
Abstract
Background
In the right colon surgery, there is a growing literature comparing the safety of robotic right colectomy (RRC) to that of laparoscopic right colectomy (LRC). With this paper we aim to systematically revise and meta-analyze the latest comparative studies on these two minimally invasive procedures.
Methods
A systematic review of studies published from 2000 to 2017 in the PubMed, Scopus, and Embase databases was performed. Primary endpoints were postoperative morbidity and mortality. Secondary endpoints were blood loss, conversion to open surgery, harvested lymph node anastomotic leak, postoperative hemorrhage, abdominal abscess, postoperative ileus, time to first flatus, non-surgical complications, wound infections, hospital stay, and incisional hernia and costs. A subgroup analysis was performed on those series presenting only extracorporeal anastomosis in both arms.
Results
After screening 355 articles, 11 articles with a total of 8257 patients were eligible for inclusion. Operative time was found to be significantly shorter for the laparoscopic procedures in the pooled analysis (SMD − 0.99 95% CI − 1.4 to − 0.6, p < 0.001). Conversion to open surgery was more common during laparoscopic procedures than during the robotic ones (RR 1.7; 95% CI 1.1–2.6, p = 0.02). No significant differences in mortality (RR 0.47; 95% CI 0.18–1.23, p = 0.124) and postoperative complications (RR 1.05; 95% CI 0.9–1.2, p = 0.5) were found between LRC versus RRC. The pooled mean time to first flatus was higher in the laparoscopic group (SMD 0.85 days; 95% CI 0.16–1.54, p = 0.016). Hospital costs were significantly higher in RRCs (SMD − 0.52; 95% CI − 0.52 to − 0.04, p = 0.035).
Conclusions
RRC can be regarded as a feasible and safe technique. Its superiority in terms of postoperative recovery must be confirmed by further large prospective series comparing RRC and LRC performed with the same anastomotic technique. RRC seemed to be associated with higher costs than LRC.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Minimally invasive approach in colorectal disease is recognized as safe and feasible [1, 2]. In particular, robotic colorectal surgery appears to have technical advantages over the conventional laparoscopic approach due to higher degrees of rotation, articulation, and tri-dimensional imaging [1]. In the right colon surgery, there is a growing literature comparing the safety of robotic right colectomy (RRC) to that of laparoscopic right colectomy (LRC) [3,4,5,6,7]. In trying to meta-analyze these experiences, five studies were published between 2014 and early 2016 [8,9,10,11,12]. Nevertheless, only a few papers [3,4,5, 7, 13, 14] could be included and, thus, these meta-analyses were conducted on a limited number of patients, returning conflicting results. After that, several experiences, including larger series comparing RRC versus LRC, have been published [15,16,17,18,19,20], adding further data and allowing for a more comprehensive analysis.
In the light of these new experiences an updated systematic review of the literature was here performed in order to re-apprise evidences on the use of the robotic system versus standard laparoscopy to perform right colectomy.
Methods
Literature search strategy
This study was conducted and reported according to the 2010 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [21]. A systematic literature search was performed in PubMed, Embase, and Scopus databases for pertinent studies published between January 1st 2000 and May 11th 2017. Search terms used were right AND robot* AND (laparosc* OR “minimally invasive”) AND [(colo* AND resection) OR (colectomy OR hemicolectomy)]. “Related articles” function and manual reference screening were also used.
Results from the databases were compared to obtain a single list of articles for screening. Titles, abstracts and, subsequently, full-text articles, were screened and selected independently by two authors. (LS and AC). Disagreement on eligibility was addressed by discussion and followed by consensus. Additional articles were searched in the International Clinical Trials Registry Platform (ICTRP), which includes clinicaltrials.gov, without retrieving any additional available study. Grey literature search was not considered in the present study.
Eligibility criteria
Only full-text studies in English language which specifically compared RRC versus LRC were included. Comparative studies with less than 15 patients per arm and on pediatric patients were excluded. Abstract, editorials, and reviews were also excluded from the analysis at this point of study selection.
Primary endpoints were postoperative morbidity and mortality. Secondary endpoints were blood loss, conversion to open surgery, harvested lymph node anastomotic leak, postoperative hemorrhage, abdominal abscess, postoperative ileus, time to first flatus, non-surgical complications, wound infections, hospital stay, and incisional hernia and costs.
For overlapping series, only the most recent paper was included.
Assessment of methodological quality and data extraction
Methodological quality was assessed independently by two authors (LS and AC). Jadad scoring [22] was used to evaluate the quality of randomized controlled trials while the methodological index for non-randomized studies (MINORS) [23] scale was used for cohort studies.
Data extracted included study characteristics (country of origin, study period, study design), patients’ characteristics [age, sex, and body mass index (BMI), indication for surgery, American Society of Anesthesiologists (ASA) score], intraoperative (type of anastomosis, operative time, blood loss, conversion to open surgery, and harvested lymph nodes) and postoperative variables (in-hospital mortality, overall morbidity, anastomotic leak, postoperative hemorrhage, abdominal abscess, postoperative ileus, time to first flatus, non-surgical complications, wound infections, hospital stay, and incisional hernia), and costs (surgery only and total costs).
Subgroup analysis
As the majority of the comparative studies differed for the technique adopted for the ileocolic anastomosis, a subgroup analysis was performed on those series presenting only extracorporeal anastomosis in both arms.
Statistical analysis
For categorical variables, the weighted pooled rates with 95% confidence intervals (95% CI) were obtained by the Freeman–Tukey transformation [24] and comparisons were reported as relative risk (RR). Continuous variables were pooled in weighted means and 95% CI exploiting the inverse variance method. Comparisons were reported as standardized mean difference (SMD). When continuous variables were shown as median and interquartile range (or median and range), they were transformed in mean and standard deviation (SD) as suggested by Hozo et al. [25]. Funnel plots were also constructed to look for potential publication bias. Heterogeneity between included studies was explored by inconsistency (I2) statistics [26]. I2 values of < 25% were interpreted as low heterogeneity, between 25 and 50% as medium, between 50 and 75% as substantial, and above 75% as considerable. Statistical analysis was performed using MedCalc Statistical Software version 15.8 (MedCalc Software bvba, Ostend, Belgium; https://www.medcalc.org; 2015).
Results
Literature search results
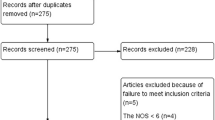
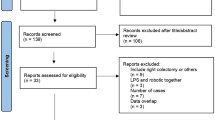
Database search and manual screening of reference lists yielded a total of 175 potentially relevant articles (Fig. 1). Of these, 11 studies published between 2007 and 2017 were considered eligible for data extraction and were therefore included in the meta-analysis [3,4,5,6,7, 15,16,17,18,19,20]. A total of 8257 individual patients who underwent RRC (n = 869) or LRC (n = 7388) from 2007 to 2017 were identified. The quality assessments for each study are summarized in Table 1. Funnel plots did not show evidence of significant bias among studies.

Flow-chart of included articles
Study and patient characteristics
Details of included study are reported in Table 1. Only one RCT [6] was included. Trastulli et al. [20] reported a comparison between intracorporeal anastomosis during RRC and LRC and extracorporeal anastomosis in LRC only; for this paper we considered as a control group only those 40 patients who had LRC with intracorporeal anastomosis.
Patients’ characteristics are reported in Table 2. Preoperative variables did not significantly differ between the two groups. Overall, pooled intracorporeal anastomosis rate, which was not reported by the studies with the largest sample size [15, 17], was higher in the robotic group (RRC 39.7% vs LRC 7.1%, p = 0.105).
Perioperative outcomes
Perioperative outcomes are reported in Tables 3 and 4. Operative time, which could be extracted from all included papers, was found to be significantly shorter for the laparoscopic procedures in the pooled analysis (SMD − 0.99 95% CI − 1.4 to − 0.6, p < 0.001). Conversion to open surgery was more common during laparoscopic procedures than during the robotic ones (RR 1.7; 95% CI 1.1–2.6, p = 0.02). In the robotic group, 27 conversions were to open surgery and 2 [5] to laparoscopic single-incision right hemicolectomy. There was a tendency towards statistical significance for a higher number of lymph node retrieval during RRC than LRC (23.4 versus 24.3), p = 0.057.
As shown in Table 4, there were no significant differences in mortality (RR 0.47; 95% CI 0.18–1.23, p = 0.124) and postoperative complications (RR 1.05; 95% CI 0.9–1.2, p = 0.5) between the two procedures. The pooled mean time to first flatus was higher in the laparoscopic group (SMD 0.85 days; 95% CI 0.16–1.54, p = 0.016). Other complications such as anastomotic leak, postoperative hemorrhage, ileus, wound infection, abdominal abscess, and incisional hernia did not differ between the groups.
Extracorporeal anastomosis subgroup analysis
Five articles [3,4,5, 16, 18] were included in this subgroup analysis. No significant differences were found in any intraoperative or postoperative outcome variables. In particular, the SMD of operative time and time to first flatus between LRC versus RRC were − 0.71 (95% CI − 1.68 to 0.256, p = 0.149—I 2 95.6; 95% CI 92.3–97.5, p < 0.0001) and 0.51 (95% CI − 308 to 1.334, p = 0.22—I 2 86.5%; 95% CI 61.32–95.3, p = 0.0006), respectively. Also the pooled conversion rate did not differ between the groups (RR 0.9; 95% CI 0.34–2.39, p = 0.831—I 2 7.3; 95% CI 0–81.8. p = 0.365).
Costs
Data about total hospital costs could be extracted from five studies [6, 7, 15, 16, 18] and are reported in Table 4. The SMD of the costs between LRC versus RRC was − 0.52 (95% CI − 0.52 to − 0.04, p = 0.035). The pooled mean surgery-only related costs, calculated on data from three studies [6, 7, 16], was higher in the robotic group (5953 $; 95% CI 2223–9684) than in the laparoscopic one (3930 $; 95% CI 1733–6127; p = 0.051).
Discussion
Robotic right colectomy could be regarded as a feasible and safe procedure, having postoperative morbidity and mortality rates comparable with the laparoscopic counterpart. In addition, specific surgical complications such as anastomotic leak, postoperative hemorrhage, postoperative ileus, wound infections, and abdominal abscess were similar between the two procedures. Results from our analysis on more than eight thousand patients confirmed some of what has already been suggested by largest series to date [8,9,10,11], and highlighted other differences not previously found.
With regards to intraoperative blood loss a few conflicting data have been reported so far: three [8, 10, 11] out of five metanalyses showed that blood loss was significantly higher in the laparoscopic group. Again, this should be interpreted in light of the limited number of studies available for those analyses which could have affected the pooled outcome. Present results, based on a more representative sample size, showed that blood loss was comparable between the two procedures in the overall and subgroup analyses. Furthermore, it must be noted that the pooled blood losses were extremely low in both groups (RRC 77 ml versus LRC 80 ml), indicating the comparable, well-established safety of both procedures.
Operative time was demonstrated to be significantly longer in RRCs. Differently from previous studies, the present analysis showed that this could have been partly due to the type of anastomosis performed. In fact, in the subgroup analysis comparing only the extracorporeal anastomoses we found no significant differences between RRC and LRC. Unfortunately we did not have enough data to perform a subgroup analysis on intraoperative anastomosis as only two papers reported this technique in the laparoscopic group [6, 20]. Only Trastulli et al. [20] reported a retrospective comparison between RRC versus LRC both performed with the intracorporeal anastomosis. The authors found that RRC had a significantly longer operative time than LRC. However, confounding factors such as docking time and learning curve could have played a role in increasing the operative time in the robotic procedures. As expected, most of the surgeons preferred to perform the intracorporeal anastomosis with the robotic system as this dramatically decreases the difficulties of intracorporeal suturing. Unfortunately, this resulted in comparative retrospective studies which were difficult to compare and further studies on RRC versus LRC with intracorporeal anastomosis are needed to understand the real value of each approach in right colonic.
Our analysis showed a tendency to a higher number of harvested lymph nodes during RRC, and this, together with a significantly reduced rate of conversions may indicate the advantage of using the robotic approach in performing the tissue dissection. However, it must be highlighted that these latter differences, even if significant, were minimal and they should be verified in future high quality randomized clinical trials.
Overall, time to first flatus was shorter in the robotic group. It must be considered that one of the included paper reported a large cohort from an ACS-NSQIP database [17]; this may have been associated with a great heterogeneity in approach, technique, and recovery pathways which may have affected the postoperative course. Still, differences in time to first flatus were not significant when extracorporeal anastomosis was performed in both the arms. This confirmed the superiority of intracorporeal anastomosis in improving the recovery of the bowel function. Costs, which were significantly higher for robotic procedures, may be the only obstacle for a routine use of the robotic system. We expect that a faster bowel recovery and thus, a shorter hospital stay may decrease general costs for the robotic procedures. Nevertheless, we found no differences in hospital stay and persistent significantly higher costs in the robotic group. Again, this should be seen in light of the fact that among all the papers reporting data on costs [6, 7, 15, 16, 18] only Park et al. [6] performed intracorporeal anastomosis in the robotic group and thus, there could be a benefit in terms of costs only for a negligible number of patients.
This meta-analysis presents a few limitations. First, it included only one randomized controlled trial as the remaining were only retrospective comparative series. Second, most of the papers (also the RCT) presented an intergroup difference in terms of the technique used to perform the anastomosis which could have significantly biased the comparison between the groups. Third, operative and postoperative outcomes of few of the included studies, might be affected by learning curve and results of this meta-analysis should be interpreted also in light of this variable. Finally, the data on surgery-related costs were still based on a limited number of procedures from different health systems and results from this study still need to be confirmed by further cost–benefit analysis. In conclusion, RRC can be regarded as a feasible and safe technique. Its superiority in terms of postoperative recovery should be confirmed by further large prospective series comparing RRC and LRC performed with the same anastomotic technique. In terms of costs, RRC seemed to be a more expensive procedure than LRC.
References
Formisano G, Misitano P, Giuliani G, Calamati G, Salvischiani L, Bianchi PP (2016) Laparoscopic versus robotic right colectomy: technique and outcomes. Updates Surg 68(1):63–69. https://doi.org/10.1007/s13304-016-0353-4
Zerey M, Hawver LM, Awad Z, Stefanidis D, Richardson W, Fanelli RD (2013) SAGES evidence-based guidelines for the laparoscopic resection of curable colon and rectal cancer. Surg Endosc 27(1):1–10. https://doi.org/10.1007/s00464-012-2592-x
Casillas MA Jr, Leichtle SW, Wahl WL, Lampman RM, Welch KB, Wellock T, Madden EB, Cleary RK (2014) Improved perioperative and short-term outcomes of robotic versus conventional laparoscopic colorectal operations. Am J Surg 208(1):33–40. https://doi.org/10.1016/j.amjsurg.2013.08.028
deSouza AL, Prasad LM, Park JJ, Marecik SJ, Blumetti J, Abcarian H (2010) Robotic assistance in right hemicolectomy: is there a role? Dis Colon Rectum 53(7):1000–1006. https://doi.org/10.1007/DCR.0b013e3181d32096
Deutsch GB, Sathyanarayana SA, Gunabushanam V, Mishra N, Rubach E, Zemon H, Klein JD, Denoto G 3rd (2012) Robotic vs. laparoscopic colorectal surgery: an institutional experience. Surg Endosc 26 (4):956–963. https://doi.org/10.1007/s00464-011-1977-6
Park JS, Choi GS, Park SY, Kim HJ, Ryuk JP (2012) Randomized clinical trial of robot-assisted versus standard laparoscopic right colectomy. Br J Surg 99(9):1219–1226. https://doi.org/10.1002/bjs.8841
Rawlings AL, Woodland JH, Vegunta RK, Crawford DL (2007) Robotic versus laparoscopic colectomy. Surg Endosc 21(10):1701–1708. https://doi.org/10.1007/s00464-007-9231-y
Lorenzon L, Bini F, Balducci G, Ferri M, Salvi PF, Marinozzi F (2016) Laparoscopic versus robotic-assisted colectomy and rectal resection: a systematic review and meta-analysis. Int J Colorectal Dis 31(2):161–173. https://doi.org/10.1007/s00384-015-2394-4
Petrucciani N, Sirimarco D, Nigri GR, Magistri P, La Torre M, Aurello P, D’Angelo F, Ramacciato G (2015) Robotic right colectomy: a worthwhile procedure? Results of a meta-analysis of trials comparing robotic versus laparoscopic right colectomy. J Minim Access Surg 11(1):22–28. https://doi.org/10.4103/0972-9941.147678
Rondelli F, Balzarotti R, Villa F, Guerra A, Avenia N, Mariani E, Bugiantella W (2015) Is robot-assisted laparoscopic right colectomy more effective than the conventional laparoscopic procedure? A meta-analysis of short-term outcomes. Int J Surg 18:75–82. https://doi.org/10.1016/j.ijsu.2015.04.044
Xu H, Li J, Sun Y, Li Z, Zhen Y, Wang B, Xu Z (2014) Robotic versus laparoscopic right colectomy: a meta-analysis. World J Surg Oncol 12:274. https://doi.org/10.1186/1477-7819-12-274
Zarak A, Castillo A, Kichler K, de la Cruz L, Tamariz L, Kaza S (2015) Robotic versus laparoscopic surgery for colonic disease: a meta-analysis of postoperative variables. Surg Endosc 29(6):1341–1347. https://doi.org/10.1007/s00464-015-4197-7
Delaney CP, Lynch AC, Senagore AJ, Fazio VW (2003) Comparison of robotically performed and traditional laparoscopic colorectal surgery. Dis Colon Rectum 46(12):1633–1639. https://doi.org/10.1097/01.DCR.0000098941.42470.D9
Shin JY (2012) Comparison of short-term surgical outcomes between a robotic colectomy and a laparoscopic colectomy during early experience. J Korean Soc Coloproctol 28(1):19–26. https://doi.org/10.3393/jksc.2012.28.1.19
Davis BR, Yoo AC, Moore M, Gunnarsson C (2014) Robotic-assisted versus laparoscopic colectomy: cost and clinical outcomes. J Soc Laparoendosc Surg 18(2):211–224. https://doi.org/10.4293/108680813X13753907291035
de’Angelis N, Lizzi V, Azoulay D, Brunetti F (2016) Robotic versus laparoscopic right colectomy for colon cancer: analysis of the initial simultaneous learning curve of a surgical fellow. J Laparoendosc Adv Surg Tech A 26(11):882–892. https://doi.org/10.1089/lap.2016.0321
Dolejs SC, Waters JA, Ceppa EP, Zarzaur BL (2016) Laparoscopic versus robotic colectomy: a national surgical quality improvement project analysis. Surg Endosc. https://doi.org/10.1007/s00464-016-5239-5
Kang J, Park YA, Baik SH, Sohn SK, Lee KY (2016) A comparison of open, laparoscopic, and robotic surgery in the treatment of right-sided colon cancer. Surg Laparosc Endosc Percutan Tech 26(6):497–502. https://doi.org/10.1097/SLE.0000000000000331
Lujan HJ, Plasencia G, Rivera BX, Molano A, Fagenson A, Jane LA, Holguin D (2017) Advantages of robotic right colectomy with intracorporeal anastomosis. Surg Laparosc Endosc Percutan Tech. https://doi.org/10.1097/SLE.0000000000000384
Trastulli S, Coratti A, Guarino S, Piagnerelli R, Annecchiarico M, Coratti F, Di Marino M, Ricci F, Desiderio J, Cirocchi R, Parisi A (2015) Robotic right colectomy with intracorporeal anastomosis compared with laparoscopic right colectomy with extracorporeal and intracorporeal anastomosis: a retrospective multicentre study. Surg Endosc 29(6):1512–1521. https://doi.org/10.1007/s00464-014-3835-9
Moher D, Liberati A, Tetzlaff J, Altman DG (2010) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg 8(5):336–341. https://doi.org/10.1016/j.ijsu.2010.02.007
Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, McQuay HJ (1996) Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials 17(1):1–12. https://doi.org/10.1016/0197-2456(95)00134-4
Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J (2003) Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg 73(9):712–716. https://doi.org/10.1046/j.1445-2197.2003.02748.x
Freeman MF, Tukey JW (1950) Transformations related to the angular and the square root. Ann Math Statist (4):607–611. https://doi.org/10.1214/aoms/1177729756
Hozo SP, Djulbegovic B, Hozo I (2005) Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol 5(1):13. https://doi.org/10.1186/1471-2288-5-13
Higgins JPT, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ 327(7414):557–560
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Drs. Leonardo Solaini, Francesca Bazzocchi, Davide Cavaliere, Andrea Avanzolini, Alessandro Cucchetti, and Giorgio Ercolani have no conflicts of interest or financial ties to disclose.
Rights and permissions
About this article

Cite this article
Solaini, L., Bazzocchi, F., Cavaliere, D. et al. Robotic versus laparoscopic right colectomy: an updated systematic review and meta-analysis. Surg Endosc 32, 1104–1110 (2018). https://doi.org/10.1007/s00464-017-5980-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-017-5980-4