
Abstract
EQ-5D is becoming the preferred instrument to measure health-state utilities involved in health technology assessment. The objective of this study is to assess the state of EQ-5D research in musculoskeletal disorders in 8 Central and Eastern European countries and to provide a meta-analysis of EQ-5D index scores. Original research articles published in any language between Jan 2000 and Sept 2016 were included, if they reported any EQ-5D outcome from at least two musculoskeletal patients from Austria, Bulgaria, the Czech Republic, Hungary, Poland, Romania, Slovakia, or Slovenia. Risk of bias was assessed with the Cochrane Collaboration’s tool. Twenty-nine articles (5992 patients) were included on rheumatoid arthritis (n = 7), osteoporosis (n = 5), chronic pain (n = 5), osteoarthritis (n = 4), ankylosing spondylitis (n = 2), psoriatic arthritis (n = 2), total hip replacement (n = 2), and scleroderma (n = 2). Low back pain was under-represented, while studies in neck pain, systemic lupus erythematosus, gout, and childhood disorders were lacking. EQ-5D index scores were reported in 24 studies, while the version of the instrument and the value-set was not specified in 41% and 46% of the articles, respectively. Meta-analysis was performed on 24 disease states involving 6876 observation points. Intervention effect was reported in 22 subgroups, out of which risk of bias was low in 41%. This review provides recommendations to improve reporting standards of EQ-5D results and highlights potential areas for future research. Coordinated research in conditions with greatest public health impact as well as a development of a regional value-set could provide locally relevant health-state utilities that are transferable among countries within the region.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Due to population ageing, musculoskeletal disorders have become important drivers of disease burden in high-income countries. The global increase of disability adjusted life years (DALYs) has been the highest in musculoskeletal disorders among all disease categories between 2005 and 2013 both in absolute and relative terms [1]. Low back and neck pain rank among all disease burden causes first in Slovenia, second in Austria, Czech Republic and Slovakia, and third in Bulgaria, Hungary, Poland, and Romania [1]. Musculoskeletal disorders are responsible for an estimated total of 635 000 DALYs in the selected eight countries [2, 3].
Biological drugs are available for the treatment of several musculoskeletal disorders, including rheumatoid arthritis (RA), ankylosing spondylitis (AS), psoriatic arthritis (PsA), osteoporosis (OP), and systemic lupus erythematosus (SLE). Being a significant cost driver in these conditions and causing a significant budget impact [4,5,6,7], the entry of biological drugs has speeded up research on patient reported outcome (PRO) measures as well as health economic evaluations in the field of rheumatology [8, 9]. While disease-specific PROs (e.g., Bath Ankylosing Spondylitis Activity Index—BASDAI, Health Assessment Questionnaire Disability Index—HAQ-DI) became key elements of medical decision-making, generic health-state measures such as SF-36 or EQ-5D have been intensively studied to support health economic analyses and financial decision-making in rheumatology [10, 11].
The EQ-5D questionnaire consists of two parts [12, 13]. The descriptive system assesses the current self-reported health status in five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. In the EQ-5D-3L version, there are three response categories resulting in 243 distinct health-state descriptions. To increase its responsiveness and sensitivity, a five-level version of the EQ-5D has been developed (EQ-5D-5L) [14], and there is a youth-version for assessing children and adolescents (EQ-5D-Y). The second part is a 20-cm visual analogue scale (EQ VAS) ranging from 0 (worst imaginable health) to 100 (best imaginable health) [15]. The EQ-5D index score (health-state utility value) is derived by attaching the preference weight of the general population to each distinct health state. The terms EQ-5D index score, EQ-5D utility, or health-state utility will be used interchangeably in this text. The EQ-5D index score of 1 represents perfect health, 0 represents death, and negative values represent “worse than dead” health states. The EuroQol Group provides guidelines about using the different versions of EQ-5D and presenting results [15]. The standard reporting involves the EQ-5D index score, the EQ VAS score, and the percentage of responses across the five health dimensions (health profile). Alternative reporting methods have also been suggested, although these have not been widely established yet [16].
As a generic health-state measure, EQ-5D makes possible the comparison of disease burden between patients and the general population, enables analyses across different diseases and provides preference weights (utilities) to each specific health state.
Health-state utilities are used to calculate quality-adjusted life years (QALYs), a measure that incorporates survival time and changes in quality of life expressed in utilities. In cost-utility analyses, incremental health benefits in QALYs are analyzed in the light of incremental costs to inform decision-makers about the value of new medical strategies [17]. Over the past decade, formal health technology assessment (HTA) meeting international standards has been implemented with proper institutional background in most CEE countries [18]. HTA provides information about the medical, social, economic, and ethical issues related to the use of a health technology. EQ-5D has been the preferred tool to calculate QALYs by the HTA guidelines in the majority of CEE countries [19]. With the development of HTA implementation in CEE countries, the need for local data generation on health-state utilities is increasing also in rheumatology [19].
This research has two objectives: first, to systematically review the EQ-5D literature generated in musculoskeletal disorders in eight selected CEE countries and to analyze the scope of studies and quality of reporting; second, to synthesize the available health-state utility data via meta-analysis and describe the quality of life (QoL) in various musculoskeletal disorders for baseline clinical populations and patients treated with biologicals in a real-life setting. Results aim to support research planning in rheumatology by revealing the areas in which EQ-5D data are deficient, convergent, or contradictory in the region. Authors and editors of both international and local journals can make use of the quality checking experiences to improve their standards for EQ-5D publications. Summary of EQ-5D utilities can help QALY estimations and transferability studies in health economic analyses.
Methods
Search strategy
This study builds on a systematic review of EQ-5D studies in Central and Eastern Europe (CEE) between 2000 and 2015 [19], and focuses on diseases of the musculoskeletal system and connective tissue (International Classification of Diseases ICD-10, Chapter XIII: M00–M99) [20]. We have updated the systematic search for the period between 1st July 2015 and the 1st Sept 2016 applying the same methodology. In brief, MEDLINE via PubMed, EMBASE, Web of Science, CINAHL, PsychINFO, the Cochrane Library, and the EuroQol Group databases [21] were searched using the combination of the following terms: (euroqol OR euro qol OR Eq 5d OR Eq-5d OR eq-5d) AND (Austria* OR Bulgaria* OR Hungar* OR Czech OR Poland OR Polish OR Romania* OR Slovak* OR Sloven*). Building on their country-expertise, authors (A.R., D.G., F.R., G.P., J.S., J.Z., M.P., and V.P.R.) have conducted a hand-search in non-indexed local rheumatology papers or local databases.
Inclusion and exclusion criteria of publications
Studies were included without language restrictions. The PRISMA checklist for reporting systematic reviews was followed [22]. Full-text journal articles that met the following criteria were included in the review: (1) the study was conducted on patients with a musculoskeletal or connective tissue disorder, (2) the study population originated from Austria, Bulgaria, the Czech Republic, Hungary, Poland, Romania, Slovakia, or Slovenia, (3) the article reported an EQ-5D outcome (EQ-5D index, health profile, or EQ VAS score) on more than two patients, and (4) the study represented an original research on a pediatric or adult population. Multi-country studies were excluded if relevant country-level data were not reported. In case of duplicate reports from the same study population, the one with more data was included. Abstracts and full-text articles were assessed for eligibility by two independent investigators (Z.Z. and M.P.)
Main outcome variables
A Microsoft Excel spreadsheet was developed for data extraction. General characteristics of the publications (year of publication, language, and source of funding), study methodology (data collection, study setting, design, and duration), study population (sample size, demographics, diagnosis, disease duration, and subgroups by disease state or treatment), version of the EQ-5D questionnaire (EQ-5D-3L, EQ-5D-5L, and EQ-5D-Y), value-sets used, EQ-5D results reported (health profiles, index, and EQ VAS scores), and other relevant outcome measures were recorded. In addition, EQ-5D utility values were collected by patient subgroups. Data extraction was performed by F.R., L.G., and Z.Z., and reviewed by M.P.
Qualitative analysis and risk of bias assessment
The methodology and reporting quality of EQ-5D studies were matched to the EuroQol guidelines [15]. In studies which reported a treatment effect measured by EQ-5D index score (either versus a control group in a randomized controlled trial, or as a non-randomized cohort versus baseline, or as a comparison of subgroups in a cross-sectional design), general risk of bias was assessed using the Cochrane Collaboration’s tool [23]. Selection (sequence generation/allocation concealment), performance (blinding of participants and personnel), detection (blinding of outcome assessment), attrition (incomplete outcome data), reporting, and other bias were assessed with respect to EQ-5D index scores by each subgroup, and studies as well as outcomes by subgroups were categorized as low, high, or unclear risk of bias. Risk of bias assessment was performed by Z.Z. and M.P.
Statistical analysis and meta-analysis of EQ-5D index scores
For summarizing the study characteristics, descriptive statistics were applied. When combining patient groups within the same study, weighted means were calculated for demographics and EQ-5D index scores. Where not reported, standard deviations were obtained from confidence intervals, interquartile ranges, or ranges [23]. Missing standard deviations were imputed from studies with closest possible match in terms of patient group and sample size.
To reflect the clinical and methodological heterogeneity of studies, the following patient subgroups were developed.
-
Ankylosing spondylitis (AS): biologic therapy and synthetic disease modifying antirheumatic drug (sDMARD).
-
Chronic pain: baseline score of prospective studies involving patients with shoulder pain and low back pain.
-
Osteoarthritis (OA): baseline score of prospective studies involving patients with hand OA, knee OA, and hip OA.
-
Osteoporosis (OP): no fracture, fracture within 2 months, after fracture separately for upper limb, hip, and vertebral fractures.
-
Psoriatic arthritis (PsA): biologic therapy, traditional systemic therapy, and no systemic therapy.
-
Rheumatoid arthritis (RA): biologic therapy (≥3 months) and non-biological therapy.
-
Scleroderma (SCL): localized SCL and systemic sclerosis (SSC).
Reported EQ-5D index scores of alternative subgroups such as disease severity, age groups, or resource utilization were not included in the meta-analysis. Both follow-up time in cohorts and inclusion criteria in cross-sectional studies were considered when setting time criteria for selected patient groups in OP and RA. Follow-up results of studies reporting the effect of balneotherapy and mud therapy were not included in the quantitative synthesis due to the lack of feasible subgroups from the highly diverse patient populations and interventions.
According to the comments of the Cochrane Handbook, we assumed potentially limited value of testing statistical heterogeneity formally [23]. Therefore, based on the known clinical and methodological heterogeneity of the studies, a random-effects meta-analysis was performed using the DerSimonian and Laird method [24]. Analysis of results was conducted by M.P., V.B., P.B., and Z.Z. All authors reviewed and commented the manuscript.
Results
Search results
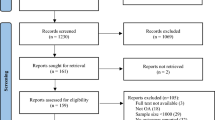
The results of the study selection process and reasons of exclusion are detailed in Fig. 1. According to a systematic review, 143 articles on EQ-5D were published between 2000 and 1st July 2015 [19], from which 23 publications were identified as musculoskeletal disorders. The electronic search of databases provided 117 additional articles on EQ-5D up to 1st Sept 2016, out of which 11 studies were conducted on musculoskeletal disorders, four met the predefined inclusion criteria, and additional two papers [25, 26] were identified through hand-search in non-indexed journals. Overall, 29 papers were included in the qualitative synthesis. Six publications [27,28,29,30,31,32] (including both total hip replacement (THR) studies [28, 32]) did not report EQ-5D utility values, so the meta-analysis of utility results was performed on 23 studies.

PRISMA flowchart of study selection. Searched: 1 Sept 2016
Distribution of studies by time, countries, and diagnoses
Among the 29 included studies, the first was published in 2003. There was a noted increase in publication activity concerning EQ-5D in the past 5 years, as 76% of studies have been published since 2012 (Table 1). The number of studies by diagnoses and countries is presented in Fig. 2. Most studies (n = 7, 24%) were performed in RA [26, 33,34,35,36,37,38], followed by OP (n = 5, 17%) [31, 39,40,41,42] and chronic pain (n = 5, 17%) [27, 29, 30, 43, 44]. While 18 studies originated from Hungary (62%), no studies were found in Romania.

Number of studies and cumulative sample size by diagnoses and by country
Study design, interventions, and bias assessment
The main characteristics of the included studies are summarized in Table 1. The majority were prospective cohorts (n = 13, 45%) [26, 27, 29,30,31,32,33, 38,39,40,41, 50, 52] and cross-sectional studies (n = 9, 31%) [25, 34, 35, 37, 42, 49, 51,52,53]. Only two studies (7%) analyzed data from patient registries. Two papers (7%) missed to report the setting.
Treatment effects were measured in 21 studies. Six RCTs involving a total of 319 patients focused on OA (n = 4) and chronic pain (n = 2), examining the effect of balneotherapy (n = 5) [43,44,45,46,47] or mud therapy (n = 1) [48]. All RCTs were conducted in Hungary. The effect of biological therapy was measured in two cross-sectional [34, 52] and five prospective [33, 34, 36, 38, 50] studies (including the two registries) in RA [26, 33, 34, 36, 38], AS [50] and PsA [52]. Other drug treatments and surgical therapy were assessed in two studies [31, 41] and four studies [27, 28, 32, 40], respectively. Physical therapy [29] and magnetic field therapy [30] were also evaluated in two smaller studies. From the 22 distinct patient subgroups, where the EQ-5D index score was measured either before or after an intervention, risk of bias was assessed as low in nine subgroups (41%) [40, 41, 43,44,45,46,47,48] mainly due to involving only baseline data, and potentially high in 13 subgroups (59%) [33, 34, 36, 38, 40, 50, 60] due to measuring the effect in open-label design (Table 3).
There was no specific intervention measured in the other 8 studies involving altogether 2001 patients [25, 35, 37, 39, 42, 49, 51, 53] (Table 2).
The source of funding was not reported in 8 studies (28%), and 7 studies (24%) were conducted without funding. The industry sponsored 4 studies, one study was jointly funded by a foundation and the industry, and 9 studies (31%) were reportedly funded by independent bodies.
Summary of EQ-5D reports
The 29 papers reported 306 distinct EQ-5D outcomes (any outcome, any time-point) in 95 different patient subgroups, out of which 23 papers (79%) reported a total of 131 EQ-5D index scores in 87 different patient groups (4147 patients). Table 2 summarizes the EQ-5D reports by publication. Repeated measurements provided a total of 12 026 individual EQ-5D index score data points. In addition, one paper reported the pre- and post-treatment change of EQ-5D index score as a healthcare indicator in 9 hospitals [32]. Furthermore, EQ VAS results and health profiles were reported in 21 (72%) and 5 (17%) articles, respectively. All the three standard EQ-5D outcomes were reported simultaneously in only 4 papers (14%) [25, 36, 49, 52]. One paper [38] reported additional EQ-5D results, such as percentage of patients having negative utilities (worse than dead), percentage of patients achieving minimally important difference in index change, and the effect size of index change. Accumulated QALY gain was calculated in two articles [38, 39]. In three publications, alternative EQ-5D outcomes [16] were reported: the average of the digit scores of the responses on the descriptive system was reported in two articles [28, 29] and the average score by each dimension in one article [31].
Most of the EQ-5D questionnaires were applied on-site (25 studies, 5321 patients) and majority of the on-site studies recorded EQ-5D data for all involved patients. Only three studies reported respondent rates of 97% [51], 86% [26], and over 99% [34]. Missing EQ-5D utilities of 12 cases from two studies [25, 51] were not indicated in the publication sample sizes (Table 1), but were reflected in the number of EQ-5D index observations in the meta-analysis (Table 3).
The EQ-5D version was specified in 17 articles (59%): 16 used the EQ-5D-3L, and one the EQ-5D-5L [25]. Out of the 12 studies (41%) which did not specify the instrument, 10 reported EQ-5D index scores [26, 33, 40, 43,44,45,46,47,48, 53]. From the 24 publications which reported EQ-5D index scores, the UK time trade-off (TTO) value-set was used in 9 cases, the UK value-set without specifying the valuation method in two cases [36, 50], one study used the Slovene VAS-based value-set [32] and another the European VAS-based value-set [49]. Eleven articles (46%) did not report the value-set used for the EQ-5D index calculation [26, 33, 35, 40, 41, 43,44,45,46,47,48].
Meta-analysis of health-state utility results (EQ-5D index score)
Out of the total 131 reported EQ-5D outcome subgroups from 12 026 patient observations, 58 subgroups (44%) involving 6876 patient observations (57%) were included in the meta-analysis. Altogether, 28 subgroups (685 patient observations) from 5 studies were excluded due to assessing the effect of balneotherapy or mud therapy [43,44,45,46, 48, 51], one subgroup involving 823 patient observations [38] was excluded due to not meeting the required follow-up time, 7 groups from 6 studies [33, 34, 41, 50, 52, 53] involving 1810 patient observations were excluded due to reporting mixed groups of patient populations, and 37 subgroups from 7 articles [25, 35, 37, 40, 42, 50, 51] involving 1832 patient observations were excluded due to a different split of patients from the predefined criteria.
Baseline values of the active and control treatment groups were combined in 6 studies [43,44,45,46,47,48], the baseline before different osteoporotic fracture locations was combined in one study [39], and distal and proximal arm fractures [42] and subtypes of systemic sclerosis [53] were also combined in two studies. Three subgroups from two studies, which did not meet the predefined criteria, were added separately to the results. One study reported EQ-5D index scores of major osteoporotic fractures before and after surgical intervention [40] without further specifying the location, and another study reported a group of osteoporotic patients with a mixed history of fractures [41]. In two prospective cohort studies [33, 38], more than one follow-up measurement subgroups met the inclusion criteria and were included in the data synthesis. Altogether, in seven diagnoses, we formed 42 distinct patient groups and combined them into 24 disease states in the meta-analysis. The combined utility values by disease state are reported in Table 3.
Discussion
This systematic review includes 29 articles reporting EQ-5D index scores in 8 CEE countries between Jan 2000 and Sept 2016. The review highlights the diversity of reporting quality and provides recommendations for authors. In addition, a meta-analysis of EQ-5D index scores is provided in 24 musculoskeletal disease states involving 6876 patient observation points.
Although the significance of musculoskeletal disorders from a public health perspective was well reflected by their share within the overall EQ-5D research activity in the CEE region [19], the relative size of country or patient populations were not proportional across the 29 studies. The large majority of the studies were performed in Hungary, while no study was found from Romania. Austria was involved only in one international OP study [39]. With the existing local value-sets, population norms, and a large number of studies in other disease areas, Poland is the leader of EQ-5D research in the CEE region, while its contribution to musculoskeletal studies was relatively small with 125 involved patients (2%).
With seven conditions covered, Hungary led the number of diagnoses, while other countries covered one or two. The most studied diagnoses in the eight countries were RA and OP, which can be explained by the advances of drug therapy in these fields over the last decades. Interestingly, however, the greatest disease burden among musculoskeletal disorders is caused by low back pain [1], which was disproportionately under-represented in the sample. Although physiotherapy is a widespread and costly treatment modality [54], its effect assessed by EQ-5D was studied only in a small number of RCT’s [43,44,45,46,47,48]. EQ-5D data from some important areas were missing, such as neck pain, SLE, gout, or pediatric rheumatic diseases [juvenile idiopathic arthritis (JIA), scoliosis, and osteonecrosis]. Although one JIA study was found in Bulgaria in a multi-country survey, it was excluded from this analysis due to reporting the EQ-5D outcome of a single patient only, while recruitment was not successful in Hungary [55]. The scarcity of data from registries is a major gap in the region; the Czech ATTRA registry was the only that provided EQ-5D data. The pattern of authors suggested that some prolific research groups made significant contributions by conducting smaller cross-sectional studies or RCT’s, which hopefully will inspire other researchers in the region.
Based on our findings, we have summarized the most relevant points to consider in EQ-5D studies and data reporting in Table 4. Some further issues deserve mentioning. Age- and gender-matched comparisons with the general population can provide information on the burden related to a disease. Although representative population norms are available for Hungary, Slovenia, and Poland, and the city-norm of Burgas for Bulgaria [19], only one study [35] compared the EQ-5D utilities with population norms.
EQ-5D index scores depend on the valuation method used and significant differences have been demonstrated between countries; therefore, the choice of the value-set requires careful consideration. Transferring EQ-5D utilities between jurisdictions remains an important potential source of bias in health economic analysis [56]. For the same state with scores 21232 across the five health dimensions, the utility generated with VAS method is 0.294 with the UK value-set, 0.297 with the Slovenian one, while it is 0.424 with the Finnish one [57]. Moreover, the utility values of the EQ-5D-3L and the EQ-5D-5L differ significantly as well. Therefore, for the proper interpretation of results, studies that report EQ-5D utility values should specify which EQ-5D version and value-set were used. In our review, only 11 studies fulfilled these criteria. From the 10 studies, which did not specify the EQ-5D version, only one [53] was published before the development of EQ-5D-5L. As a result, data from 782 patients (2059 utility observations) can only be interpreted with limitations.
From the CEE region, national EQ-5D-3L value-sets are available in Slovenia and Poland. The Slovenian study [32] used the Slovenian value-set, while the Polish study [49] used the European one, despite the local value-set was available at the time of publication [58] and the Polish HTA Agency preferred reports using the local value-set [19]. In other clinical areas, the mixed use of UK, European VAS-based and local value-sets have been reported by countries [19]. Although both VAS- and TTO-based UK value-sets exist, in two articles, the valuation method could not be identified. The development of national value-sets could increase the local validity of data. However, in economic analyses, the lack of local utilities necessitates the transferring of results from other countries, and, if available, preferably a synthesis of results from multiple countries for larger sample size and improved precision. In such cases, for EQ-5D-3L data, the most commonly used UK value-set based on time trade-off (TTO) method (MVH A1) [59] may provide consistent and comparable results across countries. In the future, developing a CEE regional value-set could reflect both the specifics of regional population preferences while enabling the cross-border utilization of results [19].
We believe that one major advantage of this review is that it provides a collection of EQ-5D index scores obtained in the CEE region in seven musculoskeletal conditions. Most of the data, especially in the case of patient populations treated with biologicals, were generated in cross-sectional or open cohort real-world studies. Reimbursement restrictions often limit the use of biologicals to special populations in the CEE region [60]; therefore, the interpretation of the baseline data in these studies as well as the comparison with conventional therapies or data from other geographies requires caution.
In our study, the mean utility difference between AS patients treated with biological or the conventional therapy was 0.14. In RCTs of etanercept in AS, the QALY gain with EQ-5D was in the range of 0.2–0.24 [61, 62].
The utility difference in PsA between patients who receive biological therapy and those who do not receive systemic therapy was 0.12, while there was no difference between the biological and traditional systemic treatments. In a systematic review, the EQ-5D utility values of patients with psoriasis ranged between 0.52 and 0.9 [63]. Different severity of the skin conditions in the included PsA populations [51, 64] also needs to be considered, when interpreting the health utility results.
The utility difference between RA patient groups receiving sDMARD therapy or at least 3-month biological therapy was 0.39, which is relatively high compared to the results of similar Western-European cohort studies [65,66,67,68,69]. In the three open-cohort studies included in our review (81% of observations) [33, 36, 38], patients were initiated on biologicals, who had not responded to sDMARD therapy. Biological therapy is reimbursed in most CEE countries in severe patients with DAS28 scores ≥5.1, who frequently report health states associated with negative utilities [70]. The baseline data of these patients were included in the sDMARD group in our analysis. In the study of Závada et al. [38] and Péntek et al. [71], despite the similar DAS28 scores of 6.4 and 6.1, 60.5% and approximately 5% of patients reported extreme pain at the baseline, respectively. The corresponding difference between baseline and post-treatment EQ-5D index scores were 0.53 and 0.27, respectively. The relative sensitivity of the EQ-5D-3L UK value-set to extreme problems [57] (especially pain and mobility) may contribute to the marked difference of utility values between the biological and sDMARD groups in RA.
The utilities of baseline OA patients ranging between 0.48 and 0.61 were similar to results of other QoL studies in OA [72].
The interpretation of utilities in OP requires special care. The immediate dramatic effect of a major fracture on quality of life is probably best illustrated by the study of Dimitrov [40], demonstrating “worse than dead” (−0.28) average EQ-5D index score in men immediately prior surgery. Although the studies of Borgström et al. [39] and Vokó et al. [42] indicate considerable quality-of-life improvement in a few months after fractures, the post-fracture EQ-5D index levels remained lower by 0.08–0.13 than pre-fracture levels, with hip fractures having the greatest negative consequences. It has to be emphasized that these studies did not measure the increased mortality associated with major osteoporotic fractures, which is a major driver of QALYs lost due to OP [73].
The major limitation of the quantitative synthesis of this report, but also, one of the main findings is that nearly 66% of all observations provided incomplete information about the reported utility values, and originated from studies having potentially high bias. Although a variance measure is essential for the secondary use of EQ-5D index scores in economic analyses or meta-analyses, it was not reported and had to be imputed in three studies [33, 35, 50], involving 1336 observations, which is 19% of the data included in the meta-analysis in this report. Altogether, from the 23 articles included in the meta-analysis, only 9 (39%) provided correctly equally the EQ-5D version, the value-set, and the variance of the reported utilities. From these studies, only 4 were assessed as having low bias. Furthermore, despite the hand-search of non-indexed journals by local experts, some relevant research projects published in the grey literature may have been omitted from our review.
Conclusions
Musculoskeletal disorders are a prolific field of EQ-5D research within the CEE region both in terms of the number of publications, covered diagnoses, and involved patient numbers. The most studied areas were RA and OP, followed by chronic pain, OA, AS, PsA, THR, and SCL, which neither fully reflect the public health impact, nor the availability of expensive therapies for the respective disorders. Low back pain was under-represented, and important areas, such as neck pain, SLE, gout, and childhood disorders lacked EQ-5D studies. Research activity in countries seems to rather reflect the expertise and scientific agenda of individual research groups than the size of populations, overall health expenditure, or the state of development of local EQ-5D instruments. Most studies were conducted in Hungary, while no musculoskeletal studies were identified in Romania. Poland, the region’s most advanced country in terms of the availability of local EQ-5D instruments, was largely under-represented in the field of musculoskeletal disorders.
The large share of publications without specific funding indicates that EQ-5D is an easy-to-use and relatively inexpensive research tool for practicing physicians and health economists, yet EQ-5D studies can generate considerable value to the greater society even across country borders. Although there is a wealth of research using EQ-5D in a variety of conditions in the region, due to incomplete reporting of the results, the usefulness of the data for economic analysis was somewhat limited in many studies. To enable the proper interpretation and utilization of the data in health economic analyses, authors should pay attention to more elaborate reporting of EQ-5D results.
With the increasing demand for locally relevant, high-quality economic analyses in the CEE region, our findings call for the collection of regional utility studies in a systematic database, as well as a coordinated strategy in the generation of more well-designed utility studies to cover the gaps in high-disease-burden areas. A potentially cost-effective strategy may be a more widespread use of online data collection methods. Although the development of country-specific value-sets would be desirable, in the future, a CEE regional value-set could reflect both the specifics of regional population preferences, while enabling the cross-border transfer of results.
References
Collaborators GDaH, (2015) Global, regional, and national disability-adjusted life years (DALYs) for 306 diseases and injuries and healthy life expectancy (HALE) for 188 countries, 1990–2013: quantifying the epidemiological transition. Lancet 386(10009):2145–2191
Eurostat (2016) Population on 1 January. http://ec.europa.eu/eurostat/tgm/download.do?tab=table&plugin=1&language=en&pcode=tps00001
WHO (2004) Deaths and DALY estimates for 2004 by cause for WHO Member States: Persons, all ages. http://www.who.int/healthinfo/global_burden_disease/estimates_country/en/. Accessed 2016.09.08. 2006
Brodszky V, Bálint P, Géher P et al (2009) Disease burden of psoriatic arthritis compared to rheumatoid arthritis. Hungarian experiment. Rheumatol Int 30(2):199–205
Petříková A, Doležal T, Klimeš J, Vocelka M, Sedová L, Kolář J (2013) The economic burden of the ankylosing spondylitis in the Czech Republic: comparison between 2005 and 2008. Rheumatol Int 33:1813–1819
Brodszky V, Baji P, Balogh O, Péntek M (2014) Budget impact analysis of biosimilar infliximab (CT-P13) for the treatment of rheumatoid arthritis in six Central and Eastern European countries. Eur J Health Econ 15(Suppl 1):S65–S71
Boncz I, Sebestyén A (2006) Financial deficits in the health services of the UK and Hungary. Lancet 368(9539):917–918
Joensuu JT, Huoponen S, Aaltonen KJ, Konttinen YT, Nordstrom D, Blom M (2015) The cost-effectiveness of biologics for the treatment of rheumatoid arthritis: a systematic review. PLoS ONE 10(3):e0119683
Cawson MR, Mitchell SA, Knight C et al (2014) Systematic review, network meta-analysis and economic evaluation of biological therapy for the management of active psoriatic arthritis. BMC Musculoskelet Disord 15:26
Matcham F, Scott IC, Rayner L et al (2014) The impact of rheumatoid arthritis on quality-of-life assessed using the SF-36: a systematic review and meta-analysis. Semin Arthritis Rheum 44(2):123–130
Harrison MJ, Davies LM, Bansback NJ, Ingram M, Anis AH, Symmons DP (2008) The validity and responsiveness of generic utility measures in rheumatoid arthritis: a review. J Rheumatol 35(4):592–602
EuroQol G (1990) EuroQol–a new facility for the measurement of health-related quality of life. Health Policy 16(3):199–208
Brooks R (1996) EuroQol: the current state of play. Health Policy 37(1):53–72
Herdman M, Gudex C, Lloyd A et al (2011) Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res 20(10):1727–1736
EuroQol G (2016) EQ-5D Homepage. http://www.euroqol.org/home.html
Devlin NJ, Parkin D, Browne J (2010) Patient-reported outcome measures in the NHS: new methods for analysing and reporting EQ-5D data. Health Econ 19(8):886–905
Harrison MJ, Bansback NJ, Marra CA, Drummond M, Tugwell PS, Boonen A (2011) Valuing health for clinical and economic decisions: directions relevant for rheumatologists. J Rheumatol 38(8):1770–1775
Gulacsi L (2014) Health technology assessment in Poland, the Czech Republic, Hungary, Romania and Bulgaria. Eur J Health Econ 15:13–25
Rencz F, Gulacsi L, Drummond M et al (2016) EQ-5D in Central and Eastern Europe: 2000–2015. Qual Life Res Int J Qual Life Aspects Treatment, Care Rehabil 25(11):2693–2710
WHO (2016) International Statistical Classification of Diseases and Related Health Problems 10th Revision Version: 2016. http://apps.who.int/classifications/icd10/browse/2016/en. Accessed 14 Oct 2016
Search Engine for EuroQol and EQ-5D-related material. http://www.euroqol.org/eq-5d-publications/search.html. Accessed 09 Jan 2016
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 339:b2535
Higgins JPT, Green S, (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. (updated March 2011) The Cochrane Collaboration; 2011
DerSimonian R, Laird N (1986) Meta-analysis in clinical trials. Control Clin Trials 7(3):177–188
Péntek M, Czirjak L, Pfliegler G, et al. (2015.) Lokalizált scleroderma és szisztémás sclerosis betegséggel élők életminősége és betegségterhe: a BURQOL-RD európai felmérés magyarországi eredményei (Quality of life and burden of disease in localised scleroderma and systemic sclerosis: Hungarian results of the European BURQOL-RD study). Immunológiai Szemle VII. (4):21–9
Szűcs G, Gál J, Géher P, et al. (2015) A golimumab hatásossága és biztonságossága a betegség lefolyását módosító bázisterápiás szerek (DMARD-ok) mellett alkalmazva rheumatoid arthritisben: A GO-MORE vizsgálat magyarországi eredményei (Efficacy and safety of golimumab used in combination with disease modifying antirheumatic drugs (DMARDs) in rheumatoid arthritis: Hungarian results of the GO-MORE study). Immunológiai Szemle VII. (3):59–66
Khoshab HA, Sloboda T (2015) Minimal access spinal technologies (MAST) fusion procedures for the treatment of the degenerative lumbar spine (a part of multicentral prospective study). Case Report. Neuro Endocrinol Lett 36(3):231–235
Kiraly E, Gondos T (2012) Cardiovascular diseases and the health-related quality of life after total hip replacement. J Clin Nurs 21(19–20):2843–2850
Klemenc-Ketiš Z (2011) Disability in patients with chronic non-specific low back pain: validation of the Slovene version of the Oswestry disability index. Slov J Publ Health 50(2):87–94
Pasek J, Kwiatek P, Pasek T, Szajkowski S, Szewc A, Sieron A (2012) Application of magnetic field and visible light in the treatment of low back pain and sciatic neuralgia. Aktualnosci Neurologiczne 12(1):65–68
Rosa J, Vanuga P, Noskovic M, Ritomsky A (2004) Profile of patients presenting with postmenopausal osteoporosis treated with raloxifene. Osteol Bull 9(1):18–21
Rupel VP, Ogorevc M (2014) Use of the EQ-5D instrument and value scale in comparing health states of patients in four health care programs among health care providers. Val Health Reg Issues 4:95–99
Horak P, Skacelova M, Hejduk K, Smrzova A, Pavelka K (2013) Abatacept and its use in the treatment of rheumatoid arthritis (RA) in the Czech Republic-data from the ATTRA registry. Clin Rheumatol 32(10):1451–1458
Inotai A, Rojkovich B, Fulop A, Jaszay E, Agh T, Meszaros A (2012) Health-related quality of life and utility in patients receiving biological and non-biological treatments in rheumatoid arthritis. Rheumatol Int 32(4):963–969
Mészáros Á, Vincze Z (2003) Életminőség vizsgálata asthma bronchiálés és rheumatoid arthritises betegek körében. Orv Hetil 144(9):423–427
Pentek M, Gulacsi L, Rojkovich B, Brodszky V, van Exel J, Brouwer WB (2014) Subjective health expectations at biological therapy initiation: a survey of rheumatoid arthritis patients and rheumatologists. Eur J Health Econ 15(Suppl 1):S83–S92
Pentek M, Szekanecz Z, Czirjak L et al (2008) Impact of disease progression on health status, quality of life and costs in rheumatoid arthritis in Hungary. Orv Hetil 149(16):733–741
Závada J, Uher M, Vencovsky J, Pavelka K (2014) Assessment of utility score EQ-D and estimating the Cost-utility of the first year of treatment by TNF inhibitors in a cohort of patients with Rheumatoid Arthritis during—results from the Czech biologics registry ATTRA. Ceska Revmatol 22(1):10–16
Borgstrom F, Lekander I, Ivergard M et al (2013) The international costs and utilities related to osteoporotic fractures study (ICUROS)—quality of life during the first 4 months after fracture. Osteoporos Int 24(3):811–823
Dimitrov N, Goycheva P, Petrov D (2015) Assessment of health related quality of life in male patients with major osteoporotic fractures by two generic healt status indices: a preliminary study. J Balkan Tribol Assoc 21(3):585–593
Péntek M, Licker-Fóris E, Lovas K et al (2003) Az életminőség mérése postmenopausalis osteoporosisban szenvedő betegeknél. Ca és Csont 6(4):158–163
Voko Z, Inotai A, Horváth C, Bors K, Speer G, Kaló Z (2013) Csontritkulásban szenvedő betegek életminősége ([Quality of life of patients with osteoporosis in Hungary]). Lege Artis Medicinae KID 3(4):40–41
Tefner IK, Kovacs C, Gaal R et al (2015) The effect of balneotherapy on chronic shoulder pain. A randomized, controlled, single-blind follow-up trial. A pilot study. Clin Rheumatol 34(6):1097–1108
Tefner IK, Nemeth A, Laszlofi A, Kis T, Gyetvai G, Bender T (2012) The effect of spa therapy in chronic low back pain: a randomized controlled, single-blind, follow-up study. Rheumatol Int 32(10):3163–3169
Kovacs C, Bozsik A, Pecze M, et al. (2016) Effects of sulfur bath on hip osteoarthritis: a randomized, controlled, single-blind, follow-up trial: a pilot study. International journal of biometeorology
Kovacs C, Pecze M, Tihanyi A, Kovacs L, Balogh S, Bender T (2012) The effect of sulphurous water in patients with osteoarthritis of hand. Double-blind, randomized, controlled follow-up study. Clin Rheumatol 31(10):1437–1442
Kulisch A, Benko A, Bergmann A et al (2014) Evaluation of the effect of Lake Heviz thermal mineral water in patients with osteoarthritis of the knee: a randomized, controlled, single-blind, follow-up study. Eur J Phys Rehabil Med 50(4):373–381
Tefner IK, Gaal R, Koroknai A et al (2013) The effect of Neydharting mud-pack therapy on knee osteoarthritis: a randomized, controlled, double-blind follow-up pilot study. Rheumatol Int 33(10):2569–2576
Kawalec P, Malinowski K (2015) Disease activity, quality of life and indirect costs of reduced productivity at work, generated by Polish patients with ankylosing spondylitis. Reumatologia 53(6):301–308
Mlcoch T, Sedova L, Stolfa J, et al. (2016) Mapping the relationship between clinical and quality-of-life outcomes in patients with ankylosing spondylitis. Expert Rev Pharmacoecon Outcomes Res 1–9
Brodszky V, Pentek M, Balint PV et al (2010) Comparison of the Psoriatic Arthritis Quality of Life (PsAQoL) questionnaire, the functional status (HAQ) and utility (EQ-5D) measures in psoriatic arthritis: results from a cross-sectional survey. Scand J Rheumatol 39(4):303–309
Rencz F, Brodszky V, Pentek M et al (2014) Disease burden of psoriasis associated with psoriatic arthritis in Hungary. Orv Hetil 155(48):1913–1921
Minier T, Pentek M, Brodszky V et al (2010) Cost-of-illness of patients with systemic sclerosis in a tertiary care centre. Rheumatology (Oxford) 49(10):1920–1928
Jaromi M, Hanzel A, Endrei D et al (2014) Determination of the annual health insurance Cost Of outpatient care physiotherapy services For low back pain. Val Health J Int Soc Pharmacoecon Outcomes Res 17(7):A378
Kuhlmann A, Schmidt T, Treskova M et al (2016) Social/economic costs and health-related quality of life in patients with juvenile idiopathic arthritis in Europe. Eur J Health Econ 17(Suppl 1):79–87
Knies S, Evers SM, Candel MJ, Severens JL, Ament AJ (2009) Utilities of the EQ-5D: transferable or not? Pharmacoeconomics 27(9):767–779
Szende A, Oppe M, Devlin N (2007) EQ-5D value sets: inventory, comparative review and user guide. Springer
Golicki D, Jakubczyk M, Niewada M, Wrona W, Busschbach JJ (2010) Valuation of EQ-5D health states in Poland: first TTO-based social value set in Central and Eastern Europe. Val health J Int Soc Pharmacoecon Outcomes Res 13(2):289–297
Dolan P (1997) Modeling valuations for EuroQol health states. Med Care 35(11):1095–1108
Gulácsi L (2014) Biological and biosimilar therapies in inflammatory conditions: challenges for the Central and Eastern European countries. Eur J Health Econ 15:1–4
Boonen A, Patel V, Traina S, Chiou CF, Maetzel A, Tsuji W (2008) Rapid and sustained improvement in health-related quality of life and utility for 72 weeks in patients with ankylosing spondylitis receiving etanercept. J Rheumatol 35(4):662–667
Choi C-B, Kim T-J, Park H-J et al (2008) Safety and clinical responses in Ankylosing Spondylitis after three months of etanercept therapy. J Korean Med Sci 23(5):852–856
Møller AH, Erntoft S, Vinding GR, Jemec GBE (2015) A systematic literature review to compare quality of life in psoriasis with other chronic diseases using EQ-5D-derived utility values. Patient Related Outcome Meas 6:167–177
Rencz F, Hollo P, Karpati S et al (2015) Moderate to severe psoriasis patients’ subjective future expectations regarding health-related quality of life and longevity. J Eur Acad Dermatol Venereol 29(7):1398–1405
Russell AS, Conner-Spady B, Mintz A, Mallon C, Maksymowych WP (2003) The responsiveness of generic health status measures as assessed in patients with rheumatoid arthritis receiving infliximab. J Rheumatol 30(5):941–947
Bingham CO 3rd, Weinblatt M, Han C et al (2014) The effect of intravenous golimumab on health-related quality of life in rheumatoid arthritis: 24-week results of the phase III GO-FURTHER trial. J Rheumatol 41(6):1067–1076
Kievit W, Fransen J, Adang EM et al (2011) Long-term effectiveness and safety of TNF-blocking agents in daily clinical practice: results from the Dutch Rheumatoid Arthritis Monitoring register. Rheumatology (Oxford) 50(1):196–203
Gulfe A, Wallman JK, Kristensen LE (2016) EuroQol-5 dimensions utility gain according to British and Swedish preference sets in rheumatoid arthritis treated with abatacept, rituximab, tocilizumab, or tumour necrosis factor inhibitors: a prospective cohort study from southern Sweden. Arthritis Res Ther 18:51
Buitinga L, Braakman-Jansen LM, Taal E et al (2012) Comparative responsiveness of the EuroQol-5D and Short Form 6D to improvement in patients with rheumatoid arthritis treated with tumor necrosis factor blockers: results of the Dutch Rheumatoid Arthritis Monitoring registry. Arthritis Care Res (Hoboken) 64(6):826–832
Hurst NP, Kind P, Ruta D, Hunter M, Stubbings A (1997) Measuring health-related quality of life in rheumatoid arthritis: validity, responsiveness and reliability of EuroQol (EQ-5D). Br J Rheumatol 36(5):551–559
Pentek M, Rojkovich B, Czirjak L et al (2014) Acceptability of less than perfect health states in rheumatoid arthritis: the patients’ perspective. Eur J Health Econ 15(Suppl 1):S73–S82
Ruchlin HS, Insinga RP (2008) A review of health-utility data for osteoarthritis: implications for clinical trial-based evaluation. Pharmacoeconomics 26(11):925–935
Leboime A, Confavreux CB, Mehsen N, Paccou J, David C, Roux C (2010) Osteoporosis and mortality. Joint Bone Spine 77:S107–S112
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Fanni Rencz, Jakub Závada, Judit Simon, Valentin Brodszky, Petra Baji, Guenka Petrova László Gulácsi, and Márta Péntek have nothing to disclose. Zsombor Zrubka is a full-time employee of Sandoz Hungária Kft. The review is strictly the personal point of view of the author and it does not reflect the position of Sandoz. Dominik Golicki reports grants and non-financial support from EuroQol Group, outside the submitted work; and he is a member of the EuroQol Group, a not-for-profit organization that develops and distributes instruments that assess and value health. Valentina Prevolnik Rupel reports non-financial support from EuroQol Group, outside the submitted work; and she is member of the EuroQol Group, a not-for-profit organization that develops and distributes instruments that assess and value health. Alexandru Rotar is a salaried employee of Sanofi-Aventis Romania. The review is strictly the personal point of view of the author and it does not reflect the position of Sanofi-Aventis Romania.
Ethical approval
The study is a systematic review: for this type of study, formal consent is not required.
Human rights and animal welfare
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
The study is a systematic review: for this type of study, informed consent of participants is not required.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Rights and permissions
About this article

Cite this article
Zrubka, Z., Rencz, F., Závada, J. et al. EQ-5D studies in musculoskeletal and connective tissue diseases in eight Central and Eastern European countries: a systematic literature review and meta-analysis. Rheumatol Int 37, 1957–1977 (2017). https://doi.org/10.1007/s00296-017-3800-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00296-017-3800-8