
Abstract
Parathyroid lipoadenoma is an unusual cause of primary hyperparathyroidism. Only a few earlier reports have documented parathyroid imaging in diagnostic studies of parathyroid lipoadenoma. Our case was a 27-year-old man, who was originally diagnosed with primary hyperparathyroidism. He underwent a Tc-99m sestamibi dual-phase parathyroid imaging study, which revealed a right-inferior parathyroid hyperfunctional lesion. The first operation removed a lesion of 1.5 cm in diameter in the area, and parathyroid lipoadenoma was diagnosed by pathology. However, hypercalcemia persisted. One week later, a Tc-99m sestamibi whole-body scan and another dual-phase imagining were performed, which demonstrated a residual lesion in the inferior part of the right thyroid region, while no ectopic lesion was found. A second surgery was performed and pathological diagnosis was confirmed as parathyroid lipoadenoma again. Our case demonstrated that although hyperfunctional parathyroid lipoadenoma is rare, Tc-99m sestamibi parathyroid imaging is reliable in locating the lesion for surgical purposes. And Tc-99m sestamibi imaging is useful in reoperative and persistent hyperparathyroidism situations as well.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Parathyroid lipoadenoma is a rare entity that is composed of parathyroid chief cells and fatty stroma [1–5]. The name of parathyroid lipoadenoma was first used by Abul-Haj et al. [6] who reported such a case. This variant of adenoma has been reported to be hyperfunctional in most cases, although incidental finding at autopsy of nonfunctional case has also been documented [7]. To date, approximately, forty cases have been reported [2, 4, 8]. However, to our knowledge, only three cases used parathyroid imaging for diagnosis and localization [9–11]. Two of them showed that Tc-99m sestamibi imaging could locate the position of the parathyroid lipoadenoma [10, 11]. We report a case of parathyroid lipoadenoma in which Tc-99m sestamibi parathyroid imaging was useful to detect a residual lesion after the first operation.
Case report
A 27-year-old Chinese male patient was admitted to our hospital on account of a 3-year history of ostealgia and multiple fractures that were progressively aggravated. Physical examination showed the patient had a palpable mass in the right thyroid lobe area. Laboratory examination was remarkable for elevated calcium, parathyroid hormone, and alkaline phosphatase levels of 3.44 mmol/L (normal 2.15–2.55 mmol/L), 158.0 pmol/L (normal 1.1–7.3 pmol/L) and 1112 U/L (normal 39–117 U/L), respectively. His phosphorus level was as low as 0.60 mmol/L (normal 0.8–1.6 mmol/L). Hepatic and renal functions were normal. The diagnosis of primary hyperparathyroidism was made based on patient history, physical examination and laboratory data.
He was then referred to our department for parathyroid imaging for preoperative evaluation. Tc-99m sestamibi dual-phase parathyroid scan was performed as follows: early phase and delayed phase scans of the neck were obtained 5 min and 60 min after the injection of 15 mCi Tc-99m sestamibi, respectively. Planar images were obtained by using a high-resolution low-energy parallel-hole collimator and a large-field-of-view dual-detector SPECT/CT (Discovery VH; General Electric Medical Systems). The images were recorded in a 256 × 256 matrix, and then processed by dedicated computers. Subsequently, a right-inferior parathyroid hyperfunctional lesion was revealed (Fig. 1).

The first Tc-99m sestamibi scan. Anterior image of a early phase at 5 minutes, b delayed phase at 60 min of the neck after the injection of Tc-99m sestamibi. High uptake lesion was found in the inferior part of right thyroid gland
Nine days after the first parathyroid imaging, parathyroidectomy was performed. This operation removed a lesion of 1.5 cm in diameter. H&E staining of the histopathological specimen (magnification 40×) showed the tumor was made up of chief parathyroid cells arranged in nests or cords and interspersed adipose tissue (Fig. 2). Hence, parathyroid lipoadenoma was diagnosed.

On histopathological examination, the tumor excised during the first operation was found to be a parathyroid lipoadenoma which was made up of parathyroid cells and interspersed adipose tissue, and some areas (arrow) showed large number of adipocytes (H&E staining, magnification ×40)
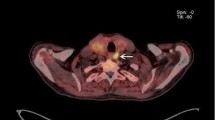
Postoperative serum monitoring showed calcium levels to be 2.95, 3.05, 2.98 and 2.86 mmol/L at 1, 2, 5 and 12 days after the first operation, respectively. Persistent hypercalcemia prompted us to perform a second Tc-99m sestamibi scan 7 days after the first operation. In the second Tc-99m sestamibi scan, we added whole body scan at 40 min after the injection of 15 mCi of Tc-99m sestamibi. Tc-99m sestamibi scan demonstrated a residual lesion in the inferior part of right thyroid region, with no ectopic lesion found (Fig. 3). The second surgery was done 12 days after the first operation, and the histopathological findings were the same as those of the first removed lipoadenoma, and residual parathyroid lipoadenoma was confirmed.

The second Tc-99m sestamibi scan. Anterior image of a early phase at 5 minutes, b delayed phase at 60 min of the neck, c whole body scan at 40 min after the injection of Tc-99m sestamibi. Residual lesion was found in the inferior part of right thyroid gland
Discussion
Lipoadenoma of the parathyroid gland is a rare histological variant of parathyroid adenoma that is usually functional and associated with clinical hyperparathyroidism. Most of the reported cases had been investigated from pathological or surgical perspectives. Differential diagnosis in pathology should include parathyroid adenoma, thyroid adenoma, thyroid lipoadenoma, parathyroid carcinoma, and thyroid carcinoma, with the last two being the lesions of the greatest concern [1–5]. This fat-containing tumor may grossly resemble lipoma more than parathyroid adenoma, so distinguishing these lesions can be challenging during intraoperative consultation, and more importantly en bloc parathyroidectomy could be compromised [5]. Although a surgeon’s experience contributes a lot to a successful parathyroidectomy, a sestamibi scan can help to focus the surgeon’s attention on a specific site, and a prominent change in surgical trends from extensive bilateral neck exploration to minimally invasive radio-guided parathyroidectomy (MIRP) also holds promise to avoid the risks of re-operation [12–14]. When planning a concise MIRP, an accurate preoperative localizing imaging, which is mainly Tc-99m sestamibi-based scintigraphy, is mandatory. During the procedure of MIRP, usually a low dose of 1 mCi of Tc-99m sestamibi is injected to the patient a few minutes before the start of operation and then hand-held gamma probes are used to guide surgeons to find the lesions. Therefore, the MIRP procedure is simple and efficient, and it shortens the mean operating time, minimizes complications and reduces the risk of re-operation.
Only few earlier cases of parathyroid lipoadenoma had parathyroid imaging data. Bleiweiss et al. [9] first reported a case in which nuclear medicine imaging was performed for diagnosis and localization. However, the radiolabeled thallium scan failed to demonstrate evidence of an adenoma, presumably because of the tumor’s high fat content. Nguyen et al. [10] and Turner et al. [11] used Tc-99m sestamibi imaging to locate parathyroid lipoadenoma. They reported that the lesion might be demonstrated on the basis of the space-occupying appearance or the target-to-background signal ratio might be low. Unlike the previously reported cases, the present case showed a good target-to-background signal ratio in Tc-99m sestamibi imaging, which is probably due to (1) the comparatively large size of the lesion and (2) the dominant percentage of the lesion being composed of parathyroid chief cells.
Tc-99m sestamibi parathyroid imaging is based on the difference in clearance rates between the thyroid and diseased parathyroid glands. Several authors have demonstrated that the use of preoperative Tc-99m sestamibi scanning in patients with primary hyperparathyroidism may reduce operative time, surgical failure rate, and complication rates [15, 16]. And most authors agree that a preoperative Tc-99m sestamibi scanning is significantly helpful in the evaluation of ectopic, recurrent, reoperative or persistent hyperparathyroidism [10, 17]. Indeed, retrospectively speaking, our case showed that whole body imaging is very necessary to rule out ectopic parathyroid lesions in the first Tc-99m sestamibi scan even though fully suspected lesions were already pointed out in other examinations, and this acquisition does not take much examination time. And more importantly, the present case justified the usefulness of Tc-99m sestamibi whole-body scan and Tc-99m sestamibi dual-phase parathyroid imaging in reoperative and persistent hyperparathyroidism situations.
References
Sheikh SS, Massloom HS. Lipoadenoma: is it arising from thyroid or parathyroid? A diagnostic dilemma. ORL J Otorhinolaryngol Relat Spec. 2002;64:448–50.
Fischer I, Wieczorek R, Sidhu GS, Pei Z, West B, Lee P. Myxoid lipoadenoma of parathyroid gland: a case report and literature review. Ann Diagn Pathol. 2006;10:294–6.
Daboin KP, Ochoa-Perez V, Luna MA. Adenolipomas of the head and neck: analysis of 6 cases. Ann Diagn Pathol. 2006;10:72–6.
Rastogi A, Jain M, Agarawal T, Mishra AK, Gupta S, Agarwal A. Parathyroid lipoadenoma: case report and review of the literature. Indian J Pathol Microbiol. 2006;49:404–6.
Ducatman BS, Wilkerson SY, Brown JA. Functioning parathyroid lipoadenoma. Report of a case diagnosed by intraoperative touch preparations. Arch Pathol Lab Med. 1986;110:645–7.
Abul-Haj SK, Conklin H, Hewitt WC. Functioning lipoadenoma of the parathyroid gland. Report of a unique case. N Engl J Med. 1962;266:121–3.
Uden P, Berglund J, Zederfeldt B, Aspelin P, Ljungberg O. Parathyroid lipoadenoma: a rare cause of primary hyperparathyroidism. Case report. Acta Chir Scand. 1987;153:635–9.
Chow LS, Erickson LA, Abu-Lebdeh HS, Wermers RA. Parathyroid lipoadenomas: a rare cause of primary hyperparathyroidism. Endocr Pract. 2006;12:131–6.
Bleiweiss IJ, Harpaz N, Strauchen JA, Wagner R, Biller HF. Functioning lipoadenoma of the parathyroid: case report and literature review. Mt Sinai J Med. 1989;56:114–7.
Nguyen BD. Parathyroid imaging with Tc-99m sestamibi planar and SPECT scintigraphy. Radiographics. 1999;19:601–14. discussion 15–6.
Turner WJ, Baergen RN, Pellitteri PK, Orloff LA. Parathyroid lipoadenoma: case report and review of the literature. Otolaryngol Head Neck Surg. 1996;114:313–6.
Rubello D, Mariani G, Pelizzo MR. Minimally invasive radio-guided parathyroidectomy on a group of 452 primary hyperparathyroid patients: refinement of preoperative imaging and intraoperative procedure. Nuklearmedizin. 2007;46:85–92.
Rubello D, Gross MD, Mariani G, AL-N A. Scintigraphic techniques in primary hyperparathyroidism: from pre-operative localisation to intra-operative imaging. Eur J Nucl Med Mol Imaging. 2007;34:926–33.
Rubello D, Pelizzo MR, Boni G, Schiavo R, Vaggelli L, Villa G, et al. Radioguided surgery of primary hyperparathyroidism using the low-dose 99mTc-sestamibi protocol: multiinstitutional experience from the Italian Study Group on Radioguided Surgery and Immunoscintigraphy (GISCRIS). J Nucl Med. 2005;46:220–6.
Denham DW, Norman J. Cost-effectiveness of preoperative sestamibi scan for primary hyperparathyroidism is dependent solely upon the surgeon’s choice of operative procedure. J Am Coll Surg. 1998;186:293–305.
Sofferman RA, Nathan MH, Fairbank JT, Foster RS Jr, Krag DN. Preoperative technetium Tc 99m sestamibi imaging Paving the way to minimal-access parathyroid surgery. Arch Otolaryngol Head Neck Surg. 1996;122:369–74.
Allendorf J, Kim L, Chabot J, DiGiorgi M, Spanknebel K, LoGerfo P. The impact of sestamibi scanning on the outcome of parathyroid surgery. J Clin Endocrinol Metab. 2003;88:3015–8.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Meng, Z., Zhang, M., Tan, J. et al. Tc-99m sestamibi parathyroid imaging in a rare case of parathyroid lipoadenoma. Ann Nucl Med 23, 317–320 (2009). https://doi.org/10.1007/s12149-009-0249-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12149-009-0249-1