
Abstract
Background
The reliability of various equations for estimating the GFR in ADPKD patients and the influence of tolvaptan on the resulting estimates have not been examined when GFR is calculated on the basis of inulin clearance.
Methods
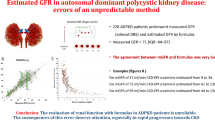
We obtained baseline and on-tolvaptan measured GFRs (mGFRs), calculated on the basis of inulin clearance, in 114 ADPKD, and these mGFRs were compared with eGFRs calculated according to four basic equations: the MDRD, CKD-EPI, and JSN-CKDI equations and the Cockcroft–Gault formula, as well as the influence of tolvaptan and of inclusion of cystatin C on accuracy of the results. Accuracy of each of the seven total equations was evaluated on the basis of the percentage of eGFR values within mGFR ± 30% (P30).
Results
mGFRs were distributed throughout CKD stages 1–5. Regardless of the CKD stage, P30s of the MDRD, CKD-EPI, and JSN-CKDI equations did not differ significantly between baseline values and on-tolvaptan values. In CKD 1–2 patients, P30 of the CKD-EPI equation was 100.0%, whether or not the patient was on-tolvaptan. In CKD 3–5 patients, P30s of the MDRD, CKD-EPI, and JSN-CKDI equations were similar. For all four equations, regression coefficients and intercepts did not differ significantly between baseline and on-tolvaptan values, but accuracy of the Cockcroft–Gault formula was inferior to that of the other three equations. Incorporation of serum cystatin C reduced accuracy.
Conclusions
The CKD-EPI equation is most reliable, regardless of the severity of CKD. Tolvaptain intake has minimal influence and cystatin C incorporation does not improve accuracy.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In patients with autosomal dominant polycystic kidney disease (ADPKD), renal function deteriorates progressively, with end-stage renal failure occurring in approximately 50% of patients by their late 60 s [1,2,3,4]. Hence, monitoring the glomerular filtration rate (GFR) is clinically important in patients with ADPKD. Different equations are used to calculate the so-called measured GFR (mGFR), with the differences lying in the markers of GFR that are incorporated into the equations. 121I-iothalam [5], 99mTc-diethylenetraminepenta-acetic acid [6], and 51Cr-ethylenediaminetetra-acetic acid (Cr-EDTA) [7] are used widely to calculate mGFR [8], but these radioactive tracers are not available in Japan. However, inulin has become commercially available [9]. In routine clinical practice, calculating GFR by measuring any of the usual test substances is troublesome, and there is widespread acceptance of the more convenient estimated GFR (eGFR). However, to date, there has been no reported study of the relation between eGFR and mGFR in Japanese patients with ADPKD.
Orskov et al. used 51Cr-EDTA in 101 Danish patients with ADPKD and reported that the Modification of Diet in Renal Disease (MDRD) Study equation based on the use of cystatin C reflected GFR most accurately [13]. Serum cystatin C is recognized as an alternative to serum creatinine for calculation of the eGFR [11, 12], but serum cystatin C is affected by factors such as age, sex, and race [13], and whether use of cystatin C improves the accuracy of eGFR measurement in, for example, Japanese patients with ADPKD or patients taking tolvaptan needs to be examined.
Tolvaptan is a vasopressin V2-receptor antagonist, and the pivotal clinical trial, the Tolvaptan Efficacy and Safety in Management of Autosomal Dominant Polycystic Kidney Disease and Its Outcomes (TEMPO) 3:4 Study, showed a reduction in the annual percentage increase in total kidney volume (TKV) and a decline in kidney function over 36 months [14]. In 2014, tolvaptan was approved in Japan for treatment of ADPKD. In fact, Japan was the first country in which tolvaptan was approved for ADPKD. To assess the safety and efficacy of tolvaptan, Muto et al. calculated the eGFR using the Japan Society of Nephrology CKD Initiative (JSN-CKDI) equation in a subset of Japanese ADPKD patients from the TEMPO 3:4 trial [15]. However, because the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) modification for Japanese was used in the original TEMPO 3:4 trial [14] and the JSN-CKDI equation was used in the subgroup analysis, concerns have been raised about the accuracy and consistency of the results of subgroup analysis [16]. There has been no reported study conducted to determine which eGFR equation is most reliable or the influence of tolvaptan on the reliability of the equations in patients with ADPKD.
Accuracy of the eGFR varies according to the different stages of CKD in patients with general renal disease unrelated to ADPKD [17]. In 12 studies of general renal diseases in North America, Europe, and Australia, the CKD-EPI equation performed better at higher GFRs (CKD stages 1–2), and the MDRD study equation performed better at lower GFRs (CKD stages 3–5) [18]. Neither the CKD-EPI nor the MDRD study equation was ideal for all patient populations and all ranges of GFR [18]. There has been no reported study that examined which eGFR equation is best or the influence of tolvaptan on the accuracy of equations for estimating GFR in patients with ADPKD.
With these issues in mind, we conducted a study to evaluate relations between mGFR and eGFR as determined by various equations in Japanese patients with ADPKD, both before and at 1 year of tolvaptan administration and per CKD stage.
Methods
Study patients
The study involved 114 patients with ADPKD diagnosed on the basis of the Pei et al. criteria [19]. All were over 20 years of age, and all were seen at our hospital between April 2014 and December 2016 for treatment of ADPKD. CKD had been staged according to the Kidney Disease Outcomes Quality Initiative (K/DOQI) guidelines [20]. TKV was measured by means of volumetric magnetic resonance imaging [21]. This study was retrospective.
Tolvaptan intake and measurement of inulin clearance
Inulin clearance was measured in all 114 patients before the tolvaptan was started and was considered the baseline inulin clearance value. Inulin clearance was measured at 1 year in 85 of the patients; at the time of this measurement, the remaining 29 patients had not yet taken tolvaptan for a full year.
Patients were hospitalized for the measurements of baseline and on-tolvaptan inulin clearance. Inulin solution was prepared by mixing 4 g of inulin (Inulead, 4 g inulin/40 mL, Fuji Pharmaceutical Company, Saitama, Japan) in 500 mL of warmed KN3B solution (NaCl: 0.175 g, KCl: 0.15 g, L-C3H5NaO: 0.224 g, Glucose: 2.7 g/100 mL). The patients drank 300 mL of warm water over 30 min before the clearance study and an additional 150 mL of water every 30 min throughout the clearance study. A total of 540 mL of inulin solution were administered intravenously (by infusion pump) over 150 min at 200 mL/h. A 120 min-urine sample was collected 30 min after the inulin infusion was started. Creatinine and inulin concentrations were measured in the 120 min-urine sample and in serum samples obtained at 35 and 145 min after the inulin infusion was started. Inulin and serum cystatin C were measured by SRL Co. (Tokyo, Japan). Creatinine was measured by the enzymatic method. Both the creatinine and cystatin C measurements were calibrated.
eGFR equations and their assessment
eGFR was calculated by means of four basic equations: the Modification of Diet in Renal Disease (MDRD) study equation with the Japanese coefficient [22,23,24], the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation with a Japanese coefficient [17, 25,26,27], a conversion equation for Japanese determined by the Japan Society of Nephrology CKD Initiative (JSN-CKDI) [24], each with and without the use of standardized serum cystatin C, and the 0.789 × Cockcroft–Gault formula (BSA) [24, 28]. Thus, a total of seven eGFR equations were evaluated (Table 1).
Because the validities of the equations differ according to CKD stage [17, 18], the equations were evaluated separately for the early (stages 1–2) and more advanced (stages 3–5) CKD.
Statistical analysis
Accuracy metrics were applied to each of the equations [24, 29, 30]. Accuracy of the eGFR value derived from each of the equations was expressed as the percentage of cases in which the eGFR fell within ± 30% of the mGFR (P30). Performance of the equations was assessed by measurement of bias, which was calculated as [mGFR–eGFR]. P30 has been reported to be the best index for comparing equations, because it incorporates both bias and precision [18, 31]. Therefore, P30 was the primary index used to judge which equation is best for calculating eGFR, and differences in P30 were analyzed by the McNemar test [32]. Bland–Altman plots were drawn to analyze agreement between mGFR and eGFR.
Mean ± standard deviation (SD) or median values are shown. Differences were analyzed by t test, χ2 test, Mann–Whitney U test, or analysis of variance, as appropriate. All statistical analyses were performed with JMP ver. 10 (SAS Institute Inc., Cary, NC, USA), and a two-sided p value of < 0.05 was regarded as significant.
Results
Clinical characteristics of the 114 patients who underwent baseline measurements of inulin clearance and the 85 patients who underwent on-tolvaptan measurements of inulin clearance are shown in Table 2. The baseline mGFR was 48.8 ± 2.29/min/1.73 m2 and the mean on-tolvaptan mGFR was 45.8 ± 2.66 mL/min/1.73 m2 (p = 0.03). For patients with CKD stage 1–2, the baseline and on-tolvaptan mGFRs were 79.4 ± 2.57 and 77.9 ± 2.86 mL/min/1.73 m2, respectively. For those with CKD stage 3–5, the baseline and on-tolvaptan mGFRs were 36.3 ± 1.46 and 31.6 ± 1.71 mL/min/1.73 m2, respectively. Baseline serum Cr was 1.35 ± 0.07 mg/mL, and the on-tolvaptan concentration was 1.63 ± 0.08 mg/mL. For patients with CKD stage 1–2, baseline serum Cr was 0.83 ± 0.03 mg/mL, and for patients with CKD stage 3–5, baseline serum Cr was 1.56 ± 0.08 mg/mL (p < 0.001). The on-tolvaptan serum Cr concentrations for patients with CKD stage 1–2 and for patients with CKD stage 3–5 were 0.84 ± 0.04 and 1.98 ± 0.09 mg/mL, respectively (p < 0.001). Baseline TKV was 2170 ± 87.3 and on-tolvaptan TKV was 2271 ± 102 mL (p = 0.45). For patients with CKD stage 1–2, baseline and on-tolvaptan TKVs were 1823 ± 159 and 1656 ± 173 mL, respectively (p = 0.12). For patients with CKD stage 3–5, baseline and on-tolvaptan TKVs were 2311 ± 101 and 2517 ± 109 mL, respectively. Overall, serum cystatin C concentrations were 1.29 ± 0.53 mg/L (baseline) and 1.45 ± 0.61 mg/L (on-tolvaptan) (p = 0.04). Systolic blood pressure of patients with CKD stage 1–2 was 124 ± 9 mmHg and that of patients with CKD stage 3–5 was 130 ± 13 mmHg (p = 0.04).
Baseline eGFRs derived from the seven equations are shown in Table 3. Performance of the seven equations per CKD stage is summarized in Table 3a. The MDRD, CKD-EPI, and JSN-CKDI equations (Equations 1. 2, and 3) were shown by P30 to be most accurate, and there was no significant difference between them. Performance of the seven equations in ADPKD patients with an mGFR ≥ 60 mL/min/1.73 m2 (CKD stage 1 or 2) is summarized in Table 3b. The CKD-EPI equation (Eq. 2) was shown by P30 to be most accurate in this group of patients. P30 of Eq. 2 was 100%, and the probabilities of 30% accuracy level between Eq. 2 and other equations could not be calculated. Performance of the seven equations when mGFR was < 60 mL/min/1.73 m2 (CKD stage 3–5) is shown in Table 3c. MDRD, CKD-EPI, and JSN-CKDI equations (Equations 1, 2, and 3) were shown by P30 to be most accurate, with no significant difference in accuracy between them.
The on-tolvaptan mGFRs derived from the seven equations are shown in Table 4. Performance of the seven equations per CKD stage is shown in Table 4a. The MDRD, CKD-EPI, and JSN-CKDI equations (Equations 1, 2, and 3) were most accurate in terms of P30, and there was no significant difference between them. Performance of the seven equations in ADPKD patients with an mGFR ≥ 60 mL/min/1.73 m2 (CKD stages 1 and 2) is summarized in Table 4b. The CKD-EPI equation (Eq. 2) was shown by P30 to be most accurate. P30 of Eq. 2 was 100%, and the probabilities of 30% accuracy level between Eq. 2 and other equations cannot be calculated. Performance of the seven equations when mGFR was < 60 mL/min/1.73 m2 (CKD stages 3–5) is shown in Table 4c. The MDRD, CKD-EPI, and JSN-CKDI equations (Equations 1, 2, and 3) were shown by P30 to be most accurate, and accuracy did not differ significantly between them.
The regression coefficients and intercepts obtained by plotting eGFR derived from each of the seven equations before and after tolvaptan treatment against mGFR are shown in Table 5. The indices did not change with tolvaptan treatment. Correlation between the eGFR values derived from the seven equations and mGFR in all patients regardless of the CKD stage is shown in Fig. 1. Values obtained from Equations 1, 2, and 3 correlated more strongly with mGFR than values obtained from equations that incorporated serum cystatin C (Equations 5, 6, and 7). The equations that incorporated serum cystatin C tended to overestimate GFR. Regardless of which of these three equations (Equations 5, 6, and 7) was used, the on-tolvaptan eGFR was higher than the baseline eGFR, but the differences between baseline eGFRs and on-tolvaptan eGFRs were not significant. Bland–Altman plots of [mGFR–eGFR] are shown in Fig. 2. The difference between mGFR and eGFR was smaller when values were derived from Equations 1, 2, and 3 than when values were derived from Equations 5, 6, and 7, which incorporated serum cystatin C.

Correlation between measured glomerular filtration rate (mGFR) and estimated GFR (eGFR) derived from each equation in all patients (regardless of CKD stage) before tolvaptan treatment and at 1 year of tolvaptan treatment. Blue lines are regression lines for values obtained before tolvaptan treatment (baseline) and red lines are regression lines for values obtained at 1 year of tolvaptan treatment. The black lines indicate equivalence between eGFR and mGFR. The dotted vertical lines indicate 30% error. Equation 1 Modification of Diet in Renal Disease (MDRD) equation, Equation 2 Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation, Equation 3 Japan Society of Nephrology CKD Initiative (JSN-CKDI) equation, Equation 4 0.789 × Cockcroft–Gault formula, Equation 5 MDRD equation with cystatin C, Equation 6 CKD-EPI equation with cystatin C, Equation 7 JSN-CKDI equation with cystatin C

Bland–Altman plots showing measured GFR (mGFR) minus estimated glomerular filtration rate (eGFR) before tolvaptan treatment and at 1 year of tolvapatan treatment. Blue dots represent values obtained before tolvaptan treatment and red dots represent values obtained at 1 year of tolvaptan treatment. Horizontal dashed lines in the center show mean bias, and the upper and lower horizontal dashed lines show mean bias ± 2 SDs. Equation 1 Modification of Diet in Renal Disease (MDRD) equation, Equation 2 Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation, Equation 3 Japan Society of Nephrology CKD Initiative (JSN-CKDI) equation, Equation 4 0.789 × Cockcroft–Gault formula, Equation 5 MDRD equation with cystatin C, Equation 6 CKD-EPI equation with cystatin C, Equation 7 JSN-CKDI equation with cystatin C
Discussion
There has been no reported study comparing the accuracy of different eGFR equations or examining the influence of tolvaptan on these equations when they are compared against mGRF obtained on the basis of inulin clearance in patients with ADPKD and across CKD stages 1–5. In CKD stages 1–5 at baseline, P30s of the MDRD (Eq. 1), CKD-EPI (Eq. 2), and JSN-CKDI (Eq. 3) equations were greater than P30s of the other equations, with no significant difference between these three equations. In CKD stage 1–2 at baseline (n = 33), P30 of the CKD-EPI equation was 100% and significantly better than P30s of the other equations. In CKD stages 3–5 at baseline (n = 81), P30s of the MDRD, CKD-EPI, and JSN-CKDI equations were significantly greater than P30s of the other equations, with no significant difference between them. Similarly, in CKD stages 1–5 on-tolvaptan (n = 85), P30s of the MDRD, CKD-EPI, and JSN-CKDI equations were greater than P30s of the other equations, with no significant difference between the three equations. In CKD stage 1–2 (n = 26), P30 of the CKD-EPI equation was 100% and significantly better than those of the other equations. In CKD stages 3–5 (n = 59), P30s of the MDRD, CKD-EPI, and JSN-CKDI equations were significantly better than those of the other equations, and estimates yielded by each of these three equations did not differ significantly. The influence of GFR on the reliability of eGFR equations reported in CKD patients in general [17, 18, 31, 33] and specifically in patients with ADPKD [10, 36] was also observed in the present study in patients with ADPKD, whether eGFR was determined at baseline or “on-tolvaptan”.
In the 12 studies of general renal diseases in North America, Europe, and Australia, the CKD-EPI equation performed better at high GFRs (CKD stages 1–2), and the MDRD equation performed better at lower GFRs [18]. Neither the CKD-EPI nor the MDRD equation was optimal for all populations and GFR ranges [17, 18, 31]. Spithoven et al. compared the CKD-EPI and MDRD equations using 125I-iothalamine clearance in Dutch ADPKD patients [36]. They found that the two equations performed similarly. In contrast, we showed that the CKD-EPI equation was most accurate for patients with stage 1–2 CKD and that the MDRD, CKD-EPI, and JSN-CKDI equations were more accurate for patients with stage 3–5 CKD. It is possible that the discrepancy between our findings and those Spithoven et al. is the result of differences in ethnic characteristics of the study patients, distribution of the GFR in the populations studied, or the substance used to measure mGFR. The Consortium for Radiologic Imaging Studies of Polycystic Kidney Disease (CRISP) requires more accurate eGFR in cases in which previously stable renal function has worsened [37]; thus, it is particularly important to assess the validity of eGFR in patients with stage 3–5 CKD.
The proportion of study participants with CKD stages 1–2 and CKD stages 3–5 differed between the Orskov et al. study [10] and ours. Patients with CKD stages 1–2 accounted for 59.5% of the total patients in the Orskov et al. study [10], but only 28.9 and 30.6% of patients in whom respective baseline and on-tolvaptan measurements were obtained in our study. Therefore, the results of CKD stages 1–2 were strongly reflected in the results of CKD stages 1–5 in the Orskov et al. study, whereas the results of CKD stages 3–5 were emphasized in our study. By examining values according to CKD stage, however, we found that values obtained from the CKD-EPI equation were most consistent with mGFRs, regardless of the CKD stage. In daily practice, mGFR cannot be determined quickly, and patients cannot be stratified according to CKD stage without testing for inulin clearance. Regardless of the CKD stage, the CKD-EPI equation yields the most reliable eGFR, and tolvaptan does not appear to affect the reliability of this equation. This is new and very useful information. The greater on-tolvapatan (vs. baseline) P30 obtained from each eGFR equation (Tables 3, 4) can be explained by the fact that tolvaptan increases urine volume and thus decreases error in measurement of this volume. The serum Cr concentration is in fact influenced by non-renal factors such muscle mass, exercise, and dietary intake [34]. To avoid the influence of non-renal factors on eGFR, serum cystatin C is used in the MDRD and CKD-EPI equations [26]. Serum cystatin C is freely filtered by the glomeruli, reabsorbed in the proximal tubules, and metabolized to amino acids; thus, it does not return to the blood. For these reasons, cystatin C is incorporated into the eGFR equation to compensate for the limitation of serum Cr [35]. However, the performance of serum cystatin C in estimating GFR was, in one study, shown to be reduced in patients with a low GFR [12]. In addition, cystatin C was shown to be affected by factors other than GFR, such as, age, sex, race, drugs, and disease status [13]. Drugs that have an effect on blood cystatin C include cyclosporine and corticosteroids. Cyclosporin A has been reported to decrease the concentration of serum cystatin C [38]. Corticosteroids have been reported to increase cystatin C production in vitro [39, 40], while in vivo, it has been reported to elevate serum cystatin C concentration markedly [38], or not to have any effect at all [41], thus, results of past studies have not been consistent. Cystatin C might be differently metabolized in ADPKD patients because of renal tubular impairment caused by enlarged cysts.
Orskov et al. compared the CKD-EPI and MDRD equations with use of serum cystatin C and the Cockcroft–Gault equations (BSA) using 51Cr-EDTA in Danish ADPKD patients without taking tolvaptan [10]. Their results showed that the MDRD study equation with cystatin C use was the most consistent with mGFR in CKD stages 1–5. In contrast to the supportive results for serum cystatin C [10], our results showed that use of serum cystatin C in three eGFR equations resulted in over-estimation. The possible reasons for the differences between the two studies may be explained by the difference in ethnic characteristics including body size and metabolic characteristics, the difference in GFR distribution among the study population, and/or difference in the substance used to measure GFR. The mechanisms are speculative and need further study. Last year, cystatin C-eGFR but not creatinine-eGFR was demonstrated to correlate with height-adjusted TKV (ht-TKV) in the early stages of ADPKD, indicating the potential usefulness of cystatin C-eGFR as an early marker of disease progression [42]. Going forward, we are intestigating the relationships between cystatin C-eGFR and mGFR by ht-TKV levels.
The limitations of this study was that the study was retrospective and conducted at a single facility, with relatively small number of patients.
To summarize the results of the present study, the CKD-EPI is the most consistent for estimation of GFR in patients with ADPKD. The reasons for this recommendation are as follows: (1) in daily outpatient department, we cannot know mGFR quickly without inulin clearance and the distribution of patient’s GFRs is various. Therefore, it is reasonable that the CKD-EPI is the most consistent at the point that the CKD-EPI is immune to various patterns of GFR distribution in ADPKD patients. (2) The CKD-EPI was optimal in all GFR ranges of ADPKD patients at baseline and on-tolvaptan. (3) The JSN-CKDI equation estimates GFR almost equally with the CKD-EPI and MDRD at stages 3–5. However, the CKD-EPI equation with a Japanese coefficient is widely used in Japan, and the CKD-EPI equation is used across the world and the results obtained using the same equation can be compared. (4) Equations with use of serum cystatin C were inferior to the CKD-EPI equation without use of cystatin C in ADPKD.
Conclusion
The results suggest that the CKD-EPI equation is the most consistent for estimation of GFR in patients with ADPKD throughout all CKD stages. Tolvaptan intake does not affect and cystatin C incorporation does not improve the accuracy of equations.
References
Milutinovic J, Fialkow PJ, Agodoa LY, et al. Autosomal dominant polycystic kidney disease: symptoms and clinical findings. Q J Med. 1984;53:511–22.
Churchill DN, Bear JC, Morgan J, et al. Prognosis of adult onset polycystic kidney disease re-evaluated. Kidney Int. 1984;26:190–3.
Gabow PA, Johnson AM, Kaehny WD, et al. Factors affecting the progression of renal disease in autosomal-dominant polycystic kidney disease. Kidney Int. 1992;41:1311–9.
Higashihara E, Nutahara K, Kojima M, et al. Prevalence and renal prognosis of diagnosed autosomal dominant polycystic kidney disease in Japan. Nephron. 1998;80:421–7.
Kopple JD, Greene T, Chumlea WC, et al. Relationship between nutritional status and the glomerular filtration rate: results from the MDRD study. Kidney Int. 2000;57:1688–703.
Carlsen JE, Møller ML, Lund JO, et al. Comparison of four commercial Tc-99m(Sn)DTPA preparations used for the measurement of glomerular filtration rate: concise communication. J Nucl Med. 1980;21:126–9.
Garnett ES, Parsons V, Veall N. Measurement of glomerular filtration-rate in man using a 51Cr-edetic-acid complex. Lancet. 1967;15:818–9.
Yanai M. Measurement of glomerular filtration rate and its estimation equation. Mod Media. 2013;59:155–60.
Horio M, Imai E, Yasuda Y, et al. Japanese equation for estimating GFR: Simple sampling strategy for measuring inulin renal clearance. Clin Exp Nephrol. 2009;13:50–4.
Orskov B, Borresen ML, Feldt-Rasmussen B, et al. Estimating glomerular filtration rate using the new CKD-EPI equation and other equations in patients with autosomal dominant polycystic kidney disease. Am J Nephrol. 2010;31:53–7.
Dharnidharka VR, Kwon C, Stevens G. Serum cystatin C is superior to serum creatinine as a marker of kidney function: a meta-analysis. Am J Kidney Dis. 2002;40:221–6.
Horio M, Imai E, Yasuda Y, et al. Performance of serum cystatin C versus serum creatinine as a marker of glomerular filtration rate as measured by inulin renal clearance. Clin Exp Nephrol. 2011;15:868 – 76.
Stevens LA, Schmid CH, Greene T, et al. Factors other than glomerular filtration rate affect serum cystatin C levels. Kidney Int. 2009;75:652–60.
Torres VE, Chapman AB, Devuyst O, et al. TEMPO 3:4 trial investigators: tolvaptan in patients with autosomal dominant polycystic kidney disease. N Engl J Med. 2012;367:2407–18.
Muto S, Kawano H, Higashihara E, et al. The effect of tolvaptan on autosomal dominant polycystic kidney disease patients: a subgroup analysis of the Japanese patient subset from TEMPO 3:4 trial. Clin Exp Nephrol. 2015;19:867–77.
Kawada T. The effect of tolvaptan on kidney function in patients with autosomal dominant polycystic kidney disease. Clin Exp Nephrol. 2016;20:147–48.
Levey AS, Stevens LA, Schmid CH, et al. CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration): a new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150:604–12.
Earley A, Miskulin D, Lamb EJ, et al. Estimating equations for glomerular filtration Rate in the era of creatinine standardization: a systematic review. Ann Intern Med. 2012;156:785–95.
Pei Y, Obaji J, Dupuis A, Paterson AD, et al. Unified criteria for ultrasonographic diagnosis of ADPKD. J Am Soc Nephrol. 2009;20:205–12.
http://www.kidney.org/professionals/kdoqi/guidelines_ckd/p4_class_gl.htm.2009. Retrieved on Sept 2015.
Higashihara E, Nutahara K, Okegawa T, et al. Kidney volume and function in autosomal dominant polycystic kidney disease. Clin Exp Nephrol. 2014;18:157–65.
Levey AS, Bosch JP, Lewis JB, et al. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of diet in renal disease study group. Ann Intern Med. 1999;130:461–70.
Levey AS, Greene T, Kusek J, et al. A simplified equation to predict glomerular filtration rate from serum creatinine. J Am Soc Nephrol. 2000;11:155A.
Matsuo S, Imai E, Horio M, et al. Collaborators developing the Japanese equation for estimated GFR. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009;53:982–92.
Horio M, Imai E, Yasuda Y, et al. Modification of the CKD epidemiology collaboration (CKD-EPI) equation for Japanese: accuracy and use for population estimates. Am J Kidney Dis 2010;56:32–8.
Inker LA, Schmid CH, Tighiouart H, CKD-EPI Investigators, et al. Estimating glomerular filtration rate from serum creatinine and cystatin C. N Engl J Med. 2012;367:20–9.
Horio M, Imai E, Yasuda Y, et al. Collaborators developing the Japanese equation for estimated GFR: GFR estimation using standardized serum cystatin C in Japan. Am J Kidney Dis. 2013;61:197–203.
Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron. 1976;16:31–41.
Klahr S, Levey AS, Beck GJ, et al. The effects of dietary protein restriction and blood-pressure control on the progression of chronic renal disease. Modification of Diet in Renal Disease Study Group. N Engl J Med. 1994;330:877–84.
Stevens LA, Coresh J, Greene T, et al. Assessing kidney function-measured and estimated glomerular filtration rate. N Engl J Med. 2006;354:2473–83.
Shen C, Landsittel D, Irazabal MV, et al. CRISP Investigators: Performance of the CKD-EPI equation to estimate GFR in a longitudinal study of autosomal dominant polycystic kidney disease. Am J Kidney Dis 2017;69:482–4.
McNemar Q. Note on the sampling error of the difference between correlated proportions or percentages. Psychometrika. 1947;12:153–7.
Michels WM, Grootendorst DC, Verduijn M, et al. Performance of the Cockcroft–Gault, MDRD, and new CKD-EPI formulas in relation to GFR, age, and body size. Clin J am Soc Nephrol. 2010;5:1003–9.
Ma YC, Zuo L, Chen JH, et al. Modified glomerular filtration rate estimating equation for Chinese patients with chronic kidney disease. J Am Soc Nephrol. 2006;17:2937–44.
Donadio C. Serum and urinary markers of early impairment of GFR in chronic kidney disease patients: diagnostic accuracy of urinary β-trace protein. Am J Physiol Renal Physiol. 2010;299:407–23.
Spithoven EM, Meijer E, Boertien WE, et al. Tubular secretion of creatinine in autosomal dominant polycystic kidney disease: consequences for cross-sectional and longitudinal performance of kidney function estimating equations. Am J Kid Dis. 2013;62:531–40.
Chapman AB, Guay-Woodford LM, Grantham JJ, et al. Consortium for Radiologic Imaging Studies of Polycystic Kidney Disease cohort. Renal structure in early autosomal-dominant polycystic kidney disease (ADPKD): the Consortium for Radiologic Imaging Studies of Polycystic Kidney Disease (CRISP) cohort. Kidney Int. 2003;64:1035–45.
Cimerman N, Brguljan PM, Krasovec M, et al. Serum cystatin C, a potent inhibitor of cysteine proteinases, is elevated in asthmatic patients. Clin Chim Acta. 2000;300:83–95.
Bjarnadóttir M, Grubb A, Olafsson I. Promoter-mediated, dexamethasone-induced increase in cystatin C production by HeLa cells. Scand J Clin Lab Invest. 1995;55:617–23.
Walser M. Assessing renal function from creatinine measurements in adults with chronic renal failure. Am J Kidney Dis 1998;32:23–31.
Kazama JJ, Kutsuwada K, Ataka K, et al. Serum cystatin C reliably detects renal dysfunction in patients with various renal diseases. Nephron. 2002;91:13–20.
Sans L, Radosevic A, Quintian C, et al. Cystatin C estimated glomerular filtration rate to assess renal function in early stages of autosomal dominant polycystic kidney disease. PLOS One. 2017;12:e0174583.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared that no conflict of interest exists.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee at which this studies were conducted and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Ethics Committee approval has been obtained (Approval number 482).
Informed consent
Informed consent was obtained from all individual participants included in the study.
About this article

Cite this article
Yamaguchi, T., Higashihara, E., Okegawa, T. et al. Optimal equation for estimation of glomerular filtration rate in autosomal dominant polycystic kidney disease: influence of tolvaptan. Clin Exp Nephrol 22, 1213–1223 (2018). https://doi.org/10.1007/s10157-018-1574-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10157-018-1574-2