
Abstract
Background
Enzymatic methods have recently been used to measure creatinine (Cr) instead of the Jaffe method. Therefore, it is necessary to determine the reference serum Cr value for these enzymatic methods to evaluate renal function in Japanese children.
Methods
To determine reference values of serum Cr in Japanese children, 1151 children (517 male, 634 female) aged between 1 month and 18 years had their serum Cr values measured by an enzymatic method. To be included in the study the children had to be without kidney disease, urogenital disease, infectious disease, inflammatory disease, dehydration, muscular disease, anomaly syndrome, cardiovascular disease, malignant disease, hypertension, liver or pancreas disease, or pregnancy.
Results
The medians of reference values increased gradually with age, i.e., 0.30 mg/dl at 4 years old and 0.41 mg/dl at 10 years old. In adolescence, they increased significantly more rapidly in males than in females. We found a linear regression equation capable of estimating the reference value of serum Cr in children aged 2–11 years, and quintic regression equations capable of estimating the reference values of serum Cr in male and female children of all ages.
Conclusion
The reference serum Cr levels determined by an enzymatic method related to age, gender, and body length, and our linear and polynomial equations showing the relationship between body length and serum Cr level will be applicable for screening of renal function in Asian as well as Japanese children.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Serum creatinine (Cr) levels are generally proportional to muscle mass and inversely proportional to renal function. Therefore, they are lower in infancy, and increase gradually with growth. Schwartz et al. [1] expressed the relationship between body length, glomerular filtration rate (GFR), and serum Cr level as estimated GFR (eGFR; ml/min/1.73 m2) =κ × body length (cm)/serum Cr value (mg/dl). The coefficient κ is 0.33 in preterm infants under 1 year old, 0.45 in full-term infants under 1 year old, 0.55 in children 2–12 years old, and 0.55 and 0.70 in females and males over 12 years old [1–4].
This formula is clinically useful as it allows estimation of the normal serum Cr level from the patient’s body length. This equation utilizes the Jaffe method to measure Cr; however, enzymatic methods have recently been used to measure Cr, making the above formula no longer applicable. In 2009, the updated Schwartz formula was reported as follows: eGFR (ml/min/1.73 m2) = 0.413 × body length (cm)/serum Cr value (mg/dl) by enzymatic Cr determination in children 7.7–14.3 years old [5].
It would be beneficial to obtain a reference serum Cr value by an enzymatic method in Japanese children according to sex and age for renal function evaluation in routine practice. We also attempted to derive a formula to estimate reference serum Cr values in Japanese children as a function of body length, based on the Schwartz formula: i.e., normal serum Cr value (mg/dl) = k × body length (m) in subjects aged 2–11 years, and to derive polynomial formulae to estimate reference serum Cr values as functions of body length in males and females between 1 month and 18 years old.
Materials and methods
A total of 1151 children (517 male and 634 female) between the ages of 1 month and 18 years presenting at the facilities of the members for the Committee of Measures for Pediatric Chronic Kidney Disease (CKD) and Tokyo Health Service Association between 2008 and 2009 were included in the study. The children had to be without kidney disease, urogenital disease, infectious disease, inflammatory disease, dehydration, muscular disease, anomaly syndrome, malignant disease, hypertension, cardiovascular disease, liver or pancreas disease, or pregnancy. The study was approved by the local ethics boards, and written informed consent was obtained from the parents of each subject.
Data regarding serum Cr values and body lengths measured at the same time were reviewed.
With the exception of 1 male and 2 females at the age of 1 month, and 1 male and 1 female at the age of 18 years, the subjects were divided into the following groups based on age: ≥3 to <6 months (n = 18; 16 male, 2 female), ≥ 6 to < 9 months old (n = 19; 15 male, 4 female), ≥ 9 months to <1 year old (n = 31; 17 male, 14 female), 1 year old (n = 70; 33 male, 37 female), 2 years old (n = 73; 40 male, 33 female), 3 years old (n = 88; 48 male, 40 female), 4 years old (n = 81; 43 male, 38 female), 5 years old (n = 96; 47 male, 49 female), 6 years old (n = 102; 43 male, 59 female), 7 years old (n = 85; 38 male, 47 female), 8 years old (n = 56; 18 male, 38 female), 9 years old (n = 36; 18 male, 18 female), 10 years old (n = 44; 12 male, 32 female), 11 years old (n = 58; 19 male, 39 female), 12 years old (n = 69; 15 male, 54 female), 13 years old (n = 68; 30 male, 38 female), 14 years old (n = 57; 17 male, 40 female), 15 years old (n = 37; 15 male, 22 female), and 16 years old (n = 57; 30 male, 27 female). Reference intervals (2.5 percentile and 97.5 percentile) of serum Cr against age were calculated in children between the age of 3 months and 11 years, and against sex and age between 12 and 16 years old. In addition, reference intervals for serum Cr were calculated in children relative to body length every 10 cm. In subjects aged 2–11 years, the relationship between body length and serum Cr level was determined by linear regression analysis according to the report of Uemura [6]. In all subjects, the relationship between body length and serum Cr level was determined by polynomial regression analysis in males and females, respectively. We expressed reference serum Cr level as a quintic equation of body length. In mathematics, a quintic equation is a polynomial equation of degree 5. We chose a quintic equation as a polynomial expression of theoretical changes in serum Cr level with growth in childhood. Age-related changes in serum Cr level have 4 phases with growth where the level decreases gradually up to around 1 year while renal function is developing, increases gradually before puberty while muscle mass is increasing, increases markedly according to the rapid increase in muscle mass in adolescence, and plateaus in adulthood. Therefore, we speculated that there were 4 inflection points in the developmental curve of reference serum Cr level.
Serum samples were stored at −70°C until serum Cr was measured at SRL Inc (Tokyo, Japan). The serum level of Cr was determined by an enzymatic method using a Bio Majesty automated analyzer (JCA-BM8060; JEOL Ltd, Tokyo, Japan) with Pureauto S CRE-L (Sekisui Medical Co., Ltd, Tokyo, Japan). The coefficient of variation was satisfactory (2.08%).
All analyses were conducted using Microsoft Excel 2007 and a statistical software package (JMP 8; SAS Institute Inc, Cary, NC, USA). We conducted linear and polynomial regression analyses to evaluate factors influencing Cr levels. We used Wilcoxon analysis to compare differences in serum Cr levels between the sexes. In all analyses, P < 0.01 was taken to indicate statistical significance.
Results
We examined the correlations between serum Cr concentration and age in all subjects divided according to sex (Fig. 1). Scattergrams showed that reference serum Cr concentrations increased gradually with age, and the increase was more marked in males than females in adolescence. We reviewed the median, 2.5 percentile, and 97.5 percentile of serum Cr reference value in each age group regardless of sex between 3 months and 11 years, because no significant differences were found between males and females in these age groups (Table 1). The median of the reference value increased gradually with age, i.e., 0.30 mg/dl at 4 years old and 0.41 mg/dl at 10 years old. In addition, we reviewed serum Cr reference value equally between 12 and 16 years old in males and females (Table 2). The median reference value in males was almost equal to that in females at the age of 12 years; however, the median reference value in males increased rapidly, and became significantly different from that in females at 16 years old (0.73 mg/dl and 0.59 mg/dl, respectively, P < 0.0001).

Correlations between serum Cr concentration and age in all subjects divided according to sex. These scattergrams show that reference serum Cr concentration gradually increases with age, and the increase is more marked in males than females in adolescence
We reviewed the median, 2.5 percentile, and 97.5 percentile of serum Cr reference values in each body length group in males and females (Table 3). We again found that the median reference values were higher in males than in females >160 cm in body length.
The correlations between serum Cr value and body length were determined in subjects aged 2–11 years. The regression equation was y = 0.34x–0.044, and that passing through the origin was y = 0.30x. A significant positive correlation was observed in 717 children aged 2–11 years, with a correlation coefficient of 0.732 (Fig. 2, P < 0.001).

Correlations between serum Cr values and body length (2–11 years). The regression equation was y = 0.34x–0.044, and that passing through the origin was y = 0.30x. A significant positive correlation was observed in 717 children aged 2–11 years, with a correlation coefficient of 0.732 (P < 0.001)
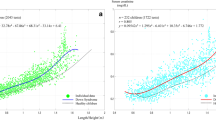
In all subjects, the relationships between body length and serum Cr level were determined by polynomial regression analysis in males and females, and reference serum Cr level was expressed as a quintic equation of body length (Figs. 3, 4). The regression equations were y = –1.259x 5 + 7.815x 4 – 18.57x 3 + 21.39x 2 – 11.71x + 2.628 in 516 males, and y = –4.536x 5 + 27.16x 4 – 63.47x 3 + 72.43x 2 – 40.06x + 8.778 in 630 females. Significant correlations were observed in males with a correlation coefficient of 0.908 (Fig. 3, P < 0.001), and in females with a correlation coefficient of 0.879 (Fig. 4, P < 0.001).

Correlations between serum Cr value and body length (males, 3 months–18 years). A significant correlation between serum Cr value and body length was determined by polynomial regression analysis in males, and reference serum Cr level was expressed as a quintic equation of body length

Correlations between serum Cr value and body length (females, 3 months–18 years). A significant correlation between serum Cr value and body length was determined by polynomial regression analysis in females, and reference serum Cr level was expressed as a quintic equation of body length
Discussion
GFR is used to assess kidney function, and is measured by renal clearance techniques. Inulin clearance is the gold standard for evaluation of kidney function, but cannot be measured easily. Therefore, various methods to determine GFR have been used. One method involves monitoring endogenous Cr clearance, but tubular secretion of Cr can result in overestimation of GFR. The eGFR ((ml/min/1.73 m2) = κ × body length (cm)/serum Cr value (mg/dl)) by the Jaffe method devised by Schwartz [1] has been used clinically. More recently, however, enzymatic methods have been used to measure Cr rather than the Jaffe method, so we cannot use the formula in this form. Therefore, it was necessary to re-evaluate the value of the coefficient κ in the formula. Recently, Zappitelli et al. [7] revised the Schwartz formula relating eGFR to serum Cr level determined enzymatically, and they reported that the κ value in the Schwartz equation decreased from 0.55 to 0.47 for children and adolescent girls. Schwartz reported the updated formula as eGFR = 0.413 × body length (cm)/serum Cr value (mg/dl) by the enzymatic method showing a 25% reduction in κ value from the previous value of 0.55 generated from Jaffe-based serum Cr measurements [5]. Counahan et al. [8] generated a similar formula using ‘near-true’ Cr determination measured by the Jaffe method after removal of non-Cr chromogen with ion-exchange resin, in children of varying ages, and the resulting κ was 0.43.
We have presented the correlations between serum Cr concentration and age by scattergrams in Fig. 1. The results indicated that reference serum Cr concentrations increase gradually with age, and the increase is more marked in males than females in adolescence. This was thought to be because muscle mass increases more rapidly in males than in females. Serum Cr reference values for each age and sex makes it possible for clinical laboratories to determine whether patients have normal renal function or not without the need to obtain height information in pediatric patients. Therefore, we reviewed the median, 2.5 percentile, and 97.5 percentile of serum Cr reference values for each age and sex (Tables 1, 2). We can use 0.30 mg/dl at the age of 4 years and 0.41 mg/dl at the age of 10 years as reference median serum Cr values to investigate renal function in children. The median reference value in males was almost equal to that in females at the age of 12 years; however, the median reference value became higher in males than in females, based on both age and body length, and became significantly higher in males than in females at age 16 years due to sex-related differences in muscle mass in adolescence. Tanaka et al. [9] reported reference intervals of serum Cr value based on an enzymatic method in Japanese children by a latent reference value extraction method. Their reference data were slightly higher than those in the present study, because they could not completely exclude cases with mild renal dysfunction.
When we transform the formula of Schwarz, the normal serum Cr will be proportional to body length: normal serum Cr value (mg/dl) = κ × body length (m). Therefore, we determined the correlation between body length and serum Cr value by an enzymatic method and determined the coefficient k of the regression equation. A significant positive correlation with correlation coefficient > 0.7 was found in Japanese children aged 2–11 years. In addition, the differences in Cr value when we substituted the minimal and the maximal variables of body length in the two types of regression equation, i.e., the conventional equation and the equation passing through the origin were < 0.025 mg/dl in each group. Therefore, we used the regression equation that passed through the origin for all children aged 2–11 years, taking clinical usefulness into account, i.e., body length (m) × 0.30 yielded a value similar to the reference serum Cr level in Japanese children aged 2–11 years. This formula is equivalent to that reported previously in a single-center study in Japanese children aged 1–12 years [6].
In all subjects, the relationship between body length and serum Cr level was determined by polynomial regression analysis separately in males and females, and the reference serum Cr level was expressed as a quintic equation of body length with highly significant correlations. As the reciprocal of serum Cr is generally correlated with GFR [1–5, 8] we could utilize the equation for eGFR derived from serum Cr, eGFR (%) = (reference serum Cr/patient’s serum Cr) × 100. Assuming a GFR with 100% equal to GFR with 120 ml/min/1.73 m2, we derived the equation eGFR (ml/min/1.73 m2) = (reference serum Cr/patient’s serum Cr) × 120. This means that it is likely that the eGFR based on the Schwartz formula will be expressed by the quintic equation instead of a linear equation of body length in Japanese children of all ages. Studies for standardization of inulin clearance in Japanese children and to develop formulae for estimation of GFR are currently underway, but large-scale studies are not possible because of the small numbers of pediatric CKD patients. Therefore, our equations may become a useful tool to support these investigations.
The correlations between age and body length were determined in all subjects and a significant positive correlation was observed with a correlation coefficient of 0.974. Therefore, due to their multicollinearity, we have not analyzed serum Cr by a multiple regression model with age and height as covariants.
Reference serum Cr levels expressed as the median, 2.5 percentile, and 97.5 percentile are useful for pediatricians to determine whether a patient shows normal renal function. Our formula, derived from body length in Japanese children aged 2–11 years, yielded reference serum Cr levels to evaluate renal function in pediatric CKD patients that are simple and easy to use. In addition, our quintic equations, derived from body length in Japanese children of all ages, will be useful to estimate their renal function, despite the complicated formulae, since computerization of medical care simplifies application of these formulae. Since we were unable to validate our equations using a different dataset, our future work will include efforts to validate these equations. Nevertheless, we consider that these reference serum Cr levels will be applicable for screening of renal function in Asian as well as Japanese children; these methods of evaluating renal function in children are available worldwide.
References
Schwartz GJ, Brion LP, Spitzer A. The use of plasma creatinine concentration for estimating glomerular filtration rate in infants, children, and adolescents. Pediatr Clin North Am. 1987;34:571–90.
Schwartz GJ, Feld LG, Langford DJ. A simple estimate of glomerular filtration rate in full-term infants during the first year of life. J Pediatr. 1984;104:849–54.
Schwartz GJ, Haycock GB, Edelmann CM Jr, Spitzer A. A simple estimate of glomerular filtration rate in children derived from body length and plasma creatinine. Pediatrics. 1976;58:259–63.
Schwartz GJ, Gauthier B. A simple estimate of glomerular filtration rate in adolescent boys. J Pediatr. 1985;106:522–6.
Schwartz GJ, Muñoz A, Schneider MF, Mak RH, Kaskel F, Warady BA, Furth SL. New equations to estimate GFR in children with CKD. J Am Soc Nephrol. 2009;20:629–37.
Uemura O, Ushijima K, Nagai T, Yamada T, Hayakawa H, Shinkai Y, Kuwabara M. Reference serum creatinine levels determined by an enzymatic method in Japanese children: relationship to body length. Clin Exp Nephrol. 2009;13:585–8.
Zappitelli M, Parvex P, Joseph L, Paradis G, Grey V, Lau S, Bell L. Derivation and validation of cystatin C-based prediction equations for GFR in children. Am J Kidney Dis. 2006;48:221–30.
Counahan R, Chantler C, Ghazali S, Kirkwood B, Rose F, Barratt TM. Estimation of glomerular filtration rate from plasma creatinine concentration in children. Arch Dis Child. 1976;51:875–8.
Tanaka T, Yamashita A, Ichihara K. Reference intervals of clinical tests in children determined by a latent reference value extraction method. J Jpn Pediatr Soc. 2008;112:1117–32. (in Japanese).
Acknowledgments
This study was financially supported by the Kidney Foundation, Japan. We thank Midori Awazu, MD, Takashi Sekine, MD, Mayumi Sako, MD, Takuji Yamada, MD, Yuko Akioka, MD, and Hirotsugu Kitayama, MD, of the Committee of Measures for Pediatric CKD, for their contributions to the improvement of this manuscript.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Uemura, O., Honda, M., Matsuyama, T. et al. Age, gender, and body length effects on reference serum creatinine levels determined by an enzymatic method in Japanese children: a multicenter study. Clin Exp Nephrol 15, 694–699 (2011). https://doi.org/10.1007/s10157-011-0452-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10157-011-0452-y