
Abstract
In this pictorial essay the authors review the normal sonographic gray-scale and Doppler appearance of the pediatric scrotum with an emphasis on technique. The authors present an update on ultrasound diagnosis and outcomes in testicular torsion and differentiation from other acute scrotal processes, as well as sonographic imaging of testicular microlithiasis and uncommon or atypical scrotal masses including splenogonadal fusion, polyorchidism, meconium peritonitis and epidermoid cyst. Further, the authors discuss testicular neoplasms in the context of testicular microlithiasis.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Normal gray-scale anatomy
High-resolution imaging of the scrotum is best accomplished with high-frequency (9- to 18-MHz) linear-array transducers. The normal scrotal wall is 2- to 3-mm thick (Fig. 1). The testes are symmetrical, oval-shape organs characterized by a homogeneous pattern of medium-amplitude echoes. Transverse-plane sonograms are important for comparing the testes’ symmetry in size and echogenicity (Fig. 1). The gray-scale appearance of the testis varies with transducer frequency (Fig. 1). To avoid misdiagnosis, one should assess the technique employed in acquiring images. On high-resolution ultrasound, the lobules of the testes are separated by interlobular hypoechoic fibrous septations. The tunica albuginea is a thick fibrous capsule surrounding the testis. The tunica folds into the testicular parenchyma parallel to the epididymis to form the linear echogenic mediastinum testis. The epididymis is a curved structure attached to the posterior testis with the epididymal head forming a cap overlying the cranial aspect of the testis (Fig. 1). The epididymis is isoechoic or slightly hypoechoic to the testis. Two vestigial remnants, the appendix epididymis and the appendix testis, can be visualized on ultrasound, particularly in the setting of a hydrocele (Fig. 1). The appendages are functionally inert but can become involved in inflammatory or neoplastic processes. The tunica vaginalis is a peritoneal reflection, surrounding the entire testis except where the testis is fixed to the epididymis and spermatic cord posteriorly. A small amount of fluid within the tunica vaginalis is normal.

Doppler ultrasound
Color and spectral Doppler US are important for assessing blood flow to the normal testes and surrounding structures. The testicular arteries arise from the abdominal aorta and are accompanied by the artery of the vas deferens, cremasteric artery and corresponding veins as they course through the spermatic cord into the scrotum. Transverse color Doppler of both testes is important for assessing the presence and symmetry of Doppler flow (Fig. 2). The asymptomatic testis serves as a control for assessing increased or decreased flow on the symptomatic side. Doppler settings should be optimized and then not be changed when comparing the testes to avoid misdiagnosis of increased or decreased flow from changes in technique. A sagittal view of the inguinal canal and upper scrotum demonstrates the normal spermatic cord as a linear rope-like structure with no evidence of rotation (Fig. 2). The cord might appear enlarged and hypervascular during Valsalva maneuver from a varicocele, which should not be mistakenly diagnosed as an inguinal hernia (Fig. 2).

Doppler ultrasound in a 14-year-old boy. a Transverse color Doppler US image shows symmetrical flow to the testes. b Sagittal color Doppler US image demonstrates normal spermatic cord (arrows), with no evidence of rotation. c Varicocele mimicking hernia. Sagittal color Doppler US at inguinal canal initially diagnosed as inguinal hernia (arrows). d Follow-up US examination with Valsalva maneuver confirms varicocele (arrows)
Doppler optimization
Understanding and applying Doppler principles are important for optimizing flow detection and accurate diagnosis of pathological processes. This is particularly true in pre-pubertal boys, in whom the testes are small and associated with relatively low flow.
To maximize detection of flow, one must be familiar with the user-controlled Doppler parameters. Testicular flow is slower in pre-puberty compared with post-puberty. To best detect testicular flow in pre-pubertal boys, it is important to use a high-frequency transducer, low pulse repetition frequency, low or absent filter, and high gain. These parameters and recommendations are discussed in greater detail in the next sections and are listed in Table 1.
Doppler frequency shift
Doppler frequency shift is governed by the following equation: fd=(2f0V cos θ)/C, where Fd represents the magnitude of the Doppler frequency shift, f0 represents the Doppler frequency of the transducer, V represents the velocity of moving tissue (blood), theta is the angle of Doppler interrogation, and C is the speed of sound in tissue. As a result, a high-frequency transducer better detects slow flow than a low-frequency transducer. Therefore the magnitude of the detected frequency shift is increased with a higher Doppler frequency irrespective of other parameters (Fig. 3).

Color Doppler technique in a 12-year-old boy (a–g). a Color Doppler frequency at 6 MHz shows no intratesticular flow. b Color Doppler frequency at 15 MHz shows good intratesticular flow. Note: all other parameters were kept constant. c Color Doppler at a high pulse repetition frequency (PRF) shows minimal testicular blood flow. d Color Doppler at low PRF setting shows good flow in the testis. Note: All other parameters were kept constant. e Low filter allows for good detection of flow. f High filter diminishes detection of normal flow in the testes. Note: All other parameters were kept constant. g Spectral Doppler image shows normal high diastolic flow. h Spectral Doppler image shows normal low diastolic flow in a 2-year-old boy
Pulse repetition frequency
Pulse repetition frequency (PRF) is the repetition rate of US pulses emitted by the transducer. As a rule of thumb, fast flow should be sampled at a high PRF and slow flow detection is optimized with a low PRF. PRF is adjusted utilizing the scale setting on most US systems. Detection of blood flow in the pediatric testis is optimized by using a lower PRF to assure detection of blood flow to the testes (Fig. 3).
Frequency filters
Frequency filters exclude undesirable low-frequency shifts that can originate from respiration and peristaltic motion. Care must be taken not to eliminate the low-frequency shifts produced by slow blood flow. Filters should be diminished to assure detection of slow blood flow as encountered in the pediatric testis (Fig. 3).
Color gain
Color gain, or gain, refers to the user-controlled amplification of the Doppler frequency shift. If the gain setting is too low, flow might not be detected. Flow detection is optimized by setting the gain to the highest level that does not demonstrate burst artifact. Power Doppler may also be utilized to increase the detection of testicular blood flow because it is more sensitive for flow detection than conventional color Doppler.
Doppler frequency shift might also be displayed as a spectral waveform over time for a user defined region of interest. The testicular artery demonstrates high diastolic flow in infants and post-pubertal males (Fig. 3) and often low or absent diastolic flow in pre-pubertal males (Fig. 3). Spectral tracings can be helpful in verifying blood flow to the testes when color Doppler signal is equivocal.
Acute scrotum
Acute scrotal pain and swelling in boys most often occur secondary to vascular compromise or inflammatory lesions. The most common causes include testicular torsion, torsion of the testicular appendages, epididymitis and epididymo-orchitis (Table 2).
Testicular torsion
Testicular torsion commonly presents in adolescents and newborns and is the final diagnosis in approximately 23% of boys presenting with an acute scrotum [8]. Prompt and accurate diagnosis is crucial for testis salvage [9]. The time from presentation to the emergency department to surgery is the most significant temporal predictor for a salvageable vs. a non-salvageable testis [10]. Salvage rates approach 100% with surgery within 6 h of presentation and less than 20% when surgery is performed after 12 h [3]. The most reliable clinical findings in testicular torsion include acute onset, nausea, abnormal lie, and loss of the ipsilateral cremasteric reflex [11, 12].
Gray-scale US findings in the testicular parenchyma in testicular torsion are variable and nonspecific. The testis might appear normal, enlarged or hypoechoic, or demonstrate a heterogeneous echo pattern [3, 10]. A heterogeneous testis on US is more likely to be non-viable at surgery, with 80% of non-viable testes appearing heterogeneous compared with 58% of viable testes (Fig. 4) [10]. Other gray-scale findings might include visualization of a twisted spermatic cord, a reactive hydrocele or a displaced epididymis (Fig. 4) [8].

Testicular torsion in a 6-year-old boy. a Transverse color Doppler image shows an enlarged, heterogeneous left testicle (small arrows) with peri-testicular blood flow but no intratesticular flow. Note normal flow in the right testicle (large arrow). Testicular torsion and infarction were confirmed at surgery. b Twisted cord within the inguinal canal. Linear cord (dashed arrow), twisted cord (solid arrow) and testicle (star). c Sagittal gray-scale image shows a displaced epididymal head (arrow) at the caudal aspect of the scrotum. Normally, the epididymal head should be at the cranial aspect of the scrotum. d Color Doppler sagittal image shows displaced, enlarged and slightly hypervascular epididymis (arrows), which might mimic epididymitis. An enlarged epididymis should not distract from the underlying diagnosis of testicular torsion
Color Doppler US is highly accurate for diagnosing testicular torsion, with recent studies reporting Doppler sensitivities of 95–100% and specificities of 85–95% for testicular torsion diagnosis [7, 13, 14]. Doppler findings include absent or diminished intra-testicular blood flow in the symptomatic testis compared to the asymptomatic side (Fig. 4). Note that false-negative Doppler ultrasounds can occur in the setting of partial torsion or torsion and detorsion.
Kalfa et al. [8] reported the presence of a twisted spermatic cord to be more sensitive than color Doppler for diagnosing torsion; however complete absence of Doppler flow was their only criterion for diagnosing torsion (Fig. 4). Galina et al. [15] reported the importance of an abnormal location and appearance at the epididymal head (Fig. 4) for diagnosing torsion in boys with preserved Doppler blood flow to the testis. In research studies using surgery as the gold standard, the Doppler findings including absent color Doppler flow or asymmetrically diminished flow are still the best studied and are highly sensitive and specific. Although a twisted spermatic cord or displaced epididymal head are important associated signs for torsion, it is rare for the Doppler to be normal when there is torsion.
Neonatal testicular torsion accounts for approximately 10% of all cases [16]. Neonatal torsion can occur within 24 h of birth or later, affecting a testis that was previously known to be normal on physical examination. The affected testis is often non-viable at the time of diagnosis in these cases (Fig. 5) [17]. Immediate surgery might be warranted to perform an orchiopexy aimed at preventing synchronous or metachronous torsion of the asymptomatic testis [18,19,20,21]. Scrotal trauma, usually associated with breech delivery, can mimic torsion [22]. Color Doppler US is usually definitive by demonstrating scrotal wall edema and preservation of intra-testicular flow in trauma cases (Fig. 6).

Neonatal torsion in a 4-week-old boy. Transverse US image shows a heterogeneous right testicle with lack of internal color flow and a typical calcified rim (three arrows). Note the normal left testis (single arrow). Findings are consistent with testicular infarction

Traumatic breech delivery in a 1-day-old boy. Transverse Doppler US image shows prominent scrotal wall edema (arrow) but preserved intratesticular flow, compatible with a history of traumatic delivery. Normal flow was confirmed on real-time imaging. Scrotum and testis were normal at 4-week follow-up US examination
Non-surgical acute scrotum
Color Doppler US is also highly accurate for differentiating acute torsion from other causes of acute scrotal swelling and pain in boys, including acute epididymitis, torsion of the testicular appendages, Henoch–Schönlein purpura and acute idiopathic scrotal edema [8, 23]. Ultrasound of epididymitis demonstrates an enlarged epididymis with hyperemia on color Doppler (Fig. 7). Torsion of a testicular appendage shows hyperemia surrounding the testicular appendage and preservation of normal flow within the testis (Fig. 8). Henoch–Schönlein purpura and acute idiopathic scrotal edema typically have scrotal wall thickening and hyperemia with preservation of flow to the testes (Fig. 9). Differentiating these lesions from torsion is important because these lesions can usually be treated medically and do not require surgical intervention.

Epididymitis in a 10-year-old boy. Doppler US shows enlargement and hyperemia of the epididymis (arrows) in this boy with acute epididymitis

Torsion of the appendix testis in a 7-year-old boy. Sagittal gray-scale US image shows an echogenic mass (solid arrow) separate from the testicle and epididymis (dashed arrow). This was noted to be avascular on color Doppler. Given the appearance and location, it is most compatible with torsion of the testicular appendage

Henoch–Schönlein purpura in a 4-year-old boy with acute scrotal pain. Color Doppler US shows thickened hypervascular scrotal wall with preservation of flow to the testes
Testicular microlithiasis
Testicular microlithiasis is often detected as an incidental finding [24, 25]. Testicular microlithiasis is characterized by five or more non-shadowing intratesticular echogenic calcific foci per testicle, which are localized to the seminiferous tubules (Fig. 10). Several studies have suggested a relationship between testicular microlithiasis and testicular cancer, particularly germ cell tumors [25, 26]. Trout et al. [27] reported a significant association between testicular microlithiasis and testicular neoplasia in a large multi-institutional retrospective study of pediatric patients. Malignant germ cell tumors were present in 2.8% of patients with microlithiasis and only 0.12% without microlithiasis. The risk of developing testicular neoplasia in the setting of testicular microlithiasis is unknown. Accurate assessment of cancer risk would require a large prospective study. There is no standardized protocol for surveillance criteria of previously diagnosed testicular microlithiasis for the onset of tumor.

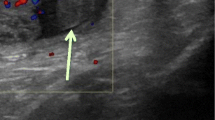
Testicular microlithiasis in a 6-year-old boy. Transverse gray-scale image shows bilateral non-shadowing punctate echogenic foci, diagnostic for microlithiasis
Uncommon non-neoplastic scrotal masses
Splenogonadal fusion
Splenogonadal fusion is a rare anomaly characterized by congenital fusion between a portion of the spleen and the gonad (Fig. 11). It is much more common in boys than girls [28,29,30]. This likely relates to the accessibility of the male gonad to palpation, which enables recognition of the anomaly [29, 30]. Splenogonadal fusion is usually an incidental finding manifesting as either an intra- or extra-testicular mass. Because splenogonadal fusion interferes with normal gonadal descent into the processus vaginalis, there is an increased association with inguinal hernia or undescended testicle.

Splenogondal fusion in an 11-year-old boy. Sagittal US image shows a circumscribed echogenic mass (solid arrow) along the superior pole of the testicle (dashed arrow). Splenic tissue was confirmed at surgery
Splenogonadal fusion can be subcategorized into continuous or discontinuous types. In the continuous type the gonad is linked to the spleen via a fibrous cord of splenic tissue that courses from the upper pole of the normal spleen to the testis. Associated anomalies include limb deficiency anomalies and micrognathia [30]. The discontinuous type of splenogonadal fusion is a variant of an accessory spleen and is rarely associated with any other congenital anomalies [29, 30]. The discontinuous type can appear as a hypoechoic mass in the testicle and can be indistinguishable from a testicular malignancy. Color Doppler flow often shows a central feeding vessel, which might branch out to the rest of the splenic tissue. Awareness of this condition could avoid unnecessary orchiectomy because the testis can be separated and preserved while the lesion is removed.
Polyorchidism
Polyorchidism is a rare congenital anomaly in which a supernumerary testis is identified in one hemiscrotum (Fig. 12). Polyorchidism is usually asymptomatic and diagnosed as an incidental finding during surgery for inguinal hernia, testicular tumor or torsion. Polyorchidism is associated with an inguinal hernia in approximately 24% of cases and undescended testis in 22% of cases, and has also been associated with microlithiasis [31, 32]. A supernumerary testis is usually seen as a solid nodule, isoechoic to the normal testis but smaller in size. A hydrocele is present in approximately 9% of cases. Color Doppler demonstrates a similar flow pattern to both the normal testis and the supernumerary testis. Management of polyorchidism is debated; however, resection and ipsilateral orchiectomy might be recommended because of the increased risk for malignancy, with a reported incidence of up to 5% [31].

Polyorchidism in a 17-year-old boy. Color Doppler US image demonstrates a supernumerary testis (solid arrows), which is isoechoic to the normal testis (dashed arrow)
Meconium peritonitis
Meconium peritonitis occurs secondary to in utero bowel perforation associated with congenital bowel obstruction. Meconium peritonitis can extend from the peritoneal cavity into the scrotum via a patent processus vaginalis and manifest on US as a scrotal mass, usually associated with calcifications. On rare occasions meconium peritonitis can appear as a very large concretion associated with a complex meconium collection in the scrotum (Fig. 13). Diagnosis is usually readily apparent given the underlying diagnosis of intestinal atresia.

Atypical meconium peritonitis in a 1-day-old boy. US image shows large concretion within the scrotal sac (solid arrow), large complex meconium-containing fluid (star), and normal testicle (dashed arrow) with ileal atresia and perforated bowel
Epidermoid cyst of the testicle
Epidermoid cysts are benign tumor-like lesions characterized by a fibrous wall and multiple layers of keratin creating an onionskin appearance that is characteristic but not always present. On sonography epidermoid cysts can manifest as a sharply defined mass with a hyperechoic rim and an onion ring appearance comprising alternating hypo- and hyperechogenic layers (Fig. 14). Absent flow on color Doppler is characteristic. The characteristic gray-scale findings should suggest the diagnosis of an epidermoid cyst and allow for testicle-sparing surgery [33].

Epidermoid cyst in a 5-year-old boy.. Doppler US image shows typical onionskin appearance of an epidermoid cyst (thin arrows) with no internal flow. Note also the presence of microlithiasis in this patient (thick arrow)
Conclusion
In this pictorial review, we have provided an overview of basic scrotal US findings in the pediatric population. Knowledge of normal sonographic anatomy of the scrotum and the application of proper sonographic technique are crucial for assuring accurate diagnosis and management of scrotal pathology in children. We described several causes of acute scrotum, with an emphasis on testicular torsion. In this essay we also reviewed the sonographic appearance and significance of testicular microlithiasis and atypical scrotal masses, including epidermoid cyst, splenogonal fusion, polyorchidism and meconium peritonitis.
References
Delaney LR, Karmazyn B (2013) Ultrasound of the pediatric scrotum. Semin Ultrasound CT MR 34:248–256
Karmazyn B (2010) Scrotal ultrasound. Ultrasound Clin 5:61–74
Sung EK, Setty BN, Castro-Aragon I (2012) Sonography of the pediatric scrotum: emphasis on the Ts — torsion, trauma, and tumors. AJR Am J Roentgenol 198:996–1003
Aso C, Enriquez G, Fite M et al (2005) Gray-scale and color Doppler sonography of scrotal disorders in children: an update. Radiographics 25:1197–1214
Carkaci S, Ozkan E, Lane D, Yang WT (2010) Scrotal sonography revisited. J Clin Ultrasound 38:21–37
Cokkinos DD, Antypa E, Tserotas P et al (2011) Emergency ultrasound of the scrotum: a review of the commonest pathologic conditions. Curr Probl Diagn Radiol 40:1–14
Yang C Jr, Song B, Liu X et al (2011) Acute scrotum in children: an 18-year retrospective study. Pediatr Emerg Care 27:270–274
Kalfa N, Veyrac C, Lopez M et al (2007) Multicenter assessment of ultrasound of the spermatic cord in children with acute scrotum. J Urol 177:297–301
Cattolica EV, Karol JB, Rankin KN et al (1982) High testicular salvage rate in torsion of the spermatic cord. J Urol 128:66–68
Liang T, Metcalfe P, Sevcik W et al (2013) Retrospective review of diagnosis and treatment in children presenting to the pediatric department with acute scrotum. AJR Am J Roentgenol 200:444–449
Beni-Israel T, Goldman M, Bar Chaim S et al (2010) Clinical predictors for testicular torsion as seen in the pediatric ED. Am J Emerg Med 28:786–789
Srinivasan A, Cinman N, Feber KM et al (2011) History and physical examination findings predictive of testicular torsion: an attempt to promote clinical diagnosis by house staff. J Pediatr Urol 7:470–474
Altinkilic B, Pilatz A, Weidner W (2013) Detection of normal intratesticular perfusion using color coded duplex sonography obviates need for scrotal exploration in patients with suspected testicular torsion. J Urol 189:1853–1858
Baker LA, Sigman D, Mathews RI et al (2000) An analysis of clinical outcomes using color doppler testicular ultrasound for testicular torsion. Pediatrics 105:604–607
Galina P, Dermentzoglou V, Baltogiannis N et al (2015) Sonographic appearances of the epididymis in boys with acute testicular torsion but preserved testicular blood flow on color Doppler. Pediatr Radiol 45:1661–1671
Driver CP, Losty PD (1998) Neonatal testicular torsion. Br J Urol 82:855–858
Snyder HM, Diamond DA (2010) In utero/neonatal torsion: observation versus prompt exploration. J Urol 183:1675–1677
Roth CC, Mingin GC, Ortenberg J (2011) Salvage of bilateral asynchronous perinatal testicular torsion. J Urol 185:2464–2468
Baglaj M, Carachi R (2007) Neonatal bilateral testicular torsion: a plea for emergency exploration. J Urol 177:2296–2299
Yerkes EB, Robertson FM, Gitlin J et al (2005) Management of perinatal torsion: today, tomorrow or never? J Urol 174:1579–1582
Djahangirian O, Ouimet A, Saint-Vil D (2010) Timing and surgical management of neonatal testicular torsions. J Pediatr Surg 45:1012–1015
Tiwary CM (1989) Testicular injury in breech delivery: possible implications. Urology 34:210–212
Ben-Sira L, Laor T (2000) Severe scrotal pain in boys with Henoch-Schönlein purpura: incidence and sonography. Pediatr Radiol 30:125–128
Middleton WD, Teefey SA, Santillan CS (2002) Testicular microlithiasis: prospective analysis of prevalence and associated tumor. Radiology 224:425–428
Backus ML, Mack LA, Middleton WD et al (1994) Testicular microlithiasis: imaging appearances and pathologic correlation. Radiology 192:781–785
Cast JE, Nelson WM, Early AS et al (2000) Testicular microlithiasis: prevalence and tumor risk in a population referred for scrotal sonography. AJR Am J Roentgenol 175:1703–1706
Trout AC, Chow J, McNamara E, Darge K (2016) Large multi-center study and the association between testicular microlithiasis and testicular neoplasia in a pediatric population. Presented at the international pediatric radiology meeting Chicago, IL. Pediatr Radiol 46:S107–S108
Basbug M, Akgun H, Ozun MT et al (2009) Prenatal sonographic findings in a fetus with splenogonadal fusion limb defect syndrome. J Clin Ultrasound 37:298–301
Varma DR, Sirineni GR, Rao MV et al (2007) Sonographic and CT features of splenogonadal fusion. Pediatr Radiol 37:916–919
Stewart VR, Sellars ME, Somers S et al (2004) Splenogonadal fusion: B-mode and color Doppler sonographic appearances. J Ultrasound Med 23:1087–1090
Danrad R, Ashker L, Smith W (2004) Polyorchidism: imaging may denote reproductive potential of accessory testicle. Pediatr Radiol 34:492–494
Amodio JB, Maybody M, Slowotsky C et al (2004) Polyorchidism: report of 3 cases and review of the literature. J Ultrasound Med 23:951–957
Arellano CM, Kozakewich HP, Diamond D, Chow JS (2011) Testicular epidermoid cysts in children: sonographic characteristics with pathological correlation. Pediatr Radiol 41:683–689
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors have no financial interests, investigational or off-label uses to disclose.
Rights and permissions
About this article

Cite this article
Alkhori, N.A., Barth, R.A. Pediatric scrotal ultrasound: review and update. Pediatr Radiol 47, 1125–1133 (2017). https://doi.org/10.1007/s00247-017-3923-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-017-3923-9