As part of this symposium honoring Leon Barnes, the authors were asked to present the case from which they learned the most. I chose a cystic sebaceous lymphadenoma (SL) as my case presentation. This paper presents this unusual case, as well as several additional sebaceous tumors that came across my desk the first few years I was in practice. These interesting cases led me to thoroughly review the literature on sebaceous tumors of the salivary glands, resulting in several publications, the largest series of sebaceous tumors published at this time as well as a careful review of all cases in the literature. The author will also review the current and previous literature on the five types of salivary gland sebaceous tumors: sebaceous adenoma, SL (and non-sebaceous lymphadenoma), sebaceous carcinoma, sebaceous lymphadenocarcinoma, and sebaceous differentiation in other types of salivary gland lesions.
As part of this symposium honoring Leon Barnes, the authors were asked to present the case from which they learned the most. I thought about the many unusual tumors I’ve come across over my career and decided to present an unusual salivary gland tumor that was involved in one of my earliest publications. Approximately a year after I finished my residency and started working at West Virginia University, I came across an unusual cystic salivary gland tumor (see below) that led me to review the literature, determining only 2 other similar tumors had been previously published.
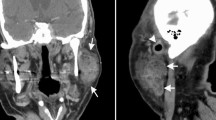
The patient was a 57-year-old white male who was seen for a mass posterior to and below the angle of the right ramus of the mandible. This was present for approximately 6 years. The mass occasionally fluctuated in size and measured 3 cm in greatest dimension. It was non-tender, mobile and at the tail of the right parotid. The remainder of the general physical exam was negative. The clinical impression was of a Warthin’s tumor. A right superficial parotidectomy was performed with preservation of the facial nerve. The entire mass was excised. His postoperative course was uneventful and the patient was free of disease one year after surgery.
The specimen consisted of the right parotid gland, weighing 43 g and measuring 6 × 3.5 × 2.5 cm. Within the gland, there was a thin-walled transparent cyst that measured 3.3 × 2.5 × 2.5 cm. It was filled with whitish caseous-type material, which replaced most of the parenchymal tissue (Fig. 1).
Fig. 1
The cut surface of this cystic sebaceous lymphadenoma from the superficial parotid gland demonstrated a well-circumscribed lesion with a thin wall and caseous material filling the entire cyst
Histologically, the cyst was filled with keratin debris and was lined by stratified squamous epithelium with orderly maturation, focal hyperkeratosis, and hypergranulosis (Fig. 2a). There was an occasional “trabecular” infolding of the cyst wall. Beneath the cyst wall lining, there were collections of benign appearing lymphoid cells with occasional germinal centers (Fig. 2a). In several areas, the lining epithelium of the cyst contained nests of large sebaceous cells with abundant, foamy, clear cytoplasm (Fig. 2b). Focal areas of fibrosis in the cyst wall were also present. The surrounding parotid gland acini and ducts were compressed by the cyst.
Fig. 2
a Section of cyst wall lined by a bland, stratified squamous epithelium with a uniform submucosal lymphoid population; a slightly compressed centrally located lymphoid follicle is present in the wall. b Focal areas in the cyst wall demonstrate sebaceous differentiation. Inset: Higher power detail of sebaceous focus
A diagnosis of a benign lymphoepithelial cyst with sebaceous differentiation (cystic sebaceous lymphadenoma) was made.
Conducting a literature review for this unusual sebaceous tumor revealed that there were only occasional case reports of the various types of sebaceous lesions involving the major salivary glands, so I published this rare lesion, together with the otolaryngologist, as a case report in the late 1970s [1]. A second salivary gland tumor with sebaceous differentiation was removed approximately a year later in another patient. This involved a Warthin’s Tumor with sebaceous differentiation, which also contained a prominent area with necrotizing sialometaplasia, a benign condition frequently simulating malignancy and that had been described for the first time only a few years earlier [2]. This case also had me going back to the literature and standard texts of that period (Evan and Cruckshank’s Book on Salivary Gland Tumors and the Armed Forces Institute of Pathology (AFIP) Salivary Gland Fascicle, 2nd series), again finding only a little information. A third case was sent to me several months later by a fellow resident I had trained with at Washington University in St. Louis, Dr. Stewart Cramer. This was an unusual adenoid cystic carcinoma with areas of sebaceous differentiation, the first such case described in the literature [3] (Fig. 3).
Fig. 3
Adenoid cystic carcinoma with multifocal areas of sebaceous differentiation. a The majority of this tumor was solid with focal areas showing a cribriform growth pattern. b An area with multiple sebaceous nests intermixed with the solid pattern. c Detail of sebaceous areas with numerous cytoplasmic lipid vacuoles
Because of the lack of information in the literature, and my experience with these three tumors, I became interested in putting together a thorough literature review to aid other clinicians when they were confronted with similar tumors. Also, at this time, I was traveling to the AFIP several times a year, to augment my head and neck pathology experience working with Dr. Vince Hyams, one of the fathers of head and neck pathology. Because of my interest in salivary gland pathology, I had also made arrangements to spend time in the Oral Pathology Department. One of the oral pathologists I spent time with was Dr. Robert Brannon, who also had a strong interest in salivary gland pathology, and during one of my visits we began discussing the sebaceous lesions of the salivary gland and decided to put together the AFIP experience with these tumors. Over the next several years, I made multiple trips to the AFIP, collaborating with Dr. Brannon. This resulted in the largest series of major salivary gland sebaceous tumors published at that time, 21 cases, including 5 sebaceous adenomas, 9 sebaceous lymphadenomas (SL), 5 sebaceous carcinomas and 2 sebaceous lymphadenocarcinomas (a carcinoma arising within SL) [4]. While working on the sebaceous tumor series, it became clear to me that it would be difficult to include a comprehensive literature review as part of the AFIP series, due the size of the final document. Therefore, my final comprehensive review summarizing the world literature on every type of sebaceous lesion that one may find in the major salivary glands, including [1] sebaceous differentiation in normal salivary glands, [2] the four types of primary sebaceous tumors, and [3] other salivary gland tumors with sebaceous differentiation was published separately in Pathology Annual [5]. Because of the rarity of these lesions, I contacted authors of previously published case reports to obtain current follow-up information to be able to more accurately predict biologic behavior of these tumors.
This entire process taught me how a single case report and brief literature review could provide the nidus of intellectual curiosity that would end up teaching me how to thoroughly review the world literature (there were no computer programs available to help with this; all searches were done manually at the library), how to organize and write several complicated papers and also about the generosity of other authors who went out of their way to obtain follow-up information on their previously published cases. The following is a brief literature review on the various sebaceous lesions predominantly arising in the major salivary glands.
Sebaceous Lesions
Sebaceous glands are commonly found in the parotid gland (10–42% of glands) and are found less frequently in the submandibular glands (5–6% of glands) using standard surgical pathology sampling techniques; however, they are only rarely seen in the sublingual gland or in parotid area lymph nodes [1, 4–8]. Intraoral sebaceous glands, known as Fordyce granules, are found in up to 80% of individuals, most frequently on the buccal mucosa or vermilion border of the upper lip and less frequently in the retromolar and anterior tonsillar pillar region [9]. These are considered a normal anatomic variant and may vary in number from a few to several hundred. In a recent study, the frequency of Fordyce granules was 50- to 90-fold greater in a population with hereditary non-polyposis colorectal cancer syndrome (HNPCC or Lynch syndrome) as compared to the general population, suggesting activation in this syndrome [10]. Rarely, Fordyce granules may become hyperplastic. Sebaceous glands with fewer than 15 lobules are considered normal, while those with 15 or more lobules are considered hyperplastic [11].
Salivary gland sebaceous neoplasms are classified histologically into five groups: [1] sebaceous adenoma, [2] SL, [3] sebaceous carcinoma, [4] sebaceous lymphadenocarcinoma, and [5] sebaceous differentiation in other tumors. Although parotid and submandibular gland sebaceous differentiation is relatively common, sebaceous neoplasms in these locations are extremely rare. Greater than 150 primary salivary gland sebaceous tumors have been reported in the world literature. The most frequent sebaceous tumor is SL followed by sebaceous carcinoma and sebaceous adenoma, with the least frequent being sebaceous lymphadenocarcinoma; in addition, various other salivary gland tumors have been associated with sebaceous differentiation [12].
It is worth noting that unlike cutaneous sebaceous neoplasms, which are associated with an increased risk of developing visceral, predominantly colonic, carcinomas [13, 14], there does not appear to be any increased risk of developing a visceral carcinoma in patients with salivary gland sebaceous tumors.
Sebaceous Adenoma
The sebaceous adenoma is a rare, benign tumor that accounts for 0.1% of all salivary gland neoplasms and slightly less than 0.5% of all salivary adenomas [12]. Slightly more than 30 cases have been reported to date [12, 15–17]. The mean age at initial clinical presentation is 59 years (range, 22–90 years) with a male-to-female ratio of 4:3. Sixty-one percent of reported tumors arose in the major salivary glands (48% parotid, 13% submandibular gland), and 39% in the minor salivary glands (19% in the buccal mucosa, 13% in the area of the lower molars or retromolar region and 7% in other intraoral sites) [12].
Sebaceous adenomas range in size from 0.4 to 6.0 cm in greatest dimension. They are commonly encapsulated or sharply circumscribed, varying in color from grayish-white to pinkish-white to yellow or yellowish-gray on gross examination. These tumors are composed of sebaceous cell nests, often with areas of squamous differentiation. Atypia and pleomorphism are minimal and there is no tendency to invade local structures (Fig. 4). Many tumors are microcystic or composed of dilated salivary ducts with foci of sebaceous differentiation. The sebaceous glands vary markedly in size and in tortuosity and are frequently embedded in a fibrous stroma. Occasional adenomas demonstrate marked oncocytic metaplasia, and histiocytes or foreign body giant cells, or both can be seen focally. Lymphoid follicles, cytologic atypia, necrosis, and mitoses are usually not observed in sebaceous adenomas.
Fig. 4
a Sebaceous adenoma is composed of variably-sized and shaped nests of sebaceous cells with areas of cystic change. b Higher power of a demonstrating vacuolated cytoplasm with central holocrine secretory material. Inset: High-power detail of sebaceous cyst lining
Sebaceous adenomas may be confused histologically with low-grade mucoepidermoid carcinomas (MEC) and rarely with metastatic renal cell carcinoma. This differential diagnosis is discussed in the last section.
Treatment consists of complete surgical excision. These tumors should not recur.
Sebaceous and Non-sebaceous Lymphadenoma
In 1996, the 3rd edition of the Armed Forces Institute of Pathology Atlas of Salivary Gland Tumor Pathology, written by Gary Ellis and Paul Auclair, was published [18]. These authors placed the SL group of neoplasms into the newly defined category of “lymphadenomas,” which encompassed tumors with and without sebaceous differentiation.
Sebaceous lymphadenoma is a rare, benign, well-circumscribed to encapsulated tumor composed of well-differentiated, variably shaped and sized nests of sebaceous glands and ducts within a background of lymphocytes and lymphoid follicles. Cytologic atypia is minimal and there is no tendency to invade local structures. Some of these tumors likely arise from intra-lymph nodal sebaceous nests in a fashion similar to Warthin’s tumors arising from intra-nodal ectopic salivary gland tissue (4, 5. 7). Non-sebaceous lymphadenoma (NSL) is histologically similar, but without sebaceous differentiation [19–21]. These tumors do not appear to have any association with Epstein Barr virus, papilloma virus, or HHV-8 [21].
Approximately 75% of patients with SL are first diagnosed in the sixth to eighth decade of life (range, 25–89 years), with no gender preference. Less than 100 cases have been reported to date [4, 5, 21–25]. Patients typically present with a mass, which may be slowly enlarging. Approximately 95% of tumors arise in or around the parotid gland, one tumor occurred in the anterior midline of the neck, one in the upper lip, one in the neck, two in one patient arose in the right and left buccal mucosa, respectively, and one in the midline of the maxilla.
To date, 22 NSLs have been reported [19–21, 26–28]. Patients typically present with a mass that has been present for up to 5 years. The majority of tumors arose in the parotid gland but they have been reported in the periparotid region, submandibular gland, cervical lymph node, and neck. The male:female ratio is approximately equal. The mean age at initial operation was in the mid-fifties with a range from 11 to 78 years.
Sebaceous lymphadenomas have ranged from 1.0 to 6.0 cm in greatest dimension and are usually encapsulated or well-circumscribed, but rarely may be incompletely encapsulated or unencapsulated. They can be solid, multicystic, or unicystic masses that range from yellow to yellow-white to pink-tan or gray; microcysts are frequent. Sebum or cheesy material is commonly found in many of the cysts.
The majority of tumors are composed of variably sized sebaceous glands admixed with salivary ducts in a benign lymphoid background (Fig. 5). Others consist mainly of lymphocytes and lymphoid follicles surrounding salivary ducts with only occasional sebaceous glands. Histiocytes and foreign body giant cell inflammatory reactions due to extravasated sebum are commonly found. By definition, all tumors have a lymphoid background and about one-half have well-developed lymphoid follicles. In addition, tumors may contain small areas of identifiable residual lymph node and rarely foci of Warthin tumor may be found (combined SL and Warthin tumor). Focal necrosis has been observed in one tumor.
Fig. 5
a Sebaceous lymphadenoma is composed of numerous variably-sized and shaped sebaceous glands and small ducts surrounded by a prominent lymphoid stroma with scattered histiocytic aggregates. b High-power detail of a. There are several sebaceous glands with holocrine secretion surrounded by a mixed population of lymphocytes. Lymphadenoma, non-sebaceous type. c There are nests of basaloid cells surrounded by a mixed benign lymphoid population; several nests have a central space lined by bland squamous epithelium; centrally, there is one nest with several degenerating cells with cytoplasmic clearing, however, definite sebaceous differentiation was not found in this tumor. d Sheets of irregular tumor nests composed of basaloid cells with prominent peripheral palisading; surrounding tumor nests is a dense, uniform lymphoid stroma supporting a diagnosis of chronic lymphocytic leukemia. e High-power detail of “d”
Non-sebaceous lymphadenomas are similar to SL but without the sebaceous component. These tumors have ranged in size from 0.6 to 8 cm with a mean size of almost 2.5 cm. They are typically well-demarcated and are composed of a prominent lymphoid population surrounding proliferating epithelium arranged as solid tubules or basaloid islands often with a prominent trabecular arrangement with or without cyst formation. Atypia is minimal and sebaceous or oncocytic differentiation is not found. Focal squamous differentiation and mucin-secreting cells may be observed. Epithelial membrane antigen immunohistochemistry typically stains collapsed spaces or small groups of cells in the central portion of the epithelial islands or trabeculae indicating subtle luminal differentiation. There appears to be two somewhat different morphologies included in this group: [1] One is similar to a SL (but lacking the sebaceous differentiation) with prominent microcystic change and often with focal squamous differentiation, which is the so-called “typical type” (Fig. 5c); and [2] a second group of tumors that is composed of solid nests and interconnecting trabeculae with frequent peripheral palisading, somewhat similar to the cell population of basal cell adenoma, but with a prominent lymphoid component, thus called the “basaloid type”. A tumor with similar morphology to the latter pattern has rarely been reported in the skin [30].
Complete surgical excision is the treatment of choice. These tumors should not recur if properly excised.
Sebaceous Carcinoma
Sebaceous carcinoma is a malignant tumor composed predominantly of sebaceous cells of varying maturity that are arranged in sheets and/or nests, with varying degrees of cytologic pleomorphism, nuclear atypia, and invasiveness.
To date, there are at least 44 sebaceous carcinomas reported [4, 5, 31–36]. Twenty-nine tumors arose in the parotid gland, two of which were the malignant component of a carcinoma ex pleomorphic adenoma [36], 8 arose in the oral cavity, most frequently in the buccal mucosa; 3 from the submandibular gland; and 1 each from the sublingual gland, vallecula, epiglottis, and hypopharynx. There is a biphasic age distribution with peak incidence in the third decade and the seventh to eighth decades of life (age range, 17–93 years) [4, 5, 7]. The male-to-female incidence is approximately 1:1. Patients most frequently present with a painful mass with varying degrees of facial nerve paralysis and occasional fixation to the skin; a few patients present with a nontender mass.
Sebaceous carcinomas have ranged from 0.6 to 9.5 cm in greatest dimension and vary from yellow, tan-white, grayish-white, white, to pale pink. Tumors are frequently well circumscribed or partially encapsulated, with pushing or locally infiltrating margins. Cellular pleomorphism and cytologic atypia are uniformly present and are much more prevalent than in sebaceous adenomas. Tumor cells may be arranged in multiple, variably sized nests or in sheets and have hyperchromatic nuclei surrounded by abundant clear, vacuolated to eosinophilic cytoplasm (Fig. 6). Cellular pleomorphism and atypia varies from mild to severe. Areas of cellular necrosis and fibrosis are commonly found. Perineural invasion has been observed in more than 20% of tumors, whereas vascular invasion is extremely infrequent. Rare oncocytes and foreign body giant cells with histiocytes may be observed, but lymphoid tissue with follicles or subcapsular sinuses is not seen.
Fig. 6
Sebaceous carcinoma composed of sheets of: a markedly pleomorphic hyperchromatic sebaceous cells with prominent nucleoli and varying amounts of vacuolated eosinophilic to clear cytoplasm. b Pleomorphic hyperchromatic sebaceous cells with prominent nucleoli and varying amounts of finely vacuolated clear cytoplasm
The treatment of choice is wide surgical excision for low-grade and low-stage carcinomas. Adjunctive radiation therapy is recommended for higher-stage and higher-grade tumors. Tumors may recur and rarely will metastasize. The overall 5-year survival rate is 62%, slightly less than the survival rate for similar tumors arising in the skin and orbit (84.5%) [37]. Oral sebaceous carcinomas may have a better prognosis as none in a review of 6 cases have recurred or metastasized; however, follow-up was less than 5 years in 4 of the patients [35]. The longest recorded survival, 13 years, occurred in a patient who was 22 years old at the time of diagnosis; however, because of insufficient data, it is not yet possible to predict whether the survival rates differ between younger and older patients.
Sebaceous Lymphadenocarcinoma
Sebaceous lymphadenocarcinoma is the malignant counterpart of SL and represents a carcinoma arising in a SL. It is the rarest sebaceous tumor of the salivary glands. To date, only seven have been reported [4–6, 38–41].
Four patients were in their seventh decade and one patient each was in the fourth, sixth and eighth decades; five patients were male and two female. All tumors arose within the parotid gland or in a periparotid lymph node. Patients had histories of a mass present for 1 month to more than 20 years. One patient presented with confluent reddish livid plaques of the left cheek and neck secondary to lymphangitic carcinomatosis and cervical lymph node metastasis [38].
Tumors ranged up to 6 cm in greatest dimension with tumor color ranging from tan, yellow-tan to gray, gray-white and white-tan. These carcinomas are focally encapsulated and locally invasive with foci of SL intermixed with or adjacent to regions of pleomorphic carcinoma cells exhibiting varying degrees of invasiveness. The malignant portion has ranged from squamous cell carcinoma, sebaceous carcinoma to sheets of poorly differentiated carcinoma, with areas of ductal differentiation, adenoid cystic carcinoma-like areas, or epithelial-myoepithelial carcinoma-like foci (Fig. 7). Perineural invasion was present in several tumors. Mitotic figures ranged up to 12 per 10 high-power fields. Collections of histiocytes were present in three cases, and a foreign body giant cell reaction was found in two tumors. Oncocytes have not been described. Cellular atypia is not observed in the SL portion of the tumor.
Fig. 7
Sebaceous lymphadenocarcinoma. a The sebaceous lymphadenoma component is in the lower left and the carcinoma portion is in the upper right. b Detail of the junction of the sebaceous lymphadenoma (lower left) and carcinoma component (upper right). c The carcinoma is composed of sheets of poorly-differentiated carcinoma cells (left) with areas of ductal differentiation (right)
Therapy will depend on the type of carcinoma and on clinical staging. Appropriate therapy would typically consist of wide local excision possibly with adjuvant radiation therapy for a high-grade carcinoma component or for advanced stage tumors. Long-term follow-up information is not available. Two patients died of other causes at 8 months and 1.5 years and four patients, with follow-up ranging from 4 months to 6 years, were alive without evidence of disease. One report did not include follow-up information.
Sebaceous Lesions Associated with Other Salivary Gland Neoplasms
More than 75 salivary gland tumors with sebaceous differentiation that do not fall into one of the four previously discussed categories of sebaceous neoplasia have been described in the literature [5, 18, 29, 42–51]. Warthin’s tumor and mixed tumors are the most frequent tumors with sebaceous differentiation, followed in incidence by MEC, epithelial myoepithelial carcinoma, carcinoma ex pleomorphic adenoma, and oncocytoma. Additional examples of sebaceous differentiation have been reported in benign lymphoepithelial lesion [lymphoepithelial sialadenitis (LES)], sialolipoma (lipoadenoma), oncocytic lipoadenoma, basal cell adenocarcinoma, adenoid cystic carcinoma, acinic cell carcinoma, basal cell adenoma, a basal cell adenoma from which arose an adenoid cystic carcinoma and adenocarcinoma, not otherwise specified (NOS).
Differential Diagnosis
Sebaceous adenoma, lymphadenoma, and carcinoma may be confused histologically with MEC. The presence of luminal holocrine secretions together with vacuolated cytoplasm will help with this differential diagnosis. MEC typically has clear cytoplasm that focally contains intracellular mucin; it does not have vacuolated cytoplasm with holocrine secretion unless it is a combined mucoepidermoid and sebaceous carcinoma. Also foreign body reaction, when present, can be helpful in differentiating these tumors from MEC. MEC frequently is cystic and may contain nests of clear cells, but foreign body inflammation is unusual in that malignancy. In addition, unlike MEC, which contains intracellular mucin in some clear cells, mucin positivity is never found in the clear sebaceous cells. However, intracellular and extracellular mucin may occasionally be found within ducts adjacent to sebaceous cells.
Rarely, benign lymphoepithelial lesion (myoepithelial or LES) may have focal sebaceous differentiation and needs to be considered in the differential diagnosis with SL [29]. The morphology of the lymphoepithelial islands is different than the ductal component in SL and the foreign body inflammatory reaction, frequently seen in SL, is not seen in the former.
Metastatic renal cell carcinoma is part of the differential diagnosis of any clear cell tumor of the salivary glands, but unlike most primary malignant salivary neoplasms, it is usually positive for PAX-8 [52, 53], has a more prominent vascular background, and is usually negative for cytokeratin 7 or stains in a weaker, more patchy fashion; in contrast, CD10 stains most renal carcinomas, but it also may be positive in salivary tumors with myoepithelial differentiation. Other renal tumor markers, such as RCC may also be utilized if positive, but they are not as sensitive as PAX-8 and CD10. One other antibody that appears to be useful in preliminary studies is p63. This antibody typically stains myoepithelial and basal cells. It also stains the germinative cells of the secretory portion of sebaceous glands [54]. In a recent paper, p63 stained all sebaceous and NSLs, 11 and 7, respectfully [21], while a separate study found that all 16 metastatic renal cell carcinomas were negative for this antibody [55]. In addition, three primary sebaceous carcinomas of the skin in several recent studies also stained with p63 [54, 56, 57]. Therefore, it appears that a positive p63 stain likely eliminates the possibility of a metastasis from a renal primary. If there is any doubt, the possibility of a metastasis should be excluded by imaging techniques of the kidneys and a careful history of any previously excised renal tumors.
Recently, two new immunohistochemical markers that recognize proteins associated with lipid vacuoles have been described. Adipophilin is found in milk fat globule membranes as well as in various normal cells, including the adrenal gland zona fasciculata, Sertoli cells, and in the lactating breast glandular tissue; it is also found in pathologic conditions associated with intracellular lipid deposition, such as within hepatocytes in patients with alcoholic steatosis and in liposarcoma [58, 59]. The perilipins are a family of phosphoproteins located on the surface of intracellular lipid vacuoles. They also have been found in the adrenal gland and Leydig cells, as well as brown and white fat [59]. These markers are well-characterized in sebaceous skin and eye tumors, with 95–100% of skin and eyelid sebaceous tumors staining with these markers in three recent studies [58, 60, 61]. However, in the salivary gland, these markers have only been studied in the sebaceous variant of epithelial myoepithelial carcinoma and in one sebaceous carcinoma of the tongue [62, 63]. From the skin and eyelid data, one can extrapolate and conclude that these markers appear to be very sensitive markers for sebaceous differentiation and likely can be used to confirm sebaceous differentiation in a salivary gland tumor. To be called positive, the pattern should be highlight the intracellular vacuolar membranes; if there is a cytoplasmic granular staining pattern, which may be found in macrophages and keratinocytes and has been reported in a squamous cell carcinoma in situ, this is considered non-specific and not diagnostic of sebaceous differentiation [58, 64]. However, if a metastatic renal cell carcinoma is under consideration, one should be aware that these two markers will also stain renal cell carcinoma in a membranous pattern [58, 64], as intracellular lipid material is frequently present in these tumors. An Oil Red O or Sudan Black stain may also be used to confirm intracellular lipid material, however, these latter two stains only work on frozen sections as the lipid is removed during normal tissue processing.
The differential diagnosis of NSL consists mainly of lymphoepithelial carcinoma, LES also known as benign lymphoepithelial lesion, and metastatic carcinoma. The former can be differentiated from NSL by the lack of invasion, atypia, mitotic activity, desmoplasia, lack of association with Epstein Barr virus, and the presence of ductal differentiation in NSL. The morphology of the lymphoepithelial islands in LES differs from the ductal component in NSL. The epithelial component in NSL, unlike LES, is typically more closely packed, more abundant and contains lumina, while LES is typically not well-circumscribed and is frequently multifocal; however, LES may also contain scattered lumina. Metastatic carcinoma can be differentiated from NSL by the lack of invasion, atypia, mitotic activity and desmoplasia of the latter.
References
Gnepp DR, Sporck FT. Lymphoepithelial cyst with sebaceous differentiation (cystic sebaceous lymphadenoma). Am J Clin Pathol. 1980;74:683–7.
Gnepp DR. Warthin tumor exhibiting sebaceous differentiation and necrotizing sialometaplasia. A pathological anatomy and histology. Virchows Arch A Pathol Anat Histol. 1981;391(3):267–73.
Gnepp DR, Henley JD, Simpson RHW, Eveson J. Salivary and lacrimal glands. In: Gnepp DR, editor. Diagnostic surgical pathology of the head and neck. 2nd ed. Philadelphia: W.B. Saunders; 2009. p. 508–12.
Rulon DB, Helwig EB. Multiple sebaceous neoplasms of the skin: an association with multiple visceral carcinomas, especially of the colon. Am J Clin Pathol. 1973;60:745–53.
de Vicente Rodríguez JC, Fresno Forcelledo MF, González García M, Aguilar Andrea C. Sebaceous adenoma of the parotid gland. Med Oral Patol Oral Cir Bucal. 2006;11:E446–8.
Apple SK, Moatamed NA, Lai CK, Bhuta S. Sebaceous adenoma of the parotid gland: a case report with fine needle aspiration findings and histologic correlation. Acta Cytol. 2009;53(4):419–22.
Ellis GL, Auclair PL. Atlas of tumor pathology. Tumors of the salivary gland, 3rd series, fascicle 17. Washington, DC: Armed Forces Institute of Pathology; 1996. p. 130–6, 333–6.
Chang JY, Hsiao CH. Lymphadenoma lacking sebaceous differentiation in the parotid gland. J Formos Med Assoc. 2004;103:459–62.
Seethala RR, Thompson LD, Gnepp DR, Barnes EL, Skalova A, Montone K, Kane S, Lewis JS Jr, Solomon LW, Simpson RH, Khan A, Prasad ML. Lymphadenoma of the salivary gland: clinicopathological and immunohistochemical analysis of 33 tumors. Mod Pathol. 2012;25(1):26–35.
Squillaci S, Marchione R, Piccolomini M. Cystic sebaceous lymphadenoma of the parotid gland: case report and review of the literature. Pathologica. 2011;103(2):32–9.
Maffini F, Fasani R, Petrella D, Maiorano E, Bruschini R, Pelosi G, Viale G. Sebaceous lymphadenoma of salivary gland: a case report and a review of the literature. Acta Otorhinolaryngol Ital. 2007;27(3):147–50.
Auclair PL. Tumor-associated lymphoid proliferation in the parotid gland. A potential diagnostic pitfall. Oral Surg Oral Med Oral Pathol. 1994;77:19–26.
Bos I, Meyer S, Merz H. Lymphadenoma of the parotid gland without sebaceous differentiation, immmunohistochemical investigations. Pathologe. 2003;25:73–8.
Ide F, Shimoyama T, Horie N, et al. Benign lymphoepithelial lesion of the parotid gland with sebaceous differentiation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;87:721–4.
Wang H, Yao J, Solomon M, Axiotis CA. Sebaceous carcinoma of the oral cavity: a case report and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;110:e37–40.
Alawi F, Siddiqui A. Sebaceous carcinoma of the oral mucosa: case report and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;99:79–84.
Claudius K, Ginzkey C, Gattenlöhner S, Müller J, Demmer P, Bröcker E. A red cheek as first clinical sign of a sebaceous lymphadenocarcinoma of the parotid gland with lymphangiosis carcinomatosa and lymph node metastases. Am J Dermatopathol. 2011;33:e50–3.
Seethala RR, Barnes L, Hunt JL. Epithelial-myoepithelial carcinoma: a review of clinicopathologic spectrum and immunophenotypic characteristics in 61 tumors of the salivary glands and upper aerodigestive tract. Am J Surg Pathol. 2007;31:44–57.
Uchibori N, Yoshizaki S, Shamoto M, et al. Epidermoid carcinoma arising in parotid adenolymphomatous lesion with microdeposit of amyloid substance. Acta Pathol Jpn. 1983;33:141–6.
Klieb HBE, Peerez-Ordonez B. Oncocytic lipoadenoma of the parotid gland with sebaceous differentiation. Study of its keratin profile. Virchows Arch. 2006;449:722–5.
Kadivar M, Shahzadi SZ, Javadi M. Sialolipoma of the parotid gland with diffuse sebaceous differentiation in a female child. Pediatr Dev Pathol. 2007;10(2):138–41.
Pusiol T, Franceschetti I, Scialpi M, Piscioli I. Oncocytic sialolipoma of the submandibular gland with sebaceous differentiation: a new pathological entity. Indian J Pathol Microbiol. 2009;52:379–82.
Ilie M, Hofman V, Pedeutour F, Attias R, Santini J, Hofman P. Oncocytic lipoadenoma of the parotid gland: immunohistochemical and cytogenetic analysis. Pathol Res Pract. 2010;206(1):66–72.
McNeil ML, Bullock MJ, Trites JR, Hart RD, Taylor SM. Oncocytic lipoadenoma of the parotid gland with sebaceous differentiation in a 73-year-old male. J Otolaryngol Head Neck Surg. 2010;39(5):E48–50.
Ozcan A, Shen SS, Hamilton C, et al. Pax 8 expression in non-neoplastic tissues, primary tumors, and metastatic tumors: a comprehensive immunohistochemical study. Mod Pathol. 2011;24:751–64.
Ivan D, Nash JW, Prieto VG, et al. Use of p63 expression in distinguishing primary and metastatic cutaneous adnexal neoplasms from metastatic adenocarcinoma to skin. J Cutan Pathol. 2007;34:474–80.
Qureshi HS, Ormsby AH, Lee MW, Zarbo RJ, Ma CK. The diagnostic utility of p63, CK5/6, CK 7, and CK 20 in distinguishing primary cutaneous adnexal neoplasms from metastatic carcinomas. J Cutan Pathol. 2004;31:145–52.
Plaza JA, Ortega PF, Stockman DL, Suster S. Value of p63 and podoplanin (D2-40) immunoreactivity in the distinction between primary cutaneous tumors and adenocarcinomas metastatic to the skin: a clinicopathologic and immunohistochemical study of 79 cases. J Cutan Pathol. 2010;37:403–10.
Ostler DA, Prieto VG, Reed JA, et al. Adipophilin expression in sebaceous tumors and other cutaneous lesions with clear cell histology: an immunohistochemical study of 117 cases. Mod Pathol. 2010;23:567–73.
Shinozaki A, Nagao T, Endo H, et al. Sebaceous epithelial-myoepithelial carcinoma of the salivary gland: clinicopathologic and immunohistochemical analysis of 6 cases of a new histologic variant. Am J Surg Pathol. 2008;32(6):913–23.
Rangel J, McCalmont T. Intracytoplasmic adipophilin immunopositivity: A pitfall in the distinction of metastatic renal carcinoma from sebaceous carcinoma. J Cutan Pathol. 2010;37:1194–5.
Gnepp, D.R. My Journey into the World of Salivary Gland Sebaceous Neoplasms.
Head and Neck Pathol6, 101–110 (2012). https://doi.org/10.1007/s12105-012-0343-x