphomas from small-volume intraocular liquid biopsies: new routes to targeted therapies. Oncotarget. 2017;8(5):7989–98. https://doi.org/10.18632/oncotarget.14008.
Müller C, Holtschmidt J, Auer M, Heitzer E, Lamszus K, Schulte A, et al. Hematogenous dissemination of glioblastoma multiforme. Sci Transl Med. 2014;6(247):247ra101. https://doi.org/10.1126/scitranslmed.3009095.
Stroun M, Lyautey J, Lederrey C, Olson-Sand A, Anker P. About the possible origin and mechanism of circulating DNA apoptosis and active DNA release. Clin Chim Acta. 2001;313:139–42.
Jahr S, Hentze H, Englisch S, Hardt D, Fackelmayer FO, Hesch RD, et al. DNA fragments in the blood plasma of cancer patients: quantitations and evidence for their origin from apoptotic and necrotic cells. Cancer Res. 2001;61(4):1659–65.
Aucamp J, Bronkhorst AJ, Peters DL, Van Dyk HC, Van der Westhuizen FH, Pretorius PJ. Kinetic analysis, size profiling, and bioenergetic association of DNA released by selected cell lines in vitro. Cell Mol Life Sci. 2017;74(14):2689–707. https://doi.org/10.1007/s00018-017-2495-z.
Diehl F, Schmidt K, Choti MA, Romans K, Goodman S, Li M, et al. Circulating mutant DNA to assess tumor dynamics. Nat Med. 2008;14(9):985–90. https://doi.org/10.1038/nm.1789.
Medina Diaz I, Nocon A, Mehnert DH, Fredebohm J, Diehl F, Holtrup F. Performance of Streck cfDNA blood collection tubes for liquid biopsy testing. PLoS One. 2016;11(11):e0166354. https://doi.org/10.1371/journal.pone.0166354.
Norton SE, Lechner JM, Williams T, Fernando MR. A stabilizing reagent prevents cell-free DNA contamination by cellular DNA in plasma during blood sample storage and shipping as determined by digital PCR. Clin Biochem. 2013;46(15):1561–5. https://doi.org/10.1016/j.clinbiochem.2013.06.002.
Steffensen KD, Madsen CV, Andersen RF, Waldstrøm M, Adimi P, Jakobsen A. Prognostic importance of cell-free DNA in chemotherapy resistant ovarian cancer treated with bevacizumab. Eur J Cancer. 2014;50(15):2611–8. https://doi.org/10.1016/j.ejca.2014.06.022.
El Messaoudi S, Mouliere F, Du Manoir S, Bascoul-Mollevi C, Gillet B, Nouaille M, et al. Circulating DNA as a strong multimarker prognostic tool for metastatic colorectal cancer patient management care. Clin Cancer Res. 2016;22(12):3067–77. https://doi.org/10.1158/1078-0432.CCR-15-0297.
Yanagita M, Redig AJ, Paweletz CP, Dahlberg SE, O’Connell A, Feeney N, et al. A prospective evaluation of circulating tumor cells and cell-free DNA in EGFR-mutant non-small cell lung cancer patients treated with erlotinib on a phase II trial. Clin Cancer Res. 2016;22(24):6010–20. https://doi.org/10.1158/1078-0432.CCR-16-0909.
Rossi G, Mu Z, Rademaker A, Austin L, Strickland KS, Lima Barros Costa R, et al. Cell-free DNA and circulating tumor cells: comprehensive liquid biopsy analysis in advanced breast cancer. Clin Cancer Res. 2017; https://doi.org/10.1158/1078-0432.CCR-17-2092.
• De Mattos-Arruda L, Mayor R, CKY N, Weigelt B, Martínez-Ricarte F, Torrejon D, et al. Cerebrospinal fluid-derived circulating tumour DNA better represents the genomic alterations of brain tumours than plasma. Nat Commun. 2015;6:8839. This study was the first to compare diagnostic performance between blood and CSF using NGS in PMBT.
Rothé F, Laes J-F, Lambrechts D, Smeets D, Vincent D, Maetens M, et al. Plasma circulating tumor DNA as an alternative to metastatic biopsies for mutational analysis in breast cancer. Ann Oncol. 2014;25(10):1959–65. https://doi.org/10.1093/annonc/mdu288.
Boisselier B, Gállego Pérez-Larraya J, Rossetto M, Labussière M, Ciccarino P, Marie Y, et al. Detection of IDH1 mutation in the plasma of patients with glioma. Neurology. 2012;79:1693–8.
Fiano V, Trevisan M, Trevisan E, Senetta R, Castiglione A, Sacerdote C, et al. MGMT promoter methylation in plasma of glioma patients receiving temozolomide. J Neuro-Oncol. 2014;117(2):347–57. https://doi.org/10.1007/s11060-014-1395-4.
Majchrzak-Celińska A, Paluszczak J, Kleszcz R, Magiera M, Barciszewska A-M, Nowak S, et al. Detection of MGMT, RASSF1A, p15INK4B, and p14ARF promoter methylation in circulating tumor-derived DNA of central nervous system cancer patients. J Appl Genet. 2013;54(3):335–44. https://doi.org/10.1007/s13353-013-0149-x.
Lu J, Getz G, Miska EA, Alvarez-Saavedra E, Lamb J, Peck D, et al. MicroRNA expression profiles classify human cancers. Nature. 2005;435(7043):834–8. https://doi.org/10.1038/nature03702.
Li R, Gao K, Luo H, Wang X, Shi Y, Dong Q, et al. Identification of intrinsic subtype-specific prognostic microRNAs in primary glioblastoma. J Exp Clin Cancer Res. 2014;33(1):9. https://doi.org/10.1186/1756-9966-33-9.
Wei X, Chen D, Lv T, Li G, Qu S. Serum MicroRNA-125b as a potential biomarker for glioma diagnosis. Mol Neurobiol. 2016;53(1):163–70. https://doi.org/10.1007/s12035-014-8993-1.
Regazzo G, Terrenato I, Spagnuolo M, Carosi M, Cognetti G, Cicchillitti L, et al. A restricted signature of serum miRNAs distinguishes glioblastoma from lower grade gliomas. J Exp Clin Cancer Res. 2016;35(1):124. https://doi.org/10.1186/s13046-016-0393-0.
Wang Z-Q, Zhang M-Y, Deng M-L, Weng N-Q, Wang H-Y, Wu S-X. Low serum level of miR-485-3p predicts poor survival in patients with glioblastoma. PLoS One. 2017;12(9):e0184969. https://doi.org/10.1371/journal.pone.0184969.
Raposo G, Stoorvogel W. Extracellular vesicles: exosomes, microvesicles, and friends. J Cell Biol. 2013;200(4):373–83. https://doi.org/10.1083/jcb.201211138.
Ruivo CF, Adem B, Silva M, Melo SA. The biology of cancer exosomes: insights and new perspectives. Cancer Res. 2017;
Kucharzewska P, Christianson HC, Welch JE, Svensson KJ, Fredlund E, Ringnér M, et al. Exosomes reflect the hypoxic status of glioma cells and mediate hypoxia-dependent activation of vascular cells during tumor development. Proc Natl Acad Sci U S A. 2013;110(18):7312–7. https://doi.org/10.1073/pnas.1220998110.
Manterola L, Guruceaga E, Gállego Pérez-Larraya J, González-Huarriz M, Jauregui P, Tejada S, et al. A small noncoding RNA signature found in exosomes of GBM patient serum as a diagnostic tool. Neuro-Oncology. 2014;16(4):520–7. https://doi.org/10.1093/neuonc/not218.
Chen WW, Balaj L, Liau LM, Samuels ML, Kotsopoulos SK, Maguire CA, et al. BEAMing and droplet digital PCR analysis of mutant IDH1 mRNA in glioma patient serum and cerebrospinal fluid extracellular vesicles. Mol Ther Nucleic Acids. 2013;2:e109. https://doi.org/10.1038/mtna.2013.28.
Pan W, Gu W, Nagpal S, Gephart MH, Quake SR. Brain tumor mutations detected in cerebral spinal fluid. Clin Chem. 2015;61(3):514–22. https://doi.org/10.1373/clinchem.2014.235457.
Baraniskin A, Kuhnhenn J, Schlegel U, Schmiegel W, Hahn S, Schroers R. MicroRNAs in cerebrospinal fluid as biomarker for disease course monitoring in primary central nervous system lymphoma. J Neuro-Oncol. 2012;109(2):239–44. https://doi.org/10.1007/s11060-012-0908-2.
Baraniskin A, Zaslavska E, Nöpel-Dünnebacke S, Ahle G, Seidel S, Schlegel U, et al. Circulating U2 small nuclear RNA fragments as a novel diagnostic biomarker for primary central nervous system lymphoma. Neuro-Oncology. 2015;
Drusco A, Bottoni A, Laganà A, Acunzo M, Fassan M, Cascione L, et al. A differentially expressed set of microRNAs in cerebro-spinal fluid (CSF) can diagnose CNS malignancies. Oncotarget. 2015;6(25):20829–39. https://doi.org/10.18632/oncotarget.4096.
Pochat-Cotilloux C, Bienvenu J, Nguyen A-M, Ohanessian R, Ghesquières H, Sève P, et al. Use of a threshold of interleukin-10 and IL-10/IL-6 ratio in ocular samples for the screening of vitreoretinal lymphoma. Retina (Philadelphia, Pa). 2017;
Bonzheim I, Giese S, Deuter C, Süsskind D, Zierhut M, Waizel M, et al. High frequency of MYD88 mutations in vitreoretinal B-cell lymphoma: a valuable tool to improve diagnostic yield of vitreous aspirates. Blood. 2015;126(1):76–9. https://doi.org/10.1182/blood-2015-01-620518.
Noel N, Couteau J, Maillet G, Gobet F, D’Aloisio F, Minier C, et al. TP53 and FGFR3 gene mutation assessment in urine: pilot study for bladder cancer diagnosis. Anticancer Res. 2015;35(9):4915–21.
Kinde I, Munari E, Faraj SF, Hruban RH, Schoenberg M, Bivalacqua T, et al. TERT promoter mutations occur early in urothelial neoplasia and are biomarkers of early disease and disease recurrence in urine. Cancer Res. 2013;73(24):7162–7. https://doi.org/10.1158/0008-5472.CAN-13-2498.
Botezatu I, Serdyuk O, Potapova G, Shelepov V, Alechina R, Molyaka Y, et al. Genetic analysis of DNA excreted in urine: a new approach for detecting specific genomic DNA sequences from cells dying in an organism. Clin Chem. 2000;46(8 Pt 1):1078–84.
Chen S, Zhao J, Cui L, Liu Y. Urinary circulating DNA detection for dynamic tracking of EGFR mutations for NSCLC patients treated with EGFR-TKIs. Clin Transl Oncol. 2017;19(3):332–40. https://doi.org/10.1007/s12094-016-1534-9.
Reckamp KL, Melnikova VO, Karlovich C, Sequist LV, Camidge DR, Wakelee H, et al. A highly sensitive and quantitative test platform for detection of NSCLC EGFR mutations in urine and plasma. J Thorac Oncol. 2016;11(10):1690–700. https://doi.org/10.1016/j.jtho.2016.05.035.
Pu D, Liang H, Wei F, Akin D, Feng Z, Yan Q, et al. Evaluation of a novel saliva-based epidermal growth factor receptor mutation detection for lung cancer: a pilot study. Thorac Cancer. 2016;7(4):428–36. https://doi.org/10.1111/1759-7714.12350.
Jamal-Hanjani M, Wilson GA, Horswell S, Mitter R, Sakarya O, Constantin T, et al. Detection of ubiquitous and heterogeneous mutations in cell-free DNA from patients with early-stage non-small-cell lung cancer. Ann Oncol. 2016;27(5):862–7. https://doi.org/10.1093/annonc/mdw037.
Hohaus S, Giachelia M, Massini G, Mansueto G, Vannata B, Bozzoli V, et al. Cell-free circulating DNA in Hodgkin’s and non-Hodgkin’s lymphomas. Ann Oncol. 2009;20(8):1408–13. https://doi.org/10.1093/annonc/mdp006.
• Underhill HR, Kitzman JO, Hellwig S, Welker NC, Daza R, Baker DN, et al. Fragment length of circulating tumor DNA. PLoS Genet. 2016;12:e1006162. This study explores the mechanism of release of ctDNA in plasma in GBM and provides tools to improve detection method in future studies.
Madhavan D, Wallwiener M, Bents K, Zucknick M, Nees J, Schott S, et al. Plasma DNA integrity as a biomarker for primary and metastatic breast cancer and potential marker for early diagnosis. Breast Cancer Res Treat. 2014;146(1):163–74. https://doi.org/10.1007/s10549-014-2946-2.
Leng S, Zheng J, Jin Y, Zhang H, Zhu Y, Wu J, et al. Plasma cell-free DNA level and its integrity as biomarkers to distinguish non-small cell lung cancer from tuberculosis. Clin Chim Acta. 2017;
Best MG, Sol N, In ‘t Veld SGJG, Vancura A, Muller M, A-LN N, et al. Swarm intelligence-enhanced detection of non-small-cell lung cancer using tumor-educated platelets. Cancer Cell. 2017;32:238–252.e9.
Krug AK, Enderle D, Karlovich C, Priewasser T, Bentink S, Spiel A, et al. Improved EGFR mutation detection using combined exosomal RNA and circulating tumor DNA in NSCLC patient plasma. Ann Oncol. 2017; https://doi.org/10.1093/annonc/mdx765.
Uehiro N, Sato F, Pu F, Tanaka S, Kawashima M, Kawaguchi K, et al. Circulating cell-free DNA-based epigenetic assay can detect early breast cancer. Breast Cancer Res. 2016;18(1):129. https://doi.org/10.1186/s13058-016-0788-z.
Acknowledgements
The authors thank Louise Damian for providing graphical support for figure elaboration. The research leading to these results has received funding from the program “Investissements d’Avenir” ANR-10-IAIHU-06, Institut Universitaire de Cancérologie.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
A.D.-P. declares no conflict of interest.
M.F. reports non-financial support from Hoffman-La Roche and Amgen and personal fees from “La Lettre du Cancérologue,” outside the submitted work. A.I. reports grants from Fondation ARC, other from IntselChimos, other from Hoffman-La Roche, other from Beta-Innov (July 2014); personal fees from “La Lettre du Cancérologue,” other from Cathera (June 2017), other from BMS (November 2015), other from Hoffman-La Roche (December 2015), other from Cipla (December 2015), outside the submitted work.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical collection on Neuro-oncology
Rights and permissions
About this article

Cite this article
Fontanilles, M., Duran-Peña, A. & Idbaih, A. Liquid Biopsy in Primary Brain Tumors: Looking for Stardust!. Curr Neurol Neurosci Rep 18, 13 (2018). https://doi.org/10.1007/s11910-018-0820-z
Published:
DOI: https://doi.org/10.1007/s11910-018-0820-z