
Abstract
Objectives
This network meta-analysis compares different lasers, placebo, and no treatment in terms of their effects on dentine hypersensitivity (DH) immediately after treatment and over the long term (1 month).
Methods
A systematic electronic literature search of four databases and a manual search were performed to identify randomized controlled trials (RCTs) examining different laser treatments for the treatment of DH. Pairwise and network meta-analyses were performed to analyze the desensitization effect immediately after treatment and over the long term. The risk of bias was assessed based on the Cochrane guidelines and funnel plots. The quality of the evidence, statistical heterogeneity, inconsistencies, and ranking probability were also evaluated.
Results
A total of 11 RCTs were included in the network meta-analysis; 11 and 9 of these studies analyzed immediate and long-term effects, respectively. All four types of laser had a better desensitizing effect than controls immediately after treatment and over the long term, but there were no significant differences among the four different lasers. There was a significant placebo effect immediately after treatment. The laser with the highest probability of being the most effective treatment for DH was Er,Cr:YSGG immediately after treatment and over the long term (73% and 47%, respectively).
Conclusions
All four types of laser had significantly better effects than no treatment on DH immediately after treatment and in the long term, but there were no significant differences among the four lasers. In addition, there was a significant placebo effect, supporting the importance of including a placebo group in future studies. Furthermore, Er,Cr:YSGG may be the most effective laser for the treatment of DH immediately and over the long term.
Clinical relevance
This study used network meta-analyses to compare different lasers, placebo, and no treatment over different time periods, which is to provide guidance for selecting an appropriate laser treatment in patients with DH.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Dentine hypersensitivity (DH) is a common oral symptom characterized by short and sharp pain when exposed dentine of the affected tooth receives external stimulation [1]. People of any age can suffer from DH, but middle-aged individuals are particularly susceptible [2]. Any tooth can suffer from DH, but it mostly occurs in canines and premolars [3]. In addition, the incidence of DH is greater among women than among men [2]. DH is mainly caused by occlusal wear, acid erosion, or wedge defects of the tooth neck, which leads to loss of enamel and/or the cementum layer and dentine exposure [4]. The hydrodynamic theory is the most widely accepted mechanism of DH, which was proposed by Brannstrom and Astrom [5]. Many treatments for DH have been proposed to reduce fluid flow in the dentine tubules or block pulpy nerve impulses [6, 7].
Lasers are a promising method for the treatment of DH. Various types of laser have been used for DH treatment, including GaAlAs, Nd:YAG, Er:YAG, Er,Cr:YSGG, and CO2 lasers with different wavelengths [8,9,10,11,12]. Their effectiveness ranges from 5.2 to 100% depending on the laser type and parameters [13]. The mechanism of laser desensitization is melting and recrystallizing the dentine tubules and closing the dentine tubules or causing physiological changes in the pulpy never fibers inside the dentine tubules [14, 15]. Advantages of laser therapy for the treatment of DH include reliability, immediacy, and having a reproducible analgesic effect [13, 16].
Previous systematic reviews and meta-analyses have analyzed the efficacy of lasers for the treatment of DH [17,18,19,20]. However, these have had some limitations. For example, previous meta-analyses only examined the desensitization effects of lasers or low-power lasers without specifically classifying the lasers [17, 18]. Secondly, some previous reports only considered the long-term desensitization effects of lasers without evaluating the immediate effect. In addition, the final follow-up time of these studies varied, which may lead to bias [19, 20]. Furthermore, these previous works included studies related to DH periodontal maintenance or were performed after bleaching, which may bias the results. Moreover, these reports did not provide relevant rankings of the desensitization effects of the different lasers.
Network meta-analysis (also known as multiple treatment comparison) allows us to synthesize data from both direct and indirect comparisons of various regimens [21, 22]. Clinicians should consider all data that may be relevant when comparing different treatment options and multiple treatment comparisons can be performed with a wide network of studies [23]. Furthermore, Bayesian approaches allow us to estimate the rank probability [22]. However, to the best of our knowledge, no network meta-analysis has been performed on DH of different laser therapies. Therefore, it is important to perform a more comprehensive systematic review and network meta-analysis on the effects of different lasers on DH and to provide relevance rankings for the various lasers.
Overall, our aim was to provide guidance for selecting an appropriate laser treatment in patients with DH, using network meta-analyses to compare different lasers, placebo, and no treatment over different time periods.
Methods
The network meta-analysis was performed according to the international guidelines for conducting and reporting systematic reviews as well as pairwise and network meta-analyses [24, 25]. In addition, this research has been registered in the International Prospective Register of Systematic Reviews (PROSPERO-CRD42019118739).
Search strategy
Four main databases, namely, PubMed, Embase, Web of Science, and CENTRAL (Cochrane Library), were searched for relevant studies. Only English language studies exploring the desensitization effects of different lasers, placebo, or no treatment on DH were identified from inception up to December 11, 2018. The database was searched using the following combination of text and MeSH terms: “lasers” and “dentine hypersensitivity”. The search strategy is described in the Appendix (S1). In addition, ProQuest Dissertation Abstracts, the International Clinical Trials Registry Platform, a thesis database, ClinicalTrials.gov, and the System for Information on Gray Literature in Europe database were also searched, in order to find the “gray” literatures that were written in English. Furthermore, a manual search was also performed to review the reference lists of related papers and review articles, as a supplement to the electronic search.
Study selection and data extraction
Randomized controlled trials (RCTs) comparing the different effects of lasers, placebo, or no treatment on DH were reviewed. Based on the PICOS model [26], inclusion and exclusion criteria were established, which can be summarized as follows:
Patients: systemically healthy adult patients with DH were included; studies related to DH periodontal maintenance or after bleaching were excluded.
Intervention and comparator: any lasers (GaAlAs, Nd:YAG, Er:YAG, Er,Cr:YSGG, CO2), placebo, and no treatment were included. There were no limits on the power or management method, but the first follow-up time had to be less than 30 min and the long-term follow-up time was 1 month (4 weeks and 30 days were also included). Studies on other treatments or where the follow-up time did not meet the requirements were excluded.
Outcomes: the quantitatively assessed effects of different lasers, placebo, or no treatment on DH based on the air blast test score on the VAS scale were included. Studies on other types of stimulation and measurement scales were excluded.
Studies: only RCTs were included. Case studies, in vitro studies, animal experiments, unpublished materials, and review papers were excluded.
Two authors screened the titles and abstracts of the studies, independently, which found the studies that met all the inclusion criteria for full-text evaluation. An arm that was not relevant to our analysis was excluded, if the included studies have at least three arms. Information required for this study was extracted from the selected studies by two authors. The extracted information and data included the first author of the study, publication year, country, first follow-up time, other follow-up time, intervention and comparator group, number of interventions and comparisons, laser parameters, and measurement scale. During this process, if there is any disagreement, a consensus can be reached through discussion with a third author.
Risk of bias and assessment of the quality of evidence
The Cochrane Collaboration tool in Review Manager (version 5.0 for Windows; the Cochrane Collaboration, Oxford, UK) was used to evaluate the quality and risk of bias in included studies [27]. When all bias indicators were evaluated as low risk, the RCTs had a low risk of bias, and the RCTs had a high risk of bias when one or more bias was assessed as high risk of bias; all the other conditions were regarded as moderate risk of bias [28]. Funnel plots created in Stata (version 14, Stata Corp, College Station, TX, USA) were used to evaluate the possibility of publication bias in the selected studies [29]. Grading of Recommendations Assessment, Development, and Evaluation (GRADE) was used to assess the quality of evidence of the final selected studies. All the above steps were performed by two authors independently. If there are any differing views, a consensus was reached by discussion with the third author.
Sensitivity analysis
For sensitivity analysis, the studies with a high risk of bias were excluded both in the immediate term and in the long term.
Statistical analysis
A variance calculation and node-splitting analyses were conducted in ADDIS 1.16 (Drugis.org) to evaluate inconsistencies within the network meta-analysis. If there was a difference between random effects variance and high inconsistency or the difference between direct and indirect evidence was P < 0.05, significant inconsistency was present. We adjusted included studies to obtain a consistent ideal network based on quantitative estimation.
We first performed a traditional pairwise meta-analysis using a random effects model in ADDIS 1.16 to synthesize studies comparing the same pair of treatments. The results are shown as mean differences (MDs) with 95% confidence intervals (CIs). The I2 test was used to evaluate heterogeneity across studies, and a value > 50% was considered to indicate moderate-to-high heterogeneity [30]. Statistical significance was assigned at P < 0.05.
Second, we established a random effects network within a Bayesian framework model using Markov chain Monte Carlo methods in ADDIS 1.16 [31]. We networked the translated binary outcomes of the desensitization effect and specified the relationship among the MDs across studies making different comparisons, as reported previously, which combined direct and indirect comparisons of different treatments to ensure the most comprehensive comparison of any given pair of lasers, placebo, and no treatment [32]. Statistical significance was considered at P < 0.05 based on 95% CIs.
The ranking probability of each treatment was also estimated in ADDIS 1.16 by calculating the MD of each treatment group compared with arbitrary common controls and counting the proportion of iterations of the Markov chain of the MD ranking for treatments.
Results
Study selection
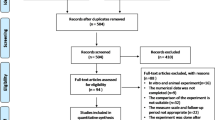
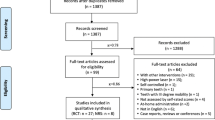
Four databases were searched, and reference sections of relevant articles were also manually searched; 893 and 106 records were identified, respectively. A total of 298 duplicate articles were excluded. After screening titles and abstracts, another 618 studies were also excluded since they did not meet the inclusion criteria. The remaining 83 studies were assessed by reviewing full texts and choosing 11 studies that compared the desensitization effect between four different lasers, placebo, and no treatment immediately after treatment and over the long term (1 month) (Fig. 1).

PRISMA flow program for study selection
Study characteristics
Basic characteristics of the 11 included studies are shown in Table 1. All the final included studies were between 2002 and 2018 that included GaAlAs, Nd:YAG, Er:YAG, and Er,Cr:YSSG lasers [8, 10, 11, 33,34,35,36,37,38,39,40].
The follow-up time of included studies ranged from the period immediately after treatment to 6 months. The follow-up time was immediately after laser treatment when assessing the immediate desensitization effects of lasers, excluding Dilsiz et al.’s [36] 30 min and Maximiano et al.’s [40] 5 min after treatment. Since 1 month (4 weeks and 30 days included) was the most common follow-up time in the studies, we chose this time point as the long-term period. Vieira et al. [35], Yilmaz et al. [11], and Soares et al. [39] only evaluated immediate outcomes.
We established networks for our comparisons (Fig. 2). In this figure, each node represents a treatment to DH. Connections between nodes denote direct comparisons; node size and the thickness of connection vary according to the number of studies performing the comparison.

Network comparing the desensitization effect of lasers, placebo, or no treatment in the immediate term and in the long term
Risk of bias
The evaluation of risk of bias of included studies showed that only one study had a low risk, six had a moderate risk, and the other four had a high risk (Fig. 3). The most common type of bias was selective reporting. The funnel plots were used to evaluate the publication bias of these studies (Fig. 4). According to the network meta-analysis, there was no significant asymmetry or evidence of significant bias among the selected studies in terms of the desensitization effect.

The risk of bias of the included RCTs. a Summary for each included RCT. b Graph of all included RCTs

Comparison-adjusted funnel plots for assessing publication bias and comparing the desensitization effect of lasers, placebo, or no treatment in the immediate term (a) and in the long term (b)
Evidence grading and sensitivity analysis
The quality of evidence of the final included studies indicated lasers vs. placebo or no treatment with a moderate or low quality in the immediate and long term, and the results of the quality of the selected studies are shown in Tables 3–4. In addition, results of the sensitivity analysis of network meta-analysis are summarized in the Appendix (S2, S3).
Inconsistency assessment
Results of the inconsistency test are provided in the Appendix (S4). Our results indicate no significant inconsistency between comparisons except Er:YAG versus Nd:YAG (P < 0.05), which shows that it conforms to the similarity assumption.
Pairwise and network meta-analyses
Results of pairwise meta-analysis are provided in the Appendix (S5, S6). Nd:YAG was better than Er:YAG, and GaAlAs was better than no treatment immediately after treatment and in the long term. In addition, Er:YAG and Er,Cr:YSGG had better immediate effects than placebo.
Results of the network meta-analysis are summarized in Table 2. The GaAlAs, Nd:YAG, Er:YAG, and Er,Cr:YSGG had better desensitization effects than no treatment at both time points. Er,Cr:YSGG was better than placebo, and placebo was better than no treatment in immediate effects.
Rank probabilities
The treatment ranking of probability results is shown in Fig. 5. Treatments with greater values on the histogram were associated with greater probabilities for a lower desensitization effect. According to the network of immediate effects, the cumulative probabilities of being the most efficacious treatments were 73% for Er,Cr:YSGG followed by Nd:YAG, GaAlAs, Er:YAG, placebo, and no treatment, sequentially. Based on the network of long-term (1-month) desensitization effects, the cumulative probabilities of being the most efficacious treatments were 47% for Er,Cr:YSGG followed by Nd:YAG, Er:YAG, GaAlAs, placebo, and no treatment, sequentially.

Ranking probability of each treatment effect on DH in the immediate term (a) and in the long term (b)
Discussion
DH is a common presentation in the dental clinic and has a negative effect on quality of life [41]. Lasers have been used to treat DH since the mid-1980s, and their effectiveness has been supported in many clinical trials [42]. However, the results of these studies have not been consistent [33, 36], and some researchers believe that previous meta-analyses did not draw the conclusion that laser therapy decreases DH based on available evidence [43, 44].
Only RCTs were included in this network meta-analysis. RCTs could minimize the confounding impact, which suggests the most objective comparison. In addition, it strengthens the validity of included studies because of reducing selection bias, but it may narrow the available database.
There are many factors that can affect the effectiveness of laser treatment toward DH, such as the laser parameters, the methods of DH evaluation, the types of stimulation, different follow-up times, and the cause of DH [9, 45]. At this time, there are no established gold standards for laser parameter settings, and few studies have applied lasers with the same parameters. Thus, there are no definitive guidelines for the laser parameter settings in this study. However, it is important to use an appropriate irradiation time, wavelength, and power, to ensure patient safety [46]. Differences in DH assessment methods may lead to differences in reproducibility, leading to high levels of heterogeneity that can affect comparisons with different studies [20]. However, there is no gold standard evaluation method for DH. Some studies have used SMD to combine data from different scales and make comparisons between studies in previous meta-analyses to reduce the impact of different measurement scales on the results [47]. Only studies that used the VAS were included in this network meta-analysis, which could eliminate the effects of different measurement scales. Various types of stimulation have been used in clinical trials such as cold air, water, thermal or tactile stimuli, and subjective evaluation [48, 49]. Only studies that used air blast tests were included in this network meta-analysis, which could eliminate the influence of different stimulations. Compared with other types of stimulation, the air blast test is a more common and reproducible method for evaluating DH [17, 50]. Besides, the distance of the air blast stimulus can affect the results, and no standardization was established. The distance of the air blast stimulus among these was from 1 mm to 1 cm, which may add bias in the results. In most studies, several follow-up periods for laser efficacy have been examined. However, the follow-up time varies between studies, particularly the time of the final follow-up. To allow for comparison of follow-up times between studies, we selected the first time which is less than 30 min as the immediate effect and 1 month (including 4 weeks and 30 days) as the long-term effect. Some patients who experience bleaching or periodontal maintenance treatment may also suffer from DH, but the different causes for the sensitivity of dentine may bias the results. Therefore, studies related to DH periodontal maintenance or after bleaching were excluded from this network meta-analysis. In addition, one thing should be noted that the feeling of pain in a patient with DH is an individual and subjective symptom that varies between individuals, which may also lead to bias.
The assessment of risk of bias showed that four had a high risk, and the most common type of bias was selective reporting. In the sensitivity analysis, the authors excluded these four high-risk studies, which indicated that it did not influence the conclusions. Besides, the results of publication bias suggest that there was no significant asymmetry or evidence of significant bias among the selected studies in terms of the desensitization effect. All these indicate that the results of this study have certain credibility.
According to the network meta-analysis of the immediate effect, the desensitization effect was in the order of Er,Cr:YSGG > Nd:YAG > GaAlAs > Er:YAG > placebo > no treatment. However, there were no significant differences among the four different lasers, and there were no significant differences among Nd:YAG, GaAlAs, Er:YAG, and placebo treatment. According to the network meta-analysis on the long-term (1-month) effect, the desensitization effect was in the order of Er,Cr:YSGG > Nd:YAG > Er:YAG > GaAlAs > placebo > no treatment. However, there were no significant differences among the four different lasers and placebo or between the placebo and no treatment. Our results indicate that Er,Cr:YSGG, Nd:YAG, Er:YAG, and GaAlAs lasers had better desensitizing effects on DH than no treatment in the immediate term and in the long term (1 month) but were not better than placebo (excluding Er,Cr:YSGG for the immediate effect). This result is in line with a previous systematic review [51]. However, it is inconsistent with Lin et al. who reported that lasers are significantly better than placebo [17]. The difference may be due to differences in the inclusion criteria, where we only included studies using the VAS measurement scale and a final check time of 1 month. Furthermore, studies related to DH periodontal maintenance or after bleaching were also excluded from our study. The placebo effect will affect evaluation of the laser desensitization effect. Some studies have reported significant reliefs in DH due to the placebo effect, which is reflected in our results on the immediate effect [52]. This result also supports the importance of including placebo groups in future studies.
DH is a subjective feeling of patients and the degree of pain, which is mainly based on patients self-report. Other relevant factors may also affect the response of patients to different treatments on DH [53]. At present, the most common method used to measure the pain of DH is VAS. However, this method does not include other oral or physical conditions that may affect the results [54]. Besides, some studies have highlighted the importance of dental patient-reported pain on oral health and show that the dental patient-reported outcome measure (dPROM) should be adopted to get the dental patient-reported outcome (dPRO) [55]. Therefore, a dPROM suitable for evaluating the pain of DH is required.
To the best of our knowledge, this is the first network meta-analysis comparing immediate and long-term (1-month) effects among lasers, placebo, and no treatment on DH. However, there were several limitations to this study. First, the sample sizes of the included studies were insufficient to draw definitive conclusions. Second, maintaining the desensitization effects of laser treatment requires long-term maintenance of oral health and regular review, but the effects of patient compliance on repair outcomes were not mentioned in most of the included studies. Third, our study was limited to articles published in English and those available in four major literature databases, which may have resulted in selection bias. Besides, the quality of evidence of the included studies with a moderate or low quality could also influence the final results of this study. To address these issues, further well-designed RCTs with enough participants and high quality of evidence grade are needed.
Conclusions
In conclusion, this network meta-analysis showed no significant differences were observed among Er,Cr:YSGG, Nd:YAG, Er:YAG, and GaAlAs lasers both in the immediate term and over the long term (1 month). However, based on the treatment ranking of probability, which indicated that Er,Cr:YSGG may be the best laser for the treatment of DH in the immediate term and in the long term (1 month). In addition, the results of this study showed that there was a significant placebo effect on DH, supporting the importance of including a placebo group in future studies.
References
Holland GR, Narhi MN, Addy M, Gangarosa L, Orchardson R (1997) Guidelines for the design and conduct of clinical trials on dentine hypersensitivity. J Clin Periodontol 24(11):808–813
Robin O, Gillam DG (2006) Managing dentin hypersensitivity. J Am Dent Assoc 137(7):990–998
Addy M, Mostafa P, Newcombe RG (1987) Dentine hypersensitivity: the distribution of recession, sensitivity and plaque. J Dent 15(6):242–248
Corona SA, Nascimento TN, Catirse AB, Lizarelli RF, Dinelli W, Palma-Dibb RG (2010) Clinical evaluation of low-level laser therapy and fluoride varnish for treating cervical dentinal hypersensitivity. J Oral Rehabil 30(12):1183–1189
Brannstrom M, Astrom A (1972) The hydrodynamics of the dentine; its possible relationship to dentinal pain. Int Dent J 22(2):219–227
(2003) Consensus-based recommendations for the diagnosis and management of dentin hypersensitivity. J Can Dent Assoc 69 (4):221–226
Walters PA (2005) Dentinal hypersensitivity: a review. J Contemp Dent Pract 6(2):107–117
Yilmaz HG, Kurtulmus-Yilmaz S, Cengiz E, Bayindir H, Aykac Y (2011) Clinical evaluation of Er,Cr:YSGG and GaAlAs laser therapy for treating dentine hypersensitivity: a randomized controlled clinical trial. J Dent 39(3):249–254. https://doi.org/10.1016/j.jdent.2011.01.003
Dilsiz A, Canakci V, Ozdemir A, Kaya Y (2009) Clinical evaluation of Nd:YAG and 685-nm diode laser therapy for desensitization of teeth with gingival recession. Photomed Laser Surg 27(6):843–848. https://doi.org/10.1089/pho.2008.2395
Aranha AC, Eduardo Cde P (2012) Effects of Er:YAG and Er,Cr:YSGG lasers on dentine hypersensitivity. Short-term clinical evaluation. Lasers Med Sci 27(4):813–818. https://doi.org/10.1007/s10103-011-0988-9
Yilmaz HG, Bayindir H (2014) Clinical and scanning electron microscopy evaluation of the Er,Cr:YSGG laser therapy for treating dentine hypersensitivity: short-term, randomised, controlled study. J Oral Rehabil 41(5):392–398. https://doi.org/10.1111/joor.12156
Ipci SD, Cakar G, Kuru B, Yilmaz S (2009) Clinical evaluation of lasers and sodium fluoride gel in the treatment of dentine hypersensitivity. Photomed Laser Surg 27(1):85–91. https://doi.org/10.1089/pho.2008.2263
Kimura Y, Wilder-Smith P, Yonaga K, Matsumoto K (2000) Treatment of dentine hypersensitivity by lasers: a review. J Clin Periodontol 27(10):715–721
Aranha AC, Pimenta LA, Marchi GM (2009) Clinical evaluation of desensitizing treatments for cervical dentin hypersensitivity. Braz Oral Res 23(3):333–339
de-Melo MA, Passos VF, Alves JJ, Barros EB, Santiago SL, Rodrigues LK (2011) The effect of diode laser irradiation on dentin as a preventive measure against dental erosion: an in vitro study. Lasers Med Sci 26(5):615–621. https://doi.org/10.1007/s10103-010-0865-y
Whitters CJ, Hall A, Creanor SL, Moseley H, Gilmour WH, Strang R, Saunders WP, Orchardson R (1995) A clinical study of pulsed Nd: YAG laser-induced pulpal analgesia. J Dent 23(3):145–150
Lin PY, Cheng YW, Chu CY, Chien KL, Lin CP, Tu YK (2013) In-office treatment for dentin hypersensitivity: a systematic review and network meta-analysis. J Clin Periodontol 40(1):53–64. https://doi.org/10.1111/jcpe.12011
Machado AC, Viana IEL, Farias-Neto AM, Braga MM, de Paula Eduardo C, de Freitas PM, Aranha ACC (2018) Is photobiomodulation (PBM) effective for the treatment of dentin hypersensitivity? A systematic review. Lasers Med Sci 33(4):745–753. https://doi.org/10.1007/s10103-017-2403-7
He S, Wang Y, Li X, Hu D (2011) Effectiveness of laser therapy and topical desensitising agents in treating dentine hypersensitivity: a systematic review. J Oral Rehabil 38(5):348–358. https://doi.org/10.1111/j.1365-2842.2010.02193.x
Sgolastra F, Petrucci A, Severino M, Gatto R, Monaco A (2013) Lasers for the treatment of dentin hypersensitivity: a meta-analysis. J Dent Res 92(6):492–499. https://doi.org/10.1177/0022034513487212
Salanti G, Higgins JP, Ades AE, Ioannidis JP (2008) Evaluation of networks of randomized trials. Stat Methods Med Res 17(3):279–301. https://doi.org/10.1177/0962280207080643
Ades AE, Sculpher M, Sutton A, Abrams K, Cooper N, Welton N, Lu G (2006) Bayesian methods for evidence synthesis in cost-effectiveness analysis. Pharmacoeconomics 24(1):1–19. https://doi.org/10.2165/00019053-200624010-00001
Hawkins N, Scott DA, Woods BS, Thatcher N (2009) No study left behind: a network meta-analysis in non-small-cell lung cancer demonstrating the importance of considering all relevant data. Value Health 12(6):996–1003. https://doi.org/10.1111/j.1524-4733.2009.00541.x
Hoaglin DC, Hawkins N, Jansen JP, Scott DA, Itzler R, Cappelleri JC, Boersma C, Thompson D, Larholt KM, Diaz M, Barrett A (2011) Conducting indirect-treatment-comparison and network-meta-analysis studies: report of the ISPOR Task Force on Indirect Treatment Comparisons Good Research Practices: part 2. Value Health 14(4):429–437. https://doi.org/10.1016/j.jval.2011.01.011
Stewart LA, Clarke M, Rovers M, Riley RD, Simmonds M, Stewart G, Tierney JF (2015) Preferred Reporting Items for Systematic Review and Meta-Analyses of individual participant data: the PRISMA-IPD statement. JAMA 313(16):1657–1665. https://doi.org/10.1001/jama.2015.3656
Stegenga B, Dijkstra PU (2007) Principles of evidence-based medicine applied to dentistry. Ned Tijdschr Tandheelkd 114(4):155–160
Higgins J (2008) Cochrane handbook for systematic reviews of interventions version 5.1.0. Wiley-Blackwell
Green S (2011) Cochrane handbook for systematic reviews of interventions: Cochrane book series. Naunyn Schmiedebergs Arch Exp Pathol Pharmakol 5(2):S38
Vandenbroucke JP (1998) Bias in meta-analysis detected by a simple, graphical test. Experts’ views are still needed. BMJ 316(7129):469–470 author reply 470-461
Higgins JP, Thompson SG (2002) Quantifying heterogeneity in a meta-analysis. Stat Med 21(11):1539–1558. https://doi.org/10.1002/sim.1186
van Valkenhoef G, Tervonen T, Zwinkels T, de Brock B, Hillege H (2013) ADDIS: a decision support system for evidence-based medicine. Decis Support Syst 55(2):459–475. https://doi.org/10.1016/j.dss.2012.10.005
Cipriani A, Furukawa TA, Salanti G, Geddes JR, Higgins JP, Churchill R, Watanabe N, Nakagawa A, Omori IM, McGuire H, Tansella M, Barbui C (2009) Comparative efficacy and acceptability of 12 new-generation antidepressants: a multiple-treatments meta-analysis. Lancet 373(9665):746–758. https://doi.org/10.1016/s0140-6736(09)60046-5
Lier BB, Rosing CK, Aass AM, Gjermo P (2002) Treatment of dentin hypersensitivity by Nd:YAG laser. J Clin Periodontol 29(6):501–506
Birang R, Poursamimi J, Gutknecht N, Lampert F, Mir M (2007) Comparative evaluation of the effects of Nd:YAG and Er:YAG laser in dentin hypersensitivity treatment. Lasers Med Sci 22(1):21–24. https://doi.org/10.1007/s10103-006-0412-z
Vieira AH, Passos VF, de Assis JS, Mendonca JS, Santiago SL (2009) Clinical evaluation of a 3% potassium oxalate gel and a GaAlAs laser for the treatment of dentinal hypersensitivity. Photomed Laser Surg 27(5):807–812. https://doi.org/10.1089/pho.2008.2364
Dilsiz A, Aydin T, Canakci V, Gungormus M (2010) Clinical evaluation of Er:YAG, Nd:YAG, and diode laser therapy for desensitization of teeth with gingival recession. Photomed Laser Surg 28(Suppl 2):S11–S17. https://doi.org/10.1089/pho.2009.2593
Yilmaz HG, Cengiz E, Kurtulmus-Yilmaz S, Leblebicioglu B (2011) Effectiveness of Er,Cr:YSGG laser on dentine hypersensitivity: a controlled clinical trial. J Clin Periodontol 38(4):341–346. https://doi.org/10.1111/j.1600-051X.2010.01694.x
Bal MV, Keskiner I, Sezer U, Acikel C, Saygun I (2015) Comparison of low level laser and arginine-calcium carbonate alone or combination in the treatment of dentin hypersensitivity: a randomized split-mouth clinical study. Photomed Laser Surg 33(4):200–205. https://doi.org/10.1089/pho.2014.3873
Soares ML, Porciuncula GB, Lucena MI, Gueiros LA, Leao JC, Carvalho AA (2016) Efficacy of Nd:YAG and GaAlAs lasers in comparison to 2% fluoride gel for the treatment of dentinal hypersensitivity. Gen Dent 64(6):66–70
Maximiano V, Machado AC, Yoshida ML, Pannuti CM, Scaramucci T, Aranha ACC (2018) Nd:YAG laser and calcium sodium phosphosilicate prophylaxis paste in the treatment of dentin hypersensitivity: a double-blind randomized clinical study. Clin Oral Investig 23:3331–3338. https://doi.org/10.1007/s00784-018-2759-5
Bekes K, John MT, Schaller HG, Hirsch C (2009) Oral health-related quality of life in patients seeking care for dentin hypersensitivity. J Oral Rehabil 36(1):45–51. https://doi.org/10.1111/j.1365-2842.2008.01901.x
Asnaashari M, Moeini M (2013) Effectiveness of lasers in the treatment of dentin hypersensitivity. J Lasers Med Sci 4:1):1–1):7
Jokstad A (2012) The effectiveness of lasers to reduce dentinal hypersensitivity remains unclear. J Evid Based Dent Pract 12(3 Suppl):231–232. https://doi.org/10.1016/s1532-3382(12)70045-3
Cunha-Cruz J (2011) Laser therapy for dentine hypersensitivity. Evid Based Dent 12(3):74–75. https://doi.org/10.1038/sj.ebd.6400807
Ladalardo TC, Pinheiro A, Campos RA, Brugnera Junior A, Zanin F, Albernaz PL, Weckx LL (2004) Laser therapy in the treatment of dentine hypersensitivity. Braz Dent J 15(2):144–150
Sicilia A, Cuesta-Frechoso S, Suarez A, Angulo J, Pordomingo A, De Juan P (2009) Immediate efficacy of diode laser application in the treatment of dentine hypersensitivity in periodontal maintenance patients: a randomized clinical trial. J Clin Periodontol 36(8):650–660. https://doi.org/10.1111/j.1600-051X.2009.01433.x
Hu ML, Zheng G, Zhang YD, Yan X, Li XC, Lin H (2018) Effect of desensitizing toothpastes on dentine hypersensitivity: a systematic review and meta-analysis. J Dent 75:12–21. https://doi.org/10.1016/j.jdent.2018.05.012
Banerjee A, Hajatdoost-Sani M, Farrell S, Thompson I (2010) A clinical evaluation and comparison of bioactive glass and sodium bicarbonate air-polishing powders. J Dent 38(6):475–479. https://doi.org/10.1016/j.jdent.2010.03.001
Gillam DG, Newman HN (1993) Assessment of pain in cervical dentinal sensitivity studies. A review. J Clin Periodontol 20(6):383–394
Ide M, Wilson RF, Ashley FP (2001) The reproducibility of methods of assessment for cervical dentine hypersensitivity. J Clin Periodontol 28(1):16–22
Sgolastra F, Petrucci A, Gatto R, Monaco A (2011) Effectiveness of laser in dentinal hypersensitivity treatment: a systematic review. J Endod 37(3):297–303. https://doi.org/10.1016/j.joen.2010.11.034
West NX, Addy M, Jackson RJ, Ridge DB (1997) Dentine hypersensitivity and the placebo response. A comparison of the effect of strontium acetate, potassium nitrate and fluoride toothpastes. J Clin Periodontol 24(4):209–215
Rosen EB, Donoff RB, Riedy CA (2016) U.S. dental school deans’ views on the value of patient-reported outcome measures in dentistry. J Dent Educ 80(6):721–725
John MT, Reissmann DR, Feuerstahler L, Waller N, Baba K, Larsson P, Celebic A, Szabo G, Rener-Sitar K (2014) Exploratory factor analysis of the Oral Health Impact Profile. J Oral Rehabil 41(9):635–643. https://doi.org/10.1111/joor.12192
John MT (2018) Health outcomes reported by dental patients. J Evid Based Dent Pract 18(4):332–335. https://doi.org/10.1016/j.jebdp.2018.09.001
Funding
This study was supported by the National Natural Science Foundation of China (81771119).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
For this type of study, formal consent is not required.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 2213 kb)
Rights and permissions
About this article

Cite this article
Kong, Y., Lei, Y., Li, S. et al. Network meta-analysis of the desensitizing effects of lasers in patients with dentine hypersensitivity. Clin Oral Invest 24, 1917–1928 (2020). https://doi.org/10.1007/s00784-019-03051-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-019-03051-3