
Abstract
Internal hernias are a worrying complication from laparoscopic Roux-en-Y gastric bypass (LRGB), with potential small bowel necrosis and obstruction. An electronic database search of Medline, Embase, and Pubmed was performed. All studies investigating the internal hernia rates in patients whose mesenteric defects were closed vs. not closed during LRGB were analysed. Odds ratios were calculated to assess the difference in internal hernia rate. A total of 14 studies totalling 20,553 patients undergoing LRGB were included. Internal hernia rate (220/12,445 (2%) closure vs. 509/8108 (6%) non-closure) and re-operation for small bowel obstruction (86/5437 (2%) closed vs. 300/3132 (10%) non-closure) were reduced when defects were closed. There was no difference observed when sutures were used to close the defects compared to clips/staples.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The prevalence of obesity is increasing, and the latest estimated figures from the World Health Organisation shows that over 650 million adults worldwide are classified as living with obesity [1]. Bariatric surgery remains an increasingly popular method for weight-loss in morbid obesity, with encouraging results alongside improved quality of life and reduced mortality [2]. Within bariatric procedures, laparoscopic Roux-en-Y gastric bypass (LRGB) remains one of the most commonly performed procedures [3], being the second most performed procedure over the last decade [4]. However despite this, practice of LRGB varies between centres within particular aspects of the operation, such as the position of the roux limb as well as the closure of mesenteric defects [5]. The latter technique has been increasingly performed in recent times in an effort to reduce internal hernias, a complication of LRGB occurring in over 10% of cases [6]. Due to the varying nature of internal hernia presentation, diagnosis can be challenging non-invasively, resulting in delayed treatment and high levels of morbidity [7]. In severe circumstances, internal hernias can present with small bowel obstruction requiring urgent surgical intervention, commonly occurring 1–2 years after the initial LRGB when mesenteric fat loss increases [8]. The debate of whether closure of the defects formed at LRGB (Petersen’s and jejunojejunostomy (J-J) site) reduces internal hernia rate has been long-standing, and the first randomised trials investigating closure vs. no closure of mesenteric defects reported a reduced internal hernia rate in the closed cohort [8, 9]. Consequently, the closure of mesenteric defects has been increasingly performed [5, 10].
A recent international survey was conducted investigating practice regarding mesenteric defect closure within bariatric units worldwide [11]. This large multicentre survey demonstrated a large majority of surgeons who responded (91.8%) opted to always close the mesenteric defects in LRGB, normally using non-absorbable sutures. Despite this, there remained a significant number of responders who opted to either not close, or to selectively close the mesenteric defects. Furthermore, a large amount of heterogeneity was observed in reasoning for not closing the defects, including believing the internal hernia rate would not be affected, or that the benefits of closing did not outweigh the risks [11]. This survey also demonstrated conflicted opinion over the optimum method for closing mesenteric defects, with no conclusions made.
Thus, the findings of this survey [11] have demonstrated a requirement for an understanding of the literature on whether closure of mesenteric defects is associated with a reduced internal hernia rate. Within the literature, the most recent reviews [12, 13] suggested a reduced internal hernia rate where mesenteric defects were closed as well as a reduced rate of small bowel obstruction; however, these studies were limited by few studies (both less than 10) and only two randomised controlled-trials. Furthermore, there was uncertainty over the finding of an increased rate of small bowel obstruction not due to an internal hernia in the closure group.
This up-to-date systematic review and meta-analysis aims to confirm the association between internal hernia rate and mesenteric defect closure, as well as note any other morbidities associated between closure and non-closure techniques.
Methods
Search Strategy
Electronic searches were performed using Ovid Medline, EMBASE and the Web of science from inception until 10/12/2022. This was performed by two authors (DM and BC), using the terms: (‘Roux-en-Y gastric bypass’ or ‘RYGB’) and (‘mesenteric defects’ or ‘mesenteric defect closure’ or ‘Petersen’s’ or ‘jejunojejunostomy’) and (‘internal hernia’ or ‘hernia’ or ‘small bowel obstruction). A subsequent manual review of references identified other studies.
Study Selection
Inclusion criteria were the following:
-
All patients undergoing a LRGB for obesity.
-
A comparison of cases where one cohort’s mesenteric defects were closed, and the other had at least one mesenteric defect left open at surgery.
-
Randomised controlled trials (RCTs) and observational studies
Exclusion criteria were the following:
-
Any study not in English
-
No full-text available
-
Abstracts, case reports, and non-peer review submissions
Data Extraction and Statistical Analysis
DM and BC independently extracted relevant outcome data from included studies. The data included the following: internal hernia rate, Petersen’s hernia rate, J-J hernia rate and reoperation for suspected small bowel obstruction.
The primary outcome was the rate of internal hernia in patients who underwent mesenteric defect closure vs. non-closure. Secondary outcomes included the specific location of the internal hernia (Petersen’s vs. J-J) and reoperation for suspected small bowel obstruction.
For each categorical complication, the odds ratio (OR) and 95% confidence interval (CI) were calculated from reported events in included studies. Both fixed-effect and random-effect models (Mantel–Haenszel statistical method) were used where appropriate. Review Manager 5.4 (Rev.Man ver 5.4.1, Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2020) was used for analysis and figure production. An outcome shifted towards the left of a figure suggested the frequency was higher in the non-closure group. Heterogeneity was assessed using the I2 statistic. A score of 0–50% was categorised as low heterogeneity, 50–75% as medium, and over 75% as high. Studies were removed individually, and the effect this had on heterogeneity noted. Furthermore, studies were categorised into subgroups of RCTs alone, observational studies alone, suture/stapler method of closure, and antecolic/retrocolic position of the roux limb to note any additional effect this had on heterogeneity (Fig. 1, 2, 3, 4, 5).

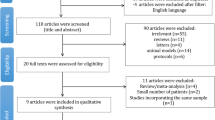
PRISMA guided flow diagram of study selection for inclusion in this meta-analysis

Forest plot in the comparison of closure vs. non-closure in mesenteric defects in LRGB for internal hernia rates accounting for all studies included

Funnel plots of studies included in the meta-analysis. A Internal hernia rates. B Reoperation for suspected small bowel obstruction

Forest plot in the comparison of closure vs. non-closure in mesenteric defects in LRGB for internal hernia rates: A at Petersen’s defect, B at J-J defect

Forest plot in the comparison of closure vs. non-closure in mesenteric defects in LRGB in studies measuring outcomes of suspected small bowel obstruction
Publication bias was assessed using visualisation of funnel plot asymmetry [14].
Risk of Bias and Quality Assessment
DM and BC independently calculated risk of bias and quality assessment for included studies. Where disagreement was encountered, a third reviewer (CC) was consulted. For randomised trials, the risk of bias was assessed using the Cochrane tool that categorises studies into low, unclear and high risk of bias. For observational studies, the Newcastle–Ottawa score was used [15]. This assessment tool rates studies out of a maximum nine stars for methodological quality. The quality of evidence provided by studies was assessed using the grade working group [16] system rating the evidence as very low, low, moderate and high (Fig. 6).

Risk of bias assessed via Cochrane tool for studies included in this meta-analysis
Results
The initial search yielded 349 citations, and the process of study selection is summarised in Fig. 1. Screening for inclusion and exclusion criteria resulted in 14 studies that were included in this meta-analysis resulting in 20,553 patients being assessed. There were no disagreements on included studies between the two independent reviewers. Of these, three were randomised-controlled trials [8, 9, 17] with the remaining being observational cohort studies [18,19,20,21,22,23,24,25,26,27,28]. Basic study demographics and study findings can be visualised in Table 1. All studies compared a group where all defects were closed, to a group where at least one mesenteric defect was not closed. All included studies suspected an internal hernia clinically or radiologically, and confirmed this at operation. Both antecolic and retrocolic roux limb outcomes were assessed in two studies [20, 25], whilst the remaining studies used solely an antecolic roux limb [8, 17, 19, 21,22,23,24, 26, 28]. A non-absorbable running suture was used in 10 studies [8, 18,19,20,21, 23,24,25,26, 28], two used non-absorbable interrupted sutures [9, 27], and the final two studies used a stapler [22] and clips [17]. Overall methodological quality of cohort studies can be seen in Table 1, with the quality assessment of the RCTs being visualised in Table 2.
Internal Hernia Rate
The overall rate of internal hernia in the closure group was 1.78%, compared to an internal hernia rate of 6.28% in the non-closure group (p = 0.003). Further analysis confirmed the reduction of internal hernia rate in the closure group compared to non-closure by an odds ratio calculation of 0.33 (95% CI 0.29–0.39, p ≤ 0.01). Calculated I2 = 83% (p ≤ 0.01), which indicated severe heterogeneity between the studies (Fig. 2). There was no difference visualised when individual studies were removed from this analysis to account for the significant heterogeneity present. A sensitivity analysis was performed investigating observational studies alone compared to RCTs. Within cohort studies alone (n = 11), overall internal hernia rate was lower in closure cohorts (OR 0.34, 95% CI 0.29–0.41, p = < 0.01), I2 = 87%, p ≤ 0.01. This was comparable to RCTs alone, also showing a lower internal hernia rate in closure cohorts (OR 0.31, 95% CI 0.21–0.44, p ≤ 0.01), I2 = 0%, p = 0.79). A funnel plot displaying all studies showed the majority of studies to fall within the 95% CI of the funnel as well as being symmetrical, indicating a low level of publication bias (Fig. 3A).
Internal Hernia Site
Studies were further analysed by calculating the rates of internal hernia at specific sites—notably Petersen’s defect and the J-J defect. With respect to Petersen’s defect, this was reported by 12 studies [8, 9, 17,18,19, 21,22,23, 25,26,27,28], totalling 18,173 patients, 3 RCTs and 9 cohort studies. The rate of internal hernia was significantly lower in the closure cohort (OR 0.26, 95% CI 0.20–0.34, p ≤ 0.01) with a calculated I2 = 29%, p = 0.17 (Fig. 4A).
J-J specific internal hernias were reported in eleven studies [8, 9, 17,18,19, 21,22,23, 25, 26, 28], 3 RCTs and 8 cohort studies (17,608 patients). A reduced rate of internal hernias was found in the closure group (OR 0.21, 95% CI 0.17–0.27) with medium calculated heterogeneity (I2 = 53%, p = 0.02) (Fig. 4B).
Reoperation for Small Bowel Obstruction
Reoperation for suspected small bowel obstruction was reported in three studies [21, 22, 26]. This included 6294 patients. There was found to be a significantly lower rate of reoperation for small bowel obstruction in the closure group compared to the non-closure group (OR 0.14, 95% CI 0.11–0.19, p ≤ 0.01). Calculated heterogeneity was medium (I2 = 74%, p = 0.02) (Fig. 5A). There was no difference in heterogeneity when individual studies were removed. Examining the funnel plot data for this outcome shows some asymmetry, which is likely due to the small number of studies specifically reporting this outcome (Fig. 3B).
Method of Repair
A further subgroup analysis was performed investigating the mode of mesenteric defect closure. Sutures were used in 12 studies [8, 9, 18,19,20,21, 23,24,25,26,27,28], normally non-absorbable running sutures. This included 16,142 patients. The overall internal hernia rate favoured the closure group (OR 0.37, 95% CI 0.31–0.45, p ≤ 0.01). Calculated heterogeneity was high (I2 = 83%, p ≤ 0.01). For reoperation for small bowel obstruction, two of the reporting studies used a suture closure [18, 23]. This showed there to be no difference between the two cohorts (OR 0.54, 95% CI 0.21–1.44, p = 0.22) and heterogeneity was low (I2 = 0%, p = 0.93).
One remaining study used clips for closure [17], and the other used staples [22]. For the purposes of this subgroup analysis, they were analysed together. This included 4411 patients. The overall rate of internal hernia was significantly less in the closure group (OR 0.25, 95% CI 0.18–0.34, p = < 0.01) with a low level of heterogeneity (I2 = 45%, p = 0.18). Due to only one of these reporting studies reporting reoperation for small bowel obstruction [22], no analyses could be performed.
A Mann–Whitney U test was performed comparing the rates of internal hernia in sutures vs. other techniques, with p = 0.23.
Discussion
This meta-analysis presents the most up-to-date review of studies comparing closure to non-closure of mesenteric defects in LRGB. We have included 8000 more patients (total included patient number = 20,553) than when this subject was previously reviewed [12, 13], allowing this review to further understanding on this debated topic. All included studies recorded the rate of internal hernia, suspected clinically/radiologically, and proven at operation. Our analysis has shown that when compared to non-closure, the closure of mesenteric defects is associated with a lower rate of internal hernia. All of our included studies had a maximum follow-up time of between 2 and 5.5 years (Table 1). The most likely time for an internal hernia to present is 1–2 years post-LRGB (due to mesenteric fat loss being greatest in this time); thus, all included studies can be said to present adequate follow-up time to investigate internal hernia rate.
Our findings of an association between mesenteric defect closure and reduced internal hernia rate (OR 0.33, 95% CI 0.29–0.39) was shown to be the case for hernias occurring at both Petersen’s and the J-J defect. Furthermore, we found a lower rate of reoperation for suspected small bowel obstruction in patients with closed mesenteric defects.
The findings of this review are in keeping with older reviews on the topic [12, 13], who also found a lower internal hernia rate in the closure cohort. It is reassuring that our more recent review which contains 6 further studies, including a RCT, shows similar results to previous work on the subject, as this strengthens the findings and the suggestion that all mesenteric defects should be closed at LRGB. Previous work has described limitations of small numbers of studies included, which our paper has overcome by having an increased number of papers (and thus patients) included. By including a larger number of new patients in this review, the likelihood of the associations demonstrated between closure of mesenteric defects and the rate of internal hernia are strengthened.
Internal hernias are a genuine concern to all when a LRGB is performed [2], with a risk of small bowel obstruction, as well as ischaemia and eventual necrosis. This review has shown an internal hernia rate of 2% in the closure group, compared to 6% in non-closure. Despite this overall rate being lower than that reported by individual studies, it remains a relatively common complication, requiring reoperation with an associated high morbidity [29]. With the associations demonstrated in this review, the number of patients presenting with a clinically significant internal hernia can be reduced to 1/3 if the mesenteric defects are closed. Furthermore, our results have shown that there is a significantly less chance of patients undergoing a reoperation for suspected small bowel obstruction if the mesenteric defects have been closed. The reasons for this are likely twofold, the first being that the likelihood of an internal hernia actually being present is reduced if the defects are closed (as highlighted by this review as well as previous work). The second involves influencing the individual surgeon’s opinion on whether the patient undergoes a reoperation. If the patient is known to have closed defects, then the individual surgeon may decide to delay a reoperation for small bowel obstruction, thus potentially giving the patient’s symptoms time to settle. As internal hernias can present with varied symptoms, the decision to reoperate is surgeon specific and will vary greatly between centres. As demonstrated recently [11], there remains large variety in clinical practice surrounding LRGB globally, with a proportion of surgeons not routinely closing mesenteric defects, and no consensus on which material should be used for closure. Thus, it is likely that the decision for reoperation for suspected internal hernia, and the timing of reoperation, will vary greatly internationally. However, we have demonstrated an association between reduced internal hernia rate and closure of mesenteric defects; therefore, closure of mesenteric defects is associated with a reduced number of operations performed. This has huge benefits for patients who do not have to undergo a further operation, aiding them both from a morbidity perspective as well as not experiencing the mental burden of reoperation. Furthermore, there are significant financial benefits from reducing total operation number. In a pressured health system, a reduced number of unplanned reoperations can have a significant impact on its longevity. Despite these positive findings, the quality of evidence on reoperation for suspected small bowel obstruction number in this review remains low. This is due to only three studies reporting this outcome, and all three studies analysing their data retrospectively.
One of the review’s subgroups investigated the different methods of closing the mesenteric defects. As referenced previously, there is currently no agreed consensus on the optimal technique to close mesenteric defects during LRGB [11]. The majority of studies included used non-absorbable sutures (16,142 patients) to close both defects, with only two studies using other methods. Both methods had a satisfactory outcome, with there being no difference in the overall internal hernia rate of the closed groups (p = 0.23). In previous literature, there have been suggestions to further investigate the method of mesenteric closure, and it is reassuring to see that despite being the preferred option in the literature, clips and staplers are demonstrating positive results with no difference when compared to sutures. One study [17] which used clips for closure was one of the three RCTs included in this meta-analysis. This demonstrates a high quality of evidence for the use of this technique in mesenteric defect closure, and that it is being utilised in LRGB, alongside the more common reported technique of suture closure. Due to the lack of studies describing other techniques, the quality of evidence on this point remains low, and should be investigated in further studies. This would ideally take the form of a randomised controlled trial, with patients randomised to one arm of suture closure, to the other of clips/stapler closure.
Despite the findings of a reduced internal hernia rate at both Petersen’s and the jejunojejunostomy defects and a lower reoperation rate in the closure group found in this review, there are some limitations. The first of these is a high reported level of heterogeneity in our primary outcome. This did not resolve by removing individual studies or by analysing RCTs vs. cohort studies. It is likely that this is due to the varying number of participants in individual studies. However, the lower level of heterogeneity observed when studies reported internal hernias at individual sites strengthens the argument that closing mesenteric defects is in fact associated with a reduced internal hernia rate. A further limitation is analysing the position of the roux limb. In our study, all studies except two [20, 25] solely reported on an antecolic roux limb position, and this position is becoming more popular compared to retrocolic over time. Of the remaining two studies, they reported a combination of antecolic and retrocolic roux limbs, thus retrocolic cases alone could not be analysed. It cannot be said that the position of the roux limb in these studies is affecting the outcomes, nor can this review comment on the benefit of roux limb position in terms to internal hernia rate. However, as the trend towards antecolic roux limbs increases as time progresses, it is likely that studies will continue to report on this preferred technique compared to the retrocolic limb technique, thus there is no clear solution to this potential limitation.
Conclusions
This systematic review and meta-analysis presents the most recent review of the topic of mesenteric defect closure in LRGB, with more than 8000 new patients. Despite varying opinions on closure globally and the absence of specified guidelines, we have demonstrated a reduced internal hernia rate at both Petersen’s and the J-J defect, as well as a reduced rate of reoperation for suspected small bowel obstruction when defects are closed.
References
World Health Organisation, Obesity and overweight, Updated 09/06/21. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight Accessed on 10/12/22
Castellana M, Procino F, Biacchi E, et al. Roux-en-Y gastric bypass vs sleeve gastrectomy for remission of type 2 diabetes. J Clin Endocrinol, Metab. 2021;106(3):922–33.
Angrisani L, Santonicola A, Iovino P, et al. Bariatric surgery and endoluminal procedures: IFSO worldwide survey 2014. Obes Surg. 2017;27(9):2279–89.
Alawan A, Friedman J, Park H, et al. US national trends in bariatric surgery: a decade of study. Surgery. 2021;170(1):13–7.
Dang J, Deprato A, Verhoeff K, et al. Variation of laparoscopic Roux-en-Y gastric bypass techniques: a survey of 518 bariatric surgeons. Obes Surg. 2022;32(7):2357–65.
Geubbels N, Lijftogt N, Fiocco M, et al. Meta-analysis of internal herniation after gastric bypass surgery. Br J Surg. 2015;102(5):451–60.
Lockhart M, Tessler F, Canon C, et al. Internal hernia after gastric bypass: sensitivity and specificity of seven CT findings with surgical correlation and controls. AJR AM J Roentgenol. 2007;188(3):745–50.
Stenberg E, Szabo E, Ågren G, et al. Closure of mesenteric defects in laparoscopic gastric bypass: a multicentre, randomised, parallel, open-label trial. Lancet. 2016;387(10026):1397–404.
Rosas U, Ahmed S, Leva N, et al. Mesenteric defect closure in laparoscopic Roux-enY gastric bypass: a randomized controlled trial. Surg Endosc. 2015;29(9):2486–90.
Madan AK, Harper JL, Tichansky DS. Techniques of laparoscopic gastric bypass: on-line survey of American Society for Bariatric Surgery practicing surgeons. Surg Obes Relat Dis. 2008;4(2):166–72.
Mohammadi-Zaniani G, Quake S, Musbahi A, et al. Establishing methods of defect closure in Roux-en-Y gastric bypass: an international survey. Obes Surg. 2023;33(4):1049–59. https://doi.org/10.1007/s11695-022-06420-2.
Hajibandeh S, Hajibandeh S, Abdelkarim A, et al. Closure versus non-closure of mesenteric defects in laparoscopic Roux-en-Y gastric bypass: a systematic review and meta-analysis. Surg Endosc. 2020;34(8):3306–20.
Magouliotis D, Tzovaras G, Tasiopoulou V, et al. Closure of mesenteric defects in laparoscopic gastric bypass: a meta-analysis. Obes Surg. 2020;30(5):1935–43.
Sterne JAC, Egger M, Moher D. Chapter 10: addressing reporting biases. In: Higgins JPT, Green S (eds). Cochrane handbook for systematic reviews of intervention. Version 5.1.0. The Cochrane Collaboration, 2011, www.handbook.cochrane.org (12 December 2022, date last accessed)
Lo C, Mertz D, Loeb M. Newcastle-Ottawa Scale: comparing reviewers’ to authors’ assessments. BMC Med Res Methodol. 2014;14:45.
Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64:401–6.
Kristensen S, Gormsen J, Naver L, et al. Randomized clinical trial on closure versus non-closure of mesenteric defects during laparoscopic gastric bypass surgery. Br J Surg. 2021;108(2):145–51.
De la Cruz-Munoz N, Cabrera J, Cuesta M, et al. Closure of mesenteric defect can lead to decrease in internal hernias after Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2011;7:176–80.
Amor I, Kassir R, Debs T, et al. Impact of mesenteric defect closure during laparoscopic roux-en-y gastric bypass (LRYGB): a retrospective study for a total of 2093 LRYGB. Obes Surg. 2019;29(10):3342–7.
Obeid A, McNeal S, Breland M, et al. Internal hernia after laparoscopic Roux-en-Y gastric bypass. J Gastrointest Surg. 2014;18(2):250–5 (discussion 255–256).
Chowbey P, Baijal M, Kantharia N, et al. Mesenteric defect closure decreases the incidence of internal hernias following laparoscopic roux-En-Y gastric bypass: a retrospective cohort study. Obes Surg. 2016;26(9):2029–34.
Aghajani E, Nergaard B, Leifson B, et al. The mesenteric defects in laparoscopic Roux-en-Y gastric bypass: 5 years follow-up of non-closure versus closure using the stapler technique. Surg Endosc. 2017;31(9):3743–8.
Rodriguez A, Mosti M, Sierra M, et al. Small bowel obstruction after antecolic and antegastric laparoscopic Roux-en-Y gastric bypass: could the incidence be reduced? Obes Surg. 2020;20:1380–4.
Nuytens F, D’Hondt M, Van Rooy F, et al. Closure of mesenteric defects is associated with a higher incidence of small bowel obstruction due to adhesions after laparoscopic antecolic Roux-en-y gastric bypass: a retrospective cohort study. Int J Surg. 2019;71:149–55.
Ribeiro-Parenti L, Arapis K, Chosidow D, et al. Gastrojejunostomy stricture rate: comparison between antecolic and retrocolic laparoscopic Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2015;11(5):1076–84.
Schneider R, Schulenberg M, Kraljevic M. Does the non-absorbable suture closure of the jejunal mesenteric defect reduce the incidence and severity of internal hernias after laparoscopic Roux-en-Y gastric bypass? Langenbecks Arch Surg. 2021;406(6):1831–8.
Lopera C, Vergnaud J, Cabrera L. Preventative laparoscopic repair of Petersen’s space following gastric bypass surgery reduces the incidence of Petersen’s hernia: a comparative study. Hernia. 2018;22(6):1077–81.
Blockhuys M, Gypen B, Heyman S. Internal hernia after laparoscopic gastric bypass: effect of closure of the Petersen defect - single-center study. Obes Surg. 2019;29(1):70–5.
Higa K, Ho T. Boone K, Internal hernias after laparoscopic Roux-en-Y gastric bypass: incidence, treatment and prevention. Obes Surg. 2003;13:350–4.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics Approval
Utilisation of the NHS Research Ethics Committee tool provided by the Medical Research Council determined that ethical approval was not required for this study as this was a meta-analysis and systematic review of published research.
Consent to Participate
Informed consent does not apply.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Key Points
• Closure of mesenteric defects is associated with lower internal hernia rates post LRGB.
• No significant difference in internal hernia rates between sutures or staples for defect closure.
• Closure of mesenteric defects resulted in fewer reoperations for suspected small bowel obstruction post LRGB.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Muir, D., Choi, B., Clements, C. et al. Mesenteric Defect Closure and the Rate of Internal Hernia in Laparoscopic Roux-en-Y Gastric Bypass: A Systematic Review and Meta-analysis. OBES SURG 33, 2229–2236 (2023). https://doi.org/10.1007/s11695-023-06597-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-023-06597-0