
Abstract
Purpose
To analyze clinical, radiographic and patient-reported outcomes of distal metaphyseal femoral nonunions treated with fixed-angle plates and screws.
Methods
All patients presenting with a distal metaphyseal femoral fracture nonunion repaired with fixed-angle plating from one urban level 1 trauma center and an orthopedic specialty hospital were identified. Baseline demographic, injury information, and outcomes (healing rates, Short Musculoskeletal Function Assessment, range of motion, and post-operative pain levels) at 12 months following nonunion repair were collected. Outcomes were evaluated between patients fixed with a blade plate and with a locking plate.
Results
Of these 31 patients, 27 (87.1%) healed after their index nonunion surgery, 2 (6.5%) healed after one reoperation, 1 (3.2%) healed after 2 reoperations, and 1 (3.2%) had a persistent nonunion but did not want further treatment. At one-year follow-up, the group demonstrated a significant improvement in functional recovery with a mean difference of 14.5 points (p = 0.007) when compared to status before fixed-angle fixation of the nonunion. There was also a significant change in patient-reported pain levels using the VAS scale with a mean difference of 2.0 points (p = 0.009). At one-year follow-up, 11 (39.3%) had full knee range of motion (0–130), 11 (39.3%) had flexion greater than 90 and less than 120°, and 6 (21.4%) had range of motion less than 90°.
Conclusion
Patients who undergo fixed angle plating and autogenous bone grafting for distal femoral metapyseal nonunions demonstrate improved functional outcomes and VAS pain score at one year follow up.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Nonunion about the distal femoral metaphysis is a rare but difficult problem to treat. Nonunion is a complication that occurs when the biological process of fracture-healing fails following bony fracture [1]. The incidence of fracture nonunion is determined by a range of patient-independent factors, such as inadequate mechanical stability, bone loss or poor reduction, and patient-dependent factors, such smoking status or underlying medical conditions [2,3,4]. Distal femoral fracture nonunions have a higher incidence in the elderly but are generally rare due to the exceptional vascular supply and prevalence of cancellous bone [5].
Implants for the treatment of these meta-diaphyseal fractures have developed and changed over the years and currently include fixed-angle options such as the 95-degree condylar blade plate or a pre-contoured locking distal femoral plate. The 95-degree condylar blade plate was previously the gold standard for distal femur fixation and is excellent for stability [6], but over the last few decades, fixed and variable angle locking screw-plate constructs have been developed and are now widely used due to less technical difficulty [7]. Several advantages of locking plates include: the lack of contact needed for the bone to attain stability [8], technically easier application and potentially less soft tissue exposure than blade plates [6, 9, 10] and the ability to place fixation in areas of the bone dictated by the specific fracture pattern. Biomechanical analyses have demonstrated that locking plates may possess improved characteristics compared to blade plates in distal femoral fractures in strength with overall and cyclic loading [9] and stiffness in axial compression and average maximal load [11].
While several studies have examined the benefits and drawbacks of using blade plates versus locking plates in metaphyseal femoral fractures, their findings conflict, and there is a lack of data investigating the outcomes of the use of fixed-angle fixation (blade and locking plates) for distal femoral nonunions as well as an absence of patient-reported outcomes to evaluate these two implants when used in these applications. The purpose of this study was to examine the radiographic, clinical and functional outcomes of a consecutive group of patients treated for a metaphyseal distal femur nonunion using a standardized algorithm of nonunion takedown, fixed-angle implants and placement of autogenous iliac crest bone graft.
Materials and methods
Between 2004 and 2022 565 patients treated by one of four orthopedic traumatologists for a long bone fracture nonunion at an urban level 1 trauma center and an orthopedic specialty hospital were enrolled prospectively at the time of their fracture nonunion treatment in an IRB-approved database.
For this study, all patients who presented with distal metaphyseal femoral fracture nonunion and underwent operative treatment with a blade plate or a locking plate were reviewed. Of the 565 patients with long bone nonunions followed prospectively 32 patients (5.7%) presented with a distal metaphyseal nonunion.
Demographic data were collected at the time of enrollment including age, sex, BMI, Charlson Comorbidity Index (CCI), tobacco, alcohol and drug use, and insurance status. Injury information was also gathered including open fracture status, soft tissue injuries, presence of additional orthopedic trauma, and nonunion class defined as atrophic, oligotrophic, or hypertrophic according Weber and Cech [12].
All patients underwent surgical treatment for their metaphyseal femoral fracture nonunion using standard operative algorithms. This included: an infection workup, removal of failed implant if present, open repair of the nonunion with or without deformity correction if present and iliac crest bone grafting as needed. Cultures were obtained at all revision surgical procedures. All patients weight bearing was limited for the first 6 weeks post-op as non or 30% weight bearing depending on factors such as age and bone quality. After 6 weeks all were advanced to weight bearing as tolerated. Physiotherapy for knee range of motion and quadriceps strengthening was begun after the first post-operative visit.
Patient follow-up medical information including radiologic healing, clinical outcomes and functional score was collected at 3 months, 6 months, 12 months, and at any subsequent annual follow-ups. Presence of infection was determined by the results of the intraoperative cultures. Functional outcome was assessed by the Short Musculoskeletal Function Assessment (SMFA) score. Clinical outcome was assessed with a visual analog scale (VAS) pain score, hip or knee range of motion (ROM) of the injured area. Radiographic healing was assessed using standard biplanar radiography and CT scans obtained for surgical planning. Complications, implant failures, and the need for reoperations were also recorded in real time.
Chi-square tests of association and independent-samples t-tests were used to determine differences of outcomes collected at 12 months between patients treated with a blade plate and patients treated with a locking plate. All analyses were conducted using IBM SPSS version 25.0 software (Armonk, NY) and were considered statistically significant for p < 0.05.
Results
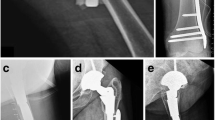
The 32 patients who underwent repair of a distal metaphyseal femoral fracture nonunion with plating were reviewed for analysis. Thirty (93.8%) were treated with a LP (Fig. 1) and 2 (6.3%) were treated with a BP. One patient with a LP was lost to follow-up and was excluded from final outcome analysis.

a An AP femoral radiograph of a 75-year-old with a nonunion of the right distal femur fracture status post previous attempt at repair elsewhere, who presents with implant failure. b Coronal CT confirmation of the nonunion. c Intraoperative picture of the nonunion site repaired with a fixed-angle locking plate and autogenous iliac crest graft packed at the site d–e AP and lateral radiographs at 9 months status post nonunion repair demonstrating bony union
The mean age was 52.6 years (19.8 to 93.5 years). Nineteen patients were female (61.3%) and twelve were male (38.7%). The time from initial injury to nonunion surgery was 16.5 months (4 to 90 months). Demographic information is provided (Online Resource 1). The majority of patients had low energy injury mechanisms (51.6%). At their initial injuries, 7 (22.6%) patients had an open fracture, 11 (35.5%) patients had bone loss, and 8 (25.8%) patients had additional orthopedic trauma. As classified by nonunion type, 18 (58.1%) patients had atrophic nonunions, 6 (19.4%) patients had hypertrophic nonunions, and 7 (22.6%) patients had oligotrophic nonunions. Two patients (6.5%) presented with gross deformity. Injury information is provided (Table 1).
Overall, 30/31 (97%) nonunions ultimately united. Of these patients, 27 (87.1%) healed after their index nonunion surgery, 2 (6.5%) had persistent nonunions and healed after one reoperation with a second bone graft, 1 (3.2%) developed a deep surgical site infection after negative intraoperative cultures and healed after 2 reoperations, and 1 (3.2%) had a persistent nonunion following their index nonunion surgery but did not want further treatment. Healing rates, number of complications, and number of implant failures between location are provided (Table 2).
At one-year follow-up, the group demonstrated a significant improvement in functional recovery and pain score when compared to pre repair status. There was an improvement in total SMFA score with a mean difference of 14.5 points (p = 0.007) when compared pre repair status. There was a significant difference in the standardized functional subcategory of the SMFA with a mean difference of 13.5 points (p = 0.014). There was no significant difference in the standardized bothersome index and emotional index (p = 0.056 and p = 0.209, respectively). There was also a significant change in patient-reported pain levels using the VAS scale with a mean difference of 2.0 points (p = 0.009; Table 3).
Regarding knee range of motion at one-year follow-up, 11 (39.3%) had full range of motion (0–130), 11 (39.3%) had knee flexion greater than 90 and less than 120°, and 6 (21.4%) had knee range of motion less than 90°. Four patients (12.9%) had complications which included two patients with persistent nonunion who underwent revision surgery including bone grafting, one who developed radiographic osteonecrosis of the anterior lateral femoral condyle and required no treatment, and one developed a deep surgical site infection after negative intraoperative cultures that underwent irrigation and debridement and intravenous antibiotic treatment. One patient (3.2%) had surprise positive intraoperative cultures and was treated with IV antibiotics and never developed symptoms of infection. None of these patients had complications with their iliac crest graft site.
Discussion
This study indicates that patients with fixed-angle plating with iliac crest bone graft for distal femoral nonunions is a successful strategy for repair of these metaphyseal nonunion. Patients have improved patient-reported functional outcomes and VAS pain scores at one year of follow-up. Our analysis demonstrated the majority of patients with this fixed-angle plating healed following initial nonunion surgery.
Poor bone quality of the metaphysis plays a major role in the ability for implants to maintain stability over the length of time needed for healing of metaphyseal fractures. The establishment of fixed-angle internal fixation has improved the management of periarticular fractures as the fixed-angle element of the implant provides direct support for the articulating fragment [13]. Locking plates, which have become increasingly popular over the last 20 years, are a relatively more recent development which lock the screw head in the plate with a threaded chamber on the plate, allowing the plate and screws to function as a fixed-angle implant and offer angular stability [5, 14]. Locking plates have the theoretical advantages that they need less contact on the bone for stability [8] and that they require less soft tissue exposure to implant than traditional historic fixed-angle blade plates [6, 9, 10].
One study comparing plating of distal femoral fractures reported that those treated with a locking plate for an acute distal femoral fracture developed a nonunion at a greater rate 15.8% vs. 3.4% than those treated with a blade plate for an acute fracture [15]. Another institution reviewed four cases of failure of locking plates for acute distal femoral fractures over one year (18% incidence) and found the cause of failure to be delayed union/nonunion, early weight bearing, and unacceptable plate placement [16]. This conflicts with a review of ununited distal femoral fractures in which the authors observed a higher incidence of distal femoral fracture nonunions for fractures treated with angled blade plates compared to locking plates [17]. The material properties of plates may also influence the healing rates of these fractures as one study found that 41% of distal femur fractures treated with stainless steel plates resulted in nonunion while only 10% of those treated with titanium plates resulted in nonunion [18]. The feeling that the lower modulus of titanium allowing for more flexibility during healing may be advantageous. The length of the working length of the plate and screw construct also may impact healing as one study demonstrated that it was less likely for locking plates with a length of ≥ 9 holes to fail than shorter plates for distal femur fractures [19]. Our study differs from these in that we report on use of these implants for established nonunions, rather than acute fractures.
Patients treated for distal femoral nonunions have comparable functional outcomes to patients treated for acute distal femur fractures as long as union is achieved [20]. Another study reported that age should not be a factor to decide against surgical treatment of distal femur fractures as elderly patients treated with modern operative techniques experience good clinical and radiographic outcomes when compared to younger patients [21]. A systematic review of distal femoral fracture nonunions determined that the most common treatment for this complication is fixed-angle plating with cancellous autografting, with union achieved under this method in 75 out of 77 cases (97.4%) [17]. Our report of 31 patients confirms these conclusions, with all but one patient ultimately achieving union. We feel the conclusions from the current study contribute to a more comprehensive understanding of outcomes of patients undergoing surgical treatment of distal metaphyseal femoral fracture nonunion with fixed-angle implants by including patient-reported functional outcomes. In comparison, one paper that investigated treatment techniques of distal tibia fracture nonunions also recommended fixed-angle plating as this method led to high union rates and low complication rates with union achieved in 36 out of 37 cases reported (97.3%) [22].
This study has several limitations, including the distribution of implant type. In the population tested, the majority of distal metaphyseal femoral fracture nonunions were treated with a locking plate or blade plate. We do not have a comparison group of similar injuries treated with nails. Also, this distribution restricted our ability to run statistical analyses comparing the two types of fixed-angle plates. A larger sample size with a more even distribution of implant would help to compare outcomes more accurately by implant type. Furthermore, there are large standard deviations for the SMFA index scores meaning that there is a large spread of the patients’ SMFA scores at one-year follow-up. This limitation could also be remedied with a larger sample size, as a greater number of patients could produce more accurate mean values and therefore a more accurate comparison of mean values.
In conclusion, the strategy of using fixed-angle plating with autogenous iliac crest autograft for a distal metaphyseal femoral nonunion is a successful one. There is a great healing rate with a low complication profile. Clinical and functional results demonstrate improvement from baseline. Surgeons should feel confident in the use of this algorithm when treating these complex injuries.
References
Brinker MR, O’Connor DP (2016) The biological basis for nonunions. JBJS Rev. https://doi.org/10.2106/JBJS.RVW.15.00078
Niikura T, Lee SY, Sakai Y, Nishida K, Kuroda R, Kurosaka M (2014) Causative factors of fracture nonunion: the proportions of mechanical, biological, patient-dependent, and patient-independent factors. J Orthop Sci 19(1):120–124. https://doi.org/10.1007/s00776-013-0472-4
Zura R, Xiong Z, Einhorn T, Watson JT, Ostrum RF, Prayson MJ et al (2016) Epidemiology of fracture nonunion in 18 human bones. JAMA Surg 151(11):e162775. https://doi.org/10.1001/jamasurg.2016.2775
Egol KA, Bechtel C, Spitzer AB, Rybak L, Walsh M, Davidovitch R (2012) Treatment of long bone nonunions: factors affecting healing. Bull NYU Hosp Jt Dis 70(4):224–231
Egol KA, Koval KJ, Zuckerman J (2015) Handbook of fractures, 5th edn. Wolters Kluwer Health, New York
Harder Y, Martinet O, Barraud GE, Cordey J, Regazzoni P (1999) The mechanics of internal fixation of fractures of the distal femur: a comparison of the condylar screw (DCS) with the condylar plate (CP). Injury 30(Suppl 1):A31–A39. https://doi.org/10.1016/s0020-1383(99)00124-2
Hake ME, Davis ME, Perdue AM, Goulet JA (2019) Modern implant options for the treatment of distal femur fractures. J Am Acad Orthop Surg 27(19):e867–e875. https://doi.org/10.5435/JAAOS-D-17-00706
Wagner M (2003) General principles for the clinical use of the LCP. Injury 34(Suppl 2):B31-42. https://doi.org/10.1016/j.injury.2003.09.023
Higgins TF, Pittman G, Hines J, Bachus KN (2007) Biomechanical analysis of distal femur fracture fixation: fixed-angle screw-plate construct versus condylar blade plate. J Orthop Trauma 21(1):43–46. https://doi.org/10.1097/BOT.0b013e31802bb372
Strauss EJ, Schwarzkopf R, Kummer F, Egol KA (2008) The current status of locked plating: the good, the bad, and the ugly. J Orthop Trauma 22(7):479–486. https://doi.org/10.1097/BOT.0b013e31817996d6
Jaakkola JI, Lundy DW, Moore T, Jones B, Ganey TM, Hutton WC (2002) Supracondylar femur fracture fixation: mechanical comparison of the 95 degrees condylar side plate and screw versus 95 degrees angled blade plate. Acta Orthop Scand 73(1):72–76. https://doi.org/10.1080/000164702317281440
Weber BG, Cech O (1976) Pseudarthrosis: pathophysiology, biomechanics, therapy, results. Grune & Stratton, New York
Orbay J, Badia A, Khoury RK, Gonzalez E, Indriago I (2004) Volar fixed-angle fixation of distal radius fractures: the DVR plate. Tech Hand Up Extrem Surg 8(3):142–148. https://doi.org/10.1097/01.bth.0000126570.82826.0a
Cronier P, Pietu G, Dujardin C, Bigorre N, Ducellier F, Gerard R (2010) The concept of locking plates. Orthop Traumatol Surg Res. https://doi.org/10.1016/j.otsr.2010.03.008
Vallier HA, Immler W (2012) Comparison of the 95-degree angled blade plate and the locking condylar plate for the treatment of distal femoral fractures. J Orthop Trauma 26(6):327–332. https://doi.org/10.1097/BOT.0b013e318234d460
Button G, Wolinsky P, Hak D (2004) Failure of less invasive stabilization system plates in the distal femur: a report of four cases. J Orthop Trauma 18(8):565–570. https://doi.org/10.1097/00005131-200409000-00015
Ebraheim NA, Martin A, Sochacki KR, Liu J (2013) Nonunion of distal femoral fractures: a systematic review. Orthop Surg 5(1):46–50. https://doi.org/10.1111/os.12017
Rodriguez EK, Zurakowski D, Herder L, Hall A, Walley KC, Weaver MJ et al (2016) Mechanical construct characteristics predisposing to non-union after locked lateral plating of distal femur fractures. J Orthop Trauma 30(8):403–408. https://doi.org/10.1097/BOT.0000000000000593
Ricci WM, Streubel PN, Morshed S, Collinge CA, Nork SE, Gardner MJ (2014) Risk factors for failure of locked plate fixation of distal femur fractures: an analysis of 335 cases. J Orthop Trauma 28(2):83–89. https://doi.org/10.1097/BOT.0b013e31829e6dd0
Monroy A, Urruela A, Singh P, Tornetta P 3rd, Egol KA (2014) Distal femur nonunion patients can expect good outcomes. J Knee Surg 27(1):83–87. https://doi.org/10.1055/s-0033-1349402
Shulman BS, Patsalos-Fox B, Lopez N, Konda SR, Tejwani NC, Egol KA (2014) Do elderly patients fare worse following operative treatment of distal femur fractures using modern techniques? Geriatr Orthop Surg Rehabil 5(1):27–30. https://doi.org/10.1177/2151458514525041
Reed LK, Mormino MA (2008) Distal tibia nonunions. Foot Ankle Clin 13(4):725–735. https://doi.org/10.1016/j.fcl.2008.09.001
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflicts of interest related to the contents of this manuscript. Authorship has been granted only to those individuals who have contributed substantially to the research or manuscript. No sources of funding have been granted for this study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Landes, E.K., Konda, S.R., Leucht, P. et al. Fixed-angle plate fixation and autogenous iliac crest graft for repair of distal metaphyseal femoral nonunion. Eur J Orthop Surg Traumatol 33, 1835–1839 (2023). https://doi.org/10.1007/s00590-022-03366-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00590-022-03366-0