
Abstract
Posterior reversible encephalopathy syndrome (PRES) is a rare neurological disease. Recently, an increase in the number of transplantations has led to more cases being associated with PRES than what was previously reported. Calcineurin inhibitors (CNIs) are major risk factors for PRES in posttransplantation patients. The mechanisms of the development of PRES remain to be unclear. The typical clinical symptoms of PRES include seizures, acute encephalopathy syndrome, and visual symptoms. The hyperintense signal on fluid-attenuated inversion recovery image is the characteristic of the imaging appearance in these patients. In addition, other abnormal signals distributed in multiple locations are also reported in some atypical cases. Unfortunately, PRES is often not recognized or diagnosed too late due to complicated differential diagnoses, such as ischemic stroke, progressive multifocal leukoencephalopathy, and neurodegenerative diseases. Thus, this review emphasizes the importance of considering the possibility of PRES when neurological disturbances appear after solid organ transplantation or hematopoietic cell transplantation. Moreover, this review demonstrates the molecular mechanisms of PRES associated with CNIs after transplantation, which aims to help clinicians further understand PRES in the transplantation era.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Posterior reversible encephalopathy syndrome (PRES), initially described by Hinchey [1] in 1996, is a neurological disturbance coupled with different clinical symptoms and appearances of distinctive imaging features. The etiology of this syndrome is complicated, varied, and often includes hypertensive encephalopathy, eclampsia, immunosuppressive drugs, and autoimmune diseases [1, 2]. So far, the mechanisms of PRES development are still unknown. Seizures, acute encephalopathy syndrome, and visual symptoms are the typical clinical symptoms of PRES [3–5]. The fluid-attenuated inversion recovery (FLAIR) images usually show an abnormal and reversible increased signal, mostly distributed in the parietal and occipital lobes. However, the abnormal signal can also be distributed in the posterior frontal, temporal lobe, cerebellum, brainstem, thalamus, and basal ganglia. The incidence of atypical distribution and imaging appearances may even be higher than what is commonly seen in the literature [5–7]. The management of PRES is still unclear. Although this disease is reversible, permanent neurological deficits and cerebral infarcts may appear because of late recognition of this syndrome and persistence in the incorrect usage of drugs [5].
PRES after transplantation, as a rare complication, should not be ignored, especially in developing countries, where the numbers of transplantations are rising rapidly. There is an upward trend of the reports about PRES with an increasing number of transplantations. There are about 160 publications that have mentioned PRES after transplantation since the disease was first reported in 1996. More than 80 publications regarding PRES after transplantation have been published from 2010 to 2014, including 78 cases that report after solid organ transplantation (SOT) or hematopoietic cell transplantation (Table 1) [8–31]. There have been significant advances in PRES research after transplantation in the past 4 years, but only few review articles concerning PRES after transplantation. The aim of our paper is to review the prevalence, mechanism, diagnosis, differential diagnoses, and management of PRES and to help clinicians to consider the possibility of PRES appearing as a neurological disturbance after transplantation.
Prevalence
PRES is increasingly recognized as a neurological disturbance with various clinical symptoms and characteristic images. PRES can occur in both male and females as well as in adults and children. The incidence of PRES after SOT is approximately 0.5–5 % [10, 13, 15, 25]. One study [32], which evaluated 4222 patients that underwent transplantation, reported that the incidence of PRES after SOT is about 0.49 %, with a similar incidence among subtypes. Another study considered that the incidence of PRES after lung transplantation is closely 5.7 %, while only 12 cases had been published among 25,755 lung transplant recipients from 1999 to 2009 [24]. Meanwhile, the incidence of PRES after allogeneic hematopoietic stem cell transplantation (HSCT) is 1.1–20 % [14, 16, 17, 33].
The etiology of PRES is complicated and varied, including hypertensive encephalopathy, eclampsia, immunosuppressive drugs, and autoimmune diseases [1, 2, 5]. There are also other risk factors, such as the following: hypomagnesemia, hypocholesterolemia, vasoactive agents, erythropoietin, blood transfusion, antineoplastic drugs, peritoneal dialysis, and parathyroid hormone-related peptide [19, 34, 35]. Immunosuppressive drugs, especially calcineurin inhibitors (CNIs), are widely used for preventing acute rejection reaction in patients with various transplantations. Seventy-five patients with PRES seem to be related with immunosuppressive drugs in 78 transplantation patients from 2010 to 2014. One study proposed that PRES can occur in patients receiving CNIs after kidney, allogeneic peripheral blood stem cell, liver, and lung transplantations [36]. CNIs may be a major risk factor for PRES in posttransplantation patients. In addition, hypertension is sometimes accompanied with PRES after transplantation. Hypertension presents in approximately 70–80 % of patients [2, 4]. Fifty-six percent of the patients may have a history of hypertension [37]. High-dose corticosteroid use, ischemia reperfusion during surgery, the use of multiple medications, and antibiotics may be associated with PRES after SOT and hematopoietic cell transplantation, as well [11].
Clinical Features of PRES
The features of PRES after transplantation include clinical symptoms and neuroimaging. The typical clinical symptoms are involved in seizures, acute encephalopathy syndrome, and visual symptoms. Dysarthria, incoordination of the limbs, paresis, sensory deficits, and visual hallucinations are atypical clinical symptoms. The characteristic neuroimaging is a hyperintense signal, distributing in the parietal and occipital lobes on FLAIR images. Other magnetic resonance sequences can also show the specific appearances of PRES. Furthermore, angiography and magnetic resonance angiography (MRA) are also useful diagnosis approaches for PRES.
Clinical Symptoms
Seizures, acute encephalopathy syndrome, and visual symptoms are the mainly clinical symptoms of PRES after transplantation. One study identified 120 cases of PRES, which reported that seizures (74 %), encephalopathy (28 %), headache (26 %), and visual disturbances (20 %) are the clinical presentations of PERS [38]. The acute encephalopathy syndrome includes confusion, headache, vomiting, altered consciousness, and mental status changes [4, 9, 10, 22, 29]. Visual symptoms involve hemianopsia [4], loss of visual acuity [11], visual blurring [11], blindness [20], and diplopia [30]. Seizures with secondary generalization, multiple seizures, and status epilepticus are reported as the common symptoms in some literatures [4, 26]. Status epilepticus is also reported as a main manifestation of PRES after pediatric HSCT [14]. Residual epilepsy may be continued despite clinical and neuroradiological normalization in PERS patients [12]. In addition, other atypical symptoms like dysarthria, incoordination of the limbs, paresis, sensory deficits, and visual hallucinations can occur in PRES [10, 23, 30, 31]. One study suggested that the incidence of atypical distribution and imaging appearances may even be higher [7]. Intracranial hemorrhage can occur simultaneously in PRES, with an incidence of approximately 15 %. Intracranial hemorrhage is more common after allogeneic bone marrow transplantation than after SOT [31, 39].
The time course of PRES presentation varies in posttransplantation patients. PRES typically develops within 2–3 months after liver transplantation [5, 15]. The timing is even later in renal transplantation patients [32]. Some cases showed an onset time within 1 week after transplantation [10, 11, 19, 25, 26, 29, 40]. Therefore, PRES can occur during acute and subacute onset neurological disturbances after transplantation. The time course of PRES may be associated with the type and dosage of CNIs and the organ of transplantation surgery.
Neuroimaging
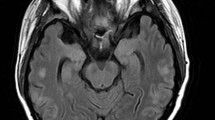
The MRI is one of the most useful imaging tools for diagnosing PRES. MRI scan usually shows an abnormal and reversible increased signal on FLAIR images, which is the most sensitive sequence for recognition of cortical and subcortical edema in PRES [5]. The hyperintense signal alterations on FLAIR images usually distribute in the parietal and occipital lobes. The lesions also appear as iso-intense or hyperintense signals on T1-weighted images (T1WI) and hyperintense signals on T2-weighted images (T2WI) [41, 42]. Diffusion-weighted MRI (DWI) and apparent diffusion coefficient (ADC) are instrumental in distinguishing the type of edema in PRES lesions. Hyperintense on the DWI and hypointense in the ADC mapping are the characteristics of a cytotoxic edema, whereas an iso-intense or hyperintense signal in DWI and hyperintense in ADC are typical presentations of a vasogenic edema. Vasogenic edema can generally be completely reversible; however, severe vasogenic edema can exacerbate cytotoxic edema, leading to worse outcome [2, 4–6]. PRES can also be identified in other MRI imaging. Gadolinium enhancement, hemorrhage, and restricted diffusion have been observed in some patients with PRES [7, 12, 18, 21, 24, 43]. The abnormal signal of PRES can be distributed throughout the posterior frontal, temporal lobe, cerebellum, brainstem, thalamus, and basal ganglia [7, 10, 11, 24, 43]. In addition, angiography is another measure for PRES patients. Angiography can reveal focal or diffuse vasoconstriction, vasodilatation, or a “string-of-beads” appearance [43]. One study also mentioned that the dilation and constriction in the secondary and tertiary branches of intracranial artery could be observed in PRES patients by angiography and MRA [2].
Differential Diagnosis
It is often very difficult to recognize PRES at the beginning, since this syndrome has various atypical symptoms and imaging appearances. The diagnosis of PRES was further confirmed in most cases, when neuroimaging showed a reversible lesion. Clarity of the differential diagnoses of PRES is needed in order to make a diagnosis. Encephalopathy associated with ischemia, thrombosis, hemorrhage, infection, immune-inflammation, and others are general differential diagnoses. Most diseases mentioned above can be distinguished by symptoms, radiography, and laboratory examinations. Here, we present some differential diagnosis for PRES in Table 2.
Osmotic Demyelination Syndrome
Osmotic demyelination syndrome (ODS) is a neurological disorder with new onset neurological symptoms and a recent rapid increase in serum sodium. Typical MRI lesions of ODS reveal hypointense images on T1WI and hyperintense images on FLAIR and T2WI [44]. The incidence of ODS is higher in liver transplant recipients than the general population [45]. However, the distributions of lesions are common in the striatum and pons. Mental status changes, movement disorders, dysphagia, and dysarthria are major presentations [44–46]. Monitoring serum sodium may also be helpful in identifying the disease. Of patients, 50–67 % may have good outcomes, but even in those patients who have made a complete or nearly complete clinical recovery, imaging findings do not improve [44, 46].
Posttransplantation Lymphoproliferative Disorder
Posttransplantation lymphoproliferative disorder (PTLD) is a heterogeneous disease with variable benign or malignant types and unspecific symptoms. The incidence varies from 1 to 2 % after kidney transplantation to 20 % after small bowel transplantation [47, 48]. The risk is 20–120-fold higher in the posttransplantation patients than in the normal subjects [47, 49]. PTLD is also a malignant complication of cyclosporine A (CsA) with an incidence between 2 and 4 % [50]. PTLD in the central nervous system is a more rare form but has been increasing with the rise in popularity of SOTs. Focal neurological deficits, headaches, and altered mental status are common symptoms of central nervous system PTLD. Neuroimaging usually reveals multiple contrast-enhancing mass lesions in supratentorial, lobar, periventricular, corpus callosum, basal ganglia, and pituitary [47, 51, 52]. Epstein–Barr virus (EBV) deoxyribonucleic acid (DNA), biopsy, and cerebrospinal fluid (CSF) cytology and immunology are measures for the distinction between PTLD and PRES [47, 48, 53]. Prognosis is variable but not reversible. Rate of survival depends on the malignant degree, early detection, and timely treatment [48].
Progressive Multifocal Leukoencephalopathy
Progressive multifocal leukoencephalopathy (PML) is a demyelinating disease due to John Cunningham (JC) virus, which leads to a destructive infection of oligodendrocytes in immunosuppressed patients. Seventy-nine percent PML occurs in AIDS patients. The usage of immunosuppressant in organ transplantation recipients is associated with the development of 5 % PML [54]. The clinical symptoms are usually nonspecific and variable, including limb weakness, cognitive deficits, speech or visual difficulties, ataxia, seizures, and headache [55]. Radiographic characteristic of PML is single or multifocal white matter lesion, which may become confluent and large with the progression of this disease. The lesions of PML are generally hypointense on T1WI and hyperintense on T2WI, with high signals on the DWI and normal-to-low signals in the ADC. The parietal, occipital, and frontal lobes are the most frequent sites of PML. The lesions can occasionally be seen in the pontomesencephalon, basal ganglia, and cerebellum in PML patients [54, 56]. The neuroimaging appearance can also reveal mass effects and enhancements [55, 57]. JC virus DNA in CSF and proton magnetic resonance spectroscopy (MRS), which reveals low levels of N-acetylaspartate, high levels of choline, and elevated levels of lactate and variable myo-inositol in PML patients, may be helpful in distinguishing PML from PRES [56]. Brain biopsy is the gold standard of PML. The outcome of PML ranges from stabilization or even remission to brain herniation or even death [54, 58].
Management and Prognosis
PRES following transplantation is reversible, when culprit drugs are discontinued or decreased early, or when related symptoms are controlled immediately such as hypertension or seizures. Unfortunately, permanent neurological deficits and cerebral infarcts may appear because of late recognition of this syndrome or persistent use of culprit drugs. The occurrence of intracranial hemorrhage also worsens the prognosis. Increasing studies suggested that not all PRESs are reversible [17, 59]. Therefore, timely and effective treatments for PRES after transplantation are essential for the outcomes of patients.
Management of Immunosuppressive Drugs
CNIs may be one of the major risk factors for PRES in posttransplantation patients. Management of immunosuppressive drugs is one of the primary tasks. However, there are several strategies for managing culprit immunosuppressive drugs. In some studies, the drugs were switched or substituted [9, 10, 20]. Some cases lowered the dosages of immunosuppressive drugs [11, 60]. A reduction of the culprit drugs accompanied with adding other similar drugs can also be seen in some other cases [18, 26]. Moreover, other studies have reported some cases in which CsA was ceased without substitution [24, 61].
In a study of 19 patients after hematopoietic allogeneic stem cell transplantation [17], 40 % of the patients survived without using tacrolimus (TAC) to manage PRES. About 40 % of the patients survived when TAC was continued. Meanwhile, 50 % of the patients who were switched to another agent survived and were eventually discharged. The results of this study suggest that there is no difference among these strategies, since the survival percentages were similar. In addition, another study showed that switching the immunosuppressive regimen may be detrimental and even fatal. It is recommended to completely cease treatment of CNIs as a treatment of PRES [62]. However, some cases that switch the immunosuppressive regimen have good outcomes [9, 20, 24, 25, 27, 30]. So, the management of immunosuppressive drugs still needs more researches. In most cases, reducing the dosage, switching the immunosuppressive drugs, or cessation of treatment are still the therapeutic strategy of PRES. Continuing using the culprit drugs should be discreet. The risk of rejection after transplantation should be taken into consideration. Meanwhile, therapeutic effects and related risks should be weighed.
Symptomatic Treatment
Seizures, one of the typical clinical symptoms of PRES after transplantation, should be controlled immediately. Uncontrolled seizures may shorten life span and increase the risk of death significantly. Approximately 20–30 % of patients with epilepsy are not fully controlled with available drugs [63]. The efficiency and adverse effects of the antiepileptic drug should be considered. Since there are several advantages and limitations for each drug, it is often difficult to choose appropriate antiepileptic drugs. One review [64] discussed all relevant data about epilepsy and other comorbidities, which concluded that gabapentin, levetiracetam, pregabalin, and topiramate are the most appropriate antiepileptic drugs to treat epilepsy in patients with liver transplantation. Additionally, the most appropriate drugs in kidney transplantation are benzodiazepines, lamotrigine, and valproic acid. The most appropriate drugs in bone marrow transplantation are gabapentin, levetiracetam, lamotrigine, and topiramate.
Blood pressure is often high in PRES patients. Of patients, 32–52 % have high blood pressure after transplantation. In all these cases, antihypertension treatments were used for controlling blood pressure. A treatment regimen of a diuretic plus an angiotensin-converting enzyme inhibitor (ACEI) is often recommended in patients with cerebrovascular disease [65]. Intravenous antihypertensive agents are necessary in patients with hypertensive emergency, which decrease blood pressure by 25 % [66]. However, some articles suggest that hypertension is a compensatory way to improve cerebral blood flow [15]. Thus, controlling blood pressure should be appropriate and prudent. The management of hypertension in PRES patients after transplantation still needs more evidence-based studies.
In addition, other symptoms, such as vomiting, mental status changes, and intracranial hemorrhage, should be examined since all of these are associated with patient outcomes. Monitoring vital signs, maintenance of arterial oxygenation, sufficient hydration, and correction of coagulopathies and electrolyte disturbances are general strategies for managing PRES patients.
Prognosis
The prognosis of PRES is generally reversible and benign. Seventy-two percent of patients present a reversion of imaging abnormalities with a mean duration of 41 days [67]. Recurrence of PRES is also infrequent and benign [13, 27]. Only a part of the patients after transplantation were reported to become worse, even died. But the death is rarely directly related with PRES [15]. However, one study included 302 patients, who underwent allogeneic HSCT, which suggested that the 1-year survival rate is significantly inferior in patients who developed PRES [68]. Permanent neurological deficit and cerebral infarcts also appear in some cases [69]. Therefore, early diagnosis and appropriate treatments are still essential for a good recovery of patients.
Pathophysiology Mechanisms
Until recently, there was a lot of controversy about the mechanism of PRES. There are two major hypotheses, which included the hyperperfusion and hypoperfusion theories [5, 40, 70, 71]. The first theory suggests that severe hypertension leads to transient impairment of autoregulation, causing cerebral vasodilatation and vasogenic cerebral edema. The other theory suggests that the neurotoxicity of culprit drugs and hypertension induces autoregulatory vasoconstriction, leading to hypoperfusion, ischemia, and edema. Hyperperfusion remains the most popular hypothesis for the development of brain edema that occurs in PRES. Endothelial dysfunction and disruption of the blood brain barrier are another mechanisms, which lead to the development of PRES. There are several clinical and neuroimaging evidences about the occurrence of hypertension, failed autoregulation, and vasogenic cerebral edema [5, 70]. However, the molecular mechanisms of PRES after transplantation are still unclear. Here, we review the molecular mechanisms of PRES, which are mainly associated with CNIs after transplantation.
TAC and CsA are both CNIs, which are the main immunosuppressant drugs after transplantation. They are widely used for preventing acute rejection, since they provide potent inhibitory effects on T lymphocyte activation in patients with various transplantations. TAC (the Japanese drug FK506), a macrolide immunosuppressant, was discovered in 1984 [72]. TAC binds to the FK506-binding protein 12 (FKBP12) in the cytoplasm. The complex then inhibits the activity of calcineurin, and the signal transduction pathways in T cells are also downregulated [73–76]. CsA, a cyclic 11-amino acid peptide, was discovered earlier than TAC. CsA binds to cyclophilin and forms a complex, which can inhibit calcineurin and block the phosphatase activity, causing a decrease in T lymphocyte activation [74, 76, 77].
The Mechanism of Vasogenic Cerebral Edema in CNIs Induced by PRES
The final pathophysiological manifestation of PRES is brain edema. Previous studies suggested that severe hypertension exceeds the potential of autoregulation and the autoregulation dysfunction leads to vasogenic cerebral edema. In some cases, neuroimaging shows evidence of vasogenic cerebral edema, such as increased diffusions consistent with vasogenic edema in DWI and ADC [6, 25, 29]. In the posttransplantation patients, CNIs may participate in the formation of vasogenic cerebral edema in PRES through multiple molecular mechanisms.
Vasogenic edema of PRES may be caused by the dysfunction of the blood–brain barrier. There are two aspects of blood–brain barrier dysfunction induced by CNIs: (1) hyperpermeability of the blood–brain barrier and (2) the inhibited expression of P-glycoprotein (Fig. 1). Previous studies have shown that CsA and TAC can damage the tight junction and the cell membrane directly and that CsA can induce apoptosis on the brain capillary endothelial cells [78, 79]. This leads to an increased permeability of the blood–brain barrier. Moreover, it is known that TAC can induce a calcium ion leakage from the endoplasmic reticulum [77, 80, 81]. FKBP12 binds to inositol 1,4,5-trisphosphate receptor (IP3R), which is associated with regulation of IP3-mediated Ca2+ flux. Calcineurin anchors to the IP3R via FKBP12 which participates in the regulation of the receptor [77, 80, 82]. When TAC dissociates FKBP12–IP3R complex or CsA inhibits calcineurin, the binding of calcineurin to the FK506–FKBP12 complex is stimulated, resulting in the phosphorylation of IP3R by protein kinase C, causing an increase in Ca2+ flux [77, 80, 83]. The increased intracellular Ca2+ can disrupt the tight junctions, which is the major constitution of the blood–brain barrier, via Ca2+-dependent pathways [84–88]. Eventually, permeability of the blood–brain barrier is increased because of the disruption of the tight junction. In addition, CsA can decrease cAMP formation by inhibiting adrenomedullin-induced activation of adenylyl cyclase. The expression and phosphorylation of claudin-5 are weakened via a PKA pathway, when the intracellular cAMP concentration is decreased. This causes an increased permeability of the brain–blood barrier by the loosening of the intercellular junctions [89–91]. Furthermore, another current study showed that plasminogen activator inhibitor-1(PAI-1) increased the tightness of the brain endothelial barrier in a dose-dependent manner [92]. Previous research also reported that the inducers of PAI-1 involve the product of proinflammatory mediators, such as tumor necrosis factor-α and interleukin-1 [93, 94]. However, the production of the proinflammatory mediators is suppressed by CNIs through inhibiting the transcription of genes of early T cell activation [75]. Thus, the permeability of the blood–brain barrier may be influenced by this mechanism indirectly.

Schematic illustration of the mechanism of vasogenic cerebral edema in PRES associated with CNIs. The blood–brain barrier is formed by endothelial cells, pericytes, and astrocytes. CsA and TAC can injure the tight junction of the endothelial cells via causing the Ca2+ leakage, weakening the expression and phosphorylation of claudin-5, and decreasing the production of PAI-1. CsA also decreases the production of TGF-β1 in brain pericytes and causes the dysfuction of NO production in astrocytes, leading to the hyperpermeability and dysfunction of P-glycoprotein
Several previous studies demonstrated that CsA can cause dysfunction of P-glycoprotein, which leads to the breakdown of the blood–brain barrier, via several ways. P-glycoprotein is an adenosine triphosphate (ATP)-dependent transmembrane transport protein and critical component of the blood–brain barrier. One such way is to decrease production of transforming growth factor-β1 (TGF-β1) in brain pericytes or to cause the dysfunction of nitric oxide (NO) production in astrocytes [77, 78, 89, 95, 96]. The inhibition of P-glycoprotein activity by CsA is also shown by using PET of 11C-verapamil distribution into the brain [97]. Interestingly, the effect of CsA on NO production is still controversial. Some experiments demonstrated that CsA induces NO synthase expression and causes an increase of NO [77, 98, 99]. However, other experiments showed that CsA reduces NO synthase expression [100, 101]. The effect of NO production by CsA may be dependent on the dose of CsA. In any way, the dysfunction of the NO production may contribute to the endothelial dysfunction, which leads to the permeability variation. Moreover, a study found that CsA causes hyperpermeability and P-glycoprotein (P-gp) dysfunction by inhibiting TGF-β1 production [96]. However, another study concluded that CsA does not induce TGF-β1 biosynthesis. It is the cell type and concentrations used that the different effects on TGF-β1, caused by CsA, depend on [102].
The hyperpermeability of the blood–brain barrier and the inhibited expression of P-gp eventually result in brain swelling which is termed vasogenic cerebral edema. The dysfunction of the blood–brain barrier may be transient or improved by discontinuing or decreasing CNIs. As far as we know, acute hypertension is also a major cause of PRES and can change the function of the blood–brain barrier. During acute hypertension, the increased NO may increase permeability and contribute to disruption of the blood–brain barrier [103–105]. It is also reported that the change of Ca2+ may be responsible for the permeability and disruption of the blood–brain barrier in acute hypertension [106]. These mechanisms, resulting in the development of PRES, may commonly exist in CNIs and hypertension. Hypertension can disrupt the blood–brain barrier via other ways, such as inflammation and oxidative stress [107, 108]. Recently, it is found that short-term hypertension impairs the antioxidant defense system in the brain by diminishing claudins and gene transcription in the endothelial cells of the blood–brain barrier, which causes changes to the blood–brain barrier [109]. More studies are needed for further understanding of the development of PRES.
The Mechanism of Cytotoxic Edema in PRES Associated with CNIs
Most neuroimaging of PRES reveals vasogenic cerebral edema; nevertheless, a coexistence of vasogenic and cytotoxic edema exists in several cases. The DWI of these cases also shows restricted diffusions of the lesions [5, 7, 10]. Moreover, the previous mechanism also mentions that autoregulatory vasoconstriction, caused by several pathogenic factors, leads to the hypoperfusion and results in ischemia and edema. Severe vasogenic edema progressing to cytotoxic edema may represent an early sign of irreversible damage. Currently, the molecular mechanisms about the development of cytotoxic edema in PRES associated with CNIs have not been reviewed. Here, we conclude that the development of cytotoxic edema caused by CNIs may be involved in two ways: vasoconstriction resulting in hypoperfusion or mitochondrial dysfunction resulting in energy abnormality (Fig. 2).

Schematic illustration of the mechanism of cytotoxic edema in PRES associated with CNIs. CsA can cause the release of endothelin-1 leading to vasoconstriction and decrease the concentration of ATP leading to mitochondrial dysfunction. TAC can decrease the production of NO via several ways. Vasoconstriction resulting in hypoperfusion and mitochondrial dysfunction resulting in energy abnormality may lead to hypoxia that causes cytotoxic edema eventually
The endothelin-1 and decrease of NO may contribute to the vasoconstriction in cerebral artery. One study found that CsA-mediated capillary disruption causes the release of endothelin-1, which plays a significant role in CsA-induced endothelial dysfunction [110]. Their experiment also described that endothelin-1 gene is expressed during capillary breakdown by CsA. Another study reported that the use of CsA is associated with an increase in plasma levels of endothelin-1 [111]. However, other literatures considered that CsA does not elevate the level of endothelin-1 but increases the expression of the endothelin receptor [100]. In any way, endothelin-1 may play a role in endothelial dysfunction and may cause vasoconstriction of the arteries in the brain. Besides, TAC has been reported to decrease the production of NO in several ways. TAC inhibits calcineurin and decreases the dephosphorylation of NO synthase [112]. Calcineurin is also reported to directly modulate N-methyl-D-aspartic acid (NMDA) receptors. Hence, TAC affects NMDA-stimulated neurotransmitter release indirectly and inhibits glutamate-induced NO synthase activity [113, 114]. In addition, TAC can increase asymmetric dimethylarginine (ADMA), an endogenous NO synthase inhibitor, which competes with L-arginine to block NO synthesis [115, 116]. Moreover, TAC can activate KPCβII, which is an isoform of conventional PKC. The activated KPCβII phosphorylates endothelial NO synthase at its inhibitory site Thr495 and reduces the production of NO [81, 117].
CsA is associated with mitochondrial dysfunction, which results in abnormal cerebral energy metabolism. Even in the therapeutic range of CsA in transplant patients, ATP concentration is also decreased by 20 %, accompanied by the inhibition of the Krebs cycle and a reduction of NAD+ concentration [118–120]. Moreover, 4 to 10 h after CsA perfusion, cytosolic glycolysis shows an increase, which compensates for the inhibition of mitochondrial glucose metabolism. Lactate concentration is increased in the rat brain after 6 days of CsA treatment [120]. Furthermore, CsA can induce hyperpermeability and P-gp dysfunction after hypoxia/reoxygenation injury [121]. So when the shortage of cerebral energy metabolism is compensated, CsA may still cause the dysfunction of the blood–brain barrier.
Vasoconstriction resulting in hypoperfusion and mitochondrial dysfunction resulting in energy abnormality may lead to hypoxia that causes cytotoxic edema in PRES associated with CNIs, which plays a significant role in the progression of the disease. However, some mechanisms may possibly participate in the development of cytotoxic edema with TAC-induced leukoencephalopathy as well. The mechanism concerning the reversal of cytotoxic edema in the PRES requires further study.
The etiology of PRES includes hypertensive encephalopathy, eclampsia, immunosuppressive drugs, and autoimmune diseases. All of these are systemic factors. How do these systemic factors cause a disease in the brain? These may be associated with the sensitivity of white matter, the difference of hypoxia tolerance, and the difference of vascular development. The mechanism of the PRES is also probably related to the differences in gene expression. More researches and clinical cases are the keys to make the pathophysiological mechanism of PRES more clear.
Conclusion
PRES is rare in daily clinical work and has an upward trend related to the increasing number of the transplantations. The usage of CNIs can be a major risk factor for PRES in posttransplantation patients. The complicated differential diagnoses and late recognition may make the early diagnosis difficult. A familiarity with atypical clinical presentations, uncommon neuroimaging, and various differential diagnoses is necessary for early diagnosis. Also, the therapeutic effects and related risks should be measured when dealing with immunosuppressive drugs. Reviewing pathophysiology mechanisms of PRES may also provide novel management approaches and methods. However, the effects of inflammation and oxidative stress and the mechanisms of the reversal of cytotoxic edema after PRES should be further studied.
Abbreviations
- ACEI:
-
Angiotensin-converting enzyme inhibitors
- ADC:
-
Apparent diffusion coefficient
- CNIs:
-
Calcineurin inhibitors
- CsA:
-
Cyclosporine A
- CSF:
-
Cerebrospinal fluid
- DNA:
-
Deoxyribonucleic acid
- DWI:
-
Diffusion weighted MRI
- EBV:
-
Epstein–Barr virus
- FLAIR:
-
Fluid-attenuated inversion recovery
- HSCT:
-
Hematopoietic stem cell transplantation
- MRI:
-
Magnetic resonance imaging
- ODS:
-
Osmotic demyelination syndrome
- PAI-1:
-
Plasminogen activator inhibitor-1
- PKA:
-
Protein kinase A
- PKC:
-
Protein kinase C
- PRES:
-
Posterior reversible encephalopathy syndrome
- PTLD:
-
Posttransplantation lymphoproliferative disorder
- T1WI:
-
T1-weighted image
- T2WI:
-
T2-weighted image
- TAC:
-
Tacrolimus
- SOT:
-
Solid organ transplantation
References
Hinchey J, Chaves C, Appignani B, Breen J, Pao L, Wang A, Pessin MS, Lamy C et al (1996) A reversible posterior leukoencephalopathy syndrome. N Engl J Med 334:494–500
Bartynski WS (2008) Posterior reversible encephalopathy syndrome, part 1: fundamental imaging and clinical features. AJNR Am J Neuroradiol 29:1036–1042
Lamy C, Oppenheim C, Mas JL (2014) Posterior reversible encephalopathy syndrome. Handb Clin Neurol 121:1687–1701
Staykov D, Schwab S (2012) Posterior reversible encephalopathy syndrome. J Intensive Care Med 27:11–24
Wu Q, Marescaux C, Wolff V, Jeung MY, Kessler R, Lauer V, Chen Y (2010) Tacrolimus-associated posterior reversible encephalopathy syndrome after solid organ transplantation. Eur Neurol 64:169–177
Agildere AM, Basaran C, Cakir B, Ozgul E, Kural F, Haberal M (2006) Evaluation of neurologic complications by brain MRI in kidney and liver transplant recipients. Transplant Proc 38:611–618
McKinney AM, Short J, Truwit CL, McKinney ZJ, Kozak OS, SantaCruz KS, Teksam M (2007) Posterior reversible encephalopathy syndrome: incidence of atypical regions of involvement and imaging findings. AJR Am J Roentgenol 189:904–912
Alexander S, David VG, Varughese S, Tamilarasi V, Jacob CK (2013) Posterior reversible encephalopathy syndrome in a renal allograft recipient: a complication of immunosuppression? Indian J Nephrol 23:137–139
Alparslan M, Bora U, Huseyin K, Ayhan D, Gultekin S (2013) Posterior reversible encephalopathy syndrome in a renal transplanted patient. Am J Case Rep 14:241–244
Apuri S, Carlin K, Bass E, Nguyen PT, Greene JN (2014) Tacrolimus associated posterior reversible encephalopathy syndrome—a case series and review. Mediterr J Hematol Infect Dis 6:e2014014
Arimura FE, Camargo PC, Costa AN, Teixeira RH, Carraro RM, Afonso JE Jr, Campos SV, Samano MN et al (2014) Posterior reversible encephalopathy syndrome in lung transplantation: 5 case reports. Transplant Proc 46:1845–1848
Baldini M, Bartolini E, Gori S, Bonanni E, Cosottini M, Iudice A, Murri L (2010) Epilepsy after neuroimaging normalization in a woman with tacrolimus-related posterior reversible encephalopathy syndrome. Epilepsy Behav 17:558–560
Barbas AS, Rege AS, Castleberry AW, Gommer J, Ellis MJ, Brennan TV, Collins BH, Martin AE et al (2013) Posterior reversible encephalopathy syndrome independently associated with tacrolimus and sirolimus after multivisceral transplantation. Am J Transplant Off J Am Soc Transplant Am Soc Transplant Surg 13:808–810
Cordelli DM, Masetti R, Bernardi B, Barcia G, Gentile V, Biagi C, Prete A, Pession A et al (2012) Status epilepticus as a main manifestation of posterior reversible encephalopathy syndrome after pediatric hematopoietic stem cell transplantation. Pediatr Blood Cancer 58:785–790
Cruz RJ Jr, DiMartini A, Akhavanheidari M, Iacovoni N, Boardman JF, Donaldson J, Humar A, Bartynski WS (2012) Posterior reversible encephalopathy syndrome in liver transplant patients: clinical presentation, risk factors and initial management. Am J Transplant Off J Am Soc Transplant Am Soc Transplant Surg 12:2228–2236
Fukuyama T, Tanaka M, Nakazawa Y, Motoki N, Inaba Y, Higuchi T, Koike K (2011) Prophylactic treatment for hypertension and seizure in a case of allogeneic hematopoietic stem cell transplantation after posterior reversible encephalopathy syndrome. Pediatr Transplant 15:E169–E173
Hammerstrom AE, Howell J, Gulbis A, Rondon G, Champlin RE, Popat U (2013) Tacrolimus-associated posterior reversible encephalopathy syndrome in hematopoietic allogeneic stem cell transplantation. Am J Hematol 88:301–305
Hayes D Jr, Adler B, Turner TL, Mansour HM (2014) Alternative tacrolimus and sirolimus regimen associated with rapid resolution of posterior reversible encephalopathy syndrome after lung transplantation. Pediatr Neurol 50:272–275
Heo S, Cho HJ, Jeon IS (2010) A case of posterior reversible encephalopathy syndrome in a child with myelodysplastic syndrome following allogenic bone marrow transplantation. Pediatr Hematol Oncol 27:59–64
Jennane S, el Mahtat M, Konopacki J, Malfuson JV, Doghmi K, Mikdame M, De Revel T (2013) Cyclosporine-related posterior reversible encephalopathy syndrome after cord blood stem cell transplantation. Hematol Oncol Stem Cell Ther 6:71
Loar RW, Patterson MC, O’Leary PW, Driscoll DJ, Johnson JN (2013) Posterior reversible encephalopathy syndrome and hemorrhage associated with tacrolimus in a pediatric heart transplantation recipient. Pediatr Transplant 17:E67–E70
Moris D, Vernadakis S, Lionaki S, Daikos G, Zavos G (2014) An uncommon cause of acutely altered mental status in a renal transplant recipient. Ups J Med Sci 119:50–54
Qin W, Tan CY, Huang X, Huang Z, Tao Y, Fu P (2011) Rapamycin-induced posterior reversible encephalopathy in a kidney transplantation patient. Int Urol Nephrol 43:913–916
Rosso L, Nosotti M, Mendogni P, Palleschi A, Tosi D, Montoli M, Pappalettera M, Tarsia P et al (2012) Lung transplantation and posterior reversible encephalopathy syndrome: a case series. Transplant Proc 44:2022–2025
Santos MM, Tannuri AC, Gibelli NE, Ayoub AA, Maksoud-Filho JG, Andrade WC, Velhote MC, Silva MM et al (2011) Posterior reversible encephalopathy syndrome after liver transplantation in children: a rare complication related to calcineurin inhibitor effects. Pediatr Transplant 15:157–160
Shao X, He Z, Tang L, Gao L (2012) Tacrolimus-associated ischemic optic neuropathy and posterior reversible encephalopathy syndrome after small bowel transplantation. Transplantation 94:e58–e60
Shoji T, Bando T, Fujinaga T, Chen F, Kohno M, Yabe M, Yabe H, Date H (2012) Posterior reversible encephalopathy syndrome due to immunosuppressant after living-donor lobar lung transplantation: report of a case. Gen Thorac Cardiovasc Surg 60:514–517
Torelli GF, Natalino F, Barberi W, Iori AP, Andreoli C, Valle V, Mercanti C, Perrone S et al (2011) Early onset of posterior reversible encephalopathy syndrome (PRES) during Cyclosporine-A infusion. Leuk Res 35:1423–1424
Ueda N, Kawamura M, Nakazawa S, Hirai T, Kishikawa H, Nishimura K (2014) Posterior reversible encephalopathy syndrome (PRES) after kidney transplantation: a case report. Hinyokika Kiyo Acta Urologica Jpn 60:387–392
Yilmaz S, Gokben S, Arikan C, Calli C, Serdaroglu G (2010) Reversibility of cytotoxic edema in tacrolimus leukoencephalopathy. Pediatr Neurol 43:359–362
Zaman S R (2012) Posterior reversible encephalopathy syndrome postautologous peripheral stem cell transplantation for multiple myeloma. BMJ Case Rep 2012
Bartynski WS, Tan HP, Boardman JF, Shapiro R, Marsh JW (2008) Posterior reversible encephalopathy syndrome after solid organ transplantation. AJNR Am J Neuroradiol 29:924–930
Wong R, Beguelin GZ, de Lima M, Giralt SA, Hosing C, Ippoliti C, Forman AD, Kumar AJ et al (2003) Tacrolimus-associated posterior reversible encephalopathy syndrome after allogeneic haematopoietic stem cell transplantation. Br J Haematol 122:128–134
Graham BR, Pylypchuk GB (2014) Posterior reversible encephalopathy syndrome in an adult patient undergoing peritoneal dialysis: a case report and literature review. BMC Nephrol 15:10
Nakajima N, Ueda M, Nagayama H, Yamazaki M, Katayama Y (2013) Posterior reversible encephalopathy syndrome due to hypercalcemia associated with parathyroid hormone-related peptide: a case report and review of the literature. Intern Med 52:2465–2468
Tsang BK, Kermeen FD, Hopkins PM, Chambers DC (2010) Reversible posterior leukoencephalopathy syndrome: diagnosis and management in the setting of lung transplantation. Int Med J 40:716–720
Rabinstein AA, Mandrekar J, Merrell R, Kozak OS, Durosaro O, Fugate JE (2012) Blood pressure fluctuations in posterior reversible encephalopathy syndrome. J Stroke Cerebrovasc Dis Off J Natl Stroke Assoc 21:254–258
Fugate JE, Claassen DO, Cloft HJ, Kallmes DF, Kozak OS, Rabinstein AA (2010) Posterior reversible encephalopathy syndrome: associated clinical and radiologic findings. Mayo Clin Proc 85:427–432
Hefzy HM, Bartynski WS, Boardman JF, Lacomis D (2009) Hemorrhage in posterior reversible encephalopathy syndrome: imaging and clinical features. AJNR Am J Neuroradiol 30:1371–1379
Araz C, Camkiran A, Zeyneloglu P, Sezgin A, Moray G, Pirat A, Arslan G (2013) Early-onset posterior reversible encephalopathy syndrome after solid organ transplantation in pediatric patients: a report of 2 cases. Transplant Proc 45:3555–3557
Hugonnet E, Da Ines D, Boby H, Claise B, Petitcolin V, Lannareix V, Garcier JM (2013) Posterior reversible encephalopathy syndrome (PRES): features on CT and MR imaging. Diagn Interv Imaging 94:45–52
Zivkovic SA (2013) Neurologic complications after liver transplantation. World J Hepatol 5:409–416
Stevens CJ, Heran MK (2012) The many faces of posterior reversible encephalopathy syndrome. Br J Radiol 85:1566–1575
King JD, Rosner MH (2010) Osmotic demyelination syndrome. Am J Medi Sci 339:561–567
de Souza A (2013) Movement disorders and the osmotic demyelination syndrome. Parkinsonism Relat Disord 19:709–716
Alleman AM (2014) Osmotic demyelination syndrome: central pontine myelinolysis and extrapontine myelinolysis. Semin Ultrasound CT MR 35:153–159
Lake W, Chang JE, Kennedy T, Morgan A, Salamat S, Baskaya MK (2013) A case series of primary central nervous system posttransplantation lymphoproliferative disorder: imaging and clinical characteristics. Neurosurgery 72:960–970, discussion 970
Vegso G, Hajdu M, Sebestyen A (2011) Lymphoproliferative disorders after solid organ transplantation-classification, incidence, risk factors, early detection and treatment options. Pathol Oncol Res 17:443–454
Pruitt AA, Graus F, Rosenfeld MR (2013) Neurological complications of solid organ transplantation. Neurohospitalist 3:152–166
Fung JJ, Alessiani M, Abu-Elmagd K, Todo S, Shapiro R, Tzakis A, Van Thiel D, Armitage J et al (1991) Adverse effects associated with the use of FK 506. Transplant Proc 23:3105–3108
Hewer E, Kellner-Weldon F, Abu-Isa J, Schmitt AM (2014) Multiple cerebral lesions in a 60-year-old female patient with a history of liver transplantation. Neuropathol Off J Jpn Soc Neuropathol 34:425–427
Meriden Z, Bullock GC, Bagg A, Bonatti H, Cousar JB, Lopes MB, Robbins MK, Cathro HP (2010) Posttransplantation lymphoproliferative disease involving the pituitary gland. Hum Pathol 41:1641–1645
Baehring JM, Landry ML, Cooper D, Hui P, Bannykh S (2008) CSF IgH gene rearrangement analysis in isolated post-transplant lymphoproliferative disorder of the central nervous system. J Neuro-Oncol 86:57–60
Shah R, Bag AK, Chapman PR, Cure JK (2010) Imaging manifestations of progressive multifocal leukoencephalopathy. Clin Radiol 65:431–439
Sahraian MA, Radue EW, Eshaghi A, Besliu S, Minagar A (2012) Progressive multifocal leukoencephalopathy: a review of the neuroimaging features and differential diagnosis. Eur J Neurol Off J Eur Fed Neurol Soc 19:1060–1069
Horger M, Beschorner R, Beck R, Nagele T, Schulze M, Ernemann U, Heckl S (2012) Common and uncommon imaging findings in progressive multifocal leukoencephalopathy (PML) with differential diagnostic considerations. Clin Neurol Neurosurg 114:1123–1130
Pruitt AA, Graus F, Rosenfeld MR (2013) Neurological complications of transplantation: part I: hematopoietic cell transplantation. Neurohospitalist 3:24–38
Weissert R (2011) Progressive multifocal leukoencephalopathy. J Neuroimmunol 231:73–77
Stott VL, Hurrell MA, Anderson TJ (2005) Reversible posterior leukoencephalopathy syndrome: a misnomer reviewed. Int Med J 35:83–90
Dzudie A, Boissonnat P, Roussoulieres A, Cakmak, Mosbah K, Bejui FT, Obadia JF, Sebbag L (2009) Cyclosporine-related posterior reversible encephalopathy syndrome after heart transplantation: should we withdraw or reduce cyclosporine?: case reports. Transplant Proc 41:716–720
Munoz R, Espinoza M, Espinoza O, Andrade A, Bravo E, Gonzalez F (2006) Cyclosporine-associated leukoencephalopathy in organ transplant recipients: experience of three clinical cases. Transplant Proc 38:921–923
Heidenhain C, Puhl G, Neuhaus P (2009) Late fulminant posterior reversible encephalopathy syndrome after liver transplant. Exp Clin Transplant Off J Middle East Soc Organ Transplant 7:180–183
Schmidt D, Schachter SC (2014) Drug treatment of epilepsy in adults. BMJ 348:g254
Ruiz-Gimenez J, Sanchez-Alvarez JC, Canadillas-Hidalgo F, Serrano-Castro PJ, Andalusian Epilepsy S (2010) Antiepileptic treatment in patients with epilepsy and other comorbidities. Seizure 19:375–382
Aronow WS, Fleg JL, Pepine CJ, Artinian NT, Bakris G, Brown AS, Ferdinand KC, Ann Forciea M et al (2011) ACCF/AHA 2011 expert consensus document on hypertension in the elderly: a report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus documents developed in collaboration with the American Academy of Neurology, American Geriatrics Society, American Society for Preventive Cardiology, American Society of Hypertension, American Society of Nephrology, Association of Black Cardiologists, and European Society of Hypertension. J Am Soc Hypertens 5:259–352
Price RS, Kasner SE (2014) Hypertension and hypertensive encephalopathy. Handb Clin Neurol 119:161–167
Roth C, Ferbert A (2010) Posterior reversible encephalopathy syndrome: long-term follow-up. J Neurol Neurosurg Psychiatry 81:773–777
Siegal D, Keller A, Xu W, Bhuta S, Kim DH, Kuruvilla J, Lipton JH, Messner H et al (2007) Central nervous system complications after allogeneic hematopoietic stem cell transplantation: incidence, manifestations, and clinical significance. Biol Blood Marrow Transplant J Am Soc Blood Marrow Transplant 13:1369–1379
Prasad N, Gulati S, Gupta RK, Kumar R, Sharma K, Sharma RK (2003) Is reversible posterior leukoencephalopathy with severe hypertension completely reversible in all patients? Pediatr Nephrol 18:1161–1166
Bartynski WS (2008) Posterior reversible encephalopathy syndrome, part 2: controversies surrounding pathophysiology of vasogenic edema. AJNR Am J Neuroradiol 29:1043–1049
Dineen RA, Sibtain N, Karani JB, Lenthall RK (2008) Cerebral manifestations in liver disease and transplantation. Clin Radiol 63:586–599
Spencer CM, Goa KL, Gillis JC (1997) Tacrolimus. An update of its pharmacology and clinical efficacy in the management of organ transplantation. Drugs 54:925–975
Gerard M, Deleersnijder A, Demeulemeester J, Debyser Z, Baekelandt V (2011) Unraveling the role of peptidyl-prolyl isomerases in neurodegeneration. Mol Neurobiol 44:13–27
Ho S, Clipstone N, Timmermann L, Northrop J, Graef I, Fiorentino D, Nourse J, Crabtree GR (1996) The mechanism of action of cyclosporin A and FK506. Clin Immunol Immunopathol 80:S40–S45
Plosker GL, Foster RH (2000) Tacrolimus: a further update of its pharmacology and therapeutic use in the management of organ transplantation. Drugs 59:323–389
Schreiber SL, Crabtree GR (1992) The mechanism of action of cyclosporin A and FK506. Immunol Today 13:136–142
Dohgu S, Yamauchi A, Nakagawa S, Takata F, Kai M, Egawa T, Naito M, Tsuruo T et al (2004) Nitric oxide mediates cyclosporine-induced impairment of the blood–brain barrier in cocultures of mouse brain endothelial cells and rat astrocytes. Eur J Pharmacol 505:51–59
Kochi S, Takanaga H, Matsuo H, Naito M, Tsuruo T, Sawada Y (1999) Effect of cyclosporin A or tacrolimus on the function of blood–brain barrier cells. Eur J Pharmacol 372:287–295
Kochi S, Takanaga H, Matsuo H, Ohtani H, Naito M, Tsuruo T, Sawada Y (2000) Induction of apoptosis in mouse brain capillary endothelial cells by cyclosporin A and tacrolimus. Life Sci 66:2255–2260
Ozawa T (2008) Effects of FK506 on ca release channels (review). Perspect Med Chem 2:51–55
Wang J, Guo R, Liu S, Chen Q, Zuo S, Yang M, Zuo X (2014) Molecular mechanisms of FK506-induced hypertension in solid organ transplantation patients. Chin Med J 127:3645–3650
Cameron AM, Steiner JP, Roskams AJ, Ali SM, Ronnett GV, Snyder SH (1995) Calcineurin associated with the inositol 1,4,5-trisphosphate receptor-FKBP12 complex modulates Ca2+ flux. Cell 83:463–472
Gold BG (1997) FK506 and the role of immunophilins in nerve regeneration. Mol Neurobiol 15:285–306
Abbott NJ, Revest PA (1991) Control of brain endothelial permeability. Cerebrovasc Brain Metab Rev 3:39–72
De Bock M, Wang N, Decrock E, Bol M, Gadicherla AK, Culot M, Cecchelli R, Bultynck G et al (2013) Endothelial calcium dynamics, connexin channels and blood–brain barrier function. Prog Neurobiol 108:1–20
Hawkins BT, Davis TP (2005) The blood–brain barrier/neurovascular unit in health and disease. Pharmacol Rev 57:173–185
Huber JD, Egleton RD, Davis TP (2001) Molecular physiology and pathophysiology of tight junctions in the blood–brain barrier. Trends Neurosci 24:719–725
Stuart RO, Sun A, Bush KT, Nigam SK (1996) Dependence of epithelial intercellular junction biogenesis on thapsigargin-sensitive intracellular calcium stores. J Biol Chem 271:13636–13641
Dohgu S, Sumi N, Nishioku T, Takata F, Watanabe T, Naito M, Shuto H, Yamauchi A et al (2010) Cyclosporin A induces hyperpermeability of the blood–brain barrier by inhibiting autocrine adrenomedullin-mediated up-regulation of endothelial barrier function. Eur J Pharmacol 644:5–9
Fernandes S, Salta S, Bravo J, Silva A P, Summavielle T (2014). Acetyl-L-carnitine prevents methamphetamine-induced structural damage on endothelial cells via ILK-related MMP-9 activity. Mol Neurobiol
Ishizaki T, Chiba H, Kojima T, Fujibe M, Soma T, Miyajima H, Nagasawa K, Wada I et al (2003) Cyclic AMP induces phosphorylation of claudin-5 immunoprecipitates and expression of claudin-5 gene in blood–brain-barrier endothelial cells via protein kinase A-dependent and -independent pathways. Exp Cell Res 290:275–288
Dohgu S, Takata F, Matsumoto J, Oda M, Harada E, Watanabe T, Nishioku T, Shuto H et al (2011) Autocrine and paracrine up-regulation of blood–brain barrier function by plasminogen activator inhibitor-1. Microvasc Res 81:103–107
Juhan-Vague I, Alessi MC, Mavri A, Morange PE (2003) Plasminogen activator inhibitor-1, inflammation, obesity, insulin resistance and vascular risk. J Thromb Haemost 1:1575–1579
Ko HM, Lee SH, Kim KC, Joo SH, Choi WS, Shin CY (2015) The role of TLR4 and Fyn interaction on lipopolysaccharide-stimulated PAI-1 expression in astrocytes. Mol Neurobiol 52:8–25
Dohgu S, Kataoka Y, Ikesue H, Naito M, Tsuruo T, Oishi R, Sawada Y (2000) Involvement of glial cells in cyclosporine-increased permeability of brain endothelial cells. Cell Mol Neurobiol 20:781–786
Takata F, Dohgu S, Yamauchi A, Sumi N, Nakagawa S, Naito M, Tsuruo T, Shuto H et al (2007) Inhibition of transforming growth factor-beta production in brain pericytes contributes to cyclosporin A-induced dysfunction of the blood–brain barrier. Cell Mol Neurobiol 27:317–328
Muzi M, Mankoff DA, Link JM, Shoner S, Collier AC, Sasongko L, Unadkat JD (2009) Imaging of cyclosporine inhibition of P-glycoprotein activity using 11C-verapamil in the brain: studies of healthy humans. J Nucl Med Off Publ Soc Nucl Med 50:1267–1275
Gurkan A, Emingil G, Oktem G, Selvi N, Afacan B, Tunc I, Toz H, Atilla G (2009) Immunohistochemical analysis of inducible and endothelial forms of nitric oxide synthase in cyclosporin A-induced gingival overgrowth. J Periodontol 80:1638–1647
Papachristou E, Papadimitropoulos A, Kotsantis P, Goumenos DS, Katsoris PG, Vlachojannis JG (2010) Interaction of endothelin-1 and nitric oxide pathways in human tubular epithelial cells under the influence of cyclosporine-A. Ren Fail 32:727–732
Ramzy D, Rao V, Tumiati LC, Xu N, Miriuka S, Delgado D, Ross HJ (2006) Role of endothelin-1 and nitric oxide bioavailability in transplant-related vascular injury: comparative effects of rapamycin and cyclosporine. Circulation 114:I214–I219
Yang L, Yang XC, Yang JK, Guo YH, Yi FF, Fan Q, Liu XL (2008) Cyclosporin A suppresses proliferation of endothelial progenitor cells: involvement of nitric oxide synthase inhibition. Intern Med 47:1457–1464
Minguillon J, Morancho B, Kim SJ, Lopez-Botet M, Aramburu J (2005) Concentrations of cyclosporin A and FK506 that inhibit IL-2 induction in human T cells do not affect TGF-beta1 biosynthesis, whereas higher doses of cyclosporin A trigger apoptosis and release of preformed TGF-beta1. J Leukoc Biol 77:748–758
Kalayci R, Kaya M, Uzun H, Bilgic B, Ahishali B, Arican N, Elmas I, Kucuk M (2009) Influence of hypercholesterolemia and hypertension on the integrity of the blood–brain barrier in rats. Int J Neurosci 119:1881–1904
Mayhan WG (1995) Role of nitric oxide in disruption of the blood–brain barrier during acute hypertension. Brain Res 686:99–103
Mohammadi MT, Shid Moosavi SM, Dehghani GA (2011) Contribution of nitric oxide synthase (NOS) activity in blood–brain barrier disruption and edema after acute ischemia/reperfusion in aortic coarctation-induced hypertensive rats. Iran Biomed J 15:22–30
Nukhet Turkel A, Ziya Ziylan Y (2004) Protection of blood–brain barrier breakdown by nifedipine in adrenaline-induced acute hypertension. Int J Neurosci 114:517–528
Pires PW, Dams Ramos CM, Matin N, Dorrance AM (2013) The effects of hypertension on the cerebral circulation. Am J Physiol Heart Circ Physiol 304:H1598–H1614
Poulet R, Gentile MT, Vecchione C, Distaso M, Aretini A, Fratta L, Russo G, Echart C et al (2006) Acute hypertension induces oxidative stress in brain tissues. J Cereb Blood Flow Metab Off J Int Soc Cereb Blood Flow Metab 26:253–262
Mohammadi MT, Dehghani GA (2014) Acute hypertension induces brain injury and blood–brain barrier disruption through reduction of claudins mRNA expression in rat. Pathol Res Pract 210:985–990
Wilasrusmee C, Da Silva M, Siddiqui J, Bruch D, Kittur S, Wilasrusmee S, Kittur DS (2003) Role of endothelin-1 in microvascular dysfunction caused by cyclosporin A. J Am Coll Surg 196:584–591
Cauduro RL, Costa C, Lhulier F, Garcia RG, Cabral RD, Goncalves LF, Manfro RC (2005) Endothelin-1 plasma levels and hypertension in cyclosporine-treated renal transplant patients. Clin Transpl 19:470–474
Arii T, Kamiya T, Arii K, Ueda M, Nito C, Katsura KI, Katayama Y (2001) Neuroprotective effect of immunosuppressant FK506 in transient focal ischemia in rat: therapeutic time window for FK506 in transient focal ischemia. Neurol Res 23:755–760
Kumar P, Kalonia H, Kumar A (2010) Possible nitric oxide modulation in protective effect of FK-506 against 3-nitropropionic acid-induced behavioral, oxidative, neurochemical, and mitochondrial alterations in rat brain. Drug Chem Toxicol 33:377–392
Toung TJ, Bhardwaj A, Dawson VL, Dawson TM, Traystman RJ, Hurn PD (1999) Neuroprotective FK506 does not alter in vivo nitric oxide production during ischemia and early reperfusion in rats. Stroke J Cereb Circ 30:1279–1285
Boger RH (2007) The pharmacodynamics of L-arginine. J Nutr 137:1650S–1655S
Puschel A, Lindenblatt N, Katzfuss J, Vollmar B, Klar E (2012) Immunosuppressants accelerate microvascular thrombus formation in vivo: role of endothelial cell activation. Surgery 151:26–36
Chiasson VL, Quinn MA, Young KJ, Mitchell BM (2011) Protein kinase CbetaII-mediated phosphorylation of endothelial nitric oxide synthase threonine 495 mediates the endothelial dysfunction induced by FK506 (tacrolimus). J Pharmacol Exp Ther 337:718–723
Agrawal S, Dixit A, Singh A, Tripathi P, Singh D, Patel DK, Singh MP (2015) Cyclosporine A and MnTMPyP alleviate alpha-synuclein expression and aggregation in cypermethrin-induced Parkinsonism. Mol Neurobiol 52:1619–1628
Gottschalk S, Cummins CL, Leibfritz D, Christians U, Benet LZ, Serkova NJ (2011) Age and sex differences in the effects of the immunosuppressants cyclosporine, sirolimus and everolimus on rat brain metabolism. Neurotoxicology 32:50–57
Serkova NJ, Christians U, Benet LZ (2004) Biochemical mechanisms of cyclosporine neurotoxicity. Mol Interv 4:97–107
Dohgu S, Nishioku T, Sumi N, Takata F, Nakagawa S, Naito M, Tsuruo T, Yamauchi A et al (2007) Adverse effect of cyclosporin A on barrier functions of cerebral microvascular endothelial cells after hypoxia-reoxygenation damage in vitro. Cell Mol Neurobiol 27:889–899
Author information
Authors and Affiliations
Corresponding author
Additional information
Sheng Chen and Jun Hu contributed equally to this work.
Rights and permissions
About this article

Cite this article
Chen, S., Hu, J., Xu, L. et al. Posterior Reversible Encephalopathy Syndrome After Transplantation: a Review. Mol Neurobiol 53, 6897–6909 (2016). https://doi.org/10.1007/s12035-015-9560-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12035-015-9560-0