
Abstract
Purpose
Estimate myocardial salvage index (MSI) using a single-gated Single-Photon Emission Computed Tomography (SPECT) myocardial perfusion imaging (GSMPI) early after percutaneous coronary intervention (PCI) in patients with acute myocardial infarction (AMI) and compare its predictive value with the traditional method especially for post-PCI left ventricular ejection fraction (LVEF) improvement and major adverse cardiac events (MACEs).
Methods
GSMPI was performed in 62 patients with AMI early after PCI (3–10 days). The MSI and the conventional parameters were obtained, including total perfusion deficit, LVEF, peak ejection rate (PER), and peak filling rate (PFR). The new calculation method (scoring evaluation method means the extent of abnormality is the percentage of the total scores of abnormal segments divided by the sum of the maximum scores of all myocardial segments using 4-point and 5-point scale semi-quantitative scoring method) and the reference method (number evaluation method means the extent of abnormality is the percentage of the number of abnormal segments divided by the total number of myocardial segments) were applied to acquire the MSI. We compared the predictive ability of the 2 methods based on the area under the receiver operating characteristic curve for LVEF improvement 6 months after PCI using MSI. The Kaplan–Meier method was used for depicting survival curves for predicting MACEs by the 2 methods. Cox proportional-hazards regression was applied to confirm the independent predictors of MACEs.
Results
The MSI obtained by the new method indicated stronger prognostic significance in LVEF improvement [area under the curve (AUC): 0.793, 95% confidence interval (CI) 0.620–0.912, P < .001] compared with the reference method (AUC: 0.634, 95%CI 0.452–0.792, P = .187). Delong’s test revealed a statistically significant difference in AUCs between the 2 methods (P < .05, 95%CI 0.003–0.316). The diagnostic value of the scoring evaluation method was higher than that of the number evaluation method. The Cox prevalence of MACEs was substantially higher in the < median MSI group than in the ≥ median MSI group (hazard ratio: 0.172; 95% CI 0.041–0.724; P < .05] using the new method, whereas no considerable differences were observed between the 2 groups using the reference method (P = .12). Further, the multivariate Cox regression analysis revealed that MSI was an independent indicator for predicting MACEs (P < .05).
Conclusion
The MSI obtained from a simple GSMPI early after PCI, using the scoring evaluation method, was a reliable prognostic indicator for predicting LVEF improvement and MACEs in AMI. It remarkably improved the prognostic value compared with the previous reference methods.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Acute myocardial infarction (AMI) remains one of the leading causes of death and disability [1]. Successful percutaneous coronary intervention (PCI) aims to achieve myocardial salvage (MS) and improve the prognosis [2]. Patients with a smaller MS may receive more intensive drug therapy and a more suitable follow-up plan and rehabilitation training.
MS acquired by comparing the final infarct size (FIS) with the myocardial area at risk (AAR) using 2 single-gated Single-Photon Emission Computed Tomography (SPECT) myocardial perfusion imaging (GSMPI) images has demonstrated prognostic significance [3,4,5]. Several studies have confirmed myocardial salvage index (MSI), which is the ratio of the degree of MS to AAR and is an independent predictor of the benefit from reperfusion treatment in patients with AMI [3,4,5,6,7]. Research indicated that the MSI could replace “mortality” for prognostic evaluation, suggesting the feasibility of MSI as an endpoint indicator. However, tracer injection is required before PCI to obtain AAR, thus limiting its widespread application. A lack of adequate conditions for night emergency examination in most departments, and the long distance from the nuclear medicine department are both concerns; also, the image might not be actualized on time because of patient safety concerns [8]. These factors render it difficult to inject the tracer before PCI and thus acquire AAR. Although AAR can also be detected after PCI with dual-nuclide myocardial SPECT using the fatty acid tracer 123I-β-methyl-p-iodophenyl-pentadecanoic acid (BMIPP) and blood flow tracer [9, 10], the unavailability of BMIPP in most countries has limited the feasibility [14]. Even if AAR can be obtained by 123I-BMIPP, FIS still needs to be acquired by the second myocardial perfusion imaging; that is, it needs two injections and two GSMPIs to obtain MSI. Therefore, a simple and feasible method is necessary to estimate AAR and the corresponding MSI reliably.
Recently, a single GSMPI taken early after PCI was employed to acquire AAR and FIS [11,12,13] as an alternative. Because of the persistent myocardial stunning, they estimated the MSI by comparing the extent of regional functional abnormalities (which approximated the AAR) with perfusion defects that signify FIS. The MSI obtained by this method demonstrated strong agreement with the SPECT reference method taken before and after PCI (Spearman’s q: 5.92, P < 0.0001), with a 95% limit of agreement 5 ± 0.25. The agreement between the classifications in salvage index tertiles obtained by the 2 methods was remarkable (kappa 5.75) [14,15,16,17].
Nevertheless, the calculation method had certain shortcomings. In the studies in which the MSI was obtained using a single GSMPI, the extent of regional abnormalities (whether perfusion or function) was defined as the percentage of the number of abnormal segments divided by the total number of myocardial segments, without considering the degree of abnormality. This led to reduced accuracy compared with the results obtained by combining the number and degree of the abnormalities.
The present study aimed to employ a single GSMPI taken early after PCI to obtain an MSI in patients with AMI. In particular, we aimed to determine the extent of regional abnormalities based on the percentage of the total scores of abnormal segments divided by the maximal score of all myocardial segments using a 17-segment model of the left ventricle (LV) and a 4-point scale (the wall-thickening scores) and 5-point scale (the myocardial perfusion scores). By combining quantity with degree, we seek to further improve the accuracy of the results.
Methods
Study population
This retrospective study included 62 patients with primary AMI referred to our hospital for primary PCI within 6 h of symptom onset between October 2020 and August 2021. AMI was defined as a recent ischemia lasting more than 20 min at rest, with one of the following electrocardiographic features: (1) ST-segment elevation (0.1 mV or higher) in 2 or more contiguous leads, or (2) new or alleged new left bundle branch block [18].
The coronary arteriography (CAG) results of all patients were confirmed as single coronary artery occlusion to avoid potential influences from non-infarct-related vessels on the results. The degree of the remaining coronary artery stenosis was ≤ 50%. Successful PCI was defined as [19,20,21] (1) thrombolysis in myocardial infarction (TIMI) grade of infarct-related vessels of grade 3, and (2) residual stenosis of less than 20%. The study exclusion criteria were as follows: (1) previous myocardial infarction, post-revascularization, severe congestive heart failure, cardiomyopathy, valvular heart disease and severe cardiac hypertrophy, cardiogenic shock, or another serious systemic disease; (2) persistent atrial fibrillation; (3) known or suspected pregnancy; and (4) poor image quality affecting the diagnosis. The research method was approved by the hospital institutional review board. The study was approved by the local ethics committee, and all patients provided written informed consent.
Acquisition of baseline characteristics
We recorded the height and weight of each patient and calculated the body mass index (BMI). Patients’ histories of hypertension, diabetes, and smoking were also reviewed. In addition, the time from onset to balloon dilatation was recorded. The serum levels of myocardial injury markers, including cardiac troponin T(cTnT), creatine kinase (CK), and creatine kinase MB (CK-MB), were measured within 12–24 h after admission. The infarct-related blood vessel according to CAG was recorded.
GSMPI imaging
A dual-probe Symbian T6 SPECT scanner (Siemens, Munich, Germany) was used, and the Cedars Cardiac Suite [Quantitative Gated SPECT(QPS)/Quantitative Gated SPECT(QGS)] software (Cedars-Sinai,CA,USA) was used for image post-processing.99mTc-MIBI, a radionuclide imaging agent used for GSMPI, was eluted, labeled, and dispatched by Beijing Senke, Ltd. (Beijing, China).
All patients underwent a post-PCI resting GSMPI 3–10 days (at a median time of 6 days) after PCI. They were injected at rest with 740–925 MBq of 99mTc-MIBI. The images were acquired 60 min after injection, using a double-headed camera equipped with high-resolution collimators (Siemens, Munich, Germany) and with a 15% window centered on the 140-keV photopeak of technetium-99 m. GSMPI was performed in the step-and-shoot mode, with 32 projections over a 180° elliptical orbit, matrix size 128 × 128, 25 s/projection, and 8-frames/cardiac cycle.
Two experienced nuclear medicine doctors used the Cedars Cardiac Suite to process the data blindly. The myocardial perfusion images of the left ventricle short axis, horizontal long axis, and vertical long axis were reconstructed using filtered back-projection with computed tomography attenuation correction. The bull’s eye images were obtained from the projection of the LV short axis. For perfusion and functional analyses, the left ventricular polar map was divided into 17 segments according to the American Heart Association standards. The myocardial perfusion parameters [summed rest score (SRS) and total perfusion deficit (TPD)] were obtained using the QPS software, and the cardiac function parameters [LVEF, peak ejection rate (PER), and peak filling rate (PFR)] were obtained using the QGS software automatically without any user intervention.
The ventricular wall-thickening score was used to reflect the ventricular systolic function more accurately [22,23,24]. The wall-thickening images were scored using a 4-point scale (0 = normal, 1 = slightly damaged, 2 = moderately damaged, and 3 = severely damaged). The myocardial perfusion images were scored using a 5-point scale semi-quantitatively (0 = normal, 1 = slight decrease, 2 = moderate decrease, 3 = severe decrease, and 4 = defect). The perfusion scoring scheme included a higher number of degrees than wall thickening. Hence, abnormal segments with borderline perfusion were not considered (score = 1), which was consistent with previous studies [13,14,15]. To avoid the impact on the results caused by inconsistencies in the two calculation methods, we used a 4-point scale /5-point scale semi-quantitative score, and only summed the scores of 2, 3, and 4 to calculate the extent of perfusion in both the number and the scoring evaluation method to make them more comparable. The stunned myocardium is associated with a perfusion–function mismatch early after PCI. Therefore, we defined MS as the difference between the extent of functional (i.e., the AAR) and perfusion abnormalities (i.e., the FIS) early after AMI. The MSI was the percentage of MS divided by the AAR.
Number evaluation method, based on previous references [14,15,16]:
The extent of any abnormality (perfusion or wall thickening) = the number of abnormal segments/17 × 100%.
Scoring evaluation method: The semi-quantitative scoring method was used to calculate the extent of any abnormality. This extent was defined as the percentage of the total scores of abnormal segments divided by the sum of the maximum scores of all myocardial segments using a 4-point scale (the wall-thickening scores) and 5-point scale (the myocardial perfusion scores):
Extent of abnormal wall thickening = [total scores of abnormal segments of ventricular wall thickening)/(17 × 3)] × 100%.
Extent of abnormal perfusion = [total scores of segments with abnormal perfusion/(17 × 4)] × 100% [25].
Then, the statistical differences between the aforementioned 2 methods were compared.
Cardiac ultrasound
All patients underwent cardiac ultrasound within 48 h, and the results of cardiac ultrasound were followed up for 6 months after PCI, and the LVEF was acquired. The follow-up results were obtained through the reporting workstation. The patients whose LVEF increased after PCI by at least 20% compared with the baseline at the time of re-examination formed the LVEF improvement group. The remaining patients formed the no-improvement group.
Follow-up of MACEs
Patients were categorized into 2 groups according to the median MSI, over a median follow-up period of 270 (128–366) days, to estimate the prognostic significance of MSI for MACEs acquired by the 2 calculation methods.
The clinical follow-up was conducted by telephone and the inpatient case system. The occurrence of MACEs, which included recurrent angina pectoris, AMI, heart failure, and death from coronary heart disease, was considered as the primary point of this study. The median follow-up time was 270 (range: 128–366) days. The follow-up was conducted every 6 months after the GSMPI.
Statistical analysis
All data were analyzed using the Statistical Package for the Social Sciences version 19.0 software (IBM Corporation, NY, USA) and the MedCalc software. Continuous variables were expressed as mean ± standard deviation, count variables as the number of cases and percentages (%), and discrete variables as median and quartile range. The differences in the MSI obtained by the number and scoring evaluation methods were compared using the paired-samples t test. We compared the baseline data and GSMPI parameters between the LVEF improvement and no-improvement groups. The area under ROC was used to evaluate the predictions of LVEF improvement and the incidence of MACEs. The area under the curves (AUCs), specificity, sensitivity, and Youden’s index were analyzed to define the optimal cutoff values for predicting LVEF improvement. Delong’s test was applied to compare the difference in AUCs between the 2 evaluation methods (P < 0.05). The Kaplan–Meier method was used for depicting survival curves. The differences were assessed using log-rank tests. Cox proportional-hazards regression was performed to calculate the hazard ratio (HR) and 95% confidence interval (CI) and confirm the independent predictors.
Results
Patient characteristics and follow-up
A total of 62 patients with single coronary artery disease were evaluated (only 1 coronary artery had a degree of stenosis of > 50%), including 35 with left anterior descending artery disease, 16 with right coronary artery disease, and 11 with left circumflex artery disease. The TIMI grade of all patients after PCI was grade 3. GSMPI was performed 3–10 days after PCI at a median time of 6 days. The median time for the first cardiac ultrasound examination was 1.3 days after PCI. The cardiac ultrasound showed segmental wall motion abnormality in all patients, and severe valvular abnormalities and myocardial hypertrophy were not found. The median time of ultrasound re-examination after PCI was 6.2 months; 55 patients completed re-examination and follow-up. The remaining 7 patients did not return to the hospital for ultrasound within 6 months. 24 cases (43.6%) whose LVEF improved from (43.3 ± 6.9) % to (57.1 ± 6.4)%. In the improved group, the proportion of culprit vessel that were LAD and RCA was similar, and both were higher than LCX [LAD/RCA/LCX ratio (%):46.7/46.6/6.67]. LAD was the most common culprit vessel in the LVEF no-improved group [LAD/RCA/LCX ratio (%): 72.2/16.7/11.1]. The median LVEF of the no-improved group was lower than that of the improved group [(41.5 ± 12.1)% vs (45.2 ± 8.3)%.]. However, there was no statistical difference between them in our study (P > 0.05). All 62 patients were followed up for MACEs, with a median follow-up period of 270 (range 128–366) days. The primary endpoint occurred in 8 patients (12.9%), including 6 with recurrent angina pectoris and 2 with recurrent AMI. 6 patients with recurrent angina pectoris were evaluated by a hospital-specific independent committee according to the evaluation criteria for recurrent angina pectoris, and all met the following criteria: (1) Typical angina symptoms: stuffy pain or constriction in the retrosternal or precardiac area induced by physical labor or emotional agitation, lasting for several minutes. (2) Dynamic changes in electrocardiogram: horizontal ST-segment depression or T wave inversion. Two patients with recurrent AMI were admitted for CAG. The subsequent AMIs in both patients occurred in different coronary arteries that caused the first AMI in this study (LAD was the culprit vessel for the first AMI in both patients, RCA was the culprit vessel for the the second AMI). Heart failure and death from coronary heart disease were not detected in either group.
The administration rates of cardioprotective medications during follow-up were as follows: all participants were treated with dual antiplatelet drugs, 90.3% were treated with beta blockers, 93% were treated with angiotensin-converting enzyme inhibitors (ACEI) or angiotensin-II receptor antagonists (ARB), and 99% were treated with statins. There was no significant difference in the medications between the LVEF improved and the LVEF no-improved group, as was the case in the MACE and the non-MACE group (all P > 0.05).
Comparison of MSI obtained by the 2 calculation methods
The MSI value obtained by the scoring and number evaluation methods was 0.30 ± 0.2 and 0.25 ± 0.1, respectively. They were highly correlated (r = 0.767, P < 0.05, 95%CI 0.623–0.860) but with statistically significant differences (P < 0.01).
Comparison of MSI in predicting LVEF improvement through various calculation methods
When the number evaluation method was used, the ROC analysis revealed that the AUC of MSI for predicting LVEF improvement was 0.698(P < 0.05, 95%CI 0.514–0.845). The Youden index J was 0.346, and the associated criterion was ≤ 0.27 (sensitivity was 50.0% and specificity was 84.6%).
In the ROC analysis, using the scoring evaluation method, the AUC of MSI for predicting LVEF improvement was found to be 0.890 (P < 0.01, 95%CI 0.733–0.972). The Youden index J was 0.792, with an associated criterion of ≤ 0.21 (sensitivity of 95% and specificity of 84.6%). The sensitivity increased whereas the specificity was the same compared with the number evaluation method. Delong’s test revealed a statistical difference in AUCs between the 2 methods (P < 0.05, 95%CI 0.012–0.373). The MSI acquired by the scoring evaluation method was higher than that obtained by the number evaluation method in predicting LVEF improvement. The difference between areas was 0.192. The Z statistic value was 2.086 (Fig. 1 and Table 1).

Receiver operating characteristic curve (ROC) demonstrating the prognostic value of myocardial salvage index (MSI) in predicting LVEF improvement acquired using the scoring and number evaluation methods with Gated SPECT myocardial perfusion imaging (GSMPI)
With the scoring evaluation method, we observed a remarkable difference in the LVEF increase (△LVEF) between the patients with MSI ≥ median MSI (0.30) and MSI < median MSI (0.30) (13.6% ± 3.8% vs 2.0% ± 3.2%). In patients with an MSI ≥ median MSI, the percentage depicting an LVEF increase was statistically higher than in those with an MSI < median MSI (71.4% vs 25.0%). Figure 2 illustrates a representative example of a patient with a large MSI and subsequent LVEF improvement.

A representative example of a patient with a large myocardial salvage index (MSI) and subsequent LVEF improvement. Wall-thickening polar map (a), perfusion polar map (b), wall-thickening scores (c), and perfusion scores (d) in a patient with inferior acute myocardial infarction (AMI). Using the scoring evaluation method, the wall-thickening abnormality was approximately 21.6% [11/3 × 17) × 100%] of the LV wall area, together with a relatively limited perfusion defect, approximately 7% [5/4 × 17) × 100%], with an estimated MSI of 0.68. LVEF after AMI was impaired at 45%, and LVEF at 3-month follow-up after PCI increased to 64%. LV, left ventricle; LVEF, left ventricular ejection fraction
Comparison of MSI in predicting MACEs using various calculation methods
Patients were divided into 2 groups according to the median MSI obtained through the 2 calculation methods. Using the scoring evaluation method, 4 patients were reported to have recurrent angina pectoris (16.0%) and 2 had AMI (8.0%) in the < median MSI (0.25) group, and only 2 had recurrent angina pectoris (7.4%) in the ≥ median MSI (0.25) group. The ROC analysis revealed that the AUC of MSI for predicting the MACEs was 0.890 (P < 0.05, 95% CI 0.770–0.960), the Youden index J was 0.75, and the associated criterion was ≤ 0.05 (sensitivity was 75.0% and specificity was 100%).
Using the number evaluation method, 4 patients had recurrent angina pectoris (17.3%) and 2 had AMI (8.7%) in the < median MSI (0.20) group, and only 2 had recurrent angina pectoris (6.8%) in the ≥ median MSI (0.20) group. The ROC analysis revealed that the AUC of MSI for predicting the MACEs was 0.709 (P < 0.05, 95% CI 0.565–0.828), the Youden index J was 0.439, and the associated criterion was ≤ 0.1 (sensitivity was 62.5% and specificity was 81.4%).
Delong’s test revealed a statistical difference in AUCs between the 2 methods (P < 0.05, 95%CI 0.071–0.289). The MSI acquired with the scoring evaluation method had a higher value than that obtained through the number evaluation method in predicting MACEs. The difference between areas was 0.18. The Z statistic value was 3.242 (Fig. 3 and Table 2).

Receiver operating characteristic curve (ROC) revealing the prognostic value of myocardial salvage index (MSI) in predicting MACEs acquired using the scoring and number evaluation methods with Gated SPECT myocardial perfusion imaging (GSMPI)
With the scoring evaluation method, the Kaplan–Meier survival analysis revealed that the Cox prevalence of MACEs was considerably higher in the MSI < median MSI group than in the MSI ≥ median MSI group (HR 0.145; 95% CI 0.03242–0.6473; P < 0.05) (Fig. 4). With the number evaluation method, the Cox prevalence of MACEs displayed no remarkable differences between the MSI < median MSI group and the MSI ≥ median MSI group (P = 0.0963, > 0.05) (Fig. 5). Obviously, the MSI acquired using the scoring evaluation method had a higher value than that obtained with the number evaluation method in predicting MACEs.

Kaplan–Meier survival curves for 62 patients separated into 2 groups according to the median myocardial salvage index (MSI) obtained using the scoring evaluation method

Kaplan–Meier survival curves for 62 patients separated into 2 groups according to the median myocardial salvage index (MSI) obtained using the number evaluation method
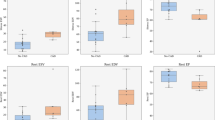
The t test indicated no substantial differences in sex, age, BMI, history of hypertension, smoking history, time from onset to balloon dilatation, and the infarct-related vessel CAG, cTnT, LVEF, and PER (all P > 0.05)(Table 3). Remarkable differences were observed in the proportion of patients with diabetes, CK, CK-MB, MSI, TPD, SRS, and PFR between the 2 groups (all P < 0.05). However, Cox multivariate regression analysis revealed that only the MSI was the independent predictor of MACEs (P < 0.01, 95% CI 1.1289E-14-0.0003 (Table 4).
Discussion
The present study evaluated the MSI using a simple procedure based on a single resting GSMPI using the scoring evaluation method early after PCI in patients with AMI. We identified the improvement in the value of MSI in predicting MACEs and LVEF improvement estimated by the optimized gated SPECT. This study was novel in evaluating the prognostic significance in reperfused AMI.
We compared the receiver operating characteristic curve (ROC) in predicting left ventricular ejection fraction improvement 6 months after PCI and the survival curves for predicting 1-year major MACEs of an MSI between the 2 methods, and we found out the MSI acquired through the scoring evaluation method had a stronger prognostic value than that obtained with the number evaluation method, which confirmed the advantage of the scoring evaluation method. To the best of our knowledge, this has not been done in previous similar studies. Our study found that both the AUCs of MSI for predicting LVEF improvement and the MACEs, using the scoring evaluation method, were larger than that done with the by number evaluation method. Delong’s test revealed a statistical difference in AUCs between the 2 methods. With the scoring evaluation method, patients with < median MSI have a significantly higher incidence of MACEs at 1-year follow-up; however, with the number evaluation method, the Cox prevalence of MACEs displayed no remarkable differences between patients with < median MSI and ≥ median MSI. Furthermore, the independent predictors of MACEs were confirmed through the scoring evaluation method that only the MSI was the independent predictor of MACEs.
These findings indicated that the MSI could be used as another prognostic indicator, and they emphasized the significance of MSI in the prognostic assessment by GSMPI using the scoring evaluation method. Previous studies with large sample sizes [3,4,5, 8], which acquired the MSI by injecting the tracer before PCI, concluded that the MSI had a prognostic value in patients with AMI, which was consistent with our findings with GSMPI early after PCI. However, the feasibility was far less than that of the present study.
This study acquired AAR from a single GSMPI early after PCI. Myocardial stunning persisting after AMI reperfusion therapy may explain this [26]. The myocardial blood flow was restored early after PCI, whereas the ventricular dysfunction began to recover 48 h after PCI and persisted for days to weeks [27]; this implied a flow–functional mismatch. Therefore, the stunned asynergic area size within 48 h can be close to the ischemia myocardium AAR.
In rats, AMI AAR was acquired with 99mTc-MIBI injection 3 days after reperfusion, thereby confirming the feasibility of this method [12]. Qin et al. acquired AAR through GSMPI perfusion imaging from 24 h to 7 days after PCI in patients with AMI [13]. In other studies [14, 15], a single GSMPI perfusion image was created 5–10 days after PCI to assess AAR and then the MSI was obtained, which was reported to be comparable with the MSI of 2 GSMPI images. A single GSMPI early after PCI can replace the 2-image procedure to calculate the MSI.
The timing of GSMPI to assess the FIS is another crucial factor. The FIS displayed by GSMPI 18–48 h after AMI is likely overestimated compared with that before discharge (i.e., 1–2 weeks after AMI) [28]. Moreover, the unstable status of patients with AMI within 48 h after PCI should also be considered. Therefore, a time point between 48 h and 1 week after PCI may be the best time to assess MSI. In the present study, Gate SPECT was performed 3–10 days after PCI to acquire MS and MSI (the median time was 6.2 days).
The MSI was acquired by early GSMPI after PCI and predicted LVEF improvement in patients with AMI 6 months after PCI [17]. However, the number evaluation method differed from ours in that the extent of abnormality (perfusion or wall thickening) was the percentage of the number of abnormal segments divided by the total number of myocardial segments, without considering the degree of abnormality. In our study, the percentage of the total scores of abnormal segments was the degree of abnormality divided by the sum of the maximum scores of all myocardial segments using a 4-point scale (the wall-thickening scores; the sum of the maximum scores was 3 × 17) and a 5-point scale (the myocardial perfusion scores; the sum of the maximum scores was 4 × 17). The semi-quantitative scoring method was used to calculate the extent of any abnormality.
The MSI acquired by the aforementioned 2 assessment methods indicated a remarkable correlation, but with a considerable difference. The MSI obtained using the scoring evaluation method could provide a better predictive value than just counting the segments. This might be because the final data were quantitative. The scoring evaluation method considered the degree of anomalies rather than just counting the number, likely imparting more objectivity to the data. The present study preliminarily established the threshold of MSI to predict the LVEF increase after PCI in AMI acquired using the scoring evaluation method. The approach was the major innovation of our study. Moreover, the preferred software automatically provided data in this study, which was more objective than previous visual judgment methods and reduced the subjective error caused by inexperience. Another point of variation in our study was that patients with multi-vessel disease were excluded, thus avoiding the interference caused by non infarct-related vessels. These additional differences in methodology could account for the divergence in findings between our study and others.
Limitation
This study had a number of limitations. First, despite weighing both AAR and FIS, GSMPI performed nearly 1 week after PCI could still underestimate the AAR, compared with the direct measurement using 2 SPECT images. Myocardial stunning is a time-dependent phenomenon, and hence partial ventricular dysfunction disappeared. However, patient safety must be considered, as acquiring the ultra-early GSMPI is challenging. We still confirmed the feasibility and practicability of a single post-intervention GSMPI to assess the MSI, and the results of the predictive value for MACEs were meaningful. Another limitation was that this study was conducted in a single center with a small cohort, so the number of positive patients was small in the MACE statistics. The small sample size was also related to the safety of clinicians considering the early stage after PCI in patients with AMI.
Conclusion
In conclusion, the MSI obtained using a simple GSMPI procedure with the scoring evaluation method early after PCI could be used for predicting the LVEF improvement and the MACE rate in AMI. It considerably improved the prognostic value compared with the previous reference methods. The MSI can be used as a new indicator to optimize risk stratification and orient subsequent patient management, such as rehabilitation training and medication treatment.
The authors affirm that human research participants provided informed consent for publication of the images in Figs 1, 2, 3, 4, 5.
References
Fan ZY, Wu CW, Wesemann LD, Ouchi E, Bautista M, Qiu J, Xu JR, Zhou Y, Wu LM. Predictive value of major adverse cardiac events by T2-mapping texture analysis of the myocardial remote zone in patients with acute myocardial infarction. Clin Radiol. 2022;77(3):e241–9. https://doi.org/10.1016/j.crad.2021.12.015.
Fan ZY, Wu CW, An DA, et al. Myocardial area at risk and salvage in reperfused acute MI measured by texture analysis of cardiac T2 mapping and its prediction value of functional recovery in the convalescent stage. Int J Cardiovasc Imaging. 2021;37(12):3549–60. https://doi.org/10.1007/s10554-021-02336-7.
Takehana K, Ruiz M, Petruzella FD, et al. Tc-99m sestamibi defect magnitude predicts the am-ount of viable myocardium after coronary reperfusion despite the presence of severe residual stenosis. J Nucl Cardiol. 2001;8(1):40–8. https://doi.org/10.1067/mnc.2001.110387.
Parodi G, Ndrepepa G, Kastrati A, et al. Beyond 12 hours Reperfusion AlternatiVe Evaluation (BRAVE-2) Trial Investigators. Ability of mechanical reperfusion to salvage myocardium in patients with acute myocardial infarction presenting beyond 12 hours after onset of symptoms. AM Heart J. 2006;152(6):1133–9. https://doi.org/10.1016/j.ahj.2006.08.007.
Busk M, Kaltoft A, Nielsen SS, Bøttcher M, et al. Infarct size and myocardial salvage after pri-mary angioplasty in patients presenting with symptoms for <12 h vs. 12–72 h. Eur Heart J. 2009; 30(11):1322–30. https://doi.org/10.1093/eurheartj/ehp113.
Kastrati A, Mehilli J, Dirschinger J, et al. Stent versus thrombolysis for occluded coronary ar-teries in patients with acute myocardial infarction (STOPAMI-2) Study. Myocardial salvage af-ter coronary stenting plus abciximab versus fibrinolysis plus abciximab in patients with acute myocardial infarction: a randomised trial. Lancet. 2002;359(9310):920–5. https://doi.org/10.1016/S0140-6736(02) 08022–4.
Ndrepepa G, Mehilli J, Schwaiger M, et al. Prognostic value of myocardial salvage achieved by reperfusion therapy in patients with acute myocardial infarction. J Nucl Med. 2004;45(5):725–9.
Engblom H, Aletras AH, Heiberg E, Arheden H, Carlsson M. Quantification of myocardial salv-alvage by myocardial perfusion SPECT and cardiac magnetic resonance-reference standards for ECG development. J Electrocardiol. 2014; 47(4):525–34. https://doi.org/10.1016/j.jelectrocard.2014.04.001.
Mochizuki T, Murase K, Higashino H, et al. Ischemic “memory image” in acute myocardial infarction of 123I-BMIPP after reperfusion therapy: a comparison with 99mTc-pyrophosphate and 201Tl dual-isotope SPECT. Ann Nucl Med. 2002;16(8):563–8. https://doi.org/10.1007/BF02988634.
Shibata N, Takagi K, Morishima I, et al. The impact of the excimer laser on myocardial salvage in ST-elevation acute myocardial infarction via nuclear scintigraphy. Int J Cardiovasc Imaging. 2020;36(1):161–70. https://doi.org/10.1007/s10554-019-01690-x.
Yoshida R, Takagi K, Ishii H, Morishima I, et al. Myocardial salvage after ST-segment-elevation myocardial infarction: comparison between prasugrel and clopidogrel in the presence or absence of high-residual platelet reactivity. J Nucl Cardiol. 2021;28(4):1422–34. https://doi.org/10.1007/s12350-019-01852-3.
Wakabayashi H, Taki J, Mori H, et al. Visualization of Dynamic Expression of Myocardial Sig-ma-1 receptor after myocardial ischemia and reperfusion using radioiodine-labeled2-[4-(2-iodophenyl) piperidino] cyclopentanol (OI5V) imaging. Circ J. 2021;85(11):2102–108. https://doi.org/10.1253/circj.CJ-21-0320.
Qin H, Li S, Liu Z. Protective effect of shexiang baoxin pill on myocardial ischemia/reperfusi-on injury in patients with STEMI. Front Pharmacol. 2021;10(12): 721011. https://doi.org/10.3389/fphar.2021.721011.
Sotgia B, Sciagrà R, Parodi G, Kastrati A, Antoniucci D, Schömig A, Pupi A. Estimate of myocardial salvage in late presentation acute myocardial infarction by comparing functional and perfusion abnormalities in predischarge gated SPECT. Eur J Nucl Med Mol Imaging. 2008;35(5):906–11. https://doi.org/10.1007/s00259-007-0663-3.
Sciagrà R, Dona M, Coppola A, Leoncini M, Maioli M, Castagnoli A, Bellandi F, Pupi A. Feasi-bility of an accurate assessment of myocardial salvage by comparing functional and perfusion a-bnormalities in post-reperfusion gated SPECT. J Nucl Cardiol. 2010;17(5):825–30. https://doi.org/10.1007/s12350-010-9247-x.
Calabretta R, Castello A, Linguanti F, et al. Prediction of functional recovery after primary PCI using the estimate of myocardial salvage in gated SPECT early after acute myocardial infarction. Eur J Nucl Med Mol Imaging. 2018;45(4):530–7. https://doi.org/10.1007/s00259-017-3891-1.
Romero-Farina G, Aguadé-Bruix S, Candell-Riera J, et al. Acute myocardial infarction: estimation of at-risk and salvaged myocardium at myocardial perfusion SPECT 1 month after infarction. Radiology. 2013;269(2):577–84. https://doi.org/10.1148/radiology.13122324.
Thygesen K, Alpert JS, Jaffe AS, et al. Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AH- A)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction. Fourth Universal Definition of Myocardial Infarction. J Am Coll Cardiol. 2018;72(18):2231–64. https://doi.org/10.1016/j.jacc.2018.08.1038.
Poli A, Fetiveau R, Vandoni P, et al. Integrated analysis of myocardial blush and ST-segment elevation recovery after successful primary angioplasty: real-time grading of microvascular reperfusion and prediction of early and late recovery of left ventricular function. Circulation. 2002;106(3):313–8. https://doi.org/10.1161/01.cir.0000022691.71708.94.
Ganz W. The thrombolysis in myocardial infarction (TIMI) trial. Phase I findings. TIMI Study Group. New England J Med 1985;313(16):1018. 10. 1056/NEJM198510173131611.
Jeremias A, Davies JE, Maehara A, Matsumura M, Schneider J, et al. Blinded physiological assessment of residual ischemia after successful angiographic percutaneous coronary intervention: The DEFINE PCI study. JACC Cardiovasc Interv. 2019. https://doi.org/10.1016/j.jcin.2019.05.054.
Bestetti A, Cuko B, Decarli A, Galli A, Lombardi F. Additional value of systolic wall thickening in myocardial stunning evaluated by stress-rest gated perfusion SPECT. J Nucl Cardiol. 2019;26(3):833–40. https://doi.org/10.1007/s12350-017-1115-5.
Bestetti A, Cuko B, Gasparini M, De Servi S. Better characterization of dipyridamole-induced myocardial stunning by systolic wall thickening. A gated perfusion SPECT study. J Nucl Cardiol. 2020;27(1):137–146. https://doi.org/10.1007/s12350-018-1340-6.
Sharir T. What is the value of motion and thickening in gated myocardial perfusion SPECT? J Nucl Cardiol. 2018;25(3):754–7. https://doi.org/10.1007/s12350-018-1239-2.
Miller RJH, Klein E, Gransar H, et al. Prognostic significance of previous myocardial infarction and previous revascularization in patients undergoing SPECT MPI. Int J Cardiol. 2020;3(13):9–15. https://doi.org/10.1016/j.ijcard.2020.04.012.
Kloner RA. Stunned and hibernating myocardium: where are we nearly 4 decades later? J Am Heart Assoc. 2020;9(3): e015502. https://doi.org/10.1161/JAHA.119.015502.
Ambrosio G, Zweier JL, Jacobus WE, Weisfeldt ML, Flaherty JT. Improvement of postischemic myocardial function and metabolism induced by administration of deferoxamine at the time of reflow: the role of iron in the pathogenesis of reperfusion injury. Circulation. 1987;76(4):906–15. https://doi.org/10.1161/01.cir.76.4.906.
Pellikka PA, Behrenbeck T, Verani MS, Mahmarian JJ, Wackers FJ, Gibbons RJ. Serial changes in myocardial perfusion using tomographic technetium-99m-hexakis-2-methoxy-2-methylpropyl- isonitrile imaging following reperfusion therapy of myocardial infarction. J Nucl Med. 1990;31(8):1269–75.
Acknowledgements
I would like to thank my supervisor, Professor Xu, for his guidance through each stage of the process. I would like to acknowledge Professor Gao, for inspiring my interest in the development of innovative technologies. My research partner, Dr Dou, was instrumental in defining the path of my research. For this, I am extremely grateful. We declare that we have no financial and personal relationships with other people or organizations that can inappropriately influence our work. There is no professional or other personal interest of any nature or kind in any product, service and/or company that could be construed as influencing the position presented in, or the review of, the manuscript entitled.
Funding
This study was supported by the Key Project of Scientific and Technological Support Plan of Tianjin in 2020 (No. 20YFZCSY00820), the Key Disciplines of Tianjin Health Research Project (No. TJWJ2022XK032), and the Key Projects of Tianjin Natural Science Foundation (No. 22JCZDJC00130).
Author information
Authors and Affiliations
Corresponding authors
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Li, T., Dou, J., Zhang, H. et al. Optimized gated a SPECT-derived myocardial salvage index: its prognostic significance in predicting major adverse cardiac events following acute myocardial infarction percussion. Ann Nucl Med 38, 219–230 (2024). https://doi.org/10.1007/s12149-023-01894-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12149-023-01894-1