
Abstract
Objective
Fungal rhinosinusitis occurs in different forms depending on race and region. While allergic fungal rhinosinusitis is common in Caucasians, fungal ball (FB) is more common in Asians. However, most cases are reported as unilateral, and clinical data on bilateral FB (BFB) are rare. Therefore, the purpose of this study was to analyze and to compare the clinical characteristics of BFB and unilateral FB (UFB) in Koreans.
Methods
We retrospectively analyzed medical records and computed tomography (CT) images of 434 patients diagnosed with FB. The patients were divided into two groups: BFB and UFB. Demographic data, multiple allergen simultaneous test including total or specific immunoglobulin E (IgE) levels, symptoms, CT findings, treatment, and outcomes were analyzed.
Results
Among the patients, 26 had BFB and 408 had UFB. Hypertension was noted in 61.5% of the BFB and 39% of the UBF individuals (p = 0.023). While total IgE levels were similar between the two groups, Dermatophagoides pteronyssinus (p = 0.004), Cladosporium (p = 0.017), and Aspergillus-specific IgE positivity (p = 0.025) were significantly higher in the BFB than in the UFB group. Not only symptoms such as postnasal drip (p = 0.013), mucopurulent rhinorrhea (p = 0.009), and foul odor (p = 0.037), but also sphenoid sinus involvement on CT images were more common in the BFB than in the UFB group (p = 0.011).
Conclusion
Patients with BFB in Korea showed more common hypertension and symptoms of foul odor, mucopurulent rhinorrhea, and postnasal drip with allergy positivity compared to those with UFB. Therefore, understanding clinical characteristics of BFB will allow clinicians to approach BFB more appropriately.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Fungal rhinosinusitis (FRS) is a form of sinusitis wherein fungi are involved in the immunopathogenesis [1]. FRS occurs in about 10% of patients requiring nasal or sinus surgeries and is most commonly classified into non-invasive FRS and invasive FRS depending on the presence or absence of fungal hyphae in the tissues detected using microscopic examination [2]. In general, non-invasive FRS was classified as fungal ball (FB) or allergic fungal rhinosinusitis (AFRS) [3]. These can be classified histologically according to the presence of dense conglomerated fungal hyphae without tissue invasion [2] or eosinophilic mucin with inflammatory cells, Charcot-Leyden crystals, and branching non-invasive fungal hyphae [4]. Especially, FB is known to be the most common subtype of FRS, accounting for 53.2–72% of FRS [5]. Due to the development of imaging technologies, such as endoscopy, computed tomography (CT), and magnetic resonance imaging (MRI) as well as increased life expectancy, the incidence of FRS and FB have increased over the past several decades [5,6,7].
Interestingly, prevalence and incidence of FRS is known to differ not only ethnically but also regionally. It occurs commonly in the form of AFRS in Caucasians [8], while FB is more common in Asians [9]. In addition, AFRS is more common in India, the Middle-East, and the southeastern parts of the United States, such as Alabama, Georgia, and Texas, which are hot and dry in climate [10,11,12]. Meanwhile, FB is common in France, Italy, Taiwan, and Korea [13,14,15,16,17,18]. However, FB mostly occurs unilaterally, and little is known about sinonasal FB in bilateral paranasal sinuses due to its rarity.
In addition, the incidence of unilateral fungal ball (UFB) has recently been reported to increase [19], and that of bilateral fungal ball (BFB) may follow similar tendency to UFB. Nevertheless, there have been a few reports of BFB in paranasal sinuses, only small numbers of BFB patients in these studies were included [9, 13, 20,21,22]. Additionally, studies on the clinical features of BFB and UFB are lacking. Therefore, the aim of this study was to analyze and compare the clinical characteristics of BFB and UFB in Korean patients.
Materials and methods
Study design
We retrospectively reviewed electronic medical charts including pathology reports and CT images for 434 FB patients between January 2008 and June 2018. All patients were finally diagnosed through postoperative histopathologic examination. FB was defined as an accumulation of dense conglomerated fungal hyphae in the sinuses without tissue invasion [2], and patients diagnosed with AFRS and invasive fungal rhinosinusitis were excluded. Especially, using the diagnostic criteria of AFRS described by Bent and Kuhn et al. [4] we defined AFRS as the presence of eosinophilic mucin with inflammatory cells, Charcot-Leyden crystals, and branching non-invasive fungal hyphae based on histologic findings. Periodic acid-Schiff staining or Grocott’s methenamine silver staining was performed to confirm fungal hyphae in the tissues and identify individual species according to morphology, such as the angle of hyphae. The subjects were divided into two groups depending on where lesions were located: BFB versus UFB. Demographic data, underlying diseases including hypertension, diabetes mellitus, and autoimmune disease, symptoms, treatment, and outcomes, were investigated. The Korean version of the Sniffin' Sticks Test II was used to test for olfactory disorders [23]. Total and specific Immunoglobulin E (IgE) levels in all patients were measured by multiple allergen simultaneous tests (MAST), consisting of antigens such as house dust mites, fungi, tree pollens, and weed pollens. Cases of more than Class 2 (0.70 IU/ml) were considered to be positive for the antigen [24]. CT scans were evaluated by a radiologist using the impression of chronic rhinosinusitis rather than FRS. To evaluate differences in the anatomical variations of the paranasal sinus between the two groups, the presence of septal deviation, concha bullosa, and Haller cells was examined. CT images were also used to identify the presence of calcifications or soft-tissue densities in the FB lesions and to examine the involved sinuses, including the ethmoid, maxillary, frontal, and sphenoid sinuses. In the case of BFB, the distribution of lesions on both sides was also evaluated.
Statistical analysis
All statistical analyzes were performed using IBM SPSS Statistics for Windows Version 23.0 (IBM Corp., Armonk, NY, USA). Continuous data are presented as means ± standard deviations, while categorical data are presented as a percentage of the group total. Student’s t tests were performed according to the results of a Kolmogorov–Smirnov test. Differences in categorical data between the two groups were compared using chi-square tests or Fisher’s exact test. P values < 0.05 were considered statistically significant.
Results
Subject characteristics
The demographic data of the 434 FB patients included in this study are shown in Table 1. The BFB group comprised 26 (6.0%) patients, and the UFB group included 408 (94.0%). The mean age was 63.6 ± 12.5 years in the BFB group and 60.2 ± 12.2 years in the UFB group (p = 0.174). The BFB group included 18 (69.2%) women and the UFB group included 279 (68.4%) women (p = 0.928). The proportion of patients with hypertension was larger in the BFB group (n = 16, 61.5%) than in the UFB group (n = 159, 39.0%), a statistically significant difference (p = 0.023). However, no statistical difference was observed between the two groups in the incidence of diabetes mellitus or autoimmune disease. Among the revision cases, the incidence of BFB (3 cases, 11.5%) was higher than that of UFB (13 cases, 3.2%), but there was no statistically significant difference between the two groups (p = 0.064). Although total IgE positivity showed no statistical difference (p = 0.54), specific IgE levels for Dermatophagoides pteronyssinus, Cladosporium, and Aspergillus were significantly higher in the BFB group than in the UFB group (p = 0.004, p = 0.017, and p = 0.023, respectively). Results of KVSS II revealed no statistical intergroup differences.
Differences in symptomatology
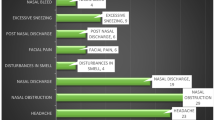
Patient symptoms in the two groups are shown in Table 2. Three (11.5%) patients in the BFB group and 74 (18.1%) in the UFB group were diagnosed incidentally without any symptoms. These patients had undergone CT or MRI as part of a health examination or diagnosis of other diseases, and FB was diagnosed via a postoperative pathological examination. Nasal obstruction was found in 26.9% of patients in the BFB group and 28.9% in the UFB group (p = 0.827). More patients complained of facial pain in the UFB group (12.3%) than in the BFB group (3.8%), but without statistical significance (p = 0.342). In addition, there were no differences between the two groups in regards to complaints of headache, toothache, and orbital pain. However, postnasal drip (50% vs. 27.2%, p = 0.013), mucopurulent rhinorrhea (46.2% vs. 23.3%, p = 0.009), and foul odor (23.1% vs. 9.3%, p = 0.037) were more frequent in the BFB group than in the UFB group, with statistical significance.
Comparison of CT findings
The CT features of the two groups are shown in Table 3. Septal deviation was observed in 46.2% of patients in the BFB group and 38.6% in the UFB group (p = 0.442). Concha bullosa was found in 19.2% in the BFB group and 7.6% in the UFB group (p = 0.054). The proportion of Haller cells was similar between the BFB and UFB groups (15.4% and 15.2%, respectively, p = 1.000). Calcification was observed in 80.8% in the BFB group and 73% in the UFB group (p = 0.383). In contrast, soft-tissue density was noted in 19.2% in the BFB group and 26.2% in the UFB group (p = 0.429). In both groups, calcification was more frequent than soft-tissue density. A comparison of the involved sinuses showed no statistically significant intergroup differences in the maxillary, ethmoid, and frontal sinuses. Meanwhile, sphenoid sinus involvement was observed in 30.8% in the BFB group and in 11.8% in the UFB group, with a statistically significant difference (p = 0.011).
We also evaluated the location of involved sinuses in patients with BFB (Table 4). In 21 (80.8%) patients, one sinus on each side was involved, whereas, in five (19.2%) patients, one or more sinuses were involved on each side. The most commonly involved sinus in BFB was the maxillary sinus on each side in 15 (57.7%) patients. In cases of more than one sinus on each side, bilateral maxillary sinus involvement was the most common; bilateral frontal sinus involvement was not observed.
Treatment and outcomes
A comparison of the treatment outcomes between the two groups is shown in Table 5. All patients in both the groups underwent endoscopic sinus surgery. The mean follow-up periods were 6.5 ± 5.4 months in the BFB group and 6.6 ± 9.1 months in the UFB group (p = 0.577). Two (7.7%) patients in the BFB group and 10 (2.5%) in the UFB group experienced recurrence, although without any statistical difference (p = 0.157). Aspergillus species was most commonly found in both groups (92.3% vs. 94.4%, respectively, p = 0.655). Mucor species (1.2%) and Candida species (1.0%) were observed only in the UFB group, although the difference was statistically insignificant. Two (7.7%) patients in the BFB group and 17 (3.4%) in the UFB group had histologically confirmed fungal ball, but the subtypes were undetermined.
Discussion
Most cases of fungal ball in the paranasal sinus are known to occur in individuals of older age, an average age of 64 years [2]. The average age of the 8 patients with BFB who participated in the study by Lee et al. was 59.3 years [9]. In this study, all patients with UFB and BFB showed a similar age range (60–63 years). In addition, we found a two times higher female predominance for the incidence of both BFB and UFB unlike the 1:1 sex ratio of BFB in Lee et al. study [9]. These differences are believed to have resulted from the small number of BFB patients in the study by Lee et al. Nevertheless, our finding is consistent with that of other studies with respect to a female predominance [25,26,27]. There are several studies on the presence or absence of underlying diseases, such as hypertension and diabetes mellitus, in patients with FB [2, 19]. In previous reports, 8–14.6% of patients with FB had diabetes mellitus, which was similar to the results in the current study [19, 28]. In addition, other studies reported that 15–21.7% of patients with FB had hypertension [19, 28], although 61.5% of patients with BFB and 39% of those with UFB had hypertension in our study. Lee et al. [9] reported that two of eight patients with BFB had hypertension (25%). On the other hand, two diagnosed with BFB among the 69 FRS patients showed that all had hypertension (100%) [17]. Although the cause of the close relationship between hypertension and FB in this study is not clear, further studies are required to verify this relationship.
In the present study, an immunologic examination did not reveal an intergroup difference in total IgE levels. However, specific IgE positivity to Dermatophagoides pteronyssinus, Clodosporium, and Aspergillus was significantly higher in the BFB group. Although Collins et al. reported that AFRS was correlated with fungus-specific IgE levels [29], there has been no report of correlation between specific IgE and occurrence of FB to this day. We think that high specific IgE levels in BFB may be associated with easy FB formation after secondary obstruction due to an allergic reaction in the sinus. In addition, the racial and regional difference in allergic reaction may be related to these reactions. Nevertheless, further study will be required to understand the reason for the increased specific IgE positivity in BFB.
Lai et al. [22] described the common symptoms of FB, including nasal obstruction, mucopurulent discharge, postnasal drip, and facial pain, which are similar to those of chronic rhinosinusitis [13]. In this study, the main symptoms in the BFB group were postnasal drip, mucopurulent rhinorrhea, nasal obstruction, foul odor, and headache, in that order. Among these symptoms, postnasal drip, mucopurulent rhinorrhea, and foul odor showed higher incidence in the BFB compared to UFB. Meanwhile, anatomical variations on CT, such as septal deviation, concha bullosa, and Haller cells, were not found to be correlated with the occurrence of FB [30]. Similarly, these anatomical variations did not significantly differ according to the occurrence of FB in this study. Maxillary sinus was the most commonly involved site of FB, similar to other reports [9, 22]. Also, sphenoid sinus in patients with BFB was more involved than in those with UFB. In addition, the percentages of calcification within the involved sinus on CT images were 80.8% in BFB and 73% in UFB, similar or somewhat higher to previous studies ranged from 66 to 69% [7, 9].
In other studies, endoscopic sinus surgery was performed for the treatment of FB, and the results were mostly successful [9, 13, 22, 28]. All patients in our study were also eligible for endoscopic surgery. Although recurrence rate was higher in BFB than in UFB, all cases of recurrence in BFB occurred in sphenoid sinus, and we assumed that it may be attributed to a poor surgical visual field and incomplete removal due to complicated anatomy. To prevent recurrence, surgeons must thoroughly examine the remaining lesion, especially parts that cannot be clearly visualized. In addition, postoperative pathological examination is needed to identify invasive or non-invasive FRS and to make a final diagnosis [3]. Aspergillus spp. are the most commonly found fungi in the FB [25]. In this study, fungal species were identified morphologically from a postoperative specimen, and more than 90% of BFB patients had Aspergillus species, which was similar to UFB patients and was in accordance with a previous report [25].
The merit of this paper is that it included more patients with BFB than did previous studies, thereby allowing for better representation of the clinical characteristics of BFB in Korea; BFB patients were more likely to have hypertension, more common nasal symptoms, and higher allergy positivity to fungi and kinds of house dust mite than UFB patients. However, the main drawback of this study is that the results can differ according to region and ethnicity. The clinical features in Western and other Asian countries may different. Thus, a comparison study according to region and ethnicity need be followed to verify our findings.
Conclusion
Although treatments and outcomes were similar between BFB and UFB in this study, patients with BFB in Korea showed more common hypertension and symptoms of foul odor, mucopurulent rhinorrhea, and postnasal drip with allergy positivity than those with UFB. Therefore, understanding clinical characteristics of BFB will help clinicians to approach BFB more appropriately.
References
Chakrabarti A, Kaur H (2016) AllergicAspergillus rhinosinusitis. J Fungi (Basel) 2(4)
Grosjean P, Weber R (2007) Fungus balls of the paranasal sinuses: a review. Eur Arch Otorhinolaryngol 264(5):461–470
Chakrabarti A, Denning DW, Ferguson BJ, Ponikau J, Buzina W, Kita H, Marple B, Panda N, Vlaminck S, Kauffmann-Lacroix C, Das A, Singh P, Taj-Aldeen SJ, Kantarcioglu AS, Handa KK, Gupta A, Thungabathra M, Shivaprakash MR, Bal A, Fothergill A, Radotra BD (2009) Fungal rhinosinusitis: a categorization and definitional schema addressing current controversies. Laryngoscope 119(9):1809–1818
Bent JP 3rd, Kuhn FA (1994) Diagnosis of allergic fungal sinusitis. Otolaryngol Head Neck Surg 111(5):580–588
Mensi M, Salgarello S, Pinsi G, Piccioni M (2004) Mycetoma of the maxillary sinus: endodontic and microbiological correlations. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 98(1):119–123
Robey AB, O'Brien EK, Richardson BE, Baker JJ, Poage DP, Leopold DA (2009) The changing face of paranasal sinus fungus balls. Ann Otol Rhinol Laryngol 118(7):500–505
Yoon YH, Xu J, Park SK, Heo JH, Kim YM, Rha KS (2017) A retrospective analysis of 538 sinonasal fungus ball cases treated at a single tertiary medical center in Korea (1996–2015). Int Forum Allergy Rhinol 7(11):1070–1075
Torres C, Ro JY, El-Naggar AK, Sim SJ, Weber RS, Agalya AG (1996) Allergic fungal sinusitis: a clinicopathologic study of 16 cases. Hum Pathol 27(8):793–799
Lee DH, Joo YE, Lim SC (2013) Fungus balls of the bilateral paranasal sinuses. Indian J Otolaryngol Head Neck Surg 65(Suppl 2):320–323
Panda NK, Sharma SC, Chakrabarti A, Mann SB (1998) Paranasal sinus mycoses in north India. Mycoses 41(7–8):281–286
Rupa V, Jacob M, Mathews MS, Job A, Kurien M, Chandi SM (2002) Clinicopathological and mycological spectrum of allergic fungal sinusitis in South India. Mycoses 45(9–10):364–367
Michael RC, Michael JS, Ashbee RH, Mathews MS (2008) Mycological profile of fungal sinusitis: an audit of specimens over a 7-year period in a tertiary care hospital in Tamil Nadu. Indian J Pathol Microbiol 51(4):493–496
Klossek JM, Serrano E, Peloquin L, Percodani J, Fontanel JP, Pessey JJ (1997) Functional endoscopic sinus surgery and 109 mycetomas of paranasal sinuses. Laryngoscope 107(1):112–117
Dufour X, Kauffmann-Lacroix C, Ferrie JC, Goujon JM, Rodier MH, Klossek JM (2006) Paranasal sinus fungus ball: epidemiology, clinical features and diagnosis. A retrospective analysis of 173 cases from a single medical center in France, 1989–2002. Med Mycol 44(1):61–67
Pagella F, Matti E, De Bernardi F, Semino L, Cavanna C, Marone P, Farina C, Castelnuovo P (2007) Paranasal sinus fungus ball: diagnosis and management. Mycoses 50(6):451–456
Hsiao CH, Li SY, Wang JL, Liu CM (2005) Clinicopathologic and immunohistochemical characteristics of fungal sinusitis. J Formos Med Assoc 104(8):549–556
Lee BJ, Kim H, Kim JH, Kim YJ (1998) Fungal sinusitis: clinical features and treatment outcomes with emphasis on endoscopic sinus surgery. Korean J Otorhinolaryngol-Head Neck Surg 41(3):318–322
Kim JS, So SS, Kwon SH (2017) The increasing incidence of paranasal sinus fungus ball: a retrospective cohort study in two hundred forty-five patients for fifteen years. Clin Otolaryngol 42(1):175–179
Lee JS, Shin SY, Lee KH, Kim SW, Cho JS (2013) Change of prevalence and clinical aspects of fungal ball according to temporal difference. Eur Arch Otorhinolaryngol 270(5):1673–1677
Ferreiro JA, Carlson BA, Cody DT 3rd (1997) Paranasal sinus fungus balls. Head Neck 19(6):481–486
Nicolai P, Lombardi D, Tomenzoli D, Villaret AB, Piccioni M, Mensi M, Maroldi R (2009) Fungus ball of the paranasal sinuses: experience in 160 patients treated with endoscopic surgery. Laryngoscope 119(11):2275–2279
Lai JC, Lee HS, Chen MK, Tsai YL (2011) Patient satisfaction and treatment outcome of fungus ball rhinosinusitis treated by functional endoscopic sinus surgery. Eur Arch Otorhinolaryngol 268(2):227–230
Hong SC, Yoo YS, Kim ES, Kim SC, Park SH, Kim JK, Kang SH (1999) Development of KVSS Test (Korean Version of Sniffin' Sticks Test). Korean J Otorhinolaryngol-Head Neck Surg 42(7):855–860
Rim JH, Park BG, Kim JH, Kim HS (2016) Comparison and clinical utility evaluation of four multiple allergen simultaneous tests including two newly introduced fully automated analyzers. Pract Lab Med 4:50–61
Callejas CA, Douglas RG (2013) Fungal rhinosinusitis: what every allergist should know. Clin Exp Allergy 43(8):835–849
Ferguson BJ (2000) Fungus balls of the paranasal sinuses. Otolaryngol Clin N Am 33(2):389–398
Nomura K, Asaka D, Nakayama T, Okushi T, Matsuwaki Y, Yoshimura T, Yoshikawa M, Otori N, Kobayashi T, Moriyama H (2013) Sinus fungus ball in the Japanese population: clinical and imaging characteristics of 104 cases. Int J Otolaryngol 2013:731640
Kim SW, Park YJ, Kim SW, Kang MG, Joo YH, Cho JH (2005) A Clinical analysis of fungal sinusitis. Korean J Otorhinolaryngol-Head Neck Surg 48(3):332–337
Collins M, Nair S, Smith W, Kette F, Gillis D, Wormald PJ (2004) Role of local immunoglobulin E production in the pathophysiology of noninvasive fungal sinusitis. Laryngoscope 114(7):1242–1246
Tsai TL, Lan MY, Ho CY (2012) There is no structural relationship between nasal septal deviation, concha bullosa, and paranasal sinus fungus balls. Sci World J 2012:181246
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
SHA: study concept and design, drafting of manuscript, manuscript revision. EJL: interpretation of data, revision of manuscript, MPH and GCS: collecting data, KSK: study concept and design, revision of manuscript, interpretation of data, approval of final version of manuscript to be published.
Corresponding author
Ethics declarations
Conflict of interest
All authors declared no conflicts of interest.
Informed consent and ethics committee review approval
This study was reviewed and approved by the Institutional Review Board (IRB). The study was also conducted in accordance with the ethical standards of the institutional and/or national research committee, 1964 Helsinki Declaration and subsequent amendments, or similar ethical standards.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ahn, S.H., Lee, E.J., Hong, M.P. et al. Comparison of the clinical characteristics of bilateral and unilateral fungal balls in Korea. Eur Arch Otorhinolaryngol 276, 1975–1980 (2019). https://doi.org/10.1007/s00405-019-05408-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-019-05408-6