
Abstract
Objective
The cause and mechanism of epilepsy after endoscopic third ventriculostomy (ETV) have still remained elusive. This single-center study aimed to explore and analyze the risk factors of post-operative seizure in pediatric patients with hydrocephalus undergoing ETV.
Methods
Data of pediatric patients with hydrocephalus who were treated with ETV from October 1, 2015, to November 31, 2021, were retrospectively analyzed. Basic demographic characteristics, etiology of hydrocephalus, surgical details, and laboratory measurements were collected. An early postoperative seizure was defined as the occurrence of at least one clinical seizure within 24 h of ETV.
Results
A total of 50 participants were included in the study, of whom 5 (10.00%) cases were in postoperative epilepsy group and 45 (90.00%) cases were in non-epilepsy group. Epilepsy patients were younger than those without epilepsy, while no statistically significant difference was found (P = 0.0836). In the age subgroup, children with epilepsy were younger than 2 years old. All patients with epilepsy received Ringer’s solution intraoperatively. The mean postoperative serum calcium and potassium concentrations were significantly lower in patients with epilepsy than in those without epilepsy (Pcalcium = 0.0429; Ppotassium = 0.0250). Moreover, a faster decrease of serum potassium and calcium levels was found in children with epilepsy compared with those without epilepsy after ETV.
Conclusion
The decrease of serum calcium and potassium levels, younger age, and using Ringer’s solution as irrigation fluid were risk factors for epilepsy after ETV.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The prevalence of hydrocephalus in infants was reported to be 0.82–1.1 per 1000 live births [1, 2]. Etiology of hydrocephalus included aqueduct stenosis, suprasellar arachnoid cyst, hemorrhage (due to prematurity and other causes), cerebrospinal fluid (CSF), infections (meningitis/ventriculitis/encephalitis), cancer (all types), dysraphism, and congenital malformation. Initial treatment of hydrocephalus mainly included Ommaya reservoir placement, shunt placement, and endoscopic third ventriculostomy (ETV) (e.g., temporary external drains/serial lumbar punctures) [3]. For children with pure communicating hydrocephalus, the success rate was 60% in CSF shunting and 67% in ETV at the last visit [4]. For patients with non-communicating hydrocephalus, a meta-analysis reported that there was no significant difference in symptom improvement between ETV and ventriculoperitoneal shunting; however, ETV was associated with a lower incidence of major complications compared with ventriculoperitoneal shunting [5]. As an effective method for the treatment of hydrocephalus, the safety of ETV has been verified in children; however, Bowes et al. identified 9 different complications related to neuroendoscopic surgery in 286 pediatric patients, including postoperative seizures (1.7%) [6]. Barkley et al. reported 60 (out of 81) cases with hydrocephalus who underwent ETV, in which early and late post-operative seizures occurred in 6.7% and 8.3% of cases, respectively [7]. Another study found that 24% of hydrocephalus children who underwent ETV developed clinical seizures within 24 h after surgery [8]. The cause and mechanism of epilepsy after ETV have still remained elusive. The present single-center study aimed to explore and analyze the risk factors of post-operative seizure in pediatric patients with hydrocephalus undergoing ETV using patients’ clinical records.
Methods
Study design and participants
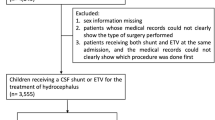
A retrospective study was performed on patients’ electronic medical records at a single medical institution, and the study protocol was approved by the Ethics Committee of Xuanwu Hospital Affiliated to Capital Medical University (Beijing, China). Pediatric patients’ data who were diagnosed with hydrocephalus and treated with ETV from October 1, 2015, to November 31, 2021, were retrospectively reviewed. Data included the medical history, clinical manifestations, physical examination results, imaging findings, surgical videos and records, pathological reports, and clinical notes. The inclusion criteria were as follows: (1) age < 18 years old; (2) hydrocephalus confirmed by neuroimaging; (3) without undergoing ventriculoperitoneal shunting before ETV; (4) without undergoing ventriculoperitoneal shunting within 7-day post-ETV; (5) no history of seizure disorders; (6) undergoing at least 4 months of follow-up after ETV. For patients with less than 4 months of documented follow-up, while more than 4 months passed from the date of undergoing ETV, phone interview was implemented.
Data collection
Relevant data were extracted, including age, sex, body mass index (BMI), blood type, nationality, etiology of hydrocephalus, operation time, entry side, the type of irrigation fluid and endoscope used during surgery, laboratory measurements, and records of early postoperative seizures. Of note, an early postoperative seizure was defined as the occurrence of at least one clinical seizure within 24 h of ETV.
Laboratory measurements
Venous blood samples were collected within 12 h before undergoing laboratory measurements. Postoperative laboratory measurements of venous blood samples, which were collected within 24 h after ETV or immediately collected after the onset of epilepsy, were also conducted. The collection of blood samples was performed in the Central Laboratory of Xuanwu Hospital. Laboratory measurements included the levels of calcium, phosphorus, chlorine, sodium, potassium, albumin, and blood glucose.
Statistical analysis
Continuous variables were described as mean ± standard deviation (SD), and categorical variables were expressed as number and percentage. The Wilcoxon test was utilized for comparison of non-parametric variables, and the Fisher’s exact test was used for comparing categorical variables. Missing values in laboratory measurements were not included in the statistical analysis. A two-tailed P < 0.05 was considered statistically significant. The statistical analysis and illustration of figures were carried out by R 4.1.2 software (http://R-project.org/).
Results
In total, 50 participants were included in the study, of whom 5 (10.00%) cases were in postoperative epilepsy group and 45 (90.00%) cases were in non-epilepsy group. Besides, 31 (62.00%) cases were male and 19 (38.00%) cases were female. The participants’ mean age was 6.6 years old. The most common etiologies of hydrocephalus were tumor-related obstructive hydrocephalus and midbrain aqueduct stenosis (Fig. 1).

Etiology of hydrocephalus
Participants’ baseline characteristics are presented in Table 1. Cases in the epilepsy group were younger than those in the non-epilepsy group, while no significant difference was found (P = 0.0836). In the age subgroup, children with epilepsy were younger than 2 years old (Fig. 4). All patients with epilepsy received Ringer’s solution intraoperatively, while 86.67% of cases without epilepsy received Ringer’s solution (Fig. 3).
The mean postoperative serum calcium and potassium levels in the epilepsy group were significantly lower than those in the non-epilepsy group (Pcalcium = 0.0429; Ppotassium = 0.0250). Moreover, a faster decrease of serum potassium and calcium levels was found in children with epilepsy compared with those without epilepsy after ETV (Table 2, Fig. 2).

The changes in laboratory measurements before and after surgery in epileptic and non-epileptic participants. a The level of albumin (g/L); b the level of chlorine (mmol/L); c the level of calcium (mmol/L); d the level of phosphorus (mmol/L); e the level of blood glucose (mmol/L); f the level of potassium (mmol/L); g the level of sodium (mmol/L)
Discussion
The cortical ETV entry site is 1 cm in front of the left/right coronal suture and 2.5–3 cm beside the midline, which is the non-eloquent area without important vessels. The surgical procedures followed the protocol in the present study.
The serum calcium and potassium levels before and after surgery significantly differed with the occurrence of epilepsy (Table 2). Although the type of irrigation fluid and the occurrence of epilepsy could not be statistically analyzed, it was revealed that epilepsy occurred in children irrigated with Ringer’s solution, while no seizure was found with injection of normal saline.
All children with epilepsy received Ringer’s solution as irrigation fluid intraoperatively (Fig. 3), which might be related to changing the concentrations of calcium and potassium ions in CSF [9,10,11]. A previous study reported that Ca2+ level in CSF was higher in patients with neonatal-onset epilepsy [12], which was consistent with our finding. Another study demonstrated that perfusion of the inferior horn in chronic awake cats with a high potassium level in CSF revealed that K+ increased epileptogenic excitability [13]. This result also supported our speculation that Ringer’s solution is a compound sodium chloride solution, containing potassium and calcium, and potassium and calcium concentrations increased in CSF. Compared with older children, younger children may have insufficient calcium and potassium metabolism, and identification of these children is particularly important.

Number of epileptic and non-epileptic participants in different irrigation fluid-based groups
Our study showed that the changes in serum potassium and blood calcium levels were related to the occurrence of seizures. The possible mechanism was that surgery changes the permeability of blood-brain barrier (BBB), making some ions easier to pass through the BBB, and the imbalance of serum calcium and potassium levels leads to the imbalance of calcium and potassium levels in neurons, resulting in epilepsy [14, 15]. In addition, intraoperative administration of irrigation fluid can change the ion concentration in CSF, because there is an increase in the permeability of BBB, making some ions more likely to pass through the BBB and may lead to epilepsy.
The incidence of immediate postoperative epilepsy in this group of cases was 10%; it was 8.3% in children younger than 1 years old, followed by 40% in children aging 1–2 years old, and 22.7% in children younger than 2 years old (Fig. 4). Children younger than 2 years old in the present study were more likely to develop postoperative seizures and all received the Ringer’s solution. In particular, children who aged 1–2 years old had the highest rate of epilepsy, while children older than 2 years old did not have epilepsy. According to the literature, the incidence of epilepsy was higher in the youngest age-based group, with an estimate of 86 per 100,000 children per year in the first year of age, followed by a downward trend to about 23–31 per 100,000 people who aged 30–59 years old. In children, the incidence of epilepsy was the highest in the first year of life and declined to adults’ incidence at the age of 10 years old [16]. Another study reported that the incidence was markedly higher in the first year of life, and structural/metabolic etiologies were more likely to present at this age than in older individuals, which might explain the higher incidence [17]. The present study also reflected this age-related susceptibility phenomenon.

Number of epileptic and non-epileptic participants in different age-based groups
Status epilepticus (SE) is an epileptic seizure that is sufficiently prolonged or repeated at sufficiently brief intervals, so as to produce an enduring epileptic condition. SE may have long-term consequences, including neuronal injury or death and alteration of neuronal networks, depending on the type and duration of seizures [16]. In our study, 2 patients developed SE. Only strong sedative drugs can control the seizures. However, all patients showed frequent seizures within 6 h after surgery and seizures did not appear again after 24 h, which also indirectly reflected the promoting effect of the surgery itself on seizures, especially with the circulation of CSF, and irrigation fluid was partly removed from the CSF intraoperatively.
The outer diameter of the sheath of the rigid endoscope was 4 mm, while the outer diameter of the working channel of the flexible endoscope was 9 mm, which both slightly damaged to the cortex. The present study showed that the incidence of epilepsy caused by both a rigid endoscope and a flexible endoscope was not statistically significant.
In a child with no seizure after ETV, ventriculoperitoneal shunting was performed 3 weeks after the first surgery, and epilepsy occurred at 4 years of follow-up, which might be associated with shunt surgery, and a meta-analysis reported that the risk of acquiring seizures/epilepsy in shunted non-infectious hydrocephalus children was 15.75 times higher than that in normal children [18]. A randomized controlled trial compared the anterior and posterior shunt entry sites, and found no significant difference in the incidence rate of new-onset epilepsy [19], which could be related to cortical injury and long-term stimulation of the shunt as a foreign body, indicating that cortical disruption or irritation from the shunt catheter itself may contribute to post-shunt seizure development. The child has been well-controlled by antiepileptic treatment.
Epileptic seizures are dangerous from a medical point of view, in which with increasing cerebral oxygen consumption, intracranial pressure and trauma could be enhanced [20]. At present, there are several antiepileptic drugs (AEDs), while few of them can be used for infants. Levetiracetam was previously recommended as a perioperative prophylactic antiepileptic medication, and there are also some researches on the administration of levetiracetam for infants with epilepsy [21,22,23]. Levetiracetam possesses an excellent oral bioavailability and a very low-protein binding, with unknown significant pharmacokinetic interactions. There is no hepatic metabolism; 66% is excreted in urine as constant form and the rest is hydrolyzed as inactive compounds. Therefore, it is not affected by other drugs and does not influence the functions of the liver and kidney. Levetiracetam is a broad-spectrum drug, which is effective against focal seizures, generalized tonic-clonic seizures, and generalized myoclonic seizures. Levetiracetam has demonstrated class I evidence of efficacy as an adjunctive therapy for refractory generalized myoclonic seizures, and is the only AED with FDA approval for treatment of such type of seizures [21, 24, 25]. It is recommended for young children receiving a loading dose of levetiracetam (20 mg/kg) at the start of surgery and a maintenance dose (10 mg/kg twice per 1 day) for the following 7 days [8]. In a previous study, a patient’s age was found as an influential factor of the success rate of ETV, and younger patients tended to undergo additional surgery after failure of ETV [4]. As the reduction of postoperative serum potassium and calcium levels was found as a risk factor for epilepsy, the changes in serum calcium and serum potassium levels should be monitored before, during, and after surgery. For children with a downward trend of serum calcium and serum potassium levels, timely potassium and calcium supplementation during and after surgery may also reduce the incidence of epilepsy.
There are some limitations in the present study. Firstly, this was a retrospective study, and epilepsy was depended on documented seizures without routine postoperative detection using electroencephalogram. Secondly, due to the small sample size, the confounding factors were not excluded, which could limit the generalizability of our findings. Finally, no causal relationship between postoperative epilepsy and serum ion level was identified because the levels of potassium and calcium were not assessed before the epilepsy onset.
Conclusions
In summary, after analyzing several factors, it was revealed that the decrease of serum calcium and potassium levels, younger age, and using Ringer’s solution as irrigation fluid were risk factors for epilepsy after ETV. It is recommended to apply normal saline as irrigation fluid for ETV of younger children, especially for children younger than 2 years old, and the changes of electrolyte should also be monitored during and after surgery. For children with an obvious downward trend of serum calcium and potassium levels, calcium and potassium should be timely supplemented. Besides, the use of AEDs is recommended to avoid the risk of epilepsy.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Code availability
Not applicable.
References
Persson EK, Hagberg G, Uvebrant P (2005) Hydrocephalus prevalence and outcome in a population-based cohort of children born in 1989–1998. Acta Paediatr 94(6):726–732
Tully HM, Dobyns WB (2014) Infantile hydrocephalus: a review of epidemiology, classification and causes. Eur J Med Genet 57(8):359–368
Holwerda JC, van Lindert EJ, Buis DR, Hoving EW, Dutch Pediatric Neurosurgery Study Group (2020) Surgical intervention for hydrocephalus in infancy; etiology, age and treatment data in a Dutch cohort. Childs Nerv Syst 36(3):577–582
Usami K, Ishisaka E, Ogiwara H (2021) Endoscopic third ventriculostomy and cerebrospinal fluid shunting for pure communicating hydrocephalus in children. Childs Nerv Syst 37(9):2813–2819
Jiang L, Gao G, Zhou Y (2018) Endoscopic third ventriculostomy and ventriculoperitoneal shunt for patients with noncommunicating hydrocephalus: a PRISMA-compliant meta-analysis. Medicine (Baltimore) 97(42):e12139
Bowes AL, King-Robson J, Dawes WJ, James G, Aquilina K (2017) Neuroendoscopic surgery in children: does age at intervention influence safety and efficacy? A single-center experience. J Neurosurg Pediatr 20(4):324–328
Barkley AS, Boop S, Barber JK, Lee A, Browd SR, Ojemann JG, Ellenbogen RG, Hauptman JS (2021) Post-operative seizure after first time endoscopic third ventriculostomy in pediatric patients. Childs Nerv Syst 37(6):1871–1875
Barnett RR, Harbert AL, Pajer HB, Wabulya A, Jewells VL, Elton SW, Quinsey CS (2021) Postoperative seizures following endoscopic third ventriculostomy and choroid plexus cauterization: a case series. J Neurosurg Pediatr 29:1–7
Moody WJ, Futamachi KJ, Prince DA (1974) Extracellular potassium activity during epileptogenesis. Exp Neurol 42(2):248–263
Formenti A, De Simoni A, Arrigoni E, Martina M (2001) Changes in extracellular Ca2+ can affect the pattern of discharge in rat thalamic neurons. J Physiol 535(Pt 1):33–45
Kadala A, Verdier D, Morquette P, Kolta A (2015) Ion homeostasis in rhythmogenesis: the interplay between neurons and astroglia. Physiology (Bethesda) 30(5):371–388
Casas-Alba D, Oliva C, Salgado MDC, Codina A, Agut T, García-Alix A, Garcia-Puig M, García-Cazorla À, Taglialatela M, Jou C, Artuch R, Fons C (2022) Cerebrospinal fluid ion analysis in neonatal seizures. Pediatr Neurol 128:16–19
Zuckermann EC, Glaser GH (1970) Slow potential shifts in dorsal hippocampus during “epileptogenic” perfusion of the inferior horn with high-potassium CSF. Electroencephalogr Clin Neurophysiol 28(3):236–246
van Vliet EA, Aronica E, Gorter JA (2015) Blood-brain barrier dysfunction, seizures and epilepsy. Semin Cell Dev Biol 38:26–34
Löscher W, Friedman A (2020) Structural, molecular, and functional alterations of the blood-brain barrier during epileptogenesis and epilepsy: a cause, consequence, or both? Int J Mol Sci 21(2):591
Beghi E (2020) The epidemiology of epilepsy. Neuroepidemiology 54(2):185–191
Wirrell EC, Grossardt BR, Wong-Kisiel LC, Nickels KC (2011) Incidence and classification of new-onset epilepsy and epilepsy syndromes in children in Olmsted County, Minnesota from 1980 to 2004: a population-based study. Epilepsy Res 95(1–2):110–118
Sobana M, Halim D, Aviani JK, Gamayani U, Achmad TH (2021) Neurodevelopmental outcomes after ventriculoperitoneal shunt placement in children with non-infectious hydrocephalus: a meta-analysis. Childs Nerv Syst 37(4):1055–1065
Whitehead WE, Riva-Cambrin J, Wellons JC, Kulkarni AV, Limbrick DD, Wall VL, Rozzelle CJ, Hankinson TC, McDonald PJ, Krieger MD, Pollack IF, Tamber MS, Pindrik J, Hauptman JS, Naftel RP, Shannon CN, Chu J, Jackson EM, Browd SR, Simon TD, Holubkov R, Reeder RW, Jensen H, Koschnitzky JE, Gross P, Drake JM, Kestle JRW (2021) Anterior versus posterior entry site for ventriculoperitoneal shunt insertion: a randomized controlled trial by the Hydrocephalus Clinical Research Network. J Neurosurg Pediatr 19:1–11
Elger CE, Schmidt D (2008) Modern management of epilepsy: a practical approach. Epilepsy Behav 12(4):501–539
Sharpe C, Reiner GE, Davis SL, Nespeca M, Gold JJ, Rasmussen M, Kuperman R, Harbert MJ, Michelson D, Joe P, Wang S, Rismanchi N, Le NM, Mower A, Kim J, Battin MR, Lane B, Honold J, Knodel E, Arnell K, Bridge R, Lee L, Ernstrom K, Raman R, Haas RH, NEOLEV2 INVESTIGATORS (2020) Levetiracetam versus phenobarbital for neonatal seizures: a randomized controlled trial. Pediatrics 145(6):e20193
Qiao MY, Cui HT, Zhao LZ, Miao JK, Chen QX (2021) Efficacy and safety of levetiracetam vs. phenobarbital for neonatal seizures: a systematic review and meta-analysis. Front Neurol 12:747745
Liu BK, Jiang L, Li XJ, Hong SQ, Chen W, Hu Y (2020) Efficacy and safety of levetiracetam in the off-label treatment of neonatal seizures. Int J Neurosci 130(4):336–342
Abou-Khalil BW (2019) Update on antiepileptic drugs 2019. Continuum (Minneap Minn) 25(2):508–536
Chamberlain JM, Kapur J, Shinnar S, Elm J, Holsti M, Babcock L, Rogers A, Barsan W, Cloyd J, Lowenstein D, Bleck TP, Conwit R, Meinzer C, Cock H, Fountain NB, Underwood E, Connor JT, Silbergleit R, Neurological emergencies treatment trials, pediatric emergency care applied research network investigators (2020) Efficacy of levetiracetam, fosphenytoin, and valproate for established status epilepticus by age group (ESETT): a double-blind, responsive-adaptive, randomised controlled trial. Lancet 395(10231):1217-1224
Author information
Authors and Affiliations
Contributions
PS: conceptualization, methodology, investigation, writing original draft preparation, writing review and editing. JY: methodology. YL: investigation. MZ: data curation. YTL: software. JD: supervision. XZ: resources. GZ: conceptualization, writing review and editing, supervision. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval
The present study was approved by the Ethics Committee of Xuanwu Hospital, Capital Medical University. All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Consent to participate
Written informed consent was obtained from the patients and their parents.
Consent for publication
Not applicable.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Wang, Y., Liu, Y., Liu, Y. et al. Analysis of the risk factors of post-operative seizure in pediatric patients with hydrocephalus undergoing endoscopic third ventriculostomy. Childs Nerv Syst 38, 2141–2148 (2022). https://doi.org/10.1007/s00381-022-05634-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-022-05634-0