
Abstract
Purpose
Breast cancer is the most common malignancy in women in terms of incidence and mortality. Age is undoubtedly the biggest breast cancer risk factor. In this study we examined clinical, histological, and biological characteristics and mortality of breast cancer in elderly women along with their changes with advancing age.
Methods
We reviewed 63 original articles published between 2006 and 2016 concerning women over 70 years with breast cancer.
Results
Compared to patients 70–79 years, patients aged 80 and over had larger tumor size with fewer T1 (42.9% vs 57.7%, p < 0.01) and more T2 lesions (43.5% vs 33.0%, p < 0.01). Lymph nodes and distant metastases were more frequent, with more N + (49.5% vs 44.0%, p < 0.01) and more M1 (8.0% vs 5.9%, p < 0.01). Infiltrating mucinous carcinomas were more frequent (4.3% vs 3.7%, p < 0.01). Tumors had lower grades, with more grade 1 (23.2% vs 19.8%, p = 0.01) and fewer grade 3 (21.5% vs 25.5%, p < 0.01), and were more hormone-sensitive: PR was more often expressed (72.6% vs 67.3%, p < 0.01). Lympho-vascular invasion was less frequent in the 80 years and over (22.9% vs 29.7%, p = 0.01). Breast cancer-specific mortality was higher both at 5 years (25.8% vs 17.2%, p < 0.01) and 10 years (32.7% vs 26.6%, p < 0.01).
Conclusion
Clinico-pathological characteristics, increased incidence, and mortality associated with aging can be explained on one hand by biological changes of the breast such as increased estrogen sensitivity, epithelial cell alterations, immune senescence, and tumor microenvironment modifications. However, sociologic factors such as increased life expectancy, under-treatment, late diagnosis, and insufficient individual screening, are also involved.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Breast cancer is the most common malignancy in women in terms of incidence and mortality, thus constituting a major public health problem. In 2012, breast cancer represented 28.1% of new cancers and 14.6% of cancer deaths in industrialized countries [1]. A number of modifiable and non-modifiable risk factors are involved in the occurrence of breast cancer including obesity [2], physical inactivity [3], hormonal treatments [4], and genetic or familial predisposition [5]. However, age is undoubtedly the predominant breast cancer risk factor. The number of women affected by breast cancer in France in 2008 was estimated at 1/430 and 1/19 for the ages below 45 years and over 75 years, respectively [6]. These data are comparable in the United States [7]. Although there is no general agreement on the age at which a person becomes old [8], in this paper we set the age threshold at 70 years, as proposed by the Breast International Group [9].
In the last fifteen years, breast cancer incidence and mortality have generally decreased. This improvement may be attributed to the progress of medical care, notably earlier screening and diagnosis, and more effective treatments, including targeted therapies. However there is evidence that this decrease in incidence and mortality has been less significant [10] or has even increased in elderly women. This was observed in the United States [7], Germany [11], Denmark [12], and France [13, 14] and it was estimated that in 2012, in developed countries, one out of two woman who died from breast cancer was over 70 [1].
Population aging is a major concern. It is estimated that between 2000 and 2050 the population of women aged over 80 will have more than tripled in developed countries [15]. Elderly women are rarely included in national breast cancer screening programs, the upper age limit varying from 65 years in Hungary [16] to 74 years in France, Italy, Sweden, Japan, Israel, and the Netherlands [16]. In the United States, recommendations are that breast cancer screening should be continued as long as life expectancy is at least 10 years, without age limit [17].
The common dogma is that cancer in the elderly spreads slowly and is less aggressive and that the leading cause of mortality in this population is related to co-morbidities. Epidemiology studies indicate that it is not true until the age of 85 [18].
Many authors have studied breast cancer treatment, but only a few studies have correlated this with the clinical and pathological characteristics in elderly women. We analyzed the literature between 2006 and 2016 and propose an updated overview on clinical, histological, and biological characteristics of breast cancer in elderly women along with changes due to aging. Incidence and mortality data have also been included.
Patients and methods
Bibliographic selection
An initial PubMed search, between 01/01/2006 and 01/04/2016, based on the following terms: “breast cancer” and “older, elder, eldest, elderly” gave 30,271 entries. A targeted search based on the following terms: “clinic/clinical,” “biology/biological,” “hormone/hormonal,” “histology/histological,” “pathology/pathological,” “clinicopathology/clinicopathological,” “histopathology/histopathological,” “survival” reduced the number of results to 3524.
We then proceeded to a further screening by title, abstract, and/or full text. This step allowed us to select 50 original articles on clinico-pathological aspects in elderly women (discovery mode, TNM, histology, predictive, and prognostic factors) and mortality. Further research through the bibliographies of selected articles and certain review articles allowed us to single out 13 additional articles that were considered relevant for the study. Reviews, articles without abstracts, case reports, clinical trials, and articles including populations under the age of 70 years were excluded. Only articles in English, Spanish, and Chinese were included.
In total, our search yielded 63 original articles published between 2006 and 2016. The bibliographic approach is summarized in Fig. 1.

Bibliographic selection
Data analysis
Of the 63 articles, 49 gave general characteristics of women aged over 70 (103,408 women): we analyzed clinical presentation (clinical or radiological), TNM stage, tumor grade (classified according to the Elston-Ellis modification of Scarff-Bloom-Richardson grading system), histological sub-types, tumor receptor status (Estrogen receptor (ER), Progesterone receptor (PR), Human Epidermal growth factor Receptor 2 (HER2)), and lympho-vascular invasion.
Thirteen articles had more precise age sub-categories, allowing us to compare two age-related groups (94,070 women): those between 70–79 and those over 80 years.
Since the aim of our study was to analyze clinico-pathological characteristics of breast cancer in women over 70 years, we included all populations, from primary operated breast cancer to primary metastatic endocrine therapy-only patients. We deliberately excluded treatment analysis because it was irrelevant to the purpose of our study.
Mortality analysis was made on 27 articles, on a population of 178,202 women.
Statistical analysis was performed with the GraphPad® 6 Prism software using a two-tailed χ2 test with a 95% confidence interval. The results are expressed as means with a range.
Incidence and mortality in general population and in elderly women
Epidemiological data were retrieved from Globocan 2012 online analysis (International Agency for Research on Cancer, World Health Organization) [1]. Incidence and mortality were calculated for women only, in 2012. Industrialized countries are defined as “Very High Human Development Index” according to the United Nations Organization.
Limitations of the study
In this report, the population studied is heterogeneous because it includes all the data in the literature on breast cancer diagnosed in women aged 70 years and over. The analysis includes primary operated breast tumors, and primary metastatic breast cancers, the latter lacking information on lymph node involvement. All the clinico-pathological parameters taken into account in the review articles could not be studied in all the patients because some of them were not initially included in this literature database (most articles document the histological grade of the tumor but few reported on lympho-vascular invasion). In addition, it was not possible to make the distinction between elderly and very elderly patients in metastatic-free and loco-regional relapse-free survival because of insufficient data.
Results
Breast cancer incidence and mortality in general population and in elderly women
In 2012, breast cancer represented 747,203 (28.1%) out of 2,660,689 newly discovered cancers in women in industrialized countries [1]. Breast cancer was responsible for 161,131 (14.6%) out of 1157,394 cancer deaths in women in industrialized countries [1].
Table 1 shows breast cancer incidence and mortality with aging. Both incidence and mortality increase with age. Women aged 70 and over represent 225,080 (30.1%) out of 747,203 newly discovered breast cancers, and incidence increases between the different age sub-groups. Women aged 70 and over represent 86,592 (51.2%) out of 169,131 breast cancer deaths and increases with age.
Tumor characteristics of breast cancer in women over 70 years
Forty-nine articles described the clinico-pathological features of breast cancer in women over 70 years without further age group distinction. A summary is given in Tables 2 and 3.
Breast cancer was detected clinically in 71.8% of cases on average (7597 women) [19,20,21,22,23,24,25,26,27,28,29,30,31,32,33]. Tumor size was less than 2 cm (T1) in 47.2% of cases, while T2 sized tumors (2–5 cm) were found in 42.9% of cases (13,981 women) [18,19,20,21,22,23,24, 28, 31, 32, 34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49]. Lymph node involvement (N) was evaluated in 21,164 women [18, 19, 22, 24, 28, 31, 34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56]. When axillary surgery was performed, metastatic extension to lymph nodes was detected by histology in 36.1% of cases. Extension was not detected in 56.1% of cases. The remaining 7.8% were considered unknown as it was not clear whether surgical sampling was performed.
At the time of diagnosis, distant metastasis was present in 6.3% of cases (87,601 women) [20, 22, 24, 27, 32, 35, 37, 41, 43,44,45,46, 50,51,52, 57,58,59,60,61,62,63].
Infiltrating ductal carcinoma represented 66.1% of cases (103,408 women) [19,20,21, 23, 25, 26, 29, 31,32,33,34,35,36,37, 39,40,41,42,43,44,45, 51, 56, 58, 59, 62, 64,65,66,67]. Histological tumor grade 1 represented 22.4% of cases (20,014 women) [18, 19, 21,22,23, 26, 28, 30, 32, 35, 37,38,39,40, 42, 43, 45, 47,48,49,50,51,52, 54,55,56, 58,59,60,61,62, 66]. ER and PR were expressed in 81.1% (19,627 women) and 59.3% (16,766 women) of tumors, respectively [18,19,20,21,22,23, 25, 26, 28, 30, 32, 33, 35,36,37,38,39,40, 42,43,44,45, 47,48,49,50,51,52,53,54,55,56, 58, 59, 62, 66]. HER2 over-expression or amplification was found in 13.4% of cases (8362 women) [19,20,21, 25, 28, 30,31,32, 35, 36, 38, 39, 42,43,44,45, 47,48,49,50,51,52,53, 56, 59, 61]. Lympho-vascular invasion was present in 24.4% of cases (9924 women) [19, 20, 28, 34, 35, 37, 41, 42, 44, 45, 55, 60, 62].
Differences between two age sub-groups over 70 years
Thirteen articles dealt with changes of clinico-pathological characteristics upon aging over 70 years (Tables 2 and 3) and made a distinction between two groups of age: from 70 to 79 and from 80 and over. In 4857 women, clinical detection was more frequent among the 80 and over group than for the 70-79 years sub-group (77.8% against 61.3%, p < 0.01), and detection by imaging was rarer (22.2% against 38.7%, p < 0.01).
In 4252 women, tumor size T1 (57.7%) was predominant for the 70 to 79-year age group, while tumor size T2 (43.5%) was predominant in the 80 and over sub-group. Another significant difference between the two populations is that, in the 80 and over sub-group, T1 are less frequent (42.9% vs 57.7%, p < 0.01) and T2 are more frequent (43.5% vs 33.0%, p < 0.01). However, no statistically significant differences were found for T3 (p = 0.70) and T4 (p = 0.17) lesions.
Lymph node involvement (N) was studied in 7015 women from both sub-groups. Lymph nodes were less frequently assessed in the 80 and over sub-group; the unknown status (Nx) was significantly more frequent (12.5% vs 4.0%, p < 0.01). When axillary surgery was performed (i.e., Nx excluded), lymph node metastasis was observed more frequently in the 80 and over sub-group, with less N0 (56.0% vs 50.5%, p < 0.01) and more N + (44.0% vs 49.5%, p < 0.01).
The presence of distant metastasis at diagnosis, evaluated in 38,584 women, was more frequent in the 80 and over sub-group (8.0% vs 5.9%, p < 0.01).
The evaluation of histological type was described for 94,070 women. In the 80 and over sub-group: on one hand infiltrating ductal and lobular carcinomas were less frequently diagnosed (respectively 61.5% vs 66.8%, p < 0.01 and 6.9% vs 10.0%, p < 0.01); while mucinous (4.3% vs 3.7%, p < 0.01) and other histological type carcinomas (27.3% vs 19.6%, p < 0.01) were more frequent.
The histological tumor grade (classified according to the Elston-Ellis modification of Scarff-Bloom-Richardson grading system), assessed in 4330 women was lower in the 80 and over sub-group. Grade 1 was more frequent (23.2% vs 19.8%, p = 0.01) and grade 3 less frequent (21.5% vs 25.5%, p < 0.01), while no statistically significant difference was found in grade 2 (45.0% vs 47.1%, p = 0.20) tumors.
Hormone receptor expression was assessed for ER and PR in 4548 and 2713 women, respectively. For the 80 and over sub-group, more hormone-sensitive tumors were found; PR was more often expressed (72.6% vs 67.3%, p = 0.01), whereas no statistically significant change in ER (77.0% vs 77.9% p = 0.51) was observed. However, in 3298 women, the HER2 over-expression was not statistically different between the two sub-groups (13.1% vs 12.6%, p = 0.69).
In 1284 women the presence of lympho-vascular invasion was less frequent in the 80 and over sub-group (22.9% vs 29.7%, p = 0.03).
Breast cancer mortality in women 70 years and over and differences between the two age sub-groups
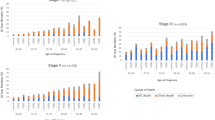
In total, 27 articles dealt with breast cancer mortality in elderly women (Table 4). At 5 years from diagnosis, the overall mortality was 34.5% (53,976 women) [18, 21, 23,24,25, 27, 30, 33, 45, 47, 50, 51, 53, 60, 62, 67,68,69,70,71]. The breast cancer-specific mortality, was 17.0% (140,775 women) [11, 18, 21,22,23, 27, 45, 47, 57, 62, 67, 69, 71]. The loco-regional recurrence at 5 years was 9.7% (5144 women) [18, 21, 23, 27, 30, 50, 53]. At 10 years from diagnosis, the overall mortality was 59.4% (2880 women) and the breast cancer-specific mortality was 28.9% (37,427 women).
Nine publications focused on the variation in mortality upon aging after 70 years (Table 4). The overall mortality was higher in the 80 years and over sub-group (53.5% vs 16.1%, p < 0.01) along with the breast cancer-specific mortality, both at 5 years (25.8% vs 17.2%, p < 0.01) and 10 years (32.7% vs 26.6%, p < 0.01).
Discussion
The analysis of the international literature from the past 10 years on breast cancer shows that aging is remarkably associated with an increased risk of breast cancer. It is important to note that breast cancer in the elderly shows different clinico-pathological features than in the younger women [72]. Furthermore, by making the distinction between two age sub-groups, we observed that cancers in the very elderly (80 years and over) are different than those in elderly women (70–79). Indeed, in women, aging is accompanied by the frequent occurrence of breast tumors with favorable histology (low grade carcinomas, low lympho-vascular invasion, hormone-sensitivity, histological types with good prognosis, lack of expression, or amplification of HER2…), but with larger tumor size, lymph node involvement and more de novo stage IV metastatic disease. In the sub-group 80 years and older, an increase in breast cancer-specific mortality from breast cancer is observed both at 5 and at 10 years. These paradoxical observations can be explained by biological and society-related mechanisms.
Biological mechanisms
Estrogen hypersensitivity
Aging is accompanied by a considerable reduction of circulating estrogens, especially estradiol, resulting in reduced stimulation of the ER. Estrogen deprivation is actually at the basis of the treatment of hormone-dependent breast cancer by castration (be it medical, surgical or by irradiation), which significantly reduces the risk of breast cancer death, recurrence, and even contralateral cancer [73]. Similarly, the occurrence of early menopause is associated epidemiologically with a significant reduction in the risk of breast cancer [74]. In elderly women the level of circulating estrogens are extremely low, yet the risk of hormone-dependent cancer is significantly higher. This apparent contradiction can be explained by deep cellular and biological changes that occur in the mammary gland after menopause.
Indeed, aging is accompanied by increased expression of genes that regulate the activity of different enzymes such as aromatase, sulfatase, or 17β-hydroxy-steroid dehydrogenase-1 involved in the intramammary synthesis of estradiol, enabling breast epithelial cells to proliferate despite low levels of circulating estrogens [75]. This adaptation is associated with greater breast sensitivity to estrogens. This was revealed by experimental data on the human cancer cell lines MCF-7 a model of luminal cancer cells [76].
Epidemiological studies confirm an age-related susceptibility to breast cancer. By exploiting four large clinical trials, Beral et al. [4] investigated the breast cancer incidence during a 5 years period, on more than 20,000 women having or not followed hormone substitution therapy. The number of cancers attributable to hormone substitution therapy was higher among women aged from 60 to 69 compared to those aged from 50 to 59. Similar findings were reported, in presence of endogenous obesity [2] and hyperthyroidism [77]. Altogether, endogenous and exogenous, hormonal stimulation associated with an increased risk of breast cancer in the elderly might be due to an increased susceptibility of epithelial breast cells to estrogens.
Mammary epithelial cell changes
Aging also changes the breast tissue with the presence of ducto-lobular tissue atrophy at the expense of connective and adipose stroma. Russo et al. [78] found that, after menopause, differentiated lobules regress to undifferentiated lobules similar to those observed before puberty. Thus puberty and elderly age are characterized by glandular immaturity. However, in contrast with puberty in older women, the atrophic ducto-lobular and immature tissue contains epithelial cells which have undergone modifications due to repeated exposure to carcinogens [79], or alterations of the double-stranded DNA repair system via a loss of the ATM protein (ataxia telangiectasia mutated) pathway repression [80], possibly increasing its transformation potential.
Tumor microenvironment (TME) (fibroblasts and adipocytes)
As mentioned above, in elderly women, ducto-lobular tissue atrophies at the expense of connective and adipose stroma. This tissue remodeling in the breasts of older women is characterized by global changes i.e., breasts becoming softer, ptosic, and of lower radiographic density. Consequently, older women’s breasts are transparent to imaging [81], which facilitates cancer detection.
Biologically, tumor development capabilities (migration and cell proliferation, resistance to cell death, induction of angiogenesis, etc.) are modulated by the interaction of cancer cells with their microenvironment [82]. The elderly mammary gland becomes particularly rich in adipocytes and fibroblasts [83]. Aging entails the accumulation in the body of senescent cells, in particular fibroblasts. Cellular senescence involves different mechanisms such as shortening of telomeres, epigenetic de-repression of the INK4a locus/ARF, and DNA damage, leading to irreversible arrest of growth [84]. Cellular senescence was previously deemed as tumor-protective. However, more recent studies suggest that senescent cells contribute to the formation of an inflammatory and hence tumor-promoting environment [85]. Several experimental studies have shown that senescent fibroblasts promote in vivo and in vitro growth of cancer cells [86, 87]. For example, senescent fibroblasts induce in vitro migration of T47D breast cancer epithelial cells, originally non-mobile, via the RhoA/ROCK/myosin pathway [85] through inflammatory factors and pro-oncogenes, including among others interleukins 6 and 8 and the vascular endothelial growth factor (VEGF) [88]. The body of experimental data suggests that the accumulation of senescent fibroblasts and the resulting alterations in tissues can partly explain the marked carcinogenicity in aged breast tissue as well as the diffusion to lymph nodes and the more frequent presence of metastases at diagnosis.
The role of the TME in cancer represents a broad field of investigation, besides cancer associated fibroblasts, which is a well-known contributor of cancer progression [89], adipocytes and cancer associated adipocytes are recognized as emerging and major components of the TME [90,91,92,93]. Several mechanisms have incriminated the adipose tissue in cancer development, either indirectly due to the consequences of their dysfunction like obesity-related inflammation [92] or directly through the physical interaction between cancer cells and adipocytes during tumor progression [93,94,95,96]. Clinical studies have showed that local adipose tissue invasion by cancer cells was associated to a poor prognosis of ductal breast carcinoma [97, 98]. Several reports have documented profound modification of the adipocyte tissue morphology and function in cancer. Notably in breast cancer, adipocytes next to cancer cells called cancer associated adipocytes (CAA) have reduced size and progressively dedifferentiate to disappear at the expense of stromal cells [94,95,96]. Moreover, experimental studies provide evidence that CAA support cancer progression, by favoring cancer cell growth, migration, and metastases [92, 93, 96, 99]. To date, adipocytes by shaping the microenvironment are important contributors of the TME, therefore it is tempting to speculate that the hypertrophy of the breast adipose tissue in elderly women plays a central role in the rapid progression of the disease.
Immune senescence
With advancing age a decreased immune response, called immuno-senescence, is observed which lowers the defense against infection and the response to vaccination, and increases the incidence of cancer [79, 82]. This process involves several factors. The first is the adipose involution of the bone marrow with alterations of the hematopoietic stem cells of B and T lymphocytes lineages. The second factor is abnormal migration, maturation and function of peripheral lymphocytes. A third factor is thymic involution, i.e., the reduction in mass and functionality of the thymus [100]. A global decrease of immune defenses can result in more rapid proliferation of cancer cells [101], and might explain that cancers found in elder women are larger in size and progress faster.
Our findings are consistent with recent data from the Surveillance, Epidemiology, and End Results (SEER) Program. In early stage breast cancer with high-risk 21-gene recurrence score assay, breast cancer-specific mortality is higher after 70 and increases with aging [102].
The biology of breast aging can only partially explain the high incidence and mortality rates of breast cancer in elderly women. This phenomenon is typical of developed countries, therefore other aspects i.e., related to societal characteristics need to be considered to get a bigger picture.
Society-related mechanisms
Life expectancy can be considered as a major factor explaining the increase incidence of breast cancer among elder women. Indeed, in developed countries, life expectancy has increased over the past two centuries, yielding an older population. However, since 2000, this phenomenon has grown exponentially [103]. This is one of the reasons for the increased incidence of breast cancer in elderly women.
National breast cancer screening programs do not involve women over 75 years of age. Moreover, since 2010 in France, participation is increasing among women aged 70–75, while it decreases among those 50–69 [104]. However, 70–75 participation rate is still significantly lower than among middle-aged women (50–70) [104]. The exclusion of the elderly from the screening can be mistakenly interpreted as a zero-risk situation by women. This may be the case also for health professionals. The net result is that breast clinical monitoring in elderly women is clearly insufficient. For example, only half of physicians perform a breast clinical examination routinely before prescribing mammography [105]. This omission may lead to late diagnosis with more advanced local lesions and more likely extension to lymph nodes or metastasis.
Common sense can also be misleading; it is not uncommon to hear that “the older the person, the slower cancer’s progress” or “cancer in the elderly does not kill”. Such die-hard lingering dogmas contribute to aggravate the problem because they lead to delays in the provision of necessary medical care. These assertions are ill conceived because it has been proven that the breast cancer-specific mortality from breast cancer increases with age [18]. In addition, up to 85 years, the leading cause of mortality in elderly women with breast cancer is the cancer itself and not co-morbidity [18]. It can be affirmed that in this respect the medical community, the patients and society in general are badly informed or not informed at all.
Moreover, co-morbidity in older women can render various therapies (chemotherapy, surgery, radiotherapy) contraindicated and thus lead to under-treatment. Proper onco-geriatric patient assessment should be made to analyze the appropriateness of a care project when therapeutic choices are difficult. In some situations, hormonotherapy is prescribed as the only therapy without considering that it is effective only on hormone-sensitive tumors. And sometimes caregivers disregard factors such as social isolation, insecurity [106], cognitive disorders, and disabilities, which are more common in the elderly. Such factors may render the therapy ineffective simply due to non-adherence.
It has been demonstrated that elderly women were less likely to receive medical and surgical treatment in concordance with guidelines [107]. Thus, different treatment patterns in the elderly may also explain the increased breast cancer-specific mortality [108].
However, unlike younger women, differences we found in clinico-pathological characteristics do not always have a clinical impact. Therapeutic impact of our findings is attenuated by co-morbidities. Nonetheless, those differences are more pertinent concerning cancer’s prognosis and screening.
Conclusion
Epidemiological and societal information indicate that breast cancer in elderly women could be more properly diagnosed in “developed” countries. Its specific characteristics should be taken into account when dealing with an elderly woman. We suggest that information campaigns should be held and that training on breast clinical examination for physicians and caregivers in general should be strengthened. Efforts should also be made to educate health professionals on the importance of conducting an appropriate assessment of the health status of older patients with cancer, by using validated instruments such as geriatric assessment tools. Also, women over the upper age limit for screening programs should not be discouraged to undergo individual screening, both clinical and mammographic, if they wish so. In all cases, including in elderly women, early diagnosis implies a better prognosis. Finally, onco-geriatric assessment limits the risk of under-treatment or over-treatment, therefore if accessible, should be systematically considered.
References
Cancer today IARC (2012) Cancer Fact Sheets: Breast Cancer. World Health Organization. http://gco.iarc.fr/today/fact-sheets-cancers?cancer=15&type=0&sex=2. Accessed October 26, 2016
Protani M, Coory M, Martin JH (2010) Effect of obesity on survival of women with breast cancer: systematic review and meta-analysis. Breast Cancer Res Treat 123(3):627–635. doi:10.1007/s10549-010-0990-0
Thune I, Brenn T, Lund E, Gaard M (1997) Physical activity and the risk of breast cancer. N Engl J Med 336(18):1269–1275. doi:10.1056/NEJM199705013361801
Beral V, Banks E, Reeves G (2002) Evidence from randomised trials on the long-term effects of hormone replacement therapy. Lancet 360(9337):942–944. doi:10.1016/S0140-6736(02)11032-4
Wacholder S, Hartge P, Prentice R, Garcia-Closas M, Feigelson HS, Diver WR, Thun MJ, Cox DG, Hankinson SE, Kraft P, Rosner B, Berg CD, Brinton LA, Lissowska J, Sherman ME, Chlebowski R, Kooperberg C, Jackson RD, Buckman DW, Hui P, Pfeiffer R, Jacobs KB, Thomas GD, Hoover RN, Gail MH, Chanock SJ, Hunter DJ (2010) Performance of common genetic variants in breast-cancer risk models. N Engl J Med 362(11):986–993. doi:10.1056/NEJMoa0907727
Colonna M, Mitton N, Grosclaude P (2014) Estimation de la prévalence (partielle et totale) du cancer en France métropolitaine chez les 15 ans et plus en 2008 - Étude à partir des registres des cancers du réseau Francim.. Institut de Veille Saniaire. http://www.cancer-environnement.fr/Portals/0/Documents PDF/Estimation-prevalence-cancer-France-metropolitaine-en-2008-2014.pdf. Accessed October 26, 2016
Siegel RL, Miller KD (2016) Jemal A (2016) Cancer statistics. CA Cancer J Clin 66(1):7–30. doi:10.3322/caac.21332
WHO (2016) Definition of an older or elderly person. http://www.who.int/healthinfo/survey/ageingdefnolder/en/. Accessed October 26, 2016
Biganzoli L, Goldhirsch A, Straehle C, Castiglione-Gertsch M, Therasse P, Aapro M, Minisini A, Piccart MJ (2004) Adjuvant chemotherapy in elderly patients with breast cancer: a survey of the Breast International Group (BIG). Ann Oncol 15(2):207–210
Smith BD, Jiang J, McLaughlin SS, Hurria A, Smith GL, Giordano SH, Buchholz TA (2011) Improvement in breast cancer outcomes over time: are older women missing out? J Clin Oncol 29(35):4647–4653. doi:10.1200/JCO.2011.35.8408
Holleczek B, Brenner H (2012) Trends of population-based breast cancer survival in Germany and the US: decreasing discrepancies, but persistent survival gap of elderly patients in Germany. BMC Cancer 12:317. doi:10.1186/1471-2407-12-317
Jensen JD, Cold S, Nielsen MH, Jylling AM, Soe KL, Larsen LB, Ewertz M, Academy of Geriatric Cancer R (2016) Trends in breast cancer in the elderly in Denmark, 1980–2012. Acta Oncol 55(Suppl 1):59–64. doi:10.3109/0284186X.2015.1115118
Molinie F, Vanier A, Woronoff AS, Guizard AV, Delafosse P, Velten M, Daubisse-Marliac L, Arveux P, Tretarre B (2014) Trends in breast cancer incidence and mortality in France 1990–2008. Breast Cancer Res Treat 147(1):167–175. doi:10.1007/s10549-014-3073-9
Cowppli-Bony A, Uhry Z, Remontet L, Guizard A-V, Voirin N, Monnereau A, Bouvier A-M, Colonna M, Bossard N, Woronoff A-S, Grosclaude P (02/2016) Survie des personnes atteintes de cancer en France métropolitaine 1989–2013. Institut de Veille Sanitaire. http://www.e-cancer.fr/content/download/183576/2424633/file/Les_cancers_en_France_en_2016_L_essentiel_des_faits_et_chiffres_mel_20170203.pdf. Accessed August 04, 2017
United Nations Department of Economic and Social Affairs—Population Division (2015) World Population Ageing 2015. United Nations. http://www.un.org/en/development/desa/population/publications/pdf/ageing/WPA2015_Report.pdf. Accessed 26/10/2016
Altobelli E, Rapacchietta L, Angeletti PM, Barbante L, Profeta FV, Fagnano R (2017) Breast cancer screening programmes across the WHO European Region: differences among countries based on national income level. Int J Environ Res Public Health. doi:10.3390/ijerph14040452
Smith RA, Andrews K, Brooks D, DeSantis CE, Fedewa SA, Lortet-Tieulent J, Manassaram-Baptiste D, Brawley OW, Wender RC (2016) Cancer screening in the United States, 2016: a review of current American Cancer Society guidelines and current issues in cancer screening. CA Cancer J Clin 66(2):96–114. doi:10.3322/caac.21336
van de Water W, Markopoulos C, van de Velde CJ, Seynaeve C, Hasenburg A, Rea D, Putter H, Nortier JW, de Craen AJ, Hille ET, Bastiaannet E, Hadji P, Westendorp RG, Liefers GJ, Jones SE (2012) Association between age at diagnosis and disease-specific mortality among postmenopausal women with hormone receptor-positive breast cancer. JAMA 307(6):590–597. doi:10.1001/jama.2012.84
Barthelemy P, Heitz D, Mathelin C, Polesi H, Asmane I, Litique V, Rob L, Bergerat JP, Kurtz JE (2011) Adjuvant chemotherapy in elderly patients with early breast cancer. Impact of age and comprehensive geriatric assessment on tumor board proposals. Crit Rev Oncol Hematol 79(2):196–204. doi:10.1016/j.critrevonc.2010.06.005
Cortadellas T, Cordoba O, Gascon A, Haladjian C, Bernabeu A, Alcalde A, Esgueva A, Rodriguez-Revuelto R, Espinosa-Bravo M, Diaz-Botero S, Xercavins J, Rubio IT, Gil-Moreno A (2015) Surgery improves survival in elderly with breast cancer. A study of 465 patients in a single institution. Eur J Surg Oncol 41(5):635–640. doi:10.1016/j.ejso.2015.01.027
Cyr A, Gillanders WE, Aft RL, Eberlein TJ, Margenthaler JA (2011) Breast cancer in elderly women (≥ 80 years): variation in standard of care? J Surg Oncol 103(3):201–206. doi:10.1002/jso.21799
Dialla PO, Dabakuyo TS, Marilier S, Gentil J, Roignot P, Darut-Jouve A, Poillot ML, Quipourt V, Arveux P (2012) Population-based study of breast cancer in older women: prognostic factors of relative survival and predictors of treatment. BMC Cancer 12:472. doi:10.1186/1471-2407-12-472
Evron E, Goldberg H, Kuzmin A, Gutman R, Rizel S, Sella A, Gutman H (2006) Breast cancer in octogenarians. Cancer 106(8):1664–1668. doi:10.1002/cncr.21788
Eaker S, Dickman PW, Bergkvist L, Holmberg L, Uppsala Orebro Breast, Cancer G (2006) Differences in management of older women influence breast cancer survival: results from a population-based database in Sweden. PLoS Med 3(3):e25. doi:10.1371/journal.pmed.0030025
Li B, Hua B, Lu X, Chen Y, Xiao WZ (2013) Treatment options for elderly breast cancer patients over 70 years old. Zhonghua Yi Xue Za Zhi 93(44):3523–3525
Litvak DA, Arora R (2006) Treatment of elderly breast cancer patients in a community hospital setting. Arch Surg 141 (10):985–990; discussion 990. doi:10.1001/archsurg.141.10.985
Malmgren JA, Parikh J, Atwood MK, Kaplan HG (2014) Improved prognosis of women aged 75 and older with mammography-detected breast cancer. Radiology 273(3):686–694. doi:10.1148/radiol.14140209
Molino A, Giovannini M, Auriemma A, Fiorio E, Mercanti A, Mandara M, Caldara A, Micciolo R, Pavarana M, Cetto GL (2006) Pathological, biological and clinical characteristics, and surgical management, of elderly women with breast cancer. Crit Rev Oncol Hematol 59(3):226–233. doi:10.1016/j.critrevonc.2006.01.007
Niu SH, Jiang YX, Zhu QL, Liu H, Dai Q (2014) Clinical and ultrasonic features of breast cancer in women older than 80 years. Zhongguo Yi Xue Ke Xue Yuan Xue Bao 36(1):57–60. doi:10.3881/j.issn.1000-503X.2014.01.011
Rudra S, Yu DS, Yu ES, Switchenko JM, Mister D, Torres MA (2015) Locoregional and distant recurrence patterns in young versus elderly women treated for breast cancer. Int J Breast Cancer 2015:213123. doi:10.1155/2015/213123
Sanchez RC, Bakal IF, Camus AM, de Besa CP (2013) Characteristics and results of breast cancer in elderly females treated with curative intent. Rev Med Chil 141(12):1534–1540. doi:10.4067/S0034-98872013001200006
Vetter M, Huang DJ, Bosshard G, Guth U (2013) Breast cancer in women 80 years of age and older: a comprehensive analysis of an underreported entity. Acta Oncol 52(1):57–65. doi:10.3109/0284186X.2012.731523
Zhao WH, Xu BH, Li Q, Zhang P, Sun Y (2006) Clinical features and prognosis in breast cancer patients over 70 years of age. Zhonghua Zhong Liu Za Zhi 28(5):385–388
Afsharfard A, Mozaffar M, Orang E, Tahmasbpour E (2013) Trends in epidemiology, clinical and histopathological characteristics of breast cancer in Iran: results of a 17 year study. Asian Pac J Cancer Prev 14(11):6905–6911
Angarita FA, Chesney T, Elser C, Mulligan AM, McCready DR, Escallon J (2015) Treatment patterns of elderly breast cancer patients at two Canadian cancer centres. Eur J Surg Oncol 41(5):625–634. doi:10.1016/j.ejso.2015.01.028
Azim HA Jr, Nguyen B, Brohee S, Zoppoli G, Sotiriou C (2015) Genomic aberrations in young and elderly breast cancer patients. BMC Med 13:266. doi:10.1186/s12916-015-0504-3
Chatzidaki P, Mellos C, Briese V, Mylonas I (2011) Does primary breast cancer in older women (≥ 80 years) have unfavorable histological characteristics? Arch Gynecol Obstet 284(3):705–712. doi:10.1007/s00404-010-1697-5
Cutuli B, Dalenc F, Cottu PH, Gligorov J, Guastalla JP, Petit T, Amrate A (2015) Impact of screening on clinicopathological features and treatment for invasive breast cancer: results of two national surveys. Cancer Radiother 19(5):295–302. doi:10.1016/j.canrad.2015.02.015
Durbecq V, Ameye L, Veys I, Paesmans M, Desmedt C, Sirtaine N, Sotiriou C, Bernard-Marty C, Nogaret JM, Piccart M, Larsimont D (2008) A significant proportion of elderly patients develop hormone-dependant “luminal-B” tumours associated with aggressive characteristics. Crit Rev Oncol Hematol 67(1):80–92. doi:10.1016/j.critrevonc.2007.12.008
Hancke K, Denkinger MD, Konig J, Kurzeder C, Wockel A, Herr D, Blettner M, Kreienberg R (2010) Standard treatment of female patients with breast cancer decreases substantially for women aged 70 years and older: a German clinical cohort study. Ann Oncol 21(4):748–753. doi:10.1093/annonc/mdp364
Kaur P, Santillan AA, McGuire K, Turaga KK, Shamehdi C, Meade T, Ramos D, Mathias M, Parbhoo J, Davis M, Khakpour N, King J, Balducci L, Cox CE (2012) The surgical treatment of breast cancer in the elderly: a single institution comparative review of 5235 patients with 1028 patients ≥ 70 years. Breast J 18(5):428–435. doi:10.1111/j.1524-4741.2012.01272.x
Ma CD, Zhou Q, Nie XQ, Liu GY, Di GH, Wu J, Lu JS, Yang WT, Chen JY, Shao ZM, Shen KW, Shen ZZ (2009) Breast cancer in Chinese elderly women: pathological and clinical characteristics and factors influencing treatment patterns. Crit Rev Oncol Hematol 71(3):258–265. doi:10.1016/j.critrevonc.2008.11.005
Montroni I, Rocchi M, Santini D, Ceccarelli C, Ghignone F, Zattoni D, Nuvola G, Zanotti S, Ugolini G, Taffurelli M (2014) Has breast cancer in the elderly remained the same over recent decades? A comparison of two groups of patients 70 years or older treated for breast cancer twenty years apart. J Geriatr Oncol 5(3):260–265. doi:10.1016/j.jgo.2014.02.006
Pappo I, Karni T, Sandbank J, Dinur I, Sella A, Stahl-Kent V, Wasserman I, Halevy A (2007) Breast cancer in the elderly: histological, hormonal and surgical characteristics. Breast 16(1):60–67. doi:10.1016/j.breast.2006.05.007
Phua CE, Bustam AZ, Yip CH, Taib NA (2010) Prognostic factors for elderly breast cancer patients in University Malaya Medical Centre, Malaysia. Asian Pac J Cancer Prev 11(5):1205–1211
Seah MD, Chan PM (2009) Rethinking undertreatment in elderly breast cancer patients. Asian J Surg 32(2):71–75. doi:10.1016/S1015-9584(09)60013-0
Syed BM, Johnston SJ, Wong DW, Green AR, Winterbottom L, Kennedy H, Simpson N, Morgan DA, Ellis IO, Cheung KL (2012) Long-term (37 years) clinical outcome of older women with early operable primary breast cancer managed in a dedicated clinic. Ann Oncol 23(6):1465–1471. doi:10.1093/annonc/mdr446
Syed BM, Green AR, Paish EC, Soria D, Garibaldi J, Morgan L, Morgan DA, Ellis IO, Cheung KL (2013) Biology of primary breast cancer in older women treated by surgery: with correlation with long-term clinical outcome and comparison with their younger counterparts. Br J Cancer 108(5):1042–1051. doi:10.1038/bjc.2012.601
Tea MK, Tang L, Di GH, Muin D, Steurer S, Delancey JW, Shao ZM, Singer CF (2012) A cross-sectional study of elderly Asian and European women with primary operable breast cancer aged 70 and older. Are there differences? Maturitas 73(3):251–254. doi:10.1016/j.maturitas.2012.08.001
Acevedo F, Camus M, Sanchez C (2015) Breast cancer at extreme ages–a comparative analysis in Chile. Asian Pac J Cancer Prev 16(4):1455–1461
Inal A, Akman T, Yaman S, Ozturk SC, Geredeli C, Bilici M, Inanc M, Harputoglu H, Demirci U, Balakan O, Cinkir HY, Alici S, Colak D, Sonmez OU, Goksel G, Dogu GG, Engin H, Unal OU, Tamozlu T, Buyukberber S, Boruban CM, Isikdogan A (2014) Pathologic and clinical characteristics of elderly patients with breast cancer: a retrospective analysis of a multicenter study (Anatolian Society of Medical Oncology). Int Surg 99(1):2–7. doi:10.9738/INTSURG-D-13-00010
Joerger M, Thurlimann B, Savidan A, Frick H, Rageth C, Lutolf U, Vlastos G, Bouchardy C, Konzelmann I, Bordoni A, Probst-Hensch N, Jundt G, Ess S (2013) Treatment of breast cancer in the elderly: a prospective, population-based Swiss study. J Geriatr Oncol 4(1):39–47. doi:10.1016/j.jgo.2012.08.002
Li JJ, Yu KD, Di GH, Shao ZM (2010) Clinicopathological features and treatment sensitivity of elderly Chinese breast cancer patients. Oncol Lett 1(6):1037–1043. doi:10.3892/ol.2010.179
Tse GM, Tan PH, Lau KM, de Andrade VP, Lui PC, Vong JS, Chaiwun B, Lam CC, Yu AM, Moriya T (2009) Breast cancer in the elderly: a histological assessment. Histopathology 55(4):441–451. doi:10.1111/j.1365-2559.2009.03400.x
Wang J, Kollias J, Boult M, Babidge W, Zorbas HN, Roder D, Maddern G (2010) Patterns of surgical treatment for women with breast cancer in relation to age. Breast J 16(1):60–65. doi:10.1111/j.1524-4741.2009.00828.x
Wildiers H, Van Calster B, van de Poll-Franse LV, Hendrickx W, Roislien J, Smeets A, Paridaens R, Deraedt K, Leunen K, Weltens C, Van Huffel S, Christiaens MR, Neven P (2009) Relationship between age and axillary lymph node involvement in women with breast cancer. J Clin Oncol 27(18):2931–2937. doi:10.1200/JCO.2008.16.7619
Bastiaannet E, Liefers GJ, de Craen AJ, Kuppen PJ, van de Water W, Portielje JE, van der Geest LG, Janssen-Heijnen ML, Dekkers OM, van de Velde CJ, Westendorp RG (2010) Breast cancer in elderly compared to younger patients in the Netherlands: stage at diagnosis, treatment and survival in 127,805 unselected patients. Breast Cancer Res Treat 124(3):801–807. doi:10.1007/s10549-010-0898-8
Hamaker ME, Schreurs WH, Uppelschoten JM, Smorenburg CH (2009) Breast cancer in the elderly: retrospective study on diagnosis and treatment according to national guidelines. Breast J 15(1):26–33. doi:10.1111/j.1524-4741.2008.00667.x
Hartman M, Drotman M, Arleo EK (2015) Annual screening mammography for breast cancer in women 75 years old or older: to screen or not to screen. AJR Am J Roentgenol 204(5):1132–1136. doi:10.2214/AJR.14.13394
Kartal M, Tezcan S, Canda T (2013) Diagnosis, treatment characteristics, and survival of women with breast cancer aged 65 and above: a hospital-based retrospective study. BMC Womens Health 13:34. doi:10.1186/1472-6874-13-34
Orucevic A, Curzon M, Curzon C, Heidel RE, McLoughlin JM, Panella T, Bell J (2015) Breast cancer in elderly caucasian women-an institution-based study of correlation between breast cancer prognostic markers, TNM stage, and overall survival. Cancers (Basel) 7(3):1472–1483. doi:10.3390/cancers7030846
Siegelmann-Danieli N, Khandelwal V, Wood GC, Mainali R, Prichard J, Murphy TJ, Evans JF, Yumen O, Bernath AM (2006) Breast cancer in elderly women: outcome as affected by age, tumor features, comorbidities, and treatment approach. Clin Breast Cancer 7(1):59–66. doi:10.3816/CBC.2006.n.014
Vyas A, Madhavan S, Sambamoorthi U (2014) Association between persistence with mammography screening and stage at diagnosis among elderly women diagnosed with breast cancer. Breast Cancer Res Treat 148(3):645–654. doi:10.1007/s10549-014-3204-3
Albrektsen G, Heuch I, Thoresen SO (2010) Histological type and grade of breast cancer tumors by parity, age at birth, and time since birth: a register-based study in Norway. BMC Cancer 10:226. doi:10.1186/1471-2407-10-226
Anderson WF, Pfeiffer RM, Dores GM, Sherman ME (2006) Comparison of age distribution patterns for different histopathologic types of breast carcinoma. Cancer Epidemiol Biomark Prev 15(10):1899–1905. doi:10.1158/1055-9965.EPI-06-0191
Cheung KL, Wong AW, Parker H, Li VW, Winterbottom L, Morgan DA, Ellis IO (2008) Pathological features of primary breast cancer in the elderly based on needle core biopsies–a large series from a single centre. Crit Rev Oncol Hematol 67(3):263–267. doi:10.1016/j.critrevonc.2008.04.002
Mathew J, Lee S, Syed BM, Morgan DA, Ellis IO, Cheung KL (2014) A study of ductal versus non-ductal invasive breast carcinomas in older women: long-term clinical outcome and comparison with their younger counterparts. Breast Cancer Res Treat 147(3):671–674. doi:10.1007/s10549-014-3094-4
Roder D, Wang JX, Zorbas H, Kollias J, Maddern G (2010) Survival from breast cancers managed by surgeons participating in the National Breast Cancer Audit of the Royal Australasian College of Surgeons. ANZ J Surg 80(11):776–780. doi:10.1111/j.1445-2197.2010.05341.x
Clough-Gorr KM, Thwin SS, Stuck AE, Silliman RA (2012) Examining five- and ten-year survival in older women with breast cancer using cancer-specific geriatric assessment. Eur J Cancer 48(6):805–812. doi:10.1016/j.ejca.2011.06.016
Patnaik JL, Byers T, Diguiseppi C, Denberg TD, Dabelea D (2011) The influence of comorbidities on overall survival among older women diagnosed with breast cancer. J Natl Cancer Inst 103(14):1101–1111. doi:10.1093/jnci/djr188
Haque R, Ahmed SA, Inzhakova G, Shi J, Avila C, Polikoff J, Bernstein L, Enger SM, Press MF (2012) Impact of breast cancer subtypes and treatment on survival: an analysis spanning two decades. Cancer Epidemiol Biomark Prev 21(10):1848–1855. doi:10.1158/1055-9965.EPI-12-0474
Diab SG, Elledge RM, Clark GM (2000) Tumor characteristics and clinical outcome of elderly women with breast cancer. J Natl Cancer Inst 92(7):550–556
Goss PE, Ingle JN, Pritchard KI, Robert NJ, Muss H, Gralow J, Gelmon K, Whelan T, Strasser-Weippl K, Rubin S, Sturtz K, Wolff AC, Winer E, Hudis C, Stopeck A, Beck JT, Kaur JS, Whelan K, Tu D, Parulekar WR (2016) Extending aromatase-inhibitor adjuvant therapy to 10 years. N Engl J Med 375(3):209–219. doi:10.1056/NEJMoa1604700
Collaborative Group on Hormonal Factors in Breast C (2012) Menarche, menopause, and breast cancer risk: individual participant meta-analysis, including 118 964 women with breast cancer from 117 epidemiological studies. Lancet Oncol 13(11):1141–1151. doi:10.1016/S1470-2045(12)70425-4
Savolainen-Peltonen H, Vihma V, Leidenius M, Wang F, Turpeinen U, Hamalainen E, Tikkanen MJ, Mikkola TS (2014) Breast adipose tissue estrogen metabolism in postmenopausal women with or without breast cancer. J Clin Endocrinol Metab 99(12):E2661–E2667. doi:10.1210/jc.2014-2550
Darbre PD (2014) Hypersensitivity and growth adaptation of oestrogen-deprived MCF-7 human breast cancer cells. Anticancer Res 34(1):99–105
Sogaard M, Farkas DK, Ehrenstein V, Jorgensen JO, Dekkers OM, Sorensen HT (2016) Hypothyroidism and hyperthyroidism and breast cancer risk: a nationwide cohort study. Eur J Endocrinol 174(4):409–414. doi:10.1530/EJE-15-0989
Russo J, Russo IH (2004) Development of the human breast. Maturitas 49(1):2–15. doi:10.1016/j.maturitas.2004.04.011
Balducci L (2000) Geriatric oncology: challenges for the new century. Eur J Cancer 36(14):1741–1754
Raynaud CM, Hernandez J, Llorca FP, Nuciforo P, Mathieu MC, Commo F, Delaloge S, Sabatier L, Andre F, Soria JC (2010) DNA damage repair and telomere length in normal breast, preneoplastic lesions, and invasive cancer. Am J Clin Oncol 33(4):341–345. doi:10.1097/COC.0b013e3181b0c4c2
Radisky DC, Visscher DW, Frank RD, Vierkant RA, Winham S, Stallings-Mann M, Hoskin TL, Nassar A, Vachon CM, Denison LA, Hartmann LC, Frost MH, Degnim AC (2016) Natural history of age-related lobular involution and impact on breast cancer risk. Breast Cancer Res Treat 155(3):423–430. doi:10.1007/s10549-016-3691-5
Hanahan D, Weinberg RA (2011) Hallmarks of cancer: the next generation. Cell 144(5):646–674. doi:10.1016/j.cell.2011.02.013
Spaeth EL, Labaff AM, Toole BP, Klopp A, Andreeff M, Marini FC (2013) Mesenchymal CD44 expression contributes to the acquisition of an activated fibroblast phenotype via TWIST activation in the tumor microenvironment. Cancer Res 73(17):5347–5359. doi:10.1158/0008-5472.CAN-13-0087
Collado M, Blasco MA, Serrano M (2007) Cellular senescence in cancer and aging. Cell 130(2):223–233. doi:10.1016/j.cell.2007.07.003
Aifuwa I, Giri A, Longe N, Lee SH, An SS, Wirtz D (2015) Senescent stromal cells induce cancer cell migration via inhibition of RhoA/ROCK/myosin-based cell contractility. Oncotarget 6(31):30516–30531. doi:10.18632/oncotarget.5854
Pazolli E, Luo X, Brehm S, Carbery K, Chung JJ, Prior JL, Doherty J, Demehri S, Salavaggione L, Piwnica-Worms D, Stewart SA (2009) Senescent stromal-derived osteopontin promotes preneoplastic cell growth. Cancer Res 69(3):1230–1239. doi:10.1158/0008-5472.CAN-08-2970
Erez N, Truitt M, Olson P, Arron ST, Hanahan D (2010) Cancer-associated fibroblasts are activated in incipient neoplasia to orchestrate tumor-promoting inflammation in an NF-kappaB-dependent manner. Cancer Cell 17(2):135–147. doi:10.1016/j.ccr.2009.12.041
Bussard KM, Mutkus L, Stumpf K, Gomez-Manzano C, Marini FC (2016) Tumor-associated stromal cells as key contributors to the tumor microenvironment. Breast Cancer Res 18(1):84. doi:10.1186/s13058-016-0740-2
Hanahan D, Coussens LM (2012) Accessories to the crime: functions of cells recruited to the tumor microenvironment. Cancer Cell 21(3):309–322. doi:10.1016/j.ccr.2012.02.022
Nieman KM, Kenny HA, Penicka CV, Ladanyi A, Buell-Gutbrod R, Zillhardt MR, Romero IL, Carey MS, Mills GB, Hotamisligil GS, Yamada SD, Peter ME, Gwin K, Lengyel E (2011) Adipocytes promote ovarian cancer metastasis and provide energy for rapid tumor growth. Nat Med 17(11):1498–1503. doi:10.1038/nm.2492
Motrescu ER, Rio MC (2008) Cancer cells, adipocytes and matrix metalloproteinase 11: a vicious tumor progression cycle. Biol Chem 389(8):1037–1041. doi:10.1515/BC.2008.110
Hefetz-Sela S, Scherer PE (2013) Adipocytes: impact on tumor growth and potential sites for therapeutic intervention. Pharmacol Ther 138(2):197–210. doi:10.1016/j.pharmthera.2013.01.008
Tan J, Buache E, Chenard MP, Dali-Youcef N, Rio MC (2011) Adipocyte is a non-trivial, dynamic partner of breast cancer cells. Int J Dev Biol 55(7–9):851–859. doi:10.1387/ijdb.113365jt
Andarawewa KL, Motrescu ER, Chenard MP, Gansmuller A, Stoll I, Tomasetto C, Rio MC (2005) Stromelysin-3 is a potent negative regulator of adipogenesis participating to cancer cell-adipocyte interaction/crosstalk at the tumor invasive front. Cancer Res 65(23):10862–10871. doi:10.1158/0008-5472.CAN-05-1231
Dirat B, Bochet L, Dabek M, Daviaud D, Dauvillier S, Majed B, Wang YY, Meulle A, Salles B, Le Gonidec S, Garrido I, Escourrou G, Valet P, Muller C (2011) Cancer-associated adipocytes exhibit an activated phenotype and contribute to breast cancer invasion. Cancer Res 71(7):2455–2465. doi:10.1158/0008-5472.CAN-10-3323
Rio MC, Dali-Youcef N, Tomasetto C (2015) Local adipocyte cancer cell paracrine loop: can “sick fat” be more detrimental? Horm Mol Biol Clin Investig 21(1):43–56. doi:10.1515/hmbci-2014-0044
Kimijima I, Ohtake T, Sagara H, Watanabe T, Takenoshita S (2000) Scattered fat invasion: an indicator for poor prognosis in premenopausal, and for positive estrogen receptor in postmenopausal breast cancer patients. Oncology 59(Suppl 1):25–30.
Yamaguchi J, Ohtani H, Nakamura K, Shimokawa I, Kanematsu T (2008) Prognostic impact of marginal adipose tissue invasion in ductal carcinoma of the breast. Am J Clin Pathol 130(3):382–388. doi:10.1309/MX6KKA1UNJ1YG8VN
Wang YY, Lehuede C, Laurent V, Dirat B, Dauvillier S, Bochet L, Le Gonidec S, Escourrou G, Valet P, Muller C (2012) Adipose tissue and breast epithelial cells: a dangerous dynamic duo in breast cancer. Cancer Lett 324(2):142–151. doi:10.1016/j.canlet.2012.05.019
Gruver A, Hudson L, Sempowski G (2007) Immunosenescence of ageing. J Pathol 211(2):144–156
Falci C, Gianesin K, Sergi G, Giunco S, De Ronch I, Valpione S, Solda C, Fiduccia P, Lonardi S, Zanchetta M, Keppel S, Brunello A, Zafferri V, Manzato E, De Rossi A, Zagonel V (2013) Immune senescence and cancer in elderly patients: results from an exploratory study. Exp Gerontol 48(12):1436–1442. doi:10.1016/j.exger.2013.09.011
Petkov VI, Miller DP, Howlader N, Gliner N, Howe W, Schussler N, Cronin K, Baehner FL, Cress R, Deapen D, Glaser SL, Hernandez BY, Lynch CF, Mueller L, Schwartz AG, Schwartz SM, Stroup A, Sweeney C, Tucker TC, Ward KC, Wiggins C, Wu XC, Penberthy L, Shak S (2016) Breast-cancer-specific mortality in patients treated based on the 21-gene assay: a SEER population-based study. NPJ Breast Cancer 2:16017. doi:10.1038/npjbcancer.2016.17
Christensen K, Doblhammer G, Rau R, Vaupel JW (2009) Ageing populations: the challenges ahead. Lancet 374(9696):1196–1208. doi:10.1016/S0140-6736(09)61460-4
Rogel A, Hamers F, Quintin C, de Maria F, Bonaldi C, Beltzer N (2016) Breast cancer in France: incidence and screening. Santé Publique France. http://invs.santepubliquefrance.fr/Publications-et-outils/Rapports-et-syntheses/Maladies-chroniques-et-traumatismes/2016/Incidence-et-depistage-du-cancer-du-sein-en-France
Larson KE, Cowher MS, O’Rourke C, Patel M, Pratt D (2016) Do primary care physician perform clinical breast exams prior to ordering a mammogram? Breast J 22(2):189–193. doi:10.1111/tbj.12546
Steptoe A, Shankar A, Demakakos P, Wardle J (2013) Social isolation, loneliness, and all-cause mortality in older men and women. Proc Natl Acad Sci U S A 110(15):5797–5801. doi:10.1073/pnas.1219686110
Giordano SH, Hortobagyi GN, Kau SW, Theriault RL, Bondy ML (2005) Breast cancer treatment guidelines in older women. J Clin Oncol 23(4):783–791. doi:10.1200/JCO.2005.04.175
Bouchardy C, Rapiti E, Fioretta G, Laissue P, Neyroud-Caspar I, Schafer P, Kurtz J, Sappino AP, Vlastos G (2003) Undertreatment strongly decreases prognosis of breast cancer in elderly women. J Clin Oncol 21(19):3580–3587. doi:10.1200/JCO.2003.02.046
Acknowledgments
We thank Dr. Andrea Lodi Ph.D., for the help with the English translation and Dr. Shanti Amé M.D., for the careful corrections of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Lodi, M., Scheer, L., Reix, N. et al. Breast cancer in elderly women and altered clinico-pathological characteristics: a systematic review. Breast Cancer Res Treat 166, 657–668 (2017). https://doi.org/10.1007/s10549-017-4448-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-017-4448-5