
Abstract
Purpose
To prospectively evaluate the clinical, radiographic, and sports-related outcomes at 24 months after isolated and combined patellofemoral inlay resurfacing (PFIR).
Methods
Between 2009 and 2010, 29 consecutive patients with patellofemoral osteoarthritis (OA) were treated with the HemiCAP® Wave Patellofemoral Resurfacing System (Arthrosurface, Franklin, MA, USA). Based on preoperative findings, patients were divided into two groups: group I, isolated PFIR (n = 20); and group II, combined PFIR with concomitant procedures to address patellofemoral instability, patellofemoral malalignment, and tibiofemoral malalignment (n = 9). Patients were evaluated preoperatively and at 24 months postoperatively. Clinical outcomes included WOMAC, subjective IKDC, Pain VAS, Tegner activity score, and a self-designed sports questionnaire. Kellgren–Lawrence grading was used to assess progression of tibiofemoral OA. The Caton–Deschamps Index was used to assess differences in patellar height.
Results
Twenty-seven patients (93 %) were available for 24-month follow-up. Eighty-one per cent of the patients were either satisfied or very satisfied with the overall outcome. Significant improvements in the WOMAC, subjective IKDC, and Pain VAS were seen in the overall patient cohort and in both subgroups. The median Tegner score and sports frequency showed a significant increase in the overall patient cohort and in group II. The number of sports disciplines increased significantly in both subgroups. No significant progression of tibiofemoral OA or changes in patellar height were observed.
Conclusion
Patellofemoral inlay resurfacing is an effective and safe procedure in patients with symptomatic patellofemoral OA. Significant improvements in functional scores and sports activity were found after both isolated and combined procedures.
Level of evidence
Prospective case series, Level III.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The treatment of isolated patellofemoral osteoarthritis (OA) is still a matter of debate [17, 23, 41]. Several surgical procedures with variable results have been proposed, including chondroplasty, lateral release, realignment or unloading osteotomies, biological cartilage restoration, and arthroplasty [19, 23, 32]. Although patellofemoral arthroplasty has been used for more than 30 years [6, 40], it is still considered controversial [32, 36, 39]. Inconsistent results and relatively high failure rates have led to a decline in popularity of patellofemoral arthroplasty in the past [1, 6, 7, 12, 18, 31, 55, 58, 60]. Drawbacks of the implant design, especially of the trochlear component, are believed to be the major reason for failures with early implants [36, 37, 39]. With the introduction of new implant designs, patellofemoral arthroplasty has produced more consistent results and has regained importance in clinical practice [33, 36, 37, 39, 59].
The HemiCAP® Wave Patellofemoral Resurfacing Prosthesis (Arthrosurface, Franklin, MA, USA) is a relatively new implant that intends to replicate the complex joint biomechanics by intraoperative joint surface mapping and implantation of a matching, contoured trochlear inlay component (Fig. 1). The availability of different implants with varying offsets and radii of curvature allows for anatomic and individualized patellofemoral inlay resurfacing (PFIR). Compared with onlay prosthetic designs, PFIR has the theoretical advantage of less mechanical patellofemoral complications, increased implant stability, unaltered soft tissue tension and extensor mechanism, and less risk of overstuffing of the patellofemoral joint [9, 14, 49]. However, results of the HemiCAP® Wave prosthesis have not been reported in the literature.

Photograph of the HemiCAP® Wave prosthesis (Arthrosurface, Franklin, MA, USA) showing titanium screw fixation stud connected via taper interlock with cobalt–chromium inlay trochlear component
In addition to age-related primary OA, isolated patellofemoral OA is often associated with patellofemoral malalignment and patellar instability [2, 22], which further complicates treatment. Isolated patellofemoral arthroplasty in these patients fails to restore the complex kinematics of the patellofemoral joint [4]. Therefore, a combined procedure, e.g. additional reconstruction of the medial patellofemoral ligament (MPFL), distal femoral osteotomy (DFO), or transfer of the tibial tuberosity, is necessary in these patients to achieve good results. Nevertheless, the results of these complex interventions have been rarely reported [4].
Patellofemoral OA commonly occurs in relatively young and active patients, and the expectation for functional outcomes, including sporting activities, is high [6, 32, 54]. To the best of our knowledge, however, sports-related outcomes after patellofemoral arthroplasty have not been studied specifically.
The purpose of this study was therefore to prospectively evaluate clinical, radiographic and sports-related results 24 months after isolated and combined PFIR using the HemiCAP® Wave prosthesis.
Materials and methods
Between 2009 and 2010, a consecutive series of 30 knees in 29 patients were treated with PFIR at the first authors’ institution. Surgery was indicated in patients with disabling patellofemoral OA (grade III–IV according to the Kellgren–Lawrence [27]) or chondrosis (grade III–IV according to Outerbridge [46]) refractory to conservative treatment and/or prior surgery [34, 35, 59]. Contraindications were symptomatic tibiofemoral OA with pain during activities of daily living, systematic inflammatory arthropathy, chondrocalcinosis, chronic regional pain syndrome, active infection, and fixed loss of knee range of motion [35, 59].
Preoperative evaluation consisted of a thorough history, clinical evaluation, plain radiographs, and magnetic resonance imaging in all patients. Additional weight bearing full-leg radiographs and computer tomography scans were obtained in patients with suspected abnormal limb alignment. Based on the findings of the preoperative evaluation, patients were divided into two groups: isolated PFIR (group I) and combined PFIR (group II). Combined procedures were performed in patients with additional patellofemoral instability, patellofemoral malalignment, and tibiofemoral malalignment (Fig. 2).

Treatment algorithm for patellofemoral inlay resurfacing based on normative values and treatment algorithms for patellofemoral instability and patellar maltracking described in the literature [4, 16, 24, 29, 50, 51, 53]. PF patellofemoral, OA osteoarthritis, MRI magnetic resonance imaging, CT computer tomography, TTTG tibial tuberosity trochlear groove distance, CDI Caton–Deschamps Index, ROM range of motion, MPFL medial patellofemoral ligament, DFO distal femoral osteotomy, HTO high tibial osteotomy
Implant design and surgical technique
The HemiCAP® Wave Patellofemoral Resurfacing System incorporates a cobalt–chrome trochlear component that is connected to a titanium bone anchoring fixation stud via a taper interlock, and an all-polyethylene patella component. Eight different implants with varying offsets and radii of curvature allow for a patient-specific geometry match.
If no additional surgery was performed, a lateral surgical approach without eversion of the patella was used. With the knee in full extension, an offset drill guide was used to establish a working axis normal to the central trochlear articular surface and to confirm trochlear defect coverage. Once the superior and inferior drill guide feet were aligned with the trochlear orientation, a guide pin was advanced into the bone. To determine the proper implant geometry, the superior/inferior and the medial/lateral offsets were measured using specific instrumentation. The implant bed was reamed three-dimensionally with the aid of a guide block (Fig. 3a). The screw fixation stud was then advanced into the bone, and the trochlear component was aligned with the appropriate offsets on the implant holder and placed into the taper of the fixation stud. The trochlear component was then seated using an impactor (Fig. 3b). Representative postoperative radiographs are shown in Fig. 4.

Intraoperative photographs of anatomic inlay resurfacing of the trochlea with the HemiCAP® Wave prosthesis. a Three-dimensional reaming of the implant bed with the aid of a guide block, b seating of the trochlear component using an impactor, and c final view of the inserted trochlear component

Postoperative radiographs after anatomic inlay resurfacing of the trochlea with the HemiCAP® Wave prosthesis. a Anterior–posterior view, b lateral view, and c axial view
Patelloplasty and circumpatellar denervation were performed in all patients; however, we did not routinely resurface the patella [44, 48]. In our clinical practice, the patella is only resurfaced in patients with patellofemoral incongruence because of severe patellar dysplasia, focal osteonecrosis or osteolysis, and subchondral bone defects [28, 44, 48]. In this series, patellar resurfacing was performed in three patients.
Relative contraindications for patellofemoral arthroplasty are uncorrected patellofemoral instability, patellofemoral malalignment, and tibiofemoral malalignment. We therefore performed combined PFIR in these patients [4, 32, 35, 59], according to the treatment algorithm described in Fig. 2.
Postoperative rehabilitation
After isolated PFIR, patients performed partial weight bearing with 20 kg for 2 weeks. Full range of motion was allowed immediately. In the case of additional high tibial osteotomy (HTO) or DFO, partial weight bearing was performed for 6 weeks. After concomitant MPFL reconstruction or transfer of the tibial tuberosity, knee flexion was restricted to 90° for 6 weeks.
Clinical and radiographic evaluation
All patients were evaluated preoperatively and at 24 months postoperatively by a special trained research assistant, who was not a participating surgeon (M.C.). The clinical outcome was evaluated using the WOMAC score [5], subjective IKDC score [26], and visual analogue scale for pain (VAS) [21]. The WOMAC score was assessed according to the KOOS User’s Guide (available at http://www.koos.nu/KOOSGuide2003.pdf). Five standardized answer options were given as 5 Likert boxes, and each question got a score from 0 to 4. A normalized percentage score (100 indicating no problems and 0 indicating extreme problems) was calculated for each subscale (pain, stiffness, function). To evaluate the sports-related outcome, the Tegner score [56] and a self-designed questionnaire, which assessed pre- and postoperative sports disciplines as well as sports frequency (defined as sessions per week), were used. Patient satisfaction with the procedure was assessed at 24-month follow-up by asking the patients if they were very satisfied, satisfied, partially satisfied, or dissatisfied. Postoperative complications and reoperations were recorded during the whole study period.
Radiographic evaluation was performed using the Picture Archiving and Communication System (PACS, Philips Medical Systems, Sectra Imtec AB, Sweden). Radiographs included weight-bearing antero-posterior view, true lateral view, and a 30° patellar axial view. The Kellgren–Lawrence grading [27] was used to assess progression of tibiofemoral OA, and the Caton–Deschamps Index [11] was used to assess differences in patellar height. Implant-related radiographic results were based on comparison of the first to last follow-up radiographs assessing periprosthetic radiolucency, implant subsidence, cyst formation, and implant disassembly.
This study was approved by the institutional review board of the Technical University of Munich (registration number 355/13), and all patients gave their written informed consent to participate in this investigation.
Statistical analysis
Data were analysed using SPSS software version 20.0 (IBM-SPSS, New York, USA). An a priori power analysis was calculated with a difference to detect of 25 points and a standard deviation of 20 points in the subjective IKDC score. It established a sample size of 10 patients with α = 0.05 and β = 0.02 for a power of 80 %.
Normal distributed data are reported as mean ± standard deviation, whereas non-normal distributed data are reported as median (interquartile range, IQR, from the 25th to the 75th percentile). The nonparametric Wilcoxon test for two related samples was used to compare pre- and postoperative values of each outcome parameter. Statistical analysis were performed two sided. The level of significance was set at p < 0.05.
Results
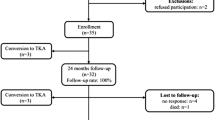
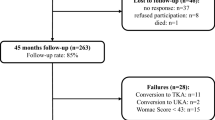
An isolated index procedure was performed in 20 patients (group I) and a combined procedure in 9 patients (10 knees; group II). The patient characteristics and surgical history of both groups are shown in Table 1. Concomitant procedures during index surgery in group II were: MPFL reconstruction (n = 4); transfer of the tibial tuberosity (n = 1); MPFL reconstruction + transfer of the tibial tuberosity (n = 1); DFO (n = 1); MPFL reconstruction + transfer of the tibial tuberosity + DFO (n = 1); transfer of the tibial tuberosity + HTO (n = 2). Of the 29 enrolled patients, two patients of group I had to be excluded during the study period; one patient refused further participation and one patient was converted to a total knee replacement because of progressing global knee pain. Therefore, 27 patients (93 %) were available for the 24-month follow-up.
One patient of group I required re-operation because of component disassembly 3 days after the index surgery. Revision surgery with implantation of a new trochlear component was performed 6 days after the index procedure. In group II, one patient required re-operation at 6 weeks after the index procedure because of graft slippage of the reconstructed MPFL at the femoral tunnel with consecutive patellar instability.
Clinical results
Eighty-one per cent of the patients were either very satisfied (33 %) or satisfied (48 %) with the overall outcome of the operation. Three patients (11 %) were partially satisfied and two patients (7 %) were dissatisfied because of persistent anterior knee pain during physical activities.
The detailed results of the clinical scores are shown in Tables 2 and 3. Compared with preoperative evaluation, significant improvements in all three scores (WOMAC total, subjective IKDC, and VAS) were observed in the overall patient cohort and in both subgroups.
The detailed sports-related results are shown in Table 4. One year before surgery, 58 % of patients were engaged in sports and recreational activities, compared with 89 % at the 24-month follow-up. Figure 5 shows all sports disciplines in which patients participated 1 year before and 24 months after surgery.

Sports disciplines in which patients participated 1 year before (left) and 24 months after the operation (right)
Radiographic results
The detailed results of the radiographic evaluation are shown in Table 5. Significant progression of tibiofemoral OA was neither seen in the overall patient cohort nor in the two subgroups. Furthermore, no significant changes in patellar height were observed. With regard to implant-related radiographic results, no evidence of periprosthetic loosening, cyst formation, or implant subsidence was found.
Discussion
The main finding of the present study was that isolated and combined anatomic PFIR with the HemiCAP® Wave prosthesis achieved promising results at the 2-year follow-up, with a low re-operation rate. Both groups showed significant improvements in all evaluated clinical scores and significantly improved sports activity. No significant progression of tibiofemoral OA or significant changes in patellar height were observed.
To date, most trochlear implants can be considered as onlay designs or anterior cut prosthesis, respectively [39, 54, 59]. These implants are based on the trochlear cuts of a total knee arthroplasty, replacing the entire anterior trochlear surface [39]. Depending on the thickness of the implant, an onlay design may overstuff the patellofemoral joint, leading to increased patellofemoral loads and soft tissue irritation [20, 25, 42]. Furthermore, a too broad component with overhang into the medial and lateral soft tissues may cause soft tissue impingement and limited range of motion [37]. Potential advantages of an inlay design prosthesis include less removal of bone, less mechanical patellofemoral complications, increased implant stability, unaltered soft tissue tension and extensor mechanism, and less risk for overstuffing of the patellofemoral joint [9, 14, 49]. However, older inlay designs were associated with higher failure rates compared with onlay designs, because the individual anatomy of the trochlea was not restored [1, 7, 31, 39, 52, 54, 55]. The HemiCAP® Wave Patellofemoral Resurfacing System uses intraoperative joint surface mapping and implantation of matching, contoured articular inlay components in order to more closely reproduce the geometry of the distal femur. In this series, no mechanical patellofemoral complications such as catching, snapping, or clunking were observed. Therefore, the anatomic design of this prosthesis might be favourable compared with conventional inlay designs, which often do not accurately mate with the articular geometry of the trochlea [1, 7, 31, 39, 52, 54, 55].
Treatment of isolated patellofemoral arthritis is often complicated by patellofemoral malalignment and patellar instability [2, 22]. Restoration of normal patellofemoral kinematics is crucial for successful treatment of patellofemoral arthritis [4]. In our treatment algorithm for patellofemoral OA (Fig. 2), patients with patellofemoral instability or malalignment are treated with a combined procedure, in order to treat the causative factors for the development of patellofemoral OA. Despite the complexity of such a combined procedure, the results of our study indicate that good results can be expected after combined PFIR.
Several studies have found better results after patellofemoral arthroplasty in patients with OA due to patellofemoral instability and/or trochlear dysplasia when compared to patients with primary OA [3, 33, 45]. One possible explanation for this finding might be that patients with primary OA may be more prone to develop degenerative changes in the tibiofemoral joint as part of the joint’s osteoarthritic reaction [3, 10, 45]. Progression of tibiofemoral OA has been determined to be the most common reason for failure of patellofemoral arthroplasty using modern prosthetic designs [30, 54]. We did not observe significant progression of tibiofemoral OA in our patient cohort. Nevertheless, it is possible that slight osteoarthritic changes in the tibiofemoral joint, which were asymptomatic at the preoperative evaluation, became symptomatic during the follow-up period in group I.
Patients presenting with patellofemoral OA are relatively young and therefore have higher demands on the functional outcome including return to sports [32, 54]. One of the goals of patellofemoral arthroplasty is to maintain an active lifestyle, including sporting activities. The results of this study indicate that PFIR improves sports activities. At the final follow-up, the overall patient cohort participated significantly more often in significantly more sports disciplines compared with preoperatively. Whether sports participation diminishes the long-term survival of patellofemoral arthroplasty is currently unknown. However, an inlay resurfacing prosthesis might be especially favourable in active patients, because the prosthesis is implanted congruent to the surrounding articular surface, providing a theoretical advantage for implant stability [8, 9, 14, 49].
Total knee arthroplasty has been proposed as an alternative treatment option for isolated patellofemoral OA [43, 47]. Since patients with isolated patellofemoral OA are commonly younger and more active than patients with tricompartimental OA, early wear and loosening of the prosthesis must be assumed [6, 13, 32, 54]. Possible advantages of patellofemoral arthroplasty compared with total knee arthroplasty include less morbidity, shorter postoperative rehabilitation, conserving bone stock, and maintaining more normal knee kinematics [13, 59]. Since patellofemoral arthroplasty has shown not to compromise the results of total knee arthroplasty [38, 57], we prefer patellofemoral arthroplasty, especially in active middle-aged patients.
A pitfall of the evaluated trochlear component is that there is no supratrochlear extension to guide the patella in terminal extension, especially in patients with patella alta. To avoid patellar instability in terminal extension, distalization of the tibial tuberosity and/or MPFL reconstruction should be considered as a concomitant procedure if necessary.
This study has several limitations. The follow-up of 24 months is relatively short, and therefore the long-term outcomes of this prosthesis remain unknown. Since patellofemoral arthroplasty is a relatively rare operation, we can only present the results of a small patient group, which, however, is comparable to other reports on this topic [1, 4, 7, 15, 31]. We have not been able to compare both groups statistically, because of insufficient study power. One patient who underwent total knee arthroplasty was excluded prior to the 24-month evaluation. This may have introduced a selection bias. Another limitation is that the implant used in this study was not compared with an established prosthesis, and therefore no conclusions can be drawn about the superiority or inferiority when compared with other implants. Further studies with a higher sample size and a longer follow-up will be necessary to confirm the results of this investigation. Nevertheless, the results of this study suggest that the HemiCAP® Wave Patellofemoral Resurfacing Prosthesis can be considered as a valuable alternative to currently used onlay designs, with the potential advantages of an inlay design.
Conclusion
Patellofemoral arthroplasty using the HemiCAP® Wave Patellofemoral Resurfacing Prosthesis is an effective and safe procedure in patients with symptomatic patellofemoral OA. Significant improvements in functional scores and sporting activities were found after both isolated and combined procedures. Detailed preoperative assessment of the underlying condition should be paired with concomitant procedures if necessary.
References
Arciero RA, Toomey HE (1988) Patellofemoral arthroplasty. A three- to nine-year follow-up study. Clin Orthop Relat Res 236:60–71
Arendt E (2005) Anatomy and malalignment of the patellofemoral joint: its relation to patellofemoral arthrosis. Clin Orthop Relat Res 436:71–75
Argenson JN, Flecher X, Parratte S, Aubaniac JM (2005) Patellofemoral arthroplasty: an update. Clin Orthop Relat Res 440:50–53
Beitzel K, Schottle PB, Cotic M, Dharmesh V, Imhoff AB (2013) Prospective clinical and radiological two-year results after patellofemoral arthroplasty using an implant with an asymmetric trochlea design. Knee Surg Sports Traumatol Arthrosc 21(2):332–339
Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW (1988) Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol 15(12):1833–1840
Blazina ME, Fox JM, Del Pizzo W, Broukhim B, Ivey FM (1979) Patellofemoral replacement. Clin Orthop Relat Res 144:98–102
Board TN, Mahmood A, Ryan WG, Banks AJ (2004) The Lubinus patellofemoral arthroplasty: a series of 17 cases. Arch Orthop Trauma Surg 124(5):285–287
Bollars P, Bosquet M, Vandekerckhove B, Hardeman F, Bellemans J (2012) Prosthetic inlay resurfacing for the treatment of focal, full thickness cartilage defects of the femoral condyle: a bridge between biologics and conventional arthroplasty. Knee Surg Sports Traumatol Arthrosc 20(9):1753–1759
Cannon A, Stolley M, Wolf B, Amendola A (2008) Patellofemoral resurfacing arthroplasty: literature review and description of a novel technique. Iowa Orthop J 28:42–48
Cartier P, Sanouiller JL, Khefacha A (2005) Long-term results with the first patellofemoral prosthesis. Clin Orthop Relat Res 436:47–54
Caton J, Deschamps G, Chambat P, Lerat JL, Dejour H (1982) Patella infera. Apropos of 128 cases. Rev Chir Orthop Reparatrice Appar Mot 68(5):317–325
Charalambous CP, Abiddin Z, Mills SP, Rogers S, Sutton P, Parkinson R (2011) The low contact stress patellofemoral replacement: high early failure rate. J Bone Joint Surg Br 93(4):484–489
Dahm DL, Al-Rayashi W, Dajani K, Shah JP, Levy BA, Stuart MJ (2010) Patellofemoral arthroplasty versus total knee arthroplasty in patients with isolated patellofemoral osteoarthritis. Am J Orthop (Belle Mead NJ) 39(10):487–491
Davidson PA, Rivenburgh D (2008) Focal anatomic patellofemoral inlay resurfacing: theoretic basis, surgical technique, and case reports. Orthop Clin North Am 39(3):337–346
de Winter WE, Feith R, van Loon CJ (2001) The Richards type II patellofemoral arthroplasty: 26 cases followed for 1–20 years. Acta Orthop Scand 72(5):487–490
Dickschas J, Harrer J, Pfefferkorn R, Strecker W (2012) Operative treatment of patellofemoral maltracking with torsional osteotomy. Arch Orthop Trauma Surg 132(3):289–298
Donell ST, Glasgow MM (2007) Isolated patellofemoral osteoarthritis. Knee 14(3):169–176
Dy CJ, Franco N, Ma Y, Mazumdar M, McCarthy MM, Gonzalez Della Valle A (2012) Complications after patello-femoral versus total knee replacement in the treatment of isolated patello-femoral osteoarthritis A meta-analysis. Knee Surg Sports Traumatol Arthrosc 20(11):2174–2190
Fulkerson JP (2005) Alternatives to patellofemoral arthroplasty. Clin Orthop Relat Res 436:76–80
Ghosh KM, Merican AM, Iranpour F, Deehan DJ, Amis AA (2009) The effect of overstuffing the patellofemoral joint on the extensor retinaculum of the knee. Knee Surg Sports Traumatol Arthrosc 17(10):1211–1216
Gould D, Kelly D, Goldstone L, Gammon J (2001) Examining the validity of pressure ulcer risk assessment scales: developing and using illustrated patient simulations to collect the data. J Clin Nurs 10(5):697–706
Grelsamer RP, Dejour D, Gould J (2008) The pathophysiology of patellofemoral arthritis. Orthop Clin North Am 39(3):269–274
Grelsamer RP, Stein DA (2006) Patellofemoral arthritis. J Bone Joint Surg Am 88(8):1849–1860
Hinterwimmer S, Rosenstiel N, Lenich A, Waldt S, Imhoff AB (2012) Femoral osteotomy for patellofemoral instability. Unfallchirurg 115(5):410–416
Hollinghurst D, Stoney J, Ward T, Pandit H, Beard D, Murray DW (2007) In vivo sagittal plane kinematics of the Avon patellofemoral arthroplasty. J Arthroplasty 22(1):117–123
Irrgang JJ, Anderson AF, Boland AL, Harner CD, Kurosaka M, Neyret P, Richmond JC, Shelborne KD (2001) Development and validation of the international knee documentation committee subjective knee form. Am J Sports Med 29(5):600–613
Kellgren JH, Lawrence JS (1957) Radiological assessment of osteo-arthrosis. Ann Rheum Dis 16(4):494–502
Kim BS, Reitman RD, Schai PA, Scott RD (1999) Selective patellar nonresurfacing in total knee arthroplasty. 10 year results. Clin Orthop Relat Res 367:81–88
Kohn LM, Meidinger G, Beitzel K, Banke IJ, Hensler D, Imhoff AB, Schottle PB (2013) Isolated and combined medial patellofemoral ligament reconstruction in revision surgery for patellofemoral instability: a prospective study. Am J Sports Med 41(9):2128–2135
Kooijman HJ, Driessen AP, van Horn JR (2003) Long-term results of patellofemoral arthroplasty. A report of 56 arthroplasties with 17 years of follow-up. J Bone Joint Surg Br 85(6):836–840
Krajca-Radcliffe JB, Coker TP (1996) Patellofemoral arthroplasty. A 2- to 18-year followup study. Clin Orthop Relat Res 330:143–151
Leadbetter WB (2008) Patellofemoral arthroplasty in the treatment of patellofemoral arthritis: rationale and outcomes in younger patients. Orthop Clin North Am 39(3):363–380
Leadbetter WB, Kolisek FR, Levitt RL, Brooker AF, Zietz P, Marker DR, Bonutti PM, Mont MA (2009) Patellofemoral arthroplasty: a multi-centre study with minimum 2-year follow-up. Int Orthop 33(6):1597–1601
Leadbetter WB, Ragland PS, Mont MA (2005) The appropriate use of patellofemoral arthroplasty: an analysis of reported indications, contraindications, and failures. Clin Orthop Relat Res 436:91–99
Leadbetter WB, Seyler TM, Ragland PS, Mont MA (2006) Indications, contraindications, and pitfalls of patellofemoral arthroplasty. J Bone Joint Surg Am 88(Suppl 4):122–137
Lonner JH (2004) Patellofemoral arthroplasty: pros, cons, and design considerations. Clin Orthop Relat Res 428:158–165
Lonner JH (2008) Patellofemoral arthroplasty: the impact of design on outcomes. Orthop Clin North Am 39(3):347–354
Lonner JH, Jasko JG, Booth RE Jr (2006) Revision of a failed patellofemoral arthroplasty to a total knee arthroplasty. J Bone Joint Surg Am 88(11):2337–2342
Lustig S, Magnussen RA, Dahm DL, Parker D (2012) Patellofemoral arthroplasty, where are we today? Knee Surg Sports Traumatol Arthrosc 20(7):1216–1226
McKeever DC (1955) Patellar prosthesis. J Bone Joint Surg Am 37-A(5):1074–1084
Mihalko WM, Boachie-Adjei Y, Spang JT, Fulkerson JP, Arendt EA, Saleh KJ (2008) Controversies and techniques in the surgical management of patellofemoral arthritis. Instr Course Lect 57:365–380
Monk AP, van Duren BH, Pandit H, Shakespeare D, Murray DW, Gill HS (2012) In vivo sagittal plane kinematics of the FPV patellofemoral replacement. Knee Surg Sports Traumatol Arthrosc 20(6):1104–1109
Mont MA, Haas S, Mullick T, Hungerford DS (2002) Total knee arthroplasty for patellofemoral arthritis. J Bone Joint Surg Am 84-A(11):1977–1981
Munoz-Mahamud E, Popescu D, Nunez E, Lozano LM, Nunez M, Sastre S, Torner P, Segur JM, Macule F (2011) Secondary patellar resurfacing in the treatment of patellofemoral pain after total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 19(9):1467–1472
Nicol SG, Loveridge JM, Weale AE, Ackroyd CE, Newman JH (2006) Arthritis progression after patellofemoral joint replacement. Knee 13(4):290–295
Outerbridge RE (1961) The etiology of chondromalacia patellae. J Bone Joint Surg Br 43-B:752–757
Parvizi J, Stuart MJ, Pagnano MW, Hanssen AD (2001) Total knee arthroplasty in patients with isolated patellofemoral arthritis. Clin Orthop Relat Res 392:147–152
Pilling RW, Moulder E, Allgar V, Messner J, Sun Z, Mohsen A (2012) Patellar resurfacing in primary total knee replacement: a meta-analysis. J Bone Joint Surg Am 94(24):2270–2278
Provencher M, Ghodadra NS, Verma NN, Cole BJ, Zaire S, Shewman E, Bach BR Jr (2009) Patellofemoral kinematics after limited resurfacing of the trochlea. J Knee Surg 22(4):310–316
Schoettle PB, Zanetti M, Seifert B, Pfirrmann CW, Fucentese SF, Romero J (2006) The tibial tuberosity-trochlear groove distance; a comparative study between CT and MRI scanning. Knee 13(1):26–31
Schottle PB, Hensler D, Imhoff AB (2010) Anatomical double-bundle MPFL reconstruction with an aperture fixation. Knee Surg Sports Traumatol Arthrosc 18(2):147–151
Smith AM, Peckett WR, Butler-Manuel PA, Venu KM, d’Arcy JC (2002) Treatment of patello-femoral arthritis using the Lubinus patello-femoral arthroplasty: a retrospective review. Knee 9(1):27–30
Strecker W, Keppler P, Gebhard F, Kinzl L (1997) Length and torsion of the lower limb. J Bone Joint Surg Br 79(6):1019–1023
Tarassoli P, Punwar S, Khan W, Johnstone D (2012) Patellofemoral arthroplasty: a systematic review of the literature. Open Orthop J 6:340–347
Tauro B, Ackroyd CE, Newman JH, Shah NA (2001) The Lubinus patellofemoral arthroplasty. A five- to ten-year prospective study. J Bone Joint Surg Br 83(5):696–701
Tegner Y, Lysholm J (1985) Rating systems in the evaluation of knee ligament injuries. Clin Orthop Relat Res 198:43–49
van Jonbergen HP, Werkman DM, van Kampen A (2009) Conversion of patellofemoral arthroplasty to total knee arthroplasty: a matched case-control study of 13 patients. Acta Orthop 80(1):62–66
van Wagenberg JM, Speigner B, Gosens T, de Waal Malefijt J (2009) Midterm clinical results of the Autocentric II patellofemoral prosthesis. Int Orthop 33(6):1603–1608
Walker T, Perkinson B, Mihalko WM (2012) Patellofemoral arthroplasty: the other unicompartmental knee replacement. J Bone Joint Surg Am 94(18):1712–1720
Yadav B, Shaw D, Radcliffe G, Dachepalli S, Kluge W (2012) Mobile-bearing, congruent patellofemoral prosthesis: short-term results. J Orthop Surg (Hong Kong) 20(3):348–352
Conflict of interest
A.B. Imhoff and P.B. Schöttle are consultants for Arthrosurface. The company had no influence on study design, data collection, and interpretation of the results or the final manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
Andreas B. Imhoff and Matthias J. Feucht have contributed equally to this work and share first authorship.
Rights and permissions
About this article
Cite this article
Imhoff, A.B., Feucht, M.J., Meidinger, G. et al. Prospective evaluation of anatomic patellofemoral inlay resurfacing: clinical, radiographic, and sports-related results after 24 months. Knee Surg Sports Traumatol Arthrosc 23, 1299–1307 (2015). https://doi.org/10.1007/s00167-013-2786-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-013-2786-3