
Abstract
Selvester QRS scoring system has an advantage of being inexpensive and easily accessible for estimating myocardial infarct (MI) size. We assessed the correlation and agreement between QRS score and total perfusion deficit (TPD) calculated by quantitative gated single-photon emission computed tomography (QGS) in patients with prior anterior MI undergoing coronary intervention. Sixty-six patients with prior anterior MI and 66 age- and sex-matched control subjects were enrolled. QRS score was obtained using a 50-criteria and 31-point system. QRS score was significantly higher in patients with prior anterior MI than control subjects (12.8 ± 8.9 vs 1.1 ± 2.7 %, p < 0.001). In overall patients (n = 132), QRS score was correlated well with TPD (r = 0.81, p < 0.001). This good correlation was found even in patients with TPD ≤40 % (n = 126) or in patients with TPD ≤30 % (n = 117). In overall patients, MI size estimated by QRS score was 7.0 ± 8.8 %, which was significantly smaller than TPD, 11.4 ± 14.0 % (p < 0.001). Bland–Altman plot showed that there was an increasing difference between QRS score and TPD with increasing MI size. When Blant–Altman plots were applied to patients with TPD ≤40 % and further in patients with TPD ≤30 %, the difference between QRS score and TPD became smaller, and the agreement became better. In overall patients, QRS score was correlated well with QGS measurements, such as end-diastolic volume (r = 0.62, p < 0.001), end-systolic volume (r = 0.67, p < 0.001), or ejection fraction (r = −0.73, p < 0.001). Our results suggest that QRS score reflects TPD well in patients with prior anterior MI, whose TPD is less than approximately 30 % even in the coronary intervention era.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The 12-lead electrocardiogram (ECG) is a routine examination in diagnosing coronary artery disease [1]. R-wave regression and pathologic Q wave can appear after myocardial infarction (MI). Selvester et al. developed a quantitative QRS scoring system for estimating MI size based on these ECG variables [2–6]. This measurement has an advantage of being inexpensive and easily accessible. On the other hand, the role of quantitative gated single-photon emission computed tomography (SPECT) is well established for evaluating MI size [7]. Total perfusion deficit (TPD) is a quantitative and reliable parameter representing both severity and extent of myocardial perfusion abnormality [8.9]. It is important to reexamine the accuracy of QRS score in comparison with TPD as the reference standard for estimating MI size in the coronary intervention era [10–14]. In this study, we assessed the correlation and agreement between QRS score and TPD in patients with prior anterior MI undergoing coronary intervention.
Methods
Patients
Between September 2013 and August 2015, 985 patients underwent ECG and SPECT for evaluating coronary artery disease. Of these, 79 patients with prior anterior MI beyond at least more than 12 months after the onset were retrospectively selected. Prior anterior MI was confirmed by the medical records of chest pain for more than 30 min, elevation of serum creatine kinase to more than twice the normal upper limit, and a culprit lesion of the left anterior descending artery on angiography. The following patients were excluded: those with atrial fibrillation (n = 3); bundle branch block (n = 3); hemodialysis (n = 3); and no emergency coronary intervention (n = 4). Finally, 66 patients with prior anterior MI were enrolled. Sixty-six age- and sex-matched control subjects who had no myocardial damage or ischemia assessed by SPECT were selected. Informed consent was obtained from all patients with prior anterior MI and control subjects.
ECG
A 12-lead ECG was recorded before SPECT at a paper speed of 25 mm/s and an amplification of 10 mm/mV. The Selvester QRS scoring system was used to estimate MI size [2–6]. With visual inspection, Q-, R- and S-wave amplitudes, Q- and R-wave durations, and R/Q and R/S ratio were measured and checked against the established criteria. QRS score was obtained using a 50-criteria and 31-point system (Table 1). All measurements were performed by the same experienced cardiologists blinded to patient characteristics-. The inter- and intra-observer variability for the repeated measurements of QRS score in 40 patients were 0.23 ± 0.80 and 0.30 ± 0.69, respectively. Each point was designed to represent 3 % MI of the left ventricle [2–6].
Thallium-201 gated SPECT
All patients fasted overnight, and underwent stress-redistribution thallium-201 (Tl-201) gated SPECT [15, 16]. Adenosine was infused at 120 µg/kg/min over 6 min. This is the usual dose clinically used in Japan. Tl-201 (111 MBq) was injected 3 min after the initiation of adenosine infusion. The stress Tl-201 SPECT acquisition was started 5 min after the stress test. Four hours later, redistribution images were also obtained. ECG-gated myocardial perfusion images were acquired with a dual-detector 90°γ-camera (Brightview X; Philips). Images were acquired with the following parameters: 36 total projections; 180° from right anterior oblique to left posterior oblique and a non-circular orbit; 64 × 64 matrix; 6.4 mm pixel size; 16 frames per cardiac cycle; low-energy, high-resolution collimation; and 40 s per stop. Tl-201 SPECT images were acquired with a 10 % symmetric window over the 80 keV Tl-201 photopeak. Images were reconstructed using ordered-subset expectation maximization (iteration, 2; subset, 9) with a Butterworth filter (order, 8; cut-off frequency, 0.50 cycles/pixel for stress image, and 0.45 cycles/pixel for redistribution image). No scatter or attenuation correction was applied.
Quantitative analysis
TPD represents both the extent and severity of a perfusion defect [8, 9]. Quantitative analysis of TPD was performed on redistribution image using a commercially available software package [quantitative gated SPECT (QGS), Cedars-Sinai Medical Center, Los Angeles, CA]. TPD was calculated as the percentage of the total surface area of the left ventricle below the pre-defined uniform average deviation threshold. In this study, TPD was defined as the reference standard method for estimating MI size. End-diastolic volume (EDV), end-systolic volume (ESV), and ejection fraction (EF) were also obtained.
Statistical analysis
Continuous variables are shown as mean ± SD, and categorical variables are presented as frequencies and percentages. Continuous variables were compared by the Kruskal–Wallis test. Categorical variables were compared by the Chi-square test. Correlations between QRS score and QGS measurements were assessed by Pearson’s correlation test. Agreements between the two methods were assessed by the Bland–Altman plot showing the difference and the limits of agreement. Multiple linear regression analysis was performed to determine which variables were significantly associated with TPD. Differences were considered significant if the p value was <0.05. Statistical analysis was conducted using the JMP 11 software (SAS Institute, Tokyo, Japan).
Results
Patient characteristics
Patient characteristics are shown in Table 2. There was no significant difference in body mass index between patients with prior anterior MI and control subjects. Compared with control subjects, patients with prior anterior MI had higher TPD (20.8 ± 14.5 vs 2.0 ± 1.9 %, p < 0.001), larger EDV (100.0 ± 61.5 vs 59.7 ± 17.4 ml, p < 0.001), larger ESV (61.7 ± 55.4 vs 22.3 ± 10.1 ml, p < 0.001), and lower EF (44.3 ± 14.0 vs 63.8 ± 10.3 %, p < 0.001) (Fig. 1). QRS score was significantly higher in patients with prior anterior MI than control subjects (12.8 ± 8.9 vs 1.1 ± 2.7 %, p < 0.001) (Fig. 2).

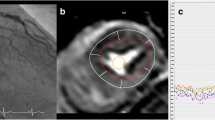
QGS measurements in a patient with prior anterior myocardial infarction (left panel) and a control subject (right panel)

Comparison of QRS score between patients with prior anterior myocardial infarction and control subjects. Data are shown as mean (SE)
QRS score and QGS variables
In overall patients (n = 132), QRS score was correlated well with TPD (r = 0.81, p < 0.001) (Fig. 3). This good correlation was found even in patients with TPD ≤40 % (n = 126) or in patients with TPD ≤30 % (n = 117).

Correlations between QRS score and total perfusion deficit (TPD) in overall patients, in patients with TPD ≤40 % and in patients with TPD ≤30 %
In overall patients, MI size estimated by QRS score was 7.0 ± 8.8 %, which was significantly smaller than TPD, 11.4 ± 14.0 % (p < 0.001). The difference between QRS score and TPD was −4.5 %. Bland–Altman plot showed that there was an increasing difference between QRS score and TPD with increasing MI size (Fig. 4). When Blant–Altman plots were applied to patients with TPD ≤40 % and further in patients with TPD ≤30 %, the difference between QRS score and TPD became smaller, and the agreement became better.

Agreements between QRS score and total perfusion deficit (TPD) in overall patients, in patients with TPD ≤40 % and in patients with TPD ≤30 %
In overall patients, QRS score was correlated well with QGS measurements, such as EDV (r = 0.62, p < 0.001), ESV (r = 0.67, p < 0.001), or EF (r = −0.73, p < 0.001) (Fig. 5). Multiple linear regression analysis showed that only QRS score was significantly associated with TPD (Table 3).

Correlations between QRS score and quantitative gated single-photon emission computed tomography (QGS) measurements, such as end-diastolic volume (EDV), end-systolic volume (ESV), or ejection fraction (EF)
Discussion
In this study, we demonstrated the following: (1) QRS score was correlated well with TPD as the reference standard for estimating MI size in patients with prior anterior MI undergoing coronary intervention, (2) the agreement was acceptable in patients with TPD less than approximately 30 %, and (3) QRS score also reflected surrogate measurements of MI size, such as EDV, ESV, or EF assessed by QGS.
Recent studies have assessed the correlation between QRS score and delayed enhancement magnetic resonance imaging (DE-MRI) which allows for direct measurement of MI size. They have shown that QRS score is correlated with % MI by DE-MRI with correlation coefficients ranging from 0.39 to 0.57 in the acute phase and 0.43–0.74 in the chronic phase [6, 17, 18]. It is well known that the QRS scoring system permits acceptable levels of both intra- and inter-observer agreement, and QRS score can be reproducibly performed [3]. Therefore, the variations in the correlation coefficients between QRS score and DE-MRI might be caused by the lack of consensus on post-processing of DE-MRI resulting in different standards of measurement of MI size [19, 20]. TPD is a reliable parameter automatically quantified using QGS, and we used TPD as the reference standard for estimating MI size. In this study, we first compared QRS score with TPD, and demonstrated that QRS score was correlated well with TPD with high correlation coefficient of 0.81. Our results strongly suggested the accuracy of QRS scoring system for estimating MI size even in the coronary intervention era. We also assessed the agreement between QRS score and TPD, and demonstrated that QRS score increasingly underestimated MI size with increasing MI size. Our results may be supported by some studies using DE-MRI [5]. Engblom et al. showed that, in patients with prior anterior MI, QRS score reflected MI size well in the middle segments, whereas increasingly underestimated MI size in the apical segments with increasing MI size [5]. According to our results and the previous studies, QRS score appears to underestimate MI size at least in patients with large MI which involves apical segments. This would be a limitation of QRS scoring system which estimates MI size electrocardiographically. However, it is noteworthy that both correlation and agreement are acceptable in patients with TPD less than approximately 30 %, indicating that QRS score can be clinically applied to patients with non-large anterior MI. The ECG is easily accessible to the clinicians, and QRS scoring system is helpful in estimating MI size or EF during the follow-up period in the coronary intervention era.
There were several limitations in this study. First, we included only patients with prior anterior MI, and did not assess the accuracy of QRS score in patients with prior non-anterior MI. Second, most of our patients underwent coronary intervention during the study period, and we have few clinical data of patients not undergoing coronary intervention. We could not examine the accuracy of QRS score in these patients. Finally, the small sample size was a major limitation of this study.
In conclusion, our results suggest that QRS score reflects TPD well in patients with prior anterior MI, whose TPD is less than approximately 30 % even in the coronary intervention era.
References
Nishizaki F, Tomita H, Yokoyama H, Higuma T, Abe N, Suzuki A, Endo T, Tateyama S, Ishida Y, Osanai T, Okumura K (2013) Re-elevation of T-wave from day 2 to day 4 after successful percutaneous coronary intervention predicts chronic cardiac systolic dysfunction in patients with first anterior acute myocardial infarction. Heart Vessel 28:704–713
Palmeri ST, Harrison DG, Cobb FR, Morris KG, Harrell FE, Ideker RE, Selvester RH, Wagner GS (1982) QRS scoring system for assessing left ventricular function after myocardial infarction. N Engl J Med 306:4–9
Wagner GS, Freye CJ, Palmeri ST, Roark SF, Stack NC, Ideker RE, Harrell FE Jr, Selvester RH (1982) Evaluation of a QRS scoring system for estimating myocardial infarct size. I. Specificity and observer agreement. Circulation 65:342–347
Selvester RH, Wagner GS, Hindman NB (1985) The Selvester QRS scoring system for estimating myocardial infarct size. The development and application of the system. Arch Intern Med 145:1877–1881
Engblom H, Wagner GS, Setser RM, Selvester RH, Billgren T, Kasper JM, Maynard C, Pahlm O, Arheden H, White RD (2003) Quantitative clinical assessment of chronic anterior myocardial infarction with delayed enhancement magnetic resonance imaging and QRS scoring. Am Heart J 146:359–366
Geerse DA, Wu KC, Gorgels AP, Zimmet J, Wagner GS, Miller JM (2009) Comparison between contrast-enhanced magnetic resonance imaging and Selvester QRS scoring system in estimating changes in infarct size between the acute and chronic phases of myocardial infarction. Ann Noninvasive Electrocardiol 14:360–365
Ko T, Utanohara Y, Suzuki Y, Kurihara M, Iguchi N, Umemura J, Sumiyoshi T, Tomoike H (2016) A preliminary feasibility study of simultaneous dual-isotope imaging with a solid-state dedicated cardiac camera for evaluating myocardial perfusion and fatty acid metabolism. Heart Vessel 31:38–45
Slomka PJ, Fieno D, Thomson L, Friedman JD, Hayes SW, Germano G, Berman DS (2005) Automatic detection and size quantification of infarcts by myocardial perfusion SPECT: clinical validation by delayed-enhancement MRI. J Nucl Med 46:728–735
Berman DS, Kang X, Gransar H, Gerlach J, Friedman JD, Hayes SW, Thomson LE, Hachamovitch R, Shaw LJ, Slomka PJ, Yang LD, Germano G (2009) Quantitative assessment of myocardial perfusion abnormality on SPECT myocardial perfusion imaging is more reproducible than expert visual analysis. J Nucl Cardiol 16:45–53
Shiraishi J, Kohno Y, Sawada T, Hashimoto S, Ito D, Kimura M, Matsui A, Yokoi H, Arihara M, Irie H, Hyogo M, Shima T, Nakamura T, Matoba S, Yamada H, Matsumuro A, Shirayama T, Kitamura M, Furukawa K, Matsubara H (2013) Prognostic impact of pulse pressure at admission on in-hospital outcome after primary percutaneous coronary intervention for acute myocardial infarction. Heart Vessel 28:434–441
Abe D, Sato A, Hoshi T, Takeyasu N, Misaki M, Hayashi M, Aonuma K (2014) Initial culprit-only versus initial multivessel percutaneous coronary intervention in patients with ST-segment elevation myocardial infarction: results from the Ibaraki Cardiovascular Assessment Study registry. Heart Vessel 29:171–177
Zencirci E, Zencirci AE, Değirmencioğlu A, Karakuş G, Uğurlucan M, Özden K, Erdem A, Güllü AÜ, Ekmekçi A, Velibey Y, Erer HB, Çelik S, Akyol A (2015) The relationship between epicardial adipose tissue and ST-segment resolution in patients with acute ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention. Heart Vessel 30:147–153
Abdelmoneim SS, Martinez MW, Mankad SV, Bernier M, Dhoble A, Pellikka PA, Chandrasekaran K, Oh JK, Mulvagh SL (2015) Resting qualitative and quantitative myocardial contrast echocardiography to predict cardiac events in patients with acute myocardial infarction and percutaneous revascularization. Heart Vessel 30:45–55
Verdoia M, Barbieri L, Schaffer A, Cassetti E, Marino P, Bellomo G, Sinigaglia F, De Luca G, Novara Atherosclerosis Study Group (NAS) (2015) Platelet-larger cell ratio and the risk of periprocedural myocardial infarction after percutaneous coronary revascularization. Heart Vessel 30:20–27
Kurisu S, Iwasaki T, Ikenaga H, Watanabe N, Higaki T, Shimonaga T, Ishibashi K, Mitsuba N, Dohi Y, Kihara Y (2014) Influence of left ventricular geometry on thallium-201 gated single-photon emission tomographic findings in patients with known or suspected coronary artery disease. Ann Nucl Med 28:120–127
Kurisu S, Iwasaki T, Abe N, Tamura M, Ikenaga H, Watanabe N, Higaki T, Shimonaga T, Ishibashi K, Dohi Y, Fukuda Y, Kihara Y (2015) Effects of myocardial perfusion abnormalities on the accuracy of left ventricular volume and ejection fraction measured by thallium-201 gated single-photon emission tomography: comparison with echocardiography as the reference standard. Nucl Med Commun 36:1127–1133
Bang LE, Ripa RS, Grande P, Kastrup J, Clemmensen PM, Wagner GS (2008) Comparison of infarct size changes with delayed contrast-enhanced magnetic resonance imaging and electrocardiogram QRS scoring during the 6 months after acutely reperfused myocardial infarction. J Electrocardiol 41:609–613
Rovers WC, van Boreen MC, Robinson M, Martin TN, Maynard C, Wagner GS, Gorgels AP (2009) Comparison of the correlation of the Selvester QRS scoring system with cardiac contrast-enhanced magnetic resonance imaging-measured acute myocardial infarct size in patients with and without thrombolytic therapy. J Electrocardiol 42:139–144
Engblom H, Arheden H, Foster JE, Martin TN (2007) Myocardial infarct quantification: is magnetic resonance imaging ready to serve as a gold standard for electrocardiography? J Electrocardiol 40:243–245
Carlsen EA, Bang LE, Ahtarovski KA, Engstrøm T, Køber L, Kelbaek H, Vejlstrup N, Jørgensen E, Helqvist S, Saunamäki K, Clemmensen P, Holmvang L, Wagner GS, Lønborg J (2012) Comparison of Selvester QRS score with magnetic resonance imaging measured infarct size in patients with ST elevation myocardial infarction. J Electrocardiol 45:414–419
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Kurisu, S., Shimonaga, T., Ikenaga, H. et al. Selvester QRS score and total perfusion deficit calculated by quantitative gated single-photon emission computed tomography in patients with prior anterior myocardial infarction in the coronary intervention era. Heart Vessels 32, 369–375 (2017). https://doi.org/10.1007/s00380-016-0884-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00380-016-0884-0