
Abstract
Purpose
This study aimed to analyze the morphology of the anterior femoral condyle using a quantitative three-dimensional reconstruction method. The morphological data were compared between genders.
Methods
Computed tomography scans of femurs were taken from 90 healthy subjects and then reconstructed in 3D modeling software. Coaxial cutting planes were created at 10° increments to measure the lateral and medial anterior condylar heights (LACH and MACH, respectively), lateral and medial trochlear groove widths (LTW and MTW, respectively), and for trochlear groove tracking. The absolute values and normalized data were compared between male and female subjects. The sulcus angle and deepest point of the trochlear groove at each cross-section were also analyzed to determine the differences in the depth of the trochlear groove.
Results
The absolute dimensions of LACH, MACH, LTW, and MTW were significantly smaller in the female subjects, by 10.5%, 36.9%, 10.3%, and 11.0%, respectively, than in the males (p < 0.05). After normalization, no significant difference was found in the condylar height between the genders. However, the female subjects had a significantly larger value of approximately 7.9% for the normalized trochlear width.
Conclusion
Male subjects had greater condylar heights and widths than the female subjects. Although the trajectory of the trochlear groove varied greatly among the subjects, the trochlear groove appeared to be wider and shallower in the female subjects than in the male subjects. These results provide important information for the design of femoral trochlea to fit Asian female patients.
Level of evidence
III.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Mapping the morphology of skeletal bone provides important information for designing orthopedic prostheses. As such, variations in the morphology of the knee between males and females have been extensively researched [11, 16, 19,20,21,22]. Three characteristic features of female knees that are different from those of males knees include an larger Q-angle, less observable prominence of the femoral trochlea, and a lower mediolateral (ML) to anteroposterior (AP) femoral condylar aspect ratio [10, 11, 16, 31]. Therefore, given such differences, gender-specific implants should be considered when developing contemporary knee prostheses [10, 17, 20].
Most studies on knee morphology used radiographic images or magnetic resonance imaging (MRI) to evaluate gender differences in the morphology of the anterior femoral condyle and trochlea [7, 8, 20, 29]. However, the femoral trochlea comprises a complex three-dimensional (3D) geometry, the curvature and trajectory of which cannot be accurately measured via two-dimensional images. More recent studies introduced reverse engineering techniques [3, 24, 25], such as image processing and computer-aided design, to reconstruct a 3D geometrical models for measuring morphological parameters. Such methods provide more accurate geometry and curvature data than two-dimensional measurements.
Using detailed 3D models, accurate measurements of the geometry of the anterior condyle and trochlear groove can be obtained at different flexion angles to represent the complete shape of the femoral trochlear groove [4, 6, 13]. Pinskerova et al.’s study [28] showed that the distal femur in Caucasian females is relatively narrower than in males. However, no significant difference was found after normalizing the dimensions of the femur. Some studies have further compared the knee geometry between Caucasian and Chinese subjects and demonstrated large dimensional differences [22, 26, 35]. Although previous studies have presented data showing differences in trochlear groove morphology among genders and races, morphometric parameters of the trochlear groove have not been reported on. The trochlear groove has a complex shape, similar to the peaks and valleys of mountains, as shown in Fig. 1 (gray region). Although the height of the medial and lateral condyles have been measured [6, 20, 21], to the authors’ knowledge, the mediolateral widths between the highest points of the medial and lateral condyles and the lowest point of the trochlear groove have not been measured. Correlating the widths may be helpful to know the lope change of the patellar groove on the ML direction (Fig. 1b). The aim of this study was to evaluate the relationship between the abovementioned highest and lowest points and the width of the anterior condyle. This information would then be used to clearly describe the geometry of the trochlear groove on the transversal plane. Furthermore, this study also aimed to evaluate differences in knee morphology between the genders.

a The anterior femoral condyle cut and viewed in the coronal plane and the definition of lateral and medial condylar heights and trochlear groove depth on the cutting plane. b The definition of lateral and medial trochlear height and width
Materials and methods
The study was approved by the Institutional Review Board of SCMH (IRB number: 1021004), and informed consent was obtained from all enrolled subjects. Images were acquired in the axial direction along the midshaft of the femur and tibia. The inclusion criterion for this study was healthy adult knees without any symptoms of soft tissue injury or osteoarthritis. Individuals with a history of knee trauma, anterior knee pain, or other chronic diseases of the musculoskeletal system were excluded. Ninety subjects were enrolled in this study (44 males and 46 females) out of a pool of 108. The median age of the female subjects was 38 years (range 20–54 years; SD 10.0) and that of the male subjects was 37 years (range, 20–52 years; SD 9.9). The median weight of the female subjects was 56 kg (range 37–90 kg; SD 11.6) and that of the male subjects was 75 kg (range 53–105 kg; SD 11.1). The median height of the female subjects was 161 cm (range 160–170 cm; SD 5.7), and that of the male subjects was 172 cm (range 160–185 cm; SD 5.5).
Reconstruction of the 3D knee model
Computed tomography (CT) was performed on both femurs of each subject using a GE Light Speed 16 system (GE Medical System, General Electric Company, Milwaukee, WI, USA). During the scan, each subject was requested to remain in a relaxed and extended supine position. CT was performed using a slice thickness of 0.625 -mm (resolution 512 × 512 pixels) with a 360 × 360 -mm field of view around the knee joint. The obtained CT images of the knee were then reconstructed into a 3D model of the knee.
Definition of coordinate system
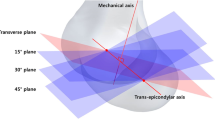
Reverse engineering software RevCAD V1.50 (PouYuen Tech Corp., Taoyuan, Taiwan) was used to measure the condylar geometry on the transversal plane. This study defined the orthogonal coordinate system based on the transepicondylar axis (TEA), which is often used a reference feature for morphological analyses and for surgery [21]. The origin of the coordinate system was defined as the lateral end point of the TEA. The X-axis was defined as the TEA, with the coronal plane passing through the TEA and parallel to the anatomical axis. The Y-axis was defined as a line parallel to the femoral mechanical axis, which was at 6° valgus to the anatomical axis (line along the femoral shaft) in the coronal plane. The Z-axis was perpendicular to the X- and Y-axes.
Measurement of anterior condylar geometry
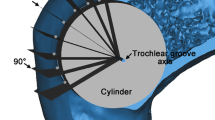
To evaluate the geometry of the anterior condyle, cutting planes were created at 10° increments rotated along the femoral TEA from the femoral cortex to the distal femur (intercondylar notch) (Fig. 1a). The anterior condyle was defined as the area of bone anterior to the anterior femoral cortex [8]. The cutting curve was defined as the intersection between the cutting plane and the femoral model, shown as a black bold line in Fig. 1. A cutting plane was created on the anterior condylar to simulate the first bone cut when performing isolated patellofemoral (PF) arthroplasty (Fig. 1a). The height of the lateral and medial anterior condyles (LACH and MACH, respectively) and height of the anterior trochlear groove (ATGH) were measured. LACH was defined as the distance between the highest point of the lateral condyle and the plane referenced to the anterior cortex of the distal femur (cutting plane in Fig. 1), MACH was the distance between the highest point of the medial condyle and the plane referenced to the anterior cortex of the distal femur, and ATGH was the distance between the lowest point of the trochlear groove and the plane referenced to the anterior cortex of the distal femur. A positive value of these parameters indicated that the point was higher than the cutting plane, whereas a negative value indicated that the point was lower than the cutting plane. The distances from the highest eminences of the lateral and medial condyles to the lowest point of the groove were defined as ∆HL and ∆HM, respectively (Fig. 1a), by Eqs. 1 and 2:
To clearly describe the contours of the trochlear groove, the relationship between the highest and lowest points to the groove width was determined. The complex contours of the anterior condyle could be simplified as peaks/valleys, similar to those of mountains. The peaks in the geometry indicated the highest points of the medial and lateral condyles, and the lowest point of the trochlear groove in each cross-section was identified as a valley. In addition to LACH and MACH, the lateral and medial trochlear groove widths (LTW and MTW, respectively) were measured (Fig. 1b). These widths were defined as the distance between the most anterior point of the lateral or medial cutting curve (ridge) and the deepest point of the trochlear groove along the X-axis. The parameters were measured at 10° increments according to the previously defined coordinate system.
To eliminate the effects of knee size on the measurements, normalized data were further analyzed [8]. The anterior condylar heights were normalized by dividing the height by the femoral AP dimension (fAP) and noted as LACH-R, MACH-R, and ATGH-R [21]. The length of fAP indicated the distance between the most posterior point of the lateral condyle and the cutting plane (Fig. 1b). The width of the anterior condylar was normalized by dividing the width by the length of TEA and noted as LTW-R and MTW-R.
Measurement of the trajectory of the trochlear groove
Figure 2 shows the typical trajectory of the trochlear groove, i.e., the connection of all projection points. Points on the trochlear groove were traced and projected onto the XY plane of the femur via a roll-out projection method [4]. The distance between each trochlear groove point (l) was defined as the vertical distance on the plotted line in a proximodistal direction (i.e., proximodistal propagation of the trochlear groove). The distance from the trochlear groove points to the mechanical axis (d) was indicated as the horizontal distance in a mediolateral direction. If a point was located on the medial side of the mechanical axis, the value was defined as positive (d); otherwise, the value was negative (−d).

Measurement of the mediolateral position and orientation of trochlear groove tracking. A roll-out projection was used to preserve the length of the trochlear groove. The distance between each trochlear groove point (l) was defined as the vertical distance on the scheme of trochlear groove tracking. The distance (mediolateral position) from the trochlear groove points to the mechanical axis (d) was defined as the horizontal distance. If a point was located on the medial side of the mechanical axis, the value was defined as positive (d); otherwise, the value was negative (− d)
The natural orientation of the trochlear groove follows a path that can be approximated by two consecutive straight lines as a bilinear approximation [4, 15]. Determining the turning point would be helpful in understanding changes in the curvature of the trochlear groove [4]. This study analyzed the trajectory of the trochlear groove to determine whether any difference exists between the genders (Fig. 2). The sulcus angle was also measured at 10° increments to understand how the angle changes. The sulcus angle was defined as the angle formed between the lines joining the highest points on the medial and lateral cutting curves to the lowest point on the cutting curves (Fig. 1) [5, 20]. All data were recorded by two authors (CP Hsu and JC Lin) to ensure inter- and intraobserver reliability.
Statistical analysis
A Kolmogorov–Smirnov test was used to analyze whether each set of data (∆HL, ∆HM, LTW, MTW, LTW-R, MTW-R, and trochlear groove tracking) were normally distributed. If data were normally distributed, an independent Student’s t test was performed to determine any significant differences between the genders. If data were not -normally distributed, a Mann–Whitney U test was performed. For normally distributed data, descriptive results were presented as means ± SD. For non-normally distributed data, the results were presented as a median and interquartile range. A p value < 0.05 was considered statistically significant. All statistical analyses were performed using the SPSS software package (Version 23, SPSS Inc, Chicago, IL, USA).
A post hoc power analysis using G*Power 3.1 (Franz Paul, Kiel, Germany) was performed to determine the power of the present study. Based on the results of the Student’s t test regarding the difference in the femoral trochlear width between the genders, an effect size of 0.66 was calculated. With the underlying effect size, an α of 0.05, and a study group of 90 subjects (male = 44 and female = 46), a power of 0.87 was calculated. The sample size was found to be satisfactory based on the power analysis (power > 0.8).
Results
Anterior condylar geometry
The male subjects had greater absolute values of ∆HL and ∆HM than the female subjects (Fig. 3, Table 1). For the lateral condyle, a significant difference was found between the genders in ∆HL in the range of 20° to − 50° (p < 0.05). The peak value of ∆HL occurred at 10° for both female and male subjects. A maximum increase of 10% was found at 20° in male subjects compared with that in female subjects. For ∆HM, there was a significant difference between the genders in the range of − 10° to − 50° (p < 0.05). The peak ∆HM occurred at 30° for both female and male subjects. A maximum increase of 31% was seen at 20° in male subjects compared with that in female subjects. However, the difference in the anterior condylar height was not significant between the genders after normalization.

∆HL and ∆HM in each cutting plane for male and female subjects
Regarding the trochlear width (Fig. 4), the male subjects had greater absolute values than the female subjects on both the lateral and medial sides. The discrepancies between the female and male condyles on each side were larger, ranging from − 20° to 50° (Fig. 4a, Table 2). However, the differences were mostly eliminated when the condylar widths were normalized to the TEA length, particularly for the medial condylar width (dashed lines) (Fig. 4b, Table 3). The average TEA from the male and female subjects was 84.1 ± 3.6 mm and 72.6 ± 3.5 mm, respectively. The male subjects had a greater absolute trochlear width than the female subjects There were significant differences between the genders for LTW-R in the range of − 20° to 0° (Table 3) (p < 0.05) as well as for MTW-R in the range of 10° to − 20°. Furthermore, significant gender differences were observed for MTW-R and LTW-R at an angle of − 40° near the anterior cortex.

a Lateral and medial trochlear groove widths and b lateral and medial trochlear groove widths of normalization in each cutting plane for male and female subjects
Trajectory of the trochlear groove and sulcus angle
Figure 5 describes the path of the trochlear groove, which was initially located on the lateral side of the anterior femur, before gradually turning to the medial side as the angles increase, and then finally shifting to the lateral side at deep flexion angles. Both genders showed a turning point in the trochlear groove tracking, indicating that the trochlear groove is bilinear. The change started at approximately − 20° for the male group and at − 10° for the female group (Fig. 5). No significant difference in the trajectory of the trochlear groove was observed between the genders.

The distance between trochlear groove points and the trochlear groove trajectory and the sulcus angle in each cutting plane for Asian male and female subjects
Regarding the sulcus angle, the average angle in the female subjects were larger than in the male subjects in the range of − 30° to − 10°. A significant difference was only detected at − 10°. Moreover, the mean sulcus angle of the female subjects appeared to be approximately 5.2° greater than that of the male subjects (p = 0.034).
Discussion
The most important finding of this study was the significant difference in trochlear width between the genders. The female subjects had than the male subjects after normalization to TEA. The relationship of the eminences on the lateral and medial condyles to the patellar groove was clear in the present study. These results show definite differences between genders in the Asian population.
A number of previous studies attempted to obtain morphometric measurements of the knee joint and determine whether any differences exist between races [22, 35] or genders [2, 7, 8, 21, 22]. Li et al. [22] compared morphological data between Chinese and Caucasian subjects and found that for both groups the ratio of AP to ML dimensions of the femur was smaller in females than in males (1.22 ± 0.05 vs. 1.29 ± 0.04; p < 0.05 and 1.18 ± 0.05 vs. 1.25 ± 0.05; p < 0.05, respectively). Another study [35] found that Chinese subjects had a lower AP:ML ratio for the knee joint than Caucasian subjects. The abovementioned studies recommended the development of gender- and race-specific knee prostheses to improve patient satisfaction and clinical outcomes.
Regarding morphological comparisons between the genders, most previous studies [7, 22, 36] reported that the absolute AP and ML dimensions of the femur are larger in males than in females and that the femoral shape in males is also different from that in females, as determined by an analysis of the aspect ratio. Following on from this, other studies further measured the detailed contours of the anterior condyle [4, 15, 20, 34]. Koh et al. [20] recorded the trochlear morphology of Korean subjects to analyze differences between the genders using 3D MRI reconstructions of the femoral trochlea. The authors indicated that there were significant differences between the female and male subjects regarding the sulcus angle and condylar height, with the former having a larger sulcus angle and lower condylar heights on both sides (p < 0.01). However, the factor of normalization was not considered in that study. The aspect ratio was calculated to determine whether patient size affects the dimensions of the anterior condyle. A significant difference (p = 0.001) was found between the genders regarding the medial condylar height, with an average difference of 1.1 mm, while there were no significant difference between the genders regarding the lateral condylar height and condylar aspect ratio. These results demonstrated that the anatomy of the anterior condylar is highly variable regardless of gender and that the aspect ratio seems to negate any difference between genders. These findings were partly consistent with those of our current study regarding anterior condylar height (Fig. 3). Furthermore, the present study also found significant differences between the genders for medial condylar height (p = 0.001), but no significant difference was noted in femoral size after normalization. Most studies of the anterior condyle mainly focused on morphometric data for the anterior condylar height and sulcus angle [7, 8, 16, 21], but other important dimensions such as condylar width were often not considered. The relationship between the anterior condylar height and trochlear width could strongly affect the geometry of the trochlear groove and the stability of patellar tracking. Therefore, this study further investigated the width of the anterior condylar to clearly understand the anterior condyle morphology.
In the present study, a significant difference in condylar width was noted in the range of − 20° to 0° for the lateral condyle (Fig. 4b, Table 3) and in the range of 10° to 20° for the medial condyle. More importantly, the female subjects had a larger value of normalized data than the male subjects, particularly for the lateral condyle. The ratio of the females’ lateral femoral trochlear width was approximately 7.9% higher than that of the males. This finding of a smaller height and a wider angle of the groove indicates that the anterior trochlear groove is shallower in the ML direction in females than in males. This observation could help explain why females have a higher incidence of patellar instability-related complications, such as lateral tilting and lateral subluxation [4, 30].
Complications following TKA are often related to misalignment or failure of the patellofemoral (PF) joint. Given that the trochlear groove guides the patella throughout knee motion, its geometry plays a key role in patellar tracking and associated complications. This study measured the trajectory of the trochlear groove and sulcus angle at 10° increments. The results showed that the trochlear groove trajectory goes from lateral to medial and then backtracks to lateral, indicating a turning point in the trochlear groove tracking. This finding is consistent with a study by Barink et al. [1], demonstrating that the nature of the trochlea is best described as bilinear. However, differences between genders regarding the curvature of the trochlear groove has not been investigated previously. The present study found that the change in curvature was slightly different between males and females (Fig. 5). The turning point for males occurred at approximately − 10°, whereas it occurred later at − 20° for females. This indicates that the trend of patellar tracking in the ML direction is steeper for males than for females. However, no significant difference in the trajectory was found between the genders. Regarding the sulcus angle, female subjects have greater angles than the males in the range of − 10° to − 30°. The mean sulcus angle of the female subjects appeared to be approximately 5.2° greater than that of the male subjects (p = 0.034), which is close to the Merchant view. Using the 3D reconstructed knee model, details of the anterior flange and trochlear groove could be easily observed to determine any differences between the genders.
The shape of the trochlear contour in current knee prostheses is quite different from the anatomical contour [12]. It has been demonstrated that an inappropriate curvature and geometry of the trochlear design may cause patellar catching and maltracking or abnormal pressure distribution [9, 33]. Many prosthesis designs have a lateral orientation of the trochlear groove, whereas others have a symmetrical design in the ML direction. However, no knee prostheses have accounted for the natural trochlear groove tracking a bilinear path, even though some manufacturers claim that their prostheses offer a design close to the anatomical shape. Regarding gender-specific designs, some manufacturers have introduced a thinner anterior flange and a larger lateral orientation angle for female patients [32, 37]. Such gender-specific prostheses can reduce the chance of femoral component overhangs. The clinical results of gender-specific designs vary in the Western population and do not seem to produce satisfactory results to support the benefits of female-specific knee prostheses [8, 10, 27]. It has also been reported that females have a narrower femoral condyle than males and that Caucasian males have a narrower femoral condyle than Chinese males [22]. The trend of measurements obtained in the above study was similar to that in this current study, but the measurements obtained in this study were smaller (Fig. 6). We assumed that the thinner anterior flange in gender-specific knee prostheses could be beneficial for Asian females due to their smaller femoral size [7, 22, 36] and thinner patella compared with Caucasian females [18]. However, the reported clinical results remain insufficient to support the advantage of using gender-specific knee prostheses in Asian females.

Comparison between Chinese and Caucasians: a typical view comparing lateral anterior condylar height (LACH) and medial anterior condylar height (MACH) as well as gender differences in the anterior condylar geometry
Further biomechanical studies are required to investigate whether a conventional or gender-specific design offers superior kinematics and joint stability. Furthermore, there is controversy around whether patellar resurfacing is suitable if a different trochlear groove design is chosen. In our previous biomechanical study [14], we compared the stress/strain distribution on the PF joint with an anatomical V-shaped and dome-shaped femoral component. The stress distribution was highly affected by the femoral contour design, with the V-shaped trochlear groove reducing the compressive strain on the unresurfaced patella. Thus, we recommended that when resurfacing the patella, a femoral component with a dome-shaped design might reduce the strain on the remaining patellar bone. Another study evaluated the geometry of the anterior flange of a femoral component and found that the flange shape only affected the conformity of the PF joint when articulating with the native patella [23]. Thus, the authors suggested that a more anatomical design of the femoral component is preferable if the surgeon decides not to resurface the patella. As the morphology of the anterior condyle is complex, with major differences between individuals, there is still room for improvement in the design of the trochlear groove to achieve better results with total knee and partial PF replacements.
Some limitations of this study should be mentioned. First, this study analyzed a bone surface model of the knee, ignoring cartilage thickness. However, although the geometry of the cartilage surface is different from that of bone in the trochlea, the difference is small [15, 29]. Second, this study observed significant differences in the morphology of the distal femur between the genders, but further investigation is required to determine whether these differences have any clinical impact. Third, this study measured the PF geometry only in healthy knees, while knees with an abnormal anterior condylar geometry were not considered. Future investigations may consider analyzing both normal and abnormal/diseased joints. Despite the abovementioned limitations, we believe that the results of this study provide useful information regarding the detailed morphology of the anterior femoral condyle.
Conclusion
In this study, male subjects had greater condylar heights and widths than the female subjects. Although the trajectory of the trochlear groove varied greatly between individuals, the trochlear groove appeared to be wider and shallower in females than in males. These results provide information on the morphology of the anterior condyle and can be used for improving the design of the trochlear groove in knee prostheses.
References
Barink M, van de Groes S, Verdonschot N, de Waal MM (2003) The trochlea is bilinear and oriented medially. Clin Orthop Relat Res 411:288–295
Chang TW, Huang CH, McClean CJ, Lai YS, Lu YC, Cheng CK (2012) Morphometrical measurement of resected surface of medial and lateral proximal tibia for Chinese population. Knee Surg Sports Traumatol Arthrosc 20:1730–1735
Chantarapanich N, Sitthiseripratip K, Mahaisavariya B, Wongcumchang M, Siribodhi P (2011) 3D geometrical assessment of femoral curvature: a reverse engineering technique. J Med Assoc Thai 91:1377
Chen S, Du Z, Yan M, Yue B, Wang Y (2017) Morphological classification of the femoral trochlear groove based on a quantitative measurement of computed tomographic models. Knee Surg Sports Traumatol Arthrosc 25:3163–3170
Dejour D, Ntagiopoulos PG, Saffarini M (2014) Evidence of trochlear dysplasia in femoral component designs. Knee Surg Sports Traumatol Arthrosc 22:2599–2607
Du Z, Chen S, Yan M, Yue B, Zeng Y, Wang Y (2017) Do size, shape, and alignment parameters of the femoral condyle affect the trochlear groove tracking? A morphometric study based on 3D-computed tomography models in Chinese people. BMC Musculoskelet Disord 18:4
Fan L, Xu T, Li X, Zan P, Li G (2017) Morphologic features of the distal femur and tibia plateau in Southeastern Chinese population: a cross-sectional study. Medicine 96:e8524
Fehring TK, Odum SM, Hughes J, Springer BD, Beaver WB Jr (2009) Differences between the sexes in the anatomy of the anterior condyle of the knee. J Bone Jt Surg Am 91:2335–2341
Fitzpatrick CK, Baldwin MA, Ali AA, Laz PJ, Rullkoetter PJ (2011) Comparison of patellar bone strain in the natural and implanted knee during simulated deep flexion. J Orthop Res 29:232–239
Greene KA (2007) Gender-specific design in total knee arthroplasty. J Arthroplasty 22:27–31
Guy S, Farndon M, Sidhom S, Al-Lami M, Bennett C, London N (2012) Gender differences in distal femoral morphology and the role of gender specific implants in total knee replacement: a prospective clinical study. Knee 19:28–31
Heinert G, Kendoff D, Preiss S, Gehrke T, Sussmann P (2011) Patellofemoral kinematics in mobile-bearing and fixed-bearing posterior stabilised total knee replacements: a cadaveric study. Knee Surg Sports Traumatol Arthrosc 19:967–972
Hochreiter B, Hess S, Moser L, Hirschmann MT, Amsler F, Behrend H (2020) Healthy knees have a highly variable patellofemoral alignment: a systematic review. Knee Surg Sports Traumatol Arthrosc 28:398–406
Huang CH, Hsu LI, Chang TK, Chuang TY, Shih SL, Lu YC et al (2017) Stress distribution of the patellofemoral joint in the anatomic V-shape and curved dome-shape femoral component: a comparison of resurfaced and unresurfaced patellae. Knee Surg Sports Traumatol Arthrosc 25:263–271
Iranpour F, Merican AM, Dandachli W, Amis AA, Cobb JP (2010) The geometry of the trochlear groove. Clin Orthop Relat Res 468:782–788
Ishimaru M, Hino K, Onishi Y, Iseki Y, Mashima N, Miura H (2014) A three-dimensional computed tomography study of distal femoral morphology in Japanese patients: gender differences and component fit. Knee 21:1221–1224
Kim JM, Kim SB, Kim JM, Lee DH, Lee BS, Bin SI (2015) Results of gender-specific total knee arthroplasty: comparative study with traditional implant in female patients. Knee Surg Relat Res 27:17–23
Kim TK, Chung BJ, Kang YG, Chang CB, Seong SC (2009) Clinical implications of anthropometric patellar dimensions for TKA in Asians. Clin Orthop Relat Res 467:1007–1014
Koh YG, Nam JH, Chung HS, Kim HJ, Chun HJ, Kang KT (2019) Gender differences in morphology exist in posterior condylar offsets of the knee in Korean population. Knee Surg Sports Traumatol Arthrosc 27:1628–1634
Koh YG, Nam JH, Chung HS, Lee HY, Kim HJ, Kim HJ et al (2019) Gender-related morphological differences in sulcus angle and condylar height for the femoral trochlea using magnetic resonance imaging. Knee Surg Sports Traumatol Arthrosc 27:3560–3566
Li P, Tsai TY, Li JS, Wang S, Zhang Y, Kwon YM et al (2014) Gender analysis of the anterior femoral condyle geometry of the knee. Knee 21:529–533
Li P, Tsai TY, Li JS, Zhang Y, Kwon YM, Rubash HE et al (2014) Morphological measurement of the knee: race and sex effects. Acta Orthop Belg 80:260–268
Ma HM, Lu YC, Kwok TG, Ho FY, Huang CY, Huang CH (2007) The effect of the design of the femoral component on the conformity of the patellofemoral joint in total knee replacement. J Bone Jt Surg Br 89:408–412
Mahaisavariya B, Saekee B, Sitthiseripratip K, Oris P, Tongdee T, Bohez E et al (2004) Morphology of the radial head: a reverse engineering based evaluation using three-dimensional anatomical data of radial bone. Proc Inst Mech Eng H 218:79–84
Mahaisavariya B, Sitthiseripratip K, Tongdee T, Bohez EL, Vander Sloten J, Oris P (2002) Morphological study of the proximal femur: a new method of geometrical assessment using 3-dimensional reverse engineering. Med Eng Phys 24:617–622
Mahfouz M, Fatah EEA, Bowers LS, Scuderi G (2012) Three-dimensional morphology of the knee reveals ethnic differences. Clin Orthop Relat Res 470:172–185
Merchant AC, Arendt EA, Dye SF, Fredericson M, Grelsamer RP, Leadbetter WB et al (2008) The female knee: anatomic variations and the female-specific total knee design. Clin Orthop Relat Res 466:3059–3065
Pinskerova V, Nemec K, Landor I (2014) Gender differences in the morphology of the trochlea and the distal femur. Knee Surg Sports Traumatol Arthrosc 22:2342–2349
Schoettle PB, Zanetti M, Seifert B, Pfirrmann CW, Fucentese SF, Romero J (2006) The tibial tuberosity–trochlear groove distance; a comparative study between CT and MRI scanning. Knee 13:26–31
Smith RM, Boden BP, Sheehan FT (2018) Increased patellar volume/width and decreased femoral trochlear width are associated with adolescent patellofemoral pain. Clin Orthop Relat Res 476:2334–2343
Smith TO, Hunt NJ, Donell ST (2008) The reliability and validity of the Q-angle: a systematic review. Knee Surg Sports Traumatol Arthrosc 16:1068–1079
Tanavalee A, Rojpornpradit T, Khumrak S, Ngarmukos S (2011) The early results of gender-specific total knee arthroplasty in Thai patients. Knee 18:483–487
Wang J, Yue B, Wang Y, Yan M, Zeng Y (2012) The 3D analysis of the sagittal curvature of the femoral trochlea in the Chinese population. Knee Surg Sports Traumatol Arthrosc 20:957–963
Yan M, Wang J, Wang Y, Zhang J, Yue B, Zeng Y (2014) Gender-based differences in the dimensions of the femoral trochlea and condyles in the Chinese population: correlation to the risk of femoral component overhang. Knee 21:252–256
Yue B, Varadarajan KM, Ai S, Tang T, Rubash HE, Li G (2011) Differences of knee anthropometry between Chinese and white men and women. J Arthroplasty 26:124–130
Yue B, Varadarajan KM, Ai S, Tang T, Rubash HE, Li G (2011) Gender differences in the knees of Chinese population. Knee Surg Sports traumatol Arthrosc 19:80–88
Yue B, Wang J, Wang Y, Yan M, Zhang J, Zeng Y (2014) How the gender or morphological specific TKA prosthesis improves the component fit in the Chinese population? J Arthroplasty 29:71–74
Acknowledgements
The authors particularly thank Colin J. McClean for his kind assistance in language editing and proofreading this manuscript.
Funding
The authors are pleased to acknowledge the financial support of the Ministry of Science and Technology in Taiwan (MOST 105-2221-E-195-001) and a supporting grant from MMH and NTUST (MMH-NTUST-106-02).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors report no conflicts of interest in this work.
Ethical approval
The study was approved by the Institutional Review Board of SCMH (IRB number: 1021004).
Informed consent
Informed consent was obtained from all enrolled subjects.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hsu, CP., Lee, PY., Wei, HW. et al. Gender differences in femoral trochlea morphology. Knee Surg Sports Traumatol Arthrosc 29, 563–572 (2021). https://doi.org/10.1007/s00167-020-05944-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-020-05944-3