
Abstract
The chapter explores the colourful world of salivary gland tumours with extensive illustrations and a very detailed index.
It covers the full range of salivary disease including normal anatomy and histology, non-neoplastic diseases, benign and malignant primary salivary gland tumours, lymphoid disorders and metastases.
Each entity includes aetiology, definition, pathogenesis, microscopy with immunohistochemistry, special staining, molecular genetics and differential diagnosis.
Chapter 5 is recommended for use in academic settings and also in routine practice as it is based on the clinical work of all the authors, all of whom have extensive experience.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
5.1 Introduction
5.1.1 Normal Salivary Glands
The salivary glands include paired major glands (parotid, submandibular and sublingual) and thousands of minor glands throughout the upper aerodigestive tract.
Structurally the salivary glands are made up of three components. Firstly, the peripheral acinus with luminal, saliva-producing acinar cells and abluminal myoepithelial cells. Secondly, the short intercalated duct with luminal cuboidal intercalated duct cells and abluminal myoepithelial cells. Thirdly, the long striated and excretory ducts, both with luminal oxyphilic cells and inconspicuous abluminal basal cells. These basal cells, stained by cytokeratin subtypes 14 and 5/6, as well as p63, comprise an important pluripotent reserve cell pool for cellular regeneration, for different types of reactive metaplasia and possibly also for the complex tumorigenesis of salivary glands [1–3].
Myoepithelial cells have contractile properties that assist in the secretion of saliva. Similar cells are found in the breast and in the tracheobronchial and sweat glands. They are plentiful in the acini and intercalated ducts, but are largely absent from striated ducts. They are thin and spindle shaped and situated between the basement membrane and epithelial cells, and ultrastructurally they possess long cytoplasmic processes. They display features of both smooth muscle and epithelium. Accordingly, immunohistochemistry shows strong staining with alpha smooth muscle actin (αSMA), calponin, smooth muscle myosin heavy chain (SMMHC) [4], h-caldesmon [5], S-100 protein [6], as well as with some cytokeratins (e.g. subtype 14) and p63 [2, 3]. Scattered nests of sebaceous cells can be seen in normal parotid and minor salivary glands [3, 7].
The acinar component in the parotid glands consists predominantly of serous cells, whilst in the submandibular and minor glands, it comprises a mixture of serous and mucous cells and in the sublingual glands purely mucous cells. Serial sectioning has shown an average of 20 lymph nodes within each parotid, and they may be affected by inflammatory processes and neoplasms, both primary and metastatic [8]. It may be difficult, especially in small biopsies, to distinguish lesions of intraparotid lymph nodes from lymphatic tissue in inflammatory lesions (i.e. lymphoepithelial sialadenitis) or from reactive tumor-associated lymphatic tissue [9, 10].
5.1.2 Developmental Disorders
Agenesis, aplasia, hypoplasia and atresia of glands or of the main ducts are all extremely rare. In contrast, parenchymal inclusions in intraparotid lymph nodes are very common [1], and epithelial tumors may develop from them [11]. Extranodal heterotopia is rare and can be subdivided into high (involvement of the ear, pituitary, mandible, etc.) or low forms (lower neck, thyroid). Accessory parotid glands comprising salivary tissue separate from the main gland, adjacent to Stensen’s duct, are found in 20 % of people.
5.2 Obstructive Disorders
5.2.1 Mucus Escape Reaction (Extravasation Mucocoele/Ranula)
Definition
Pooling of saliva in a cavity not lined by epithelium.
Epidemiology
Most patients are under 30 years of age, and the minor salivary glands (especially of the lower lip) are most often affected.
Etiology and pathogenesis
The relative incidence in lower lip is 65 %, buccal mucosa 10 %, palate 4 %, parotid 0.6 % and submandibular and lingual glands 1.2 %. The pathogenesis is in most cases traumatic severance of a duct (e.g. from biting), leading to mucus pooling.
Clinical aspects
It presents in the lip as a raised, often blue, dome-shaped swelling of the mucosa usually 2–10 mm in diameter. Cases developing from the sublingual gland in the floor of mouth where it is known as ranula (Latin for ‘small frog’) are usually significantly larger.
Macroscopy
Pseudocyst with a white wall containing mucus-like material.
Microscopy
Shows a well-defined mucin-filled cavity lined not by epithelium but by granulation tissue and macrophages (Fig. 5.1).

Extravasation mucocoele (mucous escape reaction): mucin-filled cavity lined with granulation tissue and macrophages
Differential diagnosis
The most important differential diagnosis in cases with numerous clear cell macrophages is with low-grade mucoepidermoid carcinoma. The latter includes squamous, intermediate (some of which have clear cytoplasm) and mucinous goblet cells. The differential diagnosis may be difficult in a small incisional biopsy, but immunohistochemistry separates CD68-positive macrophages from cytokeratin-positive tumor cells.
Treatment and prognosis
Treatment consists of complete surgical excision. Recurrences can occur for incompletely excised lesions.
5.2.2 Chronic Sclerosing Sialadenitis of the Submandibular Gland (Küttner Tumor)
Definition
A tumor-like condition affecting either one or both submandibular glands.
Epidemiology
It can occur at any age (mean 45 years) and affects both sexes.
Etiology and pathogenesis
It is a consequence of ductal obstruction resulting from several different causes. In up to 80 % of cases, large calculi in the excretory ducts are generally considered to be responsible, with a lower percentage due to small intraparenchymal microliths [12, 13]. In addition, IgG4-related sclerosing disease is a factor in rare cases (see below).
Clinical aspect
Patients present with recurrent or persistent unilateral submandibular pain and or swelling frequently associated with eating.
Macroscopy
The submandibular gland is replaced by white and firm tissue resembling a tumor.
Microscopy
The histopathological picture of chronic sclerosing sialadenitis varies depending on the stage of the process; it evolves from just scattered lymphoplasmacytic aggregates to severe changes of acinar atrophy and heavy chronic inflammation with germinal centre formation, leading eventually to an end stage of destruction of the lobular architecture and scarring. The inflammation is centred on the acini rather than ducts, although minor intraductal aggregates of neutrophils are often present. Lymphoepithelial lesions are absent or very rare [9, 10, 12, 13].
Differential diagnosis
The main histological differential diagnosis in surgically resected submandibular glands is hyper-IgG4 disease (see Sect. 5.4.1) and malignant lymphoma (see Sect. 5.10.3), whilst Sjögren-type lymphoepithelial sialadenitis (see Sect. 5.10.1) is only rarely diagnosed in this gland in the absence of parotid involvement.
Treatment and prognosis
The prognosis is good after complete surgical removal.
5.2.3 Chronic Sialectatic Parotitis
Definition
A tumor-like inflammatory condition affecting parotid glands.
Epidemiology
An uncommon disease occurring mostly in (male) children and only rarely in adults.
Etiology and pathogenesis
Although the pathogenesis is unknown, an allergic reaction has been postulated.
Clinical aspect
Patients present with chronic, recurrent and mostly bilateral and painful swelling of the parotid glands.
Macroscopy
Biopsies are rarely indicated or performed for chronic sialectatic parotitis.
Microscopy
Histology shows chronic lymphocytic infiltration around large, interlobular ducts with prominent germinal centres and ductal cysts, devoid of Sjögren-type lymphoepithelial lesions.
Differential diagnosis
Clinical correlation is necessary for a correct diagnosis. There is no association with Sjögren’s syndrome or HIV infection [10].
Treatment and prognosis
Surgical treatment is reserved only for extreme cases, as the prognosis is that of a recurrent and chronic disease. In the juvenile variant, the disease often subsides at the end of puberty.
5.3 Infections of Salivary Glands
Definition
Infective disease of salivary glands caused by bacteria, fungi and viruses.
5.3.1 Bacteria and Fungi
Epidemiology
Both are rather infrequent causes of infections in Europe or North America, but tuberculosis is not uncommon in Africa.
Etiology and pathogenesis
The changes are secondary to inflammation caused by the infective agent, such as tuberculosis, cat scratch disease, syphilis, tularaemia, brucellosis and toxoplasmosis.
Clinical aspect
The clinical presentation may be that of a salivary gland mass.
Macroscopy
Surgical excision is rarely performed.
Microscopy
Inflammation with or without granulomata may involve the gland itself or the intraparotid lymph nodes. Special stains for microorganisms are recommended, but may not always identify the causative organisms, particularly in tuberculosis. It may be said (particularly in high incidence areas) that any granulomatous inflammation is tuberculosis until clinically proven otherwise.
Differential diagnosis
The differential diagnosis includes non-infectious granulomatous disorders, in particular sarcoidosis (see below).
Treatment and prognosis
The patient is managed with medical therapy, which usually resolves the infection.
5.3.2 Viruses
Definition
Infective lesion caused by viruses.
Epidemiology
Several viral diseases may cause glandular infiltration by chronic inflammatory cells but are rarely biopsied. The most common are mumps and cytomegalovirus (CMV) infection. Mumps (epidemic parotitis) presents as an acute illness occurring in children and young adults. Following the introduction of a vaccine from attenuated live mumps virus, the incidence of the disease has decreased significantly.
CMV may be localised to the salivary gland or may involve the glands as part of a systemic disease in either the new-born or in immunocompromised adults particularly those with HIV (human immunodeficiency virus)/AIDS (acquired immune deficiency syndrome). The diagnosis of CMV is made by finding the characteristically enlarged acinar cells with intranuclear inclusions [14, 15].
Microscopy
The salivary glands show a non-specific chronic inflammatory cell infiltrate.
Differential diagnosis
The histopathological differential diagnosis is with other infections and chronic inflammatory infiltrates, and the diagnosis is best confirmed by virology tests.
Treatment and prognosis
Disease in the salivary glands tends to resolve without morbidity.
5.3.2.1 HIV-Related Disease
The most characteristic lesion seen in HIV/AIDS is cystic lymphoid hyperplasia (see below – Sect. 5.7.4). Other lesions seen in the salivary glands in AIDS include infections due to immune compromised state, lymphoma and intraparotid lymphadenopathy [16].
5.4 Miscellaneous Inflammatory Disorders
5.4.1 Hyper-IgG4 Disease
Definition
A fibrous inflammatory disease of exocrine glands with excess IgG4-positive plasma cells.
Epidemiology
Patients are usually adults, and there is no sex predilection.
Etiology and pathogenesis
The true incidence is not known. In the head and neck, hyper-IgG4 disease seems to comprise a small proportion of cases of chronic sclerosing submandibular sialadenitis.
Clinical aspect
Patients present with a tumor-like mass alone or associated with systemic IgG4-related sclerosing disorders such as autoimmune pancreatitis, autoimmune cholangitis, lesions in retroperitoneum/mediastinum and orbital swellings. The so-called pseudotumour of the orbit is part of the manifestations of hyper-IgG4 disease.
Macroscopy
The salivary gland is replaced by white and firm tissue which mimics a malignant tumor.
Microscopy
The histology shows preservation of salivary gland lobules, but there is significant inter- and intralobular fibrosis with acinar atrophy. There are no lymphoepithelial lesions, but there is a lymphoplasmacytic infiltrate, which contains numerous IgG4-positive plasma cells. In a series of 13 cases [17], there was a mean of 229/high-power field (HPF) (range 75–608) IgG4-positive plasma cells and an overall IgG4/IgG ratio of 0.86. This significantly higher number of IgG4-positive plasma cells contrasts with the lower number of IgG4-positive plasma cells seen in chronic sialadenitis, not otherwise specified [18].
Differential diagnosis
The main histological differential diagnosis is classical chronic sclerosing submandibular sialadenitis associated with lithiasis and Sjögren-type lymphoepithelial sialadenitis (both mainly devoid of IgG4-positive plasma cell) [19, 20].
Treatment and prognosis
Diagnosis in multisystemic disease is important as immunosuppressive therapy (systemic corticosteroid) is very effective [18–20].
5.4.2 Sarcoidosis
This multisystem granulomatous disorder of unknown etiology is an important and relatively frequent cause of granulomatous inflammation in intraparotid lymph nodes or the salivary glands themselves. The histological picture is typically that of multiple well-demarcated non-necrotising granulomata composed of epithelioid histiocytes with or without scattered multi-nucleate giant cells; asteroid and Schaumann bodies may be present on occasions.
5.4.3 Kimura’s Disease
This is seen predominantly in Oriental patients and frequently affects the salivary glands. Microscopy shows acinar atrophy and fibrosis, often affecting surrounding ducts, and a heavy lymphoid infiltrate with formation of irregularly shaped follicles, together with numerous eosinophils often forming abscesses, typically within germinal centres. There is also a proliferation of high endothelial venules with slitlike lumina lined by non-vacuolated cuboidal or atrophic endothelial cells containing pale oval nuclei. Recurrences sometimes occur after excision.
5.5 Miscellaneous Non-inflammatory Disorders
There are a variety of non-infectious inflammatory conditions such as xanthogranulomatous sialadenitis, Rosai-Dorfman disease [21] and amyloidosis [22] that will not be discussed here.
5.5.1 Necrotising Sialometaplasia (Salivary Gland Infarction)
Definition
Reactive vascular and/or inflammatory condition of salivary glands.
Epidemiology
This is a rare condition affecting mostly the intraoral minor salivary glands – palate in particular – of adults, mainly male, patients.
Etiology and pathogenesis
The classical necrotising sialometaplasia is a reaction pattern of salivary glands following salivary gland infarction. Although the underlying pathogenesis is generally considered to be ischaemia, in addition to trauma such as from an ill-fitting denture, often no predisposing factor is found.
Clinical aspect
Patients present with an ulcer in the palate which is often biopsied with a clinical suspicion of malignancy. The symptoms may also appear after oral surgery for unrelated causes. Also, there has been a case where the trauma was caused by a stalk of a peach, the patient had eaten few weeks before.
Macroscopy
The specimens are usually received as biopsy fragments.
Microscopy
Microscopy in the early stages shows partial necrosis of salivary lobules with later a moderate chronic inflammatory infiltrate and immature or mature squamous metaplasia, partly or totally replacing the lobules (Fig. 5.2) [23, 24].

Necrotising sialometaplasia. Most of the ducts and acini are replaced by mature non-keratinizing squamous epithelium. The lobular architecture of the gland is preserved
Differential diagnosis
Due to reactive cellular atypia and increased proliferative and mitotic activity, there is a superficial resemblance to mucoepidermoid and squamous cell carcinoma. The preserved lobular architecture of the lesion together with the clinical situation (mostly postoperative) is of paramount importance for the correct diagnosis [2, 24].
Treatment and prognosis
Once the diagnosis has been confirmed, the behaviour is that of a benign self-healing disease.
5.5.2 Sialadenosis
Definition
Sialadenosis is a non-inflammatory disease of the salivary glands characterised by recurrent and painless bilateral swelling mainly of the parotid glands.
Epidemiology
It is most frequent in young women, but its exact incidence is not known as the parotid enlargement may be interpreted as accumulation of facial fat clinically.
Etiology and pathogenesis
There is an association with eating disorders (e.g. anorexia, bulimia), malnutrition, chronic alcoholism and liver cirrhosis and with some drugs such as antihypertensive agents and antidepressant [25]; also, sialadenosis has been related to some endocrine disorders (diabetes mellitus, ovarian and thyroid insufficiencies). Recent data suggest that the underlying process may be a disorder of the autonomic nervous system affecting salivary gland innervation, causing a secondary functional atrophy of myoepithelial cells [25].
Clinical aspect
Patient complains of cosmetically disfiguring swelling of parotid glands which may be mildly painful.
Microscopy
Histologically, there is generalised enlargement of the serous acinar cells (two or three times the normal size) with slight compression of striated ducts but totally devoid of inflammation.
Differential diagnosis
As morphometric measurements usually are not available or performed, the subjective impression of enlarged acini should always be correlated with the clinical findings.
Treatment and prognosis
If the predisposing factors (eating disorder, drugs, alcohol, etc.) can be corrected, sialadenosis tends to regress.
5.5.3 Adenomatoid Hyperplasia of Salivary Glands
Adenomatoid hyperplasia of salivary glands can be subdivided into two categories as follows:
5.5.3.1 Acinar Adenomatoid Hyperplasia
Definition
Acinar adenomatoid hyperplasia (AAH) is a hyperplastic disorder of salivary glands.
Epidemiology
It is a rare condition mostly affecting intraoral minor salivary glands, the palate in particular. It can affect all ages, although most patients are between 30 and 60 years old. There is a slight male predominance.
Etiology and pathogenesis
The etiology is unknown; possible relevant factors include local trauma due to denture or tobacco smoking.
Clinical aspect
This lesion is usually asymptomatic, often being noted on routine oral or dental examination. Most cases occur in the palate, but other minor salivary glands can be involved [26].
Macroscopy
Examination reveals a nodular submucosal swelling up to 30 mm in diameter; usually biopsy fragments are provided.
Microscopy
Histology shows hyperplastic mucous or seromucous acini with preserved lobular arrangement usually devoid of significant inflammation or fibrosis.
Differential diagnosis
The histological diagnosis is a matter of exclusion of other hyperplastic and neoplastic conditions of minor salivary glands.
Treatment and prognosis
The treatment tends to be surgical and the prognosis is good.
5.5.3.2 Intercalated Duct Hyperplasia (Also Known as Ductal Adenomatoid Hyperplasia)
Definition
Hyperplastic disorder of intercalated ducts.
Epidemiology
Relatively rare, idiopathic condition.
Etiology and pathogenesis
The etiology is unknown, but there is an association in literature between intercalated duct hyperplasia/adenoma and benign and malignant tumors of the salivary glands [27–29]. The recognition in literature of intercalated duct hyperplasia has shed light about the histogenesis of some tumors such as epithelial-myoepithelial carcinoma as a tumor of ductal origin and also perhaps explained why in hybrid carcinomas of the salivary glands, equally very rare, the most frequent combination is that of EMC and adenoid cystic carcinoma [28].
Clinical aspect
The clinical presentation is that of the associated tumor where intercalated duct hyperplasia represents an incidental finding at histological examination.
Macro
Appearance is also that of the associated tumor for which the specimen is surgically resected.
Microscopy
It is either a well-circumscribed single nodule or multiple unencapsulated foci of proliferating intercalated ducts. The ducts are small in size and are lined by an inner layer of cuboidal cells and an outer layer of myoepithelial cells [27].
Differential diagnosis
When not associated with another tumor of salivary gland, the differential diagnosis is with a small basal cell adenoma.
Treatment and prognosis
The treatment is surgical, and the prognosis is that of the accompanying tumor. Intercalated ductal hyperplasia in itself has a good prognosis.
5.5.4 Irradiation Changes
Definition
Cytohistological changes of salivary glands following radiotherapy.
Epidemiology
Irradiation changes are relatively common in patients with head and neck cancers since radiotherapy is used as part of their treatment.
Etiology and pathogenesis
Acini (particularly serous) are very sensitive to radiation.
Clinical aspect
The common clinical sign is tenderness and swelling of the irradiated glands, which is followed by xerostomia as a common complication.
Macroscopy
The glands have increased consistency, but the lobular architecture is preserved.
Microscopy
The early changes are those of swelling, vacuolation and necrosis of ductal and acinar cells [30]. An initial acute inflammatory response is later followed by chronic, non-specific inflammation with acinar atrophy, dilatation of excretory ducts and squamous and mucous metaplasia. The metaplastic cells may display cellular atypia and cytoplasmic vacuolisation. In more advanced stages, there is a major loss of acinar parenchyma, fibrosis, lipomatosis, chronic inflammation and changes in arteries.
Differential diagnosis
Is mostly with squamous cell and mucoepidermoid carcinoma. In irradiation changes, the cytological atypia is confined within ducts and acini, whilst mucoepidermoid and squamous cell carcinomas replace the normal tissue.
Treatment and prognosis
Dependent on the extent of salivary gland involvement, loss of saliva production may be progressive and irreversible. Recent experimental studies have shown that radiation-damaged salivary glands can be restored and reacquire their morphology and function.
5.5.5 Tissue Changes Following Fine Needle Aspiration
Definition
Histological changes of normal and pathological tissue of salivary glands following fine needle aspiration (FNA).
Epidemiology
Not very common phenomenon despite the common use of FNA in the preoperative assessment of salivary gland lesions [31].
Etiology and pathogenesis
Possible causes include trauma by pressure or by FNA [32] with vascular damage and aggravated sensitivity of oncocytic cells to hypoxia.
Clinical aspect
These are non-specific and are those of a salivary gland mass for which FNA is being undertaken. In some cases tumor-like changes can develop such as so-called xanthogranulomatous sialadenitis with an exuberant inflammation after total or subtotal tumor necrosis following FNA.
Macroscopy
The surgical specimen may contain the needle tract and areas of necrosis and haemorrhage.
Microscopy
These comprise focal necrosis and inflammation up to subtotal or total infarction with or without reactive pseudo-malignant changes [31–33]. This is most frequent in Warthin’s tumor [34]. A reticulin stain may identify the ghost architecture, and immunohistochemistry with an antimitochondrial antibody may highlight residual oncocytic differentiation of the epithelial cells [35]. Significant infarction has also been noted in acinic cell carcinoma, but the histological diagnosis was not compromised [36].
Differential diagnosis
The necrotic and pseudo-malignant changes can be confused with carcinoma of squamous or mucoepidermoid type.
Treatment and prognosis
Surgical excision is usually curative. Despite some worrisome histological findings, there is general agreement that FNA of salivary gland lesion is a safe procedure, and it does not usually alter the histological diagnosis [36].
5.6 Oncocytic Lesions
Definition
Lesions composed of oncocytic cells which possess densely eosinophilic and granular cytoplasm due to excess mitochondria. Two cell types are recognised: light and dark. The former contain abundant eosinophilic cytoplasm with central, round nuclei and visible nucleoli; the latter possess pyknotic nuclei, with relatively scanty densely eosinophilic cytoplasm. Recognition of these two cell types is essential in the differential diagnosis of primary and metastatic tumors with oncocytic characteristics (see Sect. 5.8.5).
Epidemiology
Oncocytic change is frequent in salivary glands, particularly in older people. The cells can be confirmed by an antimitochondrial antibody [35, 37].
Etiology and pathogenesis
Research in mitochondrial DNA mutations suggests that a molecular genetic abnormality interferes with mitochondrial DNA which leads to the increased number of enlarged mitochondria in the cytoplasm of oncocytic cells (mitochondriopathy) [38].
In salivary glands, three main types of oncocytic lesions are recognised.
5.6.1 Focal and Diffuse Oncocytosis
Definition
Small microscopic foci of oncocytic metaplasia, usually of ducts, but occasionally also acini.
Epidemiology
Focal oncocytosis occurs with increasing frequency with advancing age (Fig. 5.3) [2]. In contrast, diffuse oncocytosis of the parotid is extremely rare.

Focal oncocytosis of the parotid gland. Some ducts and acinar cells show cytoplasmic oncocytic features
Etiology and pathogenesis
Genetic changes affecting mitochondrial DNA may have a role (see above) [38].
Clinical aspects
There are no specific clinical signs unless oncocytosis is associated with a salivary gland tumor causing a clinical mass. Specimens for histological examination usually are removed for other reasons (primary and metastatic tumors, neck dissection, etc.).
Macroscopy
The affected salivary gland may show involutional fatty changes only.
Microscopy
Histological examination shows ducts and acini replaced by light and dark oncocytic cells involving one or more lobules (focal oncocytosis) or involving virtually the whole gland (diffuse oncocytosis – very rare and often bilateral).
Differential diagnosis
In small biopsy specimens, it may be difficult to distinguish from Warthin’s tumor and oncocytoma or other tumors showing oncocytic metaplasia, e.g. pleomorphic adenoma, myoepithelioma and mucoepidermoid carcinoma (see Sects. 5.8.1, 5.8.2, 5.8.4, 5.8.5 and 5.9.3).
Treatment and prognosis
The prognosis is favourable with or without surgical resection.
5.6.2 Multifocal Nodular Oncocytic Hyperplasia
Definition
Multifocal nodular oncocytic hyperplasia (MNOH) is a partial replacement of salivary gland ducts and acini by multiple foci of oncocytic cells.
Epidemiology
It is a rare condition observed from time to time in routine surgical pathology. Adults are affected and the lesion can be bilateral.
Etiology and pathogenesis
Etiology is unknown.
Clinical aspects
Parotid swelling – sometimes bilateral – is the common clinical presentation.
Macroscopy
The parotid shows multiple nodules of varying size, but the diagnosis is essentially microscopic.
Microscopy
The oncocytic nodules appear to engulf normal acini giving a false impression of invasion. The nodules are circumscribed, but not usually encapsulated, but elicit no reaction in the surrounding normal parenchyma. The oncocytic cells often have clear and only faintly granular cytoplasm (Fig. 5.4). If a capsule or part of it is noted, a diagnosis of oncocytoma should be favoured. The two conditions can coexist, but there is little agreement on how to distinguish oncocytoma in a background of MNOH.

Multiple nodular oncocytic hyperplasia. Nodules composed of oncocytic cells that can show clear change
Differential diagnosis
The main differential diagnosis is solid-type acinic cell carcinoma. The immunohistochemical demonstration of a small component of basal cells (CK5/6, p63 positive) is in favour of an oncocytic tumor and excludes acinic cell carcinoma. A clear cell appearance of MNOH can be mistaken for other clear cell neoplasms of salivary glands [37, 39, 40].
Treatment and prognosis
The treatment is surgical. Frequent recurrences are due to the diffuse, multifocal character of this lesion.
5.6.3 Ductal Oncocytosis
Definition
Hyperplastic/metaplastic oncocytic disorder affecting ducts of minor salivary glands.
Epidemiology
Ductal oncocytosis is relatively uncommon. It affects minor salivary glands, larynx in particular, followed by the floor of the mouth.
Clinical aspects
Small and painless nodule of the floor of the mouth.
Macroscopy
Small biopsy fragments or surgical specimen of the salivary gland.
Microscopy
The ductal epithelium is replaced by oncocytic cells. Sometimes the architecture is papillary resembling Warthin’s tumor [41].
Differential diagnosis
The main differential is with Warthin’s tumor which occurs almost exclusively in the parotid.
Treatment and prognosis
Resection of the lesion is curative.
5.7 Cysts
Definition
Cystic lesions arising mainly from the ductal system of salivary glands.
Epidemiology
Some are relatively frequent; the commonest are mucocoeles (80 %) including ranula, ductal cysts (11 %) and cystic lymphoepithelial lesions (7 %) [42]. Those associated with genetic/inherited disorders are particularly rare (see Table 5.1).
Etiology and pathogenesis
Cysts can be classified according to the epidemiology and pathogenesis.
Clinical aspect
The most common clinical presentation is that of a painless mass in the salivary gland.
Macroscopy
The cyst can be single or composed of multiple locules of varying size.
Microscopy, differential diagnosis, treatment and prognosis
They will be discussed for each subtype (see Sects. 5.7.1, 5.7.2, 5.7.3, 5.7.4, 5.7.5 and 5.7.6).
5.7.1 Salivary Polycystic Dysgenetic Disease
Definition
This very rare condition resembles cystic anomalies of other organs, such as the kidney, liver and pancreas, although no association has been described [43].
Epidemiology
Rare disorder. Some cases are familial [44], and almost all cases have occurred in females. Most patients manifest in childhood, a few in adulthood. It affects the parotid glands almost exclusively, usually bilaterally.
Etiology and pathogenesis
The report of familial cases suggests a possible genetic transmission. The postulated ducts of origin in salivary polycystic dysgenetic disease are the intercalated ducts.
Clinical aspects
The children complain of recurrent parotid gland swellings.
Macroscopy
The parotid shows multiple small cysts.
Microscopy
The glands maintain the lobular architecture, and some lobules are affected more severely than others. The cysts vary in size up to a few mm, and they are irregular in shape. The lining epithelium is flat, cuboidal to low columnar resembling the epithelium of intercalated ducts. The lumina contain secretion with spherical microliths. Remnants of salivary acini are seen between the cysts, and thick fibrous interlobular septa are often prominent.
Differential diagnosis
The differential diagnosis includes sclerosing polycystic adenosis (see Sect. 5.7.5), cystadenomas and benign and malignant tumors with a cystic component. The young age of patients and the bilateral nature of the lesions are helpful diagnostic markers.
Treatment and prognosis
The treatment tends to be surgical for cosmetic reasons only. The prognosis is that of a benign lesion.
Cystic fibrosis can also involve the duct system of salivary glands with preference for submandibular gland, sublingual gland and minor salivary glands. The histological changes observed are due to the abnormal mucous plugging of excretory ducts with characteristic deposition of dense eosinophilic material in the ducts. Recent data have identified the main genetic defects of cystic fibrosis [45] with new treatment strategies [46].
5.7.2 Salivary Duct Cyst
Definition
Form of retention cyst mostly seen in parotid gland.
Epidemiology
Rare acquired cyst that can occur at any age, although usually in patients over 30 years old.
Etiology and pathogenesis
This acquired cyst is due to dilatation of a salivary duct following obstruction due to different reasons [47].
Clinical aspect
A painless swelling in one parotid (85 % of cases).
Macroscopy
Well circumscribed and unilocular, usually 10–30 mm in size; they contain viscous brown fluid.
Microscopy
The wall of the cyst comprises dense fibrous tissue, 1–3 mm thick, and there is often mild to moderate chronic inflammation, but no dense lymphoid infiltrate. The epithelial lining comprises one or a few layers of cuboidal or columnar cells with occasional goblet cells and rarely squamous epithelium [42].
Differential diagnosis
Mostly with lymphoepithelial cyst which has a more dense lymphoid infiltrate.
Treatment and prognosis
The cyst is cured with surgical excision.
5.7.3 Benign Lymphoepithelial Cyst
Definition
An epithelial lined cyst surrounded by extensive lymphoid infiltrate.
Epidemiology
This is a rather infrequent cyst of parotid gland with a slight male predominance and mean age of onset at 46 years (range 18–79) [48, 49].
Etiology and pathogenesis
Benign lymphoepithelial cysts are thought to arise from embryological salivary gland inclusions in intraparotid lymph nodes [10, 50].
Clinical aspects
Painless, usually solitary but occasionally bilateral mass in parotid gland.
Macroscopy
The average diameter of the cyst is 25 mm but may reach 70 mm.
Microscopy
Histology shows the lining epithelium to be cuboidal, columnar, lymphoepithelial, squamous or a combination thereof. Small number of goblet cells may be present (Fig. 5.5). This lining is surrounded by abundant lymphoid tissue composed of small lymphocytes, plasma cells and germinal centres. Lymphoepithelial lesions are not a feature [10].

Simple, benign lymphoepithelial cyst. The cavity is lined with columnar and cuboidal cells with scattered goblet cells. The surrounding tissue contains small lymphocytes and macrophages. Beyond this is a capsule and subcapsular space resembling that of a lymph node
Differential diagnosis
The main differential diagnosis is with Sjögren’s syndrome lymphoepithelial sialadenitis with cystic component (see Sect. 5.10.1) and cystic lymphoepithelial lesion of AIDS (see Sect. 5.7.4). Clinicopathological correlation may be necessary for definitive diagnosis [10].
Treatment and prognosis
Benign lymphoepithelial cysts are not known to recur after surgical excision.
5.7.4 Cystic Lymphoepithelial Lesion of AIDS
Definition
A diffuse and/or cystic, usually bilateral, enlargement of parotid glands.
Epidemiology
Cystic lymphoepithelial lesion has been seen in about 5 % of HIV-positive patients; however, this disease has become relatively less common in Western countries since the availability of effective antiretroviral therapy.
Etiology and pathogenesis
Infection by HIV virus, but the exact pathogenesis is unknown.
Clinical aspects
Cystic lymphoepithelial lesion of AIDS can be the first clinical manifestation of HIV disease, and thus histological identification of it means a diagnosis of AIDS.
Macroscopy
Cystic and enlarged parotid gland.
Microscopy
Microscopic examination shows a dense lymphoid infiltrate including exaggerated follicular hyperplasia. There is an elaborate dendritic reticulum cell network within which there is evidence of active HIV replication, although the exact histogenesis of this lesion is not understood. Plasma cells (polytypic) are often numerous. The glandular parenchyma is atrophic, and multiple cystic spaces are seen. The cysts are dilated striated ducts, and the lining sometimes shows squamous metaplasia. The cysts are infiltrated by lymphoid cells including a variable number of marginal zone B cells, and there are multiple typical lymphoepithelial lesions [15].
Differential diagnosis
There is considerable histomorphological overlap with lymphoepithelial sialadenitis (see Sect. 5.10.1), but the cysts are usually larger [9, 15, 50].
Treatment and prognosis
The lymphoid infiltrate is polyclonal, and although it usually does not progress to lymphoma, nevertheless patients with HIV disease are in general at risk of developing aggressive B-cell lymphomas, most commonly Burkitt’s and diffuse large B-cell lymphoma [51].
5.7.5 Sclerosing Polycystic Adenosis
Definition
Sclerosing polycystic adenosis (SPA) is a recently described rare salivary gland lesion, originally thought to be a process somewhat analogous to epithelial proliferative lesions of the breast such as fibrocystic disease and sclerosing adenosis [52]. Subsequent demonstration of clonality suggests that it is probably a neoplasm [53].
Epidemiology
SPA is a rare lesion of salivary glands. It occurs within a broad age range with a mean of 40 years (range 9–84 years of age). SPA is slightly more common in females with a male-to-female ratio approximately 2:3. Location of SPA is mostly in the parotid gland, less commonly in the submandibular gland, and minor salivary glands of oral mucosa.
Etiology and pathogenesis
The nature of this lesion was initially believed to be reactive or inflammatory [52]. However, using X chromosome-linked human androgen receptor (HUMARA analysis), later investigators have shown that SPA is a clonal process [53]. It not infrequently harbours intraductal dysplastic epithelial proliferations including cases where the degree of atypia and structural changes reaches that of ductal carcinoma in situ (DCIS) [54].
Clinical aspects
Patients typically present with slow-growing mass; some of them have pain or sensation. Onset of symptoms ranges from 10 days to 2 years. One patient, in addition, had a history of chronic recurrent parotitis.
Macroscopy
Grossly, most tumors are firm or rubbery, well circumscribed and surrounded by normal salivary gland tissue. The tumors range in size from 3 to 70 mm in greatest dimensions. The cut surface is pale and glistening with multiple small cystic spaces ranging from 1 to 3 mm in diameter.
Microscopy
Histological examination shows a well circumscribed partly encapsulated mass with preservation of the lobular architecture and a variable amount of inflammatory infiltrate in a sclerotic stroma (Fig. 5.6). Multiple dilated ducts are often lined by a flattened bilayered epithelium. The ductal cells comprise a spectrum of vacuolated, foamy, apocrine and mucous appearances (Fig. 5.7), and focal squamous metaplasia may be also present. The hallmark of the lesions is the presence of large acinar cells with numerous coarse eosinophilic periodic acid-Schiff (PAS)-positive cytoplasmic granules (Fig. 5.8). Some ducts contain solid and cribriform epithelial proliferations with vacuolated foamy cells having a sebaceous-like appearance. In all cases, there is focal intraluminal epithelial proliferation giving rise to solid, microcystic and cribriform structures. In most cases, nuclear polymorphism is noted, ranging in severity from mild up to severe and then amounting to low-grade DCIS (Fig. 5.9). In places, tiny cell aggregates and small ducts embedded in sclerotic stroma reminiscent of stromal invasion can also be seen [55]. The ductal and acinar cells are positive for cytokeratin (AE1/AE3 and CAM5.2); variably positive for epithelial membrane antigen (EMA), S-100 protein and antimitochondrial antibody; and negative for CEA, p53 and HER2/neu. The acinar cells with coarse eosinophilic cytoplasm stain positively for GCDFP-15. Oestrogen and progesterone receptors are detected focally in some cases [54, 55]. Ducts, filled with hyperplastic and dysplastic epithelium, are surrounded by an intact myoepithelial layer, positive for αSMA, p63 and calponin. Polymerase chain reaction (PCR)-based analysis of patterns of X chromosome inactivation using a HUMARA locus demonstrated that SPA is composed of a clonal population [53].

Sclerosing polycystic adenosis. Histological examination shows a well-circumscribed partly encapsulated mass with preservation of the lobular architecture and a variable amount of inflammatory infiltrate in a sclerotic stroma

Sclerosing polycystic adenosis. Multiple dilated ducts are often lined by a flattened bilayered epithelium. The ductal cells comprise a spectrum of vacuolated, foamy, apocrine and mucous appearances

Sclerosing polycystic adenosis. The hallmark is a presence of large acinar cells with numerous coarse eosinophilic cytoplasmic granules

Sclerosing polycystic adenosis. Nuclear polymorphism is present, ranging in severity from mild up to severe dysplasia and then amounting to low-grade ductal carcinoma in situ
Differential diagnosis
Most cases of SPA were initially misdiagnosed as tumors, such as mucoepidermoid and acinic cell carcinomas, cystadenocarcinoma and pleomorphic adenoma. Major microscopic clues to a correct diagnosis include maintenance of the lobular architecture of the gland, ductal ectasia, scar-like hyalinised fibrous sclerosis and a spectrum of foamy, apocrine, granular and mucous cells, in addition to the presence of tubuloacinar structures composed of large acinar cells with prominent brightly eosinophilic zymogen-like cytoplasmic granules. Intraductal hyperplasia in some cases of SPA, particularly if associated with dysplasia, may cause suspicion of a low-grade malignancy, but clues to the benign nature of SPA are that it is well circumscribed, that it lacks an invasive growth pattern and that mitotic/proliferative activity is low. Major benign differential diagnoses include pleomorphic adenoma, polycystic dysgenetic disease (see Sect. 5.7.1) and chronic sclerosing sialadenitis (see Sect. 5.2.2). Definitive lobular growth pattern and large Paneth cell-like acinic cells of SPA are not seen in pleomorphic adenomas. In contrast, SPA lacks a prominent myoepithelial cell component and chondromyxoid stroma typical of pleomorphic adenoma. Chronic sclerosing sialadenitis lacks nodular pattern and typical structural heterogeneity of SPA, though both lesions share prominent fibrosis. Moreover, large acinic cells with coarse PAS-positive zymogen-like cytoplasmic granules are not seen in chronic sclerosing sialadenitis.
Treatment and prognosis
Treatment is primarily surgical with complete conservative local excision with good margins and facial nerve preservation followed by prolonged surveillance. Recurrences, sometimes multiple, have been reported quite frequently (29 %) as summarised by Gnepp et al. [56]. The proposed mechanism behind this is either incomplete surgical resection and/or multifocal disease [55, 57]. Although rare cases of invasive carcinoma developing in SPA have been described to date [58], no patient has developed metastases or died due to disease.
5.7.6 Miscellaneous Other Cysts
Other salivary cysts include dermoid, keratocystoma and a variety of epithelial and non-epithelial cysts including parasites and gas cysts in glass blowers [59].
Dermoid cyst of the parotid is very rare. A review of the literature has shown <10 cases reported [60], one in a child [61]. The cyst had the characteristic squamous lining with sebaceous glands and hair follicles in its wall as seen in dermoid cysts occurring in the orbit and floor of mouth.
Keratocystoma is also a rare, recently described, benign parotid tumor characterised by multicystic keratin-filled spaces lined with stratified squamous epithelium with no atypical features [62, 63].
5.8 Benign Tumors
5.8.1 Pleomorphic Adenoma
Definition
Pleomorphic adenoma (PA) is a tumor composed of a mixture of epithelial and modified myoepithelial cells in varying proportions. Most authors accept that PA is part of a spectrum of salivary gland adenomas with benign myoepithelioma, which is composed almost entirely of myoepithelial cells representing one end and basal cell adenoma and canalicular adenoma at the other end [64–66]. The particular morphology of any particular tumor reflects the different proportions of the constituent cells (Fig. 5.10). (Pleomorphic adenoma spectrum. Reproduced with permission from Zarbo [65]).

Pleomorphic adenoma spectrum (Reproduced with permission from Zarbo et al. [65])
Epidemiology
PA is the most common tumor of the salivary glands. PA arises de novo in healthy salivary glands where it accounts to approximately 60 % of all salivary gland tumors. Although most often found in young to middle-aged women, PA can occur in either sex and at any age. Up to 80 % occur in the superficial lobe of the parotid gland.
Etiology and pathogenesis
Not known.
Clinical aspects
It typically presents as a painless swelling.
Macroscopy
PAs are usually well-circumscribed masses of 20–40 mm. The cut surface is white, and grey glistening areas are commonly seen. Recurrent PA occurs after incomplete surgical excision and is usually composed of multiple nodules completely separate from each other. In the first recurrence the nodules are usually seen within salivary gland tissue, but in further recurrences tumors are found in the soft tissue of the surgical bed.
Microscopy
Histologically, PA is ‘a tumor of variable capsulation characterised microscopically by architectural rather than cellular pleomorphism. Epithelial and modified myoepithelial elements intermingle most commonly with tissue of mucoid, myxoid or chondroid appearance [67]. The pattern varies from case to case and also from area to area within any individual tumor. All are composed of a mixture of ductal epithelial cells, basal and myoepithelial cells and variable amounts of stroma, both hyaline and chondromyxoid. Attempts have been made to subclassify PA based on the proportions of cell types and stroma [68], but because of the variation in any tumor, this is difficult and probably has no prognostic value. Ducts are lined with flat, cuboidal or columnar epithelial cells, with little or no atypia. The ducts are usually small tubules but can be cystically dilated and also arranged in a cribriform-basaloid pattern, resembling adenoid cystic carcinoma, but mitotic figures are rare and the proliferation index low. Squamous metaplasia with or without keratinization is seen in up to 25 % of PAs [69] (Fig. 5.11). Squamous plus mucinous metaplasia in PA resembling mucoepidermoid carcinoma is rarely present (Fig. 5.12). Myoepithelial cells are arranged in sheets, smaller islands and trabeculae and also surround epithelium-lined spaces. As in benign myoepithelioma, neoplastic myoepithelial cells may take several forms – epithelioid, spindle, plasmacytoid, clear and oncocytic, as well as transitional forms with features of two or more of these types (Fig. 5.13). The stroma varies in amount and is either densely eosinophilic hyaline material or chondromyxoid tissue (Fig. 5.14). The former is composed of basement membrane material and stains with PAS diastase and collagen type IV; the chondromyxoid material only rarely resembles true cartilage and is Alcian blue positive. Calcification and bone formation can occur in long-standing tumors. Occasionally, collagenous spherules and crystalloids are seen (Fig. 5.15), particularly in tumors rich in myoepithelial cells of the plasmacytoid type [70]. Nuclear atypia is not common but can be seen in tumors where epithelial or myoepithelial cells display oncocytic features [69, 71]. Occasional myoepithelial cell nuclei are enlarged and bizarre, somewhat analogous to ‘ancient’ change in schwannomas. Mitotic figures are generally sparse but can occur as part of the repair process after FNA. Similarly, areas of necrosis or haemorrhage may follow surgical manipulation, FNA or other trauma, and these neoplasms should also be sampled thoroughly. Tumor cells in lymphatics (‘vascular invasion’) are occasionally seen in benign PAs (Fig. 5.16), but this does not indicate malignancy [72]. None of the reported cases were followed by metastases. PAs are often completely or partly surrounded by a fibrous capsule of variable thickness, but it can be absent, especially in tumors of the minor glands. Neoplastic elements may extend into and even through the capsule in the form of microscopic pseudopodia or apparent satellite nodules. They may be the cause of future recurrence after apparent surgical removal (Fig. 5.17) [73], and their presence should be noted in the surgical pathology report. Special stains and immunohistochemistry are not necessary for the diagnosis in most cases, but can be used to identify the different cell types and also early malignant change.

Pleomorphic adenoma: myoepithelial cells with an epithelioid cytomorphology. These cells may also be spindle shaped and plasmacytoid (hyaline) or have clear cytoplasm. Note also a small duct and a focus of squamous metaplasia. Keratinizing squamous metaplasia is seen in up to a quarter of pleomorphic adenomas

Pleomorphic adenoma with squamous and focal mucinous metaplasia resembling mucoepidermoid carcinoma

Pleomorphic adenoma: myoepithelial cells showing an epithelioid and plasmacytoid appearance

Pleomorphic adenoma: chondromyxoid stroma containing isolated small ducts and small aggregates of myoepithelial cells

Collagenous crystalloids can be seen in some benign myoepitheliomas and myoepithelium-rich pleomorphic adenomas

Vascular permeation is a rare finding in benign pleomorphic adenoma, due to displacement of neoplastic cells into vascular spaces. It is not indicative of malignancy

Recurrent pleomorphic adenoma. Multiple and often well-separated tumor nodules of different sizes are seen in periglandular soft tissue
More than half of PAs can be shown to have breakpoints affecting chromosomes, 8q12 (>50 % of cases) and 12q14-15 (10–15 %). The involved genes are PLAG1 and HMGA2.
Differential diagnosis
PA should be distinguished from other adenomas of salivary gland such as myoepithelial and basal cell adenoma (see Sects. 5.8.2 and 5.8.3).
Treatment and prognosis
Complete surgical excision with a rim of normal salivary gland tissue is the treatment of choice. Incomplete excision leads to a local recurrence in the surgical bed. The long-term prognosis is excellent providing excision is complete.
5.8.1.1 Salivary Gland Anlage Tumor (‘Congenital Pleomorphic Adenoma’)
Definition
Salivary gland anlage tumor (SGAT) is a pedunculated polypoid lesion of the nasopharynx that presents with respiratory distress syndrome at birth or within first few weeks of life.
Epidemiology
Very rare tumor with fewer than 30 cases reported in literature [74–76].
Etiology and pathogenesis
The morphology of SGAT is the same as the normal salivary glands in early weeks of their development. The pathogenesis is most likely hamartomatous.
Clinical aspects
Respiratory distress usually starting at about 6 weeks after birth. There is a predilection for males. Radiological investigation helps to identify the tumor in the posterior septum.
Macroscopy
Well-circumscribed nodule usually solid but may contain necrotic and cystic areas. The gross findings are those of bosselated surface and polypoid pedunculated mass measuring between 1.3 and 3.0 cm in greatest dimension. The tumors are attached by a thick stalk to the nasopharynx, and they are soft in consistency and white to pink in colour. The mucosal surface is intact in most cases.
Microscopy
SGAT is characterised by solid cords and branching duct-like structures that appear to originate from the surface mucosa. Some of the duct-like structures have a focal squamous lining resembling sialometaplasia. The tumors are divided by variously thick septa into nodules composed of fascicles of spindle-shaped and ovoid cells with indistinctive borders, eosinophilic cytoplasm and bland nuclei. Within these nodules, the cells focally form glands, cystic spaces and squamous cell nests.
Differential diagnosis
The biphasic multinodular growth pattern and solid nodules composed of mesenchyme-like spindle-shaped cells can mimic synovial sarcoma. The presence of budding epithelium from the surface mucosa in SGAT, its actin positivity and lack of numerous mitotic figures are major distinguishing features from synovial sarcoma. Low-grade mucoepidermoid carcinoma can be distinguished because of presence of spindled actin-positive stromal cells and keratinizing squamous epithelium in SGAT.
Treatment and prognosis
Although potentially fatal due to its location causing respiratory obstruction, prognosis after surgery is good. SGAT is a benign lesion characterised by non-recurring clinical behaviour.
5.8.2 Benign Myoepithelioma
Definition
Myoepithelioma (myoepithelial adenoma) is a benign neoplasm composed almost exclusively of myoepithelial cells. It represents one end of the spectrum of benign salivary gland tumors which also includes PA and basal cell adenoma [67].
Epidemiology
The incidence of myoepithelioma depends on how strictly criteria of myoepithelial predominance are applied for diagnosis; thus, percentages vary from 0.3 to 5.7 [77]. Men and women are equally affected. The most common sites include parotid gland (48 %) and the palate (35 %), but any salivary gland may be affected [77]. Patients have ranged from 6 to 98 in age with a mean in the early to mid-40s [77].
Etiology and pathogenesis
Whether or not it is truly a separate biological entity is debatable, but most commentators believe that it represents one end of a spectrum that also includes pleomorphic and at least some basal cell adenomas.
Clinical aspects
Most cases present as a well-circumscribed mass, usually 10–50 mm in diameter, in either major or minor salivary glands.
Macroscopy
Grossly, myoepitheliomas are usually well circumscribed and encapsulated and have yellow-tan colour and glistening cut surface.
Microscopy
There are several typical appearances, reflecting the different forms that neoplastic myoepithelial cells can take. Solid, myxoid and reticular growth patterns may be seen, and the component cells may be spindle shaped, plasmacytoid (hyaline), clear, epithelioid or oncocytic (Fig. 5.18) and occasionally mucinous. Many tumors show more than one growth pattern or cell type, but myoepitheliomas of the minor glands are more often composed of plasmacytoid cells and those of the parotid spindle cells [78]. Although most authors accept the plasmacytoid cells as myoepithelial, it has been suggested that these cells originate from luminal and not from myoepithelial cells [79], and thus the tumors should possibly be reclassified as plasmacytoid adenomas [79]. A clear cell variant can occur in both major and minor glands [80] but is relatively rare. The stroma of most myoepitheliomas is usually scanty, fibrous or myxoid, and it may very occasionally contain chondroid material or mature fat cells [81]. Extracellular collagenous crystalloids are seen in 10–20 % of plasmacytoid cell-type myoepitheliomas (as well as sometimes in myoepithelial-rich PAs); these structures are about 50–100 μm in diameter and consist of radially arranged needle-shaped fibres composed of collagen types I and III, which stain red with the van Gieson method (Fig. 5.15) [70]. Immunohistochemically, there may be considerable variability in staining within the same tumor and between different tumors. However, almost all tumors express S-100 protein and broad-spectrum cytokeratins (AE1/AE3) and some cytokeratin subtypes, mostly CK14 and CK 5/6. αSMA and muscle-specific actin are expressed in spindle-shaped myoepithelial cells, but they are usually absent in epithelioid and plasmacytoid cells. Staining for CD10, calponin, smooth muscle heavy chain and maspin is inconsistent, but p63, vimentin and GFAP are positive in most benign myoepitheliomas.

Benign myoepithelioma composed of plasmacytoid (hyaline) and epithelioid cells with areas of myxoid stroma. Plasmacytoid cells have eccentric nuclei and dense eosinophilic cytoplasm
Differential diagnosis
Spindle cell myoepithelioma should be distinguished from schwannoma, solitary fibrous tumor, synovial sarcoma and spindle cell sarcomas. The clear cell variant must be distinguished from other clear cell tumors of salivary glands both primary and secondary, in particular from metastatic renal cell carcinoma. Immunohistochemistry is valuable in demonstration of myoepithelial phenotype in these tumors. Myoepithelial carcinoma, in contrast to benign myoepithelioma, shows invasive growth, necrosis and high proliferative index (MIB1). Scanty small ducts may be present (usually less than 10 % of the tumor tissue) in otherwise typical myoepitheliomas, but if more numerous, the tumor should be considered as a myoepithelial cell-rich PA.
Treatment and prognosis
The behaviour of myoepithelioma is similar to that of PA, and complete excision is curative. Neither growth pattern nor cell type appears to carry prognostic significance. Malignant change in a benign lesion has been described [82], but too little information is available about the percentage of cases involved.
5.8.3 Basal Cell Adenoma
Definition
A tumor composed of basal cells without myxoid component (previously called monomorphic adenoma).
Epidemiology
Basal cell adenoma (BCA) is a rare tumor representing about 3 % of all tumors of the salivary glands.
Etiology and pathogenesis
BCA represents the end of a spectrum of PAs; it is usually a solitary tumor, but occasionally the membranous subtype may be multifocal and associated with dermal cylindromas and trichoepitheliomas [67].
Clinical aspects
A painless tumor mass usually clinically diagnosed as PA.
Macroscopy
Well-circumscribed nodule most often found in the parotid. Occurrence in submandibular or minor glands is rare [83, 84].
Microscopy
Four histological subtypes are recognised subtypes – solid, tubular, trabecular and membranous – but it is likely that, in reality, there are only two separate biological entities [67], non-membranous BCA (Fig. 5.19) and membranous BCA (Fig. 5.20).

Basal cell adenoma. The tumor is arranged in nests, islands and trabeculae of basal cells without cytological abnormalities. Ductal differentiation is also noted

Membranous basal cell adenoma: jigsaw-like pattern: multiple epithelial islands surrounded by large amounts of basal membrane-like material. The latter is also present within the cytoplasm of some of the small dark hyperchromatic basal cells. There is little cellular pleomorphism
Non-membranous BCAs have an equal sex incidence and arise mostly in the major glands. They probably represent part of the spectrum of myoepithelioma and PA [65, 85]. The tumors are ovoid, well-circumscribed masses in which islands, nests and trabeculae of basaloid cells are each surrounded by a distinct thin PAS-positive basement membrane. The component cells may take two forms – small with scanty cytoplasm and a round, dark nucleus and larger with amphophilic or eosinophilic cytoplasm and an ovoid paler staining nucleus. These two types are intermixed, but the smaller cells tend to be arranged around the periphery of the nests and trabeculae, giving the appearance of palisading. Ductal differentiation may or may not be apparent but can be highlighted by EMA. There is little pleomorphism and mitotic figures are rare. The stroma varies in amount and cellularity, but S-100 protein-positive spindle cells may be numerous. S-100-positive cells are also present within the islands of epithelial cells, which react strongly with cytokeratins [66].
Membranous BCA (dermal analogue tumor) occurs predominantly in men and can be multicentric. Most arise in the major glands, including within intraparotid lymph nodes [86]. Microscopically, they are not encapsulated and appear multinodular, often with a jigsaw-like pattern. The most characteristic feature is the deposition of large amounts of hyaline basement membrane material, which is brightly eosinophilic and PAS positive. It surrounds the epithelial cell islands in a similar manner to a dermal cylindroma and blood vessels and is present within the islands as small droplets. There is little pleomorphism or mitotic activity. In about 40 % of cases, the salivary adenoma is associated with synchronous and often multiple skin appendage tumors of sweat gland or hair follicle origin, usually cylindromas or eccrine spiradenomas.
Differential diagnosis
The most important differential diagnosis of all types of BCA is adenoid cystic carcinoma. Useful pointers to adenoma include lack of invasiveness and cytological pleomorphism, low mitotic and proliferative activity and whorled eddies of epithelial cells. S-100 protein positivity of spindled stromal cells may help, as this does not occur in adenoid cystic carcinoma [64]. A more difficult differential diagnosis is BCA and basal cell adenocarcinoma which may lack cytological pleomorphism and mitotic figures, the diagnosis then depending principally on the presence of genuine invasion (see Sect. 5.9.9), which it may not be possible to assess on small biopsy sample.
Treatment and prognosis
The recurrence rate for non-membranous BCA is extremely low (0 out of 102 patients in one series) [85], and local excision with clear margins is sufficient treatment. There is a low rate of malignant transformation (about 4 %) into BCA [87]. In contrast, up to 24 % of membranous BCAs recur after surgery [85] probably reflecting multicentricity, and, in addition, malignancy (also as basal cell adenocarcinoma) is said to develop in 28 % [87]. Surgery for this subtype needs to be more extensive.
5.8.4 Warthin’s Tumor
Definition
Warthin’s tumor is composed of oncocytic columnar epithelial and basal cells arranged in papillary architecture and embedded in lymphoid stroma. The term adeno- and cystadenolymphoma should be discouraged for the possible confusion with malignant lymphoid neoplasms [88].
Epidemiology
It is the second most common tumor of the salivary gland after PA. It occurs almost exclusively in the parotid gland and occasionally in peri-parotid lymph nodes.
Etiology and pathogenesis
There is a known association with smoking; radiation exposure and a history of preoperative trauma such as FNA may play a role in the development of the metaplastic subtype. It is still not certain whether Warthin’s tumor is a true neoplasm or a non-neoplastic tumor-like lesion. Honda et al. examined the clonal status of epithelial cells of Warthin’s tumor by using a PCR method based on trinucleotide repeat polymorphism of the HUMARA and on random inactivation of the gene by methylation. The pattern was non-clonal, suggesting that Warthin’s tumor is a non-neoplastic mass lesion [89].
Macroscopy
Circumscribed oval encapsulated mass. The cut surface usually shows a cystic appearance containing mucoid grey and brown fluid.
Microscopy
The combination of oncocytic epithelium arranged in papillary structures and embedded in lymphoid tissue is characteristic. The light and dark oncocytic cells, which are usually columnar in shape, lie on basal-type cells and are arranged in a palisade. There is usually no cytological atypia or mitotic activity. The stroma comprises lymphoid tissue with germinal centres (Fig. 5.21). Occasional mucinous and squamous metaplastic changes may be seen but are extensive in the metaplastic subtype [32].

Warthin’s tumor. Cystic and slitlike spaces with papillary infoldings lined with oncocytic cells. Lymphoid tissue occupies the cores of most papillae
Metaplastic subtype
This subtype variously termed infarcted, infected or metaplastic accounted for 6.2 % (20/323) of Warthin’s tumors in one series [32] and 7.5 % (21/275) in another [90]. The histopathological definition is a Warthin’s tumor in which much of the original oncocytic epithelium has been replaced by squamous cells (hence the term metaplastic) resembling a ruptured epidermoid or lymphoepithelial cyst (Fig. 5.22) [88].

Metaplastic (infarcted) Warthin’s tumor. There is extensive necrosis and inflammation
Other microscopic features include extensive necrosis, in which a ghost architecture of papillary structures may be retained. Non-keratinizing squamous metaplasia is prominent, consisting of tongues and cords of often spongiotic squamous cells extending into surrounding tissues in a pseudo-infiltrative pattern. Cytological atypia can be prominent and mitotic figures numerous, although none is abnormal. Goblet cells may also be seen, but should not be numerous. At the periphery of the lesions, there is extensive fibrosis, with dense hypocellular collagen and myofibroblastic spindle cell proliferation. There is often a heavy mixed inflammatory infiltrate, comprising neutrophils, chronic inflammatory cells, as well as sheets of macrophages, some with foamy cytoplasm. Lipogranulomas, with or without cholesterol clefts, are not uncommon [67]. The definition of metaplastic Warthin’s tumor does not encompass minor microscopic foci of inflammation, necrosis and fibrosis, as these findings can be commonly seen in any Warthin’s tumor [32]. The diagnosis is straightforward if residual tumor is present, but it will not always be so, particularly if there is complete necrosis. Several cases have been reported following FNA acting on an ordinary Warthin’s tumor to produce the infarcted subtype [34, 91]. The most likely mechanism would be direct injury of a blood vessel by the needle, as Warthin’s tumors tend to contain few blood vessels within the substance of the tumors [32]. Therefore, they could be at risk of a needle harming a limited number of feeder arteries. Another possible important factor is cell type; in the well-documented injuries from FNA in other organs, tumors rich in oncocytic cells, such as Hürthle cell adenoma of the thyroid, feature prominently. Not surprisingly, similar infarction has been reported in salivary oncocytoma [92].
Differential diagnosis
The characteristic appearance means that Warthin’s tumor is generally the easiest salivary tumor to diagnose by microscopy [32], although difficulty may arise with the metaplastic subtype, particularly when there is total necrosis of the original tumor.
Treatment and prognosis
Most cases are treated with surgery. For example, with a definite cytological diagnosis, the treatment may be conservative. Malignancy occurs in fewer than 1 % of cases, involving either epithelial or lymphoid elements leading to carcinoma or lymphoma.
5.8.5 Oncocytoma
Definition
A tumor composed of oncocytic cells only, with no features of another neoplasm such as a PA.
Epidemiology
Oncocytoma accounts for approximately 1 % of salivary gland tumors and may be associated with MNOH (see Sect. 5.6.3) [69]. The mean age is 60 years; it occurs in both sexes with a slight male predominance (67 %) [93]. Parotid is the preferred site with both glands involved in cases associated with bilateral MNOH [94].
Etiology and pathogenesis
Some patients with oncocytic tumors have a history of previous radiation exposure.
Clinical aspects
Most commonly a painless mass.
Macroscopy
They are encapsulated tumors 5–30 mm.
Microscopy
Usually solid, composed of oncocytic cells with characteristic ‘light and dark’ cytoplasm arranged in sheets and duct-like and trabecular structures (Fig. 5.23). The tumor can be composed entirely of clear cells [95] or have the features of an oncocytic lipoadenoma (Figs. 5.24, 5.25 and 5.26) for the presence of variable amount of fatty tissue [96].

Oncocytoma. Light and dark oncocytic cells are arranged in a solid, trabecular and tubular configuration

Oncocytic lipoadenoma: the tumor is encapsulated and has a tan cut surface (Courtesy of Dr. Abbas Agaimy)

Oncocytic lipoadenoma. The tumor is formed by mature fatty tissue and oncocytic cells (Courtesy of Dr. Abbas Agaimy)

Oncocytic lipoadenoma. The lesion is formed by of adipose tissue and oncocytic cells with eosinophilic granular cytoplasm (Courtesy of Dr. Abbas Agaimy)
Differential diagnosis
The granular cytoplasm is PAS diastase (PASD) negative, unlike in acinic cell carcinoma. Oncocytomas composed of clear cells must be distinguished from renal cell carcinoma and other clear cell tumors. p63 immunostaining has been used to differentiate oncocytoma (and oncocytic carcinoma) from metastatic renal cell carcinoma [97].
Treatment and prognosis
With surgery, the prognosis is good. Recurrences occur when oncocytoma is associated with MNOH (see Sect. 5.6.2).
5.8.5.1 Striated Duct Adenoma
Definition
Striated duct adenomas (SDA) are ductal tumors that recapitulate normal striated ducts, which are lined by only a single layer of epithelial cells with absent (or at most, very occasional) basal or myoepithelial cells.
Epidemiology
SDA is rare with only six cases reported so far, four in the parotid gland and two in the palate [98].
Etiology and pathogenesis
Not known.
Clinical aspects
Patients complain of painless tumor mass in the parotid gland or palate.
Macroscopy
An encapsulated circumscribed mass.
Microscopy
Composed of back-to-back ducts with virtually no stroma. The ducts vary in size with some showing cystic dilatation, up to 1 mm in diameter. The cells are eosinophilic and bland, and prominent cell membranes reminiscent of ‘striations’ of normal striated ducts are characteristic. All tumors express keratins, and S-100 positivity is present in most. Occasional tumors show focal bilayered ducts with calponin or SMMHC, but in general SDAs are unilayered. Only isolated cells in some tumors are positive with p63 – a pattern identical to normal striated ducts, in contrast to normal excretory and intercalated ducts which demonstrate diffuse bilayering with basal (p63 positive) or myoepithelial (SMA, calponin, SMMHC +) cells, respectively [98].
Treatment and prognosis
SDA is part of the spectrum of benign salivary adenomas, and complete excision should be curative.
5.8.6 Canalicular Adenoma
Definition
A tumor composed of basal-type epithelial cells embedded in oedematous and highly vascular stroma.
Epidemiology
Canalicular adenoma accounts for 1 % of salivary gland tumors almost exclusively intraoral, particularly affecting the upper lip [67] and less often the palate [99].
Clinical aspects
Most tumors present when they are small, rarely more than 20 mm in diameter.
Macroscopy
Soft and well-circumscribed nodule with pale cut surface.
Microscopy
It has a characteristic morphology of branching and interconnecting bilayered strands of darkly staining epithelial cells set in a loose vascular stroma (Fig. 5.27). There is no pleomorphism or significant mitotic activity. The cells express cytokeratins and S-100 protein [100]. Not infrequently, they are bilateral [101] or multifocal [102] and can thus mimic invasion.

Canalicular adenoma of the upper lip. It is composed of bilayered strands of basal-like cells embedded in a loose oedematous stroma
Differential diagnosis
Multifocal canalicular adenoma needs to be distinguished from cribriform adenoid cystic carcinoma. The lack of destructiveness, cytological atypia and low mitotic and proliferative activity together with the presence of oedema and blood vessels in the cribriform spaces are good guides to canalicular adenoma, which is completely benign.
Treatment and prognosis
The tumor is benign, but occasional recurrences can occur as a result of multifocality [102].
5.8.7 Sebaceous Adenoma
Definition
Tumors composed of nests of sebaceous cells mixed with metaplastic squamous cells and cysts [103].
Epidemiology
It represents <1 % of salivary gland tumors with a predilection for the parotid gland, buccal mucosa and retromolar trigone [103].
Clinical aspects
Painless tumor mass with long duration of symptoms.
Macroscopy
Well-circumscribed nodule with a median size of 20 mm.
Microscopy
Histologically there is a mixture of sebaceous and squamous cells without cytological atypia. Fibrosis and foreign body-type giant cells are also noted [103].
Differential diagnosis
In small biopsies the presence of squamous cell in a sebaceous adenoma can be mistaken for squamous cell carcinoma.
Treatment and prognosis
They do not recur after complete surgical excision.
5.8.8 Sebaceous Lymphadenoma
Definition
Tumor composed of sebaceous glands mixed with lymphoid stroma and epithelial cells of various types (squamous, mucinous, ductal and basal types) [103].
Epidemiology
Sebaceous lymphadenoma is rare. In the largest series of sebaceous and non-sebaceous lymphadenoma, it comprised <1 % of parotid tumors. It occurs mainly in older adults [103, 104], but children can occasionally be affected [105].
Etiology and pathogenesis
Altered immune system may be a predisposing factor. EBV, HPV and HHV-8 do not seem to play any role. It is possible that, like Warthin’s tumor, sebaceous lymphadenoma develops from salivary inclusions within lymph nodes and shows sebaceous rather than oncocytic metaplasia [103, 104].
Clinical aspects
Patients complain of a painless mass in the parotid gland, rarely in the neck.
Macroscopy
A well-circumscribed and encapsulated tumor with multicystic cut surface.
Microscopy
This lesion comprises irregularly proliferating nests of epithelium. Oncocytic papillary changes, mucus-secreting cells and keratinization can be seen. The cysts contain eosinophilic and sebaceous-like material. The sebaceous cells are seen inside a layer of basal cells. The tubules and glands have an outer layer of basal cells and an inner layer of luminal glandular cells. The lymphoid infiltrate has a mixed population of B and T lymphocytes, with some germinal centre formation (Fig. 5.28).

Sebaceous adenoma composed of a mixture of sebaceous and squamous cells without cytological atypia
A foreign body reaction to keratin and fat material complicated 11/22 cases in one study [104].
Differential diagnosis
The most important differential diagnosis is with nodal metastases of squamous cell carcinoma, and this can be particularly difficult in preoperative core biopsies performed on neck or intraparotid nodes. The lack of atypia and mitoses favour lymphadenoma. Mucoepidermoid carcinoma is excluded by the absence in lymphadenoma of mucous and intermediate cells together with the presence of sebaceous cells.
Benign conditions such as lymphoepithelial cysts and lymphoepithelial sialadenitis (see Sect. 5.10.1) also lack the prominent sebaceous component.
Treatment and prognosis
These are benign tumors which are cured with surgical excision.
5.8.9 Ductal Papilloma
Definition
An adenoma arising mainly in the excretory duct [106]. Ductal papilloma has a fibrovascular core lined with myoepithelial and ductal cells, and it is usually seen in a dilated duct.
There are three subtypes, all rare, inverted ductal papilloma (similar to analogous sinonasal Schneiderian tumors), intraductal papilloma and sialadenoma papilliferum (similar to skin syringocystadenoma papilliferum [106]. Their main characteristic is described below.
5.8.9.1 Inverted Ductal Papilloma
Rare examples have been reported in the minor salivary glands of the palate, floor of mouth, buccal mucosa and lower lip [106]. Histologically, the squamous epithelium shows a nodular proliferation not surrounded by a capsule. The papillary islands comprise a mixture of squamous and basal cells covered by columnar cells, together with single or small groups of mucus-secreting cells.
The most important differential diagnosis is with mucoepidermoid carcinoma (see Sect. 5.9.3) especially in small-sized biopsies.
5.8.9.2 Intraductal Papilloma
This papillary-cystic tumor arises in an excretory or interlobular duct of a salivary gland. With the exception of scattered cases reported in parotid, submandibular and sublingual glands, intraoral minor salivary glands are most affected [106].
Histology shows a dilated duct containing a papillary growth. The papillae comprise fibrovascular cores lined with myoepithelial and ductal cells without cytological atypia or mitotic activity.
5.8.9.3 Sialadenoma Papilliferum
This is an exophytic papillary lesion associated with an endophytic proliferation of squamous or ductal epithelium from the mucosal surface and excretory salivary duct. It is histologically identical to syringocystadenoma of the skin. It arises in minor salivary glands of the palate, buccal mucosa, upper lip, retromolar area and exceptionally in the parotid [106].
5.8.10 Cystadenoma
Definition
Cystadenoma is a rare, benign neoplasm composed of one or usually more cystic spaces often with intraluminal papillary projections. The epithelial lining may be oncocytic, apocrine, epidermoid and mucous. Cystadenoma occurs in two major variants, as papillary oncocytic type and mucous cell type [67].
Epidemiology
The frequency of cystadenoma is between 0.7 and 8.1 % of all benign salivary tumors, but it is probably underestimated, as some examples are classified as ‘monomorphic adenomas’ [67]. The average age is about 50 years of age (range 8–89). Cystadenomas occur more frequently in females, with a female-to-male ratio 3:1. Most are located in major glands with almost 58 % arising in parotid and 7 % in submandibular gland. Cystadenoma of minor glands affect mostly the lip and buccal mucosa.
Macroscopy
Cut section reveals multiple small cystic spaces of variable sizes with intraluminal proliferations. The tumors are well circumscribed and encapsulated.
Microscopy
Most cystadenomas are multilocular with individual cystic spaces separated by limited amounts of intervening stroma [107]. The lumina often contain eosinophilic material with scattered epithelial, foamy or inflammatory cells. Rarely, psammoma bodies and crystalloids have been described within the luminal secretion [108]. The lining epithelium of the cystic spaces is mostly columnar and cuboidal. Oncocytic, mucous and apocrine cells are sometimes present focally or may predominate. An oncocytic variant of papillary cystadenoma is composed of oncocytes present in unilayered or bilayered papillary structures (Fig. 5.29). Squamous epithelium may be present but rarely predominates. Mucinous cystadenoma is composed of multiple cystic spaces lined by mucus-secreting columnar cells without atypia (Fig. 5.30).

Oncocytic (papillary) cystadenoma of the larynx. Cystically dilated ducts are lined with oncocytic cells

Mucinous cystadenoma. Cysts are lined with mucus-secreting cells without atypia
Differential diagnosis
Differential diagnosis consists of simple cyst, duct ectasia, polycystic dysgenetic disease, intraductal papilloma, low-grade mucoepidermoid carcinoma and striated duct adenoma [98]. Both duct ectasia and simple cysts have simple epithelial lining without papillary intraluminal projections. In addition, duct ectasia, in contrast to cystadenoma, is often associated with fibrosis and chronic inflammatory infiltration. Polycystic dysgenetic disease is extremely rare and involves the whole gland [43]. Intraductal papilloma has overlapping histological features with papillary cystadenoma; however, intraductal papilloma is a unicystic lesion with prominent intracystic papillary proliferation, whilst cystadenomas are multicystic tumors [77]. Low-grade mucoepidermoid carcinoma shares some histological features with the mucous cell variant of cystadenoma, but solid islands composed of intermediate cells are characteristic of mucoepidermoid carcinoma. Furthermore, cystadenoma is well circumscribed without invasive growth. Striated duct adenoma is composed mostly of closely packed unilayered ducts without a myoepithelial layer and with minimal intervening stroma and variable cystic ductal spaces [98]. In contrast, cystic formations dominate the picture in cystadenoma.
Treatment and prognosis
Cystadenomas are benign tumors; complete surgical excision is curative. The tumors are unlikely to recur, but rare cases of mucinous cystadenomas with malignant transformation have been reported (Fig. 5.31) [109].

Mucinous cystadenoma with malignant transformation. Cellular pleomorphism and signet ring cell appearance
5.9 Malignant Epithelial Tumors
5.9.1 Acinic Cell Carcinoma
Definition
Acinic cell carcinoma (AciCC) is defined as a malignant epithelial neoplasm in which at least some of the neoplastic cells demonstrate serous acinar cell differentiation [67].
Epidemiology
AciCC accounts for about 2–4 % of salivary gland tumors and approximately 5 % of malignancies; AciCC is the second most common salivary gland carcinoma occurring in childhood [77]. The reported age range is 3–91 years, with female-to-male predilection of approximately 2:1 [77]. The mean age at presentation is 38–46 years. The parotid is involved in at least 92 % of cases (3 % bilateral), with only occasional examples in the submandibular or minor glands [77].
Clinical aspects
The typical clinical history is of a slowly enlarging mass (for as long as 40 years), but occasionally patients present with pain and facial nerve weakness.
Macroscopy
Most tumors are partly circumscribed, with an average diameter of 1–3 cm, although larger tumors can be encountered.
Microscopy
By definition, AciCC is characterised by the presence of well-differentiated serous acinar cells with abundant cytoplasmic PAS-positive zymogen granules, resistant to diastase digestion (Fig. 5.32). However, several other cell types, such as intercalated ductal, vacuolated, clear and non-specific glandular cells are recognised. Solid/lobular and microcytic growth patterns are most commonly seen in AciCC, but macrocytic, follicular (thyroid gland-like) (Fig. 5.33), papillary-cystic patterns are also recognised (Fig. 5.34). The most useful special stain in AciCC is PASD which highlights cytoplasmic zymogen granules (Fig. 5.35). With one possible exception, the immunoprofile is not specific – positivity is seen with cytokeratin, amylase and CEA, but mammaglobin and myoepithelial markers are negative. Up to now, immunohistochemistry has been considered of limited diagnostic value, but a new potentially useful marker, DOG1, shows intense apical membranous staining around lumina as well as complete membranous and variable cytoplasmic staining in AciCC (Fig. 5.36) [110].

Acinic cell carcinoma solid variant. The cells show granular cytoplasm and acinar differentiation similar to normal salivary gland acini

Follicular variant of acinic cell carcinoma: the tumor is composed of follicle-like spaces of varying sizes lined with cuboidal intercalated duct-type cells

Acinic cell carcinoma, papillary subtype: papillae are lined with intercalated duct-like cells, some containing microvesicles, others showing a hobnail/clear cell appearance

Acinic cell carcinoma. Periodic acid-Schiff with diastase staining emphasises coarse zymogen granules in the cytoplasm of the tumor cells

Acinic cell carcinoma: DOG1 antibody shows an intense apical membranous staining around lumina as well as complete membranous and variable cytoplasmic staining
Differential diagnosis
The differential diagnosis depends on the subtype: solid variant, composed of prevalent serous cells, resembles normal parotid acini, but with an abnormal architecture. The papillary-cystic type bears a close similarity to the controversial entity cystadenocarcinoma. A follicular pattern suggests metastatic thyroid carcinoma but is thyroglobulin negative. The clear cell variant must be differentiated from other neoplasms composed of clear cells, but there are always some cells with PASD-positive granules in AciCC. The most common tumor entity in salivary gland pathology that mimics AciCC is a recently recognised new tumor entity, mammary analogue secretory carcinoma [111] (see Sect. 5.9.2). The neoplastic cells of mammary analogue secretory carcinoma resemble intercalated duct cells, but serous acinar cells with cytoplasmic PAS-positive granules typical of AciCC are completely absent in mammary analogue secretory carcinoma. In contrast to mammary analogue secretory carcinoma, AciCC shows an intact ETV6 gene and is mammaglobin and (usually) S-100 protein negative, as well as positive with DOG1.
Treatment and prognosis
AciCC is characterised by a protracted clinical course, but it is a genuine malignancy capable of killing the patient. Reported rates of recurrence, distant metastasis and mortality with treatment are 30 %, 13 % and 13 %, respectively [77]. Prediction of prognosis of AciCC based on grading is uncertain, although there are two studies demonstrating that Ki-67 (MIB1) is an independent prognostic indicator [112, 113]. Skálová et al. found that tumors with a proliferation MIB1 index <5 % were cured by complete excision, whereas more than half of AciCCs with indices above this either recurred or metastasised [113]. Clinical stage also gives the most prognostic information [77]. High-grade (HG) transformation of AciCCs (Fig. 5.37) has been reported; these tumors are aggressive with rapid progression and a poor outcome [114]. In contrast, Michal and colleagues have reported a well-differentiated variant that is surrounded completely by heavy lymphoid stroma which has a better prognosis than conventional AciCC [115]. Overall, the most effective treatment for AciCCs is complete surgical excision. Radiation may have a role in treatment of patient with HG-transformed AciCC [114].

Acinic cell carcinoma with high-grade transformation
5.9.2 Mammary Analogue Secretory Carcinoma
Definition
Mammary analogue secretory carcinoma (MASC) is a recently described distinctive salivary gland tumor with the ETV6 gene rearrangement [111]. As the name implies, MASC is characterised by histological and immunohistochemical resemblance to secretory carcinoma of the breast [116]. Moreover, MASC of salivary glands, like secretory carcinoma of the breast, harbours a recurrent balanced chromosomal translocation t(12;15) (p13;q25) which leads to a fusion gene between the ETV6 gene on chromosome 12 and the NTRK3 gene on chromosome 15 [111, 116].
Epidemiology
The exact incidence of this recently described entity is not yet known, but it occurs frequently enough to be encountered regularly in routine diagnostic practice, and it is most probably much more common than originally realised [117, 118]. Oddly, its incidence is much higher than its breast equivalent.
Clinical aspects
In contrast to AciCC, MASC has a slight male predilection [111, 119]. The parotid is the usual site, but it is also found in extra-parotid sites, much more commonly than AciCC [111, 117, 119].
Macroscopy
Grossly, the tumors are rubbery, with a white-tan to grey cut surface. Occasionally, on cut surface the tumors may appear cystic, containing yellow-whitish fluid. The borders of the tumors are usually circumscribed but not encapsulated (Fig. 5.38), and invasion within the salivary gland is often present.

Mammary analogue secretory carcinoma. The borders of the tumors are usually circumscribed but not encapsulated
Microscopy
MASC often has a lobulated growth pattern divided by fibrous septa (Fig. 5.39). In most cases, MASC is composed of microcystic/solid and tubular structures with abundant eosinophilic homogeneous or bubbly secretory material (Fig. 5.40). Less commonly, the tumors are dominated by one large cyst with multilayered lining, which can display tubular, follicular, macro- and microcystic or papillary architecture, with occasional solid areas (Fig. 5.41). The tumor cells have low-grade vesicular round-to-oval nuclei with finely granular chromatin and distinctive centrally located nucleoli (Fig. 5.42). The cytoplasm is pale to pink with a granular or vacuolated appearance. Cellular atypia is usually mild, and mitotic figures are in most cases sparse. Perineural invasion can be sometimes present, but the tumors usually do not have evidence of lymphovascular invasion. Necrosis is typically not identified. Abundant bubbly secretion is present within microcystic and tubular spaces (Fig. 5.43). This secretory material stains positive for PAS before and after diastase digestion and for mucicarmine and Alcian blue (Fig. 5.44). In contrast to AciCC, serous acinar differentiation is not a feature of MASC, and the cells of MASC are devoid of PAS-positive secretory zymogen cytoplasmic granules. The immunohistochemical profile of MASCs shows diffuse and strong expression of cytokeratins (AE1/AE3 and CAM 5.2), CK7, CK8, CK18, CK19, epithelial membrane antigen (EMA), S-100 protein and vimentin. The tumor cells also show strong positive expression of STAT5a (signal transducer and activator of transcription 5a) and mammaglobin (secretory material is also positive) in all cases. In addition, in most cases, there is significant positivity for gross cystic disease fluid protein 15 (GCDFP-15) (particularly secretory material is stained) and EMA. Basal cell/myoepithelial cell markers, such as p63, calponin, CK14, αSMA and CK5/6, are virtually negative as described in original report [111]; however, we have recently identified few cases of MASC, which showed focal expression of high-molecular-weight keratin (34betaE12) and p63 protein-positive cells [118, 120]. Most cases of MASC are DOG1 negative, whilst AciCCs demonstrate intense apical membranous staining around lumina and variable cytoplasmic positivity in most cases [110]. At the molecular level, MASC harbours a distinctive t(12;15) (p13;q25) translocation resulting in ETV6-NTRK3 fusion product. This defines the entity, as it has not been demonstrated in any other salivary gland tumor type [111].

Mammary analogue secretory carcinoma. The tumor often has a lobulated growth pattern divided by fibrous septa, and it is composed of microcystic/solid and tubular structures

Mammary analogue secretory carcinoma with abundant eosinophilic homogeneous or bubbly secretory material.

Less commonly, mammary analogue secretory carcinoma is formed by one large cyst with multilayered lining

Mammary analogue secretory carcinoma. The tumor cells have low-grade vesicular round-to-oval nuclei with finely granular chromatin and distinctive centrally located nucleoli

Mammary analogue secretory carcinoma. Abundant bubbly secretion is present within microcystic and tubular spaces

Mammary analogue secretory carcinoma. Secretory material stains positive for periodic acid-Schiff
Differential diagnosis
The most common salivary tumor entity that mimics MASC is AciCC (AciCC) (see Sect. 5.9.1). Classic AciCC is readily distinguishable from MASC even at the morphological level. In contrast, zymogen granule poor AciCC shows considerable overlap with MASC, and in one series more than half of such cases diagnosed morphologically turned out to be MASC when examined by FISH for ETV6 gene rearrangements [111, 119]. In general, AciCC is characterised by cytological and structural diversity, being composed of a mixture of serous acinar, intercalated duct-like, hobnail, vacuolated, clear and non-specific glandular cells arranged in solid/lobular, microcystic, papillary-cystic and follicular growth patterns. In contrast, MASCs are structurally homogenous, uniformly composed of microcystic and slightly dilated glandular spaces with secretory material in lumina. The major differential diagnostic feature of MASC is the absence of acinar cells. Furthermore, MASCs display a characteristic immunohistochemical profile (S-100 protein+, mammaglobin+, vimentin+ and DOG1 absent), largely different from AciCC. Definitive separation of these entities is by the demonstration of the ETV6-NTRK3 translocation by FISH which is diagnostic of MASC and absent in AciCC.
Adenocarcinoma, not otherwise specified (NOS), is a poorly defined category of otherwise unclassifiable salivary gland carcinomas, and it usually represents a diagnosis of exclusion. Description of the MASC with a diagnostic ETV6-NTRK3 translocation allows reclassification of some cases of adenocarcinomas NOS as MASC.
Low-grade cribriform cystadenocarcinoma (see Sect. 5.9.11.1) must be considered in the differential diagnosis of MASC as well. Although it shares with MASC strong diffuse S-100 protein expression, low-grade cribriform cystadenocarcinoma possesses a complete intact myoepithelial rim around tumor nests, unlike MASC. However, ductal involvement consisting of a morphologically apparent connection of tumor to medium-sized ducts in the major salivary glands and/or immunohistochemical evidence (p63) of a basal layer surrounding a portion of the tumor nests or cysts was noted in several cases of MASC [118, 120].
The immunohistochemical demonstration of high-molecular-weight cytokeratins (HMWK) and focal mucinous differentiation of MASC raises a differential diagnosis with mucoepidermoid carcinoma [118, 121]. The distinction can be made by the lack of a cobblestone-like appearance with intercellular bridges, true squamoid areas or basal-like intermediate cells in mucoepidermoid carcinoma. In addition, MASC typically lacks p63 staining and shows diffuse S-100 positivity in most cases, which would be distinctly unusual in mucoepidermoid carcinoma, as would papillary formations and hobnailing in the lining of the cysts. The positivity for HMWK in MASC is also less intense than is typically seen in MEC in our experience. Moreover, more than 50 % of mucoepidermoid carcinomas are characterised by a t(11;19) translocation coding for a CRTC1-MAML2 fusion protein (see Sect. 5.9.3). This is distinct from the t(12;15) translocation encoding ETV6-NTRK3 of MASC.
Treatment and prognosis
Generally, the clinical course of conventional MASC is characterised by a moderate risk of local recurrence (15 %) and lymph node metastases (20 %) and low risk of distant metastases (5 %) [111, 119]. Clinical stage at the time of diagnosis is the most powerful predictor of prognosis. Based on few cases with follow-up data, MASC is currently regarded as a low-grade carcinoma, and its prognosis seems to be favourable overall [111, 117, 119]. However, compared to AciCC, MASC has a slightly higher risk of regional lymph node involvement [119]. Distant metastatic dissemination and tumor-related deaths were reported in three patients so far [111, 119]. Clinical stage at the time of diagnosis is the most powerful predictor of prognosis [119].
Recently, a few cases of HG transformation in MASC have been reported (Fig. 5.45). This is a much more aggressive neoplasm that follows an accelerated clinical course resulting in local recurrences, cancer dissemination and death of all three of our patients reported so far [122]. In view of the aggressive nature of HG-transformed MASC, radical surgery and adjuvant radiotherapy are recommended. Unlike conventional MASC, HG-transformed MASC seems to have a high propensity for cervical lymph node metastases suggesting the need for neck dissection in the management of such patients [122].

High-grade transformation of mammary analogue secretory carcinoma
5.9.3 Mucoepidermoid Carcinoma
Definition
Mucoepidermoid carcinoma (MEC) is a malignant tumor showing mucous, squamous and intermediate cell differentiation.
Epidemiology
MEC demonstrates a wide age distribution with a mean of 45 years. It is the most frequent malignant salivary gland tumor in most series [48]. It is also the commonest salivary malignancy in childhood and can be seen even in small children [123]. There is a slight female predominance (3:2). MEC occurs in major and minor glands with roughly equal frequency. In minor glands, MEC is seen most often in the palate, but it may arise in any location. Rarely, it is seen in intra-bony locations in the mandible and the maxilla as the most frequent central salivary gland tumor.
Etiology and pathogenesis
The most common aetiologic factor associated with MEC is radiation, and MEC is the most frequent salivary malignancy arising in survivors of childhood cancers treated with radiotherapy. A majority of MECs harbour a balanced translocation t(11;19)(q21;p12-13) and a corresponding fusion gene CRTC1-MAML2 with alterations in cAMP and Notch signalling pathways suggesting pathogenetic significance for the fusion [124]. Correlating the occurrence of CRTC1-MAML2 fusion, patterns of genomic changes and follow-up information of MEC cases, tumors negative for CRTC1-MAML2 fusion appear to represent adenocarcinomas other than MEC [121, 125]. Occurrence of rarer fusions such as CRTC3-MAML2 and EWSR1-POU5F1 has been reported in minor subsets of MEC [124].
Clinical aspects
A slowly growing tumor mass is the most common presentation.
Macroscopy
A cystic and solid tumor which can be circumscribed and mimic a benign tumor.
Microscopy
MEC is composed of varying proportions of mucous (mucus-secreting) cells, epidermoid cells, clear cells and cells of intermediate differentiation. The proportion of the different cell types and their architectural configuration (including cyst formation) vary between tumors of differing grades (Fig. 5.46). Mucous cells tend to be more numerous in MECs with cyst formation. Mucous cells are cuboidal, columnar or goblet-like and may form solid proliferations or lining of cysts in single or multiple layers. Their cytoplasm is foamy or reticular and variably basophilic. Cytoplasmic mucins stain with Alcian blue and mucicarmine, which are particularly useful if there are only a few mucous cells. Epidermoid cells have large eosinophilic cytoplasm and may have intercellular bridges, but it should be noted that the term epidermoid only indicates squamous-like appearance and not necessarily squamous differentiation. Intracellular keratinization or extracellular keratin pearls are very rare in MEC, and they are much more frequent in squamous metaplasia in connection with PA or in a metastatic squamous cell carcinoma from the skin or upper aerodigestive tract. Whilst epidermoid cells may be sparse in MEC, they can be identified using immunohistochemical stains for p63 and high-molecular-weight cytokeratins. Intermediate cells are small basal-like cells with dark-staining nuclei, and they often form the lining of cysts beneath the mucous cells. Clear cells representing clear cell change in squamous or intermediate cells may be frequent in MEC.

Mucoepidermoid carcinoma: the tumor is formed by epidermoid, intermediate and mucin-producing cells
Occasionally MEC may mimic a clear cell carcinoma [80]. Sometimes, MEC may also have extensive oncocytic change involving most of the tumor [126]. A rare sclerosing variant of MEC is associated with increased numbers of IgG4 plasma cells and increased fibrosis, but there is no relationship to systemic IgG4-related sclerosing disease [127].
MECs are histologically classified as low-, intermediate- and high-grade malignancies. All MECs are regarded as malignant although only rare cases of low-grade MEC will metastasise. Low-grade MECs typically have a prominent cystic component lined by mucous cells juxtaposed to intermediate and epidermoid cells (Fig. 5.47). Nuclear atypia and mitotic activity are not usually features of low-grade MEC.

Low-grade mucoepidermoid carcinoma: typical cystic and solid pattern
Intermediate-grade MECs are less cystic with higher frequency of solid nests of squamous and intermediate cells. A minor degree of nuclear atypia and mitotic activity may be present. High-grade tumors are predominantly solid and infiltrative and show nuclear atypia (Fig. 5.47). They may resemble squamous cell carcinomas with a minor mucous component. Grading of MEC is subjective, and no universally accepted grading system exists yet. However, histological features including extent of the cystic component, mitotic activity, neural invasion, tumor necrosis and cytological pleomorphism have been widely used. Additional features including vascular/lymphatic invasion, bony invasion and invasion of tumor front in small nests have been combined to increase prognostic accuracy [128]. Assessment of MIB1 cell proliferation index has also been shown to be of value [129] (Fig. 5.48).

High-grade mucoepidermoid carcinoma: epidermoid cells arranged in a solid pattern also show nuclear pleomorphism. Mucus-secreting cells may be scarce
Differential diagnosis
Squamous cell carcinoma, clear cell carcinoma and mucous secreting lesions are the main differentials. Occasionally MEC may mimic a clear cell carcinoma [80]. Sometimes, MEC may also have extensive oncocytic change involving most of the tumor [126].
Treatment and prognosis
The treatment is surgical. Grading assessment of MEC has considerable prognostic significance, with death rates due to disease of 3.3, 9.7 and 46.3 % for low-grade, intermediate-grade and high-grade cases, respectively [130].
5.9.4 Adenoid Cystic Carcinoma
Definition
Adenoid cystic carcinoma (AdCC) is a malignant tumor composed of a dual population of basal/myoepithelial and luminal cells.
Epidemiology
Approximately 10 % of malignant tumors of salivary glands are AdCC. It can occur in any gland, but most often in the submandibular or minor salivary glands, particularly the palate. Other non-salivary anatomic sites include the breast, skin, tracheobronchial, sinonasal and female genital tract [67].
Clinical aspects
It presents itself as a slow growing but aggressive tumor mass often resulting in multiple local recurrences and metastases.
Macroscopy
Generally it is a solid tumor with hyalinised areas which may be extensive. Margins are usually ill defined, but rarely it can be partly circumscribed.
Microscopy
The cellular component is arranged in three main growth patterns:
-
Cribriform: This is the most characteristic microscopic feature, dominated by multiple cribriform structures, composed of epithelial and basal/myoepithelial cells. The nuclei are usually dark, hyperchromatic and angulated. Mitotic figures are easy to find and may be abundant. The contents of the spaces can be loose and basophilic or dense and eosinophilic (Figs. 5.49 and 5.50).
Fig. 5.49 
Adenoid cystic carcinoma, cribriform variant: multiple cribriform spaces composed of basaloid cells, with hyalinised material surrounded by small hyperchromatic cells
Fig. 5.50 
Adenoid cystic carcinoma, cribriform variant. Extensive hyalinisation with compression of tumor cells. Nuclear pleomorphism may be difficult to appreciate, leading to a false diagnosis of pleomorphic adenoma
-
Tubular: This is composed of small tubules lined with one or two cell types, luminal and abluminal without significant cytological atypia. Because of this bland cytological appearance with well-differentiated tubules, it may be difficult to diagnose on small biopsies, but it poses no problems in surgical specimens due to the presence of infiltration.
-
Solid (basaloid): This is dominated by large solid sheets of tumor cells, sometimes with comedo-like central necrosis (Fig. 5.51). Within the solid masses of tumor cells, there are small duct-like spaces surrounded by a definite layer of epithelial cells (Fig. 5.52).
Fig. 5.51 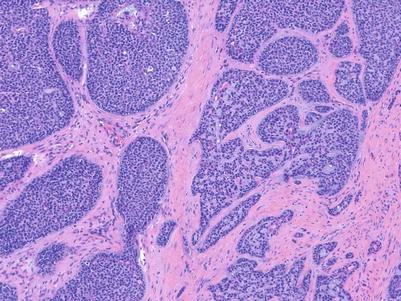
Adenoid cystic carcinoma, solid variant. This is composed of multiple solid nodules; some might display central comedo-like necrosis
Fig. 5.52 
Adenoid cystic carcinoma, solid variant. Tumor islands contain small ducts lined with a layer of epithelial cells. In the absence of characteristic cribriform structures, the latter feature is diagnostic




A rare finding in all types of AdCC is squamous metaplasia, either as single cells or with keratin pearl formation. Another uncommon phenomenon is the presence of signet ring cell changes in AdCC of salivary glands. This is not due to the presence of mucous substance in the signet ring cells as no mucous is shown by PAS staining (Fig. 5.53) [131].

Adenoid cystic carcinoma. Signet ring cell morphology can rarely be identified (Courtesy of Dr. Albina Altemani)
On immunohistochemistry AdCC can display considerable variability in staining for epithelial and myoepithelial markers. Reactivity for broad-spectrum keratins (AE1/AE3, CAM5.2) and myoepithelial markers αSMA, p63 protein, CD10, GFAP, calponin and SMMHC is helpful for the diagnosis. In particular, the presence of p63 positivity in the peripheral rim of tumor islands is helpful. S-100 protein staining is usually weak or patchy. The MIB1 proliferation index almost always exceeds 10 % [132]. AdCC has been reported to show expression of the proto-oncogene and therapeutic target c-KIT [133], but this finding has been questioned by other researchers who have not been able to demonstrate activating KIT mutations in AdCC of various anatomical sites [134].
On the other hand, AdCCs regardless of the anatomical site are characterised by similar molecular features. The majority harbour a specific chromosomal translocation t(6;9) leading to the fusion gene MYB-NFIB and overexpression of the oncogene MYB [135] which can be a diagnostically useful biomarker for primary and metastatic AdCC [136].
Differential diagnosis
The histological features of AdCC are well known, and the cribriform pattern is easily recognised by most pathologists. However, the tubular and cribriform patterns may be confused with other benign and less aggressive tumors of salivary glands such as PA/BCAc, canalicular adenoma and polymorphous low-grade adenocarcinoma. PA may contain adenoid cystic-like areas, but myxochondroid matrix and plasmacytoid or spindle-shaped myoepithelial cells are usually present [137]. Differentiation is mainly on H&E, but immunohistochemistry for MIB1 which is <5 % in PA/BCA has some value [138].
The most important histological differential diagnosis is between AdCC and polymorphous low-grade adenocarcinoma (see Sect. 5.9.5). Both are diffusely infiltrating neoplasms displaying morphological diversity but can be distinguished cytologically: the former typically have closely packed dark, angular, atypical nuclei and frequent mitotic figures, in contrast to the uniform bland nuclei of the latter. There are also some immunohistochemical guides but no absolute discriminants, e.g. S-100 staining is usually more diffuse and stronger in polymorphous low-grade adenocarcinoma, and p63 typically reacts with cells at the periphery of the islands in AdCC. This latter finding distinguishes solid variant AdCC from the relatively low-grade basal cell adenocarcinoma and with the aggressive basaloid squamous cell carcinoma, which, in addition, often shows intraepithelial dysplastic changes. CD117 is of uncertain significance and diagnostic usefulness [134].
Treatment and prognosis
The average 5- and 10-year survival rates are about 60 % and 40 %, respectively, but most patients eventually die of disease. The main prognostic factors are site (e.g. submandibular worse than parotid), histological pattern including HG transformation, perineural infiltration, resection margins and clinical TNM stage. A system of three grades based on the presence of tubular, cribriform and solid pattern [139] has shown that outcome is better in tubular AdCC, whilst the worst prognosis is seen when the solid component exceeds 30–50 % of the tumor. Rarely AdCC can undergo high-grade transformation (also referred to as dedifferentiation) characterised by nuclear enlargement and irregularity, higher mitotic counts and the loss of the biphasic ductal-myoepithelial differentiation AdCC with HG transformation that tends to be more advanced at presentation [140]. The pathological stage for this histologic subtype however is prognostically and therapeutically relevant [141]. Another unfavourable feature of AdCC is the frequent involvement of resection margins in the surgical specimen, particularly as the result of extensive perineural infiltration. As complete excision of AdCC is difficult, patients often require postoperative radiotherapy [142].
Nevertheless, clinical stage appears to be a better predictor than grade [141]. Unlike other salivary gland malignancies, when AdCC metastasises, it tends to involve distant organs such as the lung, bone, liver and more rarely the skin rather than local lymph nodes [136].
Interestingly the clinical behaviour of salivary gland and breast AdCC differs significantly; whereas salivary gland AdCC have a high proclivity to recur locally and metastasise, patients with breast AdCCs have an excellent outcome [133].
5.9.5 Polymorphous Low-Grade Adenocarcinoma
Definition
Polymorphous low-grade adenocarcinoma (PLGA) is an infiltrating tumor with cytological uniformity and architectural diversity [67]. Previously called terminal duct or lobular carcinoma, PLGA is now a well-established entity characterised by its broad variety of histological patterns [143].
Epidemiology
It is the second most common malignant tumor of minor salivary glands of the palate after MEC [48].
Clinical presentation
It is more frequent in women, and the average age at presentation is 59 years (range 21–94) [48, 144, 145]. Most cases characteristically arise in intraoral minor salivary glands, particularly the palate, with only rare examples in the parotid [146], sometimes developing from a PA [147].
Macroscopy
PLGA is often a well-circumscribed tumor which contrasts with the microscopic infiltrative growth. The median size is 25 mm.
Microscopy
The characteristic histological picture of PLGA is of an infiltrating tumor with cytological uniformity and diverse histological patterns [67]. The architectural patterns include tubular, solid, trabecular, fascicular, cribriform and papillary. Perineural infiltration is often seen (Fig. 5.54). Diffuse infiltration of tumor cells with Indian filing and concentric growth around nerves is reminiscent of lobular carcinoma of the breast (Fig. 5.55). The cells each have single regular round, ovoid or fusiform bland nuclei, sometimes with intranuclear vacuoles and absent or small nucleoli [148]. Variably present are oncocytic, clear or mucous cells. Mitotic figures are scanty and never atypical. The stroma varies from fibromyxoid to densely hyaline, but the chondroid matrix of a PA is not seen.

Polymorphous low-grade adenocarcinoma. Perineural infiltration. Tumor cells show bland cytonuclear abnormality

Polymorphous low-grade adenocarcinoma. Indian filing appearance resembling lobular carcinoma of the breast
Immunohistochemistry shows positivity with epithelial markers (cytokeratins, EMA), S-100, bcl-2 and sometimes CEA, αSMA and vimentin [149]; MIB1 proliferation is low, mean 2.4 % (range 0.2–6.4) in one study [132].
Differential diagnosis
The most important histopathological differential diagnoses are AdCC and PA [150]. Difficulties are particularly the case in small biopsies. Although both PLGA and AdCC are diffusely infiltrating carcinomas, separation is based on architectural and especially cytological features. The nuclei in AdCC are hyperchromatic, angulated, pleomorphic and densely packed with more frequent mitotic figures. In contrast, the nuclei in PLGA are uniform with finely speckled chromatin. The tubules of AdCC are surrounded by an outer layer or myoepithelial cells, whereas in PLGA the tubules generally have a single layer of epithelial cells. The cribriform architecture is more rigid in AdCC than in PLGA. In addition, staining with S-100 protein is usually more diffuse and stronger in PLGA than AdCC [138]. Other markers such as c-kit (CD117) are of little use in practice, as staining can be seen in AdCC and most PLGAs [151]. A much more reliable marker is the MIB1 proliferation index, which is almost always significantly lower in PLGA [132]. The differential diagnosis with PA, which in minor salivary glands can be poorly circumscribed, is based on the presence of chondroid matrix and circumscription of PA, but it is sometimes not possible to distinguish these tumors, particularly on a small biopsy. One other differential diagnosis is with cribriform adenocarcinoma of the tongue and other minor salivary glands, the most useful discriminant being the presence of clear nuclei resembling those of papillary thyroid carcinoma (see Sect. 5.9.6).
Treatment and prognosis
The treatment of choice is surgical with safe (15 mm) margins [143]. Postoperative radiation and chemotherapy have little place. PLGA behaves as a low-grade malignancy; a literature review found a recurrence rate of 21 %, regional nodal metastasis in 6.5 %, distant metastasis in 1.8 % and death due to cancer in 0.9 % [152]. However, after 10 years late recurrences and metastases can appear. In a series of 19 cases of PLGA, 5 patients had local recurrences as late as 15 years after the initial treatment. One patient had regional lymph node metastases 20 years after surgery, and another patient developed lung metastasis after local recurrence [145]. These data confirm that of the previous larger series [145, 149], but there is still debate in literature as to whether recurrences are due to incompleteness of excision – none of the 22 excised tumors recurred or caused death [153] – or whether they can occur even with histologically clear margin but after many years [145]. In a larger series of 164 PLGA, more than 95 % of the patients had no evidence of disease after a long-term follow-up [149]. Papillary structures form part of the spectrum of growth patterns seen in PLGA [154], but when extensive, there is evidence that such tumors are more aggressive [144] or may represent the newly described entity of cribriform adenocarcinoma of tongue and other minor salivary glands (see Sect. 5.9.6) although they do not seem to affect long-term survival. Perineural infiltration does not confer a worse prognosis. Genuine HG transformation can occur rarely, as either a poorly differentiated PLGA or as a salivary duct carcinoma [155].
5.9.6 Cribriform Adenocarcinoma of the Tongue and Other Minor Salivary Glands
Definition
Cribriform adenocarcinoma of the tongue (CATS) and other minor salivary glands is a distinctive hitherto poorly recognised low-grade adenocarcinoma, with several histological features reminiscent of papillary carcinoma of the thyroid and which mostly but not exclusively occurs in the tongue [67, 156]. This tumor was recognised by the latest issue of the WHO classification as a possible variant of polymorphous low-grade adenocarcinoma (PLGA), but it was noted then that it was not yet clear whether this represented a genuine separate entity [157].
Epidemiology
In 1999, Michal et al. published a series of a distinctive type of adenocarcinoma occurring in the tongue characterised by synchronous metastases in lateral neck lymph nodes, but no distant spread [156]. Of the so far 31 published cases in the literature [156–161], 21 tumors were located in the tongue (usually the base), 3 in the soft palate, 2 in the retromolar buccal mucosa, 3 in the lingual tonsils, 1 in the upper lip and 1 in the floor of the mouth. One tumor located in the tongue was described to have a pedunculated configuration [160]. The sex was known in 27 cases: the tumors occurred in 15 women and 12 men. The age of the patients ranged from 21 to 85 (mean 56.8 years).
Clinical aspects
The majority of patients (19 of 31) present with metastases in the cervical lymph nodes, mostly at approximately the same time as the diagnosis of the primary (bilateral in three cases) and one after an interval of 8 years. The primary sites in the lymph node-positive cases were in most cases posterior tongue and retromolar mucosa. However, cervical lymph node metastasis appeared also in extralingual cases including primary of tonsils (two cases) and the palate (two cases).
Macroscopy
The tumor size ranges from 3 to 8 cm in greatest dimension. Grossly, the tumors are covered by intact mucosa devoid of ulceration. They are unencapsulated, white-tan to grey in colour, hard in consistency with no areas of haemorrhage or necrosis.
Microscopy
Histologically, the tumors have invasive margins, in most cases with infiltration of the muscular layer of the tongue and/or adjacent tissues. Lymphovascular invasion is observed in about half of cases. There are often deposits of haemosiderin in focally hyalinised interstitial stroma close to the invasive border of the lesions. The tumors are composed predominantly of cribriform and solid structures in variable proportions (Fig. 5.56). In most instances the tumor architecture consists mainly of a solid mass, often divided by fibrous septa into irregularly shaped and sized nodules composed of solid, cribriform and microcystic structures (Fig. 5.56). In the solid areas, the tumor nests may become detached from the surrounding fibrous stroma by (presumably artefactual) clefts, giving a glomeruloid appearance. The peripheral layer of such solid tumor nests often display hyperchromatic nuclei in a somewhat palisaded pattern (Fig. 5.57). Typically, the tumors also include intermingled tubular, solid and cribriform growth patterns. The tubules are approximately all of the same size, and they consist of one cell layer (Fig. 5.58).

Cribriform adenocarcinoma of the tongue. A vaguely nodular growth pattern is composed of solid nests with tubular structures

Cribriform adenocarcinoma of the tongue. In solid areas, peripheral epithelial layer is detached from the surrounding fibrous stroma by (presumably artefactual) clefts and often displays hyperchromatic nuclei in a palisaded pattern

Cribriform adenocarcinoma of the tongue includes intermingled tubular, solid and cribriform growth patterns. The tubules were approximately all of the same size, and they consisted of one cell layer
The most prominent feature of the tumors, however, is the appearance of the nuclei. These overlap one another and are pale, optically clear and vesicular with a ground glass appearance, so that the tumors cytologically strongly resemble papillary carcinoma of the thyroid gland (Fig. 5.59). Cellular atypia is usually mild, and mitotic figures are in most cases rare. The cytoplasm is clear to eosinophilic and often abundant. Cytologically, all the tumors are composed of one cell type. The overall morphology of the tumor, particularly with focal papillary growth and with overlapping clear ‘Orphan Annie eye-like nuclei’, is remarkably similar to the solid variants of papillary thyroid carcinoma. The cervical lymph node metastases have identical appearances to the primary tumors.

Cribriform adenocarcinoma of the tongue. The most prominent feature is the appearance of the nuclei. They overlap one another and are optically clear and vesicular with a ground glass appearance resembling thus papillary carcinoma of the thyroid gland
On immunohistochemistry CATS is characterised by co-expression of cytokeratins (AE1/AE3, CAM5.2, CK7, CK8 and CK18), S-100 protein and vimentin. Basal and myoepithelial cell markers, such as p63, calponin, CK14, αSMA and CK5/6, are positive in all tumors with variable proportions up to 60 %. Often the palisaded cells surrounding the glomeruloid structures were positive for these markers. Expression of CK19 was variable with mild to moderate focal staining of membranes and cytoplasm in few cases (range 3–5 % of cells, mean 3 %), other cases being completely devoid of staining, but no case was diffusely positive. Proliferative activity was low. EMA, EGFR and HER2/neu were negative in all cases. More importantly all the tumors were completely devoid of any staining for TTF1 and thyroglobulin. No somatic mutations of BRAF, K-RAS, H-RAS, N-RAS, c-kit and PDGFRa genes were found in any of the analyzable cases in two papers [157, 161]. However, in RET proto-oncogene, heterozygous polymorphism Gly691Ser in exon 11 (one case), heterozygous polymorphism p.Leu769Leu in exon 13 (one case), heterozygous polymorphism Ser904Ser in exon 15 (one case) and intronic variant p.IVS14-24 G/A of exon 14 (two cases) were found in one study [161].
Differential diagnosis
The most important differential diagnosis of CATS is PLGA. This neoplasm typically has a wide range of architectural appearances, including tubule and fascicle formation, as well as solid, cribriform and sometimes small papillary structures. A particularly characteristic feature of PLGA is the occurrence of streaming columns of single file or narrow trabeculae of cells forming concentric whorls, thereby creating a target-like appearance [67]; perineural invasion is often seen. At the cellular level, PLGA quite often contains clear cells and, less frequently, mucous cells. Perhaps most importantly, the most striking feature of CATS is the great nuclear similarity to papillary carcinoma of the thyroid, and this is not seen to any great extent in PLGA. Consequently, the other most significant differential diagnosis of CATS is from metastatic papillary carcinoma of the thyroid, particularly if nodal disease is the first presentation. CATS is always thyroglobulin and TTF1 negative and devoid of colloid. However, both CATS and papillary thyroid carcinoma may show variable expression of galectin-3, CK 19 and HBME-1 [161]. In contrast to thyroid cancer, all cases of CATS stain strongly for S-100 protein, and focal myoepithelial differentiation with calponin and actin positivity is common.
Treatment and prognosis
The tumors were treated by surgical excision often accompanied by neck lymph node dissection. Of the 31 patients, 14 individuals additionally received radiotherapy and 1 adjuvant chemotherapy. Clinical follow-up was known in 21 cases. All patients with available follow-up (range 2 months to 13 years; mean 4.3 years) were alive without signs of metastasis [157].
5.9.7 Epithelial-Myoepithelial Carcinoma
Definition
Epithelial-myoepithelial carcinoma (EMC) is a malignant tumor composed throughout of both epithelial and myoepithelial cells (‘biphasic tumor’) in varying proportions.
Epidemiology
EMC has a wide age range (8–103, mean 60 years) and a slight female predominance [67]. Most cases occur in the parotid, less often in other salivary glands. Analogous neoplasms have been described in the breast (adenomyoepithelioma) and elsewhere.
Etiology and pathogenesis
EMC usually arises de novo but occasionally develops in a pre-existing PA [162].
In addition, cases of EMC (and other tumors such as BCA) have been associated with multiple nodules of intercalated duct adenomas and hyperplasia in the surrounding parotid gland [27–29]. This suggests a ductal origin of EMC and also perhaps why in hybrid carcinomas of the salivary glands, themselves very rare, the most frequent combination is that of two typical biphasic tumors, EMC and AdCC [28].
Clinical aspects
The usual clinical presentation is a slow-growing mass, with ulceration in mucosal minor gland tumors. The duration of symptoms before diagnosis ranges from a few months to many years.
Macroscopy
The typical macroscopic appearance of EMC is that of a multinodular, unencapsulated mass, mainly solid, although cystic change is seen in 30 %. The size is usually 20–30 mm but can be as large as 120 mm.
Microscopy
EMC is composed of lumina lined by two distinct layers of cells, epithelial and myoepithelial, beyond which is a basement membrane of variable thickness. The inner epithelial cells are generally small, cuboidal to low columnar and composed of scanty pale to eosinophilic cytoplasm and a round-to-oval nucleus; they can be identified by low-molecular-weight cytokeratin. The surrounding myoepithelial cells typically are larger and polygonal in shape but at times can be spindled or plasmacytoid; their cytoplasm is usually clear, but not always (Fig. 5.60). Immunohistochemically, they express αSMA, SMMHC, calponin and p63 and S-100. CD10 and cytokeratin 14 are less specific, sometimes reacting with both cell layers. Cytological pleomorphism in EMC is usually mild but was classed as severe in 6.6 % of cases [163]; schwannoma-like ‘ancient change’ has also been described. Mitotic figures vary in number and can be numerous; similarly, Ki-67 proliferative activity has a wide range 0–50 and a mean of 17 %. The biphasic pattern of EMC is reproduced throughout most of the tumor (and, indeed, is retained in cell cultures [164]) though each element may vary in prominence between cases as well as within any given lesion [165]. Myoepithelial cells with clear cytoplasm usually dominate the picture, but more than 20 % of EMCs lack clear cells altogether [163], and immunohistochemistry is necessary to demonstrate the double cell population. Variants involving the epithelial cells include apocrine [166] and sebaceous differentiation [167]. Either or both cell types can show oncocytic change [163]. The stroma of EMC is usually a fine network of PAS-positive basement membrane material surrounding the bilayered ducts, but on occasions, it is much thicker with relatively inconspicuous bilayered ducts overall resembling a PA [168]. Although most EMCs are minimally invasive often in a ‘pushing’ pattern, one study identified perineural infiltration in 34 % and involvement of lymphovascular spaces in 11 %; there was extensively infiltrating growth in 13 % [163]. Areas of necrosis are found in about 20 % of EMCs.

Epithelial-myoepithelial carcinoma: characteristic biphasic appearance with an inner layer of ductal cells and outer layer of clear myoepithelial cells. Basal membrane-like material surrounds the outer cells
Differential diagnosis
The differential diagnosis is mainly with other biphasic tumors of salivary glands such as PA and AdCC. Bilayered ducts are not uncommon in any PA, but this appearance will always be only focal. AdCC may have occasional EMC-like areas, and extensive sampling may help to identify typical areas (see Sect. 5.9.4). AdCC has hyperchromatic and angulated nuclei with the three, tubular, cribriform and solid, characteristic growth pattern. Similarly myoepithelial carcinoma may contain occasional ducts resembling an EMC. Therefore, any tumor with EMC-like areas must be sampled widely in order to identify their diagnostic features. When EMC is composed of clear cells, the differential diagnosis includes other clear cell lesions, e.g. other clear cell tumors [169].
Treatment and prognosis
Surgical excision with or without neck dissection is the treatment of choice. The behaviour of EMC is low grade, typically with recurrences in 31 %, cervical node metastases in 18 %, distant metastases and death due to tumor in 7 % [169], although more recent studies suggest a lower rate of distant metastases, probably a consequence of better clinical management [166]. Higher rates of recurrence (50 %) and death (40 %) in a series from a large referral centre in Portugal likely reflected a patient population with advanced disease [170]. Morphological features found to correlate with a poor prognosis include positive margin status, angiolymphatic invasion, necrosis and myoepithelial anaplasia [163]. EMC can occasionally dedifferentiate as a HG myoepithelial neoplasm [171] or adenocarcinoma [172].
5.9.8 Hyalinizing Clear Cell Carcinoma
Definition
Hyalinizing clear cell carcinoma (HCCC) is a malignant tumor composed of epithelial cells usually with clear cytoplasm. Until recently, the diagnosis required the exclusion of other salivary tumors with a clear cell component [67], but it is now recognised that HCCC is a distinct neoplastic entity. Most cases harbour a unique (in salivary glands) molecular genetic abnormality [173]. As such, it is expected to be included as a distinct tumor in the coming WHO classification rather than as part of clear cell carcinoma, not otherwise specified (NOS) [67] as it was in the 2005 WHO classification.
Epidemiology
The sex incidence of HCCC is equal or with a slight female predominance [173] and the age range wide. Most cases arise in minor salivary glands, mainly the palate [48, 67, 173–176] and much less frequently elsewhere such as the parotid [174].
Etiology and pathogenesis
Ultrastructural studies have demonstrated desmosomes and tonofilaments, suggesting squamous differentiation [177]. Most cases of HCCC harbour a recurrent and consistent rearrangement of the EWSR1 gene, usually a EWSR1-ATF1 fusion [178, 179]. This is not found in any other primary salivary carcinoma but is seen in clear cell odontogenic carcinoma, suggesting the two entities may be related or even identical [180].
Clinical aspects
Patients typically present with a painless mass in the palate or, more rarely, in the parotid gland. Exceptionally, cervical lymph node metastases are seen at initial presentation.
Macroscopy
A circumscribed tumor usually <30 mm in diameter with pale cut surface.
Microscopy
HCCC is composed of invasive nests, sheets and trabeculae of polygonal glycogen-rich cells characteristically separated by dense hyaline basement membrane material and fibrocellular stroma [67]. The predominance of clear cells is seen in a minority of cases, and the tumor cells in most cases have pale eosinophilic cytoplasm rather than clear cytoplasm, or they may have a mixture of both (Fig. 5.61). HCCC is composed of nests, sheets and trabeculae of polygonal cells with clear cytoplasm separated by fibrocellular stroma (Fig. 5.62). Occasional HCCCs demonstrate squamous or ductal differentiation. Mucin is often present in small amounts and occasionally is readily apparent [173]. The nuclei display generally mild pleomorphism and inconspicuous nucleoli; mitotic figures are rare. In most cases, HCCCs express epithelial markers, including cytokeratin 7 (but not 20), EMA and 34βE12 as well as p63 (Fig. 5.63) [181], but other myoepithelial markers (e.g. S-100 protein, actin) are consistently negative.

Hyalinizing clear cell carcinoma. Cells in which the cytoplasm appears weakly eosinophilic rather than clear are usually present and may predominate in some tumors

Hyalinizing clear cell carcinoma is composed of nests, sheets and trabeculae of polygonal cells with clear cytoplasm separated by fibrocellular stroma

Hyalinizing clear cell carcinomas express epithelial markers and p63 in all tumor cells
Differential diagnosis
Includes other primary salivary neoplasms composed of clear cells [169, 174] (Table 5.2) as well as metastases principally from renal cell carcinoma, which can present as a parotid mass.
Treatment and prognosis
The treatment of HCCC is surgical excision. The prognosis is generally good; occasional patients have developed metastases in the neck nodes and rarely the lungs [67, 174], but recently a few higher-grade tumors have been identified with the EWSR1 gene rearrangement suggesting that not all HCCCs behave indolently [173].
5.9.9 Basal Cell Adenocarcinoma
Definition
Basal cell adenocarcinoma (BCAc) is a malignant tumor composed of basal-type cells with an infiltrative pattern and potential for metastasis. The WHO classification of salivary gland tumor in 1991 [88] named this tumor ‘adenocarcinoma’ to separate BCAc from the more common basal cell carcinoma of the skin.
Epidemiology
BCAc is rare. It accounts for approximately 2 % of salivary gland carcinomas. Most cases arise in patients over 50 years of age, and there is an equal sex incidence [85]. The usual site is the parotid gland, but they have been described in the submandibular [182], sublingual [183] and minor glands [184, 185].
Etiology and pathogenesis
BCAc can arise de novo, but about 25 % develop in a pre-existing BCA usually of the membranous type [186] (see Sect. 5.8.3). The association between dermal cylindroma and BCA is well known, but BCAc can also arise in association with malignant dermal cylindroma [187].
Macroscopy
Usually unencapsulated tumor mass ranging from 7 to 70 mm, infiltrating the surrounding salivary gland, rarely can be circumscribed.
Microscopy
Microscopically, the general morphological and cytological appearances are almost identical to BCA, and likewise, four growth patterns are recognised – solid, tubular, trabecular and membranous – although these are not thought to have prognostic significance. The tumor islands contain a mixture of large, paler and small basaloid cells, with the latter usually demonstrating peripheral palisading, though this is less marked than in the benign counterpart. The large cells sometimes form ‘eddies’, and the tumor islands may also contain small tubules and foci of squamous metaplasia. The amount of basement membrane material varies but can be marked, especially in the membranous variant. Occasional cases show cytological pleomorphism, but generally this is absent, and mitotic figures are usually sparse (Fig. 5.64).

Basal cell adenocarcinoma. In spite of the lack of significant cellular atypia, the infiltrative pattern is diagnostic of malignancy
Differential diagnosis
This is mostly with BCA and AdCC.
The most reliable indicator of malignancy is infiltration of the surrounding gland and less frequently of blood vessels and nerves [186]. In addition, the Ki-67 proliferation index is usually higher in BCA than its benign counterpart (>5 % vs. <2.7 %) [188]. More than half the BCAcs in one study expressed p53, and 3 out of 11 cases were positive for epidermal growth factor receptor (EGFR); in contrast, all the adenomas were negative [188]. The differential diagnosis of BCAc includes solid forms of AdCC (see Sect. 5.9.4), which are much more aggressive neoplasms with cytological pleomorphism and plentiful mitotic figures; these are generally associated with other growth patterns such as small luminal structures. Although distinction between AdCC and BCAc is usually obvious on morphology, the p63 pattern may help, in that it stains particularly the peripheral cells of tumor islands in the former and most cells in the latter. In the rare case of minor salivary gland BCAc and multiple malignant cylindromas of the skin, immunocytochemical studies showed positive staining for high- and low-molecular-weight keratins and S-100 with negative staining for CEA in both skin and salivary gland tumors [187].
Treatment and prognosis
BCAc is treated with surgery of the primary tumor with clear margins.
The behaviour of most BCAcs is that of a low-grade malignant tumor. A review found an incidence of local recurrence of 37 %, cervical lymph node metastasis of 8 % and distant metastases of 4 %, and one patient died of disseminated disease [186]. Rarely BCAc can show aggressive behaviour with cerebral and pulmonary metastases and death of the patient [189].
5.9.10 Myoepithelial Carcinoma
Definition
Myoepithelial carcinoma is a neoplasm composed almost exclusively of cells with myoepithelial differentiation showing infiltrative growth and metastatic potential. The terms myoepithelial carcinoma and malignant myoepithelioma are interchangeable, but the former is preferred by the 2005 WHO classification [67].
Epidemiology
Myoepithelial carcinoma accounts for about 1–2 % of malignant salivary neoplasms, but it may not be as rare as supposed earlier. The mean age of patients at presentation is about 55 years (range 14–86 years), and the sex incidence is approximately equal [77]. Most cases arise in the parotid gland, but they also occur in submandibular and minor glands, usually the palate; rarely they are found in the base of the tongue, maxillary sinus and larynx [77, 190].
Etiology and pathogenesis
Myoepithelial carcinomas may arise de novo, but at least half of them develop in pre-existing PAs or benign myoepitheliomas particularly recurrences [190].
Clinical aspects
The commonest complaint is that of a mass in the parotid region. When myoepithelial carcinoma arises in recurrent PA, the patient often gives a history of previous surgical resections.
Macroscopy
Grossly, myoepithelial carcinomas are unencapsulated but may be well defined with nodular surfaces. The cut surface is grey-white and can be glassy. Some tumors reveal areas of haemorrhage, necrosis and pseudocystic degeneration.
Microscopy
The architecture is often multinodular with infiltration into adjacent tissues (Fig. 5.65). The nodules comprise solid and sheet-like growths of tumor cells often with plentiful myxoid or hyaline material and sometimes displaying central necrosis (Fig. 5.66). The range of cell types reflects that seen in benign myoepitheliomas and includes epithelioid cells (the most frequent) often arranged in trabecular or pseudo-acinar structures with cleft-like spaces. Cells with clear cytoplasm or vacuolation (resembling lipoblasts) and cells with hyaline (plasmacytoid) and spindle to stellate forms are also seen (Fig. 5.67). In most myoepithelial carcinomas, one cell type predominates, but there is usually a minor component of other cell types. Some authors (including ourselves) feel that a few true glands or lumina are allowable in otherwise typical myoepithelial carcinomas, but others feel they preclude the diagnosis [77]. The nuclei vary from relatively uniform, small with finely distributed chromatin, lacking obvious nucleoli, to markedly enlarged and pleomorphic, showing chromatin clumping and large nucleoli. Mitotic figures may be plentiful (range 3–51 per 10 HPF) and include atypical forms [190]. Multinucleated and bizarre tumor giant cells may occasionally be present. The tumor-related matrix is generally prominent and is hyalinised or myxoid. Special stains show no mucicarmine positive mucus, but plentiful glycogen is found in clear cells, and the myxoid matrix is positive with Alcian blue. Metaplastic changes are frequent and include areas showing squamous differentiation, often with keratinization (Fig. 5.68). Perineural invasion is seen in 44 % and vascular invasion in 16 %. In one series, 40 % of tumors were categorised as HG and 60 % as low grade [190].

Myoepithelial carcinoma. Multiple nodules infiltrate dense fibrous tissue

Myoepithelial carcinoma, solid growth pattern with central necrosis in one of the nodules. This finding may mimic salivary duct carcinoma with comedo-like necrosis

Myoepithelial carcinoma. The spindle cell component shows nuclear pleomorphism resembling a soft tissue sarcoma. A helpful diagnostic pointer is that other types of myoepithelial cell are usually identified elsewhere

Myoepithelial carcinoma: focal squamous metaplasia with keratin pearl formation
Immunohistochemically, there may be considerable variability in staining within the same tumor and between tumors [77]. Reactivity for broad-spectrum cytokeratins (AE1/AE3, CAM 5.2 or MNF116) and at least some of myoepithelial markers, including αSMA, GFAP, CD10, p63 protein, calponin and SMMHC, is required for diagnosis [64]. All myoepithelial carcinomas display diffuse or patchy staining for S-100 protein and vimentin; about half of cases are positive for cytokeratins CK14 and CK5/6 [67]. In contrast, CK7 is often absent. The mean MIB1 (Ki-67) index in one series was 35 % (range 15–65), with any count above 10 % said to be diagnostic of malignancy in a myoepithelial neoplasm [191]. Recent molecular genetic data suggest that EWSR1 gene rearrangement is a common event in myoepithelial tumors arising outside the salivary glands, irrespective of anatomical location [192]. In general, salivary myoepithelial carcinomas have been shown to have an intact EWSR1 gene [193, 194], but recent data suggests that a subset of salivary myoepithelial carcinomas composed mainly of clear cells exhibit EWSR1 gene rearrangements [195].
Differential diagnosis
The variable appearance of myoepithelial carcinoma results in a wide differential diagnosis [64], including salivary duct carcinoma, a spectrum of clear cell tumors [80] and MEC. Nodular structures with central necrosis in myoepithelial carcinomas mimic salivary duct carcinoma, but there is more stromal myxoid and hyaline material in myoepithelial carcinomas; and also S-100 protein and other myoepithelial markers are absent in salivary duct carcinoma. There is no expression of androgen receptors and HER2/neu in myoepithelial carcinoma. The spindle cell variant of myoepithelial carcinoma can mimic various soft tissue sarcomas, and plasmacytoid cell variant should be differentiated from melanoma and plasmacytoma. The clear cell variant of myoepithelial carcinoma [196] resembles a variety of clear cell neoplasms primary and metastatic, including EMC, clear cell carcinoma NOS, HCCC and metastatic renal cell carcinoma (see Table 5.2). In almost every case, immunohistochemistry is helpful in excluding these neoplasms.
Treatment and prognosis
Treatment consists of wide surgical excision combined with radiation, but any role of chemotherapy is not yet established. Whether low-grade and low-stage tumors can be treated only with wide excision needs to be further studied.
The prognosis of myoepithelial carcinoma is variable. Approximately one third of patients die of disease, another third have multiple recurrences, and the remaining third are disease-free [67]. Tumors arising in conventional PAs behave in the same way as those that arise de novo, but it has been suggested that neoplasms developing in recurrent PAs may pursue a prolonged clinical course [197]. Marked cellular pleomorphism, high mitotic rate and high proliferative activity (MIB1 index) correlate with poor prognosis [190].
5.9.11 Salivary Duct Carcinoma
Definition
Salivary duct carcinoma (SDC) is an adenocarcinoma which histologically resembles ductal carcinoma of the breast [67].
Epidemiology
It accounts for about 4–6 % of all salivary carcinomas [198]. Most patients are over 50 years old with an at least 4:1 male-to-female ratio. It arises mainly in the parotid gland, less often in the submandibular and only occasionally in the minor glands. SDC can arise de novo, but recent evidence suggests that approximately half develop as the malignant component of carcinoma ex pleomorphic adenoma [199]. A few others represent HG transformation of low-grade cribriform cystadenocarcinoma SDC, and a single case has been reported arising in (or in association with) a polymorphous low-grade adenocarcinoma of the palate [155].
Etiology and pathogenesis
There are no known aetiological factors, although one case was reported in a patient with long-standing chronic obstructive sialadenitis [200] and another in a patient with IgG4-related sclerosing disease of the parotid [201].
Clinical aspects
Patients complain of a rapidly growing often painful tumor mass sometimes with facial nerve palsy. A long history of a mass with rapid growth is described in SDCs arising from PAs.
Macroscopy
Poorly circumscribed tumor infiltrating the salivary gland and surrounding soft tissues with scar-like cut surface.
Microscopy
All histological studies on SDC have confirmed the strong morphological resemblance to in situ and invasive ductal carcinoma of the breast (Fig. 5.69). The former component comprises expanded salivary ducts with solid, papillary, ‘Roman bridge’, cribriform and comedo patterns, and the infiltrating element can include small ducts, cribriform structures, small nests of cells and trabeculae, all accompanied by stromal desmoplasia; perineural and lymphovascular invasion are frequent. SDC is composed mainly of cells with eosinophilic cytoplasm and often vesicular nuclei containing prominent central nucleoli. Frequently, there is marked nuclear pleomorphism, also apparent on FNA cytology. In better differentiated areas, cells may show definite apocrine features, such as luminal snouts [202]. Other than in the genuine mucin-rich variant [203], mucus is scanty at most, and goblet cells are absent (Fig. 5.70). Usually, mitotic figures are numerous and the Ki-67 index over 25 %.

Salivary duct carcinoma: invasive irregular ducts and cribriform structures strongly resemble ductal carcinoma of the breast

Salivary duct carcinoma, mucin-rich variant. This is composed of a mixture of usual-type salivary duct carcinoma and lakes of mucinous adenocarcinoma
Relatively uncommon morphological variants of SDC include papillary [204], micropapillary [205], mucin-rich [203] and oncocytic [206] subtypes (Fig. 5.71), as well as sarcomatoid SDC, a composite of usual salivary duct and spindle cell carcinomas; this may account for some tumors previously classified as carcinosarcoma (‘true malignant mixed tumor’) [207].

Salivary duct carcinoma with oncocytic differentiation. The cells have ample granular cytoplasm with vesicular nuclei and prominent nucleoli. A clear distinction between oncocytic salivary duct carcinoma and true oncocytic carcinoma may not be possible, as they may not be separate entities
Pure salivary duct carcinoma in situ (SDCIS) is occasionally encountered in either major or minor glands, the diagnosis requiring strict criteria, particularly the absence of local invasion, determined by adequate sampling of the whole lesion and the presence of an intact myoepithelial layer around all tumor islands [208]. Immunohistochemically, SDC expresses broad-spectrum and low-molecular-weight cytokeratins and EMA (EMA). It is also strongly and diffusely positive with CK7 and occasionally and focally with CK20 [209]; GCDFP-15 is found in more than 80 % of SDCs [210]. S-100 protein and myoepithelial markers (e.g. CK14, calponin and SMMHC) are negative, other than in the non-neoplastic cells of in situ lesions; CK5/6 and p63 patterns are similar, except in basal phenotype SDC [see below]. HER2 protein overexpression has been reported in up to 90 % of cases, due to considerable variation between different antibody clones and scoring systems [211]. However, when stricter criteria are used or when HER2 positivity is defined by fluorescence or chromogenic in situ hybridisation amplification, HER2 positivity is identified in only 15 % to a maximum of 40 % [211–213]. Oestrogen receptor α (ERα) and progesterone receptor expression is extremely rare [210, 214], although 73 % of SDCs react with the oestrogen receptor β isoform (ERβ) [213]. More importantly, most SDCs express androgen receptor (AR) – 67–83 % [210, 212, 213] – this is often used as a diagnostic marker due to its near absence in other tumor types [215]. Prostatic marker staining has been described [216], but other studies and personal experience suggest this is exceptional [212, 217, 218].
It has recently been proposed that, similar to schemes in the breast, SDC could be divided into three molecular subtypes: luminal-AR+, HER2 positive and basal phenotype. AR expression in SDC is analogous to ERα reactivity in breast carcinoma and can be used as a marker of the luminal phenotype. HER2 positivity is established by a combination of immunohistochemistry and FISH/SISH for the HER2/neu protein or amplified gene. The basal type is identified by markers such as high-molecular-weight cytokeratins [212]. In that study the relative percentages for each subtype were 69 % luminal-AR+, 17 % HER2, 5 % basal and 10 % indeterminate. There was no correlation between nuclear grade and subtype, except that both basal subtype SDCs were HG [212].
Differential diagnosis
The range of differential diagnosis for both in situ (SDCIS) and invasive SDC includes low-grade cribriform cystadenocarcinoma, myoepithelial carcinoma and metastatic adenocarcinomas to the salivary gland. The relationship of SDCIS to low-grade cribriform cystadenocarcinoma remains unclear. They could perhaps be separate entities with significant immunohistochemical differences, but more probably, low-grade cribriform cystadenocarcinoma represents the extreme low-grade end of the spectrum of salivary DCIS. In favour of the latter is the overlap of architectural patterns with SDCIS, together with cases showing apparent progression to HG invasive SDC [199]. Thus, the entity of low-grade cribriform cystadenocarcinoma may better be termed low-grade intraductal carcinoma [219]. Myoepithelial carcinoma with prominent comedo-like necrosis may simulate SDC. Immunohistochemistry is required to distinguish between primary and metastatic carcinoma with ductal architecture (see Sect. 5.9.20).
Treatment and prognosis
The standard treatment at present is complete surgical excision with radical neck dissection followed by radiotherapy to the tumor bed and possibly chemotherapy [198]. In the future, the subdivision of SDCs into molecular subtypes could lead to new approaches for patients with these cancers. As luminal-AR+ SDCs by definition consistently express AR, anti-androgen therapy may be of value, and preliminary studies on limited numbers of patients have shown a positive result in some patients [220]. Rare examples of patients with HER2-subtype SDCs benefitting from targeted therapies with anti-HER2 monoclonal antibodies (trastuzumab, pertuzumab) or HER2 tyrosine kinase inhibitors (lapatinib) have been reported [221, 222]. Further studies are warranted to determine whether basal-like SDCs, in a way akin to basal-like breast cancers, are sensitive to platinum salts and inhibitors of the poly (ADP) ribose polymerase (PARP). Finally, it has recently been found that some SDCs harbour PIK3CA mutations and/or PTEN loss; it is possible that this may lead to therapeutic targeting of the PI3K pathway [223].
Overall, SDC is one of the most aggressive salivary malignancies. At present, about a third develops local recurrence and 50 % distant metastases; death occurs in 60–80 % of patients, usually within 5 years. Amongst possible prognostic indicators, tumors smaller than 30 mm may have a better outlook [224], but nevertheless several fatal lesions of 20 mm have been reported [204, 218, 225, 226]. More recently, it was found that SDCs negative for both AR and ERβ were more aggressive than tumors which expressed one or both markers, and in addition, carcinomas which were HER2 protein 3+ had a worse outcome than those which were HER2 protein 0–2+ [213]. The outcome for pure SDCIS should be good, provided it is completely excised.
5.9.11.1 Low-Grade Cribriform Cystadenocarcinoma
Definition
Low-grade cribriform cystadenocarcinoma (LGCCC) [67] is a neoplasm of ductal origin composed of cytologically low-grade cells arranged in solid, cribriform or cystic structures surrounded by a rim of myoepithelial cells. It was previously named ‘low-grade salivary duct carcinoma’ [227, 228] but is perhaps better termed low-grade intraductal carcinoma [219].
Epidemiology
The average age of patients is 64 years (range 32–93), with an equal sex incidence. Most cases arise in the parotid glands, rarely at other sites.
Etiology and pathogenesis
The relation between LGCCC and SDC is discussed in Sect. 5.9.11.
Macroscopy
It is unencapsulated and generally displaces rather than truly invades salivary tissue.
Microscopy
Microscopically, it is formed of multiple cysts and solid structures of varying sizes, which are composed of regular small, bland ductal cells with uniform nuclei and clear to eosinophilic cytoplasm (Fig. 5.72). They proliferate to form papillae or cribriform structures, but no necrosis or comedo-like appearance are seen. Occasional cells contain lipofuscin pigment. Mitotic figures are sparse and the Ki-67 index usually <1 %. At the periphery of the tumor islands, there is usually a population of flattened myoepithelial cells.

Low-grade cribriform carcinoma is composed of regular small, bland ductal cells with uniform nuclei and clear to eosinophilic cytoplasm
The epithelial cells express low-molecular-weight cytokeratin and CK7 as well as S-100 protein, but not GCDFP-15 or HER2/neu; variable results have been found with ARs [228, 229].
Differential diagnosis
The relationship of LGCCC to HG SDCIS [208] remains uncertain, as the immune-profile of both lesions often differs, particularly S-100 protein expression, suggesting two distinct entities. However, Weinreb et al. have described overlap cases [229], as well as transformation to high-grade salivary duct carcinoma [199]. This group proposes that the entity be named low-grade intraductal carcinoma [219].
Treatment and prognosis
LGCCC is treated with surgical excision. If excision margins are clear, the prognosis is excellent.
5.9.12 Mucinous Adenocarcinoma
Definition
An epithelial malignancy showing carcinoma cells lying in lakes of abundant extracellular mucus.
Epidemiology
Mucinous (colloid) adenocarcinoma is a rare tumor arising most often in the major glands of adults [230].
Etiology and pathogenesis
Unknown.
Macroscopy
Macroscopically it is a poorly defined tumor with a gelatinous and cystic cut surface.
Microscopy
Histologically it is composed of round and irregularly shaped clusters of epithelial cells floating in mucus-filled lakes, themselves separated by fibrous strands. The cells are cuboidal, columnar or irregular in shape, usually possessing clear cytoplasm and small dark nuclei; signet ring cells may be present. The mucus is PASD and mucicarmine positive. The carcinoma cells express epithelial markers, but not high molecular weight (MW) cytokeratins or actin [67].
Differential diagnosis
Mucinous cystadenocarcinoma arises more often from the minor glands and is identified by mucin pools largely lined by carcinoma cells, which have larger nuclei than in colloid carcinoma [230]. The differential diagnosis of mucinous adenocarcinoma also includes other mucinous neoplasms such as MEC and mucin-rich SDC.
It is unclear whether low-grade signet ring cell (mucin-producing) adenocarcinomas of minor salivary gland are related, as they lack mucus pools [231]. Some may represent examples of the recently described mucinous myoepithelioma, in which many of the component cells contained abundant mucin in their cytoplasm, and all expressed some myoepithelial markers including S-100 protein [232, 233].
Treatment and prognosis
Surgical resection with or without subsequent radiotherapy is the current treatment. Mucinous adenocarcinoma tends to recur and give metastases.
From the relatively few published cases, mucinous cystadenocarcinoma has a relatively favourable clinical behaviour [230].
5.9.13 Oncocytic Carcinoma
Definition
A tumor composed of malignant oncocytic cells. However, some investigators have suggested that it is probably not a single entity but a mixture of several carcinomas showing oncocytic differentiation, most often SDC [206].
Epidemiology
Several carcinoma types have variants composed of oncocytic cells, but fewer than 100 cases of pure oncocytic carcinoma have been reported. The average age is 63 years (range 29–91), and most have occurred in the parotid [39, 234].
Etiology and pathogenesis
Oncocytic carcinoma can arise de novo or in association with a benign oncocytoma (up to 50 %) [235] and some have arisen in Warthin’s tumors [236].
Clinical aspects
Most cases present with a slow-growing swelling. The history is longer if the carcinoma has arisen from an underlying oncocytoma. Pain and facial paralysis are reported in some patients.
Macroscopy
Nodular/multinodular mass with brown and soft cut surface.
Microscopy
The diagnosis of a pure oncocytic carcinoma requires the identification of malignancy, oncocytic differentiation and lack of features of any other tumor type. Dark and light oncocytic cells are arranged in solid-trabecular and nested patterns. Necrosis, infiltration of periglandular and salivary tissue with infiltration of nerves and vessels is seen in aggressive cases. The tumor cells show positive staining for antimitochondrial antibodies [35].
Differential diagnosis
Benign oncocytoma is a well-circumscribed tumor without signs of invasion. MNOH can simulate invasion, but the characteristic lobular pattern leads to the correct diagnosis. MEC contains other cells types such as mucous/intermediate and clear cells. The separation of oncocytic carcinoma from SDC may be difficult in absence of ductal differentiation. SDC shows characteristic DCIS-like areas.
Treatment and prognosis
The tumor is treated surgically with or without neck dissection. It is likely that a pure oncocytic carcinoma is an aggressive tumor, as over half of the patients reported either died of disease or suffered recurrences [234].
5.9.14 Carcinoma Ex Pleomorphic Adenoma
Definition
Carcinoma ex pleomorphic adenoma (CXPA) is an epithelial malignancy arising from a PA [67]. There is still confusion about terminology of these tumors, but based on the degree of invasion of carcinoma beyond the capsule of maternal PA, three main categories are recognised – widely invasive, minimally invasive and non-invasive CXPA. A proposal for two prognostically relevant main categories (widely invasive and early CXPA) is used in this chapter [237, 238]. The clinicopathological features of widely invasive CXPA and early CXPA are discussed separately.
5.9.14.1 Widely Invasive CXPA
Epidemiology
This is the most common form of CXPA; it represents 3.6 % of all salivary gland tumors. 82 % of cases arise in the parotid gland and most of the rest in the submandibular gland; the minor salivary glands, particularly in the palate, can also be affected [239]. In exceptional cases the seromucinous glands of the sinonasal tract are involved [240]. In several large series [241–244] CXPA represents 3.6 % of all salivary gland tumors, 11.7 % of all salivary gland malignancies and 6.2 % of all PAs (range in different series from 1.9 % to 23.3 %).
Etiology and pathogenesis
The incidence of malignant transformation increases with the length of history of the PA, from 1.5 % at 5 years to 10 % after 15 years [242]. Older patient age, larger size (and origin from submandibular site) and the presence of marked hyalinisation tend to be associated with more frequent malignant transformation [244, 245].
Clinical aspects
Most patients are men over 60 years old with a typical presentation of a long history of a salivary gland nodule that suddenly increases in size. Because by definition CXPA must arise in association with PA with histological evidence of co-existent or pre-existing PA, a clinical history of long-standing parotid tumor is not sufficient evidence for a pre-existing PA, whilst a previously excised PA at the site of a carcinoma is acceptable [237, 238, 246].
Macroscopy
Widely invasive CXPAs are often larger than benign PAs [242–244]. They are firm and ill-defined tumors with infiltration of adjacent tissue. A well-circumscribed nodule may be seen representing pre-existent PA, but it may be seen only after extensive sectioning because the proportion between carcinoma and PA favours carcinoma [244].
Microscopy
Histologically the dominant picture is the carcinoma. The pre-existing PA may be obscured by the carcinoma or may only show degenerate changes such as scarring, dystrophic calcification, necrosis and haemorrhage [238, 243, 244, 247]. A relevant proportion of tumors (probably a quarter of all cases) is not correctly diagnosed as CXPA, because the pre-existent PA is not identified for insufficient sampling.
When present, the contrast between maternal PA and carcinoma is usually obvious, and the recognition of widely invasive carcinoma ex PA is relatively simple. The malignant cells tend to have pronounced nuclear pleomorphism and increased number of mitoses (Fig. 5.73). Capsular, perineural and vascular invasion are easily identified as well as extension into neighbouring tissues. However, a notorious problem is the diagnosis of well-differentiated myoepithelial type of CXPA due to a lack of relevant cellular atypia, mitoses and blunt infiltration.

Carcinoma ex pleomorphic adenoma. Salivary duct carcinoma with high-grade features arising in pleomorphic adenoma that is apparent at the lower part of the image
Several studies show SDC, adenocarcinoma NOS and frequently misdiagnosed myoepithelial carcinoma to be the most frequent histological types [238, 247], but it is not uncommon to find other differentiation, e.g. squamous, mucoepidermoid, polymorphous low-grade adenocarcinoma or AdCC (Fig. 5.74) [238, 240–244]. The immunohistochemical profile of widely invasive CXPA (excluding myoepithelial type) shows strong expression of pan-cytokeratin (AE1/AE3 and CAM5.2), CK7, CK8, CK18, CK19 and EMA. Staining for p63, αSMA, CK5/6 and CK14 may be focally present in myoepithelial cells of residual non-invasive/intraductal CXPA. MIB1 proliferative activity shows a higher (35 %) index in the malignant component in contrast to the low proliferation index in the maternal PA.

Carcinoma ex pleomorphic adenoma. In the centre of the image, the residual pleomorphic adenoma is apparent. The malignant component has the morphology of adenoid cystic carcinoma and basal cell adenocarcinoma
In addition, nuclear staining for AR and p53 can be detected in the malignant component. Similarly immunohistochemistry for HER2 protein is seen in the malignant cells of CXPA as a distinct membrane staining (3+) in cases of HG CXPA, whilst lower grades show moderate (2+), weak or absent (1+/0) membrane staining [211].
Gene amplifications of the HER2 gene as detected by in situ hybridisation (ISH) techniques are seen mostly in cases of CXPA with HG morphology. Mutation of TP53 gene [246] as detected by gene sequencing is often noted in the malignant cells of CXPA.
Other molecular studies have confirmed that the development of CXPA follows a multistep model of carcinogenesis with loss of heterozygosity at chromosomal arms 8q, 12q and 17p and inactivation of tumor suppressor genes [248–250]. A recent study has demonstrated that PLAG1 and HMGA2 are rearranged in about 50 % of SDC ex PA [199].
Differential diagnosis
Widely invasive CXPA can be confused with other primary and metastatic carcinomas of salivary glands when the maternal PA cannot be identified, but the most important differential diagnosis is the separation of widely invasive carcinoma from early CXPA.
Treatment and prognosis
Widely invasive CXPA is treated with surgical resection usually associated with neck dissection. Surgery is followed by radiotherapy and in some cases chemotherapy. The prognosis depends on the degree of invasion beyond the capsule of PA [237, 238, 251–253]. Histological grade, lymph node metastases and perineural invasion and extent of invasion are important factors of CXPA. Widely invasive CXPA is an aggressive tumor with local recurrences, lymph node and distant metastases. In a series of 51 patients, Zhao et al. [254] found 39.2 % developing loco-regional recurrence and 27.5 % distant metastases with an overall survival of 62.7 % at 3 years and 50.3 % at 5 years up to 70 %. Prognosis may have improved with the more recent use of targeted therapy for epidermal growth factor receptor 2 (HER2).
The goal of HER2 testing in CXPA is on one hand to assist the histological diagnosis and on the other hand to identify patients eligible for trastuzumab therapy in case of metastatic disease [221, 255]. The possibility of assessing HER2 gene amplification by newly developed in situ hybridisation techniques may encourage the assessment of HER2 status of salivary gland carcinomas in routine diagnostic reporting [212, 221, 256].
5.9.14.2 Early Carcinoma Ex Pleomorphic Adenoma
Definition
There is no agreement in the literature. In the authors’ opinion, early carcinoma ex pleomorphic adenoma (ECXPA) includes both DCIS-like and micro-invasive-like carcinoma still confined in the capsule of PA and carcinomas with extension beyond the capsule of PA of no more than 6 mm (see Table 5.3).
Epidemiology, etiology and pathogenesis
Are similar to that of widely invasive CXPA.
Macroscopy
ECXPA are well-circumscribed and small-sized (stage T1-2) tumors without or with minor invasive growth outside the capsule of PA (Figs. 5.75, 5.76 and 5.77). Those arising in the deep parotid lobe may be larger in size.

Non-invasive carcinoma in a pleomorphic adenoma. Ducts contain cells with atypical nuclei. Focal necrosis and calcification are also present

Non-invasive carcinoma ex pleomorphic adenoma. On low-power view, hyalinisation is apparent as well as highly cellular areas

Non-invasive carcinoma ex pleomorphic adenoma. On high-power view of the previous image, the classical appearance of salivary duct carcinoma is apparent
Microscopy
The maternal PA is usually identified in all cases. Within pre-existing ducts of PA are cytologically malignant cells, surrounded by small bland-looking actin/CK14/p63-positive myoepithelial cells. These ducts frequently show central necrosis giving a comedo-like appearance and papillary and cribriform architecture resembling intraductal carcinoma of the breast [253]. With progression of disease, intraductal carcinoma can be associated with extraductal (invasive but still intracapsular) and extracapsular invasion with invasive component of no more than 6 mm [237, 238, 246]. Immunohistochemistry for MIB1 [238, 253] and AR is suggested as useful tools to recognise microscopic foci of CXPA.
However, AR should not be used in isolation as up to 10 % of PAs express nuclear staining for AR which may lead to an overdiagnosis of CXPA [257]. The immunoprofile of ECXPA [258] is similar to that of widely invasive CXPA described in the corresponding paragraph.
Differential diagnosis
The most important differential diagnosis is between ECXPA and widely invasive CXPA, and it is based essentially on the degree of invasion of <6mm.
Treatment and prognosis
Surgery with clear margin is the preferred treatment, preoperative diagnosis is rare, and the tumor is clinically diagnosed as PA. ECXPA behaves in a benign fashion after excision providing sampling is complete and diagnosis is accurate. This favourable prognosis has been proved by several studies (see Table 5.4).
As shown in Table 5.4, the concept of ECXPA – i.e. early malignant changes but still of carcinoma – was first noted in 1977 by LiVolsi and Perzin who raised the issue of non-invasive CXPA [241]. In 6/47 cases of CXPA, there was no evidence of invasion. The clinical behaviour in these patients was identical to PA with no local recurrence or distant metastases. In 1984 Tortoledo et al. reported 16 patients with extracapsular invasion ranging from 9 to 20 mm who died of their disease, whilst none of 16 patients with extracapsular invasion less than 8 mm died [147].
Brandwein et al. [252] reported 12 patients with capsular invasion of <1.5 mm. The study did not include patients with extracapsular invasion of more than 1.5 mm. No patient developed local recurrences or metastases, and this figure of 1.5 mm has been adopted as a threshold by the WHO classification of Salivary Gland Tumors 2005 [67]. More recently (see Table 5.5) at least five studies have appeared in literature suggesting a wider pattern of histological appearances and proposing a higher prognostic threshold of up to 5 mm of extracapsular invasion [238, 246, 253, 256, 259] to be used to separate clinically favourable from unfavourable cases of CXPA. There has been only one study [260] where lymph node metastasis developed in a properly sampled non-invasive epithelial CXPA. The explanation for these cases is uncertain but may include microinvasion not identified even with thorough sampling of the tumor edge.
5.9.14.3 Carcinosarcoma Ex Pleomorphic Adenoma
Definition
A malignant tumor showing a mixture of carcinomatous and sarcomatous elements. True malignant mixed tumor (TMMT) is a common synonism for carcinosarcoma (CS).
Epidemiology
CS is rare. There are fewer than 100 cases reported in literature [242, 261–263].
Etiology and pathogenesis
CS can arise de novo in a healthy salivary gland or as a complication of PA. In a subset with osteoclast-type giant cells, the same mutation was found of the same allele on chromosome 17p13, a known mutation of SDC. This suggests that CSs are in reality metaplastic carcinomas, possibly sarcomatoid SDCs.
Clinical aspect
The mean age at presentation is 58 years (range 14–87), and most cases are found in the parotid gland. In CS arising in a pre-existing PA, the history will usually be that of rapid growth in a long-standing salivary nodule [262].
Macroscopy
Usually it is a poorly circumscribed tumor. A separate nodule can be seen in those cases where CS arises in pre-existing PA [263].
Microscopy
CS is a biphasic tumor in which the mesenchymal element is usually chondrosarcoma, but osteosarcoma, fibrosarcoma, malignant fibrous histiocytoma, pleomorphic rhabdomyosarcoma and osteoclast-type giant cell neoplasms have also been described [261]. The epithelial component is generally a poorly differentiated (adeno)carcinoma with features of SDC increasingly reported (Fig. 5.78) [247]. CS can also differentiate into TTF1-positive large cell neuroendocrine carcinoma [263]. On immunohistochemistry epithelial markers are usually detected in the epithelial component and may or may not also be expressed in the sarcomatous component. Positive staining for epithelial markers has been used as proof of the fact that CSs are carcinomas showing divergent differentiation (possibly sarcomatoid variants of SDC) and as an indication of their monoclonal origin. However, keratin staining can be negative casting doubt onto the monoclonal-carcinomatous nature of the whole tumor. Molecular studies using comparative genomic hybridization (CGH) have revealed similar genomic profiles in epithelial and mesenchymal component, confirming their monoclonal histogenesis [264].

True malignant mixed tumor/carcinosarcoma. The epithelial component is a poorly differentiated carcinoma with some features suggesting salivary duct carcinoma. The sarcomatous component is a high-grade spindle cell sarcoma, in this case, without specific differentiation
Differential diagnosis
Includes spindle cell squamous carcinoma, primary salivary sarcomas and CXPA. The first arises from the mucosal surface and may simulate CS of minor salivary glands. Its epithelial component is epidermoid, not glandular; dysplasia of the surface squamous epithelium is diagnostic. Primary salivary sarcomas are exceptionally rare and must be well sampled to identify any minor carcinomatous component. The possibility of metastatic melanoma with spindle cell morphology should not be forgotten; immunohistochemistry shows positivity for appropriate markers.
It has not yet been established whether all or some CS are examples of the sarcomatoid variant of SDC, but any positivity for ARs would suggest that diagnosis.
The main diagnostic problem is the rarity of CS. Even specialist pathologists generally have little familiarity in reporting this tumor type.
Treatment and prognosis
The treatment of CS is surgical, and the outcome is usually poor with 60 % of patients dying of disease.
5.9.14.4 Metastasising Pleomorphic Adenoma
Definition
Metastasising pleomorphic adenoma (MPA) is a histologically benign PA, which recurs locally and gives distant metastases.
Epidemiology
MPA is rare, and the largest series [265] published in the last decade where the literature was reviewed between 1953 and 2005 revealed 42 patients with an average age of 33 years. Bone was the most common site for metastases (45 %), followed by the head and neck (43 %) and lung (36 %). Other cases published more recently are still regarded as fascinating enigma or dramatic case report [266–268].
Etiology and pathogenesis
The development of metastasis seems to require a background of multiple loco-regional recurrences following incomplete resection of the primary tumor. Therefore, the postulated pathogenesis is vascular implantation or invasion eventually leading to metastases, but in many cases of MPA, it was not possible histologically to demonstrate actual vascular permeation [267, 269]. However, some authors [270, 271] have speculated that MPA are unrecognised (low-grade) carcinomas with a potential to kill the patient.
Clinical aspects
There is usually a clinical history of multiple recurrences of PA with additional development of a tumor mass in the local lymph nodes widely or distant sites such as the bone, lung and kidney. Unusual locations include the sphenoid bone [272].
Macroscopy
Well-circumscribed nodule/s similar to primary PA.
Microscopy
The typical features (epithelial ducts mixed with chondromyxoid tissue) of PA are present. The tumor remains histologically ‘benign’ in the primary site, local recurrences and metastatic deposits [269, 273].
Treatment and prognosis
Local recurrences and metastatic deposits are treated surgically. The prognosis depends on the sites and number of metastases and their development within the first 10 years of primary surgery [265].
5.9.15 Sebaceous Carcinoma
Definition
Sebaceous carcinoma is a malignant tumor composed predominantly of sebaceous cells with varying degrees of pleomorphism and invasiveness.
Epidemiology
It is rare with <50 cases reported so far [103, 274–277]. The majority occur in the parotid gland, followed by oral cavity, submandibular and sublingual gland. There is no sex predilection, and age distribution reported in literature is after the third decade [274, 275], but one group reported two cases in children [278].
Etiology and pathogenesis
Sebaceous carcinoma can arise from PA [277] and sebaceous lymphadenoma [104].
Clinical aspects
Patients can either present with a painful mass and facial nerve paralysis or with a painless parotid swelling.
Macroscopy
Sebaceous carcinomas are frequently well or partially circumscribed tumors ranging from 6 to 95 mm in greatest dimension.
Microscopy
The tumor cells are arranged in nests or sheets and show characteristic abundant clear and vacuolated cytoplasm. Nuclei show varying degree of pleomorphism that is more pronounced than the nuclear features of sebaceous adenomas. Areas of cellular necrosis and fibrosis are commonly found. In some cases, perineural invasion has been noted, but vascular invasion seems particularly uncommon. There is a background of lymphoid tissue with follicles mixed with foreign body giant cells with histiocytes [103].
Differential diagnosis
Mostly with sebaceous adenoma and clear cells tumors.
Treatment and prognosis
Surgery usually followed by radiotherapy in tumors of advanced stage. Metastasis is rare, but local recurrences are documented. The survival rate is approximately 60 %, but prognosis is better for oral sebaceous carcinomas [276].
5.9.15.1 Sebaceous Lymphadenocarcinoma
Definition
Sebaceous lymphadenocarcinoma is the malignant counterpart of sebaceous lymphadenoma.
Epidemiology
An extremely rare tumor of the salivary glands with <10 cases reported in literature [274, 275, 279–282]. It occurs in adult patients and parotid is the preferred site.
Etiology and pathogenesis
The rare case reported indicates an origin from sebaceous lymphadenoma.
Clinical aspects
Patients had histories of a tumor mass of varying duration up to 20 years. In one patient there was a history of cervical lymph node metastasis and involvement of the skin left cheek and neck [279].
Macroscopy
Partly encapsulated, cystic and solid tumor up to 60 mm in maximum diameter.
Microscopy
Malignant sebaceous cells are organised in sheets showing evidence of squamous and ductal differentiation. Identification of the underlying sebaceous lymphadenoma or pleomorphic carcinoma requires extensive sampling. Some cases show a background lymphoid infiltrate with collections of histiocytes and a foreign body giant cells.
Differential diagnosis
Clear cell tumors and tumors showing sebaceous differentiation.
Treatment and prognosis
Surgical excision often followed by radiotherapy. Given the limited number of cases reported in literature, the long-term prognosis is not well established yet.
5.9.16 Primary Squamous Cell Carcinoma
Definition
Squamous cell carcinoma (SCC) arising in the salivary glands.
Epidemiology
An extremely rare tumor of the salivary glands. It occurs in adults and the parotid gland, and its main excretory duct is the preferred site.
Etiology and pathogenesis
Not known.
Clinical aspects
A mass lesion of variable duration.
Macroscopy
Usually invasive mass.
Microscopy
As elsewhere in the head and neck region, the appearance is that of an invasive carcinoma of variable differentiation and keratinization.
Differential diagnosis
The vast majority of squamous carcinomas in the salivary glands represent metastases from the skin or upper aerodigestive tract.
Treatment and prognosis
Surgical excision often followed by radiotherapy.
5.9.17 Lymphoepithelial Carcinoma
Definition
A malignant tumor composed of undifferentiated epithelial cells mixed with lymphocytes. It is histologically similar to undifferentiated nasopharyngeal carcinoma.
Epidemiology
In the Western countries, it is an extremely rare tumor accounting for <0.5 % of all salivary gland malignancies. In contrast in southern China and in Eskimos (Inuit), the reported incidence is exceptionally high representing 80 % of the cases reported in literature. The median age is 40 years (range 10–86), and it is slightly commoner in females [48]. Familial clusters have been identified amongst patients from Greenland [283]. The parotid is involved in 80 % of cases where it can arise in an intra-glandular lymph node [284], with the rest occurring in the submandibular glands [285].
Etiology and pathogenesis
Infection with Epstein-Barr virus (EBV) is a major factor. Other contributing associations are with certain human leucocyte antigen (HLA) types [286].
Clinical aspects
Patients complain of a parotid mass, but in 40 % of the cases, the clinical first presentation is a metastasis in a cervical lymph node [287].
Macroscopy
An invasive mass or a lymph node metastasis from the neck.
Microscopy
There is a marked histological similarity to undifferentiated nasopharyngeal carcinoma, which has also been linked to EBV. Microscopic examination shows syncytial groups of large epithelial cells with vesicular nuclei and prominent nucleoli, intimately mixed with lymphocytes and plasma cells, sometimes with germinal centre formation. Mitotic figures are often numerous. At times, the epithelium is difficult to identify, but it can be highlighted by cytokeratins. Epstein-Barr virus encoded small RNA (EBER) staining of nuclei is diagnostic in this situation.
Differential diagnosis
The most important differential diagnosis is a metastasis from a nasopharyngeal primary, which can present as a parotid mass [288] or possibly very poorly differentiated squamous carcinoma of usual type originating in the skin or upper aerodigestive tract. Fluorodeoxyglucose positron emission tomography-computed tomography (FDG PET-CT) has been widely recommended as sensitive at detecting both primary malignancy and metastatic spread [289].
For differential diagnosis with lymphoepithelial sialadenitis, lymphadenoma and lymphoma (see Sects. 5.10.1, 5.8.8 and 5.10.3).
Treatment and prognosis
Radiotherapy has been the mainstay of treatment of nasopharyngeal carcinoma due to its radiosensitivity. Other therapy modalities include superficial parotidectomy with neck dissection. The outcome is surprisingly good for such an aggressive-looking carcinoma, and the 5-year survival rate is 60 % [287]. One report estimated 2-, 5- and 10-year survival at 91 %, 66 % and 29 %, respectively, for lymphoepithelial carcinoma of the salivary glands [290]. Further research is needed to determine the effect of different treatment modalities on survival.
5.9.18 Small Cell Carcinoma
Definition
Small cell carcinoma (SmCC) is a malignant epithelial tumor composed of cells with scanty cytoplasm, round nuclei with fine chromatin and inconspicuous nucleoli similar to pulmonary SCC.
Epidemiology
Primary salivary gland SmCC is very rare, accounting for <1 % of all salivary gland tumors [291]. They are seen more often in men, with a mean age of 56 years (range 5–86). Parotid gland is the most involved site in the <100 cases reported in literature [291–293].
Etiology and pathogenesis
There is a known association with smoking. The pathogenesis is unknown, but SmCC is unlikely to be a single entity, as electron microscopy reveals that some neoplasms show neuroendocrine differentiation, whilst others have squamous and ductal features not apparent histologically [294, 295], and occasionally both patterns are evident in the same tumors. Unlike Merkel cell carcinomas of the skin, CK20+ SmCCs show no association with virus [295a]. Some neoplasms called SmCC may in fact be primary primitive neuroectodermal tumors and NUT gene rearrangement carcinomas.
Clinical aspects
Patients note a rapidly growing salivary gland swelling often accompanied with lymph node enlargement.
Macroscopy
The surgical specimen shows a poorly circumscribed mass often with areas of necrosis.
Microscopy
The microscopic appearance may be similar to SmCC of the lung or Merkel cell carcinoma of the skin. Both comprise solid sheets, nests and cords of closely packed cells; the difference is in the cell size, small and dark cells in the former and slightly larger and with pale chromatin in the latter. Immunohistochemistry shows positive staining for chromogranin, synaptophysin, neuron-specific enolase and CAM5.2, often with paranuclear dots in both types. However, immunohistochemistry for CK 20 seems to identify two subtypes of SmCC: CK20− lung cell type and CK20+ Merkel cell-type carcinoma [292, 293, 296].
Differential diagnosis
The most important differential diagnosis is with metastases from lung SmCC and Merkel cell carcinoma of the skin, and these must be excluded before a primary SmCC can be said to be of salivary origin. Clinicopathological information is usually helpful. The solid variant of AdCC may be confused with SmCC (see Sect. 5.9.4). Lymphomas and primary primitive neuroectodermal tumors of the salivary glands may be somewhat similar morphologically and can be excluded immunohistochemically.
Treatment and prognosis
Surgery with adjuvant chemotherapy is the treatment of choice. The prognosis is poor, but a study by Nagao et al. [291, 292] showed that CK20+ SmCC of the salivary glands have a better prognosis than CK20− cases [292].
5.9.19 Well and Moderately Differentiated Neuroendocrine Carcinoma (‘Typical’ and ‘Atypical’ Carcinoid)
Definition
A malignant tumor showing neuroendocrine differentiation, corresponding to similar neoplasms at other sites, such as the lung. These carcinomas do not exhibit the cytomorphological features of SmCC (see Sect. 5.9.18).
Epidemiology
Both well- and moderately differentiated neuroendocrine carcinomas (NEC) are very rare, with only occasional cases described. Patients reported have been adults of either sex. All reported cases have been in the major glands [296a, 296b].
Etiology and pathogenesis
No known factors.
Clinical aspects
Salivary gland swelling is the first clinical presentation; occasionally patients experienced pain.
Macroscopy
Generally, a fairly well-circumscribed tumor but with an infiltrative pattern.
Microscopy
The tumors are arranged in nests, cords and trabeculae infiltrating surrounding tissue; focal ductal differentiation was described in one case and occasional rosette-like structures in another [296a]. The cells are spindle to polygonal in shape, and the nuclei may be vesicular or display stippled chromatin; nucleoli can be prominent. In moderately differentiated NECs, mitotic figures are relatively easy to find with counts up to 8/10 HPFs. Moderately differentiated NECs may also display variable amounts of necrosis and show lymphovascular or perineural infiltration. NECs stain for neuroendocrine markers, such as synaptophysin and chromogranin, although the latter may be patchy, as well as cytokeratins; however, staining for cytokeratin 20 has not been demonstrated, unlike in SmCC (see Sect. 5.9.18). No figures are available for Ki-67 counts, but in personal experience of a single case of moderately differentiated NEC by one of the authors (RHWS), the index was 15 %.
Differential diagnosis
The main differential diagnosis of a primary salivary NEC is from metastatic NEC, and this must be done by the clinical and imaging exclusion of a primary elsewhere. It can be distinguished from other primary salivary neoplasms by the almost unique immunohistochemical profile of NEC, which is shared only with SmCC, itself composed of small dark cells.
Treatment and prognosis
Treatment is surgical resection. The few cases described have survived several years, in some cases even with distant metastases. However, it is reasonable to speculate that moderately differentiated NEC could cause death by extensive disseminated disease.
5.9.20 Desmoplastic Small Round Cell Tumor
Definition
A malignant tumor composed of cells with polyphenotypic differentiation.
Epidemiology
Exceptionally rare but possibly underdiagnosed. A recent literature review has shown six cases of extra-abdominal desmoplastic small round cell tumor reported so far [297]. Patients are young, but in one case the patient was 41 years old.
Etiology and pathogenesis
Desmoplastic small round cell tumors harbour the EWS gene translocation that can be detected by fluorescence in situ hybridisation (FISH). The EWS-WT1 gene fusion is also demonstrated by RT-PCR.
Clinical aspects
Salivary gland rapid swelling is the first clinical presentation [297, 298].
Macroscopy
Poorly circumscribed tumor with infiltrative pattern.
Microscopy
The tumor is arranged in nests embedded in desmoplastic stroma. The cells have moderate amount of cytoplasm and hyperchomatic nuclei. They stain positively for cytokeratins, desmin, WT-1, EMA, NSE and CD56.
Differential diagnosis
SmCC, solid variant of AdCC and other poorly differentiated carcinomas of salivary glands are the main differential diagnosis. The young age of the patient, the polyphenotypic immunoprofile and the characteristic EWS gene translocation are diagnostic of desmoplastic small round cell tumor.
Treatment and prognosis
The affected salivary gland is surgically resected, but the prognosis is poor.
5.9.21 Nuclear Protein in Testis Rearrangement Carcinoma
Definition
Nuclear protein in testis (NUT) rearrangement carcinoma is defined by abnormalities of the NUT gene on chromosome 15q14.
Epidemiology
It has a wide age range (3–78 years), and although found throughout the body, it is well described in the head and neck region and occasionally in the salivary glands.
Microscopy
The appearance is that of sheets and islands of undifferentiated malignant cells but with occasional well-differentiated squamous islands; p63 staining is seen beyond these islands, suggesting a squamous lineage. Areas of necrosis are frequent and the mitotic rate high.
Treatment and prognosis
Too few cases have been reported to comment, but behaviour at other sites is generally aggressive and the development of metastases a particularly poor sign.
5.9.22 Higher-Grade Change in Carcinomas
Definition
High-grade (HG) transformation (originally called ‘dedifferentiation’) is defined as the histologic progression of a low-grade malignant neoplasm to a high-grade one, within which the original line of differentiation is lost.
Epidemiology
Rare in salivary glands. The phenomenon was first reported in mesenchymal tumors, such as dedifferentiated chondrosarcoma [299] and liposarcoma [300]. The phenomenon of HG transformation has subsequently been recognised in a variety of salivary gland carcinomas, including AciCC [114], AdCC [301], PLGA [155], EMC [163] and MASC [122].
Etiology and pathogenesis
Although HG transformation of salivary gland carcinomas is always associated with tumor progression, characterised by development of a subpopulation of tumor cells within a low-grade malignancy that fails to develop along the expected lineage of differentiation, little is known about molecular genetic events that regulate this. Alteration of the p53 pathway has been recognised in AdCCs [302] and EMC [163], but no alterations of the TP53 gene were detected so far in previous studies of HG-transformed AciCCs [114, 303] and MASC [122].
Clinical aspects
Patients complain of tumor swelling with rapid increase in size.
Macroscopy
Partly unencapsulated nodule with necrotic and haemorrhagic areas.
Microscopy
Tumors with HG transformation are composed of conventional carcinomas juxtaposed with areas of HG morphology. The conventional/low-grade component has the features of AciCC [114], AdCC [301], PLGA [155], EMC [163] and MASC [122]. The HG component is either poorly differentiated adenocarcinoma or undifferentiated carcinoma, usually arranged in solid nests, sometimes in cribriform pattern of cells with large vesicular nuclei, prominent nucleoli and abundant cytoplasm. Frequent mitoses and extensive necrosis are evident. The Ki-67 labelling index is consistently higher in the HG component.
Treatment and prognosis
Salivary gland carcinomas with HG transformation are aggressive tumors characterised by rapid progression accompanied by a higher local recurrence rate and propensity for cervical lymph node metastasis. Generally, the tumors have a very poor prognosis and therefore should be managed as high-grade carcinomas. Wide local excision, cervical lymph node dissection and aggressive radiotherapy are the treatments of choice.
5.9.23 Metastatic Malignancies
Definition
Salivary gland localisation of a tumor originating from another site.
Epidemiology
Metastases to the major glands and the intraparotid lymph nodes constitute approximately 10 % of all salivary carcinomas [304]; the exact figure varies from study to study depending on local factors such as different incidences of particular cancers. For example, Bergersen et al. [305] in Australia reported that metastases constituted 72 % of all malignancies, resulting from the high incidence of skin cancer. In an AFIP series and literature review in 1991 of 785 parotid metastases [304], 64 % were found to have originated from the head and neck region (including the skin), 11 % from distant sites and 25 % from an unknown primary. Of the distant sites, lung, kidney and breast accounted for more than four-fifths (Table 5.6); only four cases were from the prostate, but it is perhaps underrecognised [306]. Metastases to the submandibular glands are less common than to the parotids but are more likely to be from distant sites [307].
Clinical aspects
Patients are usually older with a clinical history of cutaneous resection of a tumor. Salivary gland (mostly parotid) swelling is the typical clinical presentation.
Macroscopy
Poorly circumscribed solid and cystic tumor with areas of necrosis.
Microscopy
The appearance is varied depending on the nature of the primary. Sometimes the primary site cannot be identified, and the tumor may have originated from the parotid [308, 309].
Differential diagnosis
Metastases in the salivary glands can resemble almost any primary tumor, so that, for example, mammary duct carcinoma is morphologically identical (but immunohistochemically different) to SDC (see Sect. 5.9.11). Similarly, renal cell carcinoma is part of the differential diagnosis of any clear cell tumor of the salivary glands, and examples of prostate carcinoma have been mistaken for AciCC [306]. Immunohistochemistry is of some value and can identify prostate and thyroid primaries and melanoma with a reasonable degree of accuracy. Unlike most primary malignant salivary tumors, renal cell carcinomas are usually negative with cytokeratin 7; in contrast, CD10 stains most kidney carcinomas but is only positive in salivary tumors with myoepithelial differentiation. However, the possibility of metastasis is still best confirmed or excluded by imaging techniques of the kidneys.
Treatment and prognosis
Surgery of salivary gland and neck dissection is the elective treatment. The long-term survival is usually poor, as the salivary glands are often only affected when metastatic dissemination is widespread.
5.9.24 Hybrid Carcinoma
Definition
Hybrid tumors are defined as two separate types of tumor, each of which conforms to an exactly defined category, arising at a single site.
Epidemiology
They are rare, comprising <0.1 % of neoplasms of salivary tumors [310].
Etiology and pathogenesis
Some authors have speculated that hybrid tumors arise from intercalated duct lesions (adenomas and hyperplasia) with differentiation down two separate pathways [28, 29].
Clinical aspects
The clinical features depend largely on the aggressiveness of the component tumor entities.
Macroscopy
The reported tumor size ranged between 20 and 100 mm with a mean size of 40 mm.
Microscopy
The appearance will be that of the component tumors, not infrequently a combination of adenoid cystic and EMCs.
Differential diagnosis
The most important differential diagnosis is with carcinoma with high-grade transformation CS which typically shows multiple differentiation and CXPA (see Sects. 5.9.19, 5.9.14.1 and 5.9.14.3).
Treatment and prognosis
Hybrid carcinomas are treated surgically. The prognosis depends on the aggressiveness of the individual components [310].
5.9.25 Endodermal Sinus Tumor
Definition
Endodermal sinus tumor (EST) (yolk sac tumor) is an aggressive malignant germ cell-derived neoplasms characterised by the presence of Schiller-Duval bodies admixed with papillae, tubules, microcysts and sheets of primitive cells within myxoid extracellular background.
Epidemiology and clinical presentation
ESTs are very aggressive malignant tumors with short survival time. ESTs were documented in both adults and children. Within the head and neck area, these tumors occur mostly in sinonasal tract and in the nasopharynx. There are only two reports of primary EST of the parotid gland. One that recurred after chemotherapy was in a 2-year-old girl [311] and the other in a 16-month-old girl, who is alive and well 2 years after chemotherapy [312].
Microscopy
Histologically, the tumor often consists of reticular pattern characterised by anastomosing small glandular spaces. In other places, the tumor may be composed of microcystic, solid and papillary structures lined by irregular neoplastic cell. PAS-positive diastase-resistant intracellular and extracellular globules are present.
Immunohistochemistry
The tumor cells are positive for alpha-fetoprotein (AFP) and placental alkaline phosphatase (PLAP).
Differential diagnosis
In differential diagnosis immature teratoma, sialoblastoma and poorly differentiated adenocarcinoma should be considered. Schiller-Duval bodies and positive staining for alpha-fetoprotein characterise EST. Particularly immature teratomas with papillary areas may be reminiscent of EST but must be distinguished because their prognosis in children is favourable after complete resection.
Treatment and prognosis
ESTs in children are very aggressive neoplasms that require adjuvant cisplatin-based chemotherapy. The serum AFP is elevated, and it returns to normal levels after surgical resection of the EST.
5.9.26 Sialoblastoma
Definition
Sialoblastoma is low-grade malignant neoplasm usually present at birth or shortly thereafter, composed of epithelial basaloid and myoepithelial cells that recapitulate primitive salivary gland anlage.
Epidemiology
Sialoblastoma was first reported in 1996 by Vawter and Tefft [313] who used the term embryoma. Since that time, approximately 40 tumors that fit into the definition of sialoblastoma were reported under different names, such as congenital BCA, congenital hybrid BCA/AdCC and sialoblastoma [314].
Clinical presentation
Sialoblastoma arises almost exclusively in the perinatal period with only exceptionally rare cases presenting after 2 years of age [315].
Macroscopy
Grossly, the tumors range up to 15 cm in greatest dimension and are well circumscribed and even partly encapsulated. In other cases, they may be locally invasive with extension to adjacent soft tissues and bone.
Microscopy
Microscopically, sialoblastoma is composed of numerous solid hypercellular islands of primitive basaloid cells, some with peripheral palisading, and often with small central ducts (Fig. 5.79) [316]. The tumors have variable histological patterns, composed of variably sized nests and solid sheets of basaloid cells with focal ductal differentiation and cystic and microcystic change. The tumor cells are fairly uniform with minimal cytoplasm and round-to-oval nuclei with only slight polymorphism. Mitoses are may be numerous, but none is atypical. Neural and occasionally vascular invasion may be found (Fig. 5.80). On immunohistochemistry anti-cytokeratin and EMA antibodies stain ductal elements and occasional basaloid epithelial cells in the solid nests. Luminal cells express S-100 protein and actin [316].

Sialoblastoma is composed of solid hypercellular islands of primitive basaloid cells, some with peripheral palisading, and often with small central ducts

Sialoblastoma. Neural and occasionally vascular invasion may be found
Differential diagnosis
PA is exceedingly rare in neonatal age group and is distinguished by chondromyxoid stroma and combination of epithelial and myoepithelial cells with duct formation and metaplastic changes. BCA is also very rare in neonatal population, and it consists of uniform basaloid cells without mitoses and polymorphism. AdCC is vanishingly rare in the neonatal age group; it is characterised by invasive growth and formation of abundant extracellular matrix presenting with cribriform and pseudocystic patterns.
Treatment and prognosis
Criteria for malignancy include invasion of nerves or vascular spaces, necrosis and marked cytological atypia [317]. Of 15 reported cases, 4 had recurrences and another metastases to regional lymph nodes.
5.10 Benign and Malignant Lymphoid Infiltrates
5.10.1 Lymphoepithelial Sialadenitis (Sjögren’s Syndrome-Type Sialadenitis)
Definition
Lymphoepithelial sialadenitis (LESA) is a destructive autoimmune lymphoid infiltrate affecting mainly salivary and lacrimal glands, in most cases correlating or progressing to sicca syndrome, clinically called Sjögren’s syndrome (SS).
Epidemiology
The histological correlate of the clinical disease entity SS has long been characterised by a confusing terminology, embracing terms like Mikulicz syndrome, myoepithelial sialadenitis and benign lymphoepithelial lesion, none of which was satisfactory [318]. Recently, it has been shown that the original case report by Mikulicz in 1896 has been a MALT lymphoma with multifocal manifestation in salivary glands [319]. The term myoepithelial sialadenitis also proved to be inaccurate as myoepithelial cells are not involved in the pathogenesis of the lymphoepithelial lesions/islands, previously called ‘epimyoepithelial islands’ [320]. In 1999 Harris et al. introduced the much more accurate term lymphoepithelial sialadenitis (LESA) [9], and this has gained general acceptance and will be used here. About 80 % of patients with LESA are female, with a mean age at presentation of 55 years.
Etiology and pathogenesis
LESA is considered to be an autoimmune disease [321–323] of unknown etiology. Several viruses have been implicated [324], but they act probably only as co-factors. Recent data suggest that low vitamin D levels in patients with SS may be more associated with complications such as lymphoma and peripheral neuropathy [325].
Clinical aspects
SS represents a clinical constellation of dry mouth and dry eyes, and it should not be used as a histopathological term. It is often associated with other autoimmune diseases, most frequently rheumatoid arthritis and less frequently scleroderma, lupus erythematosus, Hashimoto’s thyroiditis and chronic active hepatitis. There is a major, however not total, overlap with LESA: most patients with the clinical diagnosis of Sjögren’s syndrome develop the typical histological features of LESA, and most patients with LESA develop the clinical features of SS, but not all [326].
Generally, all salivary glands are involved; however, clinical manifestation with tumorous, painless and mostly bilateral swellings is most frequent and most intense in the parotid glands [321, 326]. Tumor-like lesions and, hence surgical resections, of other salivary glands due to LESA are rare.
Macroscopy
Tumorous enlargement of glands with preserved lobular architecture.
Microscopy
In the early stages of LESA, striated ducts are surrounded by a lymphoid infiltrate with germinal centres. B cells concentrate around the ducts and intensely infiltrate the epithelium, unlike many non-autoimmune chronic inflammatory infiltrates. Many B cells are of monocytoid or centrocyte-like type, without cellular atypia [327]. A strong plasma cell component and many T lymphocytes may be present. With advanced lymphocytic infiltration, most striated ducts transform into lymphoepithelial lesions, representing a total functional destruction of striated ducts (Fig. 5.81) [42, 318, 320, 327, 328]. These were previously inaccurately called epimyoepithelial islands [320]. As the disease progresses, the acini become atrophied and are finally totally replaced by lymphoid tissue with still preserved lobular architecture. This leads to clinical enlargement of the salivary glands and sicca syndrome. Monoclonality by PCR can be demonstrated in up to 60 % of cases with LESA [329], but this alone is obviously insufficient for a diagnosis of lymphoma [51] (Table 5.7).

Sjögren’s syndrome-type lymphoepithelial sialadenitis of parotid gland: keratin stain identifies multiple, tightly packed lymphoepithelial lesions, embedded in reactive lymphocytic infiltration with germinal centres (arrows)
The degree of infiltration in minor salivary glands is usually less intense than in parotid glands, and lymphoepithelial duct lesions are lacking. Although lymphocytic infiltration in labial glands is not specific for LESA, a semi-quantitative assessment of the amount of inflammation in a lip biopsy (so-called focus score) is advocated as part of the investigation of patients with sicca syndrome [330].
Differential diagnosis
Cystic lymphoepithelial lesion of AIDS histologically is very similar to lymphoepithelial sialadenitis but is characterised by hyperplastic and bizarre-shaped secondary follicles and intense multifocal cystic dilatation of lymphoepithelial duct lesions [15]. Sporadic lymphoepithelial cysts of the parotid gland are a solitary cystic process without the clinical and serological characteristic of SS. The distinction of LESA from associated marginal zone B-cell lymphoma is crucial (see Sect. 5.10).
Treatment and prognosis
There is still a lack of treatment for Sjögren’s syndrome patients. Different types of stimulation of saliva production and of substitution of saliva are recommended. There is usually a slow deterioration of the sicca syndrome. The major complication is transformation into lymphoma (see Sect. 5.10.2).
5.10.2 Sjögren Syndrome-Associated Marginal Zone Lymphoma
Definition
Marginal zone lymphoma (MALT) developing in a background of LESA/Sjögren’s syndrome.
Epidemiology
Overall, extranodal and nodal lymphomas represented 16 % of all malignant tumors of the major salivary glands at the AFIP [48, 331]. About half of lymphomas manifesting in salivary glands represent marginal zone B-cell lymphoma (of MALT type), which is the preferred terminology of the current WHO classification of lymphomas [332]. The vast majority develop in long-standing LESA/syndromes.
Clinical aspects
Most present clinically as gradual and painless parotid enlargement, sometimes bilateral [333].
Etiology and pathogenesis
The histopathology of MALT lymphoma is intimately linked with that of LESA from which it usually develops – the risk of lymphoma in LESA has been estimated at approximately 4–7 % [329]. MALT lymphoma begins as an antigen-driven lymphoid proliferation in long-standing LESA with acquisition of secondary genetic changes and slow transformation to MALT lymphoma, which can pose significant diagnostic problems in early transformational stages [327, 334].
Microscopy
A restricted proliferation of marginal zone B cells to form a narrow, so-called halo around the lymphoepithelial lesions still is a physiological feature of LESA. The prerequisite to diagnose an associated MALT lymphoma is broad and focally coalescing halos of monocytoid or centrocyte-like B lymphocytes. Fully developed lymphomas are characterised by a confluent monomorphous expansion of B lymphocytes, usually involving colonisation of secondary follicles (Fig. 5.82) [10, 327, 335]. Immunohistological evidence of light chain restriction within the tumorous lymphomatous expansion is more helpful as a diagnostic criterion for manifest lymphoma as is monoclonality in PCR, which is often also positive in reactive LESA. Transformation into blastic/high-grade B-cell lymphoma is rare [333].

Sjögren’s syndrome-associated marginal zone (MALT) lymphoma: the keratin-stained, Sjögren’s syndrome-associated lymphoepithelial lesions are widely separated by expanding lymphoma areas (bright Hemalaun counterstain: confluent right and focal around lesions on the left, arrows); the dark blue areas represent remnants of pre-existent reactive lymphoepithelial sialadenitis
Prognosis and treatment
Sjögren’s syndrome-associated MALT lymphoma restricted to the salivary glands is an indolent disease that is often curable with local treatment [48, 331]. General lymphadenopathy and bone marrow involvement are unusual in these MALT lymphomas. Prognosis remains favourable even in the presence of other extranodal manifestation, including the bone marrow. Rituximab (anti-CD20) therapy, with or without additional chemotherapy, has been shown to be effective. Radiotherapy may aggravate the existing sicca syndrome and should be avoided.
5.10.3 Other Types of Malignant Lymphoma
Non-MALT-type lymphomas in salivary glands – especially in the parotid glands – in the majority of cases represent nodal lymphomas involving intraparotid lymph nodes. The most frequent lymphomas are follicular lymphoma and diffuse large B-cell lymphoma. They are classified according to nodal lymphomas [10, 336–338].
5.11 Other Tumors
A variety of soft tissue and other non-salivary neoplasms may rarely present as tumors of the salivary glands. These include solitary fibrous tumor, granular cell tumor, follicular dendritic cell sarcoma, inflammatory pseudotumor (inflammatory myofibroblastic tumor), primary malignant melanoma, primitive neuroectodermal tumor (PNET) and teratoma.
5.12 Unclassified Tumors
The 2005 WHO classification defined this group as benign or malignant tumors that cannot be placed in any of the categories [67]. This designation may be unavoidable if only a small quantity of tissue is available for study.
References
Martinez-Madrigal F, Micheau C. Histology of the major salivary glands. Am J Surg Pathol. 1989;13(10):879–99.
Ihrler S, et al. A morphogenetic concept of salivary duct regeneration and metaplasia. Virchows Arch. 2002;440(5):519–26.
Ihrler S, et al. Regeneration in chronic sialadenitis: an analysis of proliferation and apoptosis based on double immunohistochemical labelling. Virchows Arch. 2004;444(4):356–61.
Prasad AR, et al. The myoepithelial immunophenotype in 135 benign and malignant salivary gland tumors other than pleomorphic adenoma. Arch Pathol Lab Med. 1999;123(9):801–6.
Foschini MP, et al. Differential expression of myoepithelial markers in salivary, sweat and mammary glands. Int J Surg Pathol. 2000;8(1):29–37.
Jones H, Moshtael F, Simpson RH. Immunoreactivity of alpha smooth muscle actin in salivary gland tumors: a comparison with S100 protein. J Clin Pathol. 1992;45(10):938–40.
Batsakis JG, el-Naggar AK. Sebaceous lesions of salivary glands and oral cavity. Ann Otol Rhinol Laryngol. 1990;99(5 Pt 1):416–8.
Auclair PL. Tumor-associated lymphoid proliferation in the parotid gland. A potential diagnostic pitfall. Oral Surg Oral Med Oral Pathol. 1994;77(1):19–26.
Harris NL. Lymphoid proliferations of the salivary glands. Am J Clin Pathol. 1999;111(1 Suppl 1):S94–103.
Ihrler S, et al. Pattern recognition in the differential diagnosis of salivary lymphoepithelial lesions. Pathologe. 2009;30(6):432–41.
Seifert G. Primary salivary gland tumors in lymph nodes of the parotid gland. Report of 3 cases and review of the literature. Pathologe. 1997;18(2):141–6.
Harrison J. Histology and pathology of sialolithiasis. In: Surgical and medical management. New York: Thieme; 2006. p. 71–8.
Harrison JD. Causes, natural history, and incidence of salivary stones and obstructions. Otolaryngol Clin North Am. 2009;42(6):927–47. Table of Contents.
Werning J. Infectious and systemic diseases. In: Auclair P, Ellis GL, Gnepp DR, editors. Surgical pathology of the salivary glands. Philadelphia: Saunders; 1991.
Ihrler S, et al. HIV-related parotid lymphoepithelial cysts. Immunohistochemistry and 3-D reconstruction of surgical and autopsy material with special reference to formal pathogenesis. Virchows Arch. 1996;429(2–3):139–47.
Jeffers L, Webster-Cyriaque JY. Viruses and salivary gland disease (SGD): lessons from HIV SGD. Adv Dent Res. 2011;23(1):79–83.
Geyer JT, et al. Chronic sclerosing sialadenitis (Kuttner tumor) is an IgG4-associated disease. Am J Surg Pathol. 2010;34(2):202–10.
Strehl JD, Hartmann A, Agaimy A. Numerous IgG4-positive plasma cells are ubiquitous in diverse localised non-specific chronic inflammatory conditions and need to be distinguished from IgG4-related systemic disorders. J Clin Pathol. 2011;64(3):237–43.
Harrison JD, Rodriguez-Justo M. Commentary on IgG4-related sialadenitis: Mikulicz’s disease, Kuttner’s tumor, and eponymy. Histopathology. 2011;58(7):1164–6.
Harrison JD, Rodriguez-Justo M. IgG4-related sialadenitis is rare: histopathological investigation of 129 cases of chronic submandibular sialadenitis. Histopathology. 2013;63(1):96–102.
Foucar E, Rosai J, Dorfman R. Sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease): review of the entity. Semin Diagn Pathol. 1990;7(1):19–73.
Herold J, Nicholson AG. Fine needle aspiration cytology in the diagnosis of amyloid in the submandibular gland. Br J Oral Maxillofac Surg. 1992;30(6):393–4.
Brannon RB, Fowler CB, Hartman KS. Necrotizing sialometaplasia. A clinicopathologic study of sixty-nine cases and review of the literature. Oral Surg Oral Med Oral Pathol. 1991;72(3):317–25.
Batsakis JG, Manning JT. Necrotizing sialometaplasia of major salivary glands. J Laryngol Otol. 1987;101(9):962–6.
Ihrler S, et al. Pathogenesis of sialadenosis: possible role of functionally deficient myoepithelial cells. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;110(2):218–23.
Buchner A, et al. Adenomatoid hyperplasia of minor salivary glands. Oral Surg Oral Med Oral Pathol. 1991;71(5):583–7.
Di Palma S. Epithelial-myoepithelial carcinoma with co-existing multifocal intercalated duct hyperplasia of the parotid gland. Histopathology. 1994;25(5):494–6.
Chetty R. Intercalated duct hyperplasia: possible relationship to epithelial-myoepithelial carcinoma and hybrid tumors of salivary gland. Histopathology. 2000;37(3):260–3.
Weinreb I, et al. Intercalated duct lesions of salivary gland: a morphologic spectrum from hyperplasia to adenoma. Am J Surg Pathol. 2009;33(9):1322–9.
Konings AW, Coppes RP, Vissink A. On the mechanism of salivary gland radiosensitivity. Int J Radiat Oncol Biol Phys. 2005;62(4):1187–94.
Chan JKC, Tang S, Tsang WYW, Lee KC, Batsakis JG. Histologic changes induced by fine-needle aspiration. Adv Anat Pathol. 1996;3:71–90.
Eveson JW, Cawson RA. Infarcted (‘infected’) adenolymphomas. A clinicopathological study of 20 cases. Clin Otolaryngol Allied Sci. 1989;14(3):205–10.
Li S, et al. Worrisome histologic alterations following fine-needle aspiration of benign parotid lesions. Arch Pathol Lab Med. 2000;124(1):87–91.
Di Palma S, et al. Metaplastic (infarcted) Warthin’s tumor of the parotid gland: a possible consequence of fine needle aspiration biopsy. Histopathology. 1999;35(5):432–8.
Shintaku M, Honda T. Identification of oncocytic lesions of salivary glands by anti-mitochondrial immunohistochemistry. Histopathology. 1997;31(5):408–11.
Mukunyadzi P, et al. Tissue effects of salivary gland fine-needle aspiration. Does this procedure preclude accurate histologic diagnosis? Am J Clin Pathol. 2000;114(5):741–5.
Palmer TJ, et al. Oncocytic adenomas and oncocytic hyperplasia of salivary glands: a clinicopathological study of 26 cases. Histopathology. 1990;16(5):487–93.
Pereira L, et al. Somatic mitochondrial DNA mutations in cancer escape purifying selection and high pathogenicity mutations lead to the oncocytic phenotype: pathogenicity analysis of reported somatic mtDNA mutations in tumors. BMC Cancer. 2012;12:53.
Brandwein MS, Huvos AG. Oncocytic tumors of major salivary glands. A study of 68 cases with follow-up of 44 patients. Am J Surg Pathol. 1991;15(6):514–28.
Sato S, et al. Multifocal nodular oncocytic hyperplasia of bilateral parotid glands: a case report with a histological variant of clear cells. Pathol Res Pract. 2011;207(7):452–5.
Kontaxis A, et al. Diffuse hyperplastic oncocytosis of the parotid gland. Laryngorhinootologie. 2004;83(3):185–8.
Seifert G. Tumor-like lesions of the salivary glands. The new WHO classification. Pathol Res Pract. 1992;188(7):836–46.
Seifert G, Thomsen S, Donath K. Bilateral dysgenetic polycystic parotid glands. Morphological analysis and differential diagnosis of a rare disease of the salivary glands. Virchows Arch A Pathol Anat Histol. 1981;390(3):273–88.
Smyth AG, Ward-Booth RP, High AS. Polycystic disease of the parotid glands: two familial cases. Br J Oral Maxillofac Surg. 1993;31(1):38–40.
Davis PB. Cystic fibrosis since 1938. Am J Respir Crit Care Med. 2006;173(5):475–82.
Villella VR, et al. Targeting the intracellular environment in cystic fibrosis: restoring autophagy as a novel strategy to circumvent the CFTR defect. Front Pharmacol. 2013;4:1.
Vinayachandran D, Sankarapandian S. Salivary duct cyst: histo-pathologic correlation. J Clin Imaging Sci. 2013;3 Suppl 1:3.
Ellis GL, Auclair P. Tumors of the salivary glands. In: Atlas of tumor pathology. Washington, DC: AFIP; 2008.
Jensen J. Idiopathic diseases. In: Auclair P, Ellis GL, Gnepp DR, editors. Surgical pathology of the salivary glands. Philadelphia: Saunders; 1991.
Elliott JN, Oertel YC. Lymphoepithelial cysts of the salivary glands. Histologic and cytologic features. Am J Clin Pathol. 1990;93(1):39–43.
Jaffe ES. Lymphoid lesions of the head and neck: a model of lymphocyte homing and lymphomagenesis. Mod Pathol. 2002;15(3):255–63.
Smith BC, et al. Sclerosing polycystic adenosis of major salivary glands. A clinicopathologic analysis of nine cases. Am J Surg Pathol. 1996;20(2):161–70.
Skalova A, et al. Clonal nature of sclerosing polycystic adenosis of salivary glands demonstrated by using the polymorphism of the human androgen receptor (HUMARA) locus as a marker. Am J Surg Pathol. 2006;30(8):939–44.
Skalova A, et al. Sclerosing polycystic adenosis of parotid gland with dysplasia and ductal carcinoma in situ. Report of three cases with immunohistochemical and ultrastructural examination. Virchows Arch. 2002;440(1):29–35.
Petersson F, Tan PH, Hwang JS. Sclerosing polycystic adenosis of the parotid gland: report of a bifocal, paucicystic variant with ductal carcinoma in situ and pronounced stromal distortion mimicking invasive carcinoma. Head Neck Pathol. 2011;5(2):188–92.
Gnepp DR. Sclerosing polycystic adenosis of the salivary gland: a lesion that may be associated with dysplasia and carcinoma in situ. Adv Anat Pathol. 2003;10(4):218–22.
Gnepp DR, et al. Sclerosing polycystic adenosis of the salivary gland: a report of 16 cases. Am J Surg Pathol. 2006;30(2):154–64.
Canas Marques R, Felix A. Invasive carcinoma arising from sclerosing polycystic adenosis of the salivary gland. Virchows Arch. 2014;464(5):621–5.
Pieterse AS, Seymour AE. Parotid cysts. An analysis of 16 cases and suggested classification. Pathology. 1981;13(2):225–34.
Islam S, Hoffman GR. Parotid dermoid cyst: a rare entity. J Laryngol Otol. 2009;123(2):e7.
Tas A, et al. Dermoid cyst of the parotid gland: first pediatric case. Int J Pediatr Otorhinolaryngol. 2010;74(2):216–7.
Nagao T, et al. Keratocystoma of the parotid gland: a report of two cases of an unusual pathologic entity. Mod Pathol. 2002;15(9):1005–10.
Huang XF, et al. Keratocystoma of the parotid gland: a clinicopathological study and literature review. Int J Oral Maxillofac Surg. 2012;41(2):256–60.
Simpson R. Myoepithelial tumors of the salivary glands. Curr Diagn Pathol. 2002;8:328–37.
Zarbo RJ, et al. Salivary gland basal cell and canalicular adenomas: immunohistochemical demonstration of myoepithelial cell participation and morphogenetic considerations. Arch Pathol Lab Med. 2000;124(3):401–5.
Zarbo RJ, Regezi JA, Batsakis JG. S-100 protein in salivary gland tumors: an immunohistochemical study of 129 cases. Head Neck Surg. 1986;8(4):268–75.
Barnes EL, Eveson J, Reichart P, Sidransky D. Tumors of the salivary glands. In: World Health Organization classification of tumors. Lyon; 2005.
Seifert G, Miehlke A, Haubrich J, Chilla R. Diseases of the salivary glands. Stuttgart: Thieme; 1986.
Eveson J. Oncocytic and squamous differentiation in salivary glands and tumors. Rev Esp Patol. 1999;32:433–4.
Skalova A, et al. Analysis of collagen isotypes in crystalloid structures of salivary gland tumors. Hum Pathol. 1992;23(7):748–54.
Di Palma S, et al. Oncocytic change in pleomorphic adenoma: molecular evidence in support of an origin in neoplastic cells. J Clin Pathol. 2007;60(5):492–9.
Skalova A, et al. Pleomorphic adenoma of the salivary glands with intravascular tumor deposits: a diagnostic pitfall. Am J Surg Pathol. 2012;36(11):1674–82.
Henriksson G, et al. Recurrent primary pleomorphic adenomas of salivary gland origin: intrasurgical rupture, histopathologic features, and pseudopodia. Cancer. 1998;82(4):617–20.
Dehner LP, Valbuena L, Perez-Atayde A, Reddick RL, Askin FB, Rosai J. Salivary gland anlage tumor (“congenital pleomorphic adenoma”): a clinicopathologic, immunohistochemical and ultrastructural study of nine cases. Am J Surg Pathol. 1984;18:25–36.
Herrmann BW, Dehner LP, Lieu JE. Congenital salivary gland anlage tumor: a case series and review of the literature. Int J Pediatr Otorhinolaryngol. 2005;69(2):149–56.
Tinsa F, et al. Congenital salivary gland anlage tumor of the nasopharynx. Fetal Pediatr Pathol. 2010;29(5):323–9.
Gnepp DR, Henley J, Simpson RHW. Salivary and lacrimal glands. In: Diagnostic surgical pathology of the head and neck. 2nd ed. Saunders Elsevier, Philadelphia, PA; 2011.
Simpson RH, Jones H, Beasley P. Benign myoepithelioma of the salivary glands: a true entity? Histopathology. 1995;27(1):1–9.
Ogawa Y, et al. Plasmacytoid cells in salivary-gland pleomorphic adenomas: evidence of luminal cell differentiation. Virchows Arch. 2003;443(5):625–34.
Simpson R. Clear cell tumors. Rev Esp Patol. 1999;32:432–3.
Skalova A, et al. Spindle cell myoepithelial tumors of the parotid gland with extensive lipomatous metaplasia. A report of four cases with immunohistochemical and ultrastructural findings. Virchows Arch. 2001;439(6):762–7.
Alos L, et al. Myoepithelial tumors of salivary glands: a clinicopathologic, immunohistochemical, ultrastructural, and flow-cytometric study. Semin Diagn Pathol. 1996;13(2):138–47.
Lin HC, et al. Basal cell adenoma of the sublingual gland. Ann Otol Rhinol Laryngol. 2003;112(12):1066–8.
Veeresh M, et al. Basal cell adenoma of the submandibular gland. J Maxillofac Oral Surg. 2010;9(3):289–91.
Batsakis JG, Luna MA. Basaloid salivary carcinoma. Ann Otol Rhinol Laryngol. 1991;100(9 Pt 1):785–7.
Luna MA, Tortoledo ME, Allen M. Salivary dermal analogue tumors arising in lymph nodes. Cancer. 1987;59(6):1165–9.
Luna MA, et al. Carcinomas ex monomorphic adenoma of salivary glands. J Laryngol Otol. 1989;103(8):756–9.
Seifert G. Histological typing of salivary gland tumors. In: World Health Organization international histological classification of tumors. Berlin: Springer; 1991.
Honda K, et al. Clonal analysis of the epithelial component of Warthin’s tumor. Hum Pathol. 2000;31(11):1377–80.
Seifert G, Bull HG, Donath K. Histologic subclassification of the cystadenolymphoma of the parotid gland. Analysis of 275 cases. Virchows Arch A Pathol Anat Histol. 1980;388(1):13–38.
Batsakis JG, Sneige N, el-Naggar AK. Fine-needle aspiration of salivary glands: its utility and tissue effects. Ann Otol Rhinol Laryngol. 1992;101(2 Pt 1):185–8.
Skalova A, et al. Malignancy-simulating change in parotid gland oncocytoma following fine needle aspiration. Report of 3 cases. Pathol Res Pract. 1999;195(6):399–405.
Zhou CX, Gao Y. Oncocytoma of the salivary glands: a clinicopathologic and immunohistochemical study. Oral Oncol. 2009;45(12):e232–8.
Hyde J, et al. Bilateral multinodular oncocytomas of the parotid arising in a background of bilateral oncocytic nodular hyperplasia. Ear Nose Throat J. 2008;87(1):51–4.
Ellis G. Clear cell oncocytoma of salivary gland. Hum Pathol. 1988;19:862–7.
Agaimy A, et al. Lipomatous salivary gland tumors: a series of 31 cases spanning their morphologic spectrum with emphasis on sialolipoma and oncocytic lipoadenoma. Am J Surg Pathol. 2013;37(1):128–37.
McHugh JB, et al. p63 immunohistochemistry differentiates salivary gland oncocytoma and oncocytic carcinoma from metastatic renal cell carcinoma. Head Neck Pathol. 2007;1(2):123–31.
Weinreb I, et al. Ductal adenomas of salivary gland showing features of striated duct differentiation (‘striated duct adenoma’): a report of six cases. Histopathology. 2010;57(5):707–15.
Yuce S, et al. Canalicular adenoma of the palate. J Craniofac Surg. 2012;23(5):e396–8.
Oliveira-Santos C, et al. Asymptomatic nodules of the upper lip: report of a canalicular adenoma with immunoprofile presentation. Gerodontology. 2012;29(2):e1121–4.
Yoon AJ, et al. Bilateral canalicular adenomas of the upper lip. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;102(3):341–3.
Queiroz LM, et al. A rare salivary gland neoplasm: multiple canalicular adenoma; a case report. Auris Nasus Larynx. 2004;31(2):189–93.
Gnepp DR. My journey into the world of salivary gland sebaceous neoplasms. Head Neck Pathol. 2012;6(1):101–10.
Seethala RR, et al. Lymphadenoma of the salivary gland: clinicopathological and immunohistochemical analysis of 33 tumors. Mod Pathol. 2012;25(1):26–35.
Rawlinson NJ, Almarzooqi S, Nicol K. Sebaceous lymphadenoma of the parotid gland in a 13-year-old girl: a case report. Head Neck Pathol. 2010;4(2):144–7.
Brannon RB, Sciubba JJ, Giulani M. Ductal papillomas of salivary gland origin: a report of 19 cases and a review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;92(1):68–77.
Waldron CA, el-Mofty SK, Gnepp DR. Tumors of the intraoral minor salivary glands: a demographic and histologic study of 426 cases. Oral Surg Oral Med Oral Pathol. 1988;66(3):323–33.
Skalova A, et al. Oncocytic cystadenoma of the parotid gland with tyrosine-rich crystals. Pathol Res Pract. 2000;196(12):849–51.
Michal M, Skalova A, Mukensnabl P. Micropapillary carcinoma of the parotid gland arising in mucinous cystadenoma. Virchows Arch. 2000;437(4):465–8.
Chenevert J, et al. DOG1: a novel marker of salivary acinar and intercalated duct differentiation. Mod Pathol. 2012;25(7):919–29.
Skalova A, et al. Mammary analogue secretory carcinoma of salivary glands, containing the ETV6-NTRK3 fusion gene: a hitherto undescribed salivary gland tumor entity. Am J Surg Pathol. 2010;34(5):599–608.
Hellquist HB, et al. Tumor growth fraction and apoptosis in salivary gland acinic cell carcinomas. Prognostic implications of Ki-67 and bcl-2 expression and of in situ end labelling (TUNEL). J Pathol. 1997;181(3):323–9.
Skalova A, et al. Cell proliferation correlates with prognosis in acinic cell carcinomas of salivary gland origin. Immunohistochemical study of 30 cases using the MIB 1 antibody in formalin-fixed paraffin sections. J Pathol. 1994;173(1):13–21.
Skalova A, et al. Acinic cell carcinoma with high-grade transformation: a report of 9 cases with immunohistochemical study and analysis of TP53 and HER-2/neu genes. Am J Surg Pathol. 2009;33(8):1137–45.
Michal M, et al. Well-differentiated acinic cell carcinoma of salivary glands associated with lymphoid stroma. Hum Pathol. 1997;28(5):595–600.
Tognon C, et al. Expression of the ETV6-NTRK3 gene fusion as a primary event in human secretory breast carcinoma. Cancer Cell. 2002;2(5):367–76.
Bishop JA, et al. Most nonparotid “acinic cell carcinomas” represent mammary analog secretory carcinomas. Am J Surg Pathol. 2013;37(7):1053–7.
Connor A, et al. Mammary analog secretory carcinoma of salivary gland origin with the ETV6 gene rearrangement by FISH: expanded morphologic and immunohistochemical spectrum of a recently described entity. Am J Surg Pathol. 2012;36(1):27–34.
Chiosea SI, et al. Clinicopathological characterization of mammary analogue secretory carcinoma of salivary glands. Histopathology. 2012;61(3):387–94.
Laco J, et al. Mammary analog secretory carcinoma of salivary glands: a report of 2 cases with expression of basal/myoepithelial markers (calponin, CD10 and p63 protein). Pathol Res Pract. 2013;209(3):167–72.
Chenevert J, Barnes LE, Chiosea SI. Mucoepidermoid carcinoma: a five-decade journey. Virchows Arch. 2011;458(2):133–40.
Skalova A, et al. Mammary analogue secretory carcinoma of salivary glands with high-grade transformation: report of 3 cases with the ETV6-NTRK3 gene fusion and analysis of TP53, beta-catenin, EGFR, and CCND1 genes. Am J Surg Pathol. 2014;38(1):23–33.
Sultan I, et al. Salivary gland carcinomas in children and adolescents: a population-based study, with comparison to adult cases. Head Neck. 2011;33(10):1476–81.
Stenman G. Fusion oncogenes in salivary gland tumors: molecular and clinical consequences. Head Neck Pathol. 2013;7 Suppl 1:S12–9.
Jee KJ, et al. Genomic profiles and CRTC1-MAML2 fusion distinguish different subtypes of mucoepidermoid carcinoma. Mod Pathol. 2013;26(2):213–22.
Luna MA. Salivary mucoepidermoid carcinoma: revisited. Adv Anat Pathol. 2006;13(6):293–307.
Tian W, et al. IgG4(+) plasma cells in sclerosing variant of mucoepidermoid carcinoma. Am J Surg Pathol. 2012;36(7):973–9.
Brandwein MS, et al. Mucoepidermoid carcinoma: a clinicopathologic study of 80 patients with special reference to histological grading. Am J Surg Pathol. 2001;25(7):835–45.
Skalova A, et al. Prognostic significance of cell proliferation in mucoepidermoid carcinomas of the salivary gland: clinicopathological study using MIB 1 antibody in paraffin sections. Hum Pathol. 1994;25(9):929–35.
Goode RK, Auclair PL, Ellis GL. Mucoepidermoid carcinoma of the major salivary glands: clinical and histopathologic analysis of 234 cases with evaluation of grading criteria. Cancer. 1998;82(7):1217–24.
Altemani A, et al. Signet-ring cell change in adenoid cystic carcinoma: a clinicopathological and immunohistochemical study of four cases. Histopathology. 2013;62(4):531–42.
Skalova A, et al. Assessment of proliferative activity using the MIB1 antibody help to distinguish polymorphous low grade adenocarcinoma from adenoid cystic carcinoma of salivary glands. Pathol Res Pract. 1997;193(10):695–703.
Marchio C, Weigelt B, Reis-Filho JS. Adenoid cystic carcinomas of the breast and salivary glands (or ‘The strange case of Dr Jekyll and Mr Hyde’ of exocrine gland carcinomas). J Clin Pathol. 2010;63(3):220–8.
Wetterskog D, et al. Mutation profiling of adenoid cystic carcinomas from multiple anatomical sites identifies mutations in the RAS pathway, but no KIT mutations. Histopathology. 2013;62(4):543–50.
Brill 2nd LB, et al. Analysis of MYB expression and MYB-NFIB gene fusions in adenoid cystic carcinoma and other salivary neoplasms. Mod Pathol. 2011;24(9):1169–76.
Di Palma S, et al. Primary sinonasal adenoid cystic carcinoma presenting with skin metastases – genomic profile and expression of the MYB-NFIB fusion biomarker. Histopathology. 2014;64(3):453–5.
Ogawa I, et al. Pleomorphic adenoma with extensive adenoid cystic carcinoma-like cribriform areas of parotid gland. Pathol Int. 2003;53(1):30–4.
Vargas H, Kaplan S. Mixed tumor, polymorphous low-grade adenocarcinoma and ACC of the salivary gland: pathogenic implications and differential diagnosis by Ki-67 (MIB1), BCL2 and S100 immunohistochemistry. Appl Immunohistochem. 1997;5:8–16.
Szanto PA, et al. Histologic grading of adenoid cystic carcinoma of the salivary glands. Cancer. 1984;54(6):1062–9.
Seethala RR, et al. Adenoid cystic carcinoma with high-grade transformation: a report of 11 cases and a review of the literature. Am J Surg Pathol. 2007;31(11):1683–94.
Spiro RH, Huvos AG. Stage means more than grade in adenoid cystic carcinoma. Am J Surg. 1992;164(6):623–8.
Kokemueller H, et al. Adenoid cystic carcinoma of the head and neck – a 20 years experience. Int J Oral Maxillofac Surg. 2004;33(1):25–31.
Abu El-Naaj I, et al. Polymorphous low grade adenocarcinoma: case series and review of surgical management. J Oral Maxillofac Surg. 2011;69(7):1967–72.
Evans HL, Luna MA. Polymorphous low-grade adenocarcinoma: a study of 40 cases with long-term follow up and an evaluation of the importance of papillary areas. Am J Surg Pathol. 2000;24(10):1319–28.
Pogodzinski MS, et al. Retrospective study and review of polymorphous low-grade adenocarcinoma. Laryngoscope. 2006;116(12):2145–9.
Nagao T, et al. Polymorphous low-grade adenocarcinoma of the major salivary glands: report of three cases in an unusual location. Histopathology. 2004;44(2):164–71.
Tortoledo ME, Luna MA, Batsakis JG. Carcinomas ex pleomorphic adenoma and malignant mixed tumors. Histomorphologic indexes. Arch Otolaryngol. 1984;110(3):172–6.
Simpson RH, et al. Polymorphous low-grade adenocarcinoma of the salivary glands: a clinicopathological comparison with adenoid cystic carcinoma. Histopathology. 1991;19(2):121–9.
Castle JT, et al. Polymorphous low grade adenocarcinoma: a clinicopathologic study of 164 cases. Cancer. 1999;86(2):207–19.
Verma V, Mendenhall WM, Werning JW. Polymorphous low-grade adenocarcinoma of the head and neck. Am J Clin Oncol. 2014;37(6):624–6.
Edwards PC, Bhuiya T, Kelsch RD. C-kit expression in the salivary gland neoplasms adenoid cystic carcinoma, polymorphous low-grade adenocarcinoma, and monomorphic adenoma. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;95(5):586–93.
Kemp BL, et al. Terminal duct adenocarcinomas of the parotid gland. J Laryngol Otol. 1995;109(5):466–8.
Parrett TJ, Prasad A, Raslan WF, Kakar S, Lewis JE. Long term and life-long follow-up in polymorphous low grade adenocarcinoma. Mod Pathol. 2002;15:223.
Slootweg PJ. Low-grade adenocarcinoma of the oral cavity: polymorphous or papillary? J Oral Pathol Med. 1993;22(7):327–30.
Simpson RH, et al. Polymorphous low-grade adenocarcinoma of the salivary glands with transformation to high-grade carcinoma. Histopathology. 2002;41(3):250–9.
Michal M, et al. Cribriform adenocarcinoma of the tongue: a hitherto unrecognized type of adenocarcinoma characteristically occurring in the tongue. Histopathology. 1999;35(6):495–501.
Skalova A, et al. Cribriform adenocarcinoma of minor salivary gland origin principally affecting the tongue: characterization of new entity. Am J Surg Pathol. 2011;35(8):1168–76.
Borowski-Borowy P, et al. Cribriform adenocarcinoma of the tongue. Pol J Pathol. 2011;62(3):168–71.
Cocek A, et al. Cribriform adenocarcinoma of the base of the tongue and low-grade, polymorphic adenocarcinomas of the salivary glands. Oncol Lett. 2011;2(1):135–8.
Prasad KC, et al. Pedunculated cribriform adenocarcinoma of the base of the tongue. Ear Nose Throat J. 2004;83(1):62–4.
Laco J, et al. Cribriform adenocarcinoma of minor salivary glands may express galectin-3, cytokeratin 19, and HBME-1 and contains polymorphisms of RET and H-RAS proto-oncogenes. Virchows Arch. 2012;461(5):531–40.
Li CY, et al. Epithelial-myoepithelial carcinoma arising in pleomorphic adenoma of the palate. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;90(4):460–5.
Seethala RR, Barnes EL, Hunt JL. Epithelial-myoepithelial carcinoma: a review of the clinicopathologic spectrum and immunophenotypic characteristics in 61 tumors of the salivary glands and upper aerodigestive tract. Am J Surg Pathol. 2007;31(1):44–57.
Mantesso A, et al. Analysis of epithelial-myoepithelial carcinoma based on the establishment of a novel cell line. Oral Oncol. 2003;39(5):453–8.
Cheung FM, Hioe F, Kong JH. Histologic variant of the epithelial-myoepithelial carcinoma of the salivary gland: a case report. Head Neck. 1995;17(5):437–44.
Seethala RR. Oncocytic and apocrine epithelial myoepithelial carcinoma: novel variants of a challenging tumor. Head Neck Pathol. 2013;7 Suppl 1:S77–84.
Shinozaki A, et al. Sebaceous epithelial-myoepithelial carcinoma of the salivary gland: clinicopathologic and immunohistochemical analysis of 6 cases of a new histologic variant. Am J Surg Pathol. 2008;32(6):913–23.
Simpson RH, et al. Epithelial-myoepithelial carcinoma of salivary glands. J Clin Pathol. 1991;44(5):419–23.
Cardesa A, Slootweg P, editors. Major and minor salivary glands. In: Pathology of the head and neck. Berlin: Springer; 2006.
Fonseca I, Soares J. Epithelial-myoepithelial carcinoma of the salivary glands. A study of 22 cases. Virchows Arch A Pathol Anat Histopathol. 1993;422(5):389–96.
Alos L, et al. High-grade carcinoma component in epithelial-myoepithelial carcinoma of salivary glands clinicopathological, immunohistochemical and flow-cytometric study of three cases. Virchows Arch. 1999;434(4):291–9.
Roy P, et al. Epithelial-myoepithelial carcinoma with high grade transformation. Am J Surg Pathol. 2010;34(9):1258–65.
Weinreb I. Hyalinizing clear cell carcinoma of salivary gland: a review and update. Head Neck Pathol. 2013;7 Suppl 1:S20–9.
Wang B, et al. Primary salivary clear cell tumors – a diagnostic approach: a clinicopathologic and immunohistochemical study of 20 patients with clear cell carcinoma, clear cell myoepithelial carcinoma, and epithelial-myoepithelial carcinoma. Arch Pathol Lab Med. 2002;126(6):676–85.
Simpson RH, et al. Clear cell carcinoma of minor salivary glands. Histopathology. 1990;17(5):433–8.
Milchgrub S, et al. Hyalinizing clear cell carcinoma of salivary gland. Am J Surg Pathol. 1994;18(1):74–82.
Dardick I, Leong I. Clear cell carcinoma: review of its histomorphogenesis and classification as a squamous cell lesion. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108(3):399–405.
Antonescu CR, Katabi N, Zhang L, Seethala RR, Jordan RC, Perez-Ordoñez B, Leong IT, Bradley G, Klieb H, Weinreb I. Rearrangement of the EWSR1 gene is a consistent feature in hyalinising clear cell carcinoma of salivary gland. Modern Pathol. 2011;24(Supplement 1):273.
Tanguay J, Weinreb I. What the EWSR1-ATF1 fusion has taught us about hyalinizing clear cell carcinoma. Head Neck Pathol. 2013;7(1):28–34.
Bilodeau EA, Weinreb I, Antonescu CR, Zhang L, Dacic S, Muller S, Barker B, Seethala RR. Clear cell odontogenic carcinomas show EWSR1 rearrangements: a novel finding and biological link to salivary clear cell carcinomas. Modern Pathol. 2012;25(Supplement 1):305.
O’Sullivan-Mejia ED, et al. Hyalinizing clear cell carcinoma: report of eight cases and a review of literature. Head Neck Pathol. 2009;3(3):179–85.
McCluggage G, et al. Basal cell adenocarcinoma of the submandibular gland. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995;79(3):342–50.
Petersen SK, et al. Basal cell adenocarcinoma of the sublingual gland. Ugeskr Laeger. 2010;172(7):551–2.
Jayakrishnan A, et al. Basal cell adenocarcinoma in minor salivary glands. Histopathology. 2003;42(6):610–4.
Farrell T, Chang YL. Basal cell adenocarcinoma of minor salivary glands. Arch Pathol Lab Med. 2007;131(10):1602–4.
Muller S, Barnes L. Basal cell adenocarcinoma of the salivary glands. Report of seven cases and review of the literature. Cancer. 1996;78(12):2471–7.
Antonescu CR, Terzakis JA. Multiple malignant cylindromas of skin in association with basal cell adenocarcinoma with adenoid cystic features of minor salivary gland. J Cutan Pathol. 1997;24(7):449–53.
Nagao T, et al. Basal cell adenocarcinoma of the salivary glands: comparison with basal cell adenoma through assessment of cell proliferation, apoptosis, and expression of p53 and bcl-2. Cancer. 1998;82(3):439–47.
Cui R, et al. Rare cerebral and pulmonary metastases from low-grade basal cell adenocarcinoma of the parotid gland. Clin Nucl Med. 2011;36(12):1124–6.
Savera AT, et al. Myoepithelial carcinoma of the salivary glands: a clinicopathologic study of 25 patients. Am J Surg Pathol. 2000;24(6):761–74.
Nagao T, et al. Salivary gland malignant myoepithelioma: a clinicopathologic and immunohistochemical study of ten cases. Cancer. 1998;83(7):1292–9.
Antonescu CR, et al. EWSR1-POU5F1 fusion in soft tissue myoepithelial tumors. A molecular analysis of sixty-six cases, including soft tissue, bone, and visceral lesions, showing common involvement of the EWSR1 gene. Genes Chromosomes Cancer. 2010;49(12):1114–24.
Antonescu CR, et al. EWSR1-ATF1 fusion is a novel and consistent finding in hyalinizing clear-cell carcinoma of salivary gland. Genes Chromosomes Cancer. 2011;50(7):559–70.
Shah AA, et al. EWSR1 genetic rearrangements in salivary gland tumors: a specific and very common feature of hyalinizing clear cell carcinoma. Am J Surg Pathol. 2013;37(4):571–8.
Skalova A, et al. Clear cell myoepithelial carcinoma of salivary glands showing EWSR1 rearrangement: molecular analysis of 94 salivary gland carcinomas with prominent clear cell component. Am J Surg Pathol. 2015;39(3):338–48.
Michal M, et al. Clear cell malignant myoepithelioma of the salivary glands. Histopathology. 1996;28(4):309–15.
Di Palma S, Guzzo M. Malignant myoepithelioma of salivary glands: clinicopathological features of ten cases. Virchows Arch A Pathol Anat Histopathol. 1993;423(5):389–96.
Salovaara E, et al. Management and outcome of salivary duct carcinoma in major salivary glands. Eur Arch Otorhinolaryngol. 2013;270(1):281–5.
Bahrami A, et al. An analysis of PLAG1 and HMGA2 rearrangements in salivary duct carcinoma and examination of the role of precursor lesions. Histopathology. 2013;63(2):250–62.
Hogg RP, Ayshford C, Watkinson JC. Parotid duct carcinoma arising in bilateral chronic sialadenitis. J Laryngol Otol. 1999;113(7):686–8.
Gill J, et al. Salivary duct carcinoma arising in IgG4-related autoimmune disease of the parotid gland. Hum Pathol. 2009;40(6):881–6.
Simpson RH. Salivary duct carcinoma: new developments – morphological variants including pure in situ high grade lesions; proposed molecular classification. Head Neck Pathol. 2013;7 Suppl 1:S48–58.
Simpson RH, et al. Mucin-rich variant of salivary duct carcinoma: a clinicopathologic and immunohistochemical study of four cases. Am J Surg Pathol. 2003;27(8):1070–9.
Brandwein MS, et al. Salivary duct carcinoma (cribriform salivary carcinoma of excretory ducts). A clinicopathologic and immunohistochemical study of 12 cases. Cancer. 1990;65(10):2307–14.
Nagao T, et al. Invasive micropapillary salivary duct carcinoma: a distinct histologic variant with biologic significance. Am J Surg Pathol. 2004;28(3):319–26.
Simpson RHW, Di Palma S. Carcinomas of the salivary gland. In: Underwood J, Pignatelli M, editors. Recent advances in histopathology. London: Royal Society of Medicine Press; 2007. p. 17–43.
Nagao T, et al. Sarcomatoid variant of salivary duct carcinoma: clinicopathologic and immunohistochemical study of eight cases with review of the literature. Am J Clin Pathol. 2004;122(2):222–31.
Simpson RH, Desai S, Di Palma S. Salivary duct carcinoma in situ of the parotid gland. Histopathology. 2008;53(4):416–25.
Nikitakis NG, et al. Immunohistochemical expression of cytokeratins 7 and 20 in malignant salivary gland tumors. Mod Pathol. 2004;17(4):407–15.
Kapadia SB, Barnes L. Expression of androgen receptor, gross cystic disease fluid protein, and CD44 in salivary duct carcinoma. Mod Pathol. 1998;11(11):1033–8.
Skalova A, et al. Expression of HER-2/neu gene and protein in salivary duct carcinomas of parotid gland as revealed by fluorescence in-situ hybridization and immunohistochemistry. Histopathology. 2003;42(4):348–56.
Di Palma S, et al. Salivary duct carcinomas can be classified into luminal androgen receptor-positive, HER2 and basal-like phenotypes*. Histopathology. 2012;61(4):629–43.
Williams MD, et al. Differential expression of hormonal and growth factor receptors in salivary duct carcinomas: biologic significance and potential role in therapeutic stratification of patients. Am J Surg Pathol. 2007;31(11):1645–52.
Barnes L, et al. Salivary duct carcinoma. Part II. Immunohistochemical evaluation of 13 cases for estrogen and progesterone receptors, cathepsin D, and c-erbB-2 protein. Oral Surg Oral Med Oral Pathol. 1994;78(1):74–80.
Moriki T, et al. Salivary duct carcinoma: cytologic characteristics and application of androgen receptor immunostaining for diagnosis. Cancer. 2001;93(5):344–50.
Fan CY, Wang J, Barnes EL. Expression of androgen receptor and prostatic specific markers in salivary duct carcinoma: an immunohistochemical analysis of 13 cases and review of the literature. Am J Surg Pathol. 2000;24(4):579–86.
Kay PA, Roche P, Olsen KD, Lewis JE. Salivary duct carcinoma: immunohistochemical analysis of androgen receptor, prostate markers and HER-2/neu oncoprotein in 40 cases. Mod Pathol. 2001;14:150.
Simpson RH, et al. Salivary duct adenocarcinoma. Histopathology. 1991;18(3):229–35.
Kuo YJ, Weinreb I, Perez-Ordonez B. Low-grade salivary duct carcinoma or low-grade intraductal carcinoma? Review of the literature. Head Neck Pathol. 2013;7 Suppl 1:S59–67.
Locati LD, Bossi B, Rinaldi GR, Bergamini CB, Quattrone Q, Staurengo S, Pilotti S, Licitra L. Anti-androgen therapy in recurrent and/or metastatic salivary glands carcinoma (RSGC). Ann Oncol. 2006;16:38.
Di Palma S, Whitaker S, Potter K, Pitkin L. Carcinoma ex pleomorphic adenoma successfully treated with trastuzumab and radiotherapy. Virchow Archiv. 2012;461 Suppl 1:S144.
Falchook GS, et al. Human epidermal receptor 2-amplified salivary duct carcinoma: regression with dual human epidermal receptor 2 inhibition and anti-vascular endothelial growth factor combination treatment. Head Neck. 2014;36(3):E25–7.
Griffith CC, et al. PIK3CA mutations and PTEN loss in salivary duct carcinomas. Am J Surg Pathol. 2013;37(8):1201–7.
Hui KK, et al. Salivary duct adenocarcinoma: a high grade malignancy. J Laryngol Otol. 1986;100(1):105–14.
Colmenero Ruiz C, Patron Romero M, Martin Perez M. Salivary duct carcinoma: a report of nine cases. J Oral Maxillofac Surg. 1993;51(6):641–6.
Guzzo M, et al. Salivary duct carcinoma: clinical characteristics and treatment strategies. Head Neck. 1997;19(2):126–33.
Delgado R, Klimstra D, Albores-Saavedra J. Low grade salivary duct carcinoma. A distinctive variant with a low grade histology and a predominant intraductal growth pattern. Cancer. 1996;78(5):958–67.
Brandwein-Gensler M, et al. Low-grade salivary duct carcinoma: description of 16 cases. Am J Surg Pathol. 2004;28(8):1040–4.
Weinreb I, et al. Low-grade intraductal carcinoma of salivary gland: report of 3 cases with marked apocrine differentiation. Am J Surg Pathol. 2006;30(8):1014–21.
Yakirevich E, et al. Primary mucin-producing tumors of the salivary glands: a clinicopathological and morphometric study. Histopathology. 2010;57(3):395–409.
Ghannoum JE, Freedman PD. Signet-ring cell (mucin-producing) adenocarcinomas of minor salivary glands. Am J Surg Pathol. 2004;28(1):89–93.
Esteva CJ, Slater L, Gnepp DR. Mucinous myoepithelioma, a previously unrecognized variant. Mod Pathol. 2012;92 Suppl 2:308.
Gnepp DR. Mucinous myoepithelioma, a recently described new myoepithelioma variant. Head Neck Pathol. 2013;7 Suppl 1:S85–9.
Zhou CX, et al. Primary oncocytic carcinoma of the salivary glands: a clinicopathologic and immunohistochemical study of 12 cases. Oral Oncol. 2010;46(10):773–8.
Lee TH, et al. Malignant transformation of a benign oncocytoma of the submandibular gland: a case report. Kaohsiung J Med Sci. 2010;26(6):327–32.
Therkildsen MH, et al. Malignant Warthin’s tumor: a case study. Histopathology. 1992;21(2):167–71.
Weiler C, et al. Carcinoma ex pleomorphic adenoma with special reference to the prognostic significance of histological progression: a clinicopathological investigation of 41 cases. Histopathology. 2011;59(4):741–50.
Di Palma S. Carcinoma ex pleomorphic adenoma, with particular emphasis on early lesions. Head Neck Pathol. 2013;7 Suppl 1:S68–76.
Chen HH, et al. Carcinoma ex pleomorphic adenoma of soft palate with cavernous sinus invasion. World J Surg Oncol. 2010;8:24.
Toluie S, Thompson LD. Sinonasal tract adenoid cystic carcinoma ex-pleomorphic adenoma: a clinicopathologic and immunophenotypic study of 9 cases combined with a comprehensive review of the literature. Head Neck Pathol. 2012;6(4):409–21.
LiVolsi VA, Perzin KH. Malignant mixed tumors arising in salivary glands. I. Carcinomas arising in benign mixed tumors: a clinicopathologic study. Cancer. 1977;39(5):2209–30.
Gnepp DR. Malignant mixed tumors of the salivary glands: a review. Pathol Annu. 1993;28(Pt 1):279–328.
Nagao K, et al. Histopathologic studies on carcinoma in pleomorphic adenoma of the parotid gland. Cancer. 1981;48(1):113–21.
Lewis JE, Olsen KD, Sebo TJ. Carcinoma ex pleomorphic adenoma: pathologic analysis of 73 cases. Hum Pathol. 2001;32(6):596–604.
Auclair PL, Ellis GL. Atypical features in salivary gland mixed tumors: their relationship to malignant transformation. Mod Pathol. 1996;9(6):652–7.
Ihrler S, et al. Intraductal carcinoma is the precursor of carcinoma ex pleomorphic adenoma and is often associated with dysfunctional p53. Histopathology. 2007;51(3):362–71.
Di Palma S. Malignancy in pleomorphic adenoma (malignant mixed tumor) of salivary glands. In: Proceedings in head and neck pathology. Ljubljana: University of Ljubljana; 2003.
El-Naggar AK, et al. Molecular genetic alterations in carcinoma ex-pleomorphic adenoma: a putative progression model? Genes Chromosomes Cancer. 2000;27(2):162–8.
Kujan O, et al. The expression of FHIT in salivary carcinoma ex pleomorphic adenoma. Anticancer Res. 2012;32(8):3147–52.
Antony J, et al. Carcinoma ex pleomorphic adenoma: a comprehensive review of clinical, pathological and molecular data. Head Neck Pathol. 2012;6(1):1–9.
Olsen KD, Lewis JE. Carcinoma ex pleomorphic adenoma: a clinicopathologic review. Head Neck. 2001;23(9):705–12.
Brandwein M, et al. Noninvasive and minimally invasive carcinoma ex mixed tumor: a clinicopathologic and ploidy study of 12 patients with major salivary tumors of low (or no?) malignant potential. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996;81(6):655–64.
Di Palma S, et al. Non-invasive (intracapsular) carcinoma ex pleomorphic adenoma: recognition of focal carcinoma by HER-2/neu and MIB1 immunohistochemistry. Histopathology. 2005;46(2):144–52.
Zhao J, et al. Prognostic factors affecting the clinical outcome of carcinoma ex pleomorphic adenoma in the major salivary gland. World J Surg Oncol. 2013;11(1):180.
Sharon E, Kelly RJ, Szabo E. Sustained response of carcinoma ex pleomorphic adenoma treated with trastuzumab and capecitabine. Head Neck Oncol. 2010;2:12.
Hashimoto K, et al. HER-2/neu gene amplification in carcinoma ex pleomorphic adenoma in relation to progression and prognosis: a chromogenic in-situ hybridization study. Histopathology. 2012;60(6b):E131–42.
DeRoche TC, Hoschar AP, Hunt JL. Immunohistochemical evaluation of androgen receptor, HER-2/neu, and p53 in benign pleomorphic adenomas. Arch Pathol Lab Med. 2008;132(12):1907–11.
Altemani A, et al. Carcinoma ex pleomorphic adenoma (CXPA): immunoprofile of the cells involved in carcinomatous progression. Histopathology. 2005;46(6):635–41.
Katabi N, et al. Prognostic factors of recurrence in salivary carcinoma ex pleomorphic adenoma, with emphasis on the carcinoma histologic subtype: a clinicopathologic study of 43 cases. Hum Pathol. 2010;41(7):927–34.
Felix A, et al. Intracapsular carcinoma ex pleomorphic adenoma. Report of a case with unusual metastatic behaviour. Oral Oncol. 2002;38(1):107–10.
Stephen J, et al. True malignant mixed tumors (carcinosarcoma) of salivary glands. Oral Surg Oral Med Oral Pathol. 1986;61(6):597–602.
Tanahashi J, et al. Carcinosarcoma ex recurrent pleomorphic adenoma of the submandibular gland. Apmis. 2007;115(6):789–94.
Petersson F, Loh KS. Carcinosarcoma ex non-recurrent pleomorphic adenoma composed of TTF-1 positive large cell neuroendocrine carcinoma and myofibrosarcoma: apropos a rare Case. Head Neck Pathol. 2013;7(2):163–70.
Vekony H, et al. Salivary gland carcinosarcoma: oligonucleotide array CGH reveals similar genomic profiles in epithelial and mesenchymal components. Oral Oncol. 2009;45(3):259–65.
Nouraei SA, et al. Metastasizing pleomorphic salivary adenoma. Arch Otolaryngol Head Neck Surg. 2006;132(7):788–93.
Santaliz-Ruiz LE, et al. Metastasizing pleomorphic adenoma: a fascinating enigma. Case Rep Med. 2012;2012:148103.
Manucha V, Ioffe OB. Metastasizing pleomorphic adenoma of the salivary gland. Arch Pathol Lab Med. 2008;132(9):1445–7.
Tarsitano A, et al. Metastasizing “benign” pleomorphic salivary adenoma: a dramatic case-report and literature review. J Craniomaxillofac Surg. 2014;268:42(8):1562–5.
Wenig BM, et al. Metastasizing mixed tumor of salivary glands. A clinicopathologic and flow cytometric analysis. Am J Surg Pathol. 1992;16(9):845–58.
Bradley PJ. ‘Metastasizing pleomorphic salivary adenoma’ should now be considered a low-grade malignancy with a lethal potential. Curr Opin Otolaryngol Head Neck Surg. 2005;13(2):123–6.
el-Naggar A, Batsakis JG, Kessler S. Benign metastatic mixed tumors or unrecognized salivary carcinomas? J Laryngol Otol. 1988;102(9):810–2.
Bae CH, Kim YD, Song SY. Benign pleomorphic adenoma of the soft palate metastasizing to the sphenoid sinus. Clin Exp Otorhinolaryngol. 2010;3(3):172–5.
Di Palma S, Skálová A. Malignancy in pleomorphic adenoma. Rev Esp Patol. 1999;32:431–2.
Gnepp DR, Brannon R. Sebaceous neoplasms of salivary gland origin. Report of 21 cases. Cancer. 1984;53(10):2155–70.
Gnepp DR. Sebaceous neoplasms of salivary gland origin: a review. Pathol Annu. 1983;18(Pt 1):71–102.
Wang H, et al. Sebaceous carcinoma of the oral cavity: a case report and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;110(2):e37–40.
Cohn ML, Callender DL, El-Naggar AK. Sebaceous carcinoma ex-pleomorphic adenoma: a rare phenotypic occurrence. Ann Diagn Pathol. 2004;8(4):224–6.
Altemani A, et al. Sebaceous carcinoma of the parotid gland in children: an immunohistochemical and ploidy study. Int J Oral Maxillofac Surg. 2008;37(5):433–40.
Claudius K, et al. A red cheek as first clinical sign of a sebaceous lymphadenocarcinoma of the parotid gland with lymphangiosis carcinomatosa and lymph node metastases. Am J Dermatopathol. 2011;33(4):e50–3.
Croitoru CM, Mooney JE, Luna MA. Sebaceous lymphadenocarcinoma of salivary glands. Ann Diagn Pathol. 2003;7(4):236–9.
Shukla M, Panicker S. Synchronous sebaceous lymphadenoma with squamous cell carcinoma – case report. World J Surg Oncol. 2003;1(1):30.
Ahn SH, Park SY. Sebaceous lymphadenocarcinoma of parotid gland. Eur Arch Otorhinolaryngol. 2006;263(10):940–2.
Albeck H, et al. Familial clusters of nasopharyngeal carcinoma and salivary gland carcinomas in Greenland natives. Cancer. 1993;72(1):196–200.
Gupta S, Loh KS, Petersson F. Lymphoepithelial carcinoma of the parotid gland arising in an intraglandular lymph node: report of a rare case mimicking metastasis. Ann Diagn Pathol. 2012;16(5):416–21.
Amit S, Agarwal A, Khan L. Cytomorphological features of lymphoepithelial carcinoma of submandibular gland in an adolescent male. J Cytol. 2012;29(3):216–8.
Nakao K, et al. Detection of Epstein-Barr virus in metastatic lymph nodes of patients with nasopharyngeal carcinoma and a primary unknown carcinoma. Arch Otolaryngol Head Neck Surg. 2003;129(3):338–40.
Spencer CR, et al. Lymphoepithelial carcinoma of the parotid gland: a rare neck lump. JRSM Short Rep. 2012;3(5):28.
Chong VF, Fan YF. Parotid gland involvement in nasopharyngeal carcinoma. J Comput Assist Tomogr. 1999;23(4):524–8.
Liu FY, et al. 18F-FDG PET can replace conventional work-up in primary M staging of nonkeratinizing nasopharyngeal carcinoma. J Nucl Med. 2007;48(10):1614–9.
Myers JN, Peel RL, Myers EN. Pathologic quiz case 1. Malignant lymphoepithelial lesion of the parotid gland. Arch Otolaryngol Head Neck Surg. 1995;121(4):479–82.
Gnepp DR, Corio RL, Brannon RB. Small cell carcinoma of the major salivary glands. Cancer. 1986;58(3):705–14.
Nagao T, et al. Small cell carcinoma of the major salivary glands: clinicopathologic study with emphasis on cytokeratin 20 immunoreactivity and clinical outcome. Am J Surg Pathol. 2004;28(6):762–70.
Chan JK, et al. Cytokeratin 20 immunoreactivity distinguishes Merkel cell (primary cutaneous neuroendocrine) carcinomas and salivary gland small cell carcinomas from small cell carcinomas of various sites. Am J Surg Pathol. 1997;21(2):226–34.
Batsakis JG, Luna MA. Undifferentiated carcinomas of salivary glands. Ann Otol Rhinol Laryngol. 1991;100(1):82–4.
Kraemer BB, Mackay B, Batsakis JG. Small cell carcinomas of the parotid gland. A clinicopathologic study of three cases. Cancer. 1983;52(11): 2115–21.
Chernock RD, Duncavage EJ, Gnepp DR, El-Mofty SK, Lewis J, editors. Absence of polyoma virus in primary parotid high grade neuroendocrine carcinomas. Modern Pathol. 2011;24(Suppl 1):276A
Cheuk W, et al. Immunostaining for thyroid transcription factor 1 and cytokeratin 20 aids the distinction of small cell carcinoma from Merkel cell carcinoma, but not pulmonary from extrapulmonary small cell carcinomas. Arch Pathol Lab Med. 2001;125(2):228–31.
Said-Al-Naief N, Sciandra K, Gnepp DR. Moderately differentiated neuroendocrine carcinoma (atypical carcinoid) of the parotid gland: report of three cases with contemporary review of salivary neuroendocrine carcinomas. Head and Neck Pathol. 2013;7(3):295–303.
Modlin IM, Shapiro MD, Kidd M. Primary carcinoid tumor of the parotid gland: a case report and review of the literature. Ear Nose Throat J. 2006;85(8):533–9.
Pang B, et al. Desmoplastic small round cell tumor of major salivary glands: report of 1 case and a review of the literature. Appl Immunohistochem Mol Morphol. 2011;19(1):70–5.
Yin WH, et al. Desmoplastic small round cell tumor of the submandibular gland – a rare but distinctive primary salivary gland neoplasm. Hum Pathol. 2010;41(3):438–42.
Dahlin DC, Beabout JW. Dedifferentiation of low-grade chondrosarcomas. Cancer. 1971;28(2):461–6.
Evans HL. Liposarcoma and atypical lipomatous tumors: a study of 66 cases followed for a minimum of 10 years. Surg Pathol. 1988;1:41–54.
Cheuk W, Chan JK, Ngan RK. Dedifferentiation in adenoid cystic carcinoma of salivary gland: an uncommon complication associated with an accelerated clinical course. Am J Surg Pathol. 1999;23(4):465–72.
Nagao T, et al. Dedifferentiated adenoid cystic carcinoma: a clinicopathologic study of 6 cases. Mod Pathol. 2003;16(12):1265–72.
Di Palma S, et al. Unilateral aneuploid dedifferentiated acinic cell carcinoma associated with bilateral-low grade diploid acinic cell carcinoma of the parotid gland. Virchows Arch. 1999;434(4):361–5.
Gnepp D. Metastatic disease to the major salivary glands. In: Auclair P, Ellis GL, Gnepp DR, editors. Surgical pathology of the salivary glands. Philadelphia: Saunders; 1991. p. 560–9.
Bergersen PJ, Kennedy PJ, Kneale KL. Metastatic tumors of the parotid region. Aust N Z J Surg. 1987;57(1):23–6.
Simpson RH, Skalova A. Metastatic carcinoma of the prostate presenting as parotid tumor. Histopathology. 1997;30(1):70–4.
Vessecchia G, Di Palma S, Giardini R. Submandibular gland metastasis of breast carcinoma: a case report and review of the literature. Virchows Arch. 1995;427(3):349–51.
Ying YL, Johnson JT, Myers EN. Squamous cell carcinoma of the parotid gland. Head Neck. 2006;28(7):626–32.
Nuyens M, et al. Metastatic disease to the parotid gland. Otolaryngol Head Neck Surg. 2006;135(6):844–8.
Croitoru CM, Suarez PA, Luna MA. Hybrid carcinomas of salivary glands. Report of 4 cases and review of the literature. Arch Pathol Lab Med. 1999;123(8):698–702.
Viva E, et al. Endodermal sinus (yolk sac) tumor of the parotid gland: a case report. Int J Pediatr Otorhinolaryngol. 1992;24(3):269–74.
Sredni ST, et al. Endodermal sinus tumor of the parotid gland in a child. Pediatr Dev Pathol. 2004;7(1):77–80.
Vawter GF, Tefft M. Congenital tumors of the parotid gland. Arch Pathol. 1966;82(3):242–5.
Taylor GP. Congenital epithelial tumor of the parotid-sialoblastoma. Pediatr Pathol. 1988;8(4):447–52.
Adkins GF. Low grade basaloid adenocarcinoma of salivary gland in childhood – the so-called hybrid basal cell adenoma – adenoid cystic carcinoma. Pathology. 1990;22(4):187–90.
Brandwein M, et al. Sialoblastoma: clinicopathological/immunohistochemical study. Am J Surg Pathol. 1999;23(3):342–8.
Batsakis JG, Frankenthaler R. Embryoma (sialoblastoma) of salivary glands. Ann Otol Rhinol Laryngol. 1992;101(11):958–60.
Simpson RH, Sarsfield P. Benign and malignant lymphoid lesions of the salivary glands. Curr Diagn Pathol. 1997;4:91–9.
Ihrler S, Harrison JD. Mikulicz’s disease and Mikulicz’s syndrome: analysis of the original case report of 1892 in the light of current knowledge identifies a MALT lymphoma. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;100(3):334–9.
Ihrler S, et al. Lymphoepithelial duct lesions in Sjogren-type sialadenitis. Virchows Arch. 1999;434(4):315–23.
Daniels T. Benign lymphoepithelial lesion and Sjogren’s syndrome. In: Auclair P, Ellis GL, Gnepp DR, editors. Surgical pathology of the salivary glands. Philadelphia: Saunders; 1991. p. 83–106.
Fox RI, Kang HI. Pathogenesis of Sjogren’s syndrome. Rheum Dis Clin North Am. 1992;18(3):517–38.
Mavragani CP, Moutsopoulos HM. Sjogren’s syndrome. Annu Rev Pathol. 2014;9:273–85.
Haddad J, et al. Lymphocytic sialadenitis of Sjogren’s syndrome associated with chronic hepatitis C virus liver disease. Lancet. 1992;339(8789):321–3.
Tincani A, et al. Novel aspects of Sjogren’s syndrome in 2012. BMC Med. 2013;11:93.
Gleeson MJ, Cawson RA, Bennett MH. Benign lymphoepithelial lesion: a less than benign disease. Clin Otolaryngol Allied Sci. 1986;11(1):47–51.
Isaacson PG, Norton A. Malignant lymphoma of the salivary glands. In: Norton A, Isaacson PG, editors. Extranodal lymphomas. Edinburgh: Churchill-Livingstone; 1994. p. 67–83.
Tzioufas AG, Kapsogeorgou EK, Moutsopoulos HM. Pathogenesis of Sjogren’s syndrome: what we know and what we should learn. J Autoimmun. 2012;39(1–2):4–8.
Quintana PG, et al. Salivary gland lymphoid infiltrates associated with lymphoepithelial lesions: a clinicopathologic, immunophenotypic, and genotypic study. Hum Pathol. 1997;28(7):850–61.
Daniels TE, Fox PC. Salivary and oral components of Sjogren’s syndrome. Rheum Dis Clin North Am. 1992;18(3):571–89.
Ellis GL, Auclair P. Malignant epithelial tumors. In: Atlas of tumor pathology. Washington, DC: AFIP; 1996.
Isaacson PG, Chott A, Nakamura S. Extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue (MALT lymphoma). In: Campo E, Swerdlow SH, Harris NL, et al., editors. WHO classification of tumors of haematopoetic and lymphoid tissue. Lyon: IARC; 2008. p. 214–9.
Giannouli S, Voulgarelis M. Predicting progression to lymphoma in Sjogren’s syndrome patients. Expert Rev Clin Immunol. 2014;10(4):501–512.
Suchy BH, Wolf SR. Bilateral mucosa-associated lymphoid tissue lymphoma of the parotid gland. Arch Otolaryngol Head Neck Surg. 2000;126(2):224–6.
Isaacson PG, et al. Follicular colonization in B-cell lymphoma of mucosa-associated lymphoid tissue. Am J Surg Pathol. 1991;15(9):819–28.
Chan JK, et al. T- and T/natural killer-cell lymphomas of the salivary gland: a clinicopathologic, immunohistochemical and molecular study of six cases. Hum Pathol. 1997;28(2):238–45.
Isaacson PG. Malignant lymphomas with a follicular growth pattern. Histopathology. 1996;28(6):487–95.
Jaffe ES, Harris N, Stein H, Vardiman JW. World Health Organization classification of tumors: tumors of haematopoietic and lymphoid tissues. Berlin: Springer; 2001.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Di Palma, S., Simpson, R.H.W., Skalova, A., Fonseca, I., Leivo, I., Ihrler, S. (2016). Major and Minor Salivary Glands. In: Cardesa, A., Slootweg, P., Gale, N., Franchi, A. (eds) Pathology of the Head and Neck. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-662-49672-5_5
Download citation
DOI: https://doi.org/10.1007/978-3-662-49672-5_5
Published:
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-662-49670-1
Online ISBN: 978-3-662-49672-5
eBook Packages: MedicineMedicine (R0)