
Abstract
Purpose
An unnatural design of the sagittal geometry of the femoral trochlea may cause abnormal patellofemoral kinematics and complications after knee arthroplasty. Most previous studies examined the sagittal curvature of the femoral trochlea on 2D parasagittal planes, which may not represent the true sagittal curvature of the complex 3D femoral trochlea.
Methods
The current study evaluated the sagittal geometry of the femoral trochlea of 100 healthy Chinese subjects (50 women and 50 men) with 3D analysis. A close-fit sphere was generated on the surface of the medial and lateral trochlear articular surface, respectively. The radii of the spheres represented the sagittal radii of the femoral trochlear sagittal curvature. A cylinder was then established and its radius was adjusted to allow the deepest points of the curved trochlear groove touching the cylindrical surface. The radius of the cylinder represented the sagittal radius of the trochlear groove.
Results
In the men, the average radii of the curvature of the femoral trochlea were 18.8 ± 2.5 mm and 25.5 ± 2.8 mm for the medial and lateral femoral trochleas, respectively. In the women, the average radii of the curvature of the femoral trochlea were 20.2 ± 3.0 mm and 26.6 ± 2.7 mm for the medial and lateral femoral trochleas, respectively. The average radius of the cylinder of the trochlea groove was 19.6 ± 2.0 mm with a circular arc of 123.2° ± 13.0° in the men. In the women, the radius was 20.2 ± 1.7 mm with a circular arc of 127.9° ± 11.7°.
Conclusion
The present study provided a reliable and consistent assessment of the sagittal geometry of the femoral trochlea in the Chinese population. The results of the current study may be helpful to improve the understanding of the knee kinematics and develop the physiological knee prostheses.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The abnormal patellofemoral kinematics and complications after knee arthroplasty have been attributed in part to the unnatural design of the sagittal geometry of the femoral trochlea [2, 7, 24]. For instance, Heinert et al. [11] found that the sagittal radius of the trochlear groove of some total knee arthroplasty (TKA) component was 40 ± 6 mm, significantly larger than the 23 ± 2 mm measured in the natural knees. The design of the femoral trochlea is the main determinant of the patellofemoral outcome in the TKA [14, 15, 20], and an inappropriate radius of the curvature of the femoral component design may cause patellar catching, maltracking, or abnormal pressure distributions [9, 17], particularly when the natural patella is retained during the TKA [11].
Many studies have investigated the geometry of the femoral trochlea; however, the majority of them focused on the depth and orientation of the trochlear groove in the transverse or coronal plane [1]. A few studies evaluated the sagittal curvature of the femoral trochlea with the projected images of the trochlea on to the parasagittal planes [26], or the parasagittal sections of the human knees [21]. However, the femoral trochlea is a complex 3-D structure and the measurements with the above methods depend on the measuring coordinate system and the direction of the slicing plane, resulting in great variability among the study results. For example, it has been widely recognized that the trochlear groove is bilinear in the coronal plane, with the distal half oriented 0.2° ± 2.8° laterally and the proximal half oriented 4.2° ± 3.2° medially relative to the mechanical axis of the femur [3], covering a width about 4% of the epicondylar width or around 3 mm in the mediolateral direction [3, 22]. Therefore, it seems impossible to measure the sagittal radius of the trochlear groove in a consistent way when using single circular arcs [24, 27], since slicing a cylinder at different oblique angles produces variable elliptic arcs [24].
The primary aim of the study was to define the sagittal geometry of the femoral trochlea based on 3-D analysis. It was hypothesized that the best-fit spheres could be made to match the articular surface of the medial and lateral trochlea, and a cylinder existed that allowed the whole path of the trochlear groove to spread on the cylindrical surface [12].
Materials and methods
One hundred healthy Chinese subjects (fifty men and fifty women) were recruited for this study after obtaining informed consent from the subjects and approval by the institutional review board. The median age was 44 (range, 33–56) years for the female subjects and 51 (range, 30–60) years for the male subjects. The median weight was 62 (range, 43–76) kg for the female subjects and 70 (range, 45–90) kg for the male subjects. The median height was 160 (range, 150–175) cm for the female subjects and 171 (range, 162–190) cm for the male subjects. Both knees of each subject were studied. All the knees included in this study were healthy and without any symptoms of soft tissue injuries or osteoarthritis. This was verified both via clinical examination and examination of CT images. Individuals with previous knee trauma, knee pain, and other chronic diseases of the musculoskeletal system were excluded from the study.
Creation of 3D knee model
Computed tomography scanning was performed for both femurs of each subject using a helical CT scanner (Light Speed 16, GE Medical System, USA). During the scan, the subject was supine with his or her knees in a relaxed and extended position. The scanning procedure was performed to acquire 0.625 mm CT slices (resolution 512 × 512 pixels) with a field of view of 360 × 360 mm around knee joint. The CT images were then imported into the Mimics10.01 medical imaging program (Materialise, Leuven, Belgium) for use in conducting 3-D reconstruction of the geometric pattern of the skeleton knee model [25].
Measurements of the sagittal curvature of the femoral trochlea
For the convenience of the study on the particular region of the femoral trochlea, the images of the patella and tibia were deleted in all the 3D knee models, leaving only the distal femur. The smooth osseous femoral trochlea, which started from the most anterior prominence of the femoral trochlea and end at the normal indentation where the anterior horn of the meniscus articulates with the femoral condyle at full knee extension [26], was clearly demonstrated (Fig. 1). A close-fit sphere was generated on the surface of the medial and lateral trochlear articular surface, respectively. The radius of the medial or lateral sphere represented the sagittal radius of the medial or lateral trochlear sagittal curvature, respectively. The line connecting the centers of the two spheres was defined as the trochlear axis (Fig. 2). The femur was then placed to make both the tangent line of the posterior femoral condyles and the anatomical axis of the femoral shaft to be horizontal. Then, the anteroposterior dimensions of the medial (MAP) and lateral (LAP) femoral condyles were measured, respectively (Fig. 2). The values of the sagittal radii of the medial and lateral femoral trochlea were normalized by the anteroposterior dimension of the medial and lateral femoral condyles, respectively.

The region of the femoral trochlea was defined on the 3D model of the distal femur. A close-fit sphere was generated on the surface of the medial and lateral trochlear articular surface, respectively. The line connecting the centers of the two spheres was defined as the “trochlear axis”

The radius of the medial or lateral sphere represented the sagittal radius of the medial or lateral trochlear sagittal curvature, respectively. MAP/LAP medial/lateral anteroposterior dimension of the femoral condyle
Measurements of the sagittal curvature of the femoral trochlear groove
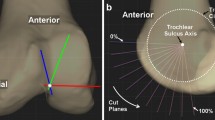
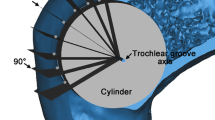
The curved path of the trochlear groove was defined by tracing the deepest points of the trochlear groove with the software (Fig. 3). A cylinder was then established with its axis (trochlear groove axis) parallel to the femoral trochlear axis (the line connecting the centers of the two best-fit spheres of the medial and lateral femoral trochlea), and its radius was adjusted to allow the deepest points of the trochlear groove touching the cylindrical surface (Fig. 3). The radius of the cylinder represented the sagittal radius of the trochlear groove. The values of the radii were normalized by the anteroposterior dimension of the lateral femoral condyle.

The measurements of the sagittal curvature of the trochlear groove. a The curved path of the trochlear groove was defined by tracing the deepest points of the trochlear groove. A cylinder was established with its axis (trochlear groove axis) parallel to the femoral trochlear axis, and its radius was adjusted to allow the deepest points of the trochlear groove touching the cylindrical surface. The radius of the cylinder represented the sagittal radius of the trochlear groove. (“Femoral trochlear axis” is the line connecting the centers of the best-fit spheres of the medial and lateral femoral trochlea. “Trochlear groove axis” is the axis of the best-fit cylinder of the trochlear groove). b The medial femoral condyle was resected to show the trochlear groove and the best-fit cylinder. The arc angle of the trochlear groove was also showed
Two coronal planes, which contained the most proximal and the most distal points of the trochlear groove, respectively, were made around the trochlear groove axis. The sector angle between the two planes represented the arc angle of the trochlear groove.
All of the measurements were finished by one surgeon to eliminate the interobserver bias. To assess the repeatability of the measurements, each parameter was measured three times in one randomly selected femur. The standard deviation of the three measuring trials was determined and used to represent the repeatability of the measurement.
Statistical analysis
A Student’s t test was performed to determine if the sagittal curvature of the femoral trochlea was statistically different between the women and men, and between the medial and lateral sides. The differences of average age, weight, and height between the men and women were also analyzed with Student’s t test. A P value of less than 0.05 was considered to indicate statistical difference. Best-fit lines representing the relationship between the anteroposterior dimension of the femoral condyle and the sagittal curvature of the femoral trochlea were calculated using least-squares regression.
Results
The differences of average age, weight, and height between the men and women were all significantly different by Student’s t test (P < 0.01).
In the men, the radii of the curvature of the femoral trochlea were 18.8 ± 2.5 and 25.5 ± 2.8 mm for the medial and lateral femoral trochleas, respectively (Table 1). In the women, the radii of the curvature of the femoral trochlea were 20.2 ± 3.0 and 26.6 ± 2.7 mm for the medial and lateral femoral trochleas, respectively (Table 1). In both the men and women, the differences between the medial and lateral femoral trochleas were statistically significant before and after normalization by the anteroposterior dimensions of the medial and lateral femoral condyles, respectively (P < 0.01) (Table 1). Additionally, the radii of the curvature of the medial and lateral femoral trochleas of the women were statistically significant larger than those of the men before and after normalization by the anteroposterior dimensions of the femoral condyles (P < 0.01) (Table 1). However, the morphological data showed a progressive decline in the sagittal radii of the femoral trochlea with increasing anteroposterior dimensions of the femoral condyles in both genders (Fig. 4). The lines representing the change in the sagittal radii of the femoral trochlea with increasing anteroposterior dimensions of the femoral condyles for the women and men were nearly coincident. Therefore, the differences in the sagittal radii of the femoral trochlea between the genders may be caused by the fact that the average femoral size of the women was generally smaller than that of the men.

The morphological data showed a progressive decline in the sagittal radii of the femoral trochlea with increasing anteroposterior dimensions of the femoral condyles in both genders. The lines representing the change in the sagittal radii of the femoral trochlea with increasing anteroposterior dimensions of the femoral condyles for the women and men were nearly coincident
The radius of the cylinder of the trochlea groove was 19.6 ± 2.0 mm with a circular arc of 123.2° ± 13.0° in the men. In the women, the radius was 20.2 ± 1.7 mm with a circular arc of 127.9° ± 11.7°. The difference of the sagittal radius of the trochlear groove was statistically significant between the men and women before and after normalization by the anteroposterior dimension of the lateral femoral condyle (P < 0.05). However, this difference was also caused by the differences of femoral sizes between the women and men (Fig. 5). The difference of the circular arc angle of the trochlear groove between the men and women was statistically significant (P < 0.05) (Table 2).

The morphological data showed a progressive decline in the radii of the femoral trochlear grooves with increasing anteroposterior dimensions of the femoral lateral condyles in both genders. The lines representing the change in the radii of the femoral trochlear grooves with increasing anteroposterior dimensions of the femoral lateral condyles for the women and men were nearly coincident
The repeatability of the measurements was 0.2 and 0.2 mm for the sagittal radii of the medial and lateral femoral trochleas, respectively; 0.3 and 0.3 mm for the anteroposterior dimensions of the medial and lateral femoral condyles, respectively; 0.3 mm for the femoral groove radius and 0.4° for the femoral groove arc angle.
Discussion
The most important findings of the present study were that the sagittal articular curvature of the femoral trochlea could be appropriately described by the best-fit spheres for the medial/lateral trochlea, and a cylinder existed that allowed the curved path of the trochlear groove to spread on the cylindrical surface.
The previous studies usually measured the sagittal profiles of the femoral trochlea with the projected contours of the trochlea on to the parasagittal planes [26], or the parasagittal sections of the human knees [21]. However, the shape of the distal femur was trapezoidal with the medial and lateral femoral condyles running obliquely and converging anteriorly to form the trochlea [6, 16]. The measurements based on the 2D images depend on the measuring coordinate system or the direction of the slicing plane. Our previous study measured the sagittal curvature of the trochlea in the 2D parasagittal plane which was perpendicular to the femoral transepicondylar axis. The results showed that the radii of the curvature for the medial and lateral trochlea of the Chinese men were 18.1 ± 3.3 and 28.3 ± 1.9 mm, respectively, and 14.5 ± 2.9 and 24.9 ± 2.1 mm for the medial and lateral trochlea in the Chinese women, respectively. After standardization by the anteroposterior dimension of the lateral femoral condyle, the radius of the medial trochlea of the men was significantly larger than that of the women [26]. Siu et al. [24] reported that for a nominally sized distal femur of 85 mm in mediolateral and 73 mm in anteroposterior dimensions, the radius of curvature for the medial and lateral femoral trochlea was 27.8 and 24.0 mm, respectively. The current study used best-fit spheres to describe the articular shape of the trochlea, showing that the radii of the curvature of the femoral trochlea in the men were 18.8 ± 2.5 and 25.5 ± 2.8 mm for the medial and lateral trochlea, respectively, and were 20.2 ± 3.0 and 26.6 ± 2.7 mm for the medial and lateral trochleas in the women, respectively. Similar to the method used in the current study, Zoghi et al. [27] showed that the lateral trochlea could be approximated to a cylinder with an average radius of 26 mm, but they only examined four cadaveric human knees. Iranpour et al. [13] used best-fit spheres to describe the distal femoral condyles. The differences among the studies may be due to the variations in the reference axis, measuring method, the racial differences in the distal femoral shape, and the different sample sizes. An inappropriate radius of curvature design may cause patellar catching, maltracking, or abnormal pressure distributions and contact locations in the patellofemoral arthroplasty or TKA [9, 17], particularly when the natural patella is retained during the surgery [11].
The present study also confirmed that the radii of the lateral femoral trochlea were significantly larger than that of the medial trochlea in both the men and women, which seemed to be a reasonable arrangement. During knee flexion, the resultant force vector from the quadriceps muscle and the patellar tendon, combined a force component caused by the Q angle, tend to pull the patella posteriorly and laterally. Theoretically, a larger radius of the articular surface of the lateral trochlea would allow greater patellofemoral contact area and more smooth patellofemoral tracking during the knee flexion [1, 19].
Lots of studies have reported the depth and orientation of the trochlear groove in the transverse or coronal plane [1]. Only a few studies evaluated the sagittal geometry of the femoral trochlear groove [8, 24]. Iranpour et al. [13] found that the trochlear groove could be fitted accurately to a simple circle, which had an average radius of 23 ± 4 mm (range, 16–34 mm). The same authors also found that the path of the center of the patella was circular after the patella engaged with the trochlear groove, and the radius of the circle fitted to the center of the patella was 44 ± 2.9 mm [12]. Elias et al. [8] examined the distal femur roentgenographically in the lateral plane, reporting that the radii of the patellar groove averaged 24 mm with the arc angle of 90 degrees. Zoghi et al. [27] examined four cadaveric human distal femurs, showed that the intertrochlear portion could be modeled using an oblique cylinder with an average radius of 22 ± 4 mm. The current study also found that a cylinder could be made to allow the whole path of the curved trochlear groove to spread on the cylindrical surface, and the radii of the cylinders averaged 19.6 ± 2.0 and 20.2 ± 1.7 mm for the men and women, respectively. The differences among the results may be due to the different measuring method used, the racial differences in femoral geometry, and the different sample sizes. Most of the modern knee prostheses had constant radius sagittally on the trochlear surface, which is believed to allow a larger patellofemoral contact area and therefore avoid excessive contact pressures during knee flexion [4, 10, 18].
The current study had several limitations. Firstly, we evaluated healthy knees, while in clinical circumstances the anatomy of the femoral trochlea in patients with knee osteoarthritis may have greatly degenerated due to the disease progression. Another limitation was that the CT scanned images were used to construct the 3D distal femur, which did not contain the cartilaginous surfaces. Although some studies have shown the geometry of the cartilage surface differed from that of the bone in the trochlea, the difference was small [13]. Thirdly, though the anatomical prosthesis design of the femoral trochlea help to restore the natural patellar tracking, the actual circularity of the patellar path may be altered by variations on the patellar side such as with/without resurfacing, overstuffing, or understuffing of the joint [12]. The information of the 3D architecture of the distal femur was relevant for the design of the femoral component of total or partial knee prosthesis to work toward an “anatomical” knee for replicating the natural kinematics [5, 23].
Conclusion
The present study provided a reliable and consistent assessment of the sagittal geometry of the femoral trochlea in the Chinese population. The results of the current study may be helpful to improve the understanding of the knee kinematics and develop the physiological knee prostheses.
References
Amis AA (2007) Current concepts on anatomy and biomechanics of patellar stability. Sports Med Arthrosc 15:48–56
Baldini A, Anderson JA, Cerulli-Mariani P, Kalyvas J, Pavlov H, Sculco TP (2007) Patellofemoral evaluation after total knee arthroplasty. Validation of a new weight-bearing axial radiographic view. J Bone Jt Surg Am 89:1810–1817
Barink M, van de Groes S, Verdonschot N, de Waal Malefijt M (2003) The trochlea is bilinear and oriented medially. Clin Orthop Relat Res 411:288–295
Buechel FF, Pappas MJ, Makris G (1991) Evaluation of contact stress in metal-backed patellar replacements. A predictor of survivorship. Clin Orthop Relat Res 273:190–197
Cheng FB, Ji XF, Zheng WX, Lai Y, Cheng KL, Feng JC, Li YQ (2010) Use of anthropometric data from the medial tibial and femoral condyles to design unicondylar knee prostheses in the Chinese population. Knee Surg Sports Traumatol Arthrosc 18:352–358
Conley S, Rosenberg A, Crowninshield R (2007) The female knee: anatomic variations. J Am Acad Orthop Surg 15(Suppl 1):S31–S36
D’Lima DD, Chen PC, Kester MA, Colwell CW Jr (2003) Impact of patellofemoral design on patellofemoral forces and polyethylene stresses. J Bone Jt Surg Am 85-A(Suppl 4):85–93
Elias SG, Freeman MA, Gokcay EI (1990) A correlative study of the geometry and anatomy of the distal femur. Clin Orthop Relat Res 260:98–103
Fitzpatrick CK, Baldwin MA, Ali AA, Laz PJ, Rullkoetter PJ (2011) Comparison of patellar bone strain in the natural and implanted knee during simulated deep flexion. J Orthop Res 29:232–239
Freeman MA, Samuelson KM, Elias SG, Mariorenzi LJ, Gokcay EI, Tuke M (1989) The patellofemoral joint in total knee prostheses. Design considerations. J Arthroplast 4(Suppl):S69–S74
Heinert G, Kendoff D, Preiss S, Gehrke T, Sussmann P (2011) Patellofemoral kinematics in mobile-bearing and fixed-bearing posterior stabilised total knee replacements: a cadaveric study. Knee Surg Sports Traumatol Arthrosc 19:567–572
Iranpour F, Merican AM, Baena FR, Cobb JP, Amis AA (2010) Patellofemoral joint kinematics: the circular path of the patella around the trochlear axis. J Orthop Res 28:589–594
Iranpour F, Merican AM, Dandachli W, Amis AA, Cobb JP (2010) The geometry of the trochlear groove. Clin Orthop Relat Res 468:782–788
Keblish PA, Varma AK, Greenwald AS (1994) Patellar resurfacing or retention in total knee arthroplasty. A prospective study of patients with bilateral replacements. J Bone Jt Surg Br 76:930–937
Kulkarni SK, Freeman MA, Poal-Manresa JC, Asencio JI, Rodriguez JJ (2001) The patello-femoral joint in total knee arthroplasty: is the design of the trochlea the critical factor? Knee Surg Sports Traumatol Arthrosc 9(Suppl 1):S8–S12
Kwak SD, Colman WW, Ateshian GA, Grelsamer RP, Henry JH, Mow VC (1997) Anatomy of the human patellofemoral joint articular cartilage: surface curvature analysis. J Orthop Res 15:468–472
Lonner JH (2007) Patellofemoral arthroplasty. J Am Acad Orthop Surg 15:495–506
Moreland JR, Thomas RJ, Freeman MA (1979) ICLH replacement of the knee: 1977 and 1978. Clin Orthop Relat Res 145:47–59
Moro-oka T, Matsuda S, Miura H, Nagamine R, Urabe K, Kawano T, Higaki H, Iwamoto Y (2002) Patellar tracking and patellofemoral geometry in deep knee flexion. Clin Orthop Relat Res 394:161–168
Muller W, Wirz D (2001) The patella in total knee replacement: does it matter? 750 LCS total knee replacements without resurfacing of the patella. Knee Surg Sports Traumatol Arthrosc 9(Suppl 1):S24–S26
O’Connor JJ, Shercliff TL, Biden E, Goodfellow JW (1989) The geometry of the knee in the sagittal plane. Proc Inst Mech Eng H 203:223–233
Shih YF, Bull AM, Amis AA (2004) The cartilaginous and osseous geometry of the femoral trochlear groove. Knee Surg Sports Traumatol Arthrosc 12:300–306
Siebold R, Axe J, Irrgang JJ, Li K, Tashman S, Fu FH (2010) A computerized analysis of femoral condyle radii in ACL intact and contralateral ACL reconstructed knees using 3D CT. Knee Surg Sports Traumatol Arthrosc 18:26–31
Siu D, Rudan J, Wevers HW, Griffiths P (1996) Femoral articular shape and geometry. A three-dimensional computerized analysis of the knee. J Arthroplast 11:166–173
Yue B, Varadarajan KM, Ai S, Tang T, Rubash HE, Li G (2011) Differences of knee anthropometry between Chinese and white men and women. J Arthroplast 26:124–130
Yue B, Varadarajan KM, Ai S, Tang T, Rubash HE, Li G (2011) Gender differences in the knees of Chinese population. Knee Surg Sports Traumatol Arthrosc 19:80–88
Zoghi M, Hefzy MS, Fu KC, Jackson WT (1992) A three-dimensional morphometrical study of the distal human femur. Proc Inst Mech Eng H 206:147–157
Acknowledgments
This study was supported by the Fund of Science and Technology Commission of Shanghai (09441900104/11QA1404100), Fund for Key Disciplines of Shanghai Municipal Education Commission (J50206), and National Natural Science Foundation of China (30901517).
Author information
Authors and Affiliations
Corresponding author
Additional information
Jun Wang and Bing Yue are the co-first authors.
Rights and permissions
About this article
Cite this article
Wang, J., Yue, B., Wang, Y. et al. The 3D analysis of the sagittal curvature of the femoral trochlea in the Chinese population. Knee Surg Sports Traumatol Arthrosc 20, 957–963 (2012). https://doi.org/10.1007/s00167-011-1679-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-011-1679-6