
Abstract
Salivary duct carcinoma (SDC) is a rare and aggressive malignancy with poor prognosis. Its histomorphology is distinctly reminiscent of the ductal carcinoma of the breast. We reviewed the treatment and outcome of SDCs at a single tertiary care centre. Twenty-five cases of SDC of major salivary gland origin, diagnosed and treated at the Department of Otolaryngology, Head and Neck Surgery, Helsinki University Central Hospital, Helsinki, Finland, during a 14-year period from 1997 to 2011, were reviewed retrospectively. Survival outcome was analyzed for 18 patients with a minimum follow-up of 24 months. There were 16 male (64 %) and 9 female (36 %) patients with a median age of 61 years (range 36–82 years). The majority of the cases occurred in the parotid gland (n = 21, 84 %) followed by the submandibular gland (n = 4, 16 %). The primary treatment consisted of surgical resection in all cases and 17 (68 %) patients also underwent neck dissection. Most of the patients (n = 18, 72 %) were treated with postoperative radiotherapy. Seven patients (28 %) had a disease recurrence within a median follow-up time of 15 months (range 3–27 months). In the group (n = 18) with a minimum follow-up time of 24 months, the 2- and 5-year overall and disease-specific survival rates were 66, 41 % and 75, 55 %, respectively. These results confirm the aggressive nature of SDCs in major salivary glands. Diagnostics and management of these tumours need to be centralized in experienced surgical Head and Neck Oncology Centres, and new treatment strategies should be investigated.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Salivary gland carcinomas (SDCs) are a histologically highly heterogenous group of malignancies. In Finland, they compose approximately 0.2 % of all human malignancies [1] and 4–6 % of them are SDCs [2].
Salivary gland carcinoma is an aggressive disease entity with a poor prognosis. The histological picture greatly resembles that of ductal carcinoma of the breast [3]. cERBB2 protein and its encoding gene HER-2/neu (human epidermal growth factor 2) are expressed in a large proportion of SDCs [4–8]. This characteristic occurs also in many cases of the ductal carcinoma of the breast, and the receptor antagonist of cERBB2 trastuzumab is used as a targeted therapy. Similarities of SDC with ductal carcinoma of the breast offer an interesting route to explore new treatment modalities in addition to surgery and chemoradiation. So far, three cases of SDC with successful treatment using trastuzumab have been reported [9–11].
Due to the low incidence of SDC, there are only a limited number of reports on treatment outcome. Lewis et al. [12] studied 26 patients with SDC at the Mayo clinic in 1996. A similar study with 15 patients was performed by Hosal et al. [13] in Pittsburgh in 2003. The largest study by Jaehne et al. [6] presents clinical data of 50 patients. In these studies, 56–77 % of the patients presented with cervical lymph node metastasis at the time of diagnosis, and 51–77 % had died of tumour-related causes at the time of evaluation [6, 12, 13]. Development of locoregional recurrences (19–48 %) and distant metastases (43–48 %) has been frequent [6, 13, 14].
The purpose of this study was to analyze the treatment modalities used and the outcome of SDC at our institution during a 14-year period.
Materials and methods
A retrospective review was performed of all patients (n = 25) with SDC diagnosed and treated at the Department of Otolaryngology, Head and Neck Surgery, Helsinki University Central Hospital (HUCH), Helsinki, Finland, between January 1997 and January 2011. All original SDC diagnoses in the present study were reviewed and confirmed to be true SDCs by an experienced head and neck pathologist with special interest in salivary gland tumours (I.L.). The histopathologic diagnostic criteria at each time point were those of the respective most recent WHO classification (WHO, 1991 and WHO, 2005). The tumours were staged according to the International Union Against Cancer (UICC 2009, 7th edition) tumour-node metastasis (TNM) classification. Data on patient characteristics, clinical and histological features of the tumour, and treatment and outcome parameters were recorded. The study design was approved by the Institutional Research Ethics Board.
The dates and causes of death were provided by Statistics Finland. Overall survival (OS) was defined as the interval between the time of diagnosis and the last follow-up or death, and estimated using the Kaplan–Meier method. Only the patients (n = 18) with a minimum follow-up time of 24 months were included in the survival analyses. Statistical analyses were conducted using the SPSS software (Version 12.0.1, Chicago, IL, USA). A P value of less than 0.05 was considered statistically significant.
Results
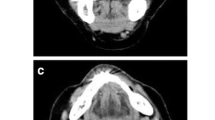
The patient characteristics of 25 cases of SDC are presented in Table 1. Fifteen (60 %) out of 25 patients were otherwise healthy or had only minor comorbidities (hearing aid, mild hypertension and spinal stenosis) at diagnosis. Five patients (20 %) had a history of another malignancy (lung, cervix, colon, mammary, prostate and pancreas). A neck lump was the initial symptom for most of the patients (n = 23, 92 %) and the median time for disease history was 27 months (range 1–240 months). Two patients presented with facial nerve paresis. Nearly all patients (n = 24; 96 %) underwent ultrasound examination and fine needle biopsy of the tumour before planning their treatments. Cytological evaluation showed a malignancy (n = 22) or a suspicion of it (n = 3) in all cases. Other preoperative investigations were MRI (n = 18, 72 %), chest radiograph (n = 11, 44 %), CT scan of body/chest (n = 10, 40 %) and CT scan of neck (n = 1, 4 %).
T1 (40 %, n = 10) and T4a (36 %, n = 9) were the most common T classes. The average tumour size evaluated by pathologists was 23 mm (range 5–60 mm). One case was classified as a carcinoma in situ, probably originating from pleomorphic adenoma. Fourteen patients (56 %) had cervical lymph node metastasis. Only one patient had distant disease in spinal column at the time of diagnosis. More than half (n = 14, 56 %) of the patients presented with Stage IVA disease.
All the patients underwent surgery. Almost half (48 %, n = 10) of the patients with a tumour in the parotid gland underwent total or near total parotidectomy. Six patients (29 %) underwent radical parotidectomy including mastoidectomy and killing of the facial nerve. Superficial parotidectomy was performed on five patients (24 %), and based on the final histomorphology in two cases it was later (1–3 weeks) extended to total parotidectomy. Also, in all patients with submandibular gland involvement surgery was the primary treatment. In addition, 17 patients (68 %) underwent neck dissection. All cases were discussed at a multidisciplinary tumour board meeting for possible additional treatment after the primary surgery with the final histopathological data available. Eighteen patients (72 %) received postoperative radiotherapy and the most frequently administered dose on the operated area was 50–60 Gy. All the patients (n = 7) who did not receive postoperative radiation therapy presented with Stage I disease. Adjuvant chemotherapy was given to six of the patients.
Follow-up time varied from 5 months to 14 years. Disease recurrence was found in 7 patients (28 %) within a median follow-up time of 15 months (range 3–27 months). Three of these had locoregional failures in the parotid area and neck, and six had distant metastases. Bone (n = 4) was the most common site for metastasis followed by the lungs (n = 3). The 2- and 5-year disease-free survival (DFS) rates were 79 and 56 %, respectively. No correlation was found between disease recurrence and TNM classification of the primary tumour. All patients with disease recurrence had undergone surgery and postoperative radiotherapy. Adjuvant chemotherapy was primarily given to three of these patients.
Data on survival and on local and regional recurrences were available for all of the 25 patients. OS and disease-specific survival (DSS) of 18 patients with a minimum follow-up of 24 months were analyzed. In this group the 2- and 5-year OS rates were 66 and 41 %, respectively (Fig. 1). The 2- and 5-year DSS rates were 75 and 55 %, respectively (Fig. 2). DSS according to Stage distribution (Stage I vs. Stage IVa) is presented in Fig. 3.

Overall survival of 18 SDC patients with a minimum follow-up time of 24 months

Disease-specific survival of 18 SDC patients with a minimum follow-up time of 24 months

Disease-specific survival in patients with Stage I and Stage IVa disease
Discussion
This is a single-institution review of 25 SDC patients treated during a 14-year period. Our results confirm the aggressive nature of this disease. Although the preoperative investigations and the administered treatment were consistent with current guidelines for management of SDC, the prognosis of this particular patient group remains poor.
In accordance with earlier studies [6, 12–14], a typical patient in our series was a male in his later adulthood with a median age of 61 years. The tumour occurred most often in the parotid gland (84 %) and less frequently in the submandibular gland (16 %). None of the cases of SDC were found in minor salivary glands. The average history ranged from 1 month to several years. The patients typically (92 %) presented with a neck lump and the most common associated symptoms were facial nerve paresis (22 %) and pain (17 %). Two patients showed facial nerve paresis as the initial symptom, thus the total occurrence of facial palsy was 28 %. Guzzo et al. [14] reviewed 86 cases of SDC in the literature finding that the most common presenting sign of disease was a painless mass in the parotid area, and 29 % of the patients presented with facial nerve paresis. This is closely similar to the present results.
A total of 56 % of our patients had cervical lymph node metastasis and a Stage IVA disease. In previous studies, nodal involvement was found in more than 50 % of the patients [6, 13, 14] and the primary tumour was most often more than 2 cm in the greatest dimension [4, 6, 13–15]. In the present study the median size of the tumour was 2.3 cm with 56 % classified as T2 or higher. SDC may also develop in a pleomorphic adenoma [6, 13, 14, 16] as was encountered in one patient in our series.
Surgery and postoperative radiation therapy are still the main treatment modalities of SDC. In the present series, all primary tumours were operated and 68 % of the cases underwent neck dissection. Eight patients with N0 disease underwent only resection of the primary tumour and the parotid gland. Postoperative radiation therapy was given to 72 % of patients. This treatment was congruent with the Finnish National Guidelines for treatment of salivary gland cancer, but nevertheless the patient outcome remained poor. Almost one-third (28 %) of the patients developed a recurrence of their disease. The 2- and 5-year DFS rates were 79 and 56 %, respectively. This corresponds well to the reported survival outcome for salivary gland cancers in general. Feinstein et al. [24] analyzed the outcome of 74 patients with locally advanced salivary gland cancers registered in the University of Pittsburgh database from 1990 to 2006. These patients were treated with surgery and postoperative radiation therapy and 45 % of them experienced disease recurrence. The probability of 5-year DFS was 49 % and the 5-year OS was 55 %. In our study the 2- and 5-year OS rates were 66 and 41 %, respectively, and the DSS rates were 75 and 55 %, respectively. The reported survival rates for SDC are even poorer. Approximately 44–77 % of patients with SDC have died of disease-related causes [6, 12–14, 19] and the 5-year OS rates have been 20–44 % [19, 23]. Therefore, the importance of a consistent treatment protocol including at least radical resection of the primary tumour, neck dissection and postoperative radiation therapy has been emphasized [6, 13, 14, 23]. Our results further support these recommendations.
The recent literature regarding the management of SDC has focused on the immunohistological and molecular characteristics of the tumour. This is due to the histomorphological resemblance between SDC and the ductal carcinoma of the breast, and the frequent expression of HER-2 oncoprotein. These cancers frequently have amplification of the HER-2/neu oncogene and they overexpress the epidermal growth factor receptor (EGFR) [25]. HER-2/neu is a protooncogene located on chromosome 17q. Amplification of HER-2/neu and overexpression of its protein product occurs also in breast cancer. Although the histomorphology of SDC shows similarities with the ductal carcinoma of the breast, SDC usually lacks oestrogen and progesterone receptors, but is almost uniformly positive for androgen receptors [7, 15, 17–19]. Both the similarity with breast carcinoma and the expression of androgen receptors have been assessed for new treatment modalities [9–11, 20, 21]. Some reports have evaluated other cell cycle regulators and oncogenes [4, 6, 22, 23]. However, there is currently no evidence for these factors as prognosticators or as targets for future treatment modalities.
There is no widely tested standard chemotherapy regimen for the treatment of advanced or metastatic SDC. Trastuzumab is a humanized monoclonal antibody directed against the extracellular domain of the HER-2 tyrosine-kinase receptor and is widely used both in adjuvant postoperative treatment of breast cancer and in the treatment of metastatic breast cancer. The overexpression of HER-2 may provide a rationale for targeted therapy with trastuzumab also in SDC. A recent study by Williams et al. [8] suggested that overexpression of HER-2 and its gene amplification defines a group of patients who may benefit from targeted therapy with trastuzumab. In the same study, mutations also in exons 18 and 19 of the EGFR gene were detected suggesting that tyrosine-kinase inhibitors such as erlotinib may provide targeted therapeutic options in a subset of SDC patients [8]. However, a recent review regarding current management options for salivary gland cancers emphasizes a more sophisticated approach needed for useful clinical applications of the targeted therapy [25–27].
The rarity of SDC makes it difficult to conduct clinical studies aiming to develop optimal combinations of surgery, radiation, targeted cancer therapies and chemotherapy. The combinations of trastuzumab and chemotherapy found to be effective in breast cancer should probably be tested also in the management of SDC based on the biological similarity of these two tumours. Diagnostics and management clearly need to be centralized in experienced multidisciplinary Head and Neck Oncology Centres, and new treatment strategies for SDC should be developed.
References
Finnish Cancer Registry, Cancer Society of Finland 2011. http://www.cancer.fi/syoparekisteri/en/. Accessed June 15th, 2011
Luukkaa H, Klemi P, Leivo I, Koivunen P, Laranne J, Mäkitie A, Virtaniemi J, Hinkka S, Grénman R (2005) Salivary gland cancer in Finland 1991–96: an evaluation of 237 cases. Acta Otolaryngol 125:207–214
Kleinsasser O, Klein HJ, Hubner G (1968) Salivary duct carcinoma: a group of salivary gland tumors analogous to mammary duct carcinoma (German). Arch Klin Exp Ohren Nasen Kehlkopfheilkd 192:100–105
Etges A, Pinto DS Jr, Kowalski LP, Soares FA, Araujo VC (2003) Salivary duct carcinoma: immunohistochemical profile of an aggressive salivary gland tumour. J Clin Pathol 56:914–918
Press MF, Pike MC, Hung G, Zhou JY, Ma Y, George J, Dietz-Band J, James W, Slamon DJ, Batsakis JG et al (1994) Amplification and overexpression of HER-2/neu in carcinomas of the salivary gland: correlation with poor prognosis. Cancer Res 54:5675–5682
Jaehne M, Roeser K, Jaekel T, Schepers JD, Albert N, Löning T (2005) Clinical and immunohistologic typing of salivary duct carcinoma: a report of 50 cases. Cancer 103:2526–2533
Skálová A, Stárek KucerováV, Szépe P, Plank L (2001) Salivary duct carcinoma—a highly aggressive salivary gland tumor with HER-2/neu oncoprotein overexpression. Pathol Res Pract 197:621–626
Williams MD, Roberts DB, Kies MS, Mao L, Weber RS, El-Naggar AK (2010) Genetic and expression analysis of HER-2 and EGFR genes in salivary duct carcinoma: empirical and therapeutic significance. Clin Cancer Res 16:2266–2274
Prat A, Parera M, Reyes V, Peralta S, Cedrés S, Andreu J, Huguet P, del Campo JM (2008) Successful treatment of pulmonary metastatic salivary ductal carcinoma with trastuzumab-based therapy. Head Neck 30:680–683
Nabili V, Tan JW, Bhuta S, Sercarz JA, Head CS (2007) Salivary duct carcinoma: a clinical and histologic review with implications for trastuzumab therapy. Head Neck 29:907–912
Nashed M, Casasola RJ (2009) Biological therapy of salivary duct carcinoma. J Laryngol Otol 123:250–252
Lewis JE, McKinney BC, Weiland LH, Ferreiro JA, Olsen KD (1996) Salivary duct carcinoma. Clinicopathologic and immunohistochemical review of 26 cases. Cancer 77:223–230
Hosal AS, Fan C, Barnes L, Myers EN (2003) Salivary duct carcinoma. Otolaryngol Head Neck Surg 129:720–725
Guzzo M, Di Palma S, Grandi C, Molinari R (1997) Salivary duct carcinoma: clinical characteristics and treatment strategies. Head Neck 19:126–133
Moriki T, Ueta S, Takahashi T, Mitani M, Ichien M (2001) Salivary duct carcinoma: cytologic characteristics and application of androgen receptor immunostaining for diagnosis. Cancer 93:344–350
Delgado R, Vuitch F, Albores-Saavedra J (1993) Salivary duct carcinoma. Cancer 72:1503–1512
Kapadia SB, Barnes L (1998) Expression of androgen receptor, gross cystic disease fluid protein, and CD44 in salivary duct carcinoma. Mod Pathol 11:1033–1038
Fan CY, Wang J, Barnes EL (2000) Expression of androgen receptor and prostatic specific markers in salivary duct carcinoma: an immunohistological analysis of 13 cases and review of the literature. Am J Surg Pathol 24:579–586
Williams MD, Roberts DE, Blumenschein GR, Temam S, Kies MS, Rosenthal DI, Weber RS, El-Naggar AK (2007) Differential expression of hormonal and growth factor receptors in salivary duct carcinomas: biologic significance and potential role in therapeutic stratification of patients. Am J Surg Pathol 31:1645–1652
Jaspers HC, Verbist BM, Schoffelen R, Mattijssen V, Slootweg PJ, van der Graaf WT, van Herpen CM (2011) Androgen receptor-positive salivary duct carcinoma: a disease entity with promising new treatment options. J Clin Oncol 29:473–476
Locati LD, Quattrone P, Bossi P, Marchianò AV, Cantù G, Licitra L (2003) A complete remission with androgen-deprivation therapy in a recurrent androgen receptor-expressing adenocarcinoma of the parotid gland. Ann Oncol 14:1327–1328
Felix A, El-Naggar AK, Press MF, Ordonez NG, Fonseca I, Tucker SL, Luna MA, Batsakis JG (1996) Prognostic significance of biomarkers (c-erbB-2, p53, proliferating cell nuclear antigen, and DNA content) in salivary duct carcinoma. Hum Pathol 27:561–566
Roh JL, Cho KJ, Kwon GY, Choi SH, Nam SY, Kim SY (2008) Prognostic values of pathologic findings and hypoxia markers in 21 patients with salivary duct carcinoma. J Surg Oncol 97:596–600
Feinstein TM, Lai SY, Lenzner D, Gooding W, Ferris RL, Grandis JR, Myers EN, Johnson JT, Heron DE, Argiris A (2011) Prognostic factors in patients with high-risk locally advanced salivary gland cancers treated with surgery and postoperative radiotherapy. Head Neck 33:318–323
Adelstein DJ, Rodriguez CP (2011) What is new in the management of salivary gland cancers? Curr Opin Oncol 23:249–253
Cornolti G, Ungari M, Morassi ML, Facchetti F, Rossi E, Lombardi D, Nicolai P (2007) Amplification and overexpression of HER2/neu gene and HER2/neu protein in salivary duct carcinoma of the parotid gland. Arch Otolaryngol Head Neck Surg 133:1031–1036
Milano A, Longo F, Basile M, Iaffaioli RV, Caponigro F (2007) Recent advances in the treatment of salivary gland cancers: emphasis on molecular targeted therapy. Oral Oncol 43:729–734
Acknowledgments
The authors want to thank the Helsinki University Central Hospital Research Funds.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Salovaara, E., Hakala, O., Bäck, L. et al. Management and outcome of salivary duct carcinoma in major salivary glands. Eur Arch Otorhinolaryngol 270, 281–285 (2013). https://doi.org/10.1007/s00405-012-1997-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-012-1997-4