
Abstract
Purpose
Both patellofemoral arthroplasty (PFA) and total knee arthroplasty (TKA) are successful in treating isolated patellofemoral osteoarthritis, but the complication rates after PFA are concerning. We performed a meta-analysis to compare the incidence of complications, re-operations, and revision following PFA and TKA for patellofemoral osteoarthritis.
Methods
We systematically identified publications with patients who underwent PFA or TKA for patellofemoral osteoarthritis with minimum 1.5 year follow-up. Demographics, implant (TKA, first [1G] or second-generation [2G] PFA), complications, and cause of re-operations were extracted. Random-effects meta-analysis was used to pool incidence data, which was compared between groups using logistic regression to adjust for length of follow-up.
Results
Twenty-eight observational studies and no randomized trials were included in this meta-analysis, which limits its generalizability. There was a higher likelihood of any re-operation (odds ratio 8.06) and revision (OR 8.11) in PFA compared to TKA. Re-operation (OR 4.33) and revision (OR 4.93) were more likely in 1G-PFA than 2G-PFA. When comparing 2G-PFA to TKA, there was no significant difference in re-operation, revision, pain, or mechanical complications.
Conclusions
Patients who undergo PFA rather than TKA are more likely to experience complications and require re-operation or revision, but subgroup analysis suggests a relation to implant design. There is no significant difference in re-operation, revision, pain, or mechanical complications between 2G-PFA and TKA.
Level of evidence
Systematic review of Level III therapeutic studies, Level III.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Patellofemoral arthroplasty (PFA) was introduced by Lubinus and Blazina in 1979 for the treatment of end stage PFOA [5, 24]. While PFA was successful in providing pain relief, the procedure did not gain widespread use because of initial design limitations, such as suboptimal trochlear implant geometry and narrow anterior femoral flange width, that predisposed to PF maltracking, catching, and subluxation [22]. The early mechanical complications associated with first-generation PFA offset the potential advantages of maintaining the knee’s native soft tissues and spurred efforts to improve implant design, and to refine surgical techniques and patient selection [7, 22, 23]. Over the past decade, second generation PFAs incorporated changes in implant design and instrumentation and have shown promising results when used in the properly selected patient population [21, 23].
Due to the previously mentioned concerns associated with PFA, many surgeons have elected to treat patients with isolated PF OA and severe pain with total knee arthroplasty (TKA). TKA has been extremely successful in relieving pain in patients with PF OA, with patient satisfaction exceeding 90% [19, 30, 32] and clinical results significantly better than a gender and age matched cohort who had TKA performed for tricompartmental OA [19]. Despite the successful, durable results, concern remains for using TKA in patients with isolated PF OA, as TKA requires a more extensive surgical exposure and bone resection, a longer recovery time, and a potentially more complex revision than that required for a patient with a failed PFA.
It is controversial as to whether PFA or TKA should be used to treat patients with isolated PF OA. The quality of evidence supporting both procedures has been objectively classified in a recent systematic review as low quality [40]. Most of the published studies are retrospective, non-comparative, or non-randomized, and report on a small number of patients. To overcome the limitations imposed by the low prevalence of severe isolated PF OA and the low utilization of arthroplasty surgery in patients with isolated PF OA, we performed a meta-analysis that attempted to answer the following four research questions:
-
1.
What are the incidences and types of complication in patients undergoing PFA and TKA for the treatment of isolated PF OA?
-
2.
What are the incidences, indications for, and types of re-operations following the use of PFA and TKA to treat patients with isolated PF OA?
-
3.
Is there a difference in the incidence of complications, re-operation, and revision arthroplasty in patients who received a first- or a second-generation PFA design?
-
4.
Is there a difference in the incidence of complications, re-operation, and revision arthroplasty between second-generation PFA and TKA when used to treat patients with isolated PF OA?
Materials and methods
Identification and eligibility of relevant studies
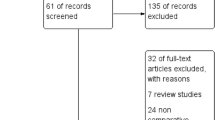
Two authors (NF and CJD) searched the Medline and Embase bibliographic databases (January 1979 to January 2010) with the following search strategy: “patellofemoral arthroplasty”, which yielded 51 results in Medline and 61 results in Embase. The overlapping results were eliminated, leaving a total of 61 articles. A second search was performed in Medline and Embase (January 1979 to January 2010) with the following search strategies: (1) “patellofemoral arthritis” AND “total knee arthroplasty”; (2) “patellofemoral arthritis” AND “knee arthroplasty”; (3) “patellofemoral arthritis” AND “arthroplasty”. Twenty-three additional articles were identified using this method. There was no language limitation for either of the searches listed above.
Blinded abstracts of all 84 articles were independently reviewed by two of the authors (NF and CJD). To be included in the meta-analysis, the study had to meet the following criteria: (1) minimum follow-up of 1.5 years; (2) report of pre-operative diagnosis; (3) report on the reason for re-operation (if any). If separate reports pertaining to the same group of patients were published at different follow-up intervals, the study with the longest duration of follow-up was included. Following selection of the abstracts that met inclusion criteria, the bibliographies of each article were reviewed to identify additional studies, which yielded 4 additional articles for potential inclusion. We did not identify any prospective randomized studies or prospective comparative studies comparing PFA and TKA for the treatment of patients with isolated PF OA. Twenty-eight observational studies (3 Level II prospective cohort studies and 25 Level IV case series) were included in the current meta-analysis (Fig. 1). There were three non-English-language studies: two in French [10, 27] and one in Danish [16]. All three were included after translation.

The flow diagram shows the identification of observational studies in the systematic review
Data extraction
The number of patients who received surgery, the number of knees that were operated upon, the duration of follow-up, the number of patients lost to follow-up, preoperative diagnosis, patient’s age and gender, and preceding surgeries were recorded. The indications for surgery were recorded. Patellofemoral instability (subluxation or dislocation) as a surgical indication was noted if stated by the authors (Appendix Table 5). Additionally, the type of prosthesis and fixation used and any concomitant surgical procedures performed in conjunction with PFA or TKA, such as bony or soft tissue procedures to realign the extensor mechanism, were recorded. PFA implants were grouped as first or second generation based on their design characteristics, as previously described by Lonner [22]. First generation implants include the Lubinus (Waldermar Link Co., Hamberg, Germany) prosthesis, the Blazina (Smith and Nephew, Memphis, TN) prosthesis, and the Richards Mod II and III (Smith and Nephew) prostheses. The second generation of PFA implants, which included alterations to the trochlear design aimed at decreasing maltracking and improvements in instrumentation, include the Avon (Stryker, Mahwah, NJ), Autocentric (DePuy, Warsaw, IN) and Low Contact Stress (LCS, DePuy) patellofemoral prostheses. One study included both first and second generation PFA implants and the knees were categorized according to the implant used [29]. Postoperative complications were grouped into four categories based on clinical principles: pain (including stiffness or effusion), mechanical (including instability, malalignment, and implant loosening), progression of OA, or other (such as wound dehiscence and medical complications). The number and type of re-operations were recorded, with the reason for re-operation chosen based on the four previously described categories. Two authors (NF and CJD) independently reviewed each study. Disagreements were discussed between the authors to reach a consensus.
Of the 28 studies included in the meta-analysis, 22 reported on the use of PFA, and 6 on the use of TKA (Table 1; Appendix Table 5). A total of 1,019 patients (1,154 knees) were included in the PFA group and a total of 187 patients (213 knees) were included in the TKA group. Within the PFA group, there were 798 first generation PFAs (69.2%) and 356 were second generation (30.8%).
Quality assessment of included studies
The methodologic quality of each non-randomized study included in the meta-analysis was assessed using the validated Methodologic Index for Non-Randomized Studies (MINORS) instrument [34]. Each study was appraised independently by a physician who was not involved in the remainder of the study (Appendix Table 6). Only one study included a comparative cohort [19]; a non-comparative score for this study is also included to allow further comparison. Scores were compared between the PFA and TKA cohorts of studies using a student’s t test, with statistical significance set at P < 0.05. The average MINORS score for all of the studies included in the meta-analysis was 11.4 (of a maximum of 16 for a non-comparative study). The average MINORS score for the PFA cohort of studies and for the TKA cohort of studies was 11.6 and 11, respectively. There was no significant difference between the MINORS scores of the PFA and TKA studies.
Methods for meta-analysis
Multiple meta-analyses were performed to pool complication rate (defined as total number of complications divided by total number of knees), reoperation rate (total number of reoperations divided by total number of knees), and rate of revision arthroplasty (total number of revision PFA or conversion to TKA divided by total number of knees). The present study focuses on the results of PFA and consequently, the report of the complications, reoperation and revision is based on the number of knees and not the number of patients.
In each case, to determine the pooled proportion, the variances of the raw proportions were stabilized by using a Freeman-Tukey-type arcsine square root transformation [14]. The pooled proportions were calculated as the back-transform of the weighted mean of the transformed proportions, using DerSimonian-Laird fixed effects or random effects models [12]. The χ2 test based on Q-statistic [8] and I2 statistic [15] were employed to assess the percentage of variability across studies attributable to heterogeneity beyond chance. A P value higher than 0.10 for the χ2 test and an I2 value of lower than 25% were interpreted as signifying low level heterogeneity [15]. Fixed effects models were only used when low level heterogeneity presents. Random effects models were applied otherwise.
Random-effects logistic regression was conducted to compare the pooled proportions between groups while adjusting for average of length of follow-up. Forest plot was utilized for presentation of summary statistics from each study along with the pooled proportion and test of homogeneity (Figs. 2, 3, 4).


Publication bias was tested using a linear regression test for funnel plot asymmetry [13] to evaluate if studies with significant result had higher chance of getting published. Publication bias was not found in any of the outcomes. The current investigation is reported using the MOOSE guidelines for meta-analyses of observational studies [36].
Results
There was a higher likelihood of any re-operation (odds ratio 8.06) and revision (OR 8.11) in PFA compared to TKA. Re-operation (OR 4.33) and revision (OR 4.93) were more likely in 1G-PFA than 2G-PFA. When comparing 2G-PFA to TKA, there was no significant difference in re-operation, revision, pain, or mechanical complications.
Description of rates of complications
PFA
Within the combined PFA group, there were 387 complications in 1,154 knees, resulting in a weighted rate of complication of 0.30 [95% confidence interval = 0.22, 0.39] (Table 2; Fig. 2a; Appendix Table 7). Mechanical complications were most commonly noted (0.10 [0.05, 0.16]), followed by persistent pain (0.07 [0.03, 0.11]) and progression to tibiofemoral osteoarthritis (0.08 [0.04, 0.12]).
TKA
Within the TKA group, there were 14 complications in 213 knees, resulting in a weighted rate of complication of 0.07 [0.03, 0.12] (Table 2; Fig. 4a; Appendix Table 7). Persistent pain was noted in 9 knees (0.05 [0.02, 0.08]), mechanical complications arose in 2 knees (0.01 [0.002, 0.03]), and other complications (patella fracture treated nonoperatively, urinary tract infection, and intraoperative hemodynamic disturbances) arose in 3 knees.

Description of rates of re-operation and revision
A detailed description of the re-operations and reasons for re-operations is listed in Appendix Table 8.
PFA
Within the PFA group, 285 knees (0.21 [0.15, 0.29]) underwent a re-operation (Table 2). Mechanical complications were the most common reason for re-operation (0.07 [0.04, 0.12]), followed by persistent pain (0.05 [0.02, 0.09]) and progression of OA (0.06 [0.04, 0.09]). One hundred fifty-four knees required a revision of the patellofemoral arthroplasty (54 knees) or conversion to total knee arthroplasty (100 knees). One hundred thirty-one knees were re-operated upon for non-arthroplasty procedures. Multiple procedures were often performed at once. There were 49 lateral releases, 47 arthroscopic or open debridements, 33 bony and/or soft tissue distal realignment procedures, 25 manipulations under anesthesia, 11 patellectomies, 6 tibial osteotomies, 3 synovectomies, 2 removals of hardware for infection, 2 meniscectomies, 2 medial plications, and 10 other various types of procedures (Appendix Table 8).
TKA
Within the TKA group, 4 knees underwent re-operation (0.02 [0.15, 0.29]) (Table 2). Mechanical complications were the cause of re-operation in 2 knees (0.01 [0.002, 0.03]), one of which underwent a revision of the patellar component only, and the other which underwent a extensor mechanism realignment with lateral release and tibial polyethylene exchange [32]. Persistent stiffness was the cause for 1 knee (0.01 [0.002, 0.03]), which underwent a manipulation under anesthesia [32]. Post-traumatic tendon disruption after a fall was the cause for re-operation in the remaining knee (categorized as “other”; 0.01 [0.002, 0.03]), which underwent a tendon repair with retention of components [30] (Appendix Table 8).
Comparison of complications, re-operations, and revision arthroplasty (adjusted for the average length of follow-up)
All PFA versus TKA
When evaluated as a single group combining first and second generation implants, patients who underwent PFA had a significantly higher likelihood (odds ratio: 5.69; P = 0.001) of complications than those who underwent TKA (Table 3). There is a significantly likelihood of mechanical complications in the PFA group (OR = 4.60; P = 0.041) than the TKA group (Table 3). There was no difference in the likelihood of pain/stiffness or other complications. Patients who underwent PFA were significantly more likely to undergo any type of reoperation (OR 8.06; P = 0.002) and significantly more likely to undergo revision arthroplasty (OR 8.11; P = 0.004) surgery than patients who underwent TKA (Table 4).
First generation PFA versus second generation PFA
The overall likelihood of experiencing complications was significantly higher with first generation PFA implants than second generation (OR 2.86; P = 0.006). There was no significant difference in the rate of persistent pain or in the rate of progression of OA. The likelihood of undergoing any re-operation was significantly higher with first generation PFA implants (OR 4.33; P = 0.001), as was the likelihood of undergoing revision PFA arthroplasty (OR 4.93; P = 0.011). The likelihoods of having a mechanical complication (OR 4.62; P = 0.023) and undergoing re-operation for mechanical reasons (OR 6.48; P = 0.004) were significantly higher in the first generation PFA cohort. The likelihood of undergoing re-operation due to progression of OA was slightly higher in the first generation PFA cohort (OR 2.22) but this difference was not statistically significant (P = 0.057). However, the influence of average length of follow-up on the likelihood of undergoing re-operation due to progression of OA was statistically significant (P = 0.01).
Second generation PFA versus TKA
There is no statistically significant difference between second-generation PFA and TKA in the development of mechanical complications, persistent pain after surgery, re-operation rate (all types), or revision arthroplasty (Tables 3, 4).
Influence of length of follow-up on complications
The random-effects model also allowed for evaluation of whether length of follow-up influenced the likelihood of complications, re-operation, or revision arthroplasty. The odds ratios given for this covariate describe the increase in the likelihood of experiencing the event with each increasing year of follow-up (Tables 3, 4). Length of follow-up was found to significantly influence event occurrence in the following comparisons. (An example interpretation is given to assist the readership.)
-
Progression of OA when comparing first generation and second generation PFA (OR 1.12; P = 0.02).
-
For each increasing year of follow-up, patients who have first generation PFA are 12% more likely chance of having progression of OA than those patients who have second generation PFA.
-
-
Any complication when comparing all PFA and TKA (OR 1.14; P = 0.003)
-
Any re-operation when comparing all PFA and TKA (OR 1.11; P = 0.02)
-
Re-operation for any reason when comparing first and second generation PFA (OR 1.14; P = 0.003)
-
Re-operation due to progression of OA when comparing first and second generation PFA (OR 1.12; P = 0.002)
-
Arthroplasty-related revision (revision PFA or conversion to TKA) when comparing first- and second-generation PFA (OR 1.10; P = 0.012)
-
Conversion to TKA when comparing first and second-generation PFA (OR 1.12; P = 0.013)
-
The influence of length of follow-up was not statistically significant in any comparisons between second-generation PFA and TKA.
Discussion
The most important finding of the present study was that patients who undergo PFA rather than TKA are more likely to experience complications and require re-operation or revision, but subgroup analysis suggests a relation to implant design. The present study was carried out to objectively and quantitatively compare the results of PFA and TKA for the treatment of patients with isolated PFA. The analysis was conducted to answer four questions that are relevant for the practicing orthopaedic surgeon to discuss benefits and drawbacks of PFA and TKA with patients presenting with severe pain and isolated PFA. We quantified the incidences and types of complications and reoperations in patients undergoing PFA and TKA for the treatment of isolated PF OA; and to determine if modern PFA designs and surgical technique have resulted in improved outcomes.
We detected that the rate of complications of patients undergoing PFA was 30% after a median follow up of 5.3 years, which is significantly higher than the 7% rate of complications in patients who underwent TKA. The most frequent type of complication associated with PFA was mechanical (including loosening and instability), which is consistent with the malalignment and maltracking-related failures previously reported by numerous authors [5, 11, 23, 37].
The incidence of re-operation after PFA (21%) was significantly higher than that seen after TKA (2%). Leadbetter et al. [21] performed a trend analysis of available data regarding poor outcomes after PFA and found a similar re-operation rate (24%). We found that the most frequent indication for re-operation after PFA was mechanical failure (7%), followed by progression of OA (6%), and persistent pain or stiffness (5%). These indications are similar to those reported by other authors in non-quantitative studies [1, 21, 28, 40]. The most common re-operations after PFA were conversion to TKA, revision of PFA components, lateral releases, open or arthroscopic debridements, manipulations under anesthesia, and bony and/or soft tissue extensor mechanism re-alignment procedures. Eleven percent of patients treated with PF OA underwent a revision arthroplasty, with 4% undergoing revision PFA and 7% undergoing conversion to TKA. Our rate of conversion to TKA is consistent with the figure reported by Leadbetter et al. of 9% [21].
There is a significantly higher chance of complications, re-operations, and revision arthroplasty surgery in patients who underwent surgery with first-generation designs of PFA when compared to second-generation designs. The complication, re-operation, and revision arthroplasty rate is significantly higher after use of first-generation designs. It can be speculated that this observation may be due to numerous factors including refined surgical technique, improved patient selection and prosthetic design. Tauro et al. [37] described their experience with the Lubinus implant, one of the first-generation PFA designs, and cited implant selection as one of the driving factors for poor results. Additionally, Lonner has qualitatively described his experience with both generations of patellofemoral implant designs and has emphasized the distinct influence that design features have on patient outcomes after PFA [23]. Our results support those posited by previous investigators—patellofemoral implant design significantly affects the complication rate, re-operation rate, and chance of undergoing a revision arthroplasty.
Our comparison of patients who were treated with second-generation PFA designs versus TKA showed no difference in the rate of complications, re-operation, or revision arthroplasty. Additionally, length of follow-up did not significantly influence any of these outcomes when comparing second-generation PFA and TKA. These observations, when coupled with our findings of an improved complication profile with second-generation PFA designs, provide support for the use of current (second-generation) designs for patellofemoral arthroplasty when treating isolated PF OA. The mechanical complications and subsequent re-operations that affected first-generation of PFA designs appear to be of less concern with proper patient selection, meticulous surgical technique, current implant designs and peri-operative care. The possibility of providing an effective surgical treatment that preserves the remaining tibiofemoral articulations without subjecting patients to a higher likelihood of complications or re-operations is certainly promising. While it is difficult to predict the survivorship of current PFA designs, it is our expectation that patient selection (such as younger or more active patients) will continue to be a critical component in determining these long-term results. The majority (16) of the 28 studies included in the current meta-analysis did not report whether patellofemoral instability or trochlear dyplasia was present in patients that were indicated for either PFA or TKA, therefore precluding us from evaluating this variable as a predictor for postoperative complications. However, the experience reported by de Cloedt and colleagues [10] revealed better outcomes in patients who undergo PFA because of arthritis in the presence of patellofemoral instability and trochlear dysplasia than those that undergo PFA for primary OA. This is likely due to the fact that PF OA is isolated to the patellofemoral compartment in patients with instability and dysplasia, while primary OA continues to progress as a tricompartmental disease.
The study has several limitations. First, patient-centered outcomes were not included as they are not always reported or are reported with a non-uniform scale. Consequently, no patient-centered outcome conclusions can be made. Instead, we focused on information that is generally reported in the clinical studies that the practicing orthopaedic surgeon may need to discuss benefits and drawbacks of PFA and TKA with patients. Moreover, given that the first-generation of PFA implants were largely abandoned, a comparison with a second generation PFA is provided. Secondly, there are no prospective cohort studies to compare the two treatments. Based on the low prevalence of isolated PFA and the low utilization rate of PFA, such study may not be feasible. To overcome this limitation and the lack of quantitative information in the current literature, we performed a rigorous pooled-proportions meta-analysis. We were able to adjust for length of follow-up and used a regression model to look at the influence of each increasing year of follow-up on complication, re-operation, and revision rates. Thirdly, all 28 studies analyzed were non-randomized observational studies. While a meta-analysis of randomized controlled trials is certainly preferred, there is a role for statistical syntheses of data from observational studies when high-quality evidence is not available [36]. Finally, our results are based on the pooled analysis of series that utilize multiple prosthetic designs, surgical technique and postoperative care. No conclusions can be drawn regarding the clinical performance of each individual design. While we recognize these limitations, we feel that our meta-analysis provides a quantitative description on the current status of arthroplasty surgery for isolated PFA.
The potential benefit of providing pain relief while preserving the tibiofemoral articulations makes PFA a promising treatment option for patients with isolated PF OA. Further refinement of the ideal patient population for patellofemoral arthroplasty may help in minimizing postoperative complications, improving postoperative function, and delaying progression to tricompartmental osteoarthritis. Our results can be used by the practicing surgeon to counsel patients on the likelihood of re-operation and revision surgery following both historical and modern designs of patellofemoral arthroplasty.
Conclusions
There is a higher likelihood of experiencing complications, re-operation, or revision surgery after PFA when compared to TKA. These differences were present when comparing all generations of PFA designs to TKA. However, when comparing only modern designs of PFA to TKA, there is no significant difference in the frequency of complications, re-operation, or revision surgery.
References
Ackroyd CE, Chir B (2005) Development and early results of a new patellofemoral arthroplasty. Clin Orthop Relat Res 436:7–13
Arciero RA, Toomey HE (1988) Patellofemoral arthroplasty: a three- to nine-year follow-up study. Clin Orthop Rel Res 236:60–71
Argenson JA, Flecher X, Parratte S, Aubaniac J (2005) Patellofemoral arthroplasty: an update. Clin Orthop Rel Res 440:50–53
Arnbjörnsson AH, Ryd L (1998) The use of isolated patellar prostheses in Sweden 1977–1986. Int Ortop 22:141–144
Blazina ME, Fox JM, Del Pizzo W, Broukhim B, Ivey FM (1979) Patellofemoral replacement. Clin Orthop 144:98–102
Butler JE, Shannon R (2009) Patellofemoral arthroplasty with a custom-fit femoral prosthesis. Orthopedics 32:81
Cartier P, Sanouiller J, Khefacha A (2005) Long-term results with the first patellofemoral prosthesis. Clin Orthop Rel Res 436:47–54
Cochran WG (1954) The combination of estimates from different experiment. Biometrics 10(1):101–129
Dalury DF (2005) Total knee replacement for patellofemoral disease. J Knee Surg 18:274–277
de Cloedt P, Legaye J, Lokietek W (1999) Femoro-patellar prosthesis. A retrospective study of 45 consecutive cases with a follow-up of 3–12 years. Acta Orthop Belg 65:170–175
de Winter WE, Feith R, van Loon CJM (2001) The Richards type II patellofemoral arthroplasty: 26 cases followed for 1–20 years. Acta Orthop Scand 72:487–490
DerSimonian R, Laird N (1986) Meta-analysis in clinical trials. Control Clin Trials 7:177–188
Egger M, Smith GD, Schneider M, Minder C (1997) Bias in meta-analysis detected by a simple, graphical test. BMJ 315:629–634
Freeman MF, Tukey JW (1950) Transformations related to the angular and the square root. Ann Math Statist 21:607–611
Higgins JP, Thompson SG (2002) Quantifying heterogeneity in a meta-analysis. Stat Med 21:1539–1558
Jørgensen PS, Konradsen LA, Mati WB, Tørholm C (2007) Treatment of patellofemoral arthritis with patello-femoral arthroplasties. Ugeskr Laeger 169:2201–2204
Kooijman HJ, Driessen APPM, van Horn JR (2003) Long-term results of patellofemoral arthroplasty: a report of 56 arthroplasties with 17 years of follow-up. J Bone Jt Surg Br 85-B:836–840
Krajca-Radcliffe J, Coker TP (1996) Patellofemoral arthroplasty: a 2- to 18-year followup study. Clin Orthop Rel Res 330:143–151
Laskin RS, van Steijn M (2009) Total knee replacement for patients with patellofemoral arthritis. Clin Orthop Rel Res 367:89–95
Leadbetter WB, Kolisek FR, Levitt RL et al (2009) Patellofemoral arthroplasty: a multi-centre study with minimum 2-year follow-up. Int Orthop 33:1597–1601
Leadbetter WB, Ragland PS, Mont MA (2005) The appropriate use of patellofemoral arthroplasty: an analysis of reported indications, contraindications, and failures. Clin Orthop Rel Res 436:91–99
Lonner JH (2008) Patellofemoral arthroplasty: the impact of design on outcomes. Orthop Clin North Am 39:347–354
Lonner JH (2004) Patellofemoral arthroplasty: pros, cons, and design considerations. Clin Orthop Rel Res 428:158–165
Lubinus HH (1979) Patella glide bearing total replacement. Orthopedics 2:119–127
Meding JA, Wing JT, Keating EM, Ritter MA (2007) Total knee arthroplasty for isolated patellofemoral arthritis in younger patients. Clin Orthop Rel Res 464:78–82
Merchant AC (2005) A modular prosthesis for patellofemoral arthroplasty: design and initial results. Clin Orthop Rel Res 36:40–46
Mertl P, Van FT, Bonhomme P, Vives P (1997) Femoropatellar osteoarthritis treated by prosthesis. Retrospective study of 50 implants. Rev Chir Orthop Reparatrice Appar Mot 83:712–718
Mihalko WM, Boachie-Adjei Y, Spang JT, Fulkerson JP, Arendt EA, Saleh KJ (2007) Controversies and techniques in the surgical management of patellofemoral arthritis. J Bone Jt Surg Am 89:2788–2802
Mohammed R, Jimulia T, Durve K, Bansal M, Green M, Learmonth D (2008) Medium-term results of patellofemoral joint arthroplasty. Acta Orthop Belg 74:472–477
Mont MA, Haas S, Mullick T, Hungerford DS (2002) Total knee arthroplasty for patellofemoral arthritis. J Bone Jt Surg Am 84:1977–1981
Odumenya M, Costa ML, Parsons N, Achten J, Dhillon M, Krikler SJ (2010) The Avon patellofemoral joint replacement: five-year results from an independent centre. J Bone Jt Surg Br 92-B:56–60
Parvizi J, Stuart MJ, Pagnano MW, Hanssen AD (2001) Total knee arthroplasty in patients with isolated patellofemoral arthritis. Clin Orthop Rel Res 392:147–152
Sisto DJ, Sarin VK (2006) Custom patellofemoral arthroplasty of the knee. J Bone Jt Surg Am 88:1475–1480
Slim K, Nini E, Forestier D, Kwiatkoski F, Panis Y, Chipponi J (2003) Methodolical index for non-randomized studies (MINORS): development and validation of a new instrument. ANZ J Surg 73:712–716
Smith AM, Peckett WRC, Butler-Manuel PA, Venu KM, d’Arcy JC (2002) Treatment of patello-femoral arthritis using the Lubinus patello-femoral arthroplasty: a retrospective review. Knee 9:27–30
Stroup DF, Berlin JA, Moron SC, Olkin I, Williamson GD, Rennie D, Moher D, Becker BJ, Sipe TA, Thacker SB (2000) Meta-analysis of observational studies in epidemiology: a proposal for reporting. JAMA 283:2008–2012
Tauro B, Ackroyd CE, Newman JH, Shah NA (2001) The Lubinus patellofemoral arthroplasty: a five- to ten-year prospective study. J Bone Jt Surg Br 83-B:696–701
Thompson NW, Ruiz AL, Breslin E, Beverland DE (2001) Total knee arthroplasty without patellar resurfacing in isolated patellofemoral osteoarthritis. J Arthroplast 5:607–612
Utukuri MM, Khanduja V, Somayaji HS, Dowd GSE (2008) Patient-based outcomes in patellofemoral arthroplasty. J Knee Surg 21:269–274
van Jonbergen H, Poolman RW, van Kampen A (2010) Isolated patellofemoral osteoarthritis: a systematic review of treatment options using the GRADE approach. Acta Orthop 81:199–205
Acknowledgments
The authors would like to thank Mr. Soloman Melkman, whose generous contributions helped to fund the current study. The authors would like to thank Mr. Timothy Roberts and Miss Indira Garcia from the Medical Library at Hospital for Special Surgery for their assistance in gathering articles for the meta-analysis; and Mr. Huibo Shao for his assistance in the statistical modeling. The authors would also like to thank Dr. Beth Shubin Stein for her critical review of the manuscript.
Conflict of interest
None of the authors have any potential conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
Investigation performed at Hospital for Special Surgery, New York, NY.
Appendices
Appendix 1
See Table 5.
Appendix 2
See Table 6.
Appendix 3
See Table 7.
Appendix 4
See Table 8.
Rights and permissions
About this article
Cite this article
Dy, C.J., Franco, N., Ma, Y. et al. Complications after patello-femoral versus total knee replacement in the treatment of isolated patello-femoral osteoarthritis. A meta-analysis. Knee Surg Sports Traumatol Arthrosc 20, 2174–2190 (2012). https://doi.org/10.1007/s00167-011-1677-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-011-1677-8