
Abstract
Background
Racial concordance between patients and clinician has been linked to improved satisfaction and patient outcomes.
Objectives
(1) To examine the likelihood of clinician-patient racial concordance in non-Hispanic White, non-Hispanic Black, Asian, and Hispanic patients and (2) to evaluate the impact of patient-clinician race concordance on healthcare use and expenditures within each racial ethnic group.
Methods
We analyzed data from the 2010–2016 Medical Expenditure Panel Survey (MEPS). We used bivariate and multivariate models to assess the association between patient-clinician race concordance and emergency department (ED) use, hospitalizations, and total healthcare expenses, controlling for patient socio-demographic factors, insurance coverage, health status, and survey year fixed effects.
Results
Of the 50,626 adults in the analysis sample, 32,350 had racial concordance with their clinician. Among Asian and Hispanic patients, low income, less education, and non-private insurance were associated with an increased likelihood of patient-clinician racial concordance. Emergency department use was lower among Whites and Hispanics with concordant clinicians compared to those without a discordant clinician (15.6% vs. 17.3%, p = 0.02 and 12.9% vs. 16.2%, p = 0.01 respectively). Total healthcare expenditures were lower among Black, Asian, and Hispanic patients with race-concordant clinicians than those with discordant clinicians (14%, 34%, and 20%, p < 0.001 respectively).
Conclusions
These results add to the body of evidence supporting the hypothesis that racial concordance contributes to a more effective therapeutic relationship and improved healthcare. These results emphasize the need for medical education surrounding cultural humility and the importance of diversifying the healthcare workforce.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Health disparities occur when avoidable social disadvantage contributes to worse health outcomes for the socially disadvantaged group [1]. Health disparities specific to race exist broadly throughout the USA [2,3,4,5]. Certain factors like socioeconomic status [6, 7], language proficiency barriers between patients and clinicians [8, 9], and health literacy [10, 11] are closely associated with race and provide partial explanations for these observed racial health disparities. However, these factors do not completely explain documented racial health disparities [3,4,5,6,7, 12, 13]. Racial health inequities often arise due to structural racism [14,15,16,17,18,19]. Within healthcare, structural racism can be mediated by clinicians’ false beliefs about biological differences between racial groups [20], differential treatment of patients [19], and unfamiliarity with tools (such as structural competency [21] and cultural humility [22]) they can employ to intervene in structural racism.
Examining the association of patient-clinician racial concordance on patient-clinician communication, patient satisfaction, and health outcomes may provide insight into the role that interpersonal dynamics play in the development of racial health disparities [23]. Concordance refers to a patient and clinician sharing a specific trait. It is well known that patients prefer racial concordance with their clinicians [24, 25], although it is less certain what effect racial concordance has on the actual delivery of healthcare and healthcare utilization. Most studies hypothesize that racial concordance is associated with improvements in communication, which facilitates improved adherence to treatment plans, deeper partnership formation between patients and clinicians, and ultimately better health outcomes [25].
In an experiment conducted in Oakland, California, Black men were more likely to accept preventive services, speak to a physician, and have more detailed documentation of their visits when seen by Black physicians. The authors estimated that, due to these differences, a larger number of Black physicians could reduce the Black-White gap in mortality due to heart disease by up to 19%.[26] In a recent observational study, patient-physician racial concordance was found to be associated with lower mortality for Black newborns [27].
Some suggest that the beneficial outcomes of racial concordance may be linked to acculturation. Studies have shown that preference for racial concordant clinician varies by the degree of acculturation [28]. Previous studies demonstrated Black, Hispanic, and Asian American patients were more likely to choose physicians from their own racial/ethnic group [29, 30]. Particularly this match between patient and provider race is more prominent among Hispanics and Asian Americans who recently immigrated to the US, not comfortable speaking English, and those adhering to traditional values of the country of origin [29, 30]. There is also evidence that demographic factors, and not necessarily patient choice or acculturation may be mediating patient-physician concordant relationships. Prior literature shows that factors such as low socioeconomic status, less education, and having non-private insurance may be associated with increased likelihood of patient-clinician racial concordance [31]. Conversely, socio-demographic factors associated with more access to healthcare like income greater than 400% FPL, private insurance, and higher education were associated with a decreased likelihood of patient-clinician racial discordance. One potential explanation is that patients with less exposure to the healthcare system and the greatest mistrust of the medical system have been shown to benefit the most from patient-clinician racial concordance [32]. Furthermore, clinicians from Hispanic, Black, and Native American backgrounds tend to practice in underserved areas at a higher rate than White clinicians [33], thereby increasing the probability of treating an underserved patient from the same race. This may be compounded by the disproportionately low number of underrepresented minority physicians in medicine overall [33], resulting in a disproportionately low number of minority physicians in more well-resourced areas where patients with higher income, more education, and private insurance may be seeking care. Structural racism may also limit minority clinicians’ access to working in more affluent, White communities as well as minority patients’ access to White clinicians and private health insurance.
In practice, patient-clinician racial concordance has been associated with improvements in patient-physician communication [23, 32, 34,35,36,37,38,39], greater time spent with physicians [18], improved shared decision-making [27], improved patient understanding of disease risk [20], improved medication adherence [34], decreased wait times for treatment [35], improved cancer screening [32, 36], improved cholesterol screening [37], and decreased implicit bias from clinicians [38]. Communication and health outcome differences between racially concordant and discordant patient-clinician dyads are not uniform, however large reviews have found a meaningful trend connecting racial concordance between patients and clinicians with improved communication23] and health outcomes [39]. Despite the known role of racial concordance on the patient-clinician relationship, it remains unknown whether racial concordance is associated with one key measure of high-quality healthcare: appropriate use of service and provision of appropriate care.
While there is little evidence showing race concordance is associated with expenditures, previous studies have shown that continuity of care and comprehensiveness, have been shown to reduce healthcare costs [40, 41]. A recent study by Ma et al. found patients having racial concordance were more likely to visit their USC clinician for preventive care, new health and ongoing medical problems [42]. Although USC is not a direct measure of comprehensiveness and continuity, having a USC is associated with four C types of care—first contact, continuity of care, comprehensive care, and care.
The primary purpose of this study is to examine use of health services—primary care visits, cancer screening services, emergency department (ED) use, hospitalizations, and healthcare expenditures across patients from different racial groups and with varying socio-demographic backgrounds to evaluate if having a racially concordant clinician impacts their healthcare use and expenditures. By comparing patients of the same racial group, our study seeks to better understand which specific socio-demographic factors are associated with an increased likelihood of having a racially concordant clinician.
Methods
We used 2010–2016 Medical Expenditure Panel Survey (MEPS) data. MEPS is administered by the Agency for Healthcare Research and Quality (AHRQ) and provides national estimates of healthcare use and expenditures of the civilian and non-institutionalized US population. Data are collected across five rounds extended over 2 years. Every year, a third of the respondents from the previous year’s National Health Interview Survey enters MEPS. Approximately 30,000–35,000 respondents are surveyed every year and the response rate varies from 58 to 66% [43]. Further details of the survey are described in detail elsewhere [44]. The study was exempted by the institutional review board of the American Academy of Family Physicians as it is based on secondary data analysis of deidentified publicly available MEPS data.
Study Sample
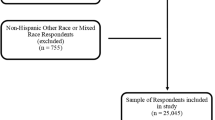
We pooled data from the 2010–2016 MEPS. We had 249,030 respondents in the original pooled sample. We included respondents who were in-scope for the survey during the entire two-year study period and had valid survey weights (n = 237,414) (Fig. 1). Since only respondents who reported having “a person” as their usual source of care (USC) or “a person in facility” as their USC were asked about the race of their clinician, we excluded those without a USC (n = 59,562), which reduced the sample to 177,762. We then excluded respondents with missing data for clinician race (n = 105,944). Next, we excluded respondents less than 18 years old, which reduced the sample to 52,494. Finally, we excluded those with missing data for education, census region of residence, health status, marital status chronic conditions, nativity status, and duration of stay in the USA yielding a final analysis sample of 50,626.

Flowchart-analysis sample, pooled medical expenditure panel survey data 2010-2016
Study Variables
We derived the variables from the MEPS consolidated and office-based files. The main explanatory variable was the racial concordance between the respondents and the physician.
Based on self-reported race, respondents in the sample were divided into four groups: non-Hispanic White, non-Hispanic Black, Hispanic, and Asian patients. We first identified the usual source of care clinician (person or person in a facility) for the individual respondent and determined the race of the physician as perceived by the respondents. Using the race of the respondent and the race/ethnicity of the physician we created a dichotomous measure of racial concordance. We coded “1” if the race of the physician was the same as the respondent (concordant) and “0” if it was different (discordant).
Response variables included healthcare use and healthcare spending. We created dichotomous measures of ED use and hospitalization, scoring each as “1” if the respondent had at least one ED visit or one hospitalization and as “0” otherwise. We also examined count data for number of primary care visits, ED use and hospitalizations. We looked at screening tests for cervical, breast and colorectal cancers with “1” indicating receipt of age and or gender appropriate screening service and “0” otherwise. Apart from the total healthcare expenditures, we also examined spending on ED, inpatient, office-based care, and prescription medications.
Covariates included age, gender, census region, education, income, insurance coverage, health status, number of chronic conditions, marital status, acculturation, English language proficiency and year fixed effects. We included age of the respondent as a continuous measure.. Based on the place of residence, we created four US Census regions: (1) South, (2) Northeast, (3) Midwest, and (4) West. We divided the sample into five groups based on the family income—(1) less than 100% federal poverty level (FPL), (2) 101–124% FPL, (3) 125–199% FPL, (4) 200–399% FPL, and (5) 400% FPL or greater.
We created three education categories—(1) less than high school, (2) completion of high school diploma or GED, and (3) greater than high school. Three types of insurance coverage were included—private, public, and uninsured. We created two health status categories, scoring the respondents reporting fair or poor health as “1” and good to excellent health as “0.” Based on the number of chronic conditions reported by the respondents, we classified them into 4 groups—(1) zero condition, (2) one condition, (3) two conditions, and (4) three or more conditions. Responses on marital status were collapsed to create a binary variable with “1” indicating married and “0” indicating not married. We combined responses on nativity status and length of stay in the USA to obtain acculturation measure. However, to avoid duplication of foreign-born status we created three categories for acculturation measure—(1) US born, (2) foreign-born with length of stay in the USA less than 10 years, and (3) foreign-born with length of stay in the USA for 10 years or more. Respondents speaking a language other than English at home were asked about how well they speak English. We combined the responses on language spoken at home and how well person speaks English to create three categories of limited English Proficiency with “0” indicating speaks English at home, “1” not comfortable speaking English and “2” comfortable speaking English.
Statistical Analysis
We used Stata 14.2 statistical software in analyzing the data [45]. All analyses were adjusted for MEPS complex sampling design [43].
We first created summary statistics for all the covariates and the outcomes for each of the racial groups by concordance. We assessed the significant differences between concordant and discordant groups within each of the racial groups using Chi-squared tests for categorical variables and t-tests for continuous variables. Finally, we ran multiple binary logistic regressions with and without controls to investigate the association between the patient-clinician racial concordance and healthcare use. We used Poisson regressions for count data on primary care visits, ED visits and hospitalizations. We performed GLM models using log link function and gamma distribution to examine the relationship between patient-clinician race concordance and healthcare expenses. We ran regressions separately for each of the health outcomes (healthcare service use, and healthcare expenses) within each of the four racial groups. We included acculturation and limited English proficiency measures in the models for non-Hispanic Asians and Hispanics.
Results
Table 1 presents demographic factors by racial concordance for each of the four race groups. Of the 50,626 adult patients in the analysis sample, 32,350 had racial concordance with their clinician). Of those patients, 72.8% were White, 6.5% were Black, 9.3% were Asian, and 11.4% were Hispanic. Our bivariate analysis demonstrated that the mean age of Asian and Hispanic respondents having a racially concordant clinician was greater than those who see a discordant clinician (50.9 vs. 48.2, p = 0.032 and 49.8 vs. 46.8, p < 0.001), respectively). In the White population, there was a higher proportion that had private insurance in the racially concordant group (78.1% vs. 72.6%, p < 0.001). In contrast, there was a higher proportion of public insurance status among Asian and Hispanic patients with racially concordant clinicians compared to the racially discordant dyads in these groups (26.9% vs. 15.7%, p < 0.001 and 34.7% vs. 25.0%, p < 0.001 respectively). Similarly, higher proportion of poor (< 200% FPL) Asian and Hispanic respondents had racially concordant clinicians than Asian and Hispanic respondents in the same income group that had discordant clinicians (26.0% vs. 17.3%, p = .0.02 and 43.9% vs. 30.9%, p < 0.001 respectively). Finally, there was a higher proportion of Asian and Hispanic patients with less than a high school education that had a concordant clinician than those with the same education level that had a discordant clinician (14.7% vs. 8.7%, p = 0.014 and 35.8% vs. 22.4%, p < 0.001 respectively).
In Table 2, we present distribution of outcomes across the race/ethnicity groups by racial concordance. The number of primary care visits was higher in the concordant group than the discordant group for Asian patients (1.9 vs. 1.5, p < 0.001) (Table 2). White patients with a race-concordant clinician had fewer primary care visits (1.9 vs. 2.3, < 0.001). ED usage was lower among White and Hispanic patients with concordant clinicians compared to those in the same racial group without a concordant clinician (15.6% vs. 17.3%, p = 0.016 and 12.9% vs. 16.2%, p = 0.014 respectively). Number of ED visits were lower among Hispanic respondents with concordant clinician than those with discordant clinician (0.17 vs. 0.23, p < 0.05).
Supplementary content (SC) Table 1 presents regression results examining factors (socio-demographic, nativity status, length of stay in the US, English speaking proficiency, poor health and number of chronic conditions) associated with racial concordance. Non-Hispanic White patients who were publicly insured and those with poor health status had lower odds of having racial/ethnic concordance. The likelihood of having patient-clinician racial concordance among non-Hispanic Black respondents was lower for those living in Northeast (odds ratio (OR) 0.73, confidence interval (CI) (0.56–0.95) and West (OR 0.38, CI 0.23–0.60) and higher for those who were foreign-born with length of stay in the USA of < 10 years.
Among non-Hispanic Asian patients, the odds of having a race-concordant clinician was higher for those living in West, who were uninsured, those who spoke English less well. Hispanics who had less than high school education, publicly insured or uninsured, poor health status, were foreign-born (irrespective of the duration of stay in the US), and those who did and did not speak English well were more likely to see a race-concordant clinician. Whereas females, those with residence in regions in other than South, and were not poor had lower odds of having racial concordance.
Table 3 (SC Table 2) summarizes regression results related to ED visit. Asian patients who saw race-concordant physicians had 0.71 times the odds of an ED visit than those who saw discordant physicians after controlling for socio-demographic and other factors (OR 0.71, 95% CI 0.52–0.93) (Table 3) Hispanic patients who saw a race-concordant physician had 0.75 times the odds of an ED visit compared to those who saw a discordant physician (OR 0.75, 95% CI 0.61–0.93). No statistically significant association between ED visits and racial concordance was found in non-Hispanic Whites and non-Hispanic Blacks. However, Poisson regression analysis showed Hispanic patients with racially concordant clinicians had 22% lower number of ED visits compared to Hispanic patients who had a discordant provider (incidence risk ratio (IRR) 0.78, 95% CI 0.64–0.94) (SC Table 3).
Hispanic patients seeing race-concordant clinicians had lower number of hospitalizations than those seeing discordant clinicians (IRR 0.76, (0.61–0.95) (SC Table 4).
SC Table 5 shows that there are no associations between receipt of cancer screening tests and racial concordance. However, odds of being screened for breast cancer were higher among women of all racial groups when they saw a gender concordant clinician. Non-Hispanic White women had 1.3 times and Hispanic women had 1.4 times the odds of receiving cervical cancer screening if seen by a female clinician. Similarly, non-Hispanic Black patients had higher odds of receiving colorectal cancer screening from gender concordant providers.
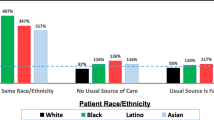
Figure 2 (Table 4, SC Table 6) illustrates that the total healthcare expenditures were lower among Black, Asian, and Hispanic respondents with race-concordant clinicians than those with discordant clinicians (14%, 34%, and 20%, p < 0.001 respectively). Additionally, Asian and Hispanic patients with a race-concordant clinician showed lower expenditures for office-based care than those who had a discordant clinician (Fig. 3, Table 4, SC Table 7). Expenditures on inpatient care (39%, p < 0.001) (Table 4, SC Table 8) and prescriptions (38.0%, < 0.001) (Table 4, SC Table 9) were lower among Blacks seeing race-concordant clinicians compared to those seeing discordant clinicians

Adjusted mean total and office-based expenditures by race concordance within each racial/ethnic group, pooled MEPS (2010–2016).a Notes: NH, non-Hispanic; C, concordant; D, discordant. aAdjusted for gender, age, region, education, poverty, insurance coverage, poor health status, marital status, number of chronic conditions, nativity status, duration of stay in the USA, and survey year. ***p < 0.01, **p < 0.05

Adjusted mean prescription and inpatient expenditures by race concordance within each racial/ethnic group, pooled MEPS (2010–2016).a Notes: NH, non-Hispanic; C, concordant; D, discordant. aAdjusted for gender, age, region, education, poverty, insurance coverage, poor health status, marital status, number of chronic conditions, English proficiency, nativity, duration of stay in the USA, and survey year. ***p < 0.01, **p < 0.05
Discussion
This cross-sectional study used MEPS data to identify socio-demographic characteristics that increase and decrease the probability of patients having a race-concordant provider. We also examined differences in healthcare utilization and total healthcare expenditures between patients of the same race with and without race-concordant clinicians.
Overall, our study findings are consistent with previous studies that showed minority populations were more likely to prefer or have a race-concordant clinician [29]. In particular Asians and Hispanics who were foreign-born, spoke English less fluently, and were publicly insured had increased likelihood of seeing a clinician of their own race. This study demonstrates that patient-clinician racial concordance for Asian, Hispanic, and Black patients is associated with lower ED use (Asian/Hispanic patients), lower rates of hospitalization (Hispanic patients), and lower total healthcare expenditures (Asian, Hispanic, and Black patients). However, having race-concordant clinician did not lead to increased use of services such as primary care visits, and receipt of screening tests for cervical, breast, and colorectal cancers. The combination of decreased ED visits, hospitalizations, and health expenditure observed for Hispanic patients with racial concordant clinicians suggests both appropriate healthcare delivery and appropriate healthcare utilization. Having established ongoing relationship with these racial concordant USC clinicians, particularly in minority populations, may have reduced healthcare expenditures. Many previous studies have shown that usual source of care and continuity with a clinician contribute to more appropriate utilization of healthcare services [46]. Whether this is due to greater disease prevention, improved disease management, improved patient counseling, or simply less healthcare utilization warrants future studies.
Interestingly, despite lower total health expenditures found in the non-Hispanic Black concordant dyads, there was no reduced odds of ED visits or hospitalizations for this concordant group compared to non-Hispanic Black respondents seen by race-discordant clinicians. While approximately 13% of Americans are Black [47], Black patients only made up 6.4% of patients in racially concordant patient-clinician dyads in our study. A larger sample size of Black patients and greater representation of older Black patients may have shown a statistically significant decrease in expenditure and ED use for Black patients in concordant dyads. This finding could also indicate a systematic difference between Black patients in concordant vs discordant dyads, such as higher medical complexity and burden of disease in the former. This difference could also be explained by disproportionate experiences of racism and barriers to accessing outpatient care for Black patients treated in underserved settings.
Future topics to explore include the following: (1) structural barriers uniquely experienced by Black patients in terms of receiving longitudinal care in outpatient settings; (2) potential protective factors uniquely experienced by Black patients receiving care in emergency departments; (3) Black patients’ interactions with appointment schedulers, front-desk staff, medical assistants, nurses, advanced practice clinicians, and physicians; and (4) disease severity and socio-demographic characteristics of Black patients seeking care in emergency departments. It is important to note that greater ED utilization and hospitalization may be indicated for some, regardless of the quality of outpatient care received. Future research can further examine the quality of care received and appropriateness of healthcare utilization in racially concordant and discordant patient-clinician dyads by comparing medical indications for treatment, timing of diagnoses, wait times for treatment, and actual health outcomes.
Our results add to a body of similar evidence supporting the initial hypothesis that improved communication from racial concordance leads to an improved and therefore more effective therapeutic relationship. A variety of overlapping explanations for a communication gap in discordant patient-clinician dyads has been presented in the literature. A leading theory points to limited English proficiency, especially among Hispanic and Latino patients seeing language discordant clinicians, which has been found to be associated with worse glycemic control9 and nonemergent ED usage [48]. While language mediates communication, it does not fully explain why a similar, yet statistically insignificant, association was seen in terms of ED use among Black and White patients in racially/ethnically concordant patient-clinician dyads.
The multivariate results for breast cancer screening tests were consistent with a recent study where patients with gender concordance had higher rates of cancer screenings [49]. There were no associations with racial concordance. Here the effect of racial concordance may be limited or less significant than gender concordance. In our study the effect of gender concordance was limited to the uptake of cervical cancer screening test in non-Hispanic White and Hispanic women and colorectal screening test in non-Hispanic Black patients. Although gender concordance plays a major role in uptake of breast and cervical cancer screening, the impact was not uniform across the racial/ethnic groups. Future studies may need to explore this with large sample sizes for Asian and non-Hispanic Black populations.
This study has a number of limitations. We cannot infer causal effects of racial concordance on healthcare use or expenditures, as our study is based on cross-sectional data and can report associations only. The MEPS data comes from a self-reported survey with limited external validation, introducing the possibility of bias in answers, particularly regarding clinician race and healthcare expenditures. Unreported healthcare costs were imputed based on local estimates, which introduces additional error into the healthcare expenditure values. As the clinicians’ race was based on patient’s perceptions, it may lead to misclassification of patient-clinician concordance. However, patients’ perceived clinician race may be as important of a mediator for our outcomes of interest as clinician self-identified race. Since only broad racial categories were used on the questionnaire, it may minimize this bias. The use of broad racial categories instead of disaggregated ethnic information, which was not available, to define concordance may underestimate the effect of patient-clinician concordance. Only those who had a USC clinician were included in the study, limiting the generalizability of the study findings to those without USC. The survey was distributed only to the non-institutionalized civilian population, limiting the ability to extrapolate results to separate health systems. Our analysis did not distinguish between nonemergent and emergent ED usage, limiting the ability to conclude that lower usage corresponds with more appropriate usage. Additionally, because minorities have decreased representation in the primary care workforce, minority patients have limited ability to choose a concordant clinician of their choice. It is impossible to infer preference on the part of the patient for a racially concordant or discordant clinician. Future qualitative or mixed-methods research may be conducted to further explore the role of patient preference for racially concordant or discordant clinicians.
Importantly, racial concordance provides a means for examining persistent racial/c disparities in healthcare only insofar as it is a useful stand-in for the explicit and implicit cultural characteristics that are closely associated with the social constructs of race and ethnicity. The inconsistent relationship in outcome shown here underscores the fact that differences in interaction with the healthcare system exist between racial groups and even within members of the same racial group. With this in mind, results reported here should be viewed as indicators for areas that need improvement within healthcare delivery and medical education regarding cultural understanding, communication training, and structural competency. Addressing these underlying contributory factors to racial health disparities will likely facilitate improvement in these disparities in the USA. To that end, we advocate improving access to medical professions for underrepresented minorities in medicine as well as expanding existing training in medical school and graduate medical education curricula on race, cultural humility, structural competency, and anti-racism. This training should take into consideration evidence-based techniques that have been shown to reduce the impact of bias, to decrease the degree of physician and patient self-categorization, and to promote a shared common identity between the patient and clinician [3].
Change history
24 February 2021
A Correction to this paper has been published: https://doi.org/10.1007/s40615-021-01003-w
References
Braveman P. Health disparities and health equity: concepts and measurement. Annu Rev Public Health. 2006;27(1):167–94. https://doi.org/10.1146/annurev.publhealth.27.021405.102103.
2016 National Healthcare Quality and Disparities Report. Rockville, MD: Agency for Healthcare Research and Quality; 2017.
Penner LA, Hagiwara N, Eggly S, Gaertner SL, Albrecht TL, Dovidio JF. Racial healthcare disparities: a social psychological analysis. Eur Rev Soc Psychol. 2013;24(1):70–122. https://doi.org/10.1080/10463283.2013.840973.
Saha S, Arbelaez JJ, Cooper LA. Patient–physician relationships and racial disparities in the quality of health care. Am J Public Health. 2003;93(10):1713–9. https://doi.org/10.2105/AJPH.93.10.1713.
Kirby JB, Taliaferro G, Zuvekas SH. Explaining racial and ethnic disparities in health care: Med Care. 2006;44(suppl):I-64-I-72. https://doi.org/10.1097/01.mlr.0000208195.83749.c3
Elster A, Jarosik J, VanGeest J, Fleming M. Racial and ethnic disparities in health care for adolescents: a systematic review of the literature. Arch Pediatr Adolesc Med. 2003;157(9):867–74. https://doi.org/10.1001/archpedi.157.9.867.
McGuire TG, Alegria M, Cook BL, et al. Implementing the Institute of Medicine definition of disparities: an application to mental health care. Health Serv Res. 2006;41(5):1979–2005. https://doi.org/10.1111/j.1475-6773.2006.00583.x.
Fernandez A, Schillinger D, Warton EM, Adler N, Moffet HH, Schenker Y, et al. Language barriers, physician-patient language concordance, and glycemic control among insured Latinos with diabetes: the diabetes study of Northern California (DISTANCE). J Gen Intern Med. 2011;26(2):170–6. https://doi.org/10.1007/s11606-010-1507-6.
Parker MM, Fernández A, Moffet HH, Grant RW, Torreblanca A, Karter AJ. Association of patient-physician language concordance and glycemic control for limited–English proficiency Latinos with type 2 diabetes. JAMA Intern Med. 2017;177(3):380–7. https://doi.org/10.1001/jamainternmed.2016.8648.
Paasche-Orlow MK, Parker RM, Gazmararian JA, Nielsen-Bohlman LT, Rudd RR. The prevalence of limited health literacy. J Gen Intern Med. 2005;20(2):175–84. https://doi.org/10.1111/j.1525-1497.2005.40245.x.
Osborn CY, Paasche-Orlow MK, Davis TC, Wolf MS. Health literacy. Am J Prev Med. 2007;33(5):374–8. https://doi.org/10.1016/j.amepre.2007.07.022.
Unequal treatment: confronting racial and ethnic disparities in health care (with CD). Washington, D.C.: National Academies Press; 2003. https://doi.org/10.17226/12875
De Lew N, Weinick R. An overview: eliminating racial, ethnic, and SES disparities in health care. Health Care Financ Rev. 2000;21(4):7.
Shen MJ, Peterson EB, Costas-Muñiz R, Hernandez MH, Jewell ST, Matsoukas K, et al. The effects of race and racial concordance on patient-physician communication: a systematic review of the literature. J Racial Ethn Health Disparities. 2018;5(1):117–40. https://doi.org/10.1007/s40615-017-0350-4.
Hernandez ND, Daley EM, Young L, Kolar SK, Wheldon C, Vamos CA, et al. HPV vaccine recommendations: does a health care clinician’s gender and ethnicity matter to unvaccinated Latina college women? Ethn Health. 2019;24(6):645–61. https://doi.org/10.1080/13557858.2017.1367761.
Saha S, Taggart SH, Komaromy M, Bindman AB. Do patients choose physicians of their own race? To provide the kind of care consumers want, medical schools might be able to justify using race as an admissions criterion. Health Aff (Millwood). 2000;19(4):76–83. https://doi.org/10.1377/hlthaff.19.4.76.
Brown TT, Scheffler RM, Tom SE, Schulman KA. Does the market value racial and ethnic concordance in physician? patient relationships? Health Serv Res. 2007;42(2):706–26. https://doi.org/10.1111/j.1475-6773.2006.00634.x.
Cooper LA, Roter DL, Johnson RL, Ford DE, Steinwachs DM, Powe NR. Patient-centered communication, ratings of care, and concordance of patient and physician race. Ann Intern Med. 2003;139(11):907–15. https://doi.org/10.7326/0003-4819-139-11-200312020-00009.
Penner LA, Gaertner S, Dovidio JF, Hagiwara N, Porcerelli J, Markova T, et al. A social psychological approach to improving the outcomes of racially discordant medical interactions. J Gen Intern Med. 2013;28(9):1143–9. https://doi.org/10.1007/s11606-013-2339-y.
Persky S, Kaphingst KA, Allen VC, Senay I. Effects of patient-clinician race concordance and smoking status on lung cancer risk perception accuracy among African-Americans. Ann Behav Med. 2013;45(3):308–17. https://doi.org/10.1007/s12160-013-9475-9.
Metzl JM, Roberts DE. Structural competency meets structural racism: race, politics, and the structure of medical knowledge. AMA J Ethics. 2014 Sep 1;16(9):674–90.
Tervalon M. and Murray-García, J. Cultural humility versus cultural competence: a critical distinction in defining physician training outcomes in multicultural education. Journal of Healthcare for the Poor and Underserved. May 1998. .
Street RL, O’Malley KJ, Cooper LA, et al. Understanding concordance in patient-physician relationships: personal and ethnic dimensions of shared identity. Ann Fam Med. 2008;6(3):198–205. https://doi.org/10.1370/afm.821.
Laveist TA, Nuru-Jeter A. Is doctor-patient race concordance associated with greater satisfaction with care? J Health Soc Behav. 2002;43(3):296–306.
Cooper-Patrick L. Race, gender, and partnership in the patient-physician relationship. JAMA. 1999;282(6):583–9. https://doi.org/10.1001/jama.282.6.583.
Alsan M, Garrick O, Graziani G. Does diversity matter for health? Experimental evidence from Oakland. :60.
Greenwood BN, Hardeman RR, Huang L, Sojourner A. Physician–patient racial concordance and disparities in birthing mortality for newborns. Proc Natl Acad Sci. 2020 Aug;13.
Oguz T. Is patient-provider racial concordance associated with Hispanics’ satisfaction with health care? Int J Environ Res Public Health. 2019 Jan;16(1):31.
Nimbal VC, Zhao B, Pu J, Romanelli RJ, Palaniappan L, Chung S. Does patient-provider racial/ethnic and language concordance impact patient-reported experience of care? J Patient Cent Res Rev. 2016;3:198.
Han W, Lee S. Racial/ethnic variation in health care satisfaction: the role of acculturation. Soc Work Health Care. 2016 Oct 20;55(9):694–710.
Kumar D, Schlundt DG, Wallston KA. Patient-physician race concordance and its relationship to perceived health outcomes. Ethnicity & Disease. 2009;19(3):345–51.
Lasser K. Missed appointment rates in primary care: the importance of site of care. J Health Care Poor Underserved. 2005;16(3):475–86. https://doi.org/10.1353/hpu.2005.0054.
Xierali IM, Nivet MA. The racial and ethnic composition and distribution of primary care physicians. J Health Care Poor Underserved. 2018;29(1):556–70. https://doi.org/10.1353/hpu.2018.0036.
Traylor AH, Schmittdiel JA, Uratsu CS, Mangione CM, Subramanian U. Adherence to cardiovascular disease medications: does patient-clinician race/ethnicity and language concordance matter? J Gen Intern Med. 2010;25(11):1172–7. https://doi.org/10.1007/s11606-010-1424-8.
King WD, Wong MD, Shapiro MF, et al. Does racial concordance between HIV-positive patients and their physicians affect the time to receipt of protease inhibitors? 2004;19:9.
Saha S, Komaromy M, Koepsell TD, Bindman AB. Patient-physician racial concordance and the perceived quality and use of health care. Arch Intern Med. 1999;159(9):997–1004. https://doi.org/10.1001/archinte.159.9.997.
Strumpf EC. Racial/ethnic disparities in primary care: the role of physician-patient concordance. Med Care. 2011;49(5):496–503. https://doi.org/10.1097/MLR.0b013e31820fbee4.
Hagiwara N, Slatcher RB, Eggly S, Penner LA. Physician racial bias and word use during racially discordant medical interactions. Health Commun. 2017;32(4):401–8. https://doi.org/10.1080/10410236.2016.1138389.
Meghani SH, Brooks JM, Gipson-Jones T, Waite R, Whitfield-Harris L, Deatrick JA. Patient–clinician race-concordance: does it matter in improving minority patients’ health outcomes? Ethn Health. 2009;14(1):107–30. https://doi.org/10.1080/13557850802227031.
Bazemore A, Petterson S, Peterson LE, Bruno R, Chung Y, Phillips RL. Higher primary care physician continuity is associated with lower costs and hospitalizations. The Annals of Family Medicine. 2018 Nov 1;16(6):492–7.
Bazemore A, Petterson S, Peterson LE, Phillips RL. More comprehensive care among family physicians is associated with lower costs and fewer hospitalizations. The Annals of Family Medicine. 2015 May 1;13(3):206–13.
Ma A, Sanchez A, Ma M. The impact of patient-provider race/ethnicity concordance on provider visits: updated evidence from the Medical Expenditure Panel Survey. J Racial Ethn Health Disparities. 2019 Oct 1;6(5):1011–20.
Chowdhury S, Machlin S, Gwet K. Sample designs of the Medical Expenditure Panel Survey Household Component, 1996–2006 and 2007–2016. Rockville, MD: Agency for Healthcare Research and Quality; 2019. https://meps.ahrq.gov/data_files/publications/mr33/mr33.pdf
Medical Expenditure Panel Survey. Agency for Healthcare Research and Quality https://meps.ahrq.gov/mepsweb/datastats/downloaddatafiles.jsp%20Accessed%20February%202019
StataCorp. Stata Statistical Software. College Station, Tx: StataCorp LP; 2015.
Liaw W, Petterson S, Rabin DL, Bazemore A. The impact of insurance and a usual source of care on emergency department use in the United States. International journal of family medicine. 2014;2014:1–5.
The United States Census Bureau. Comparative Demographic Estimates 2016 American Community Survey 1-Year Estimates. https://factfinder.census.gov/faces/tableservices/jsf/pages/productview.xhtml?pid=ACS_16_1YR_CP05&prodType=table. .
Villani J, Mortensen K. Nonemergent emergency department use among patients with a usual source of care.
Malhotra J, Rotter D, Tsui J, Llanos AA, Balasubramanian BA, Demissie K. Impact of patient–provider race, ethnicity, and gender concordance on cancer screening: findings from Medical Expenditure Panel Survey. Cancer Epidemiology and Prevention Biomarkers. 2017 Dec 1;26(12):1804–11.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Jetty, A., Jabbarpour, Y., Pollack, J. et al. Patient-Physician Racial Concordance Associated with Improved Healthcare Use and Lower Healthcare Expenditures in Minority Populations. J. Racial and Ethnic Health Disparities 9, 68–81 (2022). https://doi.org/10.1007/s40615-020-00930-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40615-020-00930-4