
Abstract
Purpose
The Open Lichtenstein technique, the Laparoscopic Trans-Abdominal PrePeritoneal (TAPP), the Totally Extra Peritoneal (TEP), and the robotic TAPP (rTAPP) are commonly performed. The aim of the present network meta-analysis was to globally compare short-term outcomes within these major surgical techniques for primary unilateral inguinal hernia repair.
Methods
PubMed, EMBASE, and Web of Science were consulted. A fully Bayesian network meta-analysis was performed.
Results
Sixteen studies (51.037 patients) were included. Overall, 35.5% underwent Open, 33.5% TAPP, 30.7% TEP, and 0.3% rTAPP. The postoperative seroma risk ratio (RR) was comparable considering TAPP vs. Open (RR 0.91; 95% CrI 0.50–1.62), TEP vs. Open (RR 0.64; 95% CrI 0.32–1.33), TEP vs. TAPP (RR 0.70; 95% CrI 0.39–1.31), and rTAPP vs. Open (RR 0.98; 95% CrI 0.37–2.51). The postoperative chronic pain RR was similar for TAPP vs. Open (RR 0.53; 95% CrI 0.27–1.20), TEP vs. Open (RR 0.86; 95% CrI 0.48–1.16), and TEP vs. TAPP (RR 1.70; 95% CrI 0.63–3.20). The recurrence RR was comparable when comparing TAPP vs. Open (RR 0.96; 95% CrI 0.57–1.51), TEP vs. Open (RR 1.0; 95% CrI 0.65–1.61), TEP vs. TAPP (RR 1.10; 95% CrI 0.63–2.10), and rTAPP vs. Open (RR 0.98; 95% CrI 0.45–2.10). No differences were found in term of postoperative hematoma, surgical site infection, urinary retention, and hospital length of stay.
Conclusions
This study suggests that Open, TAPP, TEP, and rTAPP seem comparable in the short term. The surgical management of inguinal hernia is evolving and the effect of the adoption of innovative minimally invasive techniques should be further investigated in the long term. Ultimately, the choice of the most suitable treatment should be based on individual surgeon expertise and tailored on each patient.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Worldwide, more than 20 million patients undergo groin hernia repair every year [1]. Primary unilateral inguinal hernias account for 75% of abdominal wall hernias, in which there is a lifetime risk of 27% for men and 3% for women [2]. Operative techniques have continuously evolved over the past decades to provide the best management for inguinal hernias [3]. The Open tension-free Lichtenstein technique is the most commonly worldwide performed procedure with optimal outcomes and low recurrence rate [1]. After the introduction of laparoscopy, new techniques such as the transabdominal preperitoneal (TAPP) repair and the totally extraperitoneal repair (TEP) gained progressive acceptance with promising results and comparable outcomes to the Open approach [4]. Afterward, the introduction of robotic platforms opened new horizons and the robotic TAPP (rTAPP) arouses progressive enthusiasm with growing popularity and presumed advantages [5]. The previous meta-analysis analysed these techniques in a pairwise comparison (Open vs. TAPP or TAPP vs. TEP or Open vs. TEP), but a comprehensive review is lacking.
The aim of the present network meta-analysis was to globally compare short-term and recovery outcomes within these four major surgical approaches for primary unilateral inguinal hernia repair.
Materials and methods
A systematic review was performed according to the guidelines from the Preferred Reporting Items for Systematic Reviews and network meta-analyses’ checklist (PRISMA-NMA) [6]. Institutional review board approval was not required.
PubMed, EMBASE, and Web of Science databases were used for systematic search. The last date of search was the February 28st, 2019. We searched for papers using the following search strategy: “primary unilateral inguinal hernia”, “open inguinal hernia repair”, “transabdominal preperitoneal repair”, “totally extraperitoneal endoscopic repair”, and “robotic hernia repair”. All titles were initially evaluated and suitable abstracts extracted. The reference list of included articles was also screened. The study protocol was registered at PROSPERO (International prospective register of systematic reviews) (Registration number: CRD42019130852).
Inclusion and exclusion criteria
Eligible studies for the present meta-analysis included RCT and observational retrospective and prospective clinical studies. To be included in the analysis: (a) studies comparing surgical outcomes in primary unilateral inguinal hernia repair for either Open, TAPP, TEP, and rTAPP; (b) articles written in English; (c) articles with the longest follow-up or the largest sample size when two or more papers were published by the same institution, study group, or used the same data set; (d) published after the year 2000; (e) in case of duplicate studies with accumulating numbers of patients, only the most complete reports were included for quantitative assessment. Studies were excluded if (a) they were not written in English; (b) the methodology was not clearly reported; (c) the surgical technique was not clearly reported; (d) the inguinal hernia repair was performed without mesh or plug; (e) studies that did not contain a comparative group report primary unilateral inguinal hernias.
Data extraction
The following data were retrieved: author, year of publication, country, study design, number of patients, sex, age, body mass index (BMI), surgical approach, and early postoperative outcomes. All data were entered independently by three investigators (FL, AA, and AM) and compared only at the end of the reviewing process. A fourth author (GC) eventually reviewed the database. Discrepancies were clarified.
Quality assessment
Two authors (AA and FL) independently assessed the methodologic quality of the selected trials using the Cochrane risk of bias tool [7]. This tool evaluates the following criteria: (1) method of randomization; (2) allocation concealment; (3) baseline comparability of study groups; and (4) blinding and completeness of follow-up. Trials were graded as follows: A adequate, B unclear, and C inadequate on each criterion. Thus, each RCT was graded as having low, moderate, or high risk of bias. Two authors (FL and AA) independently assessed the quality of observational studies using the ROBINS-I tool [8]. The following domains were considered: confounding bias, selection bias, classification bias, intervention bias, missing data bias, outcomes measurement bias, and reporting bias. Each domain is evaluated with one of the following: “yes”, “probably yes”, “probably no”, and “no”. The categories of judgement for each study are low, moderate, serious, and critical risk of bias. Disagreements were solved by discussion.
Outcomes of interest
Primary outcomes: haematoma, seroma, post-operative chronic pain, and recurrence. Secondary outcomes: surgical site infection (SSI), urinary retention, operative time (minutes), and postoperative hospital length of stay (HLOS).
Statistical analysis
We performed fully Bayesian arm‐based random effect network meta‐analysis, in particular, mixed treatment comparison (MTC). Briefly, the MTC simultaneously synthesizes data from all available trials within a consistent network and combines direct evidence (comparison of treatments within head‐to‐head trials) with indirect evidence (comparison of treatments across trials against a common comparator) [9]. Compared with the frequentist meta‐analysis, the Bayesian approach takes into account all sources of variations, reflects these variations in the pooled result, can provide accurate estimates for small samples, and allows computation of predictive distribution [10]. Furthermore, Bayesian posterior analysis should yield exact coverages, independent of sample size. An ordinary consistency model was adopted with the binomial/log model [11]. We used risk ratio (RR) as a pooled effect size measure. For RR on log scale, we applied two different prior distributions to the model: a “sceptical” and “vague” prior distribution. In particular, we assigned a Normal with zero mean and scale 0.4 as sceptical distribution (10% of the distribution is contained within the clinically unimportant null interval); we assigned Normal with zero mean and scale 100 as vague prior distribution, and we used it as prior distribution into prior sensitivity analysis. For the between‐study variability (τ), we used an informative half‐normal prior with zero mean and scale 0.5 [12] assuming a common heterogeneity parameter across the various treatment comparisons. Sensitivity analysis regarding the choice of prior distribution for τ was also considered [13]. For continuous outcomes, mean difference was adopted using Normal prior distribution with mean 0 and scale 10, and uniform distribution (0.5) as τ prior. To evaluate statistical heterogeneity, we calculated I2 index: value of 25% was defined as low heterogeneity, 50% as moderate heterogeneity, and 75% as high heterogeneity [14]. The inference was performed using mean and relative 95% credible intervals (CrI), based on draws from marginal posterior distribution in Monte Carlo Markov chain (MCMC), simulating 300,000 iterations after a burn‐in period of 30,000 iterations. We consider the estimated parameter statistical significant when its 95% CrI encompasses null‐hypothesis value. The accuracy of the inference was assessed by convergence of MCMC algorithm, checked using graphical inspection of running means, MCMC error, and diagnostic statistics included into R/Boa package [15]. The plot of Leverage values vs. the square root of the residual deviance (mean per data point for each study) was used to identify potentially study outlier. The transitivity assumption (i.e., studies comparing different sets of interventions needed to be sufficiently similar) was considered to provide valid indirect inferences. To assess transitivity, we generated descriptive statistics and we compared the distributions of baseline participant characteristics across studies and treatment comparisons. To assess local inconsistencies, we used the node‐splitting method [16], which was not possible to conduct a formal assessment of the consistency of the direct and indirect evidence where the evidence network included open loops. We plotted rank probabilities against the possible ranks for all competing treatments. The confidence in estimates of the outcome was assessed using Confidence in Network Meta-Analysis (CINeMA) [17]. In accordance with Cochrane guidelines, we did not investigate publication bias as our search consider less than ten studies for each data comparison [18]. Statistical analyses were carried out using JAGS and R‐Cran 3.4.3 (Distributed Statistical Computing; Vienna, Austria) [19, 20].
Review of network geometry
We appraised the geometry of the networks for each outcome separately, and provided network graphs for primary outcomes with nodes reflecting the surgical approaches and two nodes linked together by an edge, if at least one study compared the two corresponding surgical techniques. The connection between surgical approaches was analysed (Fig. 1).

Network geometry for studies reporting: a hematoma, b seroma, c postoperative chronic pain, and d hernia recurrence
Results
Systematic review
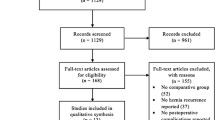
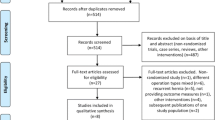
Sixteen studies met the inclusion criteria. The flowchart selection process is reported in Fig. 2. Twelve articles were RCT, three were prospective clinical studies, and one was retrospective clinical study. Overall, 51.037 patients were included in the analysis. Of these, 18.135 (35.5%) underwent Open, 17.112 (33.5%) TAPP, 15.687 (30.7%) TEP, and 103 (0.3%) rTAPP repair (Table 1). The age range from 18 to 65 years and the majority were males (81.5%). Body mass index (BMI) ranged from 24 to 52 kg/m2 (Table 1). The hernia site was reported in six studies, the type of hernia, according to the Nyhus or European Hernia Society (EHS) classification, was reported in seven studies, and the hernia size was reported in three studies. The American Society of Anesthesiologists (ASA) classification was reported in seven studies. Three studies reported the cost analysis. All studies reported the postoperative follow-up that ranged from 1 to 60 months. Quality of life according to the Short-Form 36 (SF-36) questionnaire was accomplished in two studies. We tried out to ensure transitivity by applying narrow inclusion criteria and making populations as similar as possible within and across treatment comparisons. The quality of all included studies is depicted in Fig. 3 and Table 2.

The Preferred Reporting Items for Systematic Reviews and network meta-analyses checklist (PRISMA-NMA) diagram

Risk of bias for randomized-controlled trials was assessed with the Cochrane risk-of-bias tool
Meta-analysis
Haematoma
Nine studies for a total of 54.044 patients reported the incidence of postoperative haematoma. Pooled network meta-analysis shows similar RR when comparing TAPP vs. Open (RR 0.68; 95% CrI 0.40–1.30), TEP vs. Open (RR 0.67; 95% CrI 0.43–1.20), and TEP vs. TAPP (RR 1.01; 95% CrI 0.51–1.80) (Fig. 4a). Node splitting revealed no statistical difference between the direct and indirect comparison (TAPP vs. Open p = 0.242; TEP vs. Open p = 0.202; TEP vs. TAPP p = 0.232). The prior sensitivity analysis yields robust results for TAPP vs. Open (RR 0.68; 95% CrI 0.40–1.30) and TEP vs. Open (RR 0.67; 95% CrI 0.42–1.21). The global heterogeneity is low (I2 = 24%). The SUCRA ranking was 91% for Open, 31% for TEP, and 27% for TAPP.

Forest plots of network meta-analysis estimates the RR for a hematoma, b seroma, c postoperative chronic pain, and d hernia recurrence
Seroma
Nine studies for a total of 54.138 patients reported the incidence of postoperative seroma. Pooled network meta-analysis shows similar RR when comparing TAPP vs. Open (RR 0.91; 95% CrI 0.50–1.62), TEP vs. Open (RR 0.64; 95% CrI 0.32–1.33), TEP vs. TAPP (RR 0.70; 95% CrI 0.39–1.31), and rTAPP vs. Open (RR 0.98; 95% CrI 0.37–2.51) (Fig. 4b). Node splitting revealed no statistical difference between the direct and indirect comparison (TAPP vs. Open p = 0.885; TEP vs. Open p = 0.899; TEP vs. TAPP p = 0.917). The prior sensitivity analysis yields robust results for TAPP vs. Open (RR 0.91; 95% CrI 0.49–1.60), TEP vs. Open (RR 0.63; 95% CrI 0.32–1.31), and rTAPP vs. Open (RR 0.98; 95% CrI 0.37–2.61). The global heterogeneity is moderate (I2 = 39%). The SUCRA ranking was 68% for Open, 62% for rTAPP, 55% for TAPP, and 14% for TEP.
Postoperative chronic pain
Six studies for a total of 36.724 patients reported the incidence of postoperative chronic pain. Pooled network meta-analysis shows similar RR when comparing TAPP vs. Open (RR 0.53; 95% CrI 0.27–1.20), TEP vs. Open (RR 0.86; 95% CrI 0.48–1.16), and TEP vs. TAPP (RR 1.70; 95% CrI 0.63–3.20) (Fig. 4c). Node splitting revealed no statistical difference between the direct and indirect comparison (TAPP vs. Open p = 0.872; TEP vs. Open p = 0.894; TEP vs. TAPP p = 0.974). The prior sensitivity analysis yields robust results for TAPP vs. Open (RR 0.54; 95% CrI 0.28–1.12) and TEP vs. Open (RR 0.86; 95% CrI 0.48–1.70). The global heterogeneity is moderate (I2 = 63%). The SUCRA ranking was 81% for Open, 59% for TEP, and 10% for TAPP.
Recurrence
Nine studies for a total of 111.197 patients reported the postoperative early recurrence. Pooled network meta-analysis shows similar RR when comparing TAPP vs. Open (RR 0.96; 95% CrI 0.57–1.51), TEP vs. Open (RR 1.0; 95% CrI 0.65–1.61), TEP vs. TAPP (RR 1.10; 95% CrI 0.63–2.10), and rTAPP vs. Open (RR 0.98; 95% CrI 0.45–2.10) (Fig. 4d). Node splitting revealed no statistical difference between the direct and indirect comparison (TAPP vs. Open p = 0.81; TEP vs. Open p = 0.707; TEP vs. TAPP p = 0.675). The prior sensitivity analysis yields robust results for TAPP vs. Open (RR 0.96; 95% CrI 0.58–1.50), TEP vs. Open (RR 1.0; 95% CrI 0.65–1.62), and rTAPP vs. Open (RR 0.98; 95% CrI 0.45–2.10). The global heterogeneity is zero (I2 = 0.0%). The SUCRA ranking was TEP 56%, 52% for Open, 49% for rTAPP, and 44% for TAPP. The League table for primary outcomes is depicted in Table 3.
The subgroup analysis including 12 RCT studies showed comparable non-statistically significant results in term of postoperative hematoma, seroma, chronic pain, and recurrence comparing Open, TAPP, and TEP.
Secondary outcomes
Pooled network meta-analysis does not show statistically significant RR comparing TAPP vs. Open, TEP vs. Open, TEP vs. TAPP, and rTAPP vs. Open in term of SSI (RR 0.65; 95% CrI 0.34–1.43, RR 0.59; 95% CrI 0.31–1.34, RR 0.90; 95% CrI 0.39–2.21, RR 1.10; 95% CrI 0.53–2.46, respectively). The global heterogeneity is zero (I2 = 0.0%). Similarly, the pooled network meta-analysis does not show statistically significant RR comparing TAPP vs. Open, TEP vs. Open, TEP vs. TAPP, and rTAPP vs. Open in term of urinary retention (RR 0.92; 95% CrI 0.49–1.78, RR 1.0; 95% CrI 0.55–1.91, RR 1.10; 95% CrI 0.49–2.57, RR 0.96; 95% CrI 0.45–2.14, respectively). The global heterogeneity is zero (I2 = 0.0%). Again, the pooled network meta-analysis does not show statistically significant difference comparing TAPP vs. Open, TEP vs. Open, and TEP vs. TAPP in term of operative time (smd = 2.20; 95% CrI − 1.60 to 5.90, smd = − 1.40; 95% CrI − 5.10 to 2.30, smd = − 3.60; 95% CrI − 7.70 to 0.58, respectively). By contrast, rTAPP was associated with a statistically significant longer operative time compared to Open (smd = 30.0; 95% CrI 21.01–39.02). The global heterogeneity is high (I2 = 89.4%). The pooled network meta-analysis does not show statistically significant differences comparing TAPP vs. Open, TEP vs. Open, and TEP vs. TAPP in term of postoperative length of stay (smd = − 0.73; 95% CrI − 1.70 to 0.20, smd = − 0.47; 95% CrI − 1.70 to 0.69, smd = 0.27; 95% CrI − 0.84 to 1.30, respectively).
The Leverage plots do not show the evidence of study outliers into this network meta-analysis. For all outcomes, there was no evidence of non-MCMC convergence using the diagnostic tools described in the Statistical analysis section. The assessments of confidence in the estimates using CINeMA show moderate-to-very low confidence, essentially due to study limitation, imprecision, and inconsistence.
Discussion
The aim of the present network meta-analysis was to globally compare short-term outcome of the main surgical approaches for primary unilateral inguinal hernia repair. No significant differences were found in term of postoperative hematoma, seroma, chronic pain, and early recurrence. Similarly, no differences were found in term of postoperative surgical site infections, urinary retention, and postoperative hospital length of stay. rTAPP was found to have a statistically significant longer operative time compared to the Open approach.
While the Open approach is considered the gold standard treatment for non-complicated primary inguinal hernia repair, different minimally invasive techniques have been progressively proposed with the introduction of advanced technologies [21]. In the European Hernia Society’s guidelines, the Lichtenstein procedure and the minimally invasive techniques are recommended as the best evidence-based options in experts’ hands [1]. The pros and cons have been largely discussed, but, to date, results are contrasting and a robust evidence favouring one treatment over another is lacking. The previous observational, RCT studies, and pairwise meta-analyses have been published with discordant results. These were mainly related to the heterogeneity of the included populations, surgical techniques, and indications [22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37]. We performed a fully Bayesian network meta-analysis to globally compare outcomes of the main surgical approaches to inguinal hernia. To reduce background heterogeneity, we mainly focused on mesh-reinforced tension-free techniques for primary non-complicated unilateral inguinal hernia.
Postoperative seroma and hematoma represent the most common surgery-related complications [38]. The method for mesh fixations, large hernia size, and medial hernia represent independent risk factors for seroma formation [39]. Kockerling et al. in a recently published data set-based retrospective study reported a significantly lower incidence of overall postoperative complications and seroma in patients that underwent TEP compared to Open and TAPP procedures [37]. Our study showed that Open, TAPP, TEP, and rTAPP seem associated with similar results in term of postoperative hematoma and seroma. The related-global heterogeneity was moderate and low (39% and 21%, respectively). The meta-regression analysis was not possible, because data were reported as aggregated and individual-patient comorbidity was lacking. These results are in accordance with the study by Wu et al. showing no differences comparing TAPP vs. Open [3]. This may be the result of a rigorous surgical technique and careful anatomical planes dissection performed in the experienced hands [40]. It should be noted, however, that despite the lack of statistically significance the Open approach was ranked in the SUCRA as the treatment having a higher likelihood of postoperative hematoma and seroma.
Postoperative chronic pain has been shown to be associated with perioperative nerves injury or entrapment [38]. Nerves can also be trapped in a shrinked mesh or by peri-prosthesis inflammatory processes. In addition, the type of the mesh, the weight of the mesh (g/m2), and fixation method may be contributing factors for the development of postoperative chronic pain [41]. In the present analysis, none of the studies evaluating the robotic approach reported this outcome, and the Open, TAPP, and TEP approaches seem comparable in term of postoperative chronic pain. The global heterogeneity was moderate (I2 = 63%) probably reflecting the lack of a globally accepted and standardized definition of postoperative pain. Notably, the Open approach was classified in the SUCRA ranking as the treatment with major probability for postoperative chronic pain. In the previous studies, the comparison of Lichtenstein vs. TAPP showed a significantly lower chronic pain for TAPP, whereas there was insufficient evidence to determine the best treatment comparing Open vs. TEP and TAPP vs. TEP [42]. Wu et al. revealed that, compared to the Open approach, TAPP was associated with a lower rate of paresthesia with similar chronic pain [3]. In the Open technique, the prophylactic ilioinguinal neurectomy has been proposed to avoid nerve entrapment, thus, reducing postoperative pain [43]. However, it seems that the intraoperative identification and preservation of all three inguinal nerves during open surgery reduces significantly the incidence of postoperative chronic incapacitating groin pain (< 1%) [38, 44, 45].
Age > 50 years, smoking history, BMI > 30, and medial vs. lateral hernia are independent risk factors for hernia recurrence [46, 47]. The pooled network meta-analysis showed that the four surgical approaches seem comparable in term of hernia recurrence. Therefore, this result may not be generalized and the variability in operative technique should be taken into account. Notably, the global heterogeneity was zero (I2 = 0.0%) indicating a low degree of inconsistence across studies and ultimately giving robustness to the result. No significant differences were found in term of surgical site infections, urinary retention, and postoperative length of stay.
After the introduction of robot-assisted minimally invasive surgery, the number of rTAPP has progressively increased worldwide [48, 47]. The robot-assisted approach offers increased range of instruments motion and improved surgeon ergonomics [5]. However, some concerns exist including operative time, surgeon learning curve, real patient-effectiveness, and global costs [49, 50]. In the present review, the rTAPP was associated with an estimated longer operative time compared to the Open approach, probably attributable to instruments positioning and surgeons’ learning curve. The cost analysis was reported in only three studies with a trend toward higher expenses in minimally invasive rTAPP. The pooled analysis was not performed, because the heterogeneity in cost reporting, but this seems imputable to instrument maintenance and equipment costs.
We acknowledge some limitations to the present meta-analysis, because the publication bias related to the heterogeneity of the included studies. Both RCT and observational design studies were considered. The intrinsic bias of observational studies could be considered a study limitation; however, the a priori exclusion of observational studies in systematic reviews is inappropriate and inconsistent with a comprehensive evidence-based approach [51]. Furthermore, the quality and quantity of RCT for surgical techniques comparison is acknowledged to be limited [52]. The imprecision must be considered for some of the outcomes, because the credible interval crosses null value or includes values favouring either treatment. The treatment ranking should be cautiously interpreted, because the treatment ranking does not consider the magnitude of differences in effects, and therefore, chance may explain any apparent difference between treatments. Therefore, surgeons should choose the most suitable surgical approach appraising the treatment ranking, costs, and personal expertise. Finally, the postoperative follow-up was heterogeneous across studies, thus, adding further background bias and the rTAPP was performed in a limited number of patients.
To our knowledge, this is the first network meta-analysis that globally compare outcomes within the major surgical approaches for primary unilateral inguinal hernia. Using network meta-analytical techniques, we were able to globally synthesize data from numerous studies and, therefore, rank the treatments according to our studied outcomes. The study was planned in agreements with the PRISMA guidelines, and followed a sound methodology that was a priori stated in the PROSPERO protocol. This included comprehensive outcome measures and the evaluation of quality at study level (risk of bias) and confidence in results at outcome level (CINeMA). The selection criteria led to a homogenous population for some of the primary outcomes, as confirmed by low heterogeneity. This makes us confident that the results of this study are robust. Finally, we conducted the study accounting for single-study effect performing the prior sensitivity analysis.
In conclusion, this network meta-analysis suggests that Open, TAPP, TEP, and rTAPP seem comparable in term of postoperative hematoma, seroma, postoperative chronic pain, recurrence, infectious complications, urinary retention, and hospital length of stay. The surgical management of inguinal hernia is evolving and the effect of the adoption of innovative minimally invasive techniques should be further investigated in the long term. Ultimately, the choice of the most suitable treatment should be based on individual surgeon expertise and tailored on each patient.
References
The HerniaSurge Group (2018) International guidelines for groin hernia management. Hernia 22(1):1–165. https://doi.org/10.1007/s10029-017-1668-x
Kingsnorth A, LeBlanc K (2003) Hernias: inguinal and incisional. Lancet 362(9395):1561–1571
Wu JJ, Way JA, Eslick GD, Cox MR (2018) Transabdominal pre-peritoneal versus open repair for primary unilateral inguinal hernia: a meta-analysis. World J Surg 5:1304–1311. https://doi.org/10.1007/s00268-017-4288-9
National Institute for Health and Care Excellence (2016) NICE technology appraisal guidance no. 83: laparoscopic surgery for inguinal hernia repair. https://www.nice.org.uk/guidance/ta83. Accessed 9 May 2019
Waite KE, Herman MA, Doyle PJ (2016) Comparison of robotic versus laparoscopic transabdominal preperitoneal (TAPP) inguinal hernia repair. J Robot Surg 10:239–244. https://doi.org/10.1007/s11701-016-0580-1
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J, Moher D (2009) The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 339:b2700. https://doi.org/10.1136/bmj.b2700
Higgins JP, Altman DG, Gotzsche PC, Jüni P, Moher D, Oxman AD, Savovic J, Schulz KF, Weeks L, Sterne JA (2011) The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 343:d5928
Sterne JA, Hernan MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, Henry D, Altman DG, Ansari MT, Boutron I, Carpenter JR, Chan AW, Churchill R, Deeks JJ, Hróbjartsson A, Kirkham J, Jüni P, Loke YK, Pigott TD, Ramsay CR, Regidor D, Rothstein HR, Sandhu L, Santaguida PL, Schünemann HJ, Shea B, Shrier I, Tugwell P, Turner L, Valentine JC, Waddington H, Waters E, Wells GA, Whiting PF, Higgins JP (2016) ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 4919:i355
Mills EJ, Thorlund K, Ioannidis JPA (2013) Demystifying trial networks and network meta-analysis. BMJ 346:f2914–f2914
Aiolfi A, Tornese S, Bonitta G, Rausa E, Micheletto G, Bona D (2019) Roux-En-Y gastric bypass: systematic review and Bayesian network meta-analysis comparing open, laparoscopic, and robotic approach. Surg Obes Relat Dis. https://doi.org/10.1016/j.soard.2019.03.006 (In press)
Warn DE, Thompson SG, Spiegelhalter DJ (2002) Bayesian random effects meta-analysis of trials with binary outcomes: methods for the absolute risk difference and relative risk scales. Stat Med 21(11):1601–1623
Friede T, Röver C, Wandel S, Neuenschwander B (2017) Meta-analysis of few small studies in orphan diseases. Res Synth Methods 8(1):79–91
Turner RM, Davey J, Clarke MJ, Thompson SG, Higgins JP (2012) Predicting the extent of heterogeneity in meta-analysis, using empirical data from the Cochrane database of systematic reviews. Int J Epidemiol 41(3):818–827
Higgins JP, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ 327(7414):557–560
Smith BJ (2007) boa: an R package for MCMC output convergence assessment and posterior inference. J Stat Softw 21:1–37. https://doi.org/10.18637/jss.v021.i11
Dias S, Welton NJ, Caldwell DM, Ades AE (2010) Checking consistency in mixed treatment comparison meta-analysis. Stat Med 29(7–8):932–944
Salanti G, Del Giovane C, Chaimani A, Caldwell DM, Higgins JPT (2014) Evaluating the quality of evidence from a network meta-analysis. PLoS One 9(7):e99682
Higgins JPT, Green S (2011) The Cochrane Collaboration. Cochrane handbook for systemic reviews of interventions, version 5.1.0. The Cochrane Collaboration, Australia. https://training.cochrane.org/handbook. Accessed 9 May 2019
Plummer M (2003) JAGS: a program for analysis of Bayesian graphical models using Gibbs sampling. In: Proceedings of the 3rd international workshop on distributed statistical computing, Vienna, Austria, 20–22 March 2003
R Core Team (2019) R: a language and environment for statistical computing. R Foundation for Statistical Computing, Vienna
Iraniha A, Peloquin J (2018) Long-term quality of life and outcomes following robotic assisted TAPP inguinal hernia repair. J Robot Surg 12:261–269. https://doi.org/10.1007/s11701-017-0727-8
Anadol ZA, Ersoy E, Taneri F, Tekin E (2004) Outcome and cost comparison of laparoscopic transabdominal preperitoneal hernia repair versus Open Lichtenstein technique. J Laparoendosc Adv Surg Tech A 14(3):159–163
Lau H, Patil NG, Yuen W (2006) Day-case endoscopic totally extraperitoneal inguinal hernioplasty versus open Lichtenstein hernioplasty for unilateral primary inguinal hernia in males: a randomized trial. Surg Endosc 1:76–81
Butters M, Redecke J, Köninger J (2007) Long-term results of a randomized clinical trial of Shouldice, Lichtenstein and transabdominal preperitoneal hernia repairs. Br J Surg 94:562–565
Pokorny H, Klingler A, Schmid T, Fortelny R, Hollinsky C, Kawji R, Steiner E, Pernthaler H, Függer R, Scheyer M (2008) Recurrence and complications after laparoscopic versus open inguinal hernia repair: results of a prospective randomized multicenter trial. Hernia 12:385–389. https://doi.org/10.1007/s10029-008-0357-1
Eklund AS, Montgomery AK, Rasmussen IC, Sandbue RP, Bergkvist LA, Rudberg CR (2009) Low recurrence rate after laparoscopic (TEP) and open (Lichtenstein) inguinal hernia repair: a randomized, multicenter trial with 5-year follow-up. Ann Surg 249:33–38. https://doi.org/10.1097/SLA.0b013e31819255d0
Hamza Y, Gabr E, Hammadi H, Khalil R (2010) Four-arm randomized trial comparing laparoscopic and open hernia repairs. Int J Surg 8:25–28. https://doi.org/10.1016/j.ijsu.2009.09.010
Gong K, Zhang N, Lu Y, Zhu B, Zhang Z, Du D, Zhao X, Jiang H (2011) Comparison of the open tension-free mesh-plug, transabdominal preperitoneal (TAPP), and totally extraperitoneal (TEP) laparoscopic techniques for primary unilateral inguinal hernia repair: a prospective randomized controlled trial. Surg Endosc 1:234–239. https://doi.org/10.1007/s00464-010-1165-0
Abbas AE, Abd Ellatif ME, Noaman N, Negm A, El-Morsy G, Amin M, Moatamed A (2012) Patient-perspective quality of life after laparoscopic and open hernia repair: a controlled randomized trial. Surg Endosc 26:2465–2470. https://doi.org/10.1007/s00464-012-2212-9
Dhankhar DS, Sharma N, Mishra T, Kaur N, Singh S, Gupta S (2014) Totally extraperitoneal repair under general anesthesia versus Lichtenstein repair under local anesthesia for unilateral inguinal hernia: a prospective randomized controlled trial. Surg Endosc 28:996–1002. https://doi.org/10.1007/s00464-013-3269-9
Wang WJ, Chen JZ, Fang Q, Li JF, Jin PF, Li ZT (2013) Comparison of the effects of laparoscopic hernia repair and Lichtenstein tension-free hernia repair. J Laparoendosc Adv Surg Tech A 23:301–305. https://doi.org/10.1089/lap.2012.0217
Dahlstrand U, Sandblom G, Ljungdahl M, Wollert S, Gunnarsson U (2013) TEP under general anesthesia is superior to Lichtenstein under local anesthesia in terms of pain 6 weeks after surgery: results from a randomized clinical trial. Surg Endosc 27:3632–3638. https://doi.org/10.1007/s00464-013-2936-1
Aigner F, Augustin F, Kaufmann C, Schlager A, Ulmer H, Pratschke J, Schmid T (2014) Prospective, randomized-controlled trial comparing postoperative pain after plug and patch open repair with totally extraperitoneal inguinal hernia repair. Hernia 18:237–242. https://doi.org/10.1007/s10029-013-1123-6
Pedroso LM, DE-Melo RM, DA-Silva NJ (2017) Comparative study of postoperative pain between the Lichtenstein and laparoscopy surgical techniques for the treatment of unilateral primary inguinal hernia. Arq Bras Cir Dig 30:173–176. https://doi.org/10.1590/0102-6720201700030003
Charles EJ, Mehaffey JH, Tache-Leon CA, Hallowell PT, Sawyer RG, Yang Z (2018) Inguinal hernia repair: is there a benefit to using the robot? Surg Endosc 32:2131–2136. https://doi.org/10.1007/s00464-017-5911-4
Muysoms F, Van Cleven S, Kyle-Leinhase I, Ballecer C, Ramaswamy A (2018) Robotic-assisted laparoscopic groin hernia repair: observational case–control study on the operative time during the learning curve. Surg Endosc 32:4850–4859. https://doi.org/10.1007/s00464-018-6236-7
Köckerling F, Bittner R, Kofler M, Mayer F, Adolf D, Kuthe A, Weyhe D (2019) Lichtenstein versus total extraperitoneal patch plasty versus transabdominal patch plasty technique for primary unilateral inguinal hernia repair: a registry-based, propensity score-matched comparison of 57,906 patients. Ann Surg 269:351–357. https://doi.org/10.1097/SLA.0000000000002541
Campanelli G, Bruni PG, Morlacchi A, Lombardo F, Cavalli M (2017) Primary inguinal hernia: the open repair today pros and cons. Asian J Endosc Surg 10:236–243. https://doi.org/10.1111/ases.12394
Colvin HS, Rao A, Cavalli M, Campanelli G, Amin AI (2013) (2013) Glue versus suture fixation of mesh during open repair of inguinal hernias: a systematic review and meta-analysis. World J Surg 37:2282–2292. https://doi.org/10.1007/s00268-013-2140-4
Wagner JP, Schroeder AD, Espinoza JC, Hiatt JR, Mellinger JD, Cusick RA, Fitzgibbons RJ, Campanelli G, Cavalli M, Roll S, Silva RA, Reinpold W, Télémaque LF, Matthews BD, Filipi CJ, Chen DC (2017) Global outreach using a systematic, competency-based training paradigm for inguinal hernioplasty. JAMA Surg 152:66–73. https://doi.org/10.1001/jamasurg.2016.3323
Rausa E, Asti E, Kelly ME, Aiolfi A, Lovece A, Bonitta G, Bonavina L (2019) Open inguinal hernia repair: a network meta-analysis comparing self-gripping mesh, suture fixation, and glue fixation. World J Surg 2019(43):447–456. https://doi.org/10.1007/s00268-018-4807-3
Scheuermann U, Niebisch S, Lyros O, Jansen-Winkeln B, Gockel I (2017) Transabdominal preperitoneal (TAPP) versus Lichtenstein operation for primary inguinal hernia repair—a systematic review and meta-analysis of randomized controlled trials. BMC Surg 17(1):55. https://doi.org/10.1186/s12893-017-0253-7
Mui WL, Ng CS, Fung TM, Cheung FK, Wong CM, Ma TH, Bn MY, Ng EK (2006) Prophylactic ilioinguinal neurectomy in open inguinal hernia repair: a double-blind randomized controlled trial. Ann Surg 244(1):27–33
Hsu W, Chen CS, Lee HC, Liang HH, Kuo LJ, Wei PL, Tam KW (2012) Preservation versus division of ilioinguinal nerve on open mesh repair of inguinal hernia: a meta-analysis of randomized controlled trials. World J Surgs 36:2311–2319. https://doi.org/10.1007/s00268-012-1657-2
Charalambous MP, Charalambous CP (2018) Incidence of chronic groin pain following open mesh inguinal hernia repair, and effect of elective division of the ilioinguinal nerve: meta-analysis of randomized controlled trials. Hernia 22:401–409. https://doi.org/10.1007/s10029-018-1753-9
Junge K, Rosch R, Klinge U, Schwab R, Peiper Ch, Binnebösel M, Schenten F, Schumpelick V (2006) Risk factors related to recurrence in inguinal hernia repair: a retrospective analysis. Hernia 10(4):309–315
Schjøth-Iversen L, Refsum A, Brudvik KW (2017) Factors associated with hernia recurrence after laparoscopic total extraperitoneal repair for inguinal hernia: a 2-year prospective cohort study. Hernia 21:729–735. https://doi.org/10.1007/s10029-017-1634-7
Escobar Dominguez JE, Ramos MG, Seetharamaiah R, Donkor C, Rabaza J, Gonzalez A (2016) Feasibility of robotic inguinal hernia repair, a single-institution experience. Surg Endosc 9:4042–4048. https://doi.org/10.1007/s00464-015-4717-5
Tam V, Rogers DE, Al-Abbas A, Borrebach J, Dunn SA, Zureikat AH, Zeh HJ 3rd, Hogg ME (2019) Robotic inguinal hernia repair: a large health system’s experience with the first 300 cases and review of the literature. J Surg Res 235:98–104. https://doi.org/10.1016/j.jss.2018.09.070
Henriksen NA, Jensen KK, Muysoms F (2019) Robot-assisted abdominal wall surgery: a systematic review of the literature and meta-analysis. Hernia 23:17–27. https://doi.org/10.1007/s10029-018-1872-3
Shrier I, Boivin JF, Steele RJ (2007) Should meta-analyses of interventions include observational studies in addition to randomized controlled trials? A critical examination of underlying principles. Am J Epidemiol 166:1203–1209
McCulloch P, Taylor I, Sasako M (2002) Randomised trials in surgery: problems and possible solutions. BMJ 324(7351):1448–1451
Funding
None.
Author information
Authors and Affiliations
Contributions
AA, FL, AM, and GC did the literature search; AA, FL, and GC formed the study design; Data collection was done by AA, FL, MC, and AM. AA, GB, and DB analysed the data; AA, GM, and DB interpreted the data; AA, GB, and DB wrote the manuscript; AA, DB, and GC critically reviewed the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
AA, MC, GM, FL, GB, AM, PGB, GC, and Db declare no conflicts of interest.
Ethical approval
Approval from the Institutional review board was not required for this study.
Human and animal rights
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
For this systematic review and meta-analysis, formal consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The article is part of the Topical Collection “Forum on primary monolateral uncomplicated inguinal hernia”.
Rights and permissions
About this article

Cite this article
Aiolfi, A., Cavalli, M., Micheletto, G. et al. Primary inguinal hernia: systematic review and Bayesian network meta-analysis comparing open, laparoscopic transabdominal preperitoneal, totally extraperitoneal, and robotic preperitoneal repair. Hernia 23, 473–484 (2019). https://doi.org/10.1007/s10029-019-01964-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10029-019-01964-2