
Abstract
Introduction
The 95-degree-fixed angle blade plate has been in use for decades for both acute femoral fractures and nonunions. Our objective was to examine the results of use by a single surgeon of the 95-degree-angled blade plate in proximal and distal femoral nonunion surgery.
Patients and methods
The nonunion database of a single surgeon over a 16 year period was used to identify all proximal and distal femoral nonunions that were treated with open reduction and internal fixation using the 95-degree-angled blade plate. There were 78 cases in which the blade plate was used, and 68 of 78 (87.2 % follow-up rate) were followed to a final outcome, which was defined as complete healing of the nonunion, conversion to arthroplasty, or amputation. Failure was defined as revision surgery for persistence of nonunion, conversion to arthroplasty prior to healing, or amputation. Three patients who failed were lost to follow-up prior to a final outcome.
Results
In the 71 patients who were followed to failure or complete follow-up, the rate of healing with one surgery was 77.5 % (55 of 71). Eight of 16 failures required a second surgery for persistence of nonunion and eventually went on to heal the nonunion. Eleven of the 16 failures were in patients who had a known infected nonunion. When the 21 cases of infected nonunions were excluded, the healing rate for aseptic nonunions with one surgery alone using the 95-degree-angled blade plate was 91.2 % (52 of 57) compared with 47.6 % (10 of 21) in the infected nonunion group (p < 0.0001). Eleven patients who had healed their nonunion underwent all or partial removal of the implant for irritation or prominence.
Conclusion
The 95-degree-angled blade plate is an effective reduction aid and fixation device for aseptic nonunions of the proximal and distal femur with acceptable healing rates with one surgery alone.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Nonunions of the proximal and distal femur are challenging treatment problems. With the advent of periarticular locking plates, proximal femoral and distal femoral locking plates are becoming more frequently used for both acute fracture care and nonunion surgery. Recent literature reports evidence of failure of locking plate technology in acute proximal and distal femur fractures [2, 3, 4, 5, 7, 8]. Very little evidence exists to support the use of locking plates in nonunion surgery of the femur.
In contrast, the 95-degree-angled blade plate, a fixed-angle device for which locking plate technology is largely based upon, has been used for decades in both acute femoral fractures and nonunions [1]. The blade plate offers theoretical and practical advantages over periarticular locking plate technology. The blade creates a very small footprint in metaphyseal bone, impacting it only slightly, whereas metaphyseal locking screws have large diameters and create multiple large screw paths in the metaphysis and subchondral bone, leaving very little bone available for fixation, especially in revision situations. The articulated tensioning device is a commonly used intraoperative tool employed with the blade plate to load or create compression across a fracture or nonunion. Anecdotally, when the articulated tensioning device is used to load a fracture or nonunion against a periarticular locking plate, it often tends to cause slight loosening of the tight-fitting metaphyseal locking screws and can shift the fracture into varus. However, the blade plate has its own disadvantages. It is considered a technically demanding implant and must be placed correctly in multiple planes, whereas periarticular locking plates allow for more leeway in screw placement and plate location and sometimes can even be placed sitting off of the bone with efficacy.
In this study, we report the results of a single surgeon using the 95-degree-angled blade plate for proximal and femoral nonunions. We examined the rate of healing, secondary surgeries, and implant-related complications. We hypothesized that the use of the 95-degree blade plate for proximal and distal femoral nonunion would have an acceptable rate of healing and complications given the challenge of treating these nonunions.
Materials and methods
A nonunion database approved by the Institutional Review Board containing all nonunions operated on by the senior author was searched between 1992 and 2008 using the AO/OTA classifications 31, 32, and 33 as search criteria, which were proximal, diaphyseal, and distal femoral fractures. Once all the femoral nonunions were identified, the search criteria was further narrowed to nonunions of the proximal or distal femur in which the implant used for fixation was the 95-degree fixed-angle blade plate. Two hundred and thirty-six femoral nonunions were indentified, of which 126 were proximal or distal femoral nonunions (78 proximal, 48 distal).
These patients’ charts were reviewed, and the following data recorded: age at the time of index procedure, gender, mechanism of injury, side of injury, location of the femoral nonunion, whether or not the fracture was open, number of prior surgeries for the fracture, length of time between the injury and the index procedure, active tobacco use and other comorbidities, intraoperative blood loss, any administration of intraoperative blood transfusion, length of surgery, whether or not the nonunion was infected, time to healing, length of hospital stay, complications, subsequent surgeries related to the nonunion or implant, time to healing, length of time to final follow-up, and final follow-up physical exam range of motion. A nonunion was defined as lack of bridging callus on 3 of 4 cortices on orthogonal radiographs by 6 months after surgery, no signs of healing radiographically by 2 months postoperatively with signs of progressive loss of reduction or a malreduced fracture, or failure of the prior implant after at least a month after the prior surgery. Whenever in doubt, a CT was used to confirm nonunion. Proximal femoral nonunions included all intertrochanteric, pertrochanteric, and subtrochanteric nonunions. Distal femoral nonunions included nonunions of the distal metadiaphyseal region and supracondylar femur.
Seventy-eight consecutive cases of femoral nonunion in 77 patients were identified in which the 95-degree blade plate was used for fixation of a proximal or distal femoral nonunion between 1992 and 2008 by the senior author (DLH). Average patient age was 59 years (range 19–96). Mechanism of injury was fall from standing in 34, motor vehicle accident in 14, skiing in 9, pedestrian struck in 6, fall from height in 3, pathologic in 3, previous iatrogenic osteotomy in 3, motorcycle accident in 2, bicycle accident in 2, gunshot wound in 1, and ice skating in 1. Sixty-eight of 78 cases (87.2 % follow-up rate) were followed through to a final outcome, which we defined as complete healing of the nonunion, conversion to arthroplasty, or amputation. Complete healing was defined as bridging callus on 3 of 4 cortices on orthogonal views as documented by the senior author or his fellow at the time of follow-up office visit. Failure was defined as revision surgery for persistence of nonunion, conversion to arthroplasty prior to healing, or amputation. Three patients failed the index procedure, required a revision procedure, and then were lost to follow-up prior to complete healing. They were included as failures. The remaining 7 patients were lost to follow-up prior to healing and had no known revision surgery. They were included in patient demographics and operative details, but were excluded from outcome data. Table 1 compares patient demographics, operative details, and time to healing between the patients with proximal and distal femoral nonunion.
SPSS version 16 was used for statistical analysis. The unpaired t test was used to compare means between proximal and distal femoral outcomes. The Fisher's exact text was used to compare noncontinuous values, and a p value <0.05 was considered to be statistically significant.
Surgical treatment principles
We indicate the 95-degree-angled blade plate for nonunions of the intertrochanteric, pertrochanteric, and subtrochanteric regions of the proximal femur as well as the metadiaphyseal and supracondylar regions of the distal femur (Figs. 1, 2). For femoral shaft nonunions, we normally employ an intramedullary nail for fixation of the nonunion and do not use the blade plate. For any nonunions involving intra-articular fragments, these pieces are addressed separately with supplementary lag screw fixation. In all cases, the patient is positioned supine on a radiolucent operating table, and a lateral subvastus approach to the femoral nonunion is made incorporating prior skin incisions. Prior implants are removed. The nonunion is thoroughly debrided. In cases where infection is a concern, preoperative antibiotics are held and intraoperative cultures are taken. The blade plate is implanted using standard technique described in detail elsewhere, which entails preoperatively templating from the contralateral normal femur and checking placement in coronal, sagital, and axial planes [10]. The supine position and intraoperative fluoroscopy allow intraoperative radiographs of the contralateral leg to compare alignment and confirm it is acceptable in all planes. The blade portion of the implant is normally used as a reduction device with the blade inserted first and the fracture reduced to the plate. If the blade is inserted in the correct plane and location, this maneuver will normally restore the femur to within 5 degrees or less of anatomic alignment when compared to the contralateral limb. Alternatively, if preoperative planning reveals alignment will not be restored by reducing the nonunion to the plate, a second 3.5 mm pelvic reconstruction plate placed on the anterior cortex can be used to provisionally hold the nonunion in alignment while the blade plate is implanted. In some cases, this second plate is kept in place as supplementary fixation. The articulating tensioning device is used to load the fracture when more compression across the fracture is sought. If the nonunion is not a simple fracture pattern and there is a large degree of comminution or bone defect, the articulating tensioning device is not used. Bone graft, either in the form of iliac crest bone graft or demineralized bone matrix or both, is placed at the nonunion site. The hip and knee are taken through a full range of motion prior to closure to ensure there is no block to motion and the construct is stable to range of motion. The wound is closed in layers over a drain. The patient is allowed to place 20 lbs of weight on the operative leg in the first 6 weeks postoperatively with gentle passive and active range of motion permitted. If radiographs show signs of early healing at 6 weeks postoperatively, progression to full weightbearing is begun over the ensuing 2–4 weeks.

a Anteroposterior and lateral radiographs of an 81-year-old female 14 months after a fall from standing in which she sustained a left subtrochanteric hip fracture that underwent closed reduction and cephalomedullary nailing at an outside institution. She continued to have pain and was found to have a nonunion of the subtrochanteric fracture with a broken implant. She underwent removal of the implant and revision open reduction and internal fixation with the 95-degree blade plate and demineralized bone matrix. b Follow-up radiographs of the leg at six months postoperatively showed a healed fracture with no further progression of preexisting arthritis

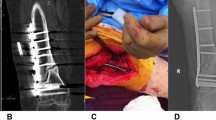
a and b A 28-year-old female was involved in a motor vehicle accident in another country in which she suffered multiple injuries including a left open supracondylar femur fracture that underwent multiple surgeries, including spanning external fixation. c She then underwent open reduction and internal fixation with bone grafting using a dynamic condylar buttress plate and multiple interfragmentary screws 3 weeks postinjury, which failed to result in union at 12 months postinjury. d She subsequently underwent removal of prior implants, revision open reduction, and internal fixation using the 95-degree-angled blade plate, along with iliac crest bone grafting and arthrolysis of the knee and had healed the nonunion by 3 months postoperatively. e The implant was eventually removed for irritation, and final knee range of motion at 4 years postoperatively was 0 to 105 degrees. (Figure published with the permission of Gardner M, Toro J, Harrison M, et al. Open reduction and internal fixation of distal femoral nonunions: long-term functional outcomes using a treatment protocol. Journal of Trauma: Injury, Infection, and Critical Care. Feb 2008: 434–8.)
Results
In the 71 patients who were followed to failure or complete follow-up, the rate of healing with one surgery using the 95-degree-angled blade plate was 77.5 % (55 of 71). Sixteen patients were considered failures. Eight of the 16 failures were in patients who needed a second surgery for persistence of nonunion and eventually went on to heal their nonunion (Table 2). Of the remaining 8 failures that did not eventually heal, 3 were lost to follow-up. Of the remaining 5 patients that failed to eventually heal, one patient had a history of 70 pack years of smoking, alcoholism, and opioid dependence with an open distal femur fracture with bone loss and had had 6 prior procedures for infected nonunion and osteomyelitis prior to the blade plate procedure. He underwent a subsequent revision procedure with persistence of nonunion that also failed and eventually went on to an above knee amputation. The rest of the failures that did not heal and were not lost to follow-up was in proximal femur patients converted to total hip arthroplasty (THA): two patients had a persistent infected nonunion and preferred staged conversion to THA rather than subsequent revision open reduction and internal fixation (ORIF); another patient had an infected nonunion in which the blade plate cut out from the femoral neck and had a staged conversion to THA; the fourth patient had an infected nonunion which underwent revision for persistence of nonunion and then suffered a fall in which she suffered a peri-implant fracture distal to the implant, at which time she elected to have a staged THA. Of the 16 cases of failure, 11 were in patients who had an infected nonunion either known prior to the index procedure or discovered at the time of the index procedure through positive intraoperative cultures. When the 21 cases of infected nonunions were excluded, the healing rate of aseptic nonunions with one surgery using the blade plate was 91.2 % (52 of 57). This was a statistically significant higher rate of healing compared with the 10 of 21 (47.6 %) cases of infected nonunion, which healed with one surgery alone when the blade plate was used (p < 0.0001) (Table 3).
Two other patients required arthroplasty conversions but were not considered failures. The first patient healed his proximal femur fracture, but went on to develop avascular necrosis of the femoral head by two years postoperatively and was converted to THA. The second patient had preexisting knee arthritis prior to the injury and healed her distal femoral nonunion, but was eventually referred for a total knee arthroplasty (TKA) for painful arthritis.
Another 11 patients required all or part of their implant removed after healing of the fracture for prominence or irritation (14.1 %, 11 of 78).
In the 35 of 37 proximal femoral patients available for final follow-up evaluation, hip range of motion was at least 0–90 degrees of flexion. One patient’s final range of motion was not recorded although he performed all functional activities well, and the other patient had hip flexion from 0 to 80 degrees. In the 27 distal femoral nonunion patients available for final follow-up range of motion evaluation, 10 had at least 0–120 degrees, another 13 had at least 0–90 degrees, and the remaining four had less than 90 degrees; however, range of motion had improved from preoperative evaluation in all of them.
Discussion
Femoral nonunions can be challenging to treat effectively and oftentimes require multiple procedures prior to successful healing [15]. For femoral diaphyseal nonunions, intramedullary nailing with or without opening of the nonunion site depending on the degree of alignment correction necessary can be employed with success. Exchange intramedullary nailing results in less soft tissue stripping, less bone devitalization, and less blood loss, with high rates of healing and minimal complications [11]. Shroeder et al. reported an 86 % healing rate with exchange nailing of femoral shaft nonunions. However, proximal and distal femoral nonunions can be more challenging to treat for several reasons. Unlike the diaphysis where fixation can be attained with a large intramedullary rod and interlocking screws, in the metaphysis and metadiaphyseal regions, there is less area for good fixation, the bone is usually more osteopenic, and tracts from prior implants make good fixation difficult [16].
Periarticular locking plate technology for both the proximal and distal femur has been introduced within the past decade as one possible solution to acute fractures of the pertrochanteric, subtrochanteric, distal femoral, and supracondylar regions. Biomechanical data in a cadaveric subtrochanteric fracture model showed a cephalomedullary nail to withstand the most load to failure and more cycles to failure compared with a proximal femoral locking plate or the 95-degree blade plate [6]. A recent biomechanical study of distal femoral fixation methods used synthetic osteoporotic bone models and compared torsional and axial loading to failure of different intramedullary implants and periarticular locking plates and found higher torsional stiffness of the locking plates but higher axial loads to failure of the intramedullary implants. The study did not test the biomechanical properties of the angled blade plate [14].
While biomechanical testing is revealing, it often does not recreate the actual clinical scenario. The 95-degree blade plate has several distinct advantages over a nail or periarticular locking plates, specifically in nonunion situations. In a proximal femoral nonunion, if a cephalomedullary device was previously used, there is usually very little bone left in the femoral neck and head for nonunion treatment using another cephalomedullary nailing. Therefore, other options must be considered, including supplemental cement fixation and conversion to arthroplasty [9, 16].
While periarticular locking plates are one option for nonunion fixation, there is little evidence for their use in proximal or distal femoral nonunion surgery. The surgeon has little to no tactile sense of the actual fixation obtained with these implants, especially in revision nonunion situations with metaphyseal bone loss and preexisting osteoporosis. Clinically, when periarticular locking plates have been compared to the 95-degree-angled blade plate in acute fracture surgery, results have been equivocal. A study comparing outcomes of a distal femoral locking plate to the 95-degree-angled blade plate found a higher rate of complications and nonunions as well as more secondary surgeries related to complications and prominent implants in the locking plate group [13]. Furthermore, in the last few years, there have been several studies reporting on complications in periarticular locking plates designed for both the proximal and distal femur [2, 3, 4, 5, 7, 8].
In this study, we found an overall 76.1 % rate of healing with one surgery with the use of the 95-degree-angled blade plate for proximal and femoral nonunions. Of the 16 patients who did not heal with the initial surgery, 8 went on to eventually heal with a secondary procedure. When we excluded the cases of infected nonunion, the healing rate of the blade plate with one surgery alone was 91.2 %. Over half of infected nonunions resulted in failure when the blade plate was utilized. This study confirms previous findings of others who have shown infected nonunions have higher failure rates with revision surgery [11, 12]. Our findings suggest that in the presence of a known infected nonunion or when underlying infection is suspected as a cause of femoral nonunion, it may be prudent to perform the nonunion surgery in two stages [12]. It is possible that the large stainless steel implant of the blade plate allows bacterial seeding permitting persistent infection and eventual failure.
There are limitations to this study. It is a retrospective study, and several patients were lost to follow-up. We also did not obtain functional outcome scores for these patients. However, final follow-up range of motion was available. Even though we do not have functional outcome scores, we would expect that final functional outcome would be lower in this group of patients, given that they all had at least one prior surgery and many of whom had several, and additionally many were infected. It would be difficult to conclude that the implant used was a major factor in the final functional outcome; it could be just as likely due to the state of the soft tissues from multiple operations. Given these potential confounders, we felt the most important outcome tested for this group of patients is the healing rate of the nonunion with the use of this technique and implant.
When only aseptic nonunions were considered, the 95-degree blade plate had a high rate of healing with one surgery and an acceptable rate of implant removal. While technically demanding, this older implant has certain clinical advantages over the newer and more expensive periarticular locking plates that have become popular in acute fracture care and nonunion surgery over the past decade. The blade plate has a smaller bony footprint, can be used more effectively with the articulated tensioning device to load the construct, and is less expensive. The inherent design of the blade plate along with a lower stiffness than locking plate constructs may also contribute to successful healing. It does however require careful preoperative planning and intraoperative vigilance. More clinical evidence comparing the blade plate to periarticular locking plate technology in the setting of femoral nonunion surgery is necessary. Until then, the 95-degree-angled blade plate remains an option to consider for proximal and distal femoral nonunion surgery.
References
Altenberg AR, Shorkey RL (1949) Blade-plate fixation in non-union and in complicated fractures of the supracondylar region of the femur. J Bone Joint Surg Am 31A(2):312–316
Berkes MB, Little MT, Lazaro LE, Cymerman RM, Helfet DL, Lorich DG (2012) Catastrophic failure after open reduction internal fixation of femoral neck fractures with a novel locking plate implant. J Orthop Trauma. doi:10.1097/BOT.0b013e31823b4cd1
Button G, Wolinsky P, Hak D (2004) Failure of less invasive stabilization system plates in the distal femur: a report of four cases. J Orthop Trauma 18(8):565–570
Ebraheim NA, Liu J, Hashmi SZ, Sochacki KR, Moral MZ, Hirschfeld AG (2012) High complication rate in locking plate fixation of lower periprosthetic distal femur fractures in patients with total knee arthroplasties. J Arthroplasty 27(5):809–813. doi:10.1016/j.arth.2011.08.007
Ehlinger M, Adam P, Arlettaz Y, Moor BK, DiMarco A, Brinkert D, Bonnomet F (2011) Minimally-invasive fixation of distal extra-articular femur fractures with locking plates: limitations and failures. Orthop Traumatol Surg Res 97(6):668–674. doi:10.1016/j.otsr.2011.05.004
Forward DP, Doro CJ, O’Toole RV, Kim H, Floyd JC, Sciadini MF (2012) A biomechanical comparison of a locking plate, a nail, and a 95 degrees angled blade plate for fixation of subtrochanteric femoral fractures. J Orthop Trauma 26(6):334–340. doi:10.1097/BOT.0b013e3182254ea3
Glassner PJ, Tejwani NC (2011) Failure of proximal femoral locking compression plate: a case series. J Orthop Trauma 25(2):76–83. doi:10.1097/BOT.0b013e3181e31ccc
Henderson CE, Kuhl LL, Fitzpatrick DC, Marsh JL (2011) Locking plates for distal femur fractures: is there a problem with fracture healing? J Orthop Trauma 25(Suppl 1):S8–S14. doi:10.1097/BOT.0b013e3182070127
Kammerlander C, Gebhard F, Meier C, Lenich A, Linhart W, Clasbrummel B, Blauth M (2011) Standardised cement augmentation of the PFNA using a perforated blade: a new technique and preliminary clinical results. A prospective multicentre trial. Injury 42(12):1484–1490. doi:10.1016/j.injury.2011.07.010
Mast J, Jakob R, Ganz R (1989) Planning and Reduction Technique in Fracture Surgery. Springer, Berlin
Shroeder JE, Mosheiff R, Khoury A, Liebergall M, Weil YA (2009) The outcome of closed, intramedullary exchange nailing with reamed insertion in the treatment of femoral shaft nonunions. J Orthop Trauma 23(9):653–657. doi:10.1097/BOT.0b013e3181a2a337
Struijs PA, Poolman RW, Bhandari M (2007) Infected nonunion of the long bones. J Orthop Trauma 21(7):507–511. doi:10.1097/BOT.0b013e31812e5578
Vallier HA, Immler W (2012) Comparison of the 95-degree angled blade plate and the locking condylar plate for the treatment of distal femoral fractures. J Orthop Trauma 26(6):327–332. doi:10.1097/BOT.0b013e318234d460
Wahnert D, Hoffmeier K, Frober R, Hofmann GO, Muckley T (2011) Distal femur fractures of the elderly–different treatment options in a biomechanical comparison. Injury 42(7):655–659. doi:10.1016/j.injury.2010.09.009
Weresh MJ, Hakanson R, Stover MD, Sims SH, Kellam JF, Bosse MJ (2000) Failure of exchange reamed intramedullary nails for ununited femoral shaft fractures. J Orthop Trauma 14(5):335–338
Zickel RE (1988) Nonunions of fractures of the proximal and distal thirds of the shaft of the femur. Instr Course Lect 37:173–179
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Amorosa, L.F., Jayaram, P.R., Wellman, D.S. et al. The use of the 95-degree-angled blade plate in femoral nonunion surgery. Eur J Orthop Surg Traumatol 24, 953–960 (2014). https://doi.org/10.1007/s00590-013-1267-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00590-013-1267-1