
Abstract
Purpose
To demonstrate that lateral to medial patellofemoral force and pressure ratios could be a surrogate marker of retinacular tension and patellar tracking.
Methods
The patellofemoral forces of six knees from three fresh-frozen half-body female cadavers were evaluated with a capacitive sensor under simulated operative conditions in six staged clinical scenarios: native knees, knee arthroplasty without patellar resurfacing, resurfaced knee and patella, resurfaced knee and patella with lateral release, gender-specific knee arthroplasty with patella resurfacing, and gender-specific knee arthroplasty with lateral release. Maximum force and peak pressure were simultaneously recorded during three to four ranges of motion. Average values were compared between lateral and medial patellofemoral compartments as an objective measure of patellar tracking for the different settings.
Results
Significant differences in lateral and medial force and pressure differentials were seen in most scenarios despite clinically normal patellar tracking. Lateral to medial ratios of maximum force and peak pressure significantly increased after TKA (2.9, 2.1) and after patella resurfacing (2.8, 2.6) compared to the native knee (1.6, 1.8). Addition of a lateral release in resurfaced knees decreased the ratio of lateral to medial patellofemoral forces and pressures as did gender knee arthroplasty (1.5 and 1.1, 2 and 1.3, respectively). Pressure and force values most closely resembled the native knee in the resurfaced knee/resurfaced patella with lateral release and in the gender knee arthroplasty scenarios.
Conclusions
Use of lateral to medial patellofemoral force ratios as a surrogate objective marker for patellar tracking was validated in this study by decreasing ratios observed after lateral release in TKA and with gender-specific implants.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Total knee arthroplasty (TKA) is becoming an increasingly common procedure throughout the world [23, 24]. The improvement of prosthetic biomaterials and design as well as a greater understanding of the knee biomechanics have shifted the focus of TKA to prosthesis longevity and patellofemoral complications such as anterior knee pain, patella fracture, patellar component loosening, patella dislocation, and wear [3, 16, 33, 36, 40].
Altered patellofemoral biomechanics in TKA are implicated as the cause of patellofemoral complications. Numerous studies have directly evaluated how static and dynamic restraints affect the patellofemoral joint forces in the native knee [12, 18, 25, 28, 30, 38] and in TKA [2, 6, 10, 13, 14, 17, 18, 25, 28, 38, 44]. Patellofemoral biomechanics have mostly been studied in biomechanical simulators using cadavers with replicated muscle and joint forces with varying degrees of soft tissue stripping. Although experimental factors can be more strictly controlled in a knee simulator, these studies’ application to the standard clinical environment of TKA is limited.
Specific medial and lateral contact areas throughout the range of motion (ROM) have been identified on the native patella as well as the resurfaced patella [12, 25, 43, 44]. While patellofemoral contact areas have been shown to decrease after TKA with patellar resurfacing, the patellofemoral stresses have been shown to increase [6, 25, 28, 44]. Theoretically, these changes, along with eccentric forces and pressures on the medial and lateral patellofemoral articulations, could lead to increased patellar complications. In addition, some authors have shown significant changes in patellar tilt and/or tracking after TKA suggestive of significant changes in patellofemoral kinematics [1, 4, 7, 37, 41]. Despite the importance of the patellofemoral biomechanics in TKA, the criteria for evaluating the success of soft tissue balancing and patellar tracking currently involve only the surgeon’s observation of intraoperative patellar tracking during a passive ROM [5, 39, 41].
A simulated intraoperative assessment of the ratios of lateral and medial patellofemoral stresses during TKA under different prosthetic designs and conditions may provide a better understanding of how intraoperative factors alter patellofemoral joint dynamics. Understanding the changes in lateral to medial ratios of patellofemoral pressures after patellar resurfacing, the use of different prosthetic designs, and the addition of a lateral release could improve preoperative and intraoperative decision-making in order to minimize future complications by objectively calculating retinacular tension and patellar tracking.
The goal of this study was to utilize an existing validated sensor technology to demonstrate that lateral to medial patellofemoral force and pressure ratios could be a surrogate marker of retinacular tension and patellar tracking. Our hypothesis is that the lateral to medial patellofemoral force and pressure ratios would increase with TKA and would subsequently decrease after lateral retinacular release and after placement of gender-specific implants showing that these ratios change appropriately with known changes in patellofemoral biomechanics. This finding would suggest that the lateral to medial patellofemoral force and pressure ratios could be used as an objective measure of soft tissue tension at the patellofemoral joint. An objective measure of patellar tracking and soft tissue tension that can be measured in the clinical setting allows further studies to be done correlating these ratios to post-operative outcomes such as anterior knee pain and patellar complications.
Materials and methods
Three fresh-frozen, half-body cadavers (six knees) were used in this study. All cadavers were female with an average age of 82 years (range 76–90 years). After institutional review board approval, all surgical procedures and data recording were performed under simulated operating room conditions by one fellowship-trained joint surgeon. Preoperative maximum knee flexion ranged from 115° to 130°, and none had a flexion contracture. The half-body was supine, and the pelvis stabilized such that flexion and extension of the knee during arthrotomy, bone cuts, implantation of prosthetic components, and testing were similar to an actual operative procedure.
The capacitive novel pliance system (Novel Electronics, Inc., St. Paul, MN) used in this study was previously described in detail by Johanson et al. [19]. The system utilized here included an S2039 patella sensor, electronics unit, pliance-x Expert software (v 11.3.12), Multiprojects-ip software (v 13.3.40), and a trublu calibration device (Novel Electronics). The patella sensor was approximately 1,988 mm3 and 1.8-mm thick. Before each trial, the sensor was calibrated on the surface being tested. The data gathered by the sensor were sent to the computer via Bluetooth technology (Bellevue, WA) and collected at 50 Hz for the purpose of this study. The pliance-x Expert software then displays these data in real-time two- and three-dimensional representation of the calibrated pressure values (Fig. 1). These data can then be analysed further. Previous studies validated the sensor technology including reproducibility when conforming to curved surfaces [27, 34].

Sensor output data during a range-of-motion cycle using the capacitive novel pliance system (Novel Electronics, Inc., St. Paul, MN)
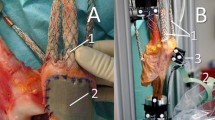
A standard medial parapatellar approach was used to expose the joint in all knees. The articular cartilage was classified according to the Outerbridge classification [31]. Four of six knees demonstrated grade IV osteochondrosis. The patella was everted in the standard fashion. The sensor device was sutured over the articular surface of the native patella (Fig. 2), and the joint capsule was closed using three sutures (one superior, one inferior, one central) prior to each trial. The native knee with native patella was taken through three to four consecutive continuous ROMs.

Inverted patella with sensor sewn to articular surface
Bone cuts were then made to the tibia and femur in standard fashion for positioning of NexGen High-Flex (Zimmer, Inc., Warsaw, IN) knee components with the goal of a posterior tibial slope of 0° to 3° and 3° of femoral component external rotation. Femoral and tibial trial components were then placed. The resurfaced knee with a native patella was then tested over three to four continuous ROMs.
Next, the patella sensor was partially removed to allow for the preparation of the patellar surface and placement of a domed 32-mm patellar component. The sensor was reapproximated with sutures. The resurfaced knee with resurfaced patella was then tested. The previous procedure was again repeated for increasing domed patella sizes of 34 and 36 mm, respectively.
Following this procedure, the left knees of all three cadavers in the resurfaced knee/resurfaced patella state were selected and underwent lateral release and were retested with all three patellar sizes. Subsequently, the femoral components were removed, and the necessary bone cuts were made in all six knees for placement of the Gender Solutions High-Flex (Zimmer) femoral component. The three right gender-specific resurfaced knees with resurfaced patella and three left gender-specific resurfaced knees with resurfaced patella after lateral release were tested and repeated for all three patellar sizes. Finally, the three right knees in the gender knee/resurfaced patella scenario underwent lateral release and were retested in the same fashion.
The sensor was zeroed immediately before each clinical scenario, including each differently sized patella component, and was taken through the three to four continuous ROMs to full flexion. Component alignment, component and joint stability, and patellar tracking were found to be clinically acceptable in all situations. A lateral release was not deemed clinically necessary in any scenario.
For the purposes of this study, six clinical scenarios were analysed which included native knee, knee replacement without patellar resurfacing, knee replacement with a resurfaced patella, total knee replacement with lateral release, gender-specific knee replacement with patellar resurfacing, and gender-specific knee replacement with patellar resurfacing and lateral release. Patellar maximum force (N) and patellar pressure (kPa) were measured after each successive reconstructive setting of the cadaveric knee over a complete ROM (Fig. 3). These recordings were summarized over the 3–4 repeated measurements for each of the six clinical scenarios. The results using different patellar component sizes were averaged together based on the type of clinical scenario tested.

Methods used to construct and subsequently evaluate each of the six clinical scenarios. NKNP native knee and native patella, RKNP resurfaced knee and native patella, RKRP resurfaced knee and resurfaced patella, RKRP-LR resurfaced knee and resurfaced patella with lateral release, GKRP gender knee and resurfaced patella, GKRP-LR gender knee and resurfaced patella with lateral release
Statistical analysis
Lateral and medial averages in maximum force and peak pressure were graphically assessed via plots of averages across designs to ensure that differences between the lateral and medial sides were consistent. In subsequent (nested) analyses, averages of the repeated observations at each unique design point served as the units of observation. The averages were summarized by type of prosthesis and treatment of the patella, and the resultant means were compared between lateral and medial sides in a pair-wise manner. A student t test with a pooled sample variance was used in comparisons, and the assumption of equal sample variances between lateral and medial sides was assessed using a folded F test. All analyses were performed using SAS for the personal computer (v8.02, SAS, Inc., Cary, NC). Descriptive statistics were generated using the univariate procedure. The GPLOT procedure was used to generate plots of averages. The t test procedure was used to perform t tests and to test sample variances for equality, and Wilcoxon rank-sum tests were performed using the NPAR1WAY procedure.
Results
Significant differences in lateral and medial force and pressure differentials were seen in most scenarios despite clinically normal patellar tracking (Tables 1 and 2). For the native knee, a statistically significant difference was seen between the lateral and medial patellofemoral maximum force means (p = 0.04) at a ratio between the lateral and medial sides of 1.63. However, this difference was not significant when comparing lateral to medial peak pressure means at a comparative ratio of 1.80. For the resurfaced knees with native patella scenario, a significant increase was seen in the ratio of lateral to medial maximum force and peak pressure means (2.86 and 1.99, respectively).
For the resurfaced knee with resurfaced patella scenario, statistically significant differences were seen in lateral to medial maximum force and peak pressure means (p < 0.01 and p < 0.01, respectively) and in the ratio between the lateral and medial sides (2.75 and 2.57, respectively). The addition of a lateral release in this scenario reduced the lateral to medial ratios of maximum force and peak pressure means to insignificant ratios (1.46 and 1.11, respectively).
In the gender knee arthroplasty, a statistically significant difference was seen in lateral to medial maximum force means (p < 0.01) at the ratio of 1.96. A statistically significant difference was not seen in the lateral to medial peak pressure means at a comparative ratio of 1.33. The addition of a lateral release to the gender knee arthroplasty did not significantly alter the ratios of lateral to medial maximum force and peak pressure.
Maximum force was significantly increased on the lateral side compared with the medial side in all scenarios except in the resurfaced knee with a lateral release. Ratios of lateral to medial forces were highest in the resurfaced knee with native patella and in the resurfaced knee with patellar resurfacing groups (2.86:1 and 2.75:1, respectively) compared with native (1.63:1) and gender (1.96:1) knees (Table 1).
Peak pressure was significantly increased only on the lateral side in the resurfaced knee with native patella (2.10:1) and with patellar resurfacing (2.57:1) groups compared with native (1.8:1) and gender (1.33:1) knees. Highest lateral peak pressure ratios were found in the resurfaced knees with patellar resurfacing but were significantly decreased after lateral release (from ratios of 2.57:1 to 1.11:1) (Table 2). The resurfaced knee with resurfaced patella and gender knee scenarios showed peak pressure and maximum force ratios that most closely resembled the native knee.
Discussion
While ratios of lateral to medial patellofemoral forces and pressures increased after TKA, the ratios subsequently decreased with lateral retinacular release and with gender knee arthroplasty. Since both lateral retinacular release and gender knee arthroplasty should decrease the soft tissue tension in the lateral retinacular tissues, these ratios may be used as surrogate marker for lateral retinacular tension and patellar tracking. The lateral to medial patellofemoral pressure and force ratios are objective assessments of retinacular tension and patellar tracking that may help elucidate the differences of soft tissue tension in the intraoperative setting of TKA.
In this study, TKA with and without patellar resurfacing had higher peak forces and maximum pressures on the lateral side of the patellofemoral joint compared with native knees, suggesting patellar maltracking. Singerman et al. [38] determined that the centre of pressure went from medial to lateral as cadaver knees were ranged from extension to full flexion in the native knee, resurfaced knee with native patella, and resurfaced knee with resurfaced patella scenarios using experimental indirect force measurements calculated from a force transducer, but specific ratios were not mentioned. However, a significant lateral pressure shift was seen only in the resurfaced knee with native patella scenario. They also found that higher patellofemoral compressive forces were present in flexion when the centre of pressure was more lateral. Becher et al. [2] also found higher pressures with a lateral shift of the centre of pressure in flexion in the resurfaced knee with native patella scenario using pressure sensitive film. Xu et al. [44] found that the ratio of lateral to medial mean patellofemoral pressure in TKA increased after patella resurfacing at 60° of flexion (1.30) compared with the unresurfaced patella (1.05) using pressure sensitive film. At the other degrees of flexion studied, lateral to medial mean pressure ratios were similar in the resurfaced knee with native patella (0.91:1.09) and resurfaced knee with resurfaced patella (0.79:0.99) scenarios. Kainz et al. [20] found the centre of pressure moved laterally in patellofemoral joint after TKA with patella resurfacing with an increase in pressure compared to the native knee; however, ratios on the medial and lateral facets were not reported. Significant edge loading on the patella was described in another study with resurfaced patellar components, suggesting a difference in peak medial to lateral patellofemoral contact forces [14]. These studies along with our study show that an increase in lateral patellofemoral forces occurs in TKA that may lead to patellar maltracking and subsequently to patellofemoral complications.
This study demonstrated a significant decrease in the ratio of patellofemoral forces between the lateral and medial sides after lateral retinacular release in TKA. In a native knee study done with cadavers using a biomechanical simulator, Ostermeier et al. [30] found that, although patellofemoral contact forces did not change after lateral retinacular release, the centre of pressure went from medial to lateral with increasing knee flexion despite lateral release, whereas patellar tilt remained fairly constant. Although this study did not compare lateral to medial pressures, it suggests that lateral retinacular release does alter the distribution of forces without necessarily changing the amount of force in the native patellofemoral joint. In another cadaver study, patellofemoral joint forces in TKA with patella resurfacing moved medially on the femur after lateral release, although no ratio between the lateral and medial sides was reported [18]. Our study, along with the trends in the current literature, validates our theory that the ratio of patellofemoral lateral to medial pressures is a surrogate marker for patellar tracking in that the ratio decreased after lateral retinacular release.
Anatomic and biomechanical differences that exist in the female knee compared with the male knee have been postulated to be the cause of the increased incidence of knee pain in women [9, 15, 42]. These differences have recently been mentioned as possible reasons for complications in TKA, although this has not been shown in the literature [8, 11, 15, 22, 26]. Because of these differences, gender-specific implants were developed. The Zimmer Gender Solutions High-Flex Knee (Zimmer, Inc., Warsaw, IN) has a thinner anterior femoral flange and has a higher trochlear groove angle than the NexGen knee (Zimmer), which was based on anatomic femoral differences seen on computed tomography in women [15]. The idea behind this design is that the thinner anterior flange will help prevent overstuffing of the patellofemoral joint in female patients and the deeper trochlear groove will improve patellar tracking. These features theoretically should allow for improved patellofemoral biomechanics.
The gender knee arthroplasty group in our study had lateral to medial peak pressures and maximum forces that most closely resembled those of the native knee compared with the other scenarios tested. This finding further validates our theory of the ratio of lateral to medial patellofemoral forces as an objective measure of retinacular tension and patellar tracking as the gender-specific implants were designed to address that issue seen in anatomic studies. Kawahara et al. [21] found that while increasing the size of the femoral component did increase patellofemoral contact forces, changing to gender-specific implants did not alter the patellofemoral forces significantly as was expected. Perhaps the ratio of lateral to medial forces is a more sensitive way to evaluate patellofemoral tracking. We also found that lateral release after gender knee arthroplasty did not significantly change the ratio of lateral to medial patellofemoral forces, unlike in the standard resurfaced knee. Peretz et al. [32] similarly found no significant change in the peak pressure of the patellofemoral articulation after lateral release in gender knee arthroplasty in a biomechanical study. The increase in peak pressure and the small decrease in maximum force ratios in the gender knee with lateral release group compared to the gender knee arthroplasty group may be explained by the scenario of normal variance in improved patellar tracking and retinacular tension with the gender-specific components.
The ratio of lateral to medial maximum force and peak pressure at the patellofemoral articulation in this setting may be viewed as a surrogate measure of soft tissue tension. These ratios are important in the intraoperative management of patellar tracking and soft tissue balancing because extensor mechanism symptoms and complications in TKA may be caused by imbalance of the peripatellar structures leading to abnormal forces in the patellofemoral joint [40].
Limitations may be present due to the small sample size studied; however, our sample size is comparable to those reported in other published studies [10, 13, 17, 18, 20, 25, 28, 38, 43, 44]. Variability in this small sample population may cause bias, although these scenarios are not unlike those encountered in the operating room during TKA. Another limitation of this study is the absence of muscle function or weight bearing during the measurements. Muscle contraction will obviously change the patellofemoral mechanics in vivo; however, the goal of our study was to evaluate the ratio of lateral to medial forces in the operative setting when muscle contraction is generally absent. Our method relied on resting muscle tension because half-body cadavers were used, a scenario which better mimics intraoperative muscle tension compared to previous studies that imitated muscle contraction with weights and biomechanical simulators. Changes in soft tissue tension in the later stages of testing may have also affected the ratios despite careful soft tissue handling. However, our model tested resting muscle tension, whereas other biomechanical models used weighted muscle tension, which is more prone to stretching over time.
Maximum force and pressure values were chosen for comparison between different clinical scenarios. Several biomechanical studies have shown that patellofemoral forces change with varying knee flexion and/or quadriceps tension [2, 7, 10, 14, 17, 18, 20, 25, 28, 30, 38, 44]. Although we understand the importance of these factors, this is not a feasible way to evaluate patellar tracking in the operative setting. The purpose of our study was to assess the patellofemoral forces in ways that would be useful to an operating surgeon. In addition, maximum values (instead of mean) were used in each setting because the maximum stresses should theoretically correlate better with patellofemoral complications and symptoms.
Although the use of a sensor placed in the patellofemoral articulation does provide direct assessment of forces on the articular surface, it is not ideal. Although the sensor is flexible and conformable, it does have some structural resistance to conforming to a convex surface as well as the addition of thickness to the patellofemoral articulation, which may impact the measurements. To minimize inaccurate measurements, the sensor was calibrated to zero in its static state before each scenario was tested. In the ideal setting, the sensor would be embedded into the patella component in order to avoid measurement inaccuracies, as published elsewhere [27, 43].
Other methods of subjective intraoperative evaluation of the patellofemoral joint besides the “no thumb” test have been described, but these methods also rely on direct visualization only [35, 41]. Objective intraoperative evaluation of patellar tracking in order to make decisions has been reported [29]. Ogata et al. [29] used measurements of medial retinacular suture tension to help make decisions on lateral release in 35 TKAs and reported good results at 2 years. However, the use of any intraoperative measurement of patellofemoral forces has not been extensively studied. The ability to intraoperatively quantitate patellar tracking and soft tissue balance may help surgeons in decision-making and facilitate a reduction in the incidence of postoperative complications. Future studies using these ratios to evaluate intraoperative patellar tracking and comparing them with clinical results may help to decrease patellofemoral complications in TKA.
Conclusion
Although patellar tracking is integral to the success of TKA, current standards of tracking assessment are limited. This study validated that the lateral to medial ratio of patellofemoral stresses is an objective, surrogate marker of patellar tracking because the ratio decreased after lateral release in TKA and was lower at baseline in gender TKA compared with standard TKA. In addition, this study showed that lateral to medial ratios of patellofemoral maximum forces and peak pressures most closely resembled the native knee in TKA with patellar resurfacing after lateral release and in gender knee arthroplasty.
References
Barink M, Meijerink H, Verdonschot N, van Kampen A, de Waal Malefijt M (2007) Asymmetrical total knee arthroplasty does not improve patella tracking: a study without patella resurfacing. Knee Surg Sports Traumatol Arthrosc 15:184–191
Becher C, Heyse TJ, Kron N, Ostermeier S, Hurschler C, Schofer MD, Fuchs-Winkelmann S, Tibesku CO (2009) Posterior stabilized TKA reduce patellofemoral contact pressure compared with cruciate retaining TKA in vitro. Knee Surg Sports Traumatol Arthrosc 17:1159–1165
Bellemans J, Vandenneucker H, Vanlauwe J (2005) Total knee replacement. Current Orthopaedics 19:446–452
Belvedere C, Catani F, Ensini A, Moctezuma de la Barrera JL, Leardini A (2007) Patellar tracking during total knee arthroplasty: an in vitro feasibility study. Knee Surg Sports Traumatol Arthrosc 15:985–993
Bengs BC, Scott RD (2006) The effect of patellar thickness on intraoperative knee flexion and patellar tracking in total knee arthroplasty. J Arthroplasty 21:650–655
Benjamin JB, Szivek JA, Hammond AS, Kubchandhani Z, Matthews AI Jr, Anderson P (1998) Contact areas and pressures between native patellas and prosthetic femoral components. J Arthroplasty 13:693–698
Chew JT, Stewart NJ, Hanssen AD, Luo ZP, Rand JA, An KN (1997) Differences in patellar tracking and knee kinematics among three different total knee designs. Clin Orthop Relat Res 345:87–98
Clarke HD, Hentz JG (2008) Restoration of femoral anatomy in TKA with unisex and gender-specific components. Clin Orthop Relat Res 466:2711–2716
Csintalan RP, Schulz MM, Woo J, McMahon PJ, Lee TQ (2002) Gender differences in patellofemoral joint biomechanics. Clin Orthop Relat Res 402:260–269
D’Lima DD, Chen PC, Kester MA, Colwell CW Jr (2003) Impact of patellofemoral design on patellofemoral forces and polyethylene stresses. J Bone Joint Surg Am 85(Suppl 4):85–93
Dalury DF, Mason JB, Murphy JA, Adams MJ (2009) Analysis of the outcome in male and female patients using a unisex total knee replacement system. J Bone Joint Surg Br 91:357–360
Elias JJ, Kilambi S, Goerke DR, Cosgarea AJ (2009) Improving vastus medialis obliquus function reduces pressure applied to lateral patellofemoral cartilage. J Orthop Res 27:578–583
Fuchs S, Schutte G, Witte H, Rosenbaum D (2000) Retropatellar contact characteristics in total knee arthroplasty with and without patellar resurfacing. Int Orthop 24:191–193
Glaser FE, Gorab RS, Lee TQ (1999) Edge loading of patellar components after total knee arthroplasty. J Arthroplasty 14:493–499
Greene KA (2007) Gender-specific design in total knee arthroplasty. J Arthroplasty 22(7 Suppl 3):27–31
Healy WL, Wasilewski SA, Takei R, Oberlander M (1995) Patellofemoral complications following total knee arthroplasty. Correlation with implant design and patient risk factors. J Arthroplasty 10:197–201
Heyse TJ, Becher C, Kron N, Ostermeier S, Hurschler C, Schofer MD, Tibesku CO, Fuchs-Winkelmann S (2010) Patellofemoral pressure after TKA in vitro: highly conforming versus posterior stabilized inlays. Arch Orthop Trauma Surg 130:191–196
Hsu HC, Luo ZP, Rand JA, An KN (1997) Influence of lateral release on patellar tracking and patellofemoral contact characteristics after total knee arthroplasty. J Arthroplasty 12:74–83
Johanson NA, Cerynik DL, Pasquale M (2011) Measuring patellofemoral forces and pressures in a simulated operating room environment. J Arthroplasty 26:137–143
Kainz H, Reng W, Augat P, Wurm S (2012) Influence of total knee arthroplasty on patellar kinematics and contact characteristics. Int Orthop 36:73–78
Kawahara S, Matsuda S, Fukagama S, Mitsuyasu H, Nakahara H, Higaki H, Shimoto T, Iwamoto Y (2012) Upsizing the femoral component increases patellofemoral contact force in total knee replacement. J Bone Joint Surg Br 94:56–61
Kim YH, Choi Y, Kim JS (2010) Comparison of standard and gender-specific posterior-cruciate-retaining high-flexion total knee replacements: a prospective, randomised study. J Bone Joint Surg Br 92:639–645
Kurtz SM, Lau E, Ong K, Zhao K, Kelly M, Bozic KJ (2009) Future young patient demand for primary and revision joint replacement: national projections from 2010 to 2030. Clin Orthop Relat Res 467:2606–2612
Kurtz SM, Ong KL, Lau E, Widmer M, Maravic M, Gomez-Barrena E, Manno V, Torre M, Walter WL, de Steiger R, Geesink RG, Peltola M, Roder C (2011) International survey of primary and revision total knee replacement. Int Orthop 35:1783–1989
Lee TQ, Gerken AP, Glaser FE, Kim WC, Anzel SH (1997) Patellofemoral joint kinematics and contact pressures in total knee arthroplasty. Clin Orthop Relat Res 340:257–266
MacDonald SJ, Charron KD, Bourne RB, Naudie DD, McCalden RW, Rorabeck CH (2008) The John Insall Award: gender-specific total knee replacement: prospectively collected clinical outcomes. Clin Orthop Relat Res 466:2612–2616
Martinelli L, Hurschler C, Rosenbaum D (2006) Comparison of capacitive versus resistive joint contact stress sensors. Clin Orthop Relat Res 447:214–220
Matsuda S, Ishinishi T, White SE, Whiteside LA (1997) Patellofemoral joint after total knee arthroplasty. Effect on contact area and contact stress. J Arthroplasty 12:790–797
Ogata K, Ishinishi T, Hara M (1997) Evaluation of patellar retinacular tension during total knee arthroplasty. Special emphasis on lateral retinacular release. J Arthroplasty 12:651–656
Ostermeier S, Holst M, Hurschler C, Windhagen H, Stukenborg-Colsman C (2007) Dynamic measurement of patellofemoral kinematics and contact pressure after lateral retinacular release: an in vitro study. Knee Surg Sports Traumatol Arthrosc 15:547–554
Outerbridge RE (1961) The etiology of chondromalacia patellae. J Bone Joint Surg Br 43-B:752–757
Peretz JI, Driftmier KR, Cerynik DL, Kumar KS, Johanson NA (2012) Does lateral release change patellofemoral forces and pressures? Clin Orthop Relat Res 470:903–909
Pickering T, Berend M (2008) Patella resurfacing in total knee arthroplasty: the sum of all parts. Semin Arthroplasty 19:112–116
Putti AB, Arnold GP, Cochrane L, Abboud RJ (2007) The Pedar in-shoe system: repeatability and normal pressure values. Gait Posture 25:401–405
Rae P, Noble J, Hodgkinson J (1990) Patellar resurfacing in total condylar knee arthroplasty: technique and results. J Arthroplasty 5:259–265
Rhee S, Haddad F (2008) Patello-femoral joint in total knee replacement. Curr Orthop 22:132–138
Sharma A, Leszko F, Komistek RD, Scuderi GR, Cates HE Jr, Liu F (2008) In vivo patellofemoral forces in high flexion total knee arthroplasty. J Biomech 41:642–648
Singerman R, Gabriel SM, Maheshwer CB, Kennedy JW (1999) Patellar contact forces with and without patellar resurfacing in total knee arthroplasty. J Arthroplasty 14:603–609
Spitzer AIVK (1995) Patellar considerations in total knee arthroplasty. In: Scuderi G (ed) The patella. Springer, New York, p 315
Stiehl JB (2005) A clinical overview patellofemoral joint and application to total knee arthroplasty. J Biomech 38:209–214
Strachan RK, Merican AM, Devadasan B, Maheshwari R, Amis AA (2009) A technique of staged lateral release to correct patellar tracking in total knee arthroplasty. J Arthroplasty 24:735–742
Varadarajan KM, Gill TJ, Freiberg AA, Rubash HE, Li G (2009) Gender differences in trochlear groove orientation and rotational kinematics of human knees. J Orthop Res 27:871–878
Wilson DR, Apreleva MV, Eichler MJ, Harrold FR (2003) Accuracy and repeatability of a pressure measurement system in the patellofemoral joint. J Biomech 36:1909–1915
Xu C, Chu X, Wu H (2007) Effects of patellar resurfacing on contact area and contact stress in total knee arthroplasty. Knee 14:183–187
Acknowledgments
Zimmer, Inc. (Warsaw, IN, USA) provided funding by sponsoring the cadavers, TKA components, and laboratory time. Zimmer also provided the funding for the study statistician. Zimmer did not play any role in the interpretation of the data, writing of the manuscript, or decision to submit the manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
King, J.J., Chakravarty, R., Cerynik, D.L. et al. Decreased ratios of lateral to medial patellofemoral forces and pressures after lateral retinacular release and gender knees in total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 21, 2770–2778 (2013). https://doi.org/10.1007/s00167-012-2200-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-012-2200-6