
Abstract
Background
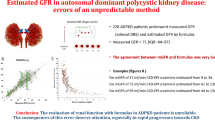
Young autosomal dominant polycystic kidney disease (ADPKD) patients are becoming the new target population for the development of new treatment options. Determination of a reliable equation for estimated glomerular filtration rate (eGFR) from early stages is needed with the promising potential interventional therapies.
Methods
Prospective and longitudinal study on a cohort of 68 genotyped ADPKD patients (age range 0–23 years) with long-term follow-up. Commonly used equations for eGFR were compared for their relative performance.
Results
The revised Schwartz formula (CKiD) showed a highly significant decline in eGFR with aging (− 3.31 mL/min/1.73 m2/year, P < 0.0001). The recently updated equation by the Schwartz group (CKiDU25) showed a smaller (− 0.90 mL/min/1.73 m2/year) but significant (P = 0.001) decline in eGFR with aging and also showed a significant sex difference (P < 0.0001), not observed by the other equations. In contrast, the full age spectrum (FAS) equations (FAS-SCr, FAS-CysC, and the combined) showed no age and sex dependency. The prevalence of hyperfiltration is highly dependent on the formula used, and the highest prevalence was observed with the CKiD Equation (35%).
Conclusions
The most widely used methods to calculate eGFR in ADPKD children (CKiD and CKiDU25 equations) were associated with unexpected age or sex differences. The FAS equations were age- and sex-independent in our cohort. Hence, the switch from the CKiD to CKD-EPI equation at the transition from pediatric to adult care causes implausible jumps in eGFR, which could be misinterpreted. Having reliable methods to calculate eGFR is indispensable for clinical follow-up and clinical trials.
Graphical abstract

A higher resolution version of the Graphical abstract is available as Supplementary information
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Autosomal dominant polycystic kidney disease (ADPKD) is the most common monogenic inherited kidney disease affecting 13 million people worldwide [1]. To date, no curative treatment for ADPKD exists, and patients often rely on kidney replacement therapy for survival [1, 2]. The development of kidney cysts begins in utero with subsequent exponential cyst growth during life [2,3,4,5,6]. For this, young patients with early stages of ADPKD represent a promising target population for intervention studies, since early alteration of the rate of disease progression has the greatest potential to preserve long-term kidney function [3, 7,8,9,10]. However, the lack of sensitive and validated endpoints in this population renders clinical trials very challenging [3, 10]. Kidney function in terms of glomerular filtration rate (GFR) is generally preserved or even increased in the first decades of life [4, 11]. Once kidney function starts to decline, a rapid and quite constant decline of approximately 4–6 mL/min/1.73 m2/year is observed, generally faster than in chronic kidney disease (CKD) from other etiologies [7, 8]. Reduced kidney function is therefore not a typical feature of childhood ADPKD [3, 4, 10]. The mean risk of reduced GFR in childhood is 8% as seen in meta-analyses but varies widely between case series (95% CI: 2–26%, range 2–39%) [3, 4]. In addition, glomerular hyperfiltration, which may herald loss of GFR, has been observed in about 20% of children with ADPKD [11]. However, there is no uniform definition of this phenomenon, studies describing a relation with an increased decline of kidney function in ADPKD children are sparse, and last but not least, the available data on pediatric estimated GFR (eGFR) are very heterogeneous as multiple equations are used [11, 12]. Moreover, a reliable estimation of eGFR over a wide age range spanning from childhood to adulthood appears essential in this regard.
Currently, total kidney volume (TKV) factored for age is the best predictor of GFR trajectory; however, it is available only for subjects older than 15 years [7,8,9]. In addition, several clinical trials showed a dissociation between the rate change of TKV and GFR [7]. Specifically, it remains unclear how to best estimate the GFR in the early stages of ADPKD. GFR is commonly estimated based on endogenous filtration markers, for example, serum creatinine (SCr) and serum cystatin C (SCysC), which are less complex and provide rapid results compared with the measured GFR (mGFR) [13]. However, eGFR has severe limitations. Separate equations (Supplementary Table S1) have been developed for children (CKiD equation is recommended in all children per the current KDIGO guidelines), and younger and middle-age adults (CKD-EPI equation) [13,14,15,16,17]. These equations lack continuity with aging and can cause implausible jumps at the transition from pediatric to adult care [15]. To this end, new equations for eGFR across the full age spectrum (FAS) were recently introduced [18,19,20,21,22]. These FAS equations are based on normalized SCr (SCr/Q), where Q is the median SCr from healthy populations to account for age- and sex-related differences in SCr generation [18,19,20,21,22]. Both a height-dependent (FAS-Height) and a height-independent equation (FAS-Age, with Q-matching on age) have been reported [18,19,20,21,22]. With the FAS equations, the adjustment for age (in children) and sex is on the level of SCr and not on the level of GFR [18,19,20,21,22]. This is more direct because a clear increase in SCr during childhood exists with a difference between sexes during adolescence [19, 20]. In contrast, the body surface area indexed GFR is not age-dependent during childhood and young adulthood, and (small) differences in GFR between sexes are still a matter of intense debate [13]. Despite the demonstrated biases associated with the use of the CKiD equation [13], it is still the most widely used and recommended equation for the follow-up of kidney function in children worldwide [14].
We aimed to evaluate all the available equations for the calculation of eGFR and compare their relative performance in a prospective, genotyped cohort of young ADPKD patients with longitudinal follow-up, in order to identify the most appropriate method for this population. Furthermore, the study evaluated the performance of eGFR equations during transition from pediatric to adult care.
Methods
Ethical statement
The study was approved by the local ethical board (Ethical Committee Research KU / UZ Leuven, S59500) and in accordance with the Declaration of Helsinki. Written informed consent was obtained from either the parents or patients.
Patients
ADPKD patients followed at the dedicated pediatric ADPKD clinic from the University Hospital of Leuven, with available longitudinal biobanking material, were included. The diagnosis of ADPKD was made on a clinical basis with genetic confirmation. Relevant demographic and anthropometric data including age, sex, height, and weight were collected yearly. Furthermore, reason and setting of diagnosis, including potential prenatal signs of cystic kidney disease, were determined for each subject.
Laboratory measurements
Longitudinally stored lithium heparin plasma samples in the biobank collected between January 2014 and June 2021 were measured for SCr and SCysC in one run in the Laboratory of the University Hospital of Leuven to exclude any sampling and/or methodology bias. SCr was determined on a Roche Cobas 8000 C702 module using an enzymatic colorimetric method (traceable to the gold standard isotope dilution mass spectrometry method), and SCysC was measured using the particle enhanced immunoturbidimetric assay on Roche Cobas 8000 C502 platform according to the manufacturer’s instructions (Roche Diagnostics, Basel, Switzerland), calibrated to the certified international reference material ERM-DA471/IFCC.
Statistical analysis
Data are described as mean and SD if normally distributed, otherwise by median and interquartile range. The evolution of SCr, SCysC, and estimated GFR with age were graphically displayed. Linear quantile regression analysis, for the longitudinal data, was used to quantify the evolution of eGFR with age. Bland-Altman correlation analysis was performed comparing the different equations against the FAS-Age equation. Significance level was set at alpha = 0.0023 (Bonferroni correction for multiple testing n = 22). SAS 9.4 (SAS Institute, Inc., Cary, North Carolina, USA) statistical package was used.
Results
Population demographics
We included 68 genotyped ADPKD patients. The cohort was equally distributed in terms of sex, with a mean age of 10.2 years (min–max: 0.0–23.0 years) and with a mean time of follow-up of 3.6 years (min–max: 1.0–8.0 years) and a mean number of measurements of 4 (min–max: 1–9) (Table 1). Approximately 20% of cases had prenatal signs of cystic kidney disease. In 70.6%, the diagnosis of ADPKD was made by screening in the context of a family history of ADPKD. A positive family history of ADPKD was described in 96.0% of cases. The majority of patients had a mutation in the PKD1 gene (92.7%), the others in PKD2 or GANAB (Table 1).
Anthropometric values and SCr and SCysC are as expected
Longitudinal measurements (n = 275 measurements) of height, weight, and BMI plotted against age were within the reference limits for a healthy population (Fig. 1). As such, there are no arguments for growth retardation in the studied population (Fig. 1b). The majority of both SCr and SCysC measurements fall within the reference intervals (Fig. 2a, b, Table 2). No significant differences in SCr (mg/dl) or SCysC (mg/l) between boys and girls were detected (0.49 (0.29) versus 0.47 (0.17), P = 0.4 and 0.87 (0.13) versus 0.88 (0.17), P = 0.8), respectively). No statistically significant difference, accounted for multiple testing (P = 0.02), in SCr/Q was observed between boys and girls (Tables 2 and 3). SCr/Q showed no significant age-dependency (slope of the median regression line is + 0.0046 mg/dL/year, 95% CI [0.0013; 0.0093], P = 0.03) (Table 4 and Fig. 3a).

a Body height (cm) longitudinally plotted against age. b Weight (kg) against age. c BMI against age. Measurements of males in red and of females in blue. P2.5, P50, and P97.5 are represented according to growth curves of Flanders 2004

a Serum creatinine longitudinally plotted against age with reference bands from Hoste et al.; light gray for girls and dark gray for boys19. The measurements of boys in red and of girls in blue. b Serum cystatin C against age. P2.5, P50, and P97.5 are presented according to Ziegelasch et al.24

Comparison of the different equations based on the longitudinally plotted values. Values of boys indicated in red, in blue for girls. a SCr/Q plotted against age with slope of the median quantile regression line of + 0.0044 mg/dL/year) and P value of (P = 0.03). b eGFR-CKiD against age (− 3.31 mL/min/1.73 m2/year, P < 0.0001). c eGFR-CKIDU25 against age (− 0.90 mL/min/1.73 m2/year, P = 0.001). d eGFR-FAS-Age against age (− 0.61 mL/min/1.73 m2/year, P = 0.03). e eGFR-FAS-Height against age (− 0.98 mL/min/1.73 m2/year, P = 0.0005). f eGFR-EFKC against age (− 0.27 mL/min/1.73 m2/year, Pp = 0.0004). g eGFR-LRM18 against age (− 0.45 mL/min/1.73 m2/year, P = 0.0004). h eGFR-CKD-EPI against age (− 0.08 mL/min/1.73 m2/year, P = 0.5). i CysC/Q against age (− 0.0010 mg/L/year, P = 0.7). j eGFR-FAS-CysC against age (0.096 mL/min/1.73 m2/year, P = 0.1). k eGFR-FAS-combined against age (− 0.2877 mL/min/1.73 m.2/year, P = 0.3)
Influence of sex and/or age on the used eGFR equation
As described in the previous paragraph, the evolution of SCr and SCysC in the young ADPKD patients falls within the reference interval for a healthy population, suggesting a preserved and stable kidney function. However, the eGFR calculated with the revised Schwartz formula (CKiD) showed a highly significant and steep decline in eGFR with aging (− 3.31 mL/min/1.73 m2/year, [− 3.69; − 2.65], P < 0.0001) (Table 4 and Fig. 2). No significant sex difference was observed with this equation (P = 0.6, Table 3). The recently updated equation by the Schwartz group (CKiDU25) showed a smaller but still significant (− 0.90 mL/min/1.73 m2/year, [− 1.81; − 0.37], P = 0.001) decline in eGFR with aging (Table 4 and Fig. 3). In addition, a significant difference in eGFR (mL/min/1.73 m2) between boys and girls was found with this new equation (124.7 (19.5) versus 109.8 (20.5), P < 0.0001) (Table 3). SCr normalized for Q and the related FAS equations did not show a clear age-or sex- dependency (Tables 3 and 4). In addition, CysC-based and combined equations were independent of age and sex in this pediatric ADPKD patient cohort (Tables 3, 4 and Fig. 3). Bland–Altman plots for the different equations against FAS-Age are added in Supplementary Fig. 1. Data from the Bland–Altman analysis is summarized in Supplementary Table S2. These plots showed the relative bias introduced by each formula against the FAS-Age equation.
The proportion of hyperfiltration is highly dependent on the used eGFR equation
The highest prevalence of values corresponding with hyperfiltration (defined as eGFR > 133.9 mL/min/1.73 m2) was observed with the use of the CKiD equation (Table 5). Almost no measurements fell within the range of hyperfiltration by using SCysC-based equations (Table 5).
The eGFR during transition from childhood to adulthood
A subgroup analysis of 16 patients who reached adulthood (18–23 years) was performed and included 60 measurements of SCr and SCysC to evaluate the eGFR equations during this transition phase. A comparison of the different equations is displayed in Table 6. For this subgroup, CKD-EPI predicts a mean eGFR = 130.35 mL/min/1.73 m2, while revised/bedside Schwartz (CKiD) predicts 103.93 mL/min/1.73 m2, a difference of 25%, and the newly updated CKiDU25 equation predicts a value of 116.25 mL/min/1.73 m2 (Table 6). Considering the median eGFR values, the difference between Schwartz (99.07 mL/min/1.73 m2) and CKD-EPI (130.26 mL/min/1.73 m2) is even larger, with a difference of 31.5% (Table 6). However, using FAS equations, no jumps at transition were observed (Table 6).
Discussion
We describe the evaluation of kidney function of a genotyped ADPKD cohort with early stages, demonstrating that the most widely used methods to calculate eGFR in children and adolescents (CKiD and CKiDU25 equations) are associated with unexpected age or sex differences and with a higher proportion of hyperfiltration. However, the FAS equations were age- and sex-independent in our cohort and could be used over the entire age spectrum.
Indeed, young CKD-stage ADPKD patients, both children and young adults, represent a promising target population for intervention studies [4, 5, 10, 12]. Since eligibility for inclusion in clinical trials is often based on GFR estimation, in order to be able to assess the impact of potential drugs on kidney function, a reliable method to follow up on kidney function is greatly needed [2, 10]. GFR, the most universally used marker of kidney function, is commonly estimated by plasma markers [13]. More than 70 equations for eGFR have been described, based on SCr and SCysC [23, 24]. The reliability of all these formulae is far from perfect [23]. A recent study on 226 adult ADPKD patients showed an average error of about 50% between the different eGFR equations and the measured GFR [23]. With the use of longitudinal follow-up data on a well-characterized and genotyped cohort of young ADPKD patients, we aimed to compare the relative performance of SCr, SCysC, and combined methods to calculate eGFR.
The current KDIGO guidelines recommend the use of the CKiD equation for the calculation of eGFR in children and the CKD-EPI equation in adults [14, 23]. The Schwartz group initially described the relationship between body length, GFR, and SCr in the following equation: eGFR = k × body length (cm)/SCr (mg/dL); the coefficient k is different in preterm infants, full-term infants, children between 2 and 12 year of age and males and females over the age of 12 years [14]. This formula was developed for the Jaffe method determined SCr [14]. In 2009, the revised/bedside Schwartz equation (CKiD equation) was introduced, designed for enzymatic SCr determination [14, 25,26,27,28,29]. This CKiD equation was initially developed and validated in children with CKD until the age of 16 years with a high prevalence of patients with poor growth [13,14,15]. However, it is commonly accepted and recommended by the KDIGO guidelines to calculate eGFR in all children until the age of 18 years with this formula [13,14,15].
However, the concern about the applicability of this formula in children without CKD and different ethnic groups was already raised [25,26,27,28,29]. It was already highlighted in literature that body composition differs between different ethnic groups which highly impact on the applicability of the CKiD equation in children from different origins [25,26,27,28,29]. For example, the CKiD equation is not applicable in Japanese children, and for this reason, Uemura’s formula was introduced [29]. Our cohort did show in the majority of cases an evolution of height, weight, SCr, and SCysC within the reference intervals for a healthy population. The CKiD-eGFR equation showed a strong decline with aging during childhood and young adulthood in ADPKD patients. However, this decline in kidney function with aging was not reflected in the evolution of SCr and SCysC against age. In addition, the recently introduced CKiDU25 equation [16], with age-specific k values, did not show such a strong decline with age, although the decrease was still statistically significant. On the other hand, the new CKiDU25 equation [16, 17] introduced significant difference between boys and girls which was unexpected based on the SCr and SCysC data. Furthermore, the switch from CKiD or CKiDU25 [16, 17] to the CKD-EPI equation [15] at the age of 18 years causes implausible jumps at the transition from pediatric to adult care [15]. eGFR is a poor outcome measure in early ADPKD; however, it has been reported that 8% of the children had CKD stage 2 or higher, and 20% have hyperfiltration [3, 4, 10, 11]. Of note, absolute hyperfiltration is defined as a supra-physiological increase of glomerular filtration rate that occurs when single nephron filtration rate increases in a kidney with a normal number of nephrons [30,31,32,33]. Absolute hyperfiltration can occur in healthy people after a high protein meal or during pregnancy and is also observed in diabetes, obesity, and ADPKD [30,31,32,33]. Persistent increases in single-nephron glomerular filtration rates that are associated with glomerular hypertension can eventually lead to proteinuria, glomerular sclerosis, and in a decline in kidney function [30,31,32,33]. In young ADPKD patients with preserved kidney function, early vasoconstriction and reduced kidney blood flow can cause an increase in filtration fraction [30,31,32,33]. Glomerular hyperfiltration in ADPKD might also be mediated by angiotensin II with a predominant effect of vasoconstriction in the efferent glomerular arterioles [31]. On the other hand, the presence of absolute hyperfiltration in this cohort of patients can itself interfere with the accuracy of the different eGFR formulae, because the equations are not developed in those reference limits [34, 35]. To the best of our knowledge there is only one study that described hyperfiltration in pediatric ADPKD with the use of mGFR [30]. They observed significantly higher GFRs in young ADPKD patients (n = 18) versus controls (n = 41) [30]. The diagnostic performance of SCysC was superior to SCr for the detection of hyperfiltration in this specific population of patients [30]. There is to date no consensus on the cutoff value for hyperfiltration; however, a cutoff of 135 mL/min/1.73 m2 is most commonly used according to the literature [32, 33]. We compared different arbitrary cut-off values calculated from the lower limits of SCr and SCysC. We demonstrated huge differences in the prevalence of hyperfiltration (based on the different arbitrary cutoffs) between the different equations. The highest prevalence of hyperfiltration was observed with the use of the CKiD equation. Of note, the majority of studies investigating and describing hyperfiltration in ADPKD used the CKiD equation [4, 5, 11, 30]. The high prevalence of hyperfiltration was not observed with the SCysC-based equations. The FAS equation better captures the fluctuations over age seen in SCr and SCysC, meaning that this normalization with Q values might be more adapted for ADPKD children [18, 19, 23]. The normalized SCr and SCysC is therefore a preferable tool to compare children of different age and sex [18, 19, 23]. The main advantage of using normalized values is that there is no need to convert SCr/SCysC into an eGFR value, which depends on the formula used [18, 19, 23]. Furthermore, the different eGFR formulas have only been validated after the age of 2 years, in contrast to the normalized biomarkers which are still useful from 6 weeks of age [13]. SCr/Q did not show an age- (+ 0.0046 mg/dL/year, P = 0.03) and sex- dependency (P = 0.02), after Bonferroni correction. The SCr-based FAS equation (FAS-Age), and cystatin C–based FAS equation (FAS-CysC) and the combined FAS equation were also age- and sex-independent in the present ADPKD cohort. The rationale to combine SCr and SCysC to calculate eGFR originated from the fact of the differences in sources of error [32,33,34,35]. SCr is dependent on muscle mass and variable tubular secretion, while SCysC may differ with alterations in volume status [33, 34]. Previous research already described the poor agreement between CKiD and CKD-EPI before and during transition with systematically higher eGFR with the CKD-EPI equation especially in males [36]. The FAS equations are applicable for all ages, thus avoiding implausible jumps at the transition from pediatric to adult nephrology. Moreover, the continuity of SCr-based eGFR was already shown in the Japanese population with the Uemura and 3-variable Japanese formula [29]. The Uemura formula, suitable for children aged between 2 and 18 years, also contains a normalization of SCr (eGFRUemura = 110.2 × (Reference SCr/SCr) + 2.93). Bland–Altman analysis was performed to analyze the relative bias of the different formulas against the FAS-age equation. FAS-age gives generally higher eGFR values (especially in adolescents) compared to the CKiD equation and lower values compared with the CKD-EPI equation in young adults [21, 22]. We observed a discrepancy in the high eGFR ranges between FAS-age and LMR18, EFKC, and CKD-EPI. Those formulas contain power coefficients based on SCr growth curves to avoid erroneous overestimation of eGFR for low SCr values. This intrinsic feature of the LMR18, EFKC, and CKD-EPI probably explains the observed discrepancy. The strengths of our study are that all the ADPKD patients had a genetic confirmation and that the methodology of the sampling and the measures of all the samples were standardized. A limitation is the absence of measured GFR, which could provide direct evidence for the choice of the best eGFR equation. Therefore, our future studies will be focused on the correlation and agreement between measured GFR and the different eGFR equations (both SCr- and SCysC-based) to confirm our findings. Furthermore, since our cohort included only Caucasian patients, racial influences were not evaluated. Moreover, applying Bonferroni’s correction for multiple testing relaxes the claim for significance and consequently makes it easier to state that “no significant difference” is a condition of a suitable formula.
Conclusion
The most widely used methods to calculate eGFR in children and adolescents (CKiD and CKiDU25 equations) were associated with unexpected age or sex differences in young ADPKD patients and high estimation of hyperfiltration. However, the FAS equations were age- and sex-independent in our cohort. Hence, the switch from the CKiD to CKD-EPI equation at the transition from pediatric to adult care causes implausible jumps in eGFR, which could be misinterpreted. We propose that the FAS equations are more appropriate to be used in order to evaluate eGFR in the early stages ADPKD.
Data availability
The data underlying this article cannot be shared publicly due to the privacy of the individuals who participated in the study. The data will be shared on reasonable request to the corresponding author.
Abbreviations
- ADPKD:
-
Autosomal dominant polycystic kidney disease
- CKD:
-
Chronic kidney disease
- TKV:
-
Total kidney volume
- EGFR:
-
Estimated glomerular filtration rate
- FAS:
-
Full age spectrum
- SCr:
-
Serum creatinine
- SCysC:
-
Serum cystatin C
References
Torres VE, Harris PC, Pirson Y (2007) Autosomal dominant polycystic kidney disease. Lancet 369:1287–1301. https://doi.org/10.1016/S0140-6736(07)60601-1
Gimpel C, Bergmann C, Bockenhauer D, Breysem L, Cadnapaphornchai MA, Cetiner M, Dudley J, Emma F, Konrad M, Harris T, Harris PC, König J, Liebau MC, Marlais M, Mekahli D, Metcalfe AM, Oh J, Perrone RD, Sinha MD, Titieni A, Torra R, Weber S, Winyard PJD, Schaefer F (2019) International consensus statement on the diagnosis and management of autosomal dominant polycystic kidney disease in children and young people. Nat Rev Nephrol 15:713–726. https://doi.org/10.1038/s41581-019-0155-2
Fick-Brosnahan GM, Tran ZV, Johnson AM, Strain JD, Gabow PA (2001) Progression of autosomal-dominant polycystic kidney disease in children. Kidney Int 59:1654–1662. https://doi.org/10.1046/j.1523-1755.2001.0590051654
Massella L, Mekahli D, Paripović D, Prikhodina L, Godefroid N, Niemirska A, Ağbaş A, Kalicka K, Jankauskiene A, Mizerska-Wasiak M, Afonso AC, Salomon R, Deschênes G, Ariceta G, Özçakar ZB, Teixeira A, Duzova A, Harambat J, Seeman T, Hrčková G, Lungu AC, Papizh S, Peco-Antic A, De Rechter S, Giordano U, Kirchner M, Lutz T, Schaefer F, Devuyst O, Wühl E, Emma F (2018) Prevalence of Hypertension in Children with Early-Stage ADPKD. Clin J Am Soc Nephrol 13:874–883. https://doi.org/10.2215/CJN.11401017
Shamshirsaz AA, Reza Bekheirnia M, Kamgar M, Johnson AM, McFann K, Cadnapaphornchai M, Nobakhthaghighi N, Schrier RW (2005) Autosomal-dominant polycystic kidney disease in infancy and childhood: progression and outcome. Kidney Int 68:2218–2224. https://doi.org/10.1111/j.1523-1755.2005.00678.x
Cadnapaphornchai MA, Masoumi A, Strain JD, McFann K, Schrier RW (2011) Magnetic resonance imaging of kidney and cyst volume in children with ADPKD. Clin J Am Soc Nephrol 6:369–376. https://doi.org/10.2215/CJN.03780410
Yu ASL, Shen C, Landsittel DP, Grantham JJ, Cook LT, Torres VE, Chapman AB, Bae KT, Mrug M, Harris PC, Rahbari-Oskoui FF, Shi T, Bennett WM, Consortium for Radiologic Imaging Studies of Polycystic Kidney Disease (CRISP) (2019) Long-term trajectory of kidney function in autosomal-dominant polycystic kidney disease. Kidney Int 95:1253–1261. https://doi.org/10.1016/j.kint.2018.12.023
Janssens P, Jouret F, Bammens B et al (2020) Implications of early diagnosis of autosomal dominant polycystic kidney disease: A post hoc analysis of the TEMPO 3:4 trial. Sci Rep 10:4294. https://doi.org/10.1038/s41598-020-61303-9
Cornec-Le Gall E, Audrézet MP, Rousseau A, Hourmant M, Renaudineau E, Charasse C, Morin MP, Moal MC, Dantal J, Wehbe B, Perrichot R, Frouget T, Vigneau C, Potier J, Jousset P, Guillodo MP, Siohan P, Terki N, Sawadogo T, Legrand D, Menoyo-Calonge V, Benarbia S, Besnier D, Longuet H, Férec C, Le Meur Y (2016) The PROPKD Score: A New Algorithm to Predict Renal Survival in Autosomal Dominant Polycystic Kidney Disease. J Am Soc Nephrol 27:942–951. https://doi.org/10.1681/ASN.2015010016
De Rechter S, Bammens B, Schaefer F, Liebau MC, Mekahli D (2018) Unmet needs and challenges for follow-up and treatment of autosomal dominant polycystic kidney disease: the paediatric perspective. Clin Kidney J 11:i14–i26. https://doi.org/10.1093/ckj/sfy088
Helal I, Reed B, McFann K, Yan XD, Fick-Brosnahan GM, Cadnapaphornchai M, Schrier RW (2011) Glomerular hyperfiltration and renal progression in children with autosomal dominant polycystic kidney disease. Clin J Am Soc Nephrol 6:2439–2443. https://doi.org/10.2215/CJN.01010211
Cachat F, Combescure C, Cauderay M, Girardin E, Chehade H (2015) A systematic review of glomerular hyperfiltration assessment and definition in the medical literature. Clin J Am Soc Nephrol 10:382–389. https://doi.org/10.2215/CJN.03080314
Soveri I, Berg UB, Björk J, Elinder CG, Grubb A, Mejare I, Sterner G, Bäck SE, SBU GFR Review Group (2014) Measuring GFR: a systematic review. Am J Kidney Dis 64:411–424. https://doi.org/10.1053/j.ajkd.2014.04.010
Schwartz GJ, Muñoz A, Schneider MF, Mak RH, Kaskel F, Warady BA, Furth SL (2009) New equations to estimate GFR in children with CKD. J Am Soc Nephrol 20:629–637. https://doi.org/10.1681/ASN.2008030287
Pottel H, Björk J, Bökenkamp A, Berg U, Åsling-Monemi K, Selistre L, Dubourg L, Hansson M, Littmann K, Jones I, Sjöström P, Nyman U, Delanaye P (2019) Estimating glomerular filtration rate at the transition from pediatric to adult care. Kidney Int 95:1234–1243. https://doi.org/10.1016/j.kint.2018.12.020
Pottel H, Björk J, Delanaye P, Nyman U (2022) Evaluation of the creatinine-based chronic kidney disease in children (under 25 years) equation in healthy children and adolescents. Pediatr Nephrol 37:2213–2216. https://doi.org/10.1007/s00467-022-05429-0
Pierce CB, Muñoz A, Ng DK, Warady BA, Furth SL, Schwartz GJ (2021) Age- and sex-dependent clinical equations to estimate glomerular filtration rates in children and young adults with chronic kidney disease. Kidney Int 99:948–956. https://doi.org/10.1016/j.kint.2020.10.047
Hoste L, Dubourg L, Selistre L, De Souza VC, Ranchin B, Hadj-Aïssa A, Cochat P, Martens F, Pottel H (2014) A new equation to estimate the glomerular filtration rate in children, adolescents and young adults. Nephrol Dial Transplant 29:1082–1091. https://doi.org/10.1093/ndt/gft277
Pottel H, Björk J, Courbebaisse M, Couzi L, Ebert N, Eriksen BO, Dalton RN, Dubourg L, Gaillard F, Garrouste C, Grubb A, Jacquemont L, Hansson M, Kamar N, Lamb EJ, Legendre C, Littmann K, Mariat C, Melsom T, Rostaing L, Rule AD, Schaeffner E, Sundin PO, Turner S, Bökenkamp A, Berg U, Åsling-Monemi K, Selistre L, Åkesson A, Larsson A, Nyman U, Delanaye P (2020) Development and Validation of a Modified Full Age Spectrum Creatinine-Based Equation to Estimate Glomerular Filtration Rate : A Cross-sectional Analysis of Pooled Data. Ann Intern Med 174:183–191. https://doi.org/10.7326/M20-4366
Björk J, Nyman U, Delanaye P, Grubb A, Larsson A, Vranken L, Åkesson A, Pottel H (2020) A novel method for creatinine adjustment makes the revised Lund-Malmö GFR estimating equation applicable in children. Scand J Clin Lab Invest 80:456–463. https://doi.org/10.1080/00365513.2020.1774641
Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI, Kusek JW, Eggers P, Van Lente F, Greene T, Coresh J, CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) (2009) A new equation to estimate glomerular filtration rate. Ann Intern Med 150:604–612. https://doi.org/10.7326/0003-4819-150-9-200905050-00006
Pottel H, Delanaye P, Schaeffner E, Dubourg L, Eriksen BO, Melsom T, Lamb EJ, Rule AD, Turner ST, Glassock RJ, De Souza V, Selistre L, Goffin K, Pauwels S, Mariat C, Flamant M, Ebert N (2017) Estimating glomerular filtration rate for the full age spectrum from serum creatinine and cystatin C. Nephrol Dial Transplant 32:497–507. https://doi.org/10.1093/ndt/gfw425
Rodríguez RM, Luis-Lima S, Fernandez JM et al (2022) Estimated GFR in autosomal dominant polycystic kidney disease: errors of an unpredictable method. J Nephrol 35:2109–2118. https://doi.org/10.1007/s40620-022-01286-0
Ziegelasch N, Vogel M, Müller E, Tremel N, Jurkutat A, Löffler M, Terliesner N, Thiery J, Willenberg A, Kiess W, Dittrich K (2019) Cystatin C serum levels in healthy children are related to age, gender, and pubertal stage. Pediatr Nephrol 34:449–457. https://doi.org/10.1007/s00467-018-4087-z
Uemura O, Honda M, Matsuyama T, Ishikura K, Hataya H, Nagai T, Ikezumi Y, Fujita N, Ito S, Iijima K, Japanese Society for Pediatric Nephrology, the Committee of Measures for Pediatric CKD (2012) Is the new Schwartz equation derived from serum creatinine and body length suitable for evaluation of renal function in Japanese children? Eur J Pediatr 171:1401–1404. https://doi.org/10.1007/s00431-012-1772-y
Uemura O, Honda M, Matsuyama T, Ishikura K, Hataya H, Yata N, Nagai T, Ikezumi Y, Fujita N, Ito S, Iijima K, Kitagawa T (2011) Age, gender, and body length effects on reference serum creatinine levels determined by an enzymatic method in Japanese children: a multicenter study. Clin Exp Nephrol 15:694–699. https://doi.org/10.1007/s10157-011-0452-y
Uemura O, Nagai T, Ishikura K, Ito S, Hataya H, Gotoh Y, Fujita N, Akioka Y, Kaneko T, Honda M (2014) Creatinine-based equation to estimate the glomerular filtration rate in Japanese children and adolescents with chronic kidney disease. Clin Exp Nephrol 18:626–633. https://doi.org/10.1007/s10157-013-0856-y
Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K, Yamagata K, Tomino Y, Yokoyama H, Hishida A, Collaborators developing the Japanese equation for estimated GFR (2009) Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis 53:982–992. https://doi.org/10.1053/j.ajkd.2008.12.034
Uemura O, Yokoyama H, Ishikura K, Gotoh Y, Sato H, Sugiyama H, Honda M, Matsuo S (2017) Performance in adolescents of the two Japanese serum creatinine based estimated glomerular filtration rate equations, for adults and paediatric patients: A study of the Japan Renal Biopsy Registry and Japan Kidney Disease Registry from 2007 to 2013. Nephrology 22:494–497. https://doi.org/10.1111/nep.12982
Wong H, Vivian L, Weiler G, Filler G (2004) Patients with autosomal dominant polycystic kidney disease hyperfiltrate early in their disease. Am J Kidney Dis 43:624–628. https://doi.org/10.1053/j.ajkd.2003.12.026
Cortinovis M, Perico N, Ruggenenti P, Remuzzi A, Remuzzi G (2022) Glomerular hyperfiltration. Nat Rev Nephrol 18:435–451. https://doi.org/10.1038/s41581-022-00559-y
Pottel H, Adebayo OC, Nkoy AB, Delanaye P (2022) Glomerular hyperfiltration: part 1 - defining the threshold - is the sky the limit? Pediatr Nephrol. https://doi.org/10.1007/s00467-022-05827-4
Adebayo OC, Nkoy AB, van den Heuvel LP, Labarque V, Levtchenko E, Delanaye P, Pottel H (2022) Glomerular hyperfiltration: part 2-clinical significance in children. Pediatr Nephrol. https://doi.org/10.1007/s00467-022-05826-5
Huang SH, Sharma AP, Yasin A, Lindsay RM, Clark WF, Filler G (2010) Hyperfiltration affects accuracy of creatinine eGFR measurement. Clin J Am Soc Nephrol 6:274–280. https://doi.org/10.2215/CJN.02760310
Sharma AP, Yasin A, Garg AX, Filler G (2011) Diagnostic accuracy of cystatin C-based eGFR equations at different GFR levels in children. Clin J Am Soc Nephrol 6:1599–1608. https://doi.org/10.2215/CJN.10161110
Webster-Clark M, Jaeger B, Zhong Y, Filler G, Alvarez-Elias A, Franceschini N, Díaz-González de Ferris ME (2018) Low agreement between modified-Schwartz and CKD-EPI eGFR in young adults: a retrospective longitudinal cohort study. BMC Nephrol 19:194. https://doi.org/10.1186/s12882-018-0995-1
Acknowledgements
The authors thank Sarah Kerselaers and Ariadne van Hulle. Above all, the authors wish to thank the participating children and their parents, as well as the nurses involved in the care of the patients.
Funding
This work was supported by the Research Foundation Flanders (FWO) (G0C8920N) (1804123N) and UZ Leuven.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval
The study was approved by the local ethical board (Ethical Committee Research KU/UZ Leuven, S59500) and in accordance with the Declaration of Helsinki. Written informed consent was obtained from either the parents or patients.
Conflict of interest
The Research Foundation Flanders (F.W.O.) supports Pieter Schellekens. DM reports research grants from Otsuka and serves in advisory boards for Otsuka, Sanofi Genzyme and Reata, all outside the submitted work and all paid to her institutions UZ Leuven and KU Leuven, Belgium. The other authors have no conflict of interest to declare related to this manuscript.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
467_2023_5926_MOESM2_ESM.pdf
Supplementary file2 (PDF 463 KB) Supplementary Table S1. Formulas for the different eGFR equations [e.g. (PDF)]. Supplementary Table S2. Results of the Bland-Altman correlation analysis comparing FAS-Age with the different equations [e.g. (PDF)].
467_2023_5926_MOESM3_ESM.pptx
Supplementary file3 (PPTX 183 KB) Supplementary Figure 1 (a) Bland-Altman plot of the difference (FAS-Age – CKiD) vs. the mean (FAS-Age + CKiD)/2. (b) Bland-Altman plot of the difference (FAS-Age – CkiDU25) vs. the mean (FAS-Age + CKiDU25)/2. (c) Bland-Altman plot of the difference (FAS-Age – FAS-Height) vs. the mean (FAS-Age + FAS-Height)/2. (d) Bland-Altman plot of the difference (FAS-Age – EFKC) vs. the mean (FAS-Age + EFKC)/2. (e) Bland-Altman plot of the difference (FAS-Age – LMR18) vs. the mean (FAS-Age + LMR18)/2. (f) Bland-Altman plot of the difference (FAS-Age – CKD-EPI40) vs. the mean (FAS-Age + CKD-EPI40)/2. (g) Bland-Altman plot of the difference (FAS-Age – FAS-CysC) vs. the mean (FAS-Age + FAS-CysC)/2. (h) Bland-Altman plot of the difference (FAS-Age – FAS-combi) vs. the mean (FAS-Age + FAS-combi)/2. (i) Bland-Altman plot of the difference (FAS-Age – FAS-Combi-Height) vs. the mean (FAS-Age + FAS-Combi-Height)/2 [e.g. (PDF)].
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Schellekens, P., Verjans, M., Janssens, P. et al. Low agreement between various eGFR formulae in pediatric and young adult ADPKD patients. Pediatr Nephrol 38, 3043–3053 (2023). https://doi.org/10.1007/s00467-023-05926-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-023-05926-w