
Abstract
Introduction
Dovitinib is an oral, potent inhibitor of FGFR and VEGFR, and can be a promising strategy in patients with recurrent or progressive glioblastoma (GBM).
Methods
This was an open label phase II study of two arms: Arm 1 included anti-angiogenic naïve patients with recurrent GBM and Arm 2 included patients with recurrent GBM that had progressed on prior anti-angiogenic therapy. Nineteen subjects were enrolled in Arm 1 and 14 subjects in Arm 2. The primary endpoint was 6-month progression-free survival (PFS-6) in Arm 1 and time to progression (TTP) in Arm 2. The secondary endpoints were toxicity, objective response rate (ORR) and overall survival.
Results
Patients in Arm 2 (compared to Arm 1) tended to have longer intervals from diagnosis to study entry (median 26.9 vs. 8.9 months, p = 0.002), experienced more recurrences (64%, had 3–4 prior recurrences compared to 0, p < 0.0001) and tended to be heavily pretreated (71% vs. 26–32% p = 0.04 or 0.02). 6-month PFS was 12% ± 6% for the Arm 1 and 0% for Arm 2. TTP was similar in both treatment arms (median 1.8 months Arm 1 and 0.7–1.8 months Arm 2, p = 0.36). Five patients (15%) had grade 4 toxicities and 22 patients (67%) had grade 3 toxicities. There were no significant differences between the two arms with respect to the amount of change in the levels of biomarkers from baseline.
Conclusion
Dovitinib was not efficacious in prolonging the PFS in patients with recurrent GBM irrespective of prior treatment with anti-angiogenic therapy (including bevacizumab).
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Until the early 2000′s, the standard of care for glioblastoma (GBM) was surgical resection followed by radiation. Stupp et al. [1] demonstrated that by adding temozolomide during and after radiation therapy in GBM patients, median survival could be improved from 12.1 months to 14.6 months. Despite this significant improvement, nearly all GBM recur with a median time to progression after treatment of approximately 6 months [1]. Treatment options at recurrence include surgery, re-radiation, and/or chemotherapy; all of which show modest activity at best and prognosis remains poor.
Anti-angiogenic therapy strategies are a promising approach due to the highly vascular nature of these tumors. GBM cells express high levels of vascular endothelial growth factor (VEGF) in situ, and inhibition of VEGF signaling impedes the growth of glioma xenografts in immunodeficient mice [2, 3]. Bevacizumab is a humanized monoclonal antibody that targets VEGF and has demonstrated significant clinical activity in a number of human tumors, including colorectal and non-small-cell lung cancer [4, 5]. Bevacizumab demonstrated improved objective response rates of 28 to 35% and 6-month progression free survival (PFS-6) rates of 29 to 43%, with no improvement in overall survival (OS) [6, 7]. The median duration of response is only 4 months and patients develop progressive disease; thus, there still remains a great need for new therapies.
Basic fibroblast growth factor (bFGF) is another proangiogenic growth factor that is upregulated in GBM [8]. Dovitinib is an oral, potent inhibitor of FGFR and VEGFR making it an attractive agent to evaluate in patients with recurrent GBM. Binding of bFGF to its receptor results in activation of the protein kinase Ca (PKCa) pathway and the ERK (extracellular signal-regulated kinase) pathway that have been showed to be involved in GBM [9]. The increase in serum levels of bFGF and SDF-1a were noted in patients treated with the pan-VEGFR inhibitor cediranib (AZD 2171) suggesting that upregulation of FGF may be an escape mechanism that confers resistance to bevacizumab. Hence inhibition of FGF as well as VEGF with Dovitinib is a promising strategy in GBM patients who progress after VEFG inhibition [10].
Materials and methods
Study design and treatment
This was prospective phase II clinical trial of patients with recurrent or progressive GBM. Arm 1 included patients who were anti-angiogenic therapy (including anti-VEGF therapy or bevacizumab) naïve. Arm 2 included patients who had progressed on anti-angiogenic therapy. All subjects received Dovitinib 500 mg PO 5 days on, 2 days off weekly on a 28-day cycle until progression. Patients underwent blood work every 2–4 weeks and MRI brain every 8 weeks until progression on both arms. All patients were followed until progression. Responses were assessed using the Response Assessment in Neuro-Oncology (RANO) criteria [11].
Eligibility criteria
Patients who were at least 18 years of age with histologically confirmed GBM; recurrent after standard external-beam fractionated radiotherapy, temozolomide chemotherapy with or without anti-angiogenic therapy. Patients who were anti-angiogenic therapy (including bevacizumab) naïve were enrolled in arm 1. Patient who progressed on anti-angiogenic therapy (including bevacizumab) were eligible to be enrolled in arm 2. Patients with Karnofsky Performance Status (KPS) of ≥ 60%, adequate metabolic and end organ function, and an estimated survival of atleast 2 months were eligible to enroll in the study. Patients had to be on a stable dose of corticosteroids for at least 5 days before obtaining their baseline MRI scan. Patients with acute intracranial hemorrhage determined by non-contrast-enhanced computed tomography scan and patients receiving anticoagulation therapy with warfarin were not eligible for the study.
Primary and secondary end-points
Progression free survival (PFS) was defined as the interval from beginning of treatment to progression or death from any cause; and PFS-6 was defined as the proportion of patients free of progression at 6 months. PFS-6 was the primary endpoint in anti-angiogenic therapy naïve patients (arm 1).
Time to progression (TTP) was defined as the interval from beginning of treatment to progression; patients who exited the trial without having progressed e.g. for adverse events or withdrawal of consent were censored as of the date off treatment. TTP was the primary endpoint in arm 2, patients who had progressed after prior anti-angiogenic therapy. The primary endpoints were different in two arms, PFS-6 in arm 1 which is a commonly used endpoint, TTP was chosen as the endpoint in arm 2 we wanted to get the preliminary efficacy of the drug and censor deaths if any from other causes. Overall survival (OS) was calculated from the start of treatment to death or last follow-up (alive patients were censored as of the last follow-up).
The secondary endpoints were toxicity of Dovitinib in both patient populations using CTCAE version 4.0 [12]. Changes in concentration of circulating cytokines and growth factors such as PlGF, PDGF-AA, PDGF-AB, PDGF-BB, SDF-1α, thrombospondin-1, Ang2, IL-6, IL-8 and FGF were an exploratory end-point. Plasma EDTA samples were collected from all patients at baseline, at cycle 1 day 28 (C1D28), and at the end of treatment. All biomarkers were measured using the CiraScan multiplex platform (Aushon Biosystems, Inc., Billerica, MA) except for CD73 and sHER3 (R&D Systems, Inc., Minneapolis, MN), which were analyzed as described previously [13].
The absolute and relative change from baseline to C1D28 was determined for each marker. In addition, the number of patients for whom the biomarker decreased or increased was also assessed. Only patients with paired baseline and C1D28 samples were included in the analysis. It should be noted nine patients had no C1D28 sample. The end of treatment time points were not further analyzed because the timing of sample acquisition was variable and did not necessarily correspond to when a patient progressed.
Isolation of extracellular vesicles (EV) and EV miRNA
Extracellular vesicles were isolated as previously described [14]. Briefly, plasma was centrifuged at 200×G, and the supernatant then centrifuged twice at 2500×G to yield platelet-free plasma (PFP). PFP was then centrifuged at 100,000×G to collect EV (microparticles and exosomes). The EV pellet was re-suspended in phosphate buffered saline (PBS) and re-centrifuged, and the final EV pellet was used for RNA extraction.
To isolate RNA, EV was re-suspended in 700 μL of QIAzol lysis buffer (Qiagen, Valencia, CA, USA). Total RNA was isolated with the miRNeasy kit (Qiagen). Quantification of EV RNA was performed with an RNA Pico Chip on an Agilent Bio-analyzer (Bio-Rad). Isolated miRNA was measured using NanoString technology at the MD Anderson Cancer Center RNA core lab.
Statistical methods
The outcome of interest differed in the two arms and therefore a separate design was used for each. For the anti-angiogenic naïve patients (arm 1) the primary outcome was PFS6 and a two-stage accrual design was used to test the hypothesis that Dovitinib could increase PFS6 from an historic rate of approximately 36% to 55%. The first accrual stage called for 19 eligible and evaluable patients with expanded accrual to 31 patients if at least 8 of the 19 achieved PFS6. If overall at least 15 patients achieved PFS6 the null hypothesis (PFS6 = 36%) would be rejected. The associated overall type I and II errors were 10% and 20%, respectively and the likelihood of early stopping for lack of efficacy was 63%. For patients progressing on anti-angiogenic therapy (arm 2) the primary outcome was TTP and a single stage accrual design was used to test the hypothesis that median TTP could be increased from an historic 1.5 months to 3.0 months. Assuming type I and II errors of 10% and 20%, respectively, and that TTP followed an exponential distribution 14 eligible and evaluable patients were required. For the correlative biomarker studies a minimum of 14 paired cases (pre-treatment and day 28) were required to ensure at least 80% power (based on 2-sided Wilcoxon signed rank and rank sum tests and 5% type I errors) to detect large but meaningful changes after treatment (≥ 0.60 of a standard deviation) and differences between patient groups (≥ 1.25 standard deviations).
PFS, PFS6, OS, and TPP were summarized using the Kaplan–Meier method. Other continuous factors such as the biomarkers described above were summarized as medians and ranges while categorical factors were summarized as frequency counts and percentages. Toxicity was categorized and graded using CTCAE version 4.0. The Cochran–Armitage trend test and log rank test were used to compare toxicity and efficacy between the two arms, and the impact on outcome of the biomarkers studied, while Spearman rank correlations and the Wilcoxon signed rank and rank sum tests were used to assess associations between biomarkers, changes from baseline, and differences between the two arms, respectively.
Results
Patient demographics and lesion characteristics
Overall 64% (21/33) of patients were male, median age at study entry was 57 years (range 26–68) and median KPS overall was 80 (range 60–100). The median interval from initial diagnosis to study entry was 14.5 months (range 5.0–100.2) and patients had experienced 1–4 recurrences prior to study entry (16 had 1 recurrence (all in arm 1), 8 had 2 recurrences, and 9 had 3 or more recurrences). Table 1 summarizes patient characteristics overall and separately for patients with and without previous anti-angiogenic therapy.
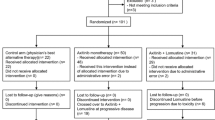
Median maximum diameter was 3.3 cm (range 0.9–7.8 cm) and median tumor area was 5.76 cm2 (range 0.81–41.34 cm2). Nineteen patients did not have prior anti-angiogenic therapy (arm 1). Of the 14 who had prior anti angiogenic therapy, 12 had received bevacizumab, one was treated with bevacizumab as well as TRC105 and bevacizumab and one received prior nintedanib. Patient characteristics were similar between the two groups, however the prior anti-angiogenic therapy group tended to have longer intervals from diagnosis to study entry (median 26.9 versus 8.9 months, p = 0.002), experienced more recurrences (64%, 9/14 had 3–4 prior recurrences compared to 0, p < 0.0001) than the non-treated group and tended to be more heavily pretreated [71% (10/14) with other chemotherapies in addition to temozolomide versus 26–32% (5–6/19), p = 0.04 or 0.02]. The prior anti-angiogenic therapy group also tended to have larger lesions (median 4.4 cm vs. 2.7, p = 0.04) with larger tumor area (11.16 vs. 4.74 cm2, p = 0.02) as shown in Table 1.
Treatment characteristics and response
Treatment was stopped in all patients: 19 (58%) due to disease progression/clinical decline, 11 (33%) for toxicity and in 3 cases (9%) patients withdrew consent. Overall, patients completed a median of one (28 day) cycle of treatment (range 1–3); 17 (52%) completed one cycle, 13 (39%) completed 2, and 3 (9%) completed 3 cycles. Treatment dose was reduced (to 400 mg) in 6 (18%) patients. Of these 6 patients, 2 patients (14%) had prior anti-angiogenic treatment and 4 patients (21%) did not receive such prior treatment. Two patients in arm 1 achieved partial responses (71% and 91% decreases in tumor area, respectively).
Progression-free survival, time to progression, and overall survival
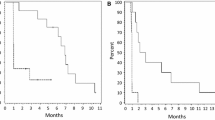
Overall 23 (70%) patients progressed and 31 (94%) died at the time of last follow up. Median (95% C.I.) PFS, TTP, and OS were: 1.8 (1.4–2.0), 1.8 months (1.4–1.8), and 5.6 (4.2–8.1), respectively. Overall 6-month PFS was estimated to be 6% ± 4%. Within the two study arms, 6-month PFS was 12% ± 6% for the anti-angiogenic treatment-naïve group (arm 1) and 0% for the prior anti-angiogenic treatment group (arm 2).
Time to progression, was similar in both treatment arms [median 1.8 months in each arm (95% [C.I. 1.3–2.8]) for patients with no history of prior anti-angiogenic therapy, and 0.7–1.8 for previously treated patients, p = 0.36, Fig. 1]; however anti-angiogenic naive patients tended to have better PFS and OS [PFS median (95% C.I.) 2.0 (1.3–3.7) versus 1.8 (0.9–1.8), p = 0.03; OS median (95% C.I.) 8.0 (4.4–11.7) versus 4.3 (2.6–6.7), p = 0.008; Fig. 1c, d, respectively)], as seen in Fig. 1.

Summarizes time to progression (TTP), progression-free survival (PFS), and overall survival (OS) showing a overall TTP, PFS, OS, b TTP by study arm, c PFS by study arm and d OS by study arm
Adverse events
Five patients (15%) had grade 4 toxicities [thrombocytopenia (n = 2); thromboembolic event (n = 1), elevated lipase (n = 1), colitis/appendicitis (n = 1)] and 22 patients (67%) had grade 3 toxicities (primarily elevated cholesterol, triglycerides, and/or lipase, fatigue, thromboembolic events, and low blood counts). Table 2 tabulates adverse events that were considered at least possibly related to treatment that occurred in > 10% of patients.
The most commonly reported events were lipid abnormalities (82%, 27/33, grade 4 in one patient and grade 3 in 13), elevated AST/ALT (70%, 23/33, grade 3 in 3 patients), thrombocytopenia (70%, 23/33, grade 4 in 2 patients, grade 3 in 1), fatigue (55%, 18/33, grade 3 in 7 patients), and mild to moderate diarrhea (52%, 17/33). The toxicity profile was similar in the two study arms, however, 42% (8/19) of patients with no history of prior anti-angiogenic therapy had thromboembolic events (severe in 5 and grade 4 in 1) compared to a single grade 1/2 event in patients who had prior treatment with such agents (p = 0.02). In contrast 6 patients (43%) who had received anti-angiogenic therapy reported hypertension compared to no reports in the untreated arm (p = 0.007) in Table 2.
Correlation between biomarkers and outcomes
Most of the biomarkers increased at cycle 1 day 28 compared to baseline. Exceptions to this were BMP 9 (decreased in all patients), and the VEGF receptors (decreased in 74–89% of patients with data). There was an inverse relationship between changes in VEGF and VEGF receptors, Table 3, Fig. 2. At baseline anti-angiogenic naïve patients had higher levels of some biomarkers compared to patients previously treated with anti-angiogenic agents, and lower levels of others, Supplemental Table 1. However there were no statistically significant differences between the two groups with respect to the amount of change from baseline that was seen at cycle 1 day 28 (data not shown).

Absolute changes from baseline in VEGF and VEGF R3 at cycle 1, day 281 (1: Negative values indicate a decrease compared to baseline, positive values an increase)
The impact of baseline levels and changes at cycle 1 day 28 on OS and PFS were also examined. While there was no impact on OS, baseline levels of BMP 9, CD73, endoglin, TSP 2 and VEGF D impacted PFS (higher BMP 9, CD73, endoglin and VEGF D, and lower TSP 2 were associated with poorer PFS); as did overall changes at cycle 1 day 28 in HER 3, TGFβ 2, and VEGF R3 Supplemental Table 2 and Supplemental Figure 1.
Discussion
In a study of GBM patients treated with the pan-VEGFR inhibitor cediranib (AZD 2171), blood levels of the pro-angiogenic factors bFGF and SDF-1α were noted to be higher in patients at the time of tumor progression or relapse as compared to the levels observed during the phase in which the patients showed a response to cediranib therapy [10] suggested that up-regulation of FGF may lead to escape mechanism and resistance to anti VEGF directed therapy. Dovitinib is an inhibitor of receptor tyrosine kinases (RTKs): FGFR, VEGFR, PDGFRβ, CSF 1R, c-Kit, RET, TrkA, and FLT3 that mediate tumor cell proliferation and survival and is an attractive agent to evaluate in patients with recurrent GBM. FGF is another proangiogenic growth factor that is upregulated in GBM, in which it is expressed focally by tumor cells and also is expressed by the vasculature [8]. The receptors for bFGF include FGFR1, FGFR2, and FGFR4. FGFR1 is upregulated in GBM and is expressed by both the tumor cells and the tumor ECs. Only the tumor cells express FGFR4 and FGFR2 is expressed in the normal brain [15, 16]. Binding of bFGF to its receptor results in activation of the protein kinase Cα (PKCα) pathway and the ERK pathway that have been shown to be involved in GBM [9, 17].
RTKs are involved in the growth of different types of tumors as well as in the initiation, growth, and maintenance of blood vessels supplying the tumor with blood, oxygen, and nutrients [18,19,20]. RTKs such as VEGF receptors, FGF receptors, and PDGFβ receptors have been shown to play an important role in tumor angiogenesis [21]. VEGF is produced by both the host and the cancer cells and has a direct effect on ECs, causing their proliferation, migration, invasion, and growth [22]. FGFs are potent stimulators of angiogenesis in both normal and pathological tissues, having a direct effect on both vessel assembly and sprouting [23]. Blockade of the FGF pathway can overcome resistance to VEGFR inhibitors, emphasizing the importance of FGFR and specifically the need for multi-targeted inhibitors [24]. PDGFβ receptors are expressed on pericytes—smooth muscle cells that surround the vasculature and provide maintenance and support to the tumor neovasculature [25]. Inhibition of these three growth factor receptor kinases should provide a powerful and broad inhibition of the angiogenesis process and provide potent anti-tumor effects. Dovitinib was investigated in many different solid tumors and demonstrated some activity in phase II clinical trials with metastatic renal cell carcinoma [26]. With its dual mechanism of action: anti-tumor effects via its anti-proliferative activity as well as anti-angiogenic activity, Dovitinib was a promising agent to evaluate in recurrent GBM.
This phase II clinical trial of Dovitinib in patients with recurrent GBM who have progressed with or without anti-angiogenic therapy failed to show benefit. PFS-6 for arm 1 was 12% ± 6% median PFS for arm 2 was 1.8 months (95% C.I. 0.9–1.8). A phase II study with nintedanib, which has activity against VEGFR, PDGFR, and FGFR, showed a PFS-6 of 0% [27]. Studies using other VEGF directed therapies such as cediranib, sunitinib and sorafenib also showed PFS-6 of less than 20% [28,29,30]. Preclinical data of these anti-angiogenic agents were promising but however, phase II trials have not been satisfactory so far.
Thirty-three percent of the patients in our study stopped treatment due to toxicity. The dose had to be reduced to 400 mg in 18% of the patients. The majority of the reported adverse events were grade 3 (67%) and grade 4(15%). The toxicity profile was similar in both arms though patients in arm 1 (anti-angiogenic therapy naïve) suffered from more thromboembolic events (42%) than arm 2 (single event). Also, PFS-6 in arm 1 was greater than that in arm 2. This difference can be attributed to the fact that patients in arm 2 were more refractory and were resistant to anti-angiogenic therapy.
Our study was negative from a clinical perspective, without documented responses. Thus, not surprisingly, there were no significant changes in extracellular vesicle (EV) miRNA profiles in patient plasma when pre- and post-treatment samples were compared. However, given that samples were generally collected 2 weeks or more after treatment, it is possible that our collection strategy may have missed transient changes in EV miRNAs that occurred soon after administration of Dovitinib.
However, our studies did demonstrate interesting differences in EV miRNA profiles when the subgroup that had received prior therapy with bevacizumab was compared with the group that had received no prior anti-angiogenic/anti-tumor therapy. Specifically, we observed significant down-regulation of four miRNAs: these included let-7a-5p, let-7g-5p, miR-150-5p and miR-191-5p. The concentrations of miR-150, along with several other miRNAs, has been previously reported to be down-regulated in malignant gliomas, and a serum signature of these miRNAs has been suggested to be of potential benefit in the diagnosis of high grade tumors [31]. In addition, miR-191 has been included as part of a prognostic miRNA signature for patients with the mesenchymal subtype of GBM [32].
Perhaps the most interesting finding with respect to miRNA profiles is decreased expression of let-7b family members. Decreased expression of let-7b has been reported in patients with GBM [33], though our findings are unique in possibly suggesting greater reductions in patients previously treated with anti-angiogenic therapy. Let-7a miRNA has been suggested to interact cooperatively with the Myc oncogene to regulate multiple downstream pathways in GBM that regulate chromosome stability and tumor growth [34]. Let-7a miRNA may function as a tumor suppressor that targets many important genes involved in tumorigenesis, including Ras, Myc and Lin28, among others [35]. Over-expression of let-7 family miRNA reverses cell proliferation induced by activating Ras mutations [36, 37], as well as the in-vitro proliferation of GBM cell lines and the growth of GBM xenografts [38]. Our findings, in which levels let-7a-5p and let7b-5p were reduced in the plasma of patients who had previously failed anti-angiogenic therapy suggests that decreased expression of let-7 family miRNA may be a mechanism of tumor resistance that may develop in response to therapy. However, it is also possible that let-7 miRNA may have been decreased in these tumors prior to initial therapy, and thus this oncogenic profile resulted in patient selection for the therapy-resistant subgroup.
Interestingly, the biomarker profiles of patients who were previously treated with anti-angiogenic therapies are consistent with prior reports evaluating biomarker changes in response to treatment. In this study, patients exposed to prior anti-VEGF therapy were observed to have higher baseline levels of PlGF and VCAM-1, and lower levels of Ang-2 and s-VEGFR1, compared to patients who were anti-angiogenic treatment naïve. Differences in these two populations align with published data describing the on-treatment change in response to anti-VEGF therapy [39,40,41]. It is interesting to note that these biomarkers remained altered in patients after stopping prior anti-angiogenic therapy for at least a month prior to enrollment to this study. Further studies are needed to definitively establish the durability of these biomarker changes observed after anti-angiogenic treatment.
Conclusion
Dovitinib is not effective in in patients with recurrent GBM irrespective of prior treatment with bevacizumab therapy. Baseline levels of BMP 9, CD73, endoglin, TSP 2, VEGF D and overall change in HER 3, TGFβ 2, and VEGF R3 impacted PFS, with no impact on OS.
References
Stupp R, Mason WP, van den Bent MJ, Weller M, Fisher B, Taphoorn MJ, Belanger K, Brandes AA, Marosi C, Bogdahn U, Curschmann J, Janzer RC, Ludwin SK, Gorlia T, Allgeier A, Lacombe D, Cairncross JG, Eisenhauer E, Mirimanoff RO (2005) Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 352(10):987–996. https://doi.org/10.1056/NEJMoa043330
Takahashi Y, Kitadai Y, Bucana CD, Cleary KR, Ellis LM (1995) Expression of vascular endothelial growth factor and its receptor, KDR, correlates with vascularity, metastasis, and proliferation of human colon cancer. Can Res 55(18):3964–3968
Stefanik DF, Fellows WK, Rizkalla LR, Rizkalla WM, Stefanik PP, Deleo AB, Welch WC (2001) Monoclonal antibodies to vascular endothelial growth factor (VEGF) and the VEGF receptor, FLT-1, inhibit the growth of C6 glioma in a mouse xenograft. J Neurooncol 55(2):91–100
Hurwitz HI, Fehrenbacher L, Hainsworth JD, Heim W, Berlin J, Holmgren E, Hambleton J, Novotny WF, Kabbinavar F (2005) Bevacizumab in combination with fluorouracil and leucovorin: an active regimen for first-line metastatic colorectal cancer. J Clin Oncol 23(15):3502–3508. https://doi.org/10.1200/jco.2005.10.017
Kerr C (2005) Bevacizumab and chemotherapy improves survival in NSCLC. Lancet Oncol 6(5):266
Friedman HS, Prados MD, Wen PY, Mikkelsen T, Schiff D, Abrey LE, Yung WK, Paleologos N, Nicholas MK, Jensen R, Vredenburgh J, Huang J, Zheng M, Cloughesy T (2009) Bevacizumab alone and in combination with irinotecan in recurrent glioblastoma. J Clin Oncol 27(28):4733–4740. https://doi.org/10.1200/jco.2008.19.8721
Kreisl TN, Kim L, Moore K, Duic P, Royce C, Stroud I, Garren N, Mackey M, Butman JA, Camphausen K, Park J, Albert PS, Fine HA (2009) Phase II trial of single-agent bevacizumab followed by bevacizumab plus irinotecan at tumor progression in recurrent glioblastoma. J Clin Oncol 27(5):740–745. https://doi.org/10.1200/jco.2008.16.3055
Morrison RS, Yamaguchi F, Bruner JM, Tang M, McKeehan W, Berger MS (1994) Fibroblast growth factor receptor gene expression and immunoreactivity are elevated in human glioblastoma multiforme. Can Res 54(10):2794–2799
Pintucci G, Froum S, Pinnell J, Mignatti P, Rafii S, Green D (2002) Trophic effects of platelets on cultured endothelial cells are mediated by platelet-associated fibroblast growth factor-2 (FGF-2) and vascular endothelial growth factor (VEGF). Thromb Haemost 88(5):834–842
Batchelor TT, Sorensen AG, di Tomaso E, Zhang WT, Duda DG, Cohen KS, Kozak KR, Cahill DP, Chen PJ, Zhu M, Ancukiewicz M, Mrugala MM, Plotkin S, Drappatz J, Louis DN, Ivy P, Scadden DT, Benner T, Loeffler JS, Wen PY, Jain RK (2007) AZD2171, a pan-VEGF receptor tyrosine kinase inhibitor, normalizes tumor vasculature and alleviates edema in glioblastoma patients. Cancer Cell 11(1):83–95. https://doi.org/10.1016/j.ccr.2006.11.021
Wen PY, Macdonald DR, Reardon DA, Cloughesy TF, Sorensen AG, Galanis E, Degroot J, Wick W, Gilbert MR, Lassman AB, Tsien C, Mikkelsen T, Wong ET, Chamberlain MC, Stupp R, Lamborn KR, Vogelbaum MA, van den Bent MJ, Chang SM (2010) Updated response assessment criteria for high-grade gliomas: response assessment in neuro-oncology working group. J Clin Oncol 28(11):1963–1972. https://doi.org/10.1200/jco.2009.26.3541
Atkinson TM, Ryan SJ, Bennett AV, Stover AM, Saracino RM, Rogak LJ, Jewell ST, Matsoukas K, Li Y, Basch E (2016) The association between clinician-based common terminology criteria for adverse events (CTCAE) and patient-reported outcomes (PRO): a systematic review. Support Care Cancer 24(8):3669–3676. https://doi.org/10.1007/s00520-016-3297-9
Hatch AJ, Sibley AB, Starr MD, Brady JC, Jiang C, Jia J, Bowers DL, Pang H, Owzar K, Niedzwiecki D, Innocenti F, Venook AP, Hurwitz HI, Nixon AB (2016) Blood-based markers of efficacy and resistance to cetuximab treatment in metastatic colorectal cancer: results from CALGB 80203 (Alliance). Cancer Med 5(9):2249–2260. https://doi.org/10.1002/cam4.806
Wu M, Barnard J, Kundu S, McCrae KR (2015) A novel pathway of cellular activation mediated by antiphospholipid antibody-induced extracellular vesicles. J Thromb Haemost JTH 13(10):1928–1940. https://doi.org/10.1111/jth.13072
Yamada SM, Yamada S, Hayashi Y, Takahashi H, Teramoto A, Matsumoto K (2002) Fibroblast growth factor receptor (FGFR) 4 correlated with the malignancy of human astrocytomas. Neurol Res 24(3):244–248. https://doi.org/10.1179/016164102101199864
Ueba T, Takahashi JA, Fukumoto M, Ohta M, Ito N, Oda Y, Kikuchi H, Hatanaka M (1994) Expression of fibroblast growth factor receptor-1 in human glioma and meningioma tissues. Neurosurgery 34(2):221–225. (discussion 225-226)
Tkachenko E, Lutgens E, Stan RV, Simons M (2004) Fibroblast growth factor 2 endocytosis in endothelial cells proceed via syndecan-4-dependent activation of Rac1 and a Cdc42-dependent macropinocytic pathway. J Cell Sci 117(Pt 15):3189–3199. https://doi.org/10.1242/jcs.01190
Arteaga CL (2001) The epidermal growth factor receptor: from mutant oncogene in nonhuman cancers to therapeutic target in human neoplasia. Journal of clinical oncology : official journal of the American Society of Clinical Oncology 19(18 Suppl):32s–40s
Cohen P (2002) Protein kinases–the major drug targets of the twenty-first century? Nat Rev Drug Discovery 1(4):309–315. https://doi.org/10.1038/nrd773
Lemmon MA, Schlessinger J (2010) Cell signaling by receptor tyrosine kinases. Cell 141(7):1117–1134. https://doi.org/10.1016/j.cell.2010.06.011
Dvorak HF (2003) Rous-Whipple Award Lecture. How tumors make bad blood vessels and stroma. Am J Pathol 162 (6):1747-1757
Nagy JA, Vasile E, Feng D, Sundberg C, Brown LF, Manseau EJ, Dvorak AM, Dvorak HF (2002) VEGF-A induces angiogenesis, arteriogenesis, lymphangiogenesis, and vascular malformations. Cold Spring Harb Symp Quant Biol 67:227–237
Auguste P, Javerzat S, Bikfalvi A (2003) Regulation of vascular development by fibroblast growth factors. Cell Tissue Res 314(1):157–166. https://doi.org/10.1007/s00441-003-0750-0
Casanovas O, Hicklin DJ, Bergers G, Hanahan D (2005) Drug resistance by evasion of antiangiogenic targeting of VEGF signaling in late-stage pancreatic islet tumors. Cancer Cell 8(4):299–309. https://doi.org/10.1016/j.ccr.2005.09.005
Bergers G, Song S, Meyer-Morse N, Bergsland E, Hanahan D (2003) Benefits of targeting both pericytes and endothelial cells in the tumor vasculature with kinase inhibitors. J Clin Investig 111(9):1287–1295. https://doi.org/10.1172/jci17929
Escudier B, Grunwald V, Ravaud A, Ou YC, Castellano D, Lin CC, Gschwend JE, Harzstark A, Beall S, Pirotta N, Squires M, Shi M, Angevin E (2014) Phase II results of Dovitinib (TKI258) in patients with metastatic renal cell cancer. Clin Cancer Res 20(11):3012–3022. https://doi.org/10.1158/1078-0432.ccr-13-3006
Norden AD, Schiff D, Ahluwalia MS, Lesser GJ, Nayak L, Lee EQ, Rinne ML, Muzikansky A, Dietrich J, Purow B, Doherty LM, LaFrankie DC, Pulverenti JR, Rifenburg JA, Ruland SF, Smith KH, Gaffey SC, McCluskey C, Ligon KL, Reardon DA, Wen PY (2015) Phase II trial of triple tyrosine kinase receptor inhibitor nintedanib in recurrent high-grade gliomas. J Neurooncol 121(2):297–302. https://doi.org/10.1007/s11060-014-1631-y
Batchelor TT, Mulholland P, Neyns B, Nabors LB, Campone M, Wick A, Mason W, Mikkelsen T, Phuphanich S, Ashby LS, Degroot J, Gattamaneni R, Cher L, Rosenthal M, Payer F, Jurgensmeier JM, Jain RK, Sorensen AG, Xu J, Liu Q, van den Bent M (2013) Phase III randomized trial comparing the efficacy of cediranib as monotherapy, and in combination with lomustine, versus lomustine alone in patients with recurrent glioblastoma. J Clin Oncol 31(26):3212–3218. https://doi.org/10.1200/jco.2012.47.2464
Galanis E, Anderson SK, Lafky JM, Uhm JH, Giannini C, Kumar SK, Kimlinger TK, Northfelt DW, Flynn PJ, Jaeckle KA, Kaufmann TJ, Buckner JC (2013) Phase II study of bevacizumab in combination with sorafenib in recurrent glioblastoma (N0776): a north central cancer treatment group trial. Clin Cancer Res 19(17):4816–4823. https://doi.org/10.1158/1078-0432.ccr-13-0708
Hutterer M, Nowosielski M, Haybaeck J, Embacher S, Stockhammer F, Gotwald T, Holzner B, Capper D, Preusser M, Marosi C, Oberndorfer S, Moik M, Buchroithner J, Seiz M, Tuettenberg J, Herrlinger U, Wick A, Vajkoczy P, Stockhammer G (2014) A single-arm phase II Austrian/German multicenter trial on continuous daily sunitinib in primary glioblastoma at first recurrence (SURGE 01–07). Neuro-oncology 16(1):92–102. https://doi.org/10.1093/neuonc/not161
Yang C, Wang C, Chen X, Chen S, Zhang Y, Zhi F, Wang J, Li L, Zhou X, Li N, Pan H, Zhang J, Zen K, Zhang CY, Zhang C (2013) Identification of seven serum microRNAs from a genome-wide serum microRNA expression profile as potential noninvasive biomarkers for malignant astrocytomas. Int J Cancer 132(1):116–127. https://doi.org/10.1002/ijc.27657
Li R, Gao K, Luo H, Wang X, Shi Y, Dong Q, Luan W, You Y (2014) Identification of intrinsic subtype-specific prognostic microRNAs in primary glioblastoma. J Exp Clin Cancer Res CR 33:9. https://doi.org/10.1186/1756-9966-33-9
Dong L, Li Y, Han C, Wang X, She L, Zhang H (2014) miRNA microarray reveals specific expression in the peripheral blood of glioblastoma patients. Int J Oncol 45(2):746–756. https://doi.org/10.3892/ijo.2014.2459
Wang G, Wang J, Zhao H, Wang J, Tony To SS (2015) The role of Myc and let-7a in glioblastoma, glucose metabolism and response to therapy. Arch Biochem Biophys 580:84–92. https://doi.org/10.1016/j.abb.2015.07.005
Boyerinas B, Park SM, Hau A, Murmann AE, Peter ME (2010) The role of let-7 in cell differentiation and cancer. Endocr Relat Cancer 17(1):F19–F36. https://doi.org/10.1677/erc-09-0184
Roush S, Slack FJ (2008) The let-7 family of microRNAs. Trends Cell Biol 18(10):505–516. https://doi.org/10.1016/j.tcb.2008.07.007
Lee ST, Chu K, Oh HJ, Im WS, Lim JY, Kim SK, Park CK, Jung KH, Lee SK, Kim M, Roh JK (2011) Let-7 microRNA inhibits the proliferation of human glioblastoma cells. J Neurooncol 102(1):19–24. https://doi.org/10.1007/s11060-010-0286-6
Corbin R, Olsson-Carter K, Slack F (2009) The role of microRNAs in synaptic development and function. BMB Rep 42(3):131–135
Liu Y, Starr MD, Brady JC, Rushing C, Bulusu A, Pang H, Honeycutt W, Amara A, Altomare I, Uronis HE, Hurwitz HI, Nixon AB (2015) Biomarker signatures correlate with clinical outcome in refractory metastatic colorectal cancer patients receiving bevacizumab and everolimus. Mol Cancer Ther 14(4):1048–1056. https://doi.org/10.1158/1535-7163.mct-14-0923-t
Liu Y, Starr MD, Bulusu A, Pang H, Wong NS, Honeycutt W, Amara A, Hurwitz HI, Nixon AB (2013) Correlation of angiogenic biomarker signatures with clinical outcomes in metastatic colorectal cancer patients receiving capecitabine, oxaliplatin, and bevacizumab. Cancer Med 2(2):234–242. https://doi.org/10.1002/cam4.71
Murukesh N, Dive C, Jayson GC (2010) Biomarkers of angiogenesis and their role in the development of VEGF inhibitors. Br J Cancer 102(1):8–18. https://doi.org/10.1038/sj.bjc.6605483
Funding
This study was supported by Novartis.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
Dr. Ahluwalia’s disclosures are: receipt of grants/research supports: Astrazeneca, Abbvie, BMS, Bayer, Incyte, Pharmacyclics, Novocure, Merck. Receipt of honoraria or consultation fees: Elsevier, Wiley, Astrazeneca, Abvvie, VBI Vaccines, Flatiron, Varian Medical Systems, Prime Education, Bayer; Stock shareholder: Doctible, Mimivax. There are no potential conflicts of interest for other authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.

11060_2019_3236_MOESM3_ESM.jpg
Supplementary file3 (JPG 385 kb). Correlation between biomarkers and progression free survival (PFS) a) BMP 9 [<27.0 (blue) vs >27.0 (red)] b) Baseline Endoglin [<250.0 (blue) vs > 250.0 (red)] c) Baseline CD73 [<1.2 (blue) vs >1.2 (red)] d) Baseline TSP 2 [<1800 (blue) vs >1800 (red)] e) Overall Change in TGFβ 2 at Cycle 1 Day 28 f) Overall Change in VEGF R3 at Cycle 1 Day 28. (Blue (-1) =decrease compared to baseline; red (1) =increase)
Rights and permissions
About this article

{kind=link}
Cite this article
Sharma, M., Schilero, C., Peereboom, D.M. et al. Phase II study of Dovitinib in recurrent glioblastoma. J Neurooncol 144, 359–368 (2019). https://doi.org/10.1007/s11060-019-03236-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11060-019-03236-6