
Abstract
Background
Recent studies have shown good correlations between echocardiography and Tl-201 gated single-photon emission computed tomography (SPECT) for the assessment of left ventricular volumes and ejection fraction. We assessed how left ventricular geometry affected correlations between these values measured by the 2 methods in patients with known or suspected coronary artery disease.
Methods and results
There were 109 patients with normal left ventricular geometry, 20 patients with concentric remodeling, 32 patients with eccentric hypertrophy and 28 patients with concentric hypertrophy. In all 4 groups, there were good correlations between end-diastolic volume (EDV) and end-systolic volume (ESV) values measured by echocardiography and quantitative gated SPECT (QGS). EDV and ESV values measured by QGS were significantly underestimated than those measured by echocardiography except for ESV in eccentric hypertrophy. In all 4 groups, ejection fraction (EF) value measured by echocardiography significantly correlated with that measured by QGS, but Bland–Altman plot showed a proportional error. EF value measured by QGS was likely to be overestimated when EF value increased from the median value, and to be underestimated when EF value decreased from the median value especially in concentric remodeling.
Conclusions
Tl-201 gated SPECT is a useful tool for the assessment of left ventricular volumes and function, but it requires methodological considerations according to left ventricular geometry.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Echocardiography or gated single-photon emission computed tomography (SPECT) have been widely used for assessing left ventricular volumes and ejection fraction [1–3]. Compared with technetium-99m (Tc-99m)-labeled agents, thallium-201 (Tl-201) is considered to possess poor image quality due to its lower photon energy and flux [4, 5]. However, its better physiological properties and the recent development of myocardial collimeters have resulted in a interest in the use of Tl-201 for gated SPECT. Although several studies have recently shown good correlations between echocardiography and Tl-201 gated SPECT for the assessment of left ventricular volumes and ejection fraction [6–9], it remains unclear whether good correlations are found even in abnormal left ventricular geometry such as concentric remodeling, eccentric hypertrophy or concentric hypertrophy.
In the current study, we assessed how left ventricular geometry affected correlations between these values measured by echocardiography and Tl-201 gated SPECT in patients with known or suspected coronary artery disease.
Methods
Patients
This study included 189 patients who underwent both transthoracic echocardiography and Tl-201 gated SPECT within 2 weeks for evaluating coronary artery disease. Patients undergoing hemodialysis were included, and transthoracic echocardiography and Tl-201 gated SPECT were performed the next day after hemodialysis. Patients with atrial fibrillation or large myocardial damage assessed by Tl-201 gated SPECT were excluded in this study.
Echocardiography and left ventricular geometry
Comprehensive echocardiographic assessment was conducted by three experienced sonographers, who had no knowledge of the clinical data, using high-quality commercially available ultrasound systems with 3.5 MHz probes (GE Healthcare Vivid 7, Milwaukee, WI, USA; TOSHIBA Medical Artida, Tokyo). Echocardiographic studies were performed in the morning after 30 min rest with the subject in a supine left lateral decubitus position. Interventricular septal thickness (IVS), posterior wall thickness (PWT) and left ventricular internal dimension (LVID) were measured at end-diastole according to established standards of the American Society of Echocardiography (ASE). Left ventricular end-diastolic volume (EDV), end-systolic volume (ESV) and ejection fraction (EF) values were obtained using a modified biplane Simpson’s method from the apical 2- and 4-chamber views [10, 11]. These echocardiographic measurements were considered as the reference standard method. Left ventricular mass (LVM) was calculated according to the ASE-recommended formula [12]:
LVM was divided to body surface area to obtain the LVM index. LVH was diagnosed as LVM index > 115 g/m2 in men and 95 g/m2 in women. Relative wall thickness (RWT) was calculated as using the formula:
Patients were divided into 4 groups according to their left ventricular geometry (Figure 1) [13]: (1) normal, no LVH and RWT < 0.42; (2) concentric remodeling, no LVH and RWT > 0.42; (3) eccentric hypertrophy, LVH and RWT < 0.42; and (4) concentric hypertrophy, LVH and RWT > 0.42.

Geometric patterns based on left ventricular hypertrophy and relative wall thickness
Tl-201 gated SPECT
All patients fasted overnight, and underwent stress-rest Tl-201 gated SPECT. Adenosine was infused over 6 min (120 μg/kgmin), and Tl-201 (111 MBq) was injected 3 min after the initiation of adenosine infusion. The stress Tl-201 SPECT acquisition was started 5 min after the stress test. Four hours later, rest Tl-201 SPECT images were also obtained. Gated SPECT images were acquired with a dual-head gamma camera system (Siemens E-CAM, Siemens Medical Solutions). Gating was performed with 8 frames per cardiac cycle, using a 60 % beat acceptance window. Tl-201 SPECT images were acquired with a 10 % symmetric window over the 80-keV Tl photopeak. The raw projection datasets were filtered with a Butterworth filter. No scatter or attenuation correction was applied.
Quantitative analysis of EDV, ESV or EF was performed on 4 h rest Tl-201 SPECT using a commercially available software package (quantitative gated SPECT, QGS, Cedars-Sinai Medical Center, Los Angeles, CA) [14]. Semiquantitative visual interpretation of Tl-201 SPECT images was performed with the short and vertical long axes divided into 17 segments. Each segment was graded using a 5-point scoring system (0 normal uptake, 1 mildly reduced uptake, 2 moderately reduced uptake, 3 severely reduced uptake, 4 absence of detectable radiotracer in a segment) in a blinded manner by the 2 experienced cardiologists (S.K. and T.I.). Patients with large myocardial damage defined as sum of rest score > 8 were excluded in this study because it might affect QGS parameters.
Statistical analysis
All data are expressed as mean ± SD. Analysis of variance was performed to test for differences of values among the 4 groups. Student’s paired t test was used to evaluate the difference in values between echocardiographic and QGS methods in each group. Pearson’s correlation coefficient and regression analysis were used to evaluate the correlation between the 2 methods. Bland–Altman plot was applied to assess the agreement between the 2 methods. The regression of the mean and the difference between values assessed by echocardiography and QGS were analyzed. Differences were considered significant if the p value was <0.05.
Results
Patient characteristics
Patient characteristics are summarized in Table 1. There were 109 patients with normal left ventricular geometry, 20 patients with concentric remodeling, 32 patients with eccentric hypertrophy and 28 patients with concentric hypertrophy. There was no significant difference in age, body mass index, hypertension, diabetes, prior myocardial infarction or prior coronary intervention among the 4 groups except for male gender. No patient needed manual adjustment of extraction of left ventricular contour because of improper auto-tracing by QGS.
Echocardiographic and QGS parameters
Echocardiographic and QGS parameters are summarized in Table 2. There was a significant difference in EDV, ESV or EF value measured by echocardiography or QGS among the 4 groups.
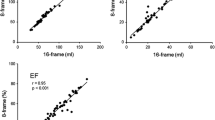
In all 4 groups, there were good correlations between EDV and ESV values measured by echocardiography and QGS (Figs. 2, 3). EDV and ESV values measured by QGS were significantly underestimated than those measured by echocardiography except for ESV value in eccentric hypertrophy. EDV value measured by QGS was underestimated by 30.1 % in normal left ventricular geometry, by 26.3 % in concentric remodeling, by 17.2 % in eccentric hypertrophy and by 21.0 % in concentric hypertrophy.

Correlation between left ventricular end-diastolic volume values measured by echocardiography and quantitative gated SPECT

Correlation between left ventricular end-systolic volume values measured by echocardiography and quantitative gated SPECT
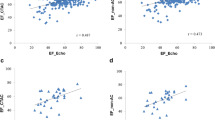
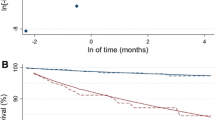
In all 4 groups, EF value measured by echocardiography significantly correlated with that measured by QGS (Fig. 4). Most excellent correlation was found in eccentric hypertrophy (r = 0.80, p < 0.001). More revealing were Bland–Altman plots, which showed significant negative slopes of −0.93, −1.34, −0.51 and −0.88 in normal LV geometry, concentric remodeling, eccentric hypertrophy and concentric hypertrophy, respectively. In all 4 groups, the difference between EF values measured by echocardiography and QGS was smallest in the median value, and increased when EF value increased or decreased from the median value (Fig. 5). This affect was manifest in concentric remodeling.

Correlation between left ventricular ejection fraction values measured by echocardiography and quantitative gated SPECT

Bland–Altman plot showing comparison between left ventricular ejection fraction values measured by echocardiography and quantitative gated SPECT
Discussion
Gated SPECT is a unique clinical tool in that it allows assessment of left ventricular perfusion, volumes and function simultaneously. In this study, EDV, ESV or EF value was obtained from 4 h rest Tl-201 SPECT because it had an advantage that potential stunning of the myocardium had already disappeared in most patients.
Wright et al. [15] previously reported that EF value assessed by Tl-201 gated SPECT was unsatisfactory for use in clinical practice with lower doses of Tl-201 (62 ± 7 MBq) as compared to the dose administered in our study. On the other hand, Cwajg et al. [7] reported that gated SPECT using Tl-201 has a good correlation with echocardiography for the assessment of left ventricular volumes and function with the similar dose administered in our study (111 MBq). The development of myocardial collimeters have also support the clinical use of Tl-201 gated SPECT, and recent studies concluded that gated Tl-201 SPECT was a reliable clinical tool for the assessment of left ventricular volumes and function with good correlation when compared with echocardiography [7–9].
The current study demonstrated that there was a good correlation in EDV or ESV value in all left ventricular geometries, but EDV or ESV value by QGS was underestimated than that by echocardiography. Previous studies have pointed out that there appears to be a difference between EDV or ESV value measured by the 2 methods [7, 16], and our results were consistent with those of previous reports. The current study also demonstrated that underestimate by QGS was larger in normal left ventricular geometry or concentric remodeling compared to eccentric hypertrophy or concentric hypertrophy. The difference in underestimate by QGS according to left ventricular geometry can be explained by the following causes. There is a known scatter of photons from myocardial walls to the left ventricular cavity [17]. Small left ventricular cavity may likely intensify the scatter problem, creating difficulties for the automatic QGS to define the endocardial surface properly. In the current study, smaller left ventricular cavity in normal left ventricular geometry or concentric remodeling possibly resulted in larger underestimate by QGS compared to eccentric hypertrophy or concentric hypertrophy.
Previous studies demonstrated a good correlation between EF values measured by echocardiography and QGS. However, almost studies have only used Pearson’s correlation coefficient for comparing the 2 methods [7]. In the current study, we also found a good correlation, but Bland–Altman plot showed a proportional error in all left ventricular geometries. EF value measured by QGS was likely to be overestimated when EF value increased from the median value, and to be underestimated when EF value decreased from the median value especially in concentric remodeling. ESV value in concentric remodeling was too small in some cases to such an extent that the scatter may even lead to complete disappearance of left ventricular cavity in end systole. This was particularly true when ESV value was measured by QGS, with a range starting from only 3 ml. These methodological characteristics were associated with a high proportional error in concentric remodeling. Thus, Tl-201 gated SPECT appears to require methodological considerations according to left ventricular geometry.
There were several limitations in this study. First, this study included only patients with stable condition, and excluded patients with atrial fibrillation or large myocardial damage. Second, EF value was acquired using 8-frame gating. 16-frame to 24-frame gating can provide more accurate estimates, but its use with Tl-201 was not feasible due to a poor statistic count. Third, cardiac magnetic resonance is increasingly utilized for dynamic imaging with the expectation which will provide more accurate measurements of left ventricular volumes and function compared to echocardiography and QGS. However, it is expensive and of limited availability. Finally, the small sample size especially in abnormal left ventricular geometry was a limitation of this study.
In conclusion, Tl-201 gated SPECT is a useful tool for the assessment of left ventricular volumes and function, but it requires methodological considerations according to left ventricular geometry.
References
Yang KT, Chen HD. Evaluation of global and regional left ventricular function using technetium-99m sestamibi ECG-gated single-photon emission tomography. Eur J Nucl Med. 1998;25:515–21.
Yoshioka J, Hasegawa S, Yamaguchi H, Tokita N, Paul AK, Xiuli M, et al. Left ventricular volumes and ejection fraction calculated from quantitative electrocardiographic-gated 99mTc-tetrofosmin myocardial SPECT. J Nucl Med. 1999;40:1693–8.
Rozanski A, Nichols K, Yao SS, Malholtra S, Cohen R, DePuey EG. Development and application of normal limits for left ventricular ejection fraction and volume measurements from 99mTc-sestamibi myocardial perfusion gates SPECT. J Nucl Med. 2000;41:1445–50.
DePuey EG, Parmett S, Ghesani M, Rozanski A, Nichols K, Salensky H. Comparison of Tc-99m sestamibi and Tl-201 gated perfusion SPECT. J Nucl Cardiol. 1999;6:278–85.
Hyun IY, Kwan J, Park KS, Lee WH. Reproducibility of Tl-201 and Tc-99m sestamibi gated myocardial perfusion SPECT measurement of myocardial function. J Nucl Cardiol. 2001;8:182–7.
Bacher-Stier C, Müller S, Pachinger O, Strolz S, Erler H, Moncayo R, et al. Thallium-201 gated single-photon emission tomography for the assessment of left ventricular ejection fraction and regional wall motion abnormalities in comparison with two-dimensional echocardiography. Eur J Nucl Med. 1999;26:1533–40.
Cwajg E, Cwajg J, He ZX, Hwang WS, Keng F, Nagueh SF, et al. Gated myocardial perfusion tomography for the assessment of left ventricular function and volumes: comparison with echocardiography. J Nucl Med. 1999;40:1857–65.
Patel CD, Nadig MR, Kurien S, Barai S, Narang R, Malhotra A. Left ventricular ejection fraction and volumes on rest gated 201Tl perfusion SPECT: comparison with two-dimensional echocardiography. Nucl Med Commun. 2006;27:425–9.
Harpaz D, Asman A, Kuperstein R, Boaz M, Chouraqui P. Left ventricular ejection fraction assessment by Tl-201 gated SPECT: a comparison with echocardiography. Clin Cardiol. 2010;33:E56–62.
Schiller NB, Shah PM, Crawford M, DeMaria A, Devereux R, Feigenbaum H, et al. Recommendations for quantitation of the left ventricle by two-dimensional echocardiography. American Society of Echocardiography Committee on Standards, Subcommittee on Quantitation of Two-Dimensional Echocardiograms. J Am Soc Echocardiogr. 1989;2:358–67.
Otterstad JE, Froeland G, John Sutton M, Holme I. Accuracy and reproducibility of biplane two-dimensional echocardiographic measurements of left ventricular dimensions and function. Eur Heart J. 1997;18:507–13.
Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, Chamber Quantification Writing Group, American Society of Echocardiography’s Guidelines and Standards Committee, European Association of Echocardiography, et al. Recommendations for chamber quantification: a report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005;18:1440–63.
Takasaki K, Miyata M, Imamura M, Yuasa T, Kuwahara E, Kubota K, et al. Left ventricular dysfunction assessed by cardiac time interval analysis among different geometric patterns in untreated hypertension. Circ J. 2012;76:1409–14.
Germano G, Kiat H, Kavanagh PB, Moriel M, Mazzanti M, Su HT, et al. Automatic quantification of ejection fraction from gated myocardial perfusion SPECT. J Nucl Med. 1995;36:2138–47.
Wright GA, McDade M, Keeble W, Martin W, Hutton I. Quantitative gated SPECT myocardial perfusion imaging with 201Tl: an assessment of the limitations. Nucl Med Commun. 2000;21:1147–51.
El-Maghraby TA, El-Rahman NA. Clinical relevance of left ventricular volumes and function assessed by gated SPECT in paediatric patients. Int J Cardiovasc Imaging. 2004;20:127–34.
Germano G, Berman DS. On the accuracy and reproducibility of quantitative gated myocardial perfusion SPECT. J Nucl Med. 1999;40:810–3.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kurisu, S., Iwasaki, T., Ikenaga, H. et al. Influence of left ventricular geometry on thallium-201 gated single-photon emission tomographic findings in patients with known or suspected coronary artery disease. Ann Nucl Med 28, 120–127 (2014). https://doi.org/10.1007/s12149-013-0786-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12149-013-0786-5