
Abstract
Purpose
To provide a systematic literature review of the impact of preoperative Modic changes (MCs) on the clinical outcome following lumbar spine surgery for degenerative lumbar spine disease.
Methods
A PubMed search until 31 October 2015 was performed to identify publications correlating preoperative MC with clinical outcome in patients undergoing spine surgery.
Results
Inclusion criteria were met by 14 articles (7 prospective and 7 retrospective studies) representing a total of 1652 surgical patients, of which at least 804 (>49 %) showed MC. Of the 14 publications, 6 concerned discectomy (n = 607), 1 fusion versus discectomy (n = 91), 3 fusion surgery (n = 454), and 4 total disc replacement (TDR, n = 500). A trend toward less improvement in low back pain or Oswestry Disability Index score was found in the discectomy studies, and a trend toward increased improvement was demonstrated in the TDR studies when MC was present preoperatively. The fusion studies were of low evidence, and showed conflicting results.
Conclusion
Preoperative MC showed a trend toward a negative correlation with clinical improvement in patients undergoing discectomy for LDH and a positive correlation with clinical improvement in patients undergoing TDR for degenerative disc disease. However, it is questionable whether the differences surpass the minimal clinically important difference (MCID). In patients undergoing fusion surgery, there was insufficient evidence to draw any conclusions. Future studies should include a larger patient material, focus on MCID, and include known confounding factors of the clinical outcome of spine surgery in the analysis.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Vertebral end-plate signal changes (VESCs) are common MRI-findings in patients with non-specific low back pain (LBP), describing signal intensity changes in the corpora of the vertebrae. However, the correlation of VESC with clinical outcome in spine surgery is debated.
VESCs are also known as Modic changes (MCs) and are subdivided into Modic type 1 changes (MC1) referring to oedema-like signal intensity changes, Modic type 2 changes (MC2) referring to fat-like signal intensity changes, and the less common Modic type 3 changes (MC3) referring to sclerosis-like signal changes thought to be late stages of MC1 or MC2 [1–3].
Surgery on the lumbar discus for herniated disc has been shown to accelerate the development of MC1 [4], especially when comparing discectomy to sequestrectomy [5, 6], although conflicting results have been published as well [7–11].
Several studies have demonstrated a correlation between VESC and LBP [12–17]. Jensen et al. showed a prevalence of VESC in 43 % of patients with non-specific LBP and/or sciatica and a prevalence of VESC in 6 % of the general population [13]. Ohtori et al. associated LBP with MC through a TNF-α induced nerve in-growth of sensory fibres in the endplate [18].
The aetiology of MC largely remains unknown, although the prevailing hypothesis suggests that a degeneration of the discus results in greater axial loading and increased mechanical stress on the vertebral endplate bodies leading to inflammation and oedema [1]. Some studies support an alternative hypothesis of MC being caused by bacterial infection, most frequently Propionibacterium acnes [12, 19–21].
Lumbar disc herniation (LDH) is also considered a risk factor for developing MC, especially MC1 [22, 23]. Patients with lumbar disc herniation (LDH) have significant improvement in leg pain after surgery when conservative treatment fails. However, the type of surgical procedure performed in a patient with LDH and preoperative MC1 is up for discussion, as MC1 may influence the outcome on back pain and MC1 has been reported to be associated with spinal instability and hypermobility [10, 24]. Thus, the preoperative presence of MC1 may indicate the need of additional stabilising surgery, such as fusion surgery [10, 25–30]. In accordance, some studies even suggest that fusion increases the conversion of MC1 to MC2, probably by correcting the mechanical instability, and these changes appear to be a good indicator of satisfactory outcome after fusion surgery [26, 31]. However, one should also consider that the natural course of MC usually is a development to MC2, MC3, or normal bone marrow over time [1, 32].
The purpose of the present systematic literature review was to investigate whether there is a correlation between preoperative MC and clinical outcome in patients undergoing lumbar spine surgery, including simple discectomy procedures, instrumented fusion surgery, and total disc replacement (TDR).
Methods
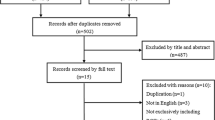
A PubMed literature search until October 31, 2015 was performed using the search term “Modic Changes OR VESC”, which generated 297 articles. Adding language “English” along with “AND (surgery OR fusion)” to the search criteria yielded 119 articles.
Inclusion in the present review required the following: (1) the presence of MC on preoperative MRI was reported, (2) the included patients, or part of them, underwent lumbar surgery, and (3) the presence of preoperative MC was correlated with the clinical outcome of surgery.
All titles and abstracts—and when relevant, the full article—were reviewed by the two authors independently, identifying 14 articles fulfilling the inclusion criteria. Cross-checking the references from the included studies revealed no additional relevant articles.
Results
Table 1 summarises the objectives and findings of the included 14 publications concerning discectomy (n = 6), fusion versus discectomy (n = 1), fusion surgery (n = 3), and total disc replacement (TDR) (n = 4). The 14 articles comprised a total of 1652 surgical patients of which at least 804 (>49 %) showed some type of MC. However, the actual number of patients with MC is higher, as one article [33] did not report the number of patients showing MC. Predominant clinical outcome measures involved ODI and VAS for LBP across the studies (Fig. 1).

Graphical representation of reported percentage change from preoperative to last follow-up in VAS for LBP and ODI. Avg. MC/no MC indicates that data on differences in MC/no MC subgroups were unavailable. D discectomy, PLF posterior lumbar (interbody) fusion, and TDR total disc replacement
Patient inclusion criteria were generally based on failed conservative treatment, presentation of chronic LBP and/or radicular pain and radiological recognition of herniated lumbar disc and/or degenerative changes.
Studies of discectomy for LDH
A total of 607 patients were evaluated in the 6 articles, of which 3 were prospective studies. Approximately 325 (54 %) patients showed MC. In general, no significant difference was found preoperatively between patients with or without MC. The number of patients in the 6 articles is subgrouped according to MC types in Fig. 2 showing for each article, the number of patients and the trend toward no impact or negative impact of MC on the clinical outcome following discectomy for LDH.

Graphical representation of the impact of preoperative MC1 on clinical outcome at final follow-up among studies of discectomy. Positive values represent no impact and negative values represent a trend toward or a statistical significant impact of preoperative MC1 on clinical outcome at final follow-up. Lengths of the bars represent the number of patients in the study
Chin et al. [11] performed a prospective pilot study including 30 patients undergoing microdiscectomy. Their main objective was to determine if MC had an impact on postoperative LBP and concordant sciatica.
All patients reported leg pain greater than back pain and presented with LBP for an average of 25.6 months. Group 1 contained 15 patients with MC1 (n = 8) or MC2 (n = 7), while group 2 contained 15 patients without MC. Follow-up was only 6 months. No significant difference was demonstrated in VAS for LBP and sciatica postoperatively in the two groups. ODI was similar in both groups preoperatively but approached a significant difference at follow-up (P = 0.09) with best improvement in the patient group without MC. The difference in VAS or ODI between patients with MC1 and MC2 was not examined.
Sørlie et al. [8] investigated if preoperative MC1 correlated with clinical outcome in a prospective study of 178 patients undergoing microdiscectomy for LDH. The patients were divided into a group with preoperative MC1 or mixed MC1/2 (n = 36) and a group (n = 142) without MC (n = 74) or MC2 (n = 68). At 12-months follow-up, the two groups had improved significantly in all of the outcome measures, including VAS, ODI, and EQ-5D. A clear trend toward less improvement of LBP and ODI was demonstrated in the group with MC1 compared with the no-MC/MC2 group, but statistical significance was not reached (P = 0.06).
A logistic regression analysis showed that smoking was the only statistical significant independent predictor of less improvement of VAS for LBP postoperatively. The authors commented that there might be synergistic effect between smoking and MC1 resulting in a significant negative impact on patient improvement of LBP. They concluded that patients with MC1 can expect less but still significant improvement of LBP after 12 months but not if they smoke.
Ohtori et al. [10] prospectively examined the relationship between preoperative MC1 and postoperative LBP in 45 patients undergoing discectomy for LDH. Patients were divided into group 1 (n = 23) with preoperative MC1 and group 2 (n = 22) without MC. Patients without MC were selected randomly from a cohort of 115 patients. Both groups had equally significant improvement of VAS for LBP after discectomy, and no significant difference was found in postoperative VAS for LBP or leg pain, Japanese Orthopaedic Association Score (JOAS) or ODI between the two groups at 24-months follow-up (P > 0.05, exact value not available). The authors concluded that discectomy was an equally effective treatment for LDH among patients with and without MC1.
Rahme et al. [34] retrospectively studied if lumbar microdiscectomy for LDH had an impact on preoperative MC in a cohort of 41 patients. They found an increase in the prevalence of MC from 46 to 78 % at the operated level. Comparing the groups with preoperative MC (n = 32, 6 MC1 and 26 MC2) and without preoperative MC (n = 9) showed no difference in improvement of ODI or VAS for low back and leg pain at a median follow-up of 41 months (range 32–59 months). As to the changes in MC, they concluded that following lumbar discectomy, most patients develop MC (type 2 in particular) at the operated level, possibly resulting from an acceleration of the degenerative process.
Schistad et al. [35] retrospectively examined the correlation between MC and clinical recovery in patients with lumbar radicular pain. Of the 243 participants, 30 showed MC1, 147 showed MC2, and 7 showed MC3. Patients were divided into a surgical group (n = 126), and a conservative group (n = 117) based on neurological deficits or lack of improvement from previous conservative treatment. Surgical treatment involved microdiscectomy or standard discectomy (the surgical procedure of 35 patients was not known). The authors found no statistical significant difference in clinical outcome between the surgical and conservative groups and divided all patients into three groups: no MC (n = 59), MC1 (n = 30), and MC2/3 (n = 154). Patients with MC1 showed significantly worse recovery in McGill sensory pain score after 6 weeks in both treatment groups (P = 0.007). When adjusted for, smoking correlated with VAS for LBP at baseline (P < 0.05) and McGill sensory pain at 6 months (P < 0.05). At final follow-up, there was no statistical significant difference in McGill, VAS for LBP or leg pain between the groups. They concluded that both surgically and non-surgically treated patients with lumbar radicular pain and MC1 may have a slower recovery of sensory pain.
Lurie et al. [7] performed a retrospective cohort study to determine which baseline MRI characteristics, including MC, are associated with surgical treatment effect. The study included 307 patients, of which 61 % (n = 187) were treated with discectomy and the remaining 39 % (n = 120) with conservative treatment. 27 % showed MC (MC1 accounted for 9 % and MC2 accounted for 18 %). For the present review, these percentages were used to extract an estimated number of surgically treated patients showing MC (Table 1), as this number was not mentioned in the study. The authors found that patients undergoing surgery with MC1 had worse outcome (P = 0.002) measured in ODI score and smaller treatment effect (P = 0.003) at 24 months follow-up and suggested that MC1 could be a risk factor of radicular pain distinct from the disc herniation and predict worse outcome following discectomy compared with similar patients without MC1. They concluded that patients with intervertebral disc herniation had worse surgical treatment effect if they presented with small disc herniation and MC1 compared with those with thecal sac compression ≥1/3.
Based on the reported numbers in each article, we calculated the percentage change in VAS for LBP and/or ODI from preoperative to postoperative follow-up. The difference in the percentage change among patients with or without MC ranged from 8 to 20 % and is shown in Fig. 1. It was not possible to calculate the corresponding standard deviations as they were not reported in the published data.
Studies of discectomy versus fusion
Cao et al. [25] performed a retrospective study of 91 patients with LDH and MC on a single level and predominant LBP undergoing discectomy (n = 47) or instrumented posterior lumbar interbody fusion (iPLIF, n = 44). All patients were offered iPLIF but those concerned with the financial costs and operation-/implant-related complications of the iPLIF procedure underwent discectomy instead. Preoperative clinical scores were equal in the two groups. At 18 months follow-up, JOAS was significantly increased (P < 0.05) and VAS for LBP was significantly decreased (P < 0.05) in patients treated with iPLIF compared with the patients undergoing discectomy. Accordingly, LBP was similar to preoperative severity in 23.4 % of the discectomy patients and in 4.5 % of the iPLIF patients. The authors concluded that iPLIF should be recommended as surgical procedure in patients suffering from LDH and MC with LBP greater than radicular pain.
Studies of lumbar spinal fusion
In the included three studies, a total of 454 patients were evaluated, of which 39 % (n = 177) showed preoperative MC. Two studies were prospective and one study retrospective.
To evaluate the impact of MC on posterolateral fusion, Ghodsi et al. [29] subgrouped a prospective cohort of 70 patients with degenerative lumbar instability into no MC (n = 18), MC1 (n = 31), MC2 (n = 20), and MC3 (n = 1 patient). Segmental instability was defined as translation ≥3 mm or angulation ≥10° on lateral radiographs at flexion and extension positions. At 1 year follow-up, no differences were found in ODI and VAS for LBP (P value not available). The authors concluded that posterolateral fusion was an effective procedure in patients showing spinal instability regardless of Modic changes or type.
Ohtori et al. [27] did a prospective cohort study of patients with MC1 (n = 21) or MC2 (n = 12) with the primary objective of examining changes in MC following posterolateral fusion surgery. The two groups presented no preoperative differences in VAS, ODI, or JOAS, and no statistical significant difference in postoperative LBP was demonstrated at 2 years follow-up (P > 0.05, exact value not available). Based on postoperative MRI, they concluded that MC1 could be expected to convert into MC2, possibly due to a regeneration of degenerated bone marrow following the surgical stabilization.
Kwon et al. [30] retrospectively investigated the efficacy of PLIF with stand alone cages in 351 patients with degenerative disc disease (DDD) and MC. The patients were grouped into four categories: no MC (n = 259), MC1 (n = 26), MC2 (n = 55), or MC3 (n = 11). At final follow-up (mean 60 months), VAS for LBP was significantly decreased in all four groups, but MC3 patients showed less improvement compared with the other groups (P < 0.05, exact value not available). They concluded that stand alone PLIF with cage was an effective treatment for patients suffering from LBP and DDD with or without MC1/2, but preoperative MC3 predicted lower clinical success and fusion rate.
Studies of total disc replacement
A total of 500 surgical patients were evaluated across the four studies of which three were prospective. More than 211 patients (>42 %) showed MC.
Siepe et al. [36] prospectively assessed clinical outcome in 92 patients treated with TDR. The patients were according to MRI findings subgrouped into group 1 with DDD (n = 40), group 2 with DDD and nucleus pulposus prolapse (n = 12), group 3 with post discectomy (n = 17), and group 4 with DDD and MC (n = 23). No statistical significant difference in ODI and VAS for LBP between the control group (group 1) and group 4 was demonstrated (P > 0.05, exact value not available) at the mean follow-up of 34 months. They concluded that predominant LBP and DDD with or without MC could be considered as an acceptable indication for lumbar TDR.
Gornet et al. [33] aimed to determine variables that may prove useful in predicting clinical outcome following TDR in their retrospective study of 99 patients. At baseline, the authors found no difference in ODI score regardless of Modic type, but at the 5-year follow-up, a lower ODI score was present in patients showing preoperative MC2 compared with patients showing MC1 or no MC (P = 0.037). They concluded that many factors could contribute toward an optimal outcome of TDR and that preoperative MC2 increased the treatment effect compared with MC1 or no MC.
Blondel et al. [37] prospectively analysed the influence of MC on clinical outcome in 221 patients undergoing TDR, of which 65 presented MC1 (30 %) and 49 MC2 (22 %) on preoperative MRI. ODI and VAS for low back and radicular pain were used, and the mean final follow-up was 30 months (range 24–72). Statistical significance was reached when a univariate analysis of ODI was performed at 12 months follow-up in the patient group with MC1 compared with the non-Modic group and MC2 group (but not at final follow-up). The MC1 group had the lowest mean ODI score (P = 0.03). Statistical significance was also reached in VAS for radicular pain (P = 0.009) and ODI (P = 0.021) in patients with MC1 in the multivariate analysis with the non-Modic group used as reference. The authors concluded that patients with preoperative MC1 had better improvement of TDR compared with patients with MC2 or no MC.
Hellum et al. [38] evaluated if certain baseline characteristics could predict worse clinical outcome in patients treated with either rehabilitation or TDR in their prospective cohort study of 154 patients. They were randomized into a surgical (n = 88) group and a non-surgical group (n = 66). Of the 88 surgical patients, MC1 were present in 26, MC2 were present in 33, and mixed MC1 and MC2 were present in 15. Patients showing MC treated with TDR had better improvement in ODI (at least 15 points improvement) at 2-year follow-up (P = 0.04) compared with patients without MC. The authors concluded that shorter duration of LBP, low Fear-Avoidance Beliefs for work and MC1 or MC2 predicted better clinical outcome after treatment with disc prosthesis.
Discussion
Persisting LBP after simple discectomy for LDH is a well-known complication with a reported prevalence of 15–25 % at 2-years follow-up in a recent review [39]. An association of MC1 with LBP and unfavourable results of conservative treatment has been reported in several studies [40–44], although not in all [45]. Thus, MC1 may also influence the outcome of lumbar surgery. To the best of our knowledge, this is the first systematic literature review examining the impact of preoperative Modic changes on clinical outcome in lumbar spine surgery.
When confronted with a patient presenting lumbar disc herniation, leg and/or low back pain and MC on a preoperative MRI, results from the present review may be relevant when informing the patient of expected improvement in LBP after surgery, and when deciding upon type of surgical procedure.
A PubMed search identified 14 relevant studies (Table 1), including a total of 1652 operated patients, of which at least 804 patients (>49 %) showed preoperative MC.
The majority of the studies (n = 607) [7, 8, 10, 11, 34, 35] encompassed discectomy for LDH as surgical procedure. The two studies with the largest patient material found that preoperative MC1 was significantly correlated with worse outcome in ODI and smaller treatment effect (n = 187) [7] and significant worse outcome in LBP (n = 178) [8]. The findings were supported by a small pilot study [11] (n = 30), which was further limited by a short follow-up of 6 months and by the fact that the Modic group included both patients with MC1 or MC2. Likewise, it was limiting for the conclusions that one of the two studies with large patient material [7] was retrospective, and the other [8] actually found that only smoking was the single-independent risk factor of less improvement in LBP following discectomy. A synergistic interaction between smoking and MC1 was suggested, leading to less favourable clinical outcome. The study was further limited by the fact that 42 % of the original cohort was excluded because of unavailable or missing preoperative MRI scans, which may have introduced a selection bias. No correlation between preoperative MC1 and clinical outcome was found in two smaller studies [10, 34] (n = 45 and n = 41), of which one did not differentiate between the subtypes of MC, as the subgroups were too small to conduct a meaningful analysis. A significant association between MC1 and slower recovery of radicular pain was found in one study [35] (n = 126), although no difference was seen at final follow-up. However, the study was not designed to assess the effect of surgery.
Conclusively, the majority of the included patients across the discectomy studies showed a trend toward less improvement in LBP or ODI following discectomy for LDH in the presence of MC1. However, none of the studies commented on whether the difference in improvement in ODI or VAS for LBP surpassed a minimal clinically important difference (MCID). In general, for patients with chronic LBP, the MCID for improvement is typically around a 32 % reduction from baseline values [46] and the noise or imprecision of the measurement around 15–20 % of the full-scale range [47, 48]. Based on data from the articles, we calculated the percentage change in VAS for LBP and/or ODI from preoperative to postoperative follow-up. The difference in the percentage change between patients with or without MC ranged from only 8 to 20 %. It is thus very questionable whether the observed differences in clinical outcome in the present articles were of any clinically detectable level for the patients.
Is discectomy then still the optimal surgical approach in LDH patients with MC1 and primary leg symptoms, or should fusion also be contemplated? The published studies do not present sufficient evidence to answer this question. One may also argue that fusion based primarily on the preoperative presence of MC1 would be unnecessary due to the dynamic nature of MC [32]. Conversely, if MC1 are considered to be signs of mechanical instability [10, 24] and possibly corrected by fusion surgery, then an improved clinical outcome in LBP may ultimately be achieved. Ohtori et al. [27] and Vital et al. [31] supported the theory of fusion surgery leading to an acceleration of the conversion of MC1 to MC2, based on their comparison of preoperative and postoperative prevalence of MC subtypes in patients undergoing lumbar fusion surgery. Likewise, the presence of MC1, possibly implying weakening of the adjacent disc, has been suggested as a risk factor for reoperation for recurrent LDH after microendoscopic discectomy, based on an MC1 prevalence of 17.2 % in reoperated patients compared with 1.5 % in patients not undergoing additional surgery [49].
Only one study specifically aimed at comparing clinical outcome of discectomy versus fusion in the presence of MC. Cao et al. (n = 91) retrospectively found a significant improvement in LBP in patients undergoing iPLIF compared with patients undergoing simple discectomy [25]. However, conclusions drawn from the study were seriously restricted by (1) the included patients presented predominant LBP, thus many spine surgeons would contemplate to fuse irrespectively of the presence of MC; (2) the selection of the patients to each treatment method was biased: Concerns of the patient about cost or implant failure lead to discectomy as opposed to fusion; and (3) lack of analysis of outcome for the different subgroups of MC.
Only three fusion studies [27, 29, 30] (n = 454) have reported on the correlation between preoperative MC and clinical outcome. In all, the indication of fusion surgery was independent of the presence of preoperative MC, and the overall success rate of clinical improvement was acceptable. Two of the studies were prospective [27, 29] (n = 133), showing no correlation between clinical outcome of posterolateral fusion and preoperative MC. However, one presented a very selected material, including only patients with segmental lumbar instability [29] and the other only compared the outcome of 21 patients with MC1 with 11 patients with MC2 [27]. The third study retrospectively analysed the outcome of a more controversial treatment for LBP—stand alone PLIF—in 351 patients with DDD, and likewise found no correlation with preoperative MC1 or MC2 [30]. Thus, it may seem that preoperative MC does not influence the clinical outcome of fusion surgery. But in reality, in the context of preoperative MC, a study has yet to be published, including a significant number of patients fulfilling the prevailing criteria for fusion surgery—that is LBP refractory for conservative treatment and radiologically diagnosed lumbar degeneration, but not necessarily instability.
In four studies of patients with LBP undergoing TDR [33, 36–38] (n = 500), clinical outcome was correlated with the presence of preoperative MC (>42 %) and the MC subtypes, reporting conflicting results. In only one study (n = 221) [37], the primary aim was to test, whether MC had an impact on clinical outcome of TDR. A statistically significant higher improvement in patients with MC1 was demonstrated in two prospective studies [37, 38] (n = 309) and with MC2 in one retrospective study [33] (n = 99), but, as for the discectomy studies, it is questionable, whether the observed difference in the percentage change, ranging from 13 to 20 % (Fig. 1), surpassed the MCID. The fourth and prospective study [36] (n = 92) found no correlation with MC and clinical outcome but did not subgroup according to type of MC. In general, the patient populations of the TDR studies were highly selective, and a satisfactory clinical improvement was observed among patients both with and without MC. Based on the presented studies, it cannot be concluded whether MC or a certain subtype predicts better outcome when TDR is performed in patients fulfilling the reigning inclusion criteria. However, the prevailing possible correlation was between MC1 and improved clinical outcome.
In the context of MC, it could be interesting to evaluate differences in clinical outcome, when comparing surgery leaving the discus intact and surgery involving the intradiscal space. Barth et al. [6] found a correlation between postoperative developments of MC in patients with LDH undergoing standard discectomy compared with sequestrectomy. However, the surgical procedure of the included discectomy studies in the present review, either involved entering the intradiscal space [7, 9–11], or it was not described whether the disc space was entered [8, 35]. Thus, the analysis could not be made, based on the present patient material. Likewise, a comparison across the fusion studies was not possible, as the fusion procedures varied, and only one study [29] left the disc space intact.
In general, the level of evidence of the studies included in the present review was low, primarily due to small patient cohorts, affecting the possible demonstration of the impact of preoperative MC on postoperative clinical outcome. Combined with the fact that the possible difference in clinical outcome does not seem to be major, most studies were underpowered, and in accordance concluded that their findings needed confirmation in larger cohort studies. Furthermore, data known to influence the clinical outcome of spine surgery, such as smoking, comorbidities, co-interventions, educational level, compensation, and psychosocial factors [50, 51], were generally not evaluated. Only two studies looked at smoking as a confounding factor. Smoking is well acknowledged as a risk factor for less improvement following spine surgery [52–54].
Conclusion
Overall, there is currently a low quality of evidence available on the impact of preoperative Modic changes on clinical outcome of lumbar spine surgery. However, the larger the cohort examined in the individual study, the greater the tendency was toward preoperative MC1 showing a statistical significant impact on clinical outcome.
In the presence of preoperative MC1, patients undergoing discectomy for lumbar disc herniation seem to present equal improvement in leg pain, but less improvement in low back pain. However, it is questionable whether the difference surpasses a minimal clinically important difference. So far, preoperative MC alone does not seem to justify adding fusion surgery to a discectomy in patients with a herniated disc and predominant leg pain.
In patients undergoing fusion surgery for predominant LBP and radiologically diagnosed lumbar degeneration, the level of evidence of the published articles does not allow any conclusions on the impact of MC alone on postoperative clinical outcome.
In patients undergoing total disc replacement for degenerative disc disease, the published articles do not allow any conclusions on the impact of MC subtypes alone on the postoperative clinical outcome, but MC1 may be correlated with improved clinical outcome.
Future studies should include a larger patient material, state whether the observed differences in clinical outcome surpass the minimal clinically important difference, as well as include an analysis of known confounding factors with potential influence on the clinical outcome of spine surgery.
References
Modic MT et al (1988) Degenerative disk disease: assessment of changes in vertebral body marrow with MR imaging. Radiology 166(1 Pt 1):193–199
Emch TM, Modic MT (2011) Imaging of lumbar degenerative disk disease: history and current state. Skelet Radiol 40(9):1175–1189
Modic MT et al (1988) Imaging of degenerative disk disease. Radiology 168(1):177–186
el Barzouhi A et al (2014) Back pain’s association with vertebral end-plate signal changes in sciatica. Spine J 14(2):225–233
Thome C et al (2005) Outcome after lumbar sequestrectomy compared with microdiscectomy: a prospective randomized study. J Neurosurg Spine 2(3):271–278
Barth M et al (2008) Two-year outcome after lumbar microdiscectomy versus microscopic sequestrectomy: part 2: radiographic evaluation and correlation with clinical outcome. Spine (Phila Pa 1976) 33(3):273–279
Lurie JD et al (2013) Magnetic resonance imaging predictors of surgical outcome in patients with lumbar intervertebral disc herniation. Spine (Phila Pa 1976) 38(14):1216–1225
Sorlie A et al (2012) Modic type I changes and recovery of back pain after lumbar microdiscectomy. Eur Spine J 21(11):2252–2258
Rahme R et al (2011) Lumbar microdiscectomy: a clinicoradiological analysis of outcome. Can J Neurol Sci 38(3):439–445
Ohtori S et al (2010) Low back pain after lumbar discectomy in patients showing endplate modic type 1 change. Spine (Phila Pa 1976) 35(13):E596–E600
Chin KR et al (2008) Success of lumbar microdiscectomy in patients with modic changes and low-back pain: a prospective pilot study. J Spinal Disord Tech 21(2):139–144
Albert HB et al (2008) Modic changes, possible causes and relation to low back pain. Med Hypotheses 70(2):361–368
Jensen TS et al (2008) Vertebral endplate signal changes (Modic change): a systematic literature review of prevalence and association with non-specific low back pain. Eur Spine J 17(11):1407–1422
Jensen RK et al (2012) Is the development of Modic changes associated with clinical symptoms? A 14-month cohort study with MRI. Eur Spine J 21(11):2271–2279
Maatta JH et al (2015) ISSLS prize winner: vertebral endplate (Modic) change is an independent risk factor for episodes of severe and disabling low back pain. Spine (Phila Pa 1976) 40(15):1187–1193
Weishaupt D et al (2001) Painful lumbar disk derangement: relevance of endplate abnormalities at MR Imaging. Radiology 218(2):420–427
Braithwaite I et al (1998) Vertebral end-plate (Modic) changes on lumbar spine MRI: correlation with pain reproduction at lumbar discography. Eur Spine J 7(5):363–368
Ohtori S et al (2006) Tumor necrosis factor-immunoreactive cells and PGP 9.5-immunoreactive nerve fibers in vertebral endplates of patients with discogenic low back Pain and Modic Type 1 or Type 2 changes on MRI. Spine (Phila Pa 1976) 31(9):1026–1031
Albert HB et al (2013) Antibiotic treatment in patients with chronic low back pain and vertebral bone edema (Modic type 1 changes): a double-blind randomized clinical controlled trial of efficacy. Eur Spine J 22(4):697–707
Albert HB et al (2013) Does nuclear tissue infected with bacteria following disc herniations lead to Modic changes in the adjacent vertebrae? Eur Spine J 22(4):690–696
Albert HB et al (2008) Antibiotic treatment in patients with low-back pain associated with Modic changes Type 1 (bone oedema): a pilot study. Br J Sports Med 42(12):969–973
Albert HB et al (2011) The prevalence of MRI-defined spinal pathoanatomies and their association with modic changes in individuals seeking care for low back pain. Eur Spine J 20(8):1355–1362
Jensen TS et al (2010) Predictors of new vertebral endplate signal (Modic) changes in the general population. Eur Spine J 19(1):129–135
Hayashi T et al (2015) Motion characteristics and related factors of Modic changes in the lumbar spine. J Neurosurg Spine 22(5):511–517
Cao P et al (2014) Comparison of simple discectomy and instrumented posterior lumbar interbody fusion for treatment of lumbar disc herniation combined with Modic endplate changes. Chin Med J (Engl) 127(15):2789–2794
Eser O et al (2013) Dynamic stabilisation in the treatment of degenerative disc disease with modic changes. Adv Orthop 2013:806267
Ohtori S et al (2010) Change in Modic type 1 and 2 signals after posterolateral fusion surgery. Spine (Phila Pa 1976) 35(12):1231–1235
Zhao D et al (2013) Surgical options and clinical outcomes in patients of lumbar disc herniation with Modic changes. Zhonghua Yi Xue Za Zhi 93(39):3111–3115
Ghodsi SM et al (2015) Frequency of vertebral endplate Modic changes in patients with unstable lumbar spine and its effect on surgical outcome. Asian Spine J 9(5):737–740
Kwon YM et al (2009) Long term efficacy of posterior lumbar interbody fusion with standard cages alone in lumbar disc diseases combined with Modic changes. J Korean Neurosurg Soc 46(4):322–327
Vital JM et al (2003) Course of Modic 1 six months after lumbar posterior osteosynthesis. Spine (Phila Pa 1976) 28(7):715–720 (discussion 721)
Jensen TS et al (2009) Characteristics and natural course of vertebral endplate signal (Modic) changes in the Danish general population. BMC Musculoskelet Disord 10:81
Gornet MF et al (2014) Optimizing success with lumbar disc arthroplasty. Eur Spine J 23(10):2127–2135
Rahme R et al (2010) What happens to Modic changes following lumbar discectomy? Analysis of a cohort of 41 patients with a 3- to 5-year follow-up period. J Neurosurg Spine 13(5):562–567
Schistad EI et al (2014) The association between Modic changes and pain during 1-year follow-up in patients with lumbar radicular pain. Skelet Radiol 43(9):1271–1279
Siepe CJ et al (2006) Clinical results of total lumbar disc replacement with ProDisc II: three-year results for different indications. Spine (Phila Pa 1976) 31(17):1923–1932
Blondel B et al (2011) Clinical results of lumbar total disc arthroplasty in accordance with Modic signs, with a 2-year-minimum follow-up. Spine (Phila Pa 1976) 36(26):2309–2315
Hellum C et al (2012) Predictors of outcome after surgery with disc prosthesis and rehabilitation in patients with chronic low back pain and degenerative disc: 2-year follow-up. Eur Spine J 21(4):681–690
Parker SL et al (2015) Incidence of low back pain after lumbar discectomy for herniated disc and its effect on patient-reported outcomes. Clin Orthop Relat Res 473(6):1988–1999
Albert HB, Manniche C (2007) Modic changes following lumbar disc herniation. Eur Spine J 16(7):977–982
Kjaer P et al (2005) Magnetic resonance imaging and low back pain in adults: a diagnostic imaging study of 40-year-old men and women. Spine (Phila Pa 1976) 30(10):1173–1180
Toyone T et al (1994) Vertebral bone-marrow changes in degenerative lumbar disc disease. An MRI study of 74 patients with low back pain. J Bone Joint Surg Br 76(5):757–764
Jarvinen J et al (2015) Association between changes in lumbar Modic changes and low back symptoms over a two-year period. BMC Musculoskelet Disord 16:98
Jensen OK et al (2014) Type 1 Modic changes was a significant risk factor for 1-year outcome in sick-listed low back pain patients: a nested cohort study using magnetic resonance imaging of the lumbar spine. Spine J 14(11):2568–2581
Keller A et al (2012) Are Modic changes prognostic for recovery in a cohort of patients with non-specific low back pain? Eur Spine J 21(3):418–424
Mannion AF et al (2006) Development of a German version of the Oswestry Disability Index. Part 2: sensitivity to change after spinal surgery. Eur Spine J 15(1):66–73
Mannion AF et al (2006) Development of a German version of the Oswestry Disability Index. Part 1: cross-cultural adaptation, reliability, and validity. Eur Spine J 15(1):55–65
Hagg O et al (2003) The clinical importance of changes in outcome scores after treatment for chronic low back pain. Eur Spine J 12(1):12–20
Hong X et al (2015) Characterization and risk factor analysis for reoperation after microendoscopic diskectomy. Orthopedics 38(6):e490–e496
Lakke SE et al (2009) Risk and prognostic factors for non-specific musculoskeletal pain: a synthesis of evidence from systematic reviews classified into ICF dimensions. Pain 147(1–3):153–164
Haugen AJ et al (2012) Prognostic factors for non-success in patients with sciatica and disc herniation. BMC Musculoskelet Disord 13:183
Sanden B, Forsth P, Michaelsson K (2011) Smokers show less improvement than nonsmokers two years after surgery for lumbar spinal stenosis: a study of 4555 patients from the Swedish spine register. Spine (Phila Pa 1976) 36(13):1059–1064
Andersen T et al (2001) Smoking as a predictor of negative outcome in lumbar spinal fusion. Spine (Phila Pa 1976) 26(23):2623–2628
Glassman SD et al (2000) The effect of cigarette smoking and smoking cessation on spinal fusion. Spine (Phila Pa 1976) 25(20):2608–2615
Acknowledgments
No funding or grants have been received for the present study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Laustsen, A.F., Bech-Azeddine, R. Do Modic changes have an impact on clinical outcome in lumbar spine surgery? A systematic literature review. Eur Spine J 25, 3735–3745 (2016). https://doi.org/10.1007/s00586-016-4609-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-016-4609-y