
Abstract
The aim of the study was to demonstrate the effectiveness of sulphurous water in patients with osteoarthritis of the hand. Forty-seven patients with osteoarthritis of the hand were enrolled into the double-blind, randomized, controlled study, satisfying ACR criteria. One group of the patients (n = 24) received balneotherapy, bathing in sulphurous thermal water for 20 min per occasion, 15 times in all during a period of 3 weeks. The control group (n = 21) had a bath exclusively in warm tap water. Assessments were carried out in both groups on four occasions: at the beginning and at the end of the treatment, and 3 and 6 months after the beginning of the treatment. The parameters studied were the following: pain in the hand, morning stiffness in the joints, grip strength of both hands, and Health Assessment Questionnaire Disability Index (HAQ) and AUSCAN Hand Osteoarthritis Index and EuroQol quality of life questionnaire. At the end of treatment, the improvement was more pronounced in the patient group treated with the sulphurous water. After 3 months, significant improvement could be detected in all parameters, except the morning stiffness and EQ5D. After 6 months, the values of pain, HAQ and AUSCAN continued to be significantly better in comparison with the baseline values. The improvement in quality of life was significant only at the end of the treatment, 6 months later not any longer. The difference between the two groups was significant after 3 months in point of pain and EQVAS. Balneotherapy and within this the sulphurous spa water alone may be effective for the attenuation of pain in patients with hand osteoarthrosis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Symptomatic hand osteoarthritis is a common musculoskeletal disorder, its prevalence being 15.9 % in women and 8.2 % in men in a population aged 58.9 (±9.9) years [1]. This disease is characterized by pain, stiffness and impairment in hand function, deterioration in handgrip strength, and the latter could decrease below the 60 % of the normal value [2]. The disease typically affects the distal and proximal interphalangeal, and the first carpometacarpal joints.
The course of the disease is less clear, but available data show that the whole joint is affected by osteoarthritis [3]. At present there do not exist such therapeutic methods that are able to modify the structure, and the studies related to symptomatic treatment are scarce [4, 5]. Balneotherapy is used usually only in countries rich in spa water. In recent decades, numerous papers appeared which proves the effectiveness of balneotherapy in musculoskeletal disorders [6–9]. With the present study, the authors wish to evaluate the effectiveness of balneotherapy in hand osteoarthritis.
Patients and methods
The outpatients of Mezőkövesd Musculoskeletal Rehabilitation Centre were enrolled into the study. Twenty-four patients (male/female, 1:23) had bath in sulphurous water (balneotherapy group), while 21 patients (male/female, 2:19) had bath in tap water (control group). The assessments took place on four occasions: at the beginning and at the end of study, and 3 and 6 months after the therapy. Neither the patients nor the investigators knew the distribution of the two groups. A computerized randomization took place; the patients got identification numbers when they were enrolled into the study. The randomization was made by an independent person. The result of the randomization was known exclusively by the physiotherapy assistant working in the bath who filled the bathtubs with spa water or tap water. The bathtubs could be filled both with spa water and with tap water, so balneotherapy could have happened in any bathtubs. Patients sitting in the bath were holding only their heads out of the water while hands were kept in the water. The sulphurous smell that could be perceived everywhere in the bath was deceptive for the control group. Both the balneotherapy group (n = 24) and the control group (n = 21) spent 20 min per occasion in the bathtub, in all 15 times during a period of 3 weeks. The temperature of the spa water and that of the tap water was 37 °C. The period of balneotherapy was measured and certified by the physiotherapy assistant. During the study period, the patients did not receive any other physiotherapy on their hands.
Inclusion criteria
Osteoarthritis of the hand was diagnosed according to the 1990 criteria of the American College of Rheumatology [10]. Inclusion criteria included Kellgren–Lawrence radiographic grade ≥2 in at least two joints and ≥30 mm hand pain as assessed by the visual analog pain scale [11].
Exclusion criteria
Patients younger than 45 years of age and older than 75 years were excluded from the study. Further exclusion criteria were: erosive or secondary hand osteoarthritis, inflammatory rheumatic disorders, psoriasis, gout, carpal tunnel syndrome, trigger finger, tendovaginitis and fibromyalgia. The patients could not receive balneotherapy in the last 9 months; they could not get steroid injection into the small joints of hands in the last 3 months, or injection of a hyaluronate in the last 6 months; and they could not take symptomatic slow-acting drugs in the last 3 months either. During the study period, the patients did not get any other therapy for hand pain than balneotherapy, they did not take non-steroid drugs. For other pain occurring eventually, they were allowed to take paracetamol or metamisole.
Composition of the thermal water
The spa water of Mezőkövesd belongs to the group of sulphurous spa waters, its content of sulphide ion (13.2 mg/L) is the highest in Hungary [12]. In addition, this spa water contains a significant amount of calcium, magnesium, bicarbonate and sodium chloride as well (Table 1). The permission necessary to carry out the study was received from the regional ethics committee (license number: 01-03-2009).
Study parameters
The parameters studied were as follows:
-
Hand pain measured by visual analogue scale (0–100), morning joint stiffness (MJS) based on the self-report of patients (in minutes) and the grip strength of hands measured by Dyna-9 dynamometer (in newtons).
-
The grip strength of both hands was measured three times; the final result was the average of three measurements [13].
In addition, completion of the following questionnaires took place:
-
Health Assessment Questionnaire Disability Index (HAQ-DI), Australian/Canadian Osteoarthritis Hand Index Likert-scaled Format (AUSCAN LK3.1) and EuroQol (EQ-5D/EQ VAS), and quality of life questionnaire. The Health Assessment Questionnaire (HAQ) is the functional index of rheumatoid arthritis; however, it is usable in hand osteoarthritis, as well [11, 14].
-
The AUSCAN is a three-dimensional, self-administered questionnaire specific for the osteoarthrosis of the hand. A higher score indicates greater impairment [15]. The AUSCAN can be used only with license. We have received the authorization necessary to use the Hungarian version of the questionnaire. The EQ-5D quality of life questionnaire consists of two parts. The first part contains items referring to five dimensions of life quality; the second part is a visual analog scale (EQVAS), by which patients self-report their actual health state [16].
-
Primary endpoint is that the pain decreases, and hand functions increase at the end of treatment, and 3 and 6 months later.
-
Secondary endpoint is to improve quality of life.
Statistics
The statistical analyses were made using SPSS 15.0 software. Regarding the data gained at the beginning of the study, the Kolmogorov–Smirnov test was used as a normality test, and the Mann–Whitney test was used as homogeneity test. The changes in state were assessed comparing the data to the baseline data or the data gained earlier (Wilcoxon test).
Comparison of data of the two groups was done by Mann–Whitney test and GLM repeated measures analysis. Taking into account the Bonferroni correction significant result, we appplied p value <0.008 (5 %/6 = 0.8 %).
Results
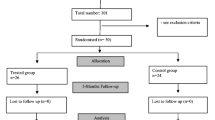
Patients were recruited by the family doctor in the Mezőkövesd rural area and sent to Mezőkövesd Muscolosceletal Rehabilitation Center, where the rheumatologist screened 60 patients for the study. The recruitment period was between May 2009 and May 2010. A total of 47 patients (male/female, 4:43) were randomised, of which 2 subjects dropped out during the treatment process for family reasons. Balneotherapy did not have to be interrupted because of side effects in any case (Fig. 1). During the whole period of the study, adverse event was not reported.

The disposition of patients
The data of the two groups at the beginning of the study are indicated in Table 2. The baseline characteristics were similar between the two groups. The balneotherapy group showed significant improvement in every parameter under the scope of the study at the end of the treatment. The improvement was pronounced also regarding pain, MJS, the grip strength, the AUSCAN, the HAQ and the EQVAS (p < 0.001). After 3 months, the improvement remained significant with the exception of MJS and EQ5D. After 6 months, all the parameters still showed significant improvement in comparison with the baseline, except the MJS, the grip strength and the EuroQol.
The control group showed significant improvement in every parameter, except pain, HAQ, EuroQol (EQ5D+EQVAS), at the end of the treatment; however, this improvement was less expressed than in the balneotherapy group. After 3 and 6 months, no improvement could be detected in any parameter in the group that had bath in the tap water.
The difference between the two groups was significant after the bath in point of pain (VAS) and 3 months later both in point of pain (VAS) and of health state (EQVAS), but it was not significant in the point of MJS, grip strenght, HAQ-DI, AUSCAN and EQ5D (Table 3). In the aspect of pain, a significant difference was experienced in the course of this assessment betweeen the two groups by GLM repeated measures analysis (Table 4). The number needed to treat (NNT) is 5,6 patients [95 % CI 2.28–10].
Discussion
Our double-blind, randomized, controlled follow-up study results suggest that balneotherapy is a succesful treatment in the osteoarthritis of the hand as well, since the pain in the hands of patients who had bath in spa water improved even during 3 months. No improvement could be detected in quality of life after 6 months. Forestier et al. [9], using the SF-36, came to the same conclusion regarding knee osteoarthritis.
Mineral water has been used for ages for the alleviation of musculoskeletal pain. The beneficial effects of balneotherapy were studied and proven in a variety of rheumatological diseases in the past decades. In osteoarthritis of the knee, pain and musculoskeletal dysfunction improved in the short to medium term [6–9]. Unfortunately there are not so many studies that support conservative therapy interventions for osteoarthritis of hand, as for osteoarthritis of the hip and knee [17].
Low-level laser therapy (LLLT) is no better than the placebo in improving subjects hand function or decreasing hand pain or morning stiffness [18]. Balneotherapy seems more efficient than LLLT treatment.
There are some modest evidence that hot wrap and steam alleviate pain and increase the grip strength of the hand in hand osteoarthritis [17]. At the EULAR task force’s recommendation, local application of heat is the beneficial treatment, but level of evidence is low [19].
This positive effect—which can be explained by the hot temperature and other physical effects of the water—was detected in the patients who had bath in tap water at the end of the treatment period. Longer lasting improvement, however, could be detected in the patients that had bath in the sulphurous spa water; this refers to the positive role of the sulphur content in the water.
The exact mechanism of action of balneotherapy is not known, but the minerals absorbed from the water can have a therapeutic role, in addition to the physical properties of the water [20, 21]. It is difficult to analyse the effects of each component of spa waters seperately, probably a complex effect occurs. In the spa water used in the present study, the high sulphide ion (S2−) content is dominant. The sulphur can get into the body through the skin and the airways. The hydrogen sulphide (H2S) gas has a known antioxidant effect in the cells [22]. The results of Benedetti et al. [23] also demonstrated this antioxidant effect, as when the sulphurous mud baths were used in combination with the drinking of sulphurous water, the quantity of the biomarkers of oxidative stress and that of biomarkers indicating inflammation and cartilage degradation decreased to a great degree in the blood.
It is assumed that this antioxidant effect of sulphurous mineral water protects against the oxidative damage of cartilage tissue in osteoarthritis [24, 25]. In addition, the sulphide ion (S2−) content is beneficial for the de novo proteoglycan synthesis in the cartilage tissue, counteracting the degradation of the cartilage. It is a remarkable fact that in 41 % of patients with knee osteoarthritis, hand osteoarthritis was found as well, so it can be assumed that balneotherapy could be effective in the case of generalized osteoarthritis, too [26].
Limitation of the study
Sample size has not been calculated, so this may cause lack of statistical power. The difference in colour between the mineral water and the tap water might have influenced the patient blinding. The consumption of analgesics was not studied and patient global assessment was not estimated. Other more objective outcome variables should be included into the study protocol, e.g. the pinch strength and the range of movements in the joints affected.
Conclusions
Balneotherapy and within this the sulphurous spa water alone may be effective for the attenuation of pain in patients with hand osteoarthrosis.
References
Haugen IK, Englund M, Aliabadi P, Niu J, Clancy M, Kvien TK, Felson DT (2011) Prevalence, incidence and progression of hand osteoarthritis in the general population: the Framingham Osteoarthritis Study. Ann Rheum Dis 70:1581–1586
Kjeken I, Dagfinrud H, Slatkowsky-Christensen B, Mowinckel P, Uhlig T, Kvien TK, Finset A (2005) Activity limitations and participation restrictions in women and hand osteoarthritis: patients descriptions and assotiations between dimensions of functioning. Ann Rheum Dis 64:1633–1638
Brandt KD, Radin EL, Dieppe PA, Van de Putte L (2006) Yet more evidence that osteoarthritis is not a cartilage disease. Ann Rheum Dis 10:1261–1264
Towheed TE (2005) Systematic review of therapies for osteoarthritis of the hand. Osteoarthritis Cartilage 13:455–462
Mahendira D, Towheed TE (2009) Systematic review of non-surgical therapies for osteoarthritis of the hand: an update. Osteoarthritis Cartilage 17:1263–1268
Szűcs L, Ratkó I, Leskó T, Szoor I, Genti G, Bálint G (1989) Double-blind trial on the effectiveness of the Püspökladány thermal water on arthrosis of the knee-joints. J R Soc Health 109:7–9
Kovács I, Bender T (2002) The therapeutic effects of Cserkeszőlő thermal water in osteoarthritis of the knee: a double blind, controlled, follow-up study. Rheumatol Int 21:218–221
Yurtkuran M, Alp A, Nasircilar A et al (2006) Balneotherapy and tap water therapy in the treatment of knee osteoarthritis. Rheumatol Int 27:19–27
Forestier R, Desfour H, Tessier J-M, Françon A, Foote AM, Genty C, Rolland C, Roques C-F, Bosson J-L (2010) Spa therapy in the treatment of knee osteoarthritis: a large randomised multicentre trial. Ann Rheum Dis 69(4):660–665
Altman R, Alarcón G, Appelrouth D, Bloch D, Borenstein D, Brandt K et al (1990) The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the hand. Arthritis Rheum 33:1601–1610
Maheu E, Altman RD, Bloch DA et al (2006) Design and conduct of clinical trials in patients with osteoarthritis of the hand: recommendations from a task force of the Osteoarthritis Research Society International. Osteoarthritis Cartilage 14:303–312
Kovács Cs (2008) SPA therapy in Hungary. Press Therm Clim 145:187–190
Dominick KL, Jordan JM, Renner JB, Kraus VB (2005) Relationship of radiographic and clinical variables to pinch and grip strength among individuals with osteoarthritis. Arthritis Rheum 52:1424–1430
Fries JF, Spitz PW, Young DY (1982) The dimensions of health outcomes: the Health Assessment Questionnaire, Disability and Pain scales. J Rheumatol 9:789–793
Bellamy N, Campbell J, Haraoui B, Buchbinder R, Hobby K, Roth JH, MacDermid JC (2002) Dimensionality and clinical importance of pain and disability in hand osteoarthritis: development of the Australian/Canadian (AUSCAN) osteoarthritis hand index. Osteoarthritis Cartilage 10(11):855–862
EuroQol Group (1990) EuroQol: a new facility fot the measurement of health related quality of life. Health Policy 16:199–208
Valdes K, Marik T (2010) A systematic review of conservative interventions for osteoarthritis of the hand. J Hand Ther 23:334–351
Brosseau L, Wells G, Marchand S, Gaboury I, Stokes B, Morin M, Casimiro L, Yonge K, Tugwell P (2005) Randomized controlled trial on low level laser therapy (LLLT) in the treatment of osteoarthritis (OA) of the hand. Lasers Surg Med 36:210–219
Zhang W, Doherty M, Leeb BF et al (2007) EULAR evidence based recommendations for the management of hand osteoarthritis: report of a Task Force of the EULAR Standing Committee for International Clinical Studies Including Therapeutics (ESCISIT). Ann Rheum Dis 66:377–388
Bender T, Karagülle Z, Bálint GP, Gutenbrunner C, Bálint PV, Sukenik S (2005) Hydrotherapy, balneotherapy and spa treatment in pain management [review]. Rheumatol Int 25:220–224
Falagas ME, Zarkadoulia E, Rafailidis PI (2009) The therapeutic effect of balneotherapy: evaluation of the evidence from randomised controlled trials. Int J Clin Pract 63(7):1068–1084
Chen Chang-qing, Xin H, Zhu Yi-zhun (2007) Hydrogen sulfide: third gaseous transmitter, but with great pharmacological potential. Acta Pharmacol Sin 28(11):1709–1716
Benedetti S, Canino C, Tonti G, Medda V, Calcaterra P, Nappi G, Salaffi F, Canestrari F (2010) Biomarkers of oxidation, inflammation and cartilage degradation in osteoarthritis patients undergoing sulfur-based spa therapies. Clin Biochem 43(12):973–978
Ekmekcioglu C, Strauss-Blasche G, Holzer F, Marktl W (2002) Effect of sulfur baths on antioxidative defense systems, peroxide concentrations and lipid levels in patients with degenerative osteoarthritis. Forsch Komplementmed Klass Natheilkd 9(4):216–220
Leibetseder V, Strauss-Blasche G, Holzer F, Marktl W, Ekmekcioglu C (2004) Improving homocysteine levels through balneotherapy: effects of sulphur baths. Clin Chim Acta 343:105–111
Forestier R, Francon A, Briole V, Genty C, Chevalier X, Richette P (2011) Prevalence of generalized osteoarthritis in a population with knee osteoarthritis. Joint Bone Spine 78(3):275–278
Disclosures
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kovács, C., Pecze, M., Tihanyi, Á. et al. The effect of sulphurous water in patients with osteoarthritis of hand. Double-blind, randomized, controlled follow-up study. Clin Rheumatol 31, 1437–1442 (2012). https://doi.org/10.1007/s10067-012-2026-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-012-2026-0