
Abstract
Introduction
Managing distal femur fracture nonunion is complex, with unpredictable results. The present investigation systematically updates current evidence, reviews existing modalities, innovations and related outcomes, and discusses future perspectives on the management of nonunion of the distal femur.
Methods
This study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses: the 2020 PRISMA statement. In April 2024, PubMed, Web of Science, Google Scholar, and Embase were accessed without time constraints. No additional filters were used in the database search. All the clinical studies investigating treatment options for nonunion of distal femur fractures were accessed.
Results
35 clinical studies (832 patients) were included. Of them, 34.2% (239 of 698 patients) reported an open fracture, and 24.5% (78 of 319 patients) reported infection at the fracture site. The mean length of the follow-up was 28.9 ± 13.2 months. The mean age of the patients was 53.8 ± 14.7 years.
Conclusion
84.5% (703 of 832) of patients reached complete union without major complications, and 3.8% (32 of 832) reached complete union with major complications at a mean of 21.7 ± 20.9 months. 8.7% (72 of 832) patients showed signs of persistent non-union.
Level of evidence
Level III, systematic review.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Distal femoral fractures account for about 3–6% of all femoral fractures [1,2,3]. Previously published reviews on distal femoral nonunion have provided valuable insights into the epidemiology, risk factors, and treatment of this condition [4,5,6]. The distal femoral nonunions, although rare, negatively impact the quality of life (QOL) and pose considerable treatment challenges [7, 8]. Patients with open and comminuted fractures and infections are most prone to develop nonunion [9, 10]. Open reduction and internal fixation (ORIF) combined with cancellous autografting is the most successful treatment option, with a union rate of 97.4% and an average time to heal of 7.8 months [11, 12].
Several non-modifiable and modifiable risk factors for non-union have been identified, including open fractures, fractures with bone loss, and those associated with osteoporosis, diabetes, obesity, and malnutrition [13, 14]. In addition, certain patient-related factors like smoking, advanced age, and obesity are also considered to affect fracture healing negatively [14, 15]. Importantly, inadequate fracture fixation is primarily responsible for non-union and implant failure [16]. The rigidity score has been advocated to predict the risk of nonunion [17, 18]. This score was significantly associated with the risk of non-union [18]. Still, no significant association was detected between non-union and postoperative weight-bearing status or other previously identified risk factors [17]. Karam et al. [19] reported an overall similar non-union rate of 17.8% in both locked plating of closed periprosthetic and non-periprosthetic distal femoral and comminution, which was the most crucial predictor of non-union.
Although nonunions are a well-known complication of fractures, evidence on this condition is limited. The present investigation systematically updates current evidence, reviews existing modalities, innovations, and related outcomes, and discusses future perspectives on the management of nonunion of the distal femur.
Methods
Eligibility Criteria
All the clinical studies investigating treatment options for nonunion distal femur fractures were accessed. According to the author’s language capabilities, English, German, Italian, French, and Spanish articles were eligible. Only studies with levels I to V of evidence, according to the Oxford Centre of Evidence-Based Medicine [20], were considered. Reviews, opinions, letters, and editorials were not considered, as were animals, in vitro, biomechanics, computational, and cadaveric investigations. Missing quantitative data under the outcomes of interests warranted the exclusion of the study.
Search Strategy
This study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses: the 2020 PRISMA statement [21]. The following PICO algorithm was established for the database search:
-
P (Problem): nonunion distal femur fractures;
-
I (Intervention): management;
-
C (Comparison): different modalities of fracture healing;
-
O (Outcomes): union.
In May 2024, PubMed, Web of Science, Google Scholar, and Embase were accessed without time constraints. The Medical Subject Headings (MeSH) used for the database search are reported in the Appendix. No additional filters were used in the database search.
Selection and Data Collection
Two authors (FM and LS) independently performed the database search. All the resulting titles were screened by hand and, if suitable, the abstract was accessed. The full text of the abstracts which matched the topic was accessed. If the full text was not accessible or available, the article was not considered for inclusion. A cross reference of the bibliography of the full-text articles was also performed for inclusion. Disagreements were debated and mutually solved by the authors. In case of further disagreements, a third senior author (RV) decided.
Data Items
Two authors (FM and LS) independently performed data extraction. The following data were extracted: author and year, name of the journal and study design, level of evidence, length of the follow-up, number of included patients, mean age, percentage of women, type of initial and definitive treatment, time to definitive treatment, number of unions with or without major complications and main findings. Data were extracted in Microsoft Office Excel version 16.72 (Microsoft Corporation, Redmond, USA).
Assessment of the Risk of Bias and Quality of the Recommendations
The risk of bias was evaluated following the guidelines outlined in the Cochrane Handbook for Systematic Reviews of Interventions [22]. Nonrandomised controlled trials (non-RCTs) were assessed using the Risk of Bias in Nonrandomised Studies of Interventions (ROBINS-I) tool [23]. Seven domains of potential bias in non-RCTs were assessed. Possible cofounding and the nature of patient selection before the start of the comparative intervention are assessed by two domains. A further domain is used to determine bias in the classification during the intervention. The final four domains assess the methodological quality after the intervention comparison has been implemented and relate to deviations from previously intended interventions, missing data, erroneous measurement of outcomes, and bias in the selection of reported outcomes. The figure of the ROBINS-I was elaborated using the Robvis Software (Risk-of-bias VISualization, Riskofbias.info, Bristol, UK).
Synthesis Methods
The main author (FM) performed the statistical analyses following the recommendations of the Cochrane Handbook for Systematic Reviews of Interventions [22]. The IBM SPSS software (version 25) was used. For dichotomic data, the number of events and observations were reported. For continuous data, the arithmetic mean and standard deviation were used.
Results
Study Selection
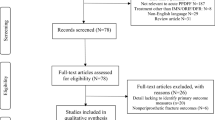
The literature search resulted in 179 articles. All search results were extracted and checked for relevance. Of these, 84 studies were discarded because they were duplicates. Following the defined inclusion criteria, the abstracts of 95 articles were reviewed, and 47 studies were excluded because they did not match the eligibility criteria. The reasons that led to exclusion were: study design (N = 28), low level of evidence (N = 2), not evaluating the un-union of distal femur fracture (N = 9), and language limitations (N = 8). An additional 13 articles were excluded because they did not offer quantitative data on the outcomes of interest. In conclusion, 35 investigations were included in the present analysis. The results of the literature search are shown in Fig. 1.

PRISMA flow chart of the literature search
Methodological Quality Assessment
The ROBINS-I was applied to investigate the risk of bias in the included studies. Given the small number of patients studied in the included investigations, the risk of bias based on confounding and the selection of participants was rated in four studies as serious and in four other studies considered critical because they reported data from only one or two patients. The remaining studies were rated as having a low to moderate risk of bias in these domains. The protocol of intervention was well reported in most studies, and no significant deviation from the interventions was identified, leading to an overall low to moderate risk of bias in the classification of interventions and deviation from intended interventions. Data were adequately reported in the most included studies, and the measurement of the outcomes was equivalent among the groups. Given the lack of randomisation of the investigators and patients, the measurement of the outcomes was evaluated with a moderate risk of bias in all of the studies. When described, the reported results corresponded to the planned protocol in most included studies. However, the exact details of a protocol are often missing, leading to a moderate risk of bias in most of the studies. Given the overall poor methodological quality in the included studies, the overall risk of bias was predominantly moderate. The assessments of the methodological quality are given in Fig. 2.

The ROBINS-I of non-randomised control trials
Study Characteristics and Results of Individual Studies
Data from 832 patients were collected. Of them, 34.2% (239 of 698 patients) reported an open fracture, and 24.5% (78 of 319 patients) reported infection at the fracture site. The mean length of the follow-up was 28.9 ± 13.2 months. The mean age of the patients was 53.8 ± 14.7 years. The generalities, patient characteristics and main results of the included studies are reported in Table 1.
Result Syntheses
At a mean of 21.7 ± 20.9 months, 84.5% (703 of 832) of patients reached complete union without major complications, and 3.8% (32 of 832) reached complete union with major complications. On the other hand, 8.7% (72 of 832) patients showed signs of persistent non-union.
Discussion
The present systematic review revealed that with surgical management of the distal femoral nonunion 84.5% (703 of 832) of patients reached complete union without major complications, and 3.8% (32 of 832) reached complete union with major complications at a mean of 21.7 ± 20.9 months. But, 8.7% (72 of 832) patients showed signs of persistent non-union.
Distal femoral nonunions are challenging to manage, and patient risk factors should be critically evaluated when treating acute distal femoral fractures, since several modifiable risks, such as intake of alcohol and steroids, smoking, and diabetic control, might reduce the risk of nonunion [4, 10, 24]. In addition, optimal fracture alignment and compression are also essential when treating acute fractures [25]. Infections are important risk factors, especially in open fractures or fractures that fail to heal [26, 27]. There is good evidence to guide decision-making and successful union with conventional trauma fixation techniques in the majority of patients. Biological augmentation of fracture healing is not necessary in most cases but needs to be considered in higher-risk cases with a mobile atrophic pattern.
The definition of nonunion is heterogeneous and is related to the time elapsed from the injury to the diagnosis [28]. Reported time intervals ranged from 3 to 12 months [28]. A cut-off of 6 months was most commonly used to define nonunion [28]. Few studies reported a cut-off of 12 months and 9 months [28]. More recently, the US Food and Drug Administration (US FDA) proposed a cut-off of 9 months without evidence of progression to healing over the previous 3 months [29, 30]. The diagnosis of nonunion is often achieved through imaging using plain radiography [31]. However, consensus on the appropriate criteria still needs to be improved [32, 33]. The absence of bridging callus on at least three of four cortices on radiographs is a common assessment criterion, as is the movement of the fracture during radiographic stress testing, lack of bony/cortical continuity, or lack of bridging bone trabeculae [34]. Clinical criteria used to diagnose nonunion are also heterogeneous and not commonly used; among them are pain over the fracture site, pain during weight bearing and natural mobility at the fracture site [35, 36].
Several strategies are used for the management of distal femoral nonunion, with each treatment option having merits and demerits [37,38,39,40]. Dynamisation is occasionally attempted as a less invasive method to achieve union in femoral diaphyseal fractures with an axial stable fracture configuration [41, 42]. The main surgical technique used is the revision ORIF, which involves osteosynthesis with freshening of bone ends and bone grafting [43, 44]. It offers a high chance of achieving union and allows for restoring the joint alignment [43, 44]. Another minimally invasive technique involves retrograde intramedullary nailing, which is more suitable for fractures where the original surgery used plates and screws [45, 46]. Being less invasive, it reduces soft tissue disruption. It may potentially provide faster healing, but it is not suitable for all non-union types, and there may be the possibility of malalignment if nail placement is inaccurate. A combined plate and nail fixation construct is also used, using a locking plate and an intramedullary nail for enhanced stability [47, 48]. Ilizarov external fixator is another surgical option used for treating distal femoral nonunion, and it can provide high union and low complication rates in experienced hands [49, 50]. Although autologous bone grafting is usually considered an essential part of any surgical fixation technique to promote bone growth and improve the chances of healing of nonunion, it requires an additional surgical site for graft harvesting, increasing the potential for pain and discomfort [51, 52]. It is also beneficial for complex non-unions or those with significant bone loss [52]. However, being more invasive than single procedures, there may be an increased risk of infection and hardware complications. In resistant and challenging distal femoral nonunion in older people with associated bone loss, osteoporosis, and secondary knee osteoarthritis, mega prosthesis has been successfully used as a one-stage salvage procedure [53,54,55].
Saxena et al. [47] reported the outcomes of 10 cases of non-union of distal femur treated by fixation with nail plate construct and bone grafting, achieving union in 10.3 months on an average duration.
The only previously systematic review on this topic was done by Ebraheim et al. [4], who assessed 19 studies and found that the most common initial treatment was ORIF with plating, and the most common definitive treatment was with fixed angle plating combined with cancellous autografting, with a union rate of 97.4% and average union time of 7.8 months.
In a retrospective study of 31 cases of distal femoral non-union, which were treated by anatomical lateral locking plates and autogenous bone grafting, stable union was achieved in all cases, with a significant improvement in the functional scores [43]. The authors concluded that optimal stability, good compression at the non-union site, maintenance of axial alignment, bone end freshening, adequate use of cortico-cancellous bone autograft, respecting the biology, and the correct choice of the implant (including the size) are essential to achieve union at the fracture site [43].
In a retrospective study of 18 cases of atrophic distal femoral non-union that were managed using a combination of J-shaped bone graft and double plating union was achieved in all cases at an average of 22.1 ± 5.5 months (range 14–34 months) postoperatively [56]. The average healing time was 6.72 ± 2.80 months [56].
A recently published bibliometric study (1990–2023) found a growing interest in fracture non-union globally through published studies [57].
Distal femoral fractures are complex injuries, and even with advancements in treatment, non-union remains a potential complication. While there has been progress in understanding and treating this condition, there are still gaps in the current research. Studies have not yet established a clear consensus on the most optimal surgical technique for nonunions, and guidelines for managing nonunion, especially of the distal femur, are missing. More research is needed on long-term patient outcomes after treatment for non-union. This can help assess the effectiveness of different approaches and identify areas for improvement. More research is needed to better understand the influence of patient characteristics, such as age, comorbidities, and bone quality, on the risk of developing non-union and treatment success. Further investigations into these areas can lead to more standardised protocols, improved success rates, and improved outcomes. Strategies to improve the outcome of the surgical management of nonunion treatment are evolving.
Logistic regression predictive models can help develop and identify patients at high risk of non-union before surgery. This would allow for early intervention and potentially a reduction in non-union rates [14]. Specific growth factors, like bone morphogenetic proteins (BMP), are used locally at the fracture site to stimulate bone formation, enhance healing, and potentially reduce the need for extensive grafting procedures [58]. However, its use is still limited, as it is a relatively new approach with ongoing research and high cost compared to traditional methods [59, 60]. Genetic influence has been proposed, especially polymorphisms in the genes ANXA3, BMP2, CALY, CYR61, FGFR1, IL1β, NOG, NOS2, PDGF gene, and TACR1 are susceptible to nonunion [61, 62]. Hence, gene therapy may help stimulate bone growth and improve healing rates in non-unions [63]. Refinement in minimally invasive surgical (MIS) techniques for treating non-unions could lead to faster recovery times and less surgical burden on patients [64, 65]. In this context, there is also interest in robotic-assisted surgery (RAS), which might improve precision and accuracy during revision surgery for non-unions [66, 67]. Developing bioactive implants that promote bone healing and enhance the fusion rate at the fracture site could be crucial [68]. Using biodegradable implants would also eliminate the need for a second surgery to remove hardware. Moreover, advanced imaging techniques like Magnetic Resonance Imaging (MRI) may better assess bone healing progress in patients [24, 69]. However, the presence of metallic implants may generate artefacts. Developing biosensors to monitor the bone healing process in real-time may thus allow for adjustments to treatment plans as needed [70, 71]. Focusing on these areas, researchers are developing more effective strategies for distal femoral nonunion, leading to improved patient outcomes and a faster return to function.
Conclusion
This systematic review of distal femoral nonunion based on 35 studies and 832 cases revealed that with appropriate surgical treatment 84.5% of patients reached complete union without major complications, and 3.8% (32 of 832) reached complete union with major complications at a mean of 21.7 ± 20.9 months. But, 8.7% (72 of 832) patients showed signs of persistent non-union.
Availability of Data and Materials
The datasets generated during and/or analysed during the current study are available throughout the manuscript.
References
Coon, M. S., & Best, B. J. (2024). Distal femur fractures. In StatPearls. Treasure Island (FL) Ineligible Companies. Disclosure: Ben Best declares no relevant financial relationships with Ineligible Companies.
Khan, A. M., Tang, Q. O., & Spicer, D. (2017). The epidemiology of adult distal femoral shaft fractures in a Central London Major Trauma Centre over five years. The Open Orthopaedics Journal, 11, 1277–1291. https://doi.org/10.2174/1874325001711011277
Von Rehlingen-Prinz, F., Eggeling, L., Dehoust, J., Huppke, C., Strahl, A., Neumann-Langen, M. V., Glaab, R., Frosch, K. H., & Krause, M. (2023). Current standard of care for distal femur fractures in Germany and Switzerland. Injury, 54(10), 110936. https://doi.org/10.1016/j.injury.2023.110936
Ebraheim, N. A., Martin, A., Sochacki, K. R., & Liu, J. (2013). Nonunion of distal femoral fractures: A systematic review. Orthopaedic Surgery, 5(1), 46–50. https://doi.org/10.1111/os.12017
Koso, R. E., Terhoeve, C., Steen, R. G., & Zura, R. (2018). Healing, nonunion, and re-operation after internal fixation of diaphyseal and distal femoral fractures: A systematic review and meta-analysis. International Orthopaedics, 42(11), 2675–2683. https://doi.org/10.1007/s00264-018-3864-4
Yoon, B. H., Park, I. K., Kim, Y., Oh, H. K., Choo, S. K., & Sung, Y. B. (2021). Incidence of nonunion after surgery of distal femoral fractures using contemporary fixation device: A meta-analysis. Archives of Orthopaedic and Trauma Surgery, 141(2), 225–233. https://doi.org/10.1007/s00402-020-03463-x
Tay, W. H., de Steiger, R., Richardson, M., Gruen, R., & Balogh, Z. J. (2014). Health outcomes of delayed union and nonunion of femoral and tibial shaft fractures. Injury, 45(10), 1653–1658. https://doi.org/10.1016/j.injury.2014.06.025
Brinker, M. R., Trivedi, A., & OʼConnor, D. P. (2017). Debilitating effects of femoral nonunion on health-related quality of life. Journal of Orthopaedic Trauma, 31(2), e37–e42. https://doi.org/10.1097/bot.0000000000000736
Kim, J. W., Byun, S. E., Oh, H. K., & Kim, J. J. (2015). Indolent infection in nonunion of the distal femur. European Journal of Orthopaedic Surgery & Traumatology, 25(3), 549–553. https://doi.org/10.1007/s00590-014-1531-z
Cone, R., Roszman, A., Conway, Y., Cichos, K., McGwin, G., & Spitler, C. A. (2023). Risk factors for nonunion of distal femur fractures. Journal of Orthopaedic Trauma, 37(4), 175–180. https://doi.org/10.1097/BOT.0000000000002553
Landes, E. K., Konda, S. R., Leucht, P., Ganta, A., & Egol, K. A. (2023). Fixed-angle plate fixation and autogenous iliac crest graft for repair of distal metaphyseal femoral nonunion. European Journal of Orthopaedic Surgery & Traumatology, 33(5), 1835–1839. https://doi.org/10.1007/s00590-022-03366-0
Peng, Y., Ji, X., Zhang, L., & Tang, P. (2016). Double locking plate fixation for femoral shaft nonunion. European Journal of Orthopaedic Surgery & Traumatology, 26(5), 501–507. https://doi.org/10.1007/s00590-016-1765-z
Wang, M. T., An, V. V. G., & Sivakumar, B. S. (2019). Non-union in lateral locked plating for distal femoral fractures: A systematic review. Injury, 50(11), 1790–1794. https://doi.org/10.1016/j.injury.2019.07.012
Sainio, H., Ramo, L., Reito, A., Silvasti-Lundell, M., & Lindahl, J. (2023). Prediction of fracture nonunion leading to secondary surgery in patients with distal femur fractures. Bone and Joint Open, 4(8), 584–593. https://doi.org/10.1302/2633-1462.48.BJO-2023-0077.R1
Christiano, A. V., Pean, C. A., Konda, S. R., & Egol, K. A. (2016). Predictors of patient reported pain after lower extremity nonunion surgery: The nicotine effect. Iowa Orthopaedic Journal, 36, 53–58.
Quan, K., Xu, Q., Zhu, M., Liu, X., & Dai, M. (2021). Analysis of risk factors for non-union after surgery for limb fractures: A case-control study of 669 subjects. Frontiers in Surgery, 8, 754150. https://doi.org/10.3389/fsurg.2021.754150
Graf, R. M., Shaw, J. T., Simske, N. M., Siy, P. N., Siy, A. B., Kliethermes, S. A., & Whiting, P. S. (2023). Distal femur nonunion: Risk factors and validation of RUST scores. OTA International: The Open Access Journal of Orthopaedic Trauma, 6, e234. https://doi.org/10.1097/oi9.0000000000000234
Rodriguez, E. K., Boulton, C., Weaver, M. J., Herder, L. M., Morgan, J. H., Chacko, A. T., Appleton, P. T., Zurakowski, D., & Vrahas, M. S. (2014). Predictive factors of distal femoral fracture nonunion after lateral locked plating: A retrospective multicenter case-control study of 283 fractures. Injury, 45(3), 554–559. https://doi.org/10.1016/j.injury.2013.10.042
Karam, J., Campbell, P., David, M., & Hunter, M. (2019). Comparison of outcomes and analysis of risk factors for non-union in locked plating of closed periprosthetic and non-periprosthetic distal femoral fractures in a retrospective cohort study. J Orthop Surg Res., 14(1), 150. https://doi.org/10.1186/s13018-019-1204-z.
Howick, J. C. I., Glasziou, P., Greenhalgh, T., Heneghan, C., Liberati, A., Moschetti, I., Phillips, B., Thornton, H., Goddard, O., & Hodgkinson, M. (2011). The 2011 Oxford CEBM levels of evidence. Oxford Centre for Evidence-Based Medicine.
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetzlaff, J. M., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J., Grimshaw, J. M., Hrobjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo-Wilson, E., McDonald, S., … Moher, D. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ, 372, n71. https://doi.org/10.1136/bmj.n71
Cumpston, M., Li, T., Page, M. J., Chandler, J., Welch, V. A., Higgins, J. P., & Thomas, J. (2019). Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database of Systematic Reviews, 10, ED000142. https://doi.org/10.1002/14651858.ED000142
Sterne, J. A., Hernan, M. A., Reeves, B. C., Savovic, J., Berkman, N. D., Viswanathan, M., Henry, D., Altman, D. G., Ansari, M. T., Boutron, I., Carpenter, J. R., Chan, A. W., Churchill, R., Deeks, J. J., Hrobjartsson, A., Kirkham, J., Juni, P., Loke, Y. K., Pigott, T. D., … Higgins, J. P. (2016). ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ, 355, i4919. https://doi.org/10.1136/bmj.i4919
Nicholson, J. A., Makaram, N., Simpson, A., & Keating, J. F. (2021). Fracture nonunion in long bones: A literature review of risk factors and surgical management. Injury, 52(Suppl 2), S3–S11. https://doi.org/10.1016/j.injury.2020.11.029
Hou, G., Zhou, F., Tian, Y., Ji, H., Zhang, Z., Guo, Y., Lv, Y., Yang, Z., & Zhang, Y. (2020). Analysis of risk factors for revision in distal femoral fractures treated with lateral locking plate: A retrospective study in Chinese patients. Journal of Orthopaedic Surgery and Research, 15(1), 318. https://doi.org/10.1186/s13018-020-01850-z
Tornetta, P., III., Della Rocca, G. J., Morshed, S., Jones, C., Heels-Ansdell, D., Sprague, S., Petrisor, B., Jeray, K. J., Del Fabbro, G., Bzovsky, S., & Bhandari, M. (2020). Risk factors associated with infection in open fractures of the upper and lower extremities. J Am Acad Orthop Surg Glob Res Rev, 4(12), e20.00188. https://doi.org/10.5435/JAAOSGlobal-D-20-00188
Hellwinkel, J. E., Working, Z. M., Certain, L., García, A. J., Wenke, J. C., & Bahney, C. S. (2022). The intersection of fracture healing and infection: Orthopaedics research society workshop 2021. Journal of Orthopaedic Research, 40(3), 541–552. https://doi.org/10.1002/jor.25261
Wittauer, M., Burch, M. A., McNally, M., Vandendriessche, T., Clauss, M., Della Rocca, G. J., Giannoudis, P. V., Metsemakers, W. J., & Morgenstern, M. (2021). Definition of long-bone nonunion: a scoping review of prospective clinical trials to evaluate current practice. Injury, 52(11), 3200–3205. https://doi.org/10.1016/j.injury.2021.09.008
Cunningham, B. P., Brazina, S., Morshed, S., & Miclau, T., 3rd. (2017). Fracture healing: a review of clinical, imaging and laboratory diagnostic options. Injury, 48(Suppl 1), S69–S75. https://doi.org/10.1016/j.injury.2017.04.020
Roberts, T. T., & Rosenbaum, A. J. (2012). Bone grafts, bone substitutes and orthobiologics: The bridge between basic science and clinical advancements in fracture healing. Organogenesis, 8(4), 114–124. https://doi.org/10.4161/org.23306
Morshed, S. (2014). Current options for determining fracture union. Advances in Medicine, 2014, 708574. https://doi.org/10.1155/2014/708574
Corrales, L. A., Morshed, S., Bhandari, M., & Miclau, T., 3rd. (2008). Variability in the assessment of fracture-healing in orthopaedic trauma studies. Journal of Bone and Joint Surgery. American Volume, 90(9), 1862–1868. https://doi.org/10.2106/jbjs.G.01580
Bhandari, M., Guyatt, G. H., Swiontkowski, M. F., Tornetta, P., 3rd., Sprague, S., & Schemitsch, E. H. (2002). A lack of consensus in the assessment of fracture healing among orthopaedic surgeons. Journal of Orthopaedic Trauma, 16(8), 562–566. https://doi.org/10.1097/00005131-200209000-00004
Knox, A. M., McGuire, A. C., Natoli, R. M., Kacena, M. A., & Collier, C. D. (2021). Methodology, selection, and integration of fracture healing assessments in mice. Journal of Orthopaedic Research, 39(11), 2295–2309. https://doi.org/10.1002/jor.25172
Thomas, J. D., & Kehoe, J. L. (2024). Bone nonunion. In StatPearls. StatPearls Publishing Copyright © 2024, StatPearls Publishing LLC.
Schmal, H., Brix, M., Bue, M., Ekman, A., Ferreira, N., Gottlieb, H., Kold, S., Taylor, A., Toft Tengberg, P., & Ban, I. (2020). Nonunion—Consensus from the 4th annual meeting of the Danish Orthopaedic Trauma Society. EFORT Open Reviews, 5(1), 46–57. https://doi.org/10.1302/2058-5241.5.190037
Claireaux, H. A., Searle, H. K., Parsons, N. R., & Griffin, X. L. (2022). Interventions for treating fractures of the distal femur in adults. Cochrane Database Systematic Review, 10(10), CD010606. https://doi.org/10.1002/14651858.CD010606.pub3
Amorosa, L. F., Jayaram, P. R., Wellman, D. S., Lorich, D. G., & Helfet, D. L. (2014). The use of the 95-degree-angled blade plate in femoral nonunion surgery. European Journal of Orthopaedic Surgery & Traumatology, 24(6), 953–960. https://doi.org/10.1007/s00590-013-1267-1
Özdemir, A., Odabaşı, E., Eravsar, E., Safalı, S., & Acar, M. A. (2023). Treatment of recalcitrant femur nonunion with pedicled corticoperiosteal medial femoral condyle flap. Science and Reports, 13(1), 20326. https://doi.org/10.1038/s41598-023-47432-x
Gangavalli, A. K., & Nwachuku, C. O. (2016). Management of distal femur fractures in adults: An overview of options. Orthopedic Clinics of North America, 47(1), 85–96. https://doi.org/10.1016/j.ocl.2015.08.011
Hu, M., Zeng, W., Zhang, J., Feng, Y., Ma, L., Huang, F., & Cai, Q. (2023). Fixators dynamization for delayed union and non-union of femur and tibial fractures: A review of techniques, timing and influence factors. Journal of Orthopaedic Surgery and Research, 18(1), 577. https://doi.org/10.1186/s13018-023-04054-3
Stolberg-Stolberg, J., Fuchs, T., Lodde, M. F., Rosslenbroich, S., Garcia, P., Raschke, M., & Everding, J. (2022). Addition of shock wave therapy to nail dynamization increases the chance of long-bone non-union healing. Journal of Orthopaedics and Traumatology, 23(1), 4. https://doi.org/10.1186/s10195-021-00620-9
Mukhopadhaya, J., Ranjan, R., Sinha, A. K., & Bhadani, J. S. (2022). The management of aseptic non-unions of distal femur fractures with anatomical lateral locking plates. Strategies in Trauma and Limb Reconstruction, 17(3), 137–143. https://doi.org/10.5005/jp-journals-10080-1564
van Trikt, C. H., Donders, J. C. E., Klinger, C. E., Wellman, D. S., Helfet, D. L., & Kloen, P. (2022). Operative treatment of nonunions in the elderly: Clinical and radiographic outcomes in patients at minimum 75 years of age. BMC Geriatrics, 22(1), 985. https://doi.org/10.1186/s12877-022-03670-8
Koval, K. J., Seligson, D., Rosen, H., & Fee, K. (1995). Distal femoral nonunion: Treatment with a retrograde inserted locked intramedullary nail. Journal of Orthopaedic Trauma, 9(4), 285–291. https://doi.org/10.1097/00005131-199509040-00003
Wu, C. C. (2016). Retrograde dynamic locked intramedullary nailing for aseptic supracondylar femoral nonunion after dynamic condylar screw treatment. European Journal of Orthopaedic Surgery & Traumatology, 26(6), 625–631. https://doi.org/10.1007/s00590-016-1800-0
Saxena, V., Akshay, V., Panwar, A., & Kumar, S. (2023). Management of non-union distal femur fractures with augmentation nail plate construct. Cureus, 15(4), e37173. https://doi.org/10.7759/cureus.37173
Liporace, F. A., Tang, A., Jankowski, J. M., & Yoon, R. S. (2022). Distal femur: Nail plate combination and the linked construct. OTA International, 5(3), e172. https://doi.org/10.1097/oi9.0000000000000172
Cavusoglu, A. T., Ozsoy, M. H., Dincel, V. E., Sakaogullari, A., Basarir, K., & Ugurlu, M. (2009). The use of a low-profile Ilizarov external fixator in the treatment of complex fractures and non-unions of the distal femur. Acta Orthopaedica Belgica, 75(2), 209–218.
Rohilla, R., Sharma, P. K., Dua, M., Singh, R., Beniwal, D., & Khokhar, A. (2023). Outcome of monolateral rail fixator in infected nonunion of femur diaphysis developing after intramedullary fixation. European Journal of Orthopaedic Surgery & Traumatology, 33(4), 1223–1230. https://doi.org/10.1007/s00590-022-03275-2
Murphy, N. J., Graan, D., Briggs, G. D., & Balogh, Z. J. (2023). Acute minimally invasive bone grafting of long bone fractures to reduce the incidence of fracture non-union. Medical Hypotheses, 178, 111131.
Flierl, M. A., Smith, W. R., Mauffrey, C., Irgit, K., Williams, A. E., Ross, E., Peacher, G., Hak, D. J., & Stahel, P. F. (2013). Outcomes and complication rates of different bone grafting modalities in long bone fracture nonunions: A retrospective cohort study in 182 patients. Journal of Orthopaedic Surgery and Research, 8, 33. https://doi.org/10.1186/1749-799X-8-33
Vaishya, R., Singh, A. P., Hasija, R., & Singh, A. P. (2011). Treatment of resistant nonunion of supracondylar fractures femur by megaprosthesis. Knee Surgery, Sports Traumatology, Arthroscopy, 19(7), 1137–1140. https://doi.org/10.1007/s00167-011-1416-1
Rajasekaran, R. B., Palanisami, D. R., Natesan, R., Jayaramaraju, D., & Rajasekaran, S. (2020). Reply to “Megaprosthesis in distal femur nonunions in elderly patients-experience from twenty-four cases: A letter to editor.” International Orthopaedics, 44(10), 2191–2192. https://doi.org/10.1007/s00264-020-04586-x
Vaishya, R., Thapa, S. S., & Vaish, A. (2020). Non-neoplastic indications and outcomes of the proximal and distal femur megaprosthesis: A critical review. Knee Surgery and Related Research, 32(1), 18. https://doi.org/10.1186/s43019-020-00034-7
Lu, J., Guo, S. C., Wang, Q. Y., Sheng, J. G., & Tao, S. C. (2020). J-bone graft with double locking plate: A symphony of mechanics and biology for atrophic distal femoral non-union with bone defect. Journal of Orthopaedic Surgery and Research, 15(1), 144. https://doi.org/10.1186/s13018-020-01636-3
Vaishya, R., Gupta, B. M., Mamdapur, G. M. N., Vaish, A., Bhadani, J. S., & Mukhopadhaya, J. (2024). Highly-cited papers on fracture non-union—A bibliometric analysis of the global literature (1990–2023). Indian Journal of Orthopaedics, 1–12.
Georgeanu, V. A., Gingu, O., Antoniac, I. V., & Manolea, H. O. (2023). Current options and future perspectives on bone graft and biomaterials substitutes for bone repair, from clinical needs to advanced biomaterials research. Applied Sciences, 13(14), 8471.
Polmear, M. M., Anderson, A. B., Lanier, P. J., Orr, J. D., Nesti, L. J., & Dunn, J. C. (2021). Bone morphogenetic protein in scaphoid nonunion: A systematic review. Journal of Wrist Surgery, 10(3), 184–189. https://doi.org/10.1055/s-0040-1722332
Lampert, F. M., Momeni, A., Filev, F., Torio-Padron, N., Finkenzeller, G., Stark, G. B., Steiner, D., & Koulaxouzidis, G. (2015). Utilization of a genetically modified muscle flap for local BMP-2 production and its effects on bone healing: A histomorphometric and radiological study in a rat model. Journal of Orthopaedic Surgery and Research, 10, 55. https://doi.org/10.1186/s13018-015-0196-6
Sadat-Ali, M., Al-Omar, H. K., AlTabash, K. W., AlOmran, A. K., AlDakheel, D. A., & AlSayed, H. N. (2023). Genetic influence of fracture nonunion (FNU): A systematic review. Pharmacogenomics and Personalized Medicine, 16, 569–575. https://doi.org/10.2147/PGPM.S407308
Salichos, L., Thayavally, R., Kloen, P., & Hadjiargyrou, M. (2024). Human nonunion tissues display differential gene expression in comparison to physiological fracture callus. Bone, 183, 117091. https://doi.org/10.1016/j.bone.2024.117091
De la Vega, R. E., Atasoy-Zeybek, A., Panos, J. A., Vang, M., Evans, C. H., & Balmayor, E. R. (2021). Gene therapy for bone healing: Lessons learned and new approaches. Translational Research, 236, 1–16. https://doi.org/10.1016/j.trsl.2021.04.009
Pietu, G., & Ehlinger, M. (2017). Minimally invasive internal fixation of distal femur fractures. Orthopaedics & Traumatology, Surgery & Research, 103(1S), S161–S169. https://doi.org/10.1016/j.otsr.2016.06.025
Beeres, F. J. P., Emmink, B. L., Lanter, K., Link, B. C., & Babst, R. (2020). Minimally invasive double-plating osteosynthesis of the distal femur. Operative Orthopädie und Traumatologie, 32(6), 545–558. https://doi.org/10.1007/s00064-020-00664-w
Schuijt, H. J., Hundersmarck, D., Smeeing, D. P. J., van der Velde, D., & Weaver, M. J. (2021). Robot-assisted fracture fixation in orthopaedic trauma surgery: A systematic review. OTA International, 4(4), e153. https://doi.org/10.1097/OI9.0000000000000153
Yi, Z., Lim, R. Q. R., Chen, W., Zhu, J., Chen, S., & Liu, B. (2024). Arthroscopic bone grafting and robot-assisted fixation for scaphoid nonunion. Orthopaedic Surgery, 16(1), 254–262. https://doi.org/10.1111/os.13930
Szwed-Georgiou, A., Plocinski, P., Kupikowska-Stobba, B., Urbaniak, M. M., Rusek-Wala, P., Szustakiewicz, K., Piszko, P., Krupa, A., Biernat, M., Gazinska, M., Kasprzak, M., Nawrotek, K., Mira, N. P., & Rudnicka, K. (2023). Bioactive materials for bone regeneration: Biomolecules and delivery systems. ACS Biomaterials Science & Engineering, 9(9), 5222–5254. https://doi.org/10.1021/acsbiomaterials.3c00609
Warwick, R., Willatt, J. M., Singhal, B., Borremans, J., & Meagher, T. (2009). Comparison of computed tomographic and magnetic resonance imaging in fracture healing after spinal injury. Spinal Cord, 47(12), 874–877. https://doi.org/10.1038/sc.2009.59
Rani, S., Bandyopadhyay-Ghosh, S., Ghosh, S. B., & Liu, G. (2020). Advances in sensing technologies for monitoring of bone health. Biosensors (Basel). https://doi.org/10.3390/bios10040042
Windolf, M., Varjas, V., Gehweiler, D., Schwyn, R., Arens, D., Constant, C., Zeiter, S., Richards, R. G., & Ernst, M. (2022). Continuous implant load monitoring to assess bone healing status-evidence from animal testing. Medicina (Kaunas, Lithuania). https://doi.org/10.3390/medicina58070858
Ali, F., & Saleh, M. (2002). Treatment of distal femoral nonunions by external fixation with simultaneous length and alignment correction. Injury, 33(2), 127–134. https://doi.org/10.1016/s0020-1383(01)00032-8.
Alt, V., Meyer, C., Litzlbauer, H. D., & Schnettler, R. (2007). Treatment of a double nonunion of the femur by rhBMP-2. Journal of Orthopaedic Trauma, 21(10), 734–737. https://doi.org/10.1097/BOT.0b013e3181589700
Bellabarba, C., Ricci, W. M., & Bolhofner, B. R. (2002). Indirect reduction and plating of distal femoral nonunions. Journal of Orthopaedic Trauma, 16(5), 287–296. https://doi.org/10.1097/00005131-200205000-00001
Chen, X., Li, J. J., Kong, Z., Yang, D. X., & Yuan, X. N. (2011). Autologous grafts of double-strut fibular cortical bone plate to treat the fractures and defects of distal femur: A case report and review of literature. Chinese Journal of Traumatology, 14(4), 241–246.
Davila, J., Malkani, A., & Paiso, J. M. (2001). Supracondylar distal femoral nonunions treated with a megaprosthesis in elderly patients: A report of two cases. Journal of Orthopaedic Trauma, 15(8), 574–578. https://doi.org/10.1097/00005131-200111000-00009
Ebraheim, N. A., Buchanan, G. S., Liu, X., Cooper, M. E., Peters, N., Hessey, J. A., & Liu, J. (2016). Treatment of distal femur nonunion following initial fixation with a lateral locking plate. Orthopaedic Surgery, 8(3), 323–330. https://doi.org/10.1111/os.12257
Gardner, M. J., Toro-Arbelaez, J. B., Harrison, M., Hierholzer, C., Lorich, D. G., & Helfet, D. L. (2008). Open reduction and internal fixation of distal femoral nonunions: Long-term functional outcomes following a treatment protocol. Journal of Trauma, 64(2), 434–438. https://doi.org/10.1097/01.ta.0000245974.46709.2e
Graves, M. L., Ryan, J. E., & Mast, J. W. (2005). Supracondylar femur nonunion associated with previous vascular repair: Importance of vascular exam in preoperative planning of nonunion repair. Journal of Orthopaedic Trauma, 19(8), 574–577. https://doi.org/10.1097/01.bot.0000151818.63175.b9
Hailer, Y. D., & Hoffmann, R. (2006). Management of a nonunion of the distal femur in osteoporotic bone with the internal fixation system LISS (less invasive stabilization system). Archives of Orthopaedic and Trauma Surgery, 126(5), 350–353. https://doi.org/10.1007/s00402-006-0102-0
Holzman, M. A., Hanus, B. D., Munz, J. W., O’Connor, D. P., & Brinker, M. R. (2016). Addition of a medial locking plate to an in situ lateral locking plate results in healing of distal femoral nonunions. Clinical Orthopaedics and Related Research, 474(6), 1498–1505. https://doi.org/10.1007/s11999-016-4709-3
Ma, C. H., Chiu, Y. C., Tu, Y. K., Yen, C. Y., & Wu, C. H. (2017). Three-stage treatment protocol for recalcitrant distal femoral nonunion. Archives of Orthopaedic and Trauma Surgery, 137(4), 489–498. https://doi.org/10.1007/s00402-017-2634-x
Monroy, A., Urruela, A., Singh, P., Tornetta, P., 3rd., & Egol, K. A. (2014). Distal femur nonunion patients can expect good outcomes. The Journal of Knee Surgery, 27(1), 83–87. https://doi.org/10.1055/s-0033-1349402
Oh, J. K., Hwang, J. H., Lee, S. J., & Kim, J. I. (2011). Dynamization of locked plating on distal femur fracture. Archives of Orthopaedic and Trauma Surgery, 131(4), 535–539. https://doi.org/10.1007/s00402-010-1202-4
Oransky, M., Galante, C., Cattaneo, S., Milano, G., Motta, M., Biancardi, E., Grava, G., Johnson, E. E., & Casiraghi, A. (2023). Endosteal plating for the treatment of malunions and nonunions of distal femur fractures. European Journal of Orthopaedic Surgery & Traumatology, 33(6), 2243–2251. https://doi.org/10.1007/s00590-022-03458-x
Ozdemir, A., Odabasi, E., Eravsar, E., Safali, S., & Acar, M. A. (2023). Treatment of recalcitrant femur nonunion with pedicled corticoperiosteal medial femoral condyle flap. Science and Reports, 13(1), 20326. https://doi.org/10.1038/s41598-023-47432-x
Palatnik, Y., & Rozbruch, S. R. (2011). Femoral reconstruction using external fixation. Advances in Orthopedics, 2011, 967186. https://doi.org/10.4061/2011/967186
Pao, J. L., & Jiang, C. C. (2005). Retrograde intramedullary nailing for nonunions of supracondylar femur fracture of osteoporotic bones. Journal of the Formosan Medical Association, 104(1), 54–59.
Rajasekaran, R. B., Palanisami, D. R., Natesan, R., Jayaramaraju, D., & Rajasekaran, S. (2020). Megaprosthesis in distal femur nonunions in elderly patients-experience from twenty four cases. International Orthopaedics, 44(4), 677–684. https://doi.org/10.1007/s00264-019-04383-1
Reynolds, A. W., Melvin, P. R., Yakish, E. J., Sotereanos, N., Altman, G. T., & Sewecke, J. J. (2021). Use of tantalum trabecular metal cones for management of nonunion of the distal femur with segmental bone defects: Technique and case series. Journal of Orthopaedic Case Reports, 11(7), 19–23. https://doi.org/10.13107/jocr.2021.v11.i07.2298
Rollo, G., Pichierri, P., Grubor, P., Marsilio, A., Bisaccia, M., Grubor, M., Pace, V., Lanzetti, R. M., Giaracuni, M., Filipponi, M., & Meccariello, L. (2019). The challenge of nonunion and malunion in distal femur surgical revision. Medicinski Glasnik (Zenica). https://doi.org/10.17392/1016-19
Saridis, A., Panagiotopoulos, E., Tyllianakis, M., Matzaroglou, C., Vandoros, N., & Lambiris, E. (2006). The use of the Ilizarov method as a salvage procedure in infected nonunion of the distal femur with bone loss. Journal of Bone and Joint Surgery. British Volume, 88(2), 232–237. https://doi.org/10.1302/0301-620X.88B2.16976
Tis, J. E., Reiter, F. O., & Saleh, M. (2005). Treatment of a supracondylar femoral nonunion in a patient with osteoporosis by square osteotomy and acute shortening. Injury, 36(3), 454–457. https://doi.org/10.1016/j.injury.2004.11.009
Vellingiri, K., & Nagakumar, J. S. (2021). Infected non-union of the distal femur. Cureus, 13(1), e12613. https://doi.org/10.7759/cureus.12613
Wang, J. W., & Weng, L. H. (2003). Treatment of distal femoral nonunion with internal fixation, cortical allograft struts, and autogenous bone-grafting. Journal of Bone and Joint Surgery. American Volume, 85(3), 436–440. https://doi.org/10.2106/00004623-200303000-00006
Waseem, Z., Ford, M., Syed, K., & Flannery, J. (2010). Chronic nonunion in a patient with bilateral supracondylar distal femur fractures treated successfully with twice daily low-intensity pulsed ultrasound. PM & R, 2(2), 159–161. https://doi.org/10.1016/j.pmrj.2009.11.008
Wu, C. C. (2011). Retrograde dynamic locked nailing for aseptic nonunion of femoral supracondyle after antegrade locked nailing. Archives of Orthopaedic and Trauma Surgery, 131(4), 513–517. https://doi.org/10.1007/s00402-010-1183-3
Wu, C. C. (2011). Modified retrograde-locked nailing for aseptic femoral supracondylar nonunion with severe osteoporosis in elderly patients. Journal of Trauma, 71(2), E26–E30. https://doi.org/10.1097/TA.0b013e3181f64ab1
Yoshida, A., Yajima, H., Murata, K., Maegawa, N., Kobata, Y., Kawamura, K., & Takakura, Y. (2009). Pedicled vascularized bone graft from the medial supracondylar region of the femur for treatment of femur nonunion. Journal of Reconstructive Microsurgery, 25(3), 165–170. https://doi.org/10.1055/s-0028-1103503
Zhang, J. H., Liu, H., Cai, T. Y., Lin, Y. Z., & Wu, J. (2023). Resistant distal femoral nonunion treated with combined nail/plate construct and reamer-irrigator-aspirator technique. Journal of International Medical Research, 51(7), 3000605231187945. https://doi.org/10.1177/03000605231187945
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Contributions
FM: literature search, statistical analysis, study selection and data extraction, risk of bias assessment, drafting (original and revision); LS: literature search, study selection and data extraction, risk of bias assessment; FS: editing; AV: editing; JSB: literature search, manuscript preparation, and editing, RV: conception and design, drafting (original and revision). All authors have agreed to the final version to be published and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have any competing interests in this article.
Ethical Approval
This study complies with ethical standards.
Informed Consent
For this type of study informed consent is not required.
Consent to Participate
Not applicable.
Consent to Publish
Not applicable.
Registration and Protocol
The present review was not registered.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Migliorini, F., Schäfer, L., Simeone, F. et al. Management of Distal Femoral Non-union: A Systematic Review. JOIO (2024). https://doi.org/10.1007/s43465-024-01205-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s43465-024-01205-4