
Abstract
This CIRSE Standards of Practice document is aimed at interventional radiologists and provides best practices for performing transarterial chemoembolisation. It has been developed by an expert writing group under the guidance of the CIRSE Standards of Practice Committee. It will encompass all technical details reflecting European practice of different TACE procedures (Lp-TACE, DEM-TACE, DSM-TACE, b-TACE) as well as revising the existing literature on the various clinical indications (HCC, mCRC, ICC, NET). Finally, new frontiers of development will also be discussed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The CIRSE Standards of Practice Committee established an expert writing group, which was tasked with updating the previous CIRSE Standards of Practice (SOP) document on performing transarterial chemoembolisation (TACE) by Basile et al. [1]. CIRSE Standards of Practice documents are not clinical practice guidelines or systematic reviews of the literature. This SOP document is not intended to impose a standard of clinical patient care but recommends a reasonable approach to best practices for performing TACE.
Methods
The writing group was established by the CIRSE Standards of Practice Committee, comprising members with internationally recognised expertise in TACE. A systematic literature search was carried out using PUBMED and EMBASE to identify relevant publications in English from 2012 to 2020. Recommendations were then formulated through consensus.
Background
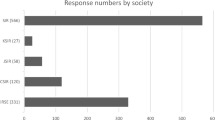
The history of TACE dates back to the late 1970s, with the first evidence for TACE being published by Yamada et al. in 1979 [2,3,4]. However, after forty years there is no standard technique regarding all aspects of the procedure including drugs, embolic materials, and microcatheter selection, as demonstrated by a recently published international survey [5, 6]. In the treatment of hepatocellular carcinoma (HCC), doxorubicin is the most commonly used chemotherapeutic agent, although several other drugs are also used, including epirubicin, cisplatin, mitomycin C, and 5-fluorouracil [7]. Concerning the embolic material, TACE has classically been performed with an emulsion of lipiodol and chemotherapeutic drugs followed by gelfoam (conventional TACE or cTACE [1]). In 2006, Hong et al. [8] were the first to report a new drug-delivery system: drug-eluting microspheres (DEM). This device is capable of slowly releasing the loaded drug to the liver. DEM showed a better safety profile with lower systemic drug-related toxicity, although without significant added value on local tumour control over cTACE [9]. Moreover, in recent years the use of a degradable embolic/carrier material (Degradable Starch Microsphere or DSMTACE) has been proposed for selected advanced HCC patients [10,11,12] intrahepatic cholangiocarcinoma (ICC) [13] and metastases from colorectal cancer (mCRC) [14]. With regards to microcatheter selection, in 2013, Irie et al. [15] developed the concept of balloon-occluded TACE (b-TACE), a modified procedure, in which a balloon microcatheter is inflated within the arterial feeder(s) permitting pressure-driven embolisation.
Nowadays, indications for TACE include primary and secondary liver tumours, including HCC, ICC, mCRC and metastases from neuroendocrine tumours (NET) [16, 17]. HCC and ICC account for 9.1% of all cancer deaths worldwide [16]. Half of all patients with CRC develop liver metastases during the course of the disease [16]. The liver is also the most common site of metastases from NET [18].
Considering the plethora of technical variations currently available, the aim of this document is to provide an update on all techniques and new developments.
Patient Preparation
Pre-Treatment Imaging
According to international guidelines, multidetector computed tomography (MDCT)/magnetic resonance imaging (MRI) is capable of establishing the diagnosis of HCC in cirrhotic patients in lesions greater than 10 mm [19]. In most other tumours (mCRC, ICC, NET), confirmatory biopsy is usually preferred before planning a TACE session. In addition, due to the increased use of precision medicine, evidence in favour of biopsy of suspected HCC is accumulating [20].
At least one dynamic contrast-enhanced imaging technique (MDCT or MRI) should be performed prior to TACE, preferably within one month before the procedure.
Several factors should be assessed: vascular anatomy, size and number of liver tumour(s), extrahepatic spread and presence of absolute and/or relative contraindications for TACE [1, 21, 22].
Vascular anatomy is best shown on MDCT imaging [23] and is not limited to identification of the anatomic variants of the hepatic vasculature but also includes identification of parasitic tumour feeders. This is crucial for determining the appropriate catheter selection and deciding on treatment plans.
With regards to tumour spread: size, numbers of lesions (single vs multifocal; uni-lobar vs bilobar) and percentage volume of tumour spread should be assessed. HCC lesions greater than 3 cm are often associated with the need for multiple treatments, and tumour involvement >50% of the liver volume is associated with a poor prognosis [24]. Presence and extension of portal vein thrombosis must be assessed, as it influences prognosis and risk of the procedure.
Finally, predisposing factors for liver abscess have to be assessed in order to establish proper treatment. These factors include:
-
dilation of the biliary tree
-
biliary/gallbladder lithiasis
-
presence of biliary prosthesis (plastic, metallic)
-
presence of a bilioenteric anastomosis
-
presence of transjugular intrahepatic portosystemic shunt (TIPS) [1, 25].
Indications and Contraindications for TACE
Since TACE is usually implemented in complex, disease-stage related treatment algorithms, it is mandatory that the therapy decision is made by a multidisciplinary tumour board, which includes hepatologists, oncologists, surgeons, diagnostic and interventional radiologists.
With regards to HCC, indications for TACE follow the Barcelona Clinic Liver Cancer (BCLC) recommendations. They have recently been amended to include Stages 0-A as well as Stage B in the transplant setting with a class of recommendation of IB and IA, respectively [26]. The aims of TACE could be: reducing the total tumour burden to within the transplant criteria (down-staging), controlling tumour growth in a patient who is on the transplant list (bridging), and increasing survival in patients not eligible for transplantation (palliative).
Indications for TACE in ICC include surgically unresectable or inoperable liver tumours with liver-only or liver-dominant disease [17].
In the setting of mCRC, patients with liver-limited disease in whom the available chemotherapeutic lines have failed, TACE may be also considered as a treatment option [27].
TACE can also be considered as an alternative therapy to surgical resection of liver metastasis in patients with NET and as an alternative to systemic treatment in those patients with NETs with disease limited to the liver [28].
Absolute contraindications for TACE include: portal vein neoplastic thrombosis or hepatofugal blood flow, impaired hepatic function (Child-Pugh B8 or greater), poor performance status (ECOG P2 or greater), contraindication for arteriography (uncorrectable thrombocytopenia, coagulopathy, severe renal insufficiency or severe reaction to contrast media) [1, 17].
Relative contraindications for TACE include: TIPS, segmental or subsegmental non-neoplastic portal vein thrombosis.
Finally, patients with tumour burden >50% of liver volume are unlikely to benefit from treatment.
Laboratory Findings
Laboratory markers for diagnosing and assessing the extent of potential hepatocytic damage, and monitoring therapy effects on liver function are:
-
aminotransferases (ALT)
-
cholinesterase
-
alkaline phosphatase (ALP)
-
γ-glutamyl transferase (γGT)
-
bilirubin
-
albumin
-
prothrombin time (e.g. PT is increased for a longer period of time in hepatocellular insufficiency, and diminished in cholestasis based on Vit K malabsorption)
-
creatinine and electrolytes
This panel of analysis may be repeated within 24–48 hours after the intervention, and throughout the clinical follow-up in order to detect potential treatment-related liver toxicity early.
Serum alpha-fetoprotein (AFP) is the most widely used tumour marker in patients with HCC and has been proven to have capability of prefiguring the prognosis [29] and aid in monitoring for tumour recurrence [30]. Recently it has been shown that protein induced by vitamin K absence, antagonist-II (PIVKA-II), effectively increases the detection rate of HCC as a valid complement to AFP and imaging surveillance [31]. Carcinoembryonic antigen (CEA) and carbohydrate antigen 19–9 (CA 19–9) are the markers usually employed in mCRC patients [32]. For NETs, the commonly used serum markers are neuron-specific enolase (NSE) and chromogranin A [33].
Although there is no ultimate risk stratification tool, several scorings systems which take into account laboratory and clinical parameters are applied in clinical routine. To estimate the procedure-related risk versus the therapeutic benefit, the Child-Pugh score is well accepted for HCC in liver cirrhosis. According to the BCLC/EASL guideline, patients with Child-Pugh score of less than B8 are well suited for TACE [34], that is based on both clinical and laboratory values. Recently, the albumin-bilirubin (ALBI) score has been proposed as a simple and objective method of assessment which removes the need for subjective clinical variables. It has been established as a prognostic tool not only for HCC [35] but also for the therapy of metastatic liver disease [36].
Finally, there is increasing evidence that systemic inflammation correlates with cancer patients’ survival and prognosis. In recent years, various markers of systemic inflammatory response including cytokines, neutrophil to lymphocyte ratio (NLR) and platelet to lymphocyte ratio (PLR) are being investigated as prognostic markers in patients treated with TACE, but these markers are currently not used in clinical practice [37].
Preparing the Patient
It is recommended that patients should fast > 6 hours prior to the procedure.
As in any other invasive intervention, some standard prerequisites are mandatory:
Medication and Peri-Procedural Care
Periprocedural medication may include intravenous hydration, analgesia, anxiolytics, antibiotic prophylaxis (only for specific situations), dexamethasone [39], non-steroidal anti-inflammatory drugs (NSAID), anti-emetics and gastric protection with proton pump inhibitors [40].
TACE in HCC has a low incidence of side effects. However, procedures in younger patients, higher dosage of applied chemotherapies, and in the absence of chronic liver disease such as patients with mCRC, are more prone to pain necessitating peri- and post-procedural analgesia [41, 42]. TACE with irinotecan in mCRC patients should not be performed without appropriate analgesia and anaesthetic support is advised. A proposed medication protocol for mCRC patients is shown in Table 1 [40]. For more information on the use of analgesia and sedation, please refer to the “CIRSE Standards of Practice on Analgesia and Sedation for Interventional Radiology in Adults” [43].
Routine antibiotic prophylaxis is not recommended. However, in scenarios with an increased risk of developing liver abscess, prophylactic antibiotics are recommended. These include biliary obstruction or the presence of a bilioenteric anastomosis. The choice of agent is dependent on the suspected pathogens (upper gastrointestinal tract flora) and consideration should be given to potential hepatotoxicity of each agent. Discussion with microbiologist may be useful in complex cases involving multiple organisms, antibiotic resistance or allergies. Guidelines on the use of antibiotics in IR procedures are presented by Chehab et al. which is endorsed by CIRSE, SIR and CIRA [44].
According to the Society of Interventional Radiology and CIRSE Standards of Practice documents on peri-procedural bleeding [45, 46], TACE carries a moderate risk of bleeding. Therefore, INR should be corrected to less than 1.5, and platelets transfusion recommended for counts less than 50,000/ul, clopidogrel should be suspended for 5 days before the procedure. Aspirin may be continued. Therapeutic dose low-molecular-weight heparin should be withheld for 24 h.
Treatment
Vascular Access to Diagnostic Angiography and CBCT
Detailed knowledge on the normal and variant anatomy of the visceral and hepatic arterial anatomy and familiarity with suitable catheters and guidewires, liquid and particulate embolic agents and applicable chemotherapeutics is vital.
Multiphasic contrast-enhanced CT and MRI and cone beam CT (CBCT) are helpful tools for pre-procedure planning [47]. CBCT has shown superior tumour and tumour feeder detection compared to digital subtraction angiography (DSA) [48], as well as permitting detection of occult nodules [49], thus improving treatment outcomes [50]. It is particularly useful for hypovascular lesions (mCRC and ICC) as it facilitates visualisation [51, 52]. A summary of recommendations is shown in Table 2. Moreover, the increased availability of hybrid angiographic/computed tomography allowing to perform CT hepatic arteriography and CT arterio-portography, may improve tumour detection, pre-treatment planning and treatment outcome [53, 54].
TACE Techniques
Conventional Transarterial Chemoembolisation (cTACE) or Lipiodol TACE
Lipiodol (Guerbet, France) is an ethyl ester of iodized fatty acids of poppy seed oil. Lipiodol TACE, also called conventional TACE (cTACE), consists of intra-arterial injection of a mixture of lipiodol and one of several anticancer drug(s), followed by the administration of an embolic agent.
Lipiodol-Based Emulsions
Lipiodol has a plastic and transient embolic effect [52, 55] but does not have a significant cytotoxic effect on its own [56], which necessitates combination with anticancer agents.
Most cytotoxic drugs are more soluble in water than in lipiodol, explaining why an emulsion (mixture of two liquids that are unmixable) is used for cTACE [57]. Two different emulsion types can be distinguished: water-in-oil (W/O) emulsion where the drug (water droplets) is “loaded” in lipiodol (oily droplets), and the opposite oil-in-water (O/W) emulsion.
Accumulating evidence shows that W/O emulsions result in:
cTACE emulsion is usually prepared using the pumping technique through a three-way metal stopcock [61]. Lipiodol can cause cracking or crazing of polycarbonate three-way stopcocks, while polypropylene, polyamide, and polysulphide have higher durability [62]. In order to favour a W/O emulsion, the volume of lipiodol should be greater than the volume of drug in aqueous solution, ideally a 2:1 or 3:1 lipiodol:drug ratio [63,64,65]. Instead of water for injection, non-ionic contrast medium can be used for preparation of doxorubicin solution in order to improve stability of doxorubicin-lipiodol [66], but this preparation is considered off-label by pharmacists.
The speed of incorporation of doxorubicin in lipiodol is crucial to favour W/O emulsions. While bolus injection (i.e. injection of the entire volume of doxorubicin into the entire volume of lipiodol) results in W/O emulsion in only 6.25% cases, incremental (subsequent injections of aliquots of doxorubicin in the entire volume of lipiodol) or continuous (continuous incorporation of doxorubicin using an electric syringe pump at 1ml/min) injection allow obtaining W/O emulsions in 93.7–100% cases [64]. As each drug has its own hydrophilic-lipophilic balance, these characteristics may not apply to other cytotoxic drugs.
Emulsion Stability
Intuitively, the more stable the emulsion, the higher chance for lipiodol to carry the drug into the tumour owing to its targeting ability for hypervascular liver tumours. Unstable lipiodol-based emulsions result in a distribution of anticancer drug within the arterial bed that is not guided by lipiodol [67]. On the contrary, stabilising emulsions reduces systemic exposure [63, 64] and increases early accumulation of the drug within the tumour [64]. From a practical perspective, high ratios of lipiodol/drug also increased emulsion stability with both doxorubicin [64] and idarubicin [63].
Whatever the technique used to emulsify lipiodol and doxorubicin, at least 20 pumping exchanges through the stopcock are needed to favour the production of “large” droplets [59] although any emulsification process basically provides polydisperse coexistence of small and large droplets [57]. “Large” droplets (70–100 µm) limit the risk of reaching the lung, which can cause subsequent toxicity, and increase tumour:non-tumoural liver uptake [55].
Given the instability of most lipiodol-drug emulsions, they should be prepared extemporaneously immediately before transcatheter administration, and they may need to be re-emulsified through the stopcock when phase separation is observed during the procedure. Most IRs use less than 10 ml of lipiodol [5] for cTACE. For safety reasons, it is recommended to use a total volume of less than 20 ml [68] in order to minimise the risk of pulmonary lipiodol embolism, which can be fatal.
Embolisation in cTACE
Embolisation is widely adopted as the second part of the cTACE procedure immediately after injection of lipiodol-based emulsion, in order to induce or enhance tumour ischaemia and prevent washout of the drug. Histological data showed increased necrosis in both the main tumour and daughter nodules with doxorubicin cTACE, versus doxorubicin/lipiodol (without embolisation) and lipiodol alone [56]. In a recent international survey [5], spherical embolic particles were used by 47.9% responders followed by gelatine sponge particles by 36.8%. There is paucity of data regarding the best embolic agent with literature recommending both agents. Gelatine sponge has the advantage of resorbability within 1–2 weeks [69], allowing for subsequent TACE session through the same tumour feeders. Hand cutting of small (≈1–1.5mm) gelfoam pieces provides more uniform particle sizes and should be recommended when using the “pumping’’ technique through a three-way stopcock [70]. As the threshold separating intra-tumoural (smaller) from extra-tumoural vessels (larger) is ≈300µm [71, 72], non-resorbable calibrated microspheres ranging 100–300 µm are recommended that favour intra-tumoural ischaemia while preserving the patency of extra-tumoural arteries, and limit the risk of complications due to very small particle size, such as pulmonary embolism [73] or biliary ischaemia. Regardless of the choice of embolic agent, only a small volume is usually required after administration of the lipiodol-based emulsion. However, the occlusion by gelatine sponge is often temporary and flow may be restored within a few minutes. In addition, calibrated microspheres can take minutes to reach the core of the tumour and the recommendation is to wait at least 5 min prior to the final embolisation to ensure a stronger embolic effect [61]. The endpoint is a ‘‘tree-in-winter’’ appearance with occlusion of small tumour-feeding radicals but preservation of flow in the major lobar and segmental arteries in order to preserve them for subsequent embolisation. With regards to what degree of portal vein visualisation should be achieved during lipiodol injection, it has been demonstrated that grade 2 segmental visualisation correlates with lower recurrence rate [61, 74].
DEM-TACE
Drug-eluting microspheres are embolic agents that allow loading with anthracyclines (doxorubicin, epirubicin, idarubicin) and irinotecan through an ionic interaction of the cationic drug with the anionic functional groups of the microspheres. Currently, various types of drug-eluting microsphere (DEM) are commercially available for use with doxorubicin, with some differences in elution and suspension characteristics [75].
As a general rule, the maximum dose of doxorubicin that can be administered safely to an adult patient in a single session is 150 mg [76]. Drug dosage does not require adjustment according to body surface area (BSA) or weight. According to this rationale, treatment priority should be given to the target lesion. Each vial of DEM, comprising of 2 ml of beads, is loaded with 50–75 mg doxorubicin or epirubicin. This equates to a loading dose of 25–37.5 mg doxorubicin per 1 ml of beads. Cardiac toxicity of anthracyclines is cumulative and observed above a certain threshold. For example, 450 mg/m2 for doxorubicin. Four sessions of 150 mg doxorubicin TACE can be performed safely with regard to cardiac toxicity, but not more [77, 78].
With regards to DEM bead size, it is worth highlighting that since 2012, when the recommended size for a standard procedure was usually 100–300 microns, there is a growing body of literature reporting a comparable safety and efficacy profile of particle sizes smaller than 100 microns [79,80,81,82,83,84,85,86]. Nevertheless, using beads less than 100 microns requires caution when superselective catheterisation of the feeder is not achieved as there is increased risk of hepatobiliary complications [87]. Combinations of different calibre beads can offer the advantage of high-drug penetration of tumour and effective obstruction of feeding arteries [88].
DEM are administered using a 1–3 ml syringe, mixed with contrast. It is important to follow preparation steps specific to each type of DEM according to the IFU of each manufacturer. In all cases, a good suspension of DEM is required before delivery. Either contrast or saline/water can be added depending on the concentration of beads and fluid density.
The aim during infusion is to deliver the maximum DEM into the target lesion. The infusion must be slow, with smooth pulses, to the normal arterial flow to push the beads into the tumour feeders. Care should be taken to avoid sedimentation of the beads in the syringe by rotating the syringe or using a three-way stopcock to gently suspend the beads in solution. The beads are administered under continuous fluoroscopic monitoring until stagnation of flow is achieved, counting 10 cardiac beats as a guide. At this point, the injection should be stopped, regardless of the volume of beads administered, in order to avoid reflux of embolic material [89].
As stated before, the basis of treatment relies on both cytotoxic and anoxic effects, and as such, the treatment endpoint is complete tumour devascularisation. Following this logic, it has been suggested that if arterial stasis is not achieved after injection of the scheduled volume of DEMs, additional unloaded beads should be injected until the endpoint of arterial stasis has been reached. However, there is no definite evidence to support this statement and some groups recommend scheduling a repeat course of treatment.
There are no technical differences in transarterial chemoembolisation of HCC, ICC and NETs. With regards to functional NETs, it is important to note that TACE should be performed early following somatostatin analogue (SSA) therapy, in order to improve hormonal symptom control and to prevent complications, such as carcinoid crisis in serotonin secreting NETs [28].
There are several technical differences to consider in chemoembolisation of mCRC. First, delayed CBCT acquisition is integral in the patient work-up to ensure detection of all hypovascular lesions [52, 90]. Second, depending on the extent and distribution of disease, it is decided to perform a single lobe (2 treatments at 4 weeks interval) or a bilobar treatment (4 treatments, at 2 weeks interval), with the first targeted to the lobe more involved by disease. Third, the embolisation endpoint is the delivery of the planned dose of anticancer agent, not complete occlusion of feeding vessels. Fourth, the recommended bead size is less than 100 microns [91]. Finally, the chemotherapy of choice is Irinotecan with the usual standard dose of 100 mg for each lobar treatment.
When the treatment is considered finished, a final angiography could be performed to assess tumour devascularisation. Alternatively, in order to save contrast media, unenhanced CBCT can be used to immediately assess the deposition of the embolic agent.
DSM-TACE
Degradable starch microspheres (Embocept®, PharmaCept) consist of resorbable amilomer (hydrolysed potato starch) based particles, ranging around average 45 ±7 μm, that can be mixed with a wide range of chemotherapeutic agents [10, 92]. These particles act as carriers and show no chemical binding with the selected drug. The microspheres are enzymatically degraded by amylase in the blood with a half-life of about 35–50 minutes. The particles are completely resorbed after approximately 2 hours [10].
The drug is usually mixed immediately before administration using 4 ml out of a 7.5 ml DSM vial, then mixed in suspension with adjunctive contrast media (around 15–20 ml). The solution is then infused via a coaxially positioned microcatheter, to control reflux [93]. The treatment consists of administering the total predicted dose of drug, followed by the residual part of the DSM vial, used as unloaded temporary embolic agent. The aim of embolisation with the non-loaded DSM is temporary cessation of flow within the treated artery. Depending on the degree of selectivity and vessel size, an additional second vial of unloaded DSM may be needed, or alternatively gelfoam can be used. Embolisation to stasis is a crucial end-point to allow adequate drug absorption within the target lesion. Since the half-life is short, the goal of the technique is to deliver the maximum amount of drug to the liver and reduce the risk of post-embolisation syndrome from a reduced ischaemic time [10].
Usually, administration is performed multiple times, at least twice for each treatment site. In case of bilobar tumour spread and to avoid whole liver treatments that could impair liver function, the lobe with greater tumour involvement is treated first, followed after 14 days by the contralateral lobe. After two more weeks, the treatment cycle can be repeated [93].
The main advantage of DSM-TACE is that it may be used in patients with a bilirubin greater than 3 mg/dl and portal vein thrombosis [10].
B-TACE
In 2013, Irie et al. [15] developed a variant of the TACE procedure using a temporary occlusion micro-balloon, the so-called b-TACE. The concept of b-TACE is redistribution of blood flow towards the target lesion by performing a pressure-driven embolisation, which occurs because of restoration of flow distal to the temporary occluded vascular segment via collaterals (interlobar, intersegmental arteries) [15, 94, 95]. Micro-balloons (Occlusafe, Terumo, Japan) are positioned proximal to all lesion feeders in order to maximise efficacy. During inflation of the micro-balloon, invasive arterial pressure is monitored to detect a pressure drop. The mean arterial pressure threshold below which the b-TACE effect will perform optimally, is 62 mmHg [96]. It should be remembered that the micro-balloon maximum diameter is 4 mm.
The conventional endpoint of TACE cannot be evaluated due to the inflated micro-balloon. Thus, composite endpoints have been proposed: reflux despite the presence of the inflated micro-balloon, inversion of flow into opened collaterals, perception of resistance, and maximum threshold of drug [95]. b-TACE has the same risks as cTACE and DEM-TACE (biloma, abscess, arterial dissection) with adjunctive potential risk of vascular injury due to micro-balloon inflation. In addition, by allowing access to the peribiliary plexus, terminal arteriosinus twigs and the vasa vasorum, b-TACE may have an increased risk of biliary and vascular damage.
Radiopaque Beads
Contrary to cTACE, where lipiodol may be retained by HCCs for several months, the contrast agent trapped between beads rapidly dissipates after DEB-TACE, which explains why the embolised territory cannot be directly visualised if CT or CBCT acquisition is not performed immediately after the procedure. DC Bead LUMI™ (Biocompatibles UK Ltd, UK) is a drug-eluting technology with iodine incorporated into its chemical structure, ensuring that it is permanently radiopaque [97]. Few studies [97,98,99] have been published with radiopaque beads in humans. They showed safety and response rates comparable to non-radiopaque beads, although no randomised or comparative data are available. Some issues are still under debate, such as the difficulty to ensure reliable imaging follow-up using CT [99] as well as the very different pharmacokinetic profile of drug elution compared to non-radiopaque beads [100]. This would imply that all prior phase I/II data published on doxorubicin-eluting microspheres are not valid with radiopaque beads, which theoretically necessitates specific clinical investigations. Therefore, its place still remains to be defined in the TACE armamentarium.
Intra-Procedural and Immediate Post-Procedural Imaging
Lipiodol use combines both therapeutic effects and visibility on imaging owing to its own radio-opacity. Vascular and tissue distribution can be visualised under fluoroscopy to monitor treatment delivery in real-time. Outside any arterio-venous shunt, lipiodol can deposit in portal branches (first distally) through arterio-portal communications [57].
Immediate post-treatment unenhanced CBCT or CT is recommended to document the precise anatomical area that has been treated and to predict tumour response [49, 101]. In addition, this may be helpful to depict incomplete targeting and to guide further TACE sessions.
Outcomes
Clinical Results
Hepatocellular Carcinoma (HCC)
TACE is recommended as the first-line therapy for intermediate stage HCC (BCLC B) [34, 102, 103]. In comparison to best supportive care (BSC), cTACE showed a decreased relative risk of death ranging from 0.45 (CI95% 0.25–0.81) [112 patients; early interrupted for cTACE superiority over control group], to 0.49 (CI95% 0.29–0.81) [randomisation 1 vs. 1; 80 patients] and a superior overall survival in two RCTs [104, 105]. Moreover, two meta-analyses [106, 107] confirmed an improved 2-year survival rate for cTACE vs. BSC (OR 0.59 [CI95% 0.29–1.20]) and a reduced overall 2-year mortality rate (OR 0.54; [CI95% 0.33–0.89]).
Two randomised controlled trials comparing cTACE to DEM-TACE (PRECISION V, a multicentre, prospective, randomised, single-blind, phase II study which enrolled 212 patients and PRECISION Italia, a multicentre, prospective, randomised, open-label, active-controlled study which enrolled 177 patients), revealed differences in oncological outcome (DEM-TACE vs. c-TACE; complete response 27% vs. 22%, objective response 52% vs. 44%, and disease control 63% vs. 52% p = 0.001). However, a better safety profile and reduced drug-eluted toxicity could be observed in the DEM-TACE group [9, 108]. These findings were confirmed by a meta-analysis which failed to demonstrate DEM-TACE superiority [109]. However, recent growing evidence shows promising results of DEM-TACE, using new material, over both cTACE and TARE (overall survival at 2-years relative risk 0.89; [CI95% 0.81–0.99], p = 0.046 and 0.40 [CI95% 0.19–0.84] p = 0.016, respectively) [110].
Few reports are present in literature regarding indications, in particular, DSM-TACE was employed for HCC as first- [12, 92] or second-line treatment (after Sorafenib cessation) [10]. Moreover, Auer et al. [111] demonstrate, in a small series, similar oncological results comparing with selective internal radiation therapy (SIRT) in multifocal hepatocellular carcinoma.
Limited evidence exists and no conclusive results were found for b-TACE in oncological response, in particular using lipidiol–Ogawa et al. [112] and Irie et al. [113] showed a better tumour response for b-TACE compared with cTACE, while Maruyama et al. [114] failed to demonstrate a difference in tumour control between the two techniques. To our knowledge, only two studies evaluated the combination of DEM-TACE with balloon microcatheter [95, 115] reporting an objective response of 90% and 100%, respectively. Thus, there is no standard indication for b-TACE procedure, however, some reports suggested better results for HCC > 3 cm with higher progression-free survival. In a retrospective European multicentric registry (96 patients b-TACE vs 434 patients non b-TACE with propensity score matching) b-TACE had a better complete response at 1 month (59.3% vs. 41.8%; p = 0.026), a lower rate of retreatment (9.9%% vs. 22.0%; p = 0.041) and a higher rate of post-embolic syndrome (41.8% vs. 8.8%; p < 0.001) [116]. Because the existing evidence is still limited, micro-balloon or flow directing microcatheters should be used only in trials.
Colorectal Liver Metastases (mCRC)
There is very limited evidence for cTACE in mCRC (RCT 112 patients). Several chemotherapy agents such as mitomycin C, mitomycin C plus irinotecan and mitomycin C plus gemcitabine [117] had been applied resulting in 1- and 2-year survival rates of 62% and 28% and a median time to progression of 5 months [118] – comparable to standard systemic chemotherapy. In contrast, in a single-arm multicentre study in 55 chemotherapy-naïve patients applying DEM-TACE loaded with irinotecan (DEBIRI), Martin et al. [119] demonstrated a median time to progression of 11 months with an overall survival of 19 months. Fiorentini et al. [120] confirmed these results in a randomised controlled trail in 74 patients where DEBIRI resulted in a significantly longer overall survival in comparison to systemic FOLFIRI (22 months [CI 95% 21–23] vs. 15 months [CI 95% 12–18]). Moreover, Iezzi et al. [121] in a single centre study with 20 patients and 54 treatments, demonstrated a role of DEBIRI + systemic Capecitabine in chemotherapy-refractory patients (first or second line). In a current meta-analysis, Levy et al. [122] highlighted comparable response rates of 23% (CI 95% 9.7–36) for cTACE and 36% (CI 95% 0–73) for DEM-TACE and 1-year survival rate of 70% (CI95% 49–87) for cTACE and 80% (CI 95% 74–86) for DEM-TACE. Current smaller studies on DSM-TACE in CRC could demonstrate an objective response in 40.0% of patients and disease control in 64.9% [14]. Latest available evidence on multicentre prospective controlled registries (CIREL cohort) demonstrated an acceptable toxicity profile and a stable or improved health-related quality of life [123]. Nevertheless, the evidence is still too scarce for any recommendation.
Intrahepatic Cholangiocarcinoma (ICC)
In ICC clinical outcome data for hepatic arterial perfusion, cTACE and TARE are still controversial [124]. While early studies report a median OS of 13 months without any difference between cTACE, bland, DEB-TACE and TARE [125], more recent reviews describe a wider range between 12 and 25.2 months of OS for TACE and between 14.9 and 43.7 months for TARE [126, 127]. Moreover, DSM-TACE showed a disease control rate in 44% of patients in 7 patients [12, 128]. Consequently, current guidelines do not make any distinct recommendations regarding a specific transarterial treatment.
Neuroendocrine Tumour (NET)
Most international guidelines endorse cTACE as a validated treatment option either to control tumour symptoms in secreting NETs and/or to control disease progression [28, 33]. In cTACE, the median overall survival ranges from 24 to 44 months in a retrospective series of 192 patients [129] reaching an overall survival rate of 36% at 5 years, also in a retrospective report of 123 patients [130]. In addition, Minh et al. [129] demonstrated a significantly longer median overall survival for cTACE (33.8 months) compared with DEM-TACE (21.7 months, p < 0.01) or Y90 (23.6 months, p = 0.02), whereas it remains unclear which patient-specific parameters might explain these results.
Procedure Specific Complications
Complications in the context of TACE occur in about 10% of cases and should be documented in a standardised fashion [131, 132].
According to the time of occurrence, adverse events can be divided into:
-
intra-procedural (e.g. catheter/guidewire induced vascular injury or haemorrhage, immediate vascular thrombosis, aberrant embolisation)
-
peri-procedural (metabolic impairment), delayed (e.g. liver failure, peribiliary necrosis)
-
minor and major (all events as abscess, bilioma, haemorrhage, liver failure, vascular damage that need some kind of intervention) (Table 3).
In contrast to adverse events, post-embolisation syndrome (PES) is not considered a complication and is expected in about 30% of cases as an effect of an efficient chemoembolisation. PES is usually self-limiting and should last only a few days within the first two weeks after the procedure. It is typically characterised by nausea, vomiting, fever, pain, and fatigue necessitating no or only symptomatic treatment. In rare, cases it may last up to four weeks post-TACE. Longer-lasting symptoms should prompt evaluation for other causes.
While most minor complications by definition do not need any or only symptomatic treatment, the management of major complications may necessitate a wide range of radiological, medical, and surgical procedures. Vascular complications as haemorrhage, dissection or pseudoaneurysm of the celiac trunk or hepatic artery are rare and should whenever possible be treated by interventional techniques. Infectious conditions, such as cholangitis, cholecystitis, but also initial abscesses, infected haemangiomas or bilomas are initially treated using antibiotics. In liquified infected fluid collections, percutaneous drainage is appropriate and a surgical intervention may be necessary in rare cases.
Post-procedural and Follow-up Care
Imaging Follow-Up
Imaging Modalities
The type of imaging follow-up used for assessment of treatment response as well as the timing and frequency of imaging follow-up varies depends on the nature of the target tumour and may also be influenced by the use of other tumour markers and metabolic imaging techniques. Imaging follow-up is mainly performed with cross-sectional techniques such as CT and MRI with nuclear imaging (PET) playing a smaller role, mainly for mCRC and mNET [133, 135].
Tumour Types
For HCC both MRI and CT are appropriate techniques, but MRI is the modality of choice for response evaluation in cTACE because tumour lipiodol deposition can make tumour enhancement difficult to appreciate on contrast-enhanced CT-scan, even though tumour lipiodol uptake at CT is associated with both tumour response [136] and survival [137].
The timing of post-procedural imaging is widely adopted and accepted as 4 weeks from the completion of treatment in the first instance [138]. Follow-up after that should be performed every 3 months [34] as this has been demonstrated to lead to a better overall survival in high-risk HCC patients as compared to using longer imaging intervals [139]. Tumour response should be categorised according to mRECIST criteria, as this takes the viable part of the tumour (arterial enhancement) into account rather than the size of both viable and non-viable tumours [140]. Tumour markers such as AFP and DCP may help to evaluate complete necrosis (therefore the effect of the treatment) in partial response setting, especially in tumours that actively produce these markers prior treatments, in which imaging may fail to demonstrate the residual/necrosis proportion and may also detect recurrence before imaging demonstrates it [138].
For mCRC, RECIST version 1.1 [141] should be used for assessing radiological response of oncological patients, but adjunctive evaluation using the Choi et al. criteria, which measure the attenuation coefficient may also be quite useful as mCRC is usually hypovascular [142]. The timing and the duration of the radiological follow-up for mCRC in stage II and III depends on different guidelines ranging from 6 to 12 months [133]. CEA is fundamental in clinical follow-up and should be assessed every 3–6 months [133].
For ICC, guidelines are less standardised in terms of follow-up timeline as compared to other tumour types, but an imaging evaluation every 2–4 months for 2 years seems reasonable, along with evaluation of CEA and CA19-9 [135].
For NET, imaging after curative surgery should be performed every year for the first 3 years [28, 134], and after TACE a more narrow imaging interval (3–6 months) is not clearly stated by internationally accepted guidelines. However, it seems reasonable to propose surveillance with 3–6-month intervals in order to promptly identify radiological recurrence, eligible for adjunctive treatment. For non-functioning NET, oncological markers are functionally useless and, although serial evaluation seems reasonable, there is no robust evidence for its use [134].
Re-TACE Planning and Scoring Systems
There is still an unmet need to recommend the treatment schedule for TACE and whether it should be performed at regular intervals or on demand based on tumour response.
The repetition of TACE procedures according to an aggressive schedule might induce liver failure in an unacceptable proportion of patients and as imaging techniques show high efficacy to detect residual viable tissue, it seems reasonable to perform a subsequent TACE session only when residual viable HCC is detected [34].
The decision whether treatment with TACE should be interrupted is complex. In recent years, various scoring systems have been proposed to identify patients who are poor candidates for repeat TACE treatment. The HAP and STATE scores [143, 144] aim to identify poor candidates before the first treatment session and the ART score aims to assess retreatment. The “six-and-twelve” score has been developed more recently to select best candidates for TACE [145]. These scores have been questioned by different groups, based on the fact that they don’t capture the established candidates to TACE according to guidelines or due to the lack of impact in clinical practice [146, 147].
Therefore, the decision on whether to re-treat patients with TACE should be based on the concept of “untreatable progression” [148]. Thus, TACE should not be repeated when substantial necrosis is not achieved after two rounds of treatment or when follow-up treatment fails to induce marked necrosis at sites that have progressed after an initial tumour response. Additionally, TACE should not be repeated in patients with tumour progression associated with a clinical profile that prevents re-treatment, e.g. development of liver failure. Definitions of untreatable progression may include major progression (extensive liver involvement, extrahepatic metastasis or vascular invasion) but also minor intrahepatic progression associated with impaired liver function and performance status [34].
Future Perspectives
New Drugs
In a recent worldwide survey regarding TACE for HCC, doxorubicin appeared as the most used cytotoxic agent (71.7% responders) especially in North America, Europe and Korea [6]. Pirarubicin was the most commonly used drug in China and epirubicin in Japan. It is important to note that most of these drugs are not approved by health authorities for locoregional treatment of HCC. Three different methods can be used to select the optimal drug for HCC TACE:
-
1.
Use of a drug that has shown a significant clinical efficacy when used intravenously. If this drug has high hepatic extraction ratio, this may be a good candidate for TACE. One trial conducted in 1975 [149] on 14 HCC patients treated by IV doxorubicin reported tumour response in 11/14, among whom three showed complete response. These results justified further use of doxorubicin for TACE of HCC. Unfortunately, the results of this trial have never been reproduced so far explaining why doxorubicin is not used for systemic treatment of HCC
-
2.
Conduct a randomised trial comparing drugs. Two randomised trials comparing doxorubicin to epirubicin did not show any difference in terms of efficacy [150, 151]. The only positive randomised trial so far has been reported in 365 patients by Shi et al., showing that a triple-drug (lobaplatin, epirubicin and mitomycin C) TACE regimen was associated with OS benefit as compared to single-drug (epirubicin) TACE [152].
-
3.
Select the appropriate drug for HCC TACE to conduct a cytotoxicity study. Such a study was conducted in 2011 to screen eleven drugs against three HCC cell lines [153] and reported that idarubicin was by far the most cytotoxic agent. Good safety profile and promising clinical efficacy has been reported either for idarubicin cTACE [154], DEM-TACE [155] or chemolipiodolisation [156]. However, no prospective randomised data are available so far.
Combination of TACE Plus Systemic Therapies
Randomised trials have evaluated the benefit of adding the following targeted therapies to TACE (either conventional or using drug-eluting microspheres): sorafenib (SPACE, TACE 2 and TACTICS trials), brivanib (BRISK-TA trial), and orantinib (ORIENTAL trial) [157]. Despite the high number of included patients (889 in the latter) in these trials, none of them has shown positive results in terms of OS improvement. Yet, there is a strong rationale for combining anti-angiogenic molecules with TACE, known to favour the release of pro-angiogenic factors (such as VEGF), which in turn, may cause tumour progression. Post-TACE serum VEGF levels have been linked to both response and survival [158]. Except the TACTICS trial [159] comparing TACE to sorafenib-TACE-sorafenib (interruption for 2 days before and after TACE) and showing a benefit in PFS (25.2 vs. 13.5 months; p = 0.006), all combination trials with tyrosine-kinase inhibitors or anti-angiogenics were all negative.
Immunotherapy has very recently become the new standard for the treatment of advanced HCC. The extensive research in this field has led to exploring the combination of various immune-checkpoint inhibitors, alone or in combination with TACE [157] durvalumab + bevacizumab (EMERALD-1 trial), nivolumab (TACE-3 trial), Lenvatinib+pembrolizumab (LEAP-012 trial), nivolumab + ipilimumab (CheckMate 74W trial). The results of these phase III randomised trials are pending and might define new standards in the future.
Abbreviations
- SOP:
-
Standards of practice
- c-TACE:
-
Conventional transarterial chemoembolisation
- DEM-TACE:
-
Drug-eluting microsphere transarterial chemoembolisation
- DSM-TACE:
-
Degradable starch microsphere transarterial chemoembolisation
- b-TACE:
-
Balloon-occluded transarterial chemoembolisation
- HCC:
-
Hepatocellular carcinoma
- ICC:
-
Intrahepatic cholangiocarcinoma
- m-CRC:
-
Metastatic colorectal cancer
- NET:
-
Neuroendocrine tumour
- MDCT:
-
Multidetector computed tomography
- MRI:
-
Magnetic resonance imaging
- TIPS:
-
Transjugular portosystemic shunt
- BCLC:
-
Barcelona Clinic Liver Cancer
- ECOG:
-
Eastern Cooperative Oncology Group
- AST:
-
Aspartate transaminase
- ALT:
-
Alanina transaminase
- γGT:
-
Gamma-glutamyltransferase
- AFP:
-
Alfa-fetoprotein
- CBCT:
-
Cone beam computed tomography
- TARE:
-
Transarterial radioembolisation
- Transarterial chemoembolisation :
-
Blockade of tumorous arterial flow through embolic material which carried chemotherapeutic drugs.
- Conventional TACE :
-
Performed with an emulsion of lipiodol (oil) and chemotherapeutic drugs, then followed by the administration of an embolic agent.
- Drug-eluting microsphere TACE :
-
Performed with permanent microspheres loaded with chemotherapeutic drugs.
- Degradable starch microsphere TACE :
-
Performed with a resorbable carrier mixed with chemotherapeutic drugs.
- Balloon-occluded microcatheter TACE :
-
Performed with a balloon microcatheter inflated prior embolisation in combination with either lipiodol or microspheres mixed with chemotherapeutic drugs.
References
Basile A, Carrafiello G, Ierardi AM, Tsetis D. Brountzos E Quality-improvement guidelines for hepatic transarterial chemoembolization. Cardiovasc Intervent Radiol. 2012;35(4):765–74.
Yamada R, Nakatsuka H, Nakamura K, et al. [Super-selective arterial embolization in unresectable hepatomas (author’s transl)] Nihon Igaku Hoshasen Gakkai zasshi. Nippon acta radiologica. 1979;39(5):540–3.
Guan Y-S, He Q, Wang M-Q. Transcatheter arterial chemoembolization: history for more than 30 years. ISRN Gastroenterol. 2012;2012:1–8.
Yamada R, Sato M, Kawabata M, Nakatsuka H, Nakamura K, Takashima S. Hepatic artery embolization in 120 patients with unresectable hepatoma. Radiology. 1983;148(2):397–401.
Craig P, Young S, Golzarian J. Current Trends in the Treatment of Hepatocellular Carcinoma with Transarterial Embolization: Variability in Technical Aspects. Cardiovasc Intervent Radiol. 2019;2(9):1322–8.
Young S, Craig P, Golzarian J. Current trends in the treatment of hepatocellular carcinoma with transarterial embolization: a cross-sectional survey of techniques. Eur Radiol. 2019;29(6):3287–95.
Sahara S, Kawai N, Sato M, et al. Prospective evaluation of transcatheter arterial chemoembolization (TACE) with multiple anti-cancer drugs (epirubicin, cisplatin, mitomycin c, 5-fluorouracil) compared with TACE with epirubicin for treatment of hepatocellular carcinoma. Cardiovasc Intervent Radiol. 2012;35(6):1363–71.
Hong K, Khwaja A, Liapi E, Torbenson MS, Georgiades CS, Geschwind JF. New intra-arterial drug delivery system for the treatment of liver cancer: preclinical assessment in a rabbit model of liver cancer. Clini cancer res Official J Am Assoc Cancer Res. 2006;12(8):2563–7.
Lammer J, Malagari K, Vogl T, et al. Prospective randomized study of doxorubicin-eluting-bead embolization in the treatment of hepatocellular carcinoma: results of the PRECISION V study. Cardiovasc Intervent Radiol. 2010;33(1):41–52.
Iezzi R, Pompili M, Rinninella E, et al. TACE with degradable starch microspheres (DSM-TACE) as second-line treatment in HCC patients dismissing or ineligible for sorafenib. Eur Radiol. 2019;29(3):1285–92.
Gross A, Albrecht T. Transarterial Chemoembolisation (TACE) with Degradable Starch Microspheres (DSM) and Anthracycline in Patients with Locally Extensive Hepatocellular Carcinoma (HCC): Safety and Efficacy. Cardiovasc Intervent Radiol. 2020;43(3):402–10.
Schicho A, Pereira PL, Haimerl M, et al. Transarterial chemoembolization (TACE) with degradable starch microspheres (DSM) in hepatocellular carcinoma (HCC): multi-center results on safety and efficacy. Oncotarget. 2017;8(42):72613–20.
Goerg F, Zimmermann M, Bruners P, Neumann U, Luedde T, Kuhl C. Chemoembolization with Degradable Starch Microspheres for Treatment of Patients with Primary or Recurrent Unresectable, Locally Advanced Intrahepatic Cholangiocarcinoma: A Pilot Study. Cardiovasc Intervent Radiol. 2019;42(12):1709–17.
Schicho A, Pereira PL, Michalik K, Beyer LP, Stroszczynski C, Wiggermann P. Safety and efficacy of transarterial chemoembolization with degradable starch microspheres (DSM-TACE) in the treatment of secondary liver malignancies. Onco Targets Ther. 2018;11:345–50.
Irie T, Kuramochi M, Takahashi N. Dense accumulation of lipiodol emulsion in hepatocellular carcinoma nodule during selective balloon-occluded transarterial chemoembolization: measurement of balloon-occluded arterial stump pressure. Cardiovasc Intervent Radiol. 2013;36(3):706–13.
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424.
Gaba RC, Lokken RP, Hickey RM, et al. Quality Improvement Guidelines for Transarterial Chemoembolization and Embolization of Hepatic Malignancy. J Vasc Interv Radiol. 2017;28(9):1210–23.
Riihimaki M, Hemminki A, Sundquist K, Sundquist J, Hemminki K. The epidemiology of metastases in neuroendocrine tumors. Int J Cancer. 2016;139(12):2679–86.
Mitchell DG, Bruix J, Sherman M, Sirlin CB. LI-RADS (Liver Imaging Reporting and Data System): Summary, discussion, and consensus of the LI-RADS Management Working Group and future directions. Hepatology. 2015;61(3):1056–65.
Di Tommaso L, Spadaccini M, Donadon M, et al. Role of liver biopsy in hepatocellular carcinoma. World J Gastroenterol. 2019;25(40):6041–52.
Lencioni R, Petruzzi P, Crocetti L. Chemoembolization of hepatocellular carcinoma. Semin Intervent Radiol. 2013;30(1):3–11.
Shin SW. The current practice of transarterial chemoembolization for the treatment of hepatocellular carcinoma. Korean J Radiol. 2009;10(5):425–34.
Schraml C, Kaufmann S, Rempp H, et al. Imaging of HCC-Current State of the Art. Diagnostics. 2015;5(4):513–45.
Golfieri R, Renzulli M, Mosconi C, et al. Hepatocellular carcinoma responding to superselective transarterial chemoembolization: an issue of nodule dimension? J Vasc Interv Radiol. 2013;24(4):509–17.
Miura JT, Rilling WS, White SB, et al. Safety and efficacy of transarterial chemoembolization in patients with transjugular intrahepatic portosystemic shunts. HPB. 2015;17(8):707–12.
Vogel A, Cervantes A, Chau I, et al. Hepatocellular carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29:238–55.
Van Cutsem E, Cervantes A, Adam R, et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann Oncol. 2016;27(8):1386–422.
de Baere T, Deschamps F, Tselikas L, et al. GEP-NETS update: Interventional radiology: role in the treatment of liver metastases from GEP-NETs. Eur J Endocrinol. 2015;172(4):R151-166.
Tangkijvanich P, Anukulkarnkusol N, Suwangool P, et al. Clinical characteristics and prognosis of hepatocellular carcinoma: analysis based on serum alpha-fetoprotein levels. J Clin Gastroenterol. 2000;31(4):302–8.
Arai T, Kobayashi A, Ohya A, et al. Assessment of treatment outcomes based on tumor marker trends in patients with recurrent hepatocellular carcinoma undergoing trans-catheter arterial chemo-embolization. Int J Clin Oncol. 2014;19(5):871–9.
Yu R, Tan Z, Xiang X, Dan Y, Deng G. Effectiveness of PIVKA-II in the detection of hepatocellular carcinoma based on real-world clinical data. BMC Cancer. 2017;17(1):608.
Michl M, Koch J, Laubender RP, et al. Tumor markers CEA and CA 19–9 correlate with radiological imaging in metastatic colorectal cancer patients receiving first-line chemotherapy. Tumour Biol. 2014;35(10):10121–7.
Pavel M, Öberg K, Falconi M, et al. Gastroenteropancreatic neuroendocrine neoplasms: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2020;31(7):844–60.
EASL Clinical Practice Guidelines. Management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236.
Johnson PJ, Berhane S, Kagebayashi C, et al. Assessment of liver function in patients with hepatocellular carcinoma: a new evidence-based approach-the ALBI grade. J Clin Oncol. 2015;33(6):550–8.
Abdel-Rahman O. Prognostic Value of Baseline ALBI Score Among Patients With Colorectal Liver Metastases: A Pooled Analysis of Two Randomized Trials. Clin Colorectal Cancer. 2019;18(1):e61–8.
Rebonato A, Graziosi L, Maiettini D, et al. Inflammatory Markers as Prognostic Factors of Survival in Patients Affected by Hepatocellular Carcinoma Undergoing Transarterial Chemoembolization. Gastroenterol Res Pract. 2017;2017:4164130–4164130.
Lee MJ, Fanelli F, Haage P, Hausegger K, Van Lienden KP. Patient safety in interventional radiology: a CIRSE IR checklist. Cardiovasc Intervent Radiol. 2012;35(2):244–6.
Ogasawara S, Chiba T, Ooka Y, et al. A randomized placebo-controlled trial of prophylactic dexamethasone for transcatheter arterial chemoembolization. Hepatology. 2018;67(2):575–85.
Iezzi R, Kovacs A, Prenen H, Chevallier P, Pereira PL. Transarterial chemoembolisation of colorectal liver metastases with irinotecan-loaded beads: What every interventional radiologist should know. Eur J Radiol Open. 2020;7:100236.
Wang TC, Zhang ZS, Xiao YD. Determination of Risk Factors for Pain After Transarterial Chemoembolization with Drug-Eluting Beads for Hepatocellular Carcinoma. J Pain Res. 2020;13:649–56.
Benzakoun J, Ronot M, Lagadec M, et al. Risks factors for severe pain after selective liver transarterial chemoembolization. Liver Int. 2017;37(4):583–91.
Romagnoli S, Fanelli F, et al. CIRSE Standards of Practice on Analgesia and Sedation for Interventional Radiology in Adults. Cardiovasc Intervent Radiol. 2020;43(9):1251–60.
Chehab MA, Thakor AS, Tulin-Silver S, et al. Adult and Pediatric Antibiotic Prophylaxis during Vascular and IR Procedures: A Society of Interventional Radiology Practice Parameter Update Endorsed by the Cardiovascular and Interventional Radiological Society of Europe and the Canadian Association for Interventional Radiology. J Vasc Interv Radiol. 2018;29(11):1483-1501.e1482.
Patel IJ, Davidson JC, Nikolic B, et al. Consensus guidelines for periprocedural management of coagulation status and hemostasis risk in percutaneous image-guided interventions. J Vasc Interv Radiol. 2012;23(6):727–36.
Hadi M, Walker C, Desborough M, et al. CIRSE Standards of Practice on Peri-operative Anticoagulation Management During Interventional Radiology Procedures. Cardiovasc Intervent Radiol. 2021;44(4):523–36.
Lucatelli P, Corona M, Argiro R, et al. Impact of 3D Rotational Angiography on Liver Embolization Procedures: Review of Technique and Applications. Cardiovasc Intervent Radiol. 2015;38(3):523–35.
Pung L, Ahmad M, Mueller K, et al. The Role of Cone-Beam CT in Transcatheter Arterial Chemoembolization for Hepatocellular Carcinoma: A Systematic Review and Meta-analysis. J Vasc Interv Radiol. 2017;28(3):334–41.
Lucatelli P, De Rubeis G, Ginnani Corradini L, et al. Intra-procedural dual phase cone beam computed tomography has a better diagnostic accuracy over pre-procedural MRI and MDCT in detection and characterization of HCC in cirrhotic patients undergoing TACE procedure. Eur J Radiol. 2020;124:108806.
Lucatelli P, Argiro R, Bascetta S, et al. Single injection dual phase CBCT technique ameliorates results of trans-arterial chemoembolization for hepatocellular cancer. Transl Gastroenterol Hepatol. 2017;2:83.
Schernthaner RE, Haroun RR, Duran R, et al. Improved Visibility of Metastatic Disease in the Liver During Intra-Arterial Therapy Using Delayed Arterial Phase Cone-Beam CT. Cardiovasc Intervent Radiol. 2016;39(10):1429–37.
Kan Z, Ivancev K, Hägerstrand I, Chuang VP, Lunderquist A. In vivo microscopy of the liver after injection of Lipiodol into the hepatic artery and portal vein in the rat. Acta Radiol. 1989;30(4):419–25.
Tanaka T, Arai Y, Inaba Y, et al. Current role of hybrid CT/angiography system compared with C-arm cone beam CT for interventional oncology. Br J Radiol. 2014;87(1041):20140126.
Toyoda H, Kumada T, Sone Y. Impact of a Unified CT Angiography System on Outcome of Patients with Hepatocellular Carcinoma. Am J Roentgenol. 2009;192(3):766–74.
de Baere T, Dufaux J, Roche A, et al. Circulatory alterations induced by intra-arterial injection of iodized oil and emulsions of iodized oil and doxorubicin: experimental study. Radiology. 1995;194(1):165–70.
Takayasu K, Shima Y, Muramatsu Y, et al. Hepatocellular carcinoma: treatment with intraarterial iodized oil with and without chemotherapeutic agents. Radiology. 1987;163(2):345–51.
Idée JM, Guiu B. Use of Lipiodol as a drug-delivery system for transcatheter arterial chemoembolization of hepatocellular carcinoma: a review. Crit Rev Oncol Hematol. 2013;88(3):530–49.
Deschamps F, Farouil G, Gonzalez W, et al. Stabilization Improves Theranostic Properties of Lipiodol(®)-Based Emulsion During Liver Trans-arterial Chemo-embolization in a VX2 Rabbit Model. Cardiovasc Intervent Radiol. 2017;40(6):907–13.
de Baere T, Zhang X, Aubert B, et al. Quantification of tumor uptake of iodized oils and emulsions of iodized oils: experimental study. Radiology. 1996;201(3):731–5.
Kan Z, Wright K, Wallace S. Ethiodized oil emulsions in hepatic microcirculation: in vivo microscopy in animal models. Acad Radiol. 1997;4(4):275–82.
de Baere T, Arai Y, Lencioni R, et al. Treatment of Liver Tumors with Lipiodol TACE: Technical Recommendations from Experts Opinion. Cardiovasc Intervent Radiol. 2016;39(3):334–43.
Kudo T, Monzawa S, Sugimura K. Evaluation of durability of three-way stopcocks to Lipiodol in making an emulsion for transcatheter arterial chemo-embolization. Medical Journal of Kobe University. 2004;64:47–52.
Boulin M, Schmitt A, Delhom E, et al. Improved stability of lipiodol-drug emulsion for transarterial chemoembolisation of hepatocellular carcinoma results in improved pharmacokinetic profile: Proof of concept using idarubicin. Eur Radiol. 2016;26(2):601–9.
Deschamps F, Moine L, Isoardo T, et al. Parameters for Stable Water-in-Oil Lipiodol Emulsion for Liver Trans-Arterial Chemo-Embolization. Cardiovasc Intervent Radiol. 2017;40(12):1927–32.
Nakamura H, Hashimoto T, Oi H, Sawada S. Transcatheter oily chemoembolization of hepatocellular carcinoma. Radiology. 1989;170(3 Pt 1):783–6.
Tzeng WS, Wu RH, Chang SC, et al. Ionic versus nonionic contrast media solvents used with an epirubicin-based agent for transarterial chemoembolization of hepatocellular carcinoma. J Vasc Interv Radiol. 2008;19(3):342–50.
Gaba RC, Baumgarten S, Omene BO, et al. Ethiodized oil uptake does not predict doxorubicin drug delivery after chemoembolization in VX2 liver tumors. J Vasc Interv Radiol. 2012;23(2):265–73.
Chung JW, Park JH, Im JG, Han JK, Han MC. Pulmonary oil embolism after transcatheter oily chemoembolization of hepatocellular carcinoma. Radiology. 1993;187(3):689–93.
Louail B, Sapoval M, Bonneau M, Wasseff M, Senechal Q, Gaux JC. A new porcine sponge material for temporary embolization: an experimental short-term pilot study in swine. Cardiovasc Intervent Radiol. 2006;29(5):826–31.
Katsumori T, Kasahara T. The size of gelatin sponge particles: differences with preparation method. Cardiovasc Intervent Radiol. 2006;29(6):1077–83.
Laurent A, Wassef M, Chapot R, et al. Partition of calibrated tris-acryl gelatin microspheres in the arterial vasculature of embolized nasopharyngeal angiofibromas and paragangliomas. J Vasc Interv Radiol. 2005;16(4):507–13.
Lee KH, Liapi E, Vossen JA, et al. Distribution of iron oxide-containing Embosphere particles after transcatheter arterial embolization in an animal model of liver cancer: evaluation with MR imaging and implication for therapy. J Vasc Interv Radiol. 2008;19(10):1490–6.
Bonomo G, Pedicini V, Monfardini L, et al. Bland embolization in patients with unresectable hepatocellular carcinoma using precise, tightly size-calibrated, anti-inflammatory microparticles: first clinical experience and one-year follow-up. Cardiovasc Intervent Radiol. 2010;33(3):552–9.
Miyayama S, Matsui O, Yamashiro M, et al. Ultraselective transcatheter arterial chemoembolization with a 2-f tip microcatheter for small hepatocellular carcinomas: relationship between local tumor recurrence and visualization of the portal vein with iodized oil. J Vasc Interv Radiol. 2007;18(3):365–76.
de Baere T, Plotkin S, Yu R, Sutter A, Wu Y, Cruise GM. An In Vitro Evaluation of Four Types of Drug-Eluting Microspheres Loaded with Doxorubicin. J Vasc Interv Radiol. 2016;27(9):1425–31.
Varela M, Real MI, Burrel M, et al. Chemoembolization of hepatocellular carcinoma with drug eluting beads: efficacy and doxorubicin pharmacokinetics. J Hepatol. 2007;46(3):474–81.
Volkova M, Russell R 3rd. Anthracycline cardiotoxicity: prevalence, pathogenesis and treatment. Curr Cardiol Rev. 2011;7(4):214–20.
McGowan JV, Chung R, Maulik A, Piotrowska I, Walker JM, Yellon DM. Anthracycline Chemotherapy and Cardiotoxicity. Cardiovasc Drugs Ther. 2017;31(1):63–75.
Veloso Gomes F, Oliveira JA, Correia MT, et al. Chemoembolization of Hepatocellular Carcinoma with Drug-Eluting Polyethylene Glycol Embolic Agents: Single-Center Retrospective Analysis in 302 Patients. J Vasc Interv Radiol. 2018;29(6):841–9.
Aliberti C, Carandina R, Lonardi S, et al. Transarterial Chemoembolization with Small Drug-Eluting Beads in Patients with Hepatocellular Carcinoma: Experience from a Cohort of 421 Patients at an Italian Center. J Vasc Interv Radiol. 2017;28(11):1495–502.
Aal AKA, Moawad S, Lune PV, et al. Survival Outcomes of Very Small Drug-Eluting Beads Used in Chemoembolization of Unresectable Hepatocellular Carcinoma. J Vasc Interv Radiol. 2019;30(9):1325-1334.e1322.
Richter G, Radeleff B, Stroszczynski C, et al. Safety and Feasibility of Chemoembolization with Doxorubicin-Loaded Small Calibrated Microspheres in Patients with Hepatocellular Carcinoma: Results of the MIRACLE I Prospective Multicenter Study. Cardiovasc Intervent Radiol. 2018;41(4):587–93.
Balli H, Aksungur E, Khalatai B, Aikimbaev K. Super-Selective Transarterial Chemoembolization with Doxorubicin-Loaded Drug-Eluting Beads Sized Below and Above 100 Microns in Hepatocellular Carcinoma: A Comparative Study. J Belg Soc Radiol. 2019;103(1):47.
Delicque J, Guiu B, Boulin M, Schwanz H, Piron L, Cassinotto C. Liver chemoembolization of hepatocellular carcinoma using TANDEM((R)) microspheres. Future Oncol. 2018;14(26):2761–72.
Greco G, Cascella T, Facciorusso A, et al. Transarterial chemoembolization using 40 µm drug eluting beads for hepatocellular carcinoma. World J Radiol. 2017;9(5):245–52.
Malagari K, Pomoni M, Moschouris H, et al. Chemoembolization of hepatocellular carcinoma with HepaSphere 30–60 μm Safety and efficacy study. Cardiovasc Intervent Radiol. 2014;37(1):165–75.
Deipolyi AR, Oklu R, Al-Ansari S, Zhu AX, Goyal L, Ganguli S. Safety and efficacy of 70–150 mum and 100–300 mum drug-eluting bead transarterial chemoembolization for hepatocellular carcinoma. J Vasc Interv Radiol. 2015;26(4):516–22.
Lucatelli P, Argirò R, De Rubeis G, et al. Polyethylene Glycol Epirubicin-Loaded Transcatheter Arterial Chemoembolization Procedures Utilizing a Combined Approach with 100 and 200 μm Microspheres: A Promising Alternative to Current Standards. J Vasc Interv Radiol. 2019;30(3):305–13.
Lencioni R, de Baere T, Burrel M, et al. Transcatheter treatment of hepatocellular carcinoma with Doxorubicin-loaded DC Bead (DEBDOX): technical recommendations. Cardiovasc Intervent Radiol. 2012;35(5):980–5.
Schernthaner RE, Lin M, Duran R, Chapiro J, Wang Z, Geschwind JF. Delayed-Phase Cone-Beam CT Improves Detectability of Intrahepatic Cholangiocarcinoma During Conventional Transarterial Chemoembolization. Cardiovasc Intervent Radiol. 2015;38(4):929–36.
Akinwande OK, Philips P, Duras P, Pluntke S, Scoggins C, Martin RC. Small versus large-sized drug-eluting beads (DEBIRI) for the treatment of hepatic colorectal metastases: a propensity score matching analysis. Cardiovasc Intervent Radiol. 2015;38(2):361–71.
Yamasaki T, Hamabe S, Saeki I, et al. A novel transcatheter arterial infusion chemotherapy using iodized oil and degradable starch microspheres for hepatocellular carcinoma: a prospective randomized trial. J Gastroenterol. 2011;46(3):359–66.
Lucatelli P, De Rubeis G, Basilico F, et al. Sequential dual-phase cone-beam CT is able to intra-procedurally predict the one-month treatment outcome of multi-focal HCC, in course of degradable starch microsphere TACE. Radiol Med (Torino). 2019;124(12):1212–9.
Aramburu J, Anton R, Rivas A, et al. Numerical zero-dimensional hepatic artery hemodynamics model for balloon-occluded transarterial chemoembolization. Int J Numer Method Biomed Eng. 2018;34(7):e2983.
Lucatelli P, Corradini LG, De Rubeis G, et al. Balloon-Occluded Transcatheter Arterial Chemoembolization (b-TACE) for Hepatocellular Carcinoma Performed with Polyethylene-Glycol Epirubicin-Loaded Drug-Eluting Embolics: Safety and Preliminary Results. Cardiovasc Intervent Radiol. 2019;42(6):853–62.
Matsumoto T, Endo J, Hashida K, et al. Balloon-occluded transarterial chemoembolization using a 1.8-French tip coaxial microballoon catheter for hepatocellular carcinoma: technical and safety considerations. Minim Invasive Ther Allied Technol. 2015;24(2):94–100.
Reicher J, Mafeld S, Priona G, et al. Early Experience of Trans-arterial Chemo-Embolisation for Hepatocellular Carcinoma with a Novel Radiopaque Bead. Cardiovasc Intervent Radiol. 2019;42(11):1563–70.
Aliberti C, Carandina R, Sarti D, et al. Transarterial chemoembolization with DC Bead LUMITM radiopaque beads for primary liver cancer treatment: preliminary experience. Future Oncol. 2017;13(25):2243–52.
Moschouris H, Malagari K, Dimakis A, Kiakidis T, Anagnostopoulou A. Transarterial Chemoembolization of HCC with Radiopaque Microspheres: Evaluation with Computed Tomography and the Complementary Role of Contrast-Enhanced Ultrasonography. Cardiovasc Intervent Radiol. 2020;43(7):1075–83.
Hagan A, Caine M, Press C, et al. Predicting pharmacokinetic behaviour of drug release from drug-eluting embolization beads using in vitro elution methods. Eur J Pharm Sci. 2019;136:104943.
Tacher V, Radaelli A, Lin M, Geschwind J-F. How I Do It: Cone-Beam CT during Transarterial Chemoembolization for Liver Cancer. Radiology. 2015;274(2):320–34.
Llovet JM, Brú C, Bruix J. Prognosis of hepatocellular carcinoma: the BCLC staging classification. Semin Liver Dis. 1999;19(3):329–38.
Forner A, Reig ME, Rodriguez de Lope C, Bruix J. Current Strategy for Staging and Treatment The BCLC Update and Future Prospects. Seminars in liver disease. 2010;30(1):061–074.
Lo CM, Ngan H, Tso WK, et al. Randomized controlled trial of transarterial lipiodol chemoembolization for unresectable hepatocellular carcinoma. Hepatology. 2002;35(5):1164–71.
Llovet JM, Real MI, Montaña X, et al. Arterial embolisation or chemoembolisation versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: a randomised controlled trial. Lancet. 2002;359(9319):1734–9.
Llovet JM, Bruix J. Systematic review of randomized trials for unresectable hepatocellular carcinoma: Chemoembolization improves survival. Hepatology. 2003;37(2):429–42.
Cammà C, Schepis F, Orlando A, et al. Transarterial chemoembolization for unresectable hepatocellular carcinoma: meta-analysis of randomized controlled trials. Radiology. 2002;224(1):47–54.
Golfieri R, Giampalma E, Renzulli M, et al. Randomised controlled trial of doxorubicin-eluting beads vs conventional chemoembolisation for hepatocellular carcinoma. Br J Cancer. 2014;111(2):255–64.
Facciorusso A, Di Maso M, Muscatiello N. Drug-eluting beads versus conventional chemoembolization for the treatment of unresectable hepatocellular carcinoma: A meta-analysis. Digestive Liver Dis. 2016;48(6):571–7.
Yang B, Liang J, Qu Z, Yang F, Liao Z, Gou H. Transarterial strategies for the treatment of unresectable hepatocellular carcinoma: A systematic review. PLoS ONE. 2020;15(2):e0227475.
Auer TA, Jonczyk M, Collettini F, et al. Trans-arterial chemoembolization with degradable starch microspheres (DSM-TACE) versus selective internal radiation therapy (SIRT) in multifocal hepatocellular carcinoma. Acta Radiol. 2020;62(3):313–21.
Ogawa M, Takayasu K, Hirayama M, et al. Efficacy of a microballoon catheter in transarterial chemoembolization of hepatocellular carcinoma using miriplatin, a lipophilic anticancer drug: Short-term results. Hepatol Res official J Japan Soc Hepatol. 2016;46(3):E60-69.
Irie T, Kuramochi M, Kamoshida T, Takahashi N. Selective balloon-occluded transarterial chemoembolization for patients with one or two hepatocellular carcinoma nodules: Retrospective comparison with conventional super-selective TACE. Hepatol Res official J Japan Soc Hepatol. 2016;46(2):209–14.
Maruyama M, Yoshizako T, Nakamura T, Nakamura M, Yoshida R, Kitagaki H. Initial Experience with Balloon-Occluded Trans-catheter Arterial Chemoembolization (B-TACE) for Hepatocellular Carcinoma. Cardiovasc Intervent Radiol. 2016;39(3):359–66.
Goldman DT, Singh M, Patel RS, et al. Balloon-Occluded Transarterial Chemoembolization for the Treatment of Hepatocellular Carcinoma: A Single-Center US Preliminary Experience. J Vasc Interv Radiol. 2019;30(3):342–6.
Golfieri R, Bezzi M, Verset G, et al. Retrospective European Multicentric Evaluation of Selective Transarterial Chemoembolisation with and without Balloon-Occlusion in Patients with Hepatocellular Carcinoma: A Propensity Score Matched Analysis. Cardiovasc Intervent Radiol. 2021;44(7):1048–59.
Vogl TJ, Wissniowski TT, Naguib NN, et al. Activation of tumor-specific T lymphocytes after laser-induced thermotherapy in patients with colorectal liver metastases. Cancer Immunol Immunother. 2009;58(10):1557–63.
Albert M, Kiefer MV, Sun W, et al. Chemoembolization of colorectal liver metastases with cisplatin, doxorubicin, mitomycin C, ethiodol, and polyvinyl alcohol. Cancer. 2011;117(2):343–52.
Martin RC, Joshi J, Robbins K, et al. Hepatic intra-arterial injection of drug-eluting bead, irinotecan (DEBIRI) in unresectable colorectal liver metastases refractory to systemic chemotherapy: results of multi-institutional study. Ann Surg Oncol. 2011;18(1):192–8.
Fiorentini G, Aliberti C, Tilli M, et al. Intra-arterial infusion of irinotecan-loaded drug-eluting beads (DEBIRI) versus intravenous therapy (FOLFIRI) for hepatic metastases from colorectal cancer: final results of a phase III study. Anticancer Res. 2012;32(4):1387–95.
Iezzi R, Marsico VA, Guerra A, et al. Trans-Arterial Chemoembolization with Irinotecan-Loaded Drug-Eluting Beads (DEBIRI) and Capecitabine in Refractory Liver Prevalent Colorectal Metastases: A Phase II Single-Center Study. Cardiovasc Intervent Radiol. 2015;38(6):1523–31.
Levy J, Zuckerman J, Garfinkle R, et al. Intra-arterial therapies for unresectable and chemorefractory colorectal cancer liver metastases: a systematic review and meta-analysis. HPB. 2018;20(10):905–15.
Pereira PL, et al. The CIREL Cohort: A Prospective Controlled Registry Studying the Real-Life Use of Irinotecan-Loaded Chemoembolisation in Colorectal Cancer Liver Metastases: Interim Analysis. CardioVasc Interv Radiol. 2020;44:50–62.
Bridgewater J, Galle PR, Khan SA, Llovet JM, Park JW, Patel T, Pawlik TM, Gores GJ. Guidelines for the diagnosis and management of intrahepatic cholangiocarcinoma. J Hepatol. 2014;60(6):1268–89.
Hyder O, Marsh JW, Salem R, et al. Intra-arterial therapy for advanced intrahepatic cholangiocarcinoma: a multi-institutional analysis. Ann Surg Oncol. 2013;20(12):3779–86.
Filippi L, Schillaci O, Cianni R, Bagni O. Yttrium-90 resin microspheres and their use in the treatment of intrahepatic cholangiocarcinoma. Future Oncol. 2018;14(9):809–18.
Labib PL, Davidson BR, Sharma RA, Pereira SP. Locoregional therapies in cholangiocarcinoma. Hepat Oncol. 2017;4(4):99–109.
Schicho A, Pereira PL, Pützler M, et al. Degradable Starch Microspheres Transcatheter Arterial Chemoembolization (DSM-TACE) in Intrahepatic Cholangiocellular Carcinoma (ICC): Results from a National Multi-Center Study on Safety and Efficacy. Med Sci Monit. 2017;23:796–800.
Do Minh D, Chapiro J, Gorodetski B, et al. Intra-arterial therapy of neuroendocrine tumour liver metastases: comparing conventional TACE, drug-eluting beads TACE and yttrium-90 radioembolisation as treatment options using a propensity score analysis model. Eur Radiol. 2017;27(12):4995–5005.
Da Dong X, Carr BI. Hepatic artery chemoembolization for the treatment of liver metastases from neuroendocrine tumors: a long-term follow-up in 123 patients. Med Oncol. 2011;28(1):286–90.
Gaba RC, Lewandowski RJ, Hickey R, et al. Transcatheter Therapy for Hepatic Malignancy: Standardization of Terminology and Reporting Criteria. J Vasc Interv Radiol. 2016;27(4):457–73.
Filippiadis DK, Binkert C, Pellerin O, Hoffmann RT, Krajina A, Pereira PL. Cirse Quality Assurance Document and Standards for Classification of Complications: The Cirse Classification System. Cardiovasc Intervent Radiol. 2017;40(8):1141–6.
Vera R, Aparicio J, Carballo F, et al. Recommendations for follow-up of colorectal cancer survivors. Clin Transl Oncol. 2019;21(10):1302–11.
Singh S, Moody L, Chan DL, et al. Follow-up Recommendations for Completely Resected Gastroenteropancreatic Neuroendocrine Tumors. JAMA Oncol. 2018;4(11):1597–604.
Rahnemai-Azar AA, Pandey P, Kamel I, Pawlik TM. Monitoring outcomes in intrahepatic cholangiocarcinoma patients following hepatic resection. Hepat Oncol. 2016;3(4):223–39.
Takayasu K, Arii S, Ikai I, et al. Overall survival after transarterial lipiodol infusion chemotherapy with or without embolization for unresectable hepatocellular carcinoma: propensity score analysis. AJR Am J Roentgenol. 2010;194(3):830–7.
Kim DY, Ryu HJ, Choi JY, et al. Radiological response predicts survival following transarterial chemoembolisation in patients with unresectable hepatocellular carcinoma. Aliment Pharmacol Ther. 2012;35(11):1343–50.
Arora A, Kumar A. Treatment Response Evaluation and Follow-up in Hepatocellular Carcinoma. J Clin Exp Hepatol. 2014;4(Suppl 3):S126-129.
Liu W, Zheng Y, Zou R, et al. Impact of follow-up interval on patients with hepatocellular carcinoma after curative ablation. BMC Cancer. 2018;18(1):1186.
Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010;30(1):52–60.
Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 11). Eur J Cancer. 2009;45(2):228–47.
Lucidarme O, Wagner M, Gillard P, et al. RECIST and CHOI criteria in the evaluation of tumor response in patients with metastatic colorectal cancer treated with regorafenib, a prospective multicenter study. Cancer Imaging. 2019;19(1):85.
Kadalayil L, Benini R, Pallan L, et al. A simple prognostic scoring system for patients receiving transarterial embolisation for hepatocellular cancer. Ann Oncol. 2013;24(10):2565–70.
Hucke F, Pinter M, Graziadei I, et al. How to STATE suitability and START transarterial chemoembolization in patients with intermediate stage hepatocellular carcinoma. J Hepatol. 2014;61(6):1287–96.
Wang Q, Xia D, Bai W, et al. Development of a prognostic score for recommended TACE candidates with hepatocellular carcinoma: A multicentre observational study. J Hepatol. 2019;70(5):893–903.
Terzi E, Terenzi L, Venerandi L, et al. The ART score is not effective to select patients for transarterial chemoembolization retreatment in an Italian series. Dig Dis. 2014;32(6):711–6.
Kudo M, Arizumi T, Ueshima K. Assessment for retreatment (ART) score for repeated transarterial chemoembolization in patients with hepatocellular carcinoma. Hepatology. 2014;59(6):2424–5.
Forner A, Gilabert M, Bruix J, Raoul JL. Treatment of intermediate-stage hepatocellular carcinoma. Nature reviews Clin Oncol. 2014;11(9):525–35.
Olweny CL, Toya T, Katongole-Mbidde E, Mugerwa J, Kyalwazi SK, Cohen H. Treatment of hepatocellular carcinoma with adriamycin. Preliminary commun Cancer. 1975;36(4):1250–7.
Kawai S, Tani M, Okamura J, et al. Prospective and randomized trial of lipiodol-transcatheter arterial chemoembolization for treatment of hepatocellular carcinoma: a comparison of epirubicin and doxorubicin (second cooperative study). The Cooperative Study Group for Liver Cancer Treatment of Japan. Semin Oncol. 1997;24:S6-38-s36-45.
Watanabe S, Nishioka M, Ohta Y, Ogawa N, Ito S, Yamamoto Y. Prospective and randomized controlled study of chemoembolization therapy in patients with advanced hepatocellular carcinoma Cooperative Study Group for Liver Cancer Treatment in Shikoku area. Cancer Chemother Pharmacol. 1994;33:S93-96.
Shi M, Lu LG, Fang WQ, et al. Roles played by chemolipiodolization and embolization in chemoembolization for hepatocellular carcinoma: single-blind, randomized trial. J Natl Cancer Inst. 2013;105(1):59–68.
Boulin M, Hillon P, Cercueil JP, et al. Idarubicin-loaded beads for chemoembolisation of hepatocellular carcinoma: results of the IDASPHERE phase I trial. Aliment Pharmacol Ther. 2014;39(11):1301–13.
Favelier S, Boulin M, Hamza S, et al. Lipiodol trans-arterial chemoembolization of hepatocellular carcinoma with idarubicin: first experience. Cardiovasc Intervent Radiol. 2013;36(4):1039–46.
Guiu B, Chevallier P, Assenat E, et al. Idarubicin-loaded Beads for Chemoembolization of Hepatocellular Carcinoma: The IDASPHERE II Single-Arm Phase II Trial. Radiology. 2019;291(3):801–8.
Guiu B, Jouve JL, Schmitt A, et al. Intra-arterial idarubicin_lipiodol without embolisation in hepatocellular carcinoma: The LIDA-B phase I trial. J Hepatol. 2018;68(6):1163–71.
Llovet JM, Kelley RK, Villanueva A, et al. Hepatocellular carcinoma Nat Rev Dis Primers. 2021;7(1):6.
Sergio A, Cristofori C, Cardin R, et al. Transcatheter arterial chemoembolization (TACE) in hepatocellular carcinoma (HCC): the role of angiogenesis and invasiveness. Am J Gastroenterol. 2008;103(4):914–21.
Kudo M, Ueshima K, Ikeda M, et al. Randomised, multicentre prospective trial of transarterial chemoembolisation (TACE) plus sorafenib as compared with TACE alone in patients with hepatocellular carcinoma: TACTICS trial. Gut. 2020;69(8):1492.
Sakamoto I, Aso N, Nagaoki K, et al. Complications associated with transcatheter arterial embolization for hepatic tumors. Radiographics. 1998;18(3):605–19.
Funding
This study was not supported by any funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Marta Burrel has been a paid speaker for BTG, Guerbet and Terumo. Boris Guiu has recieved study funding from Guerbet, Boston Scientific and Terumo. He has also acted as a consultant for Boston Scientific and Terumo. All other authors declare they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Lucatelli, P., Burrel, M., Guiu, B. et al. CIRSE Standards of Practice on Hepatic Transarterial Chemoembolisation. Cardiovasc Intervent Radiol 44, 1851–1867 (2021). https://doi.org/10.1007/s00270-021-02968-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-021-02968-1