
Abstract
BACKGROUND
Medical interactions between Black patients and non-Black physicians are less positive and productive than racially concordant ones and contribute to racial disparities in the quality of health care.
OBJECTIVE
To determine whether an intervention based on the common ingroup identity model, previously used in nonmedical settings to reduce intergroup bias, would change physician and patient responses in racially discordant medical interactions and improve patient adherence.
IINTERVENTION
Physicians and patients were randomly assigned to either a common identity treatment (to enhance their sense of commonality) or a control (standard health information) condition, and then engaged in a scheduled appointment.
DESIGN
Intervention occurred just before the interaction. Patient demographic characteristics and relevant attitudes and/or behaviors were measured before and immediately after interactions, and 4 and 16 weeks later. Physicians provided information before and immediately after interactions.
PARTICIPANTS
Fourteen non-Black physicians and 72 low income Black patients at a Family Medicine residency training clinic.
MAIN MEASURES
Sense of being on the same team, patient-centeredness, and patient trust of physician, assessed immediately after the medical interactions, and patient trust and adherence, assessed 4 and 16 weeks later.
KEY RESULTS
Four and 16 weeks after interactions, patient trust of their physician and physicians in general was significantly greater in the treatment condition than control condition. Sixteen weeks after interactions, adherence was also significantly greater.
CONCLUSIONS
An intervention used to reduce intergroup bias successfully produced greater Black patient trust of non-Black physicians and adherence. These findings offer promising evidence for a relatively low-cost and simple intervention that may offer a means to improve medical outcomes of racially discordant medical interactions. However, the sample size of physicians and patients was small, and thus the effectiveness of the intervention should be further tested in different settings, with different populations of physicians and other health outcomes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
INTRODUCTION
Approximately 75 % of Black patients receive treatment from non-Black healthcare providers,1 and communication in racially/ethnically discordant medical interactions is less positive, productive, and informative than in racially concordant ones.2–6 Negative perceptions by physicians and patients play important roles in the dynamics and outcomes of these interactions.7–10 One critical aspect of these perceptions is trust.11 Non-Black physicians see Blacks patients as less trustworthy and compliant than White patients.7,12 Black patients are less trusting of their non-Black physicians,13,14 more likely to believe they have been mistreated because of race,15 and show declines in trust following interactions with non-Black physicians.16
We explored whether an intervention derived from the common ingroup identity model, a social categorization approach to improving intergroup relations generally, could improve medical outcomes for racially discordant medical interactions by changing physician and patient reactions to one another. The model17,18 proposes that members of different groups place one another in preexisting social categories, which facilitates spontaneous negative thoughts, feelings, and behaviors toward members of other groups. However, such reactions can be reduced by inducing members of these groups to recategorize themselves as members of the same, more inclusive group.19 There is considerable evidence from nonmedical settings that this recategorization approach can improve how members of different groups view one another,17,18 and increase feelings of trust and forgiveness between groups that have distrusted and disliked one another.20–22 The present research investigated whether an intervention derived from the common ingroup model can improve race-based trust in racially discordant primary care medical interactions, and thus produce more positive medical consequences. Physicians and their patients were randomly assigned to either a common ingroup identity treatment condition or a control condition. We hypothesized that immediately after the interactions, treatment-condition physicians would report a greater sense of being on the same team with their patient than would control-condition physicians. Similarly, we predicted that treatment-condition patients would report that (a) they had a greater sense of being on the same team with the physician, (b) the interaction was more patient-centered, and (c) they trusted the physician more than would control-condition patients. We also hypothesized that in the weeks following the intervention, treatment-condition patients, compared to control-condition patients, would report (a) greater trust of their physician and physicians in general and (b) greater adherence to their physicians’ recommendations.
METHOD
Study Setting and Participants
The setting was a family medicine residency clinic operated by the Department of Family Medicine and Public Health Sciences at Wayne State University. Data were collected between February 2007 and February 2008. Physicians were 14 non-Black medical residents (M age 29.45; SD = 2.45; 50 % female) in either the second or third year of their residency. Eleven residents self-identified as Asian or South Asian (e.g. Indian, Pakistani) and three as White. Patients were 72 self-identified low-income, insured Blacks who had appointments at the clinic.
Study Variables
In an initial questionnaire, physicians provided demographic and professional information and completed a 25-item measure of explicit racial bias 23,24 (5-point scale; internal consistency α = .87) and a measure of implicit racial bias, the Implicit Association Test (IAT).25 Physicians completed these measures at the beginning of the study while they were alone in a separate room. Immediately after a scheduled appointment, physicians answered two items about their sense of being on the same team with their patient8,9 (5-point scale, inter-item correlation = .88).
In an initial questionnaire, patients provided information about demographic characteristics, mental, and overall health status (SF-20)26 (5-point scales, α’s > 0.80) and completed measures of perceived past discrimination in seven domains 27 (e.g., housing, healthcare) (yes/no answers, odd even reliability with Spearman Brown correction = 0.77), two items concerned with trust of physicians in general28 (6-point scale, inter-item correlation = 0.84), and three items about medical adherence during the past month26 (6-point scale, α = 0.68). Immediately after their scheduled appointment, patients answered two questions about their sense of being on the same team with the physician (5-point scale, inter-item correlation = 0.83),8,9 two questions about trust of the physician they had just seen 28 (inter-item correlation = 0.71), and 15 questions about perceived patient-centeredness of the interaction29 (4-point scale, α = 0.86).
Four and 16 weeks after their appointment, patients answered the same two questions about trust of their own physician28 they had answered immediately after the interaction (inter-item correlations: 4-week = 0.95, 16-week = 0.90) and about trust of physicians in general 28 they had answered at baseline (inter-item correlations: 4-week = 0.76; 16-week = 0.73). Patients also re-answered the baseline questions about adherence, 26 now referring to adherence to their physician’s recommendations (4-week α = 0.70; 16-week α = 0.63). Given the relatively high reliability for all measures, individual items were averaged to create a single score for each measure.
Recruitment/Attrition
The study was approved by Karmanos Cancer Institute and Wayne State University Institutional Review Boards. Physicians were recruited and consented by a Black female research coordinator at the beginning of the study. Physicians received a $50.00 gift card for participating. There was no physician attrition.
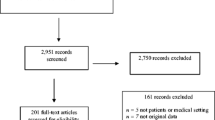
The same research coordinator recruited/consented patients when they arrived for their appointments. About 75 % of the patients approached agreed to participate. Patients received $15.00 gift cards on the day of their appointment and $20.00 cards for returning each of the two follow-up questionnaires. Of the 72 patients who agreed to be in the study, 42 were scheduled to see the treatment-condition physicians and 30 were scheduled to see the control-condition physicians. The difference in sample size between the two conditions reflects our lack of control over which physicians were in the clinic each recruitment day and their number of scheduled appointments on that day.
Fifty-three of these 72 patients (74 %) returned 4-week follow-up mail questionnaires; and 41 patients (77 % of those who returned the 4-week questionnaire and 57 % of the total sample) returned the 16-week questionnaire. There was no significant difference in attrition rates between the two conditions.
Treatment and Control Conditions
Physicians
Physicians (and thus their patients) were randomly assigned to either the common ingroup identity treatment condition (n = 7) or a general health information control condition (n = 7). Shortly after being consented, physicians in the treatment condition received written instructions that they and patients of theirs who had agreed to be in the study “will be asked to act as a team during (the) appointment with you.” Physicians would know these patients from buttons they would wear. Physicians received ten written suggestions for creating a sense of being on the same team as their patients (see Text Box). In the treatment condition interactions, these suggestions were also on a poster on the examination room wall. Physicians were asked to agree to follow the suggestions as much as possible during those interactions; all agreed. Then they received a button containing the words “Blue (or Red or Green) Team (previously established staff “teams”),” “Family Practice Clinic,” and the clinic logo, which showed schematic figures holding hands. Because clinical duties placed strong time demands on physicians, it was not possible to repeat these instructions over the course of the study. Control-condition physicians did not receive any instructions.
Text Box: Team Suggestions to Physician and Patients
1. Remember, you are a team. Both of you are responsible for what happens today. |
2. Do everything you can to answer questions as completely as possible. |
3. Do everything you can to make sure the other person understands you. |
4. Be sure to say something when you don’t understand the other person. |
5. Carefully listen to one another; try to understand the other person’s point of view. |
6. Try to find things you can agree about. |
7. If you do disagree about something, do so respectfully and try to understand the other team member’s point of view. |
8. Both of you should participate in any decisions made today. |
9. Both of you have joint responsibility for any decisions made today. |
10. Your responsibilities as a good team member do not end today. You both have to continue to follow the plan of care you agreed on today. |
Patients
Common identity treatment-condition patients were introduced to the concept of being on a team with their “doctor” via written instructions. Patients were asked to read and sign a team contract stating “that (they and their doctor) will be partners in a team that is working to solve (their medical problems),” which their physician had previously signed. All patients agreed. Patients were also informed of their team color and given the same button as their physician to wear during their appointment, and a pen in the team color with the words “Blue (Red, Green) Team Family Practice Clinic” on it. Finally, patients received the same suggestions to facilitate working together as a team with their physician. To assess fidelity of the intervention, patients were asked after the appointment whether they had received a pen and button, and whether there had been a team poster in the room. Control-condition patients received general health information before the interactions; they did not receive buttons, pens, or team suggestions.
Statistical Analysis
Because patients were nested within physicians, we conducted General Estimating Equation linear regressions with robust empirical SE estimates (SPSS 20) to examine the effects of the intervention on outcome variables. Physician explicit and implicit racial bias and patient perceived past racial discrimination were all significantly associated with one or more of the outcomes of interest7–9 and were used as covariates. We controlled for baseline trust and adherence when these were the outcomes. Statistical power for the analyses was moderate, from 0.85 for the full sample to 0.60 for the 16-week follow-up. A mediation analysis was conducted with the “Process” macro,30 using an ordinary least squares path analytical framework for estimating mediator effects. Bootstrap methods were implemented (N = 5,000) for inference about indirect effects.
RESULTS
Patient and physician characteristics are presented in Table 1. Preliminary analyses revealed no systematic differences on any measures as a function of physician race or ethnicity; thus, this factor was not included in subsequent analyses. There were no demographic differences between either physicians or patients assigned to the two conditions. Patients in the two conditions did not differ in health or initial measures of bias, discrimination, trust or adherence. On average, physicians showed a nonsignificant (D = −0.09) implicit pro-Black bias. Patients who completed the two follow-up questionnaires did not differ from those who did not on any baseline or immediate post-interaction measures.
Over 90 % of patients correctly reported receiving/not receiving the pen and button and seeing/not seeing the poster in the examination room. In order to not compromise random assignment, the few patients who incorrectly answered these questions were included in the analyses.
Immediate Post-Interaction Questionnaires
Table 2 presents baseline and outcome scores overall and separately for treatment and control conditions. Physicians in both conditions reported an equivalently strong sense of being on the same team with their patients. Patients in the two conditions also both strongly agreed they were on the same team with the physician, perceived the interaction as patient-centered, and reported equivalent high levels of trust in their physician. The first two hypotheses were thus not supported.
Follow-Up Questionnaires
As indicated in Table 2, 4 weeks after the interactions, treatment-condition patients reported greater trust of their own physician and physicians in general than did control-condition patients (B own = 0.426, SE = 0.21, Wald’s χ 2(1) = 4.30, P = 0.038); (B general =1.10, SE = 0.21, Wald’s χ 2(1) =10.56, P = 0.001). Greater patient trust of their own physicians and physicians in general was also found at 16 weeks after the interactions as well (B own = 0.347, SE = 0.15, Wald’s χ 2 (1) = 5.49, P = 0.019); (B general = 0.502, SE = 0.23, Wald’sχ 2(1) = 4.54, P = 0.033).
There was no significant effect of treatment on patients’ adherence to physician’s recommendations 4 weeks after the interaction. However, at 16 weeks treatment-condition patients reported significantly more adherence than did control-condition patients (B = 0.347, SE = 0.13, Wald’sχ 2(1) = 7.34, P = 0.007).
We also explored whether the relationship between the intervention and adherence at 16 weeks was mediated by patient trust at the 4-week follow-up. The overall model (with baseline adherence controlled) was not significant, R 2(3,34) = 0.186, P = 0.069. However, indirect effect of trust of physicians in general on adherence was significant (B = 0.407, SE = 0.24, 95 % CI = 0.017−0.992).
DISCUSSION
The common ingroup identity intervention had significant long-term effects on patient trust of physicians (4 and 16 weeks after the interaction) and adherence to physicians’ treatment recommendations (16 weeks after the interaction). Whereas patient trust declined over time in the control condition, it remained high over 16 weeks in the treatment condition. Moreover, although the findings should be interpreted cautiously because of small sample size, differences in patient trust 4 weeks after the visit mediated the greater adherence of treatment-condition patients than control-condition patients 16 weeks after their appointment.
The absence of any effects among physicians merits some comment. All physicians in this study had received some formal training in patient-centered care.31 Many concepts in patient-centered care overlap with a common identity approach to medical interactions. This training, and the associated value of taking a patient-centered approach to their patients, may have led physicians in both conditions to perceive a cooperative, “team” relationship with the patient, producing high physician team ratings regardless of experimental condition (note in Table 2 the average was over 4 on a 5-point scale). This would have reduced any differential impact of the intervention on how physicians in the two conditions answered team questions.
Moreover, any initial effect of the team intervention on physicians may have diminished over time. Although the study lasted a year, physicians’ very busy schedules at this clinic and their other rotations made it impossible to provide periodic boosters during the time physicians were in the study. Thus, even if the common identity intervention was effective with physicians at the beginning of the study, the salience and impact of the intervention likely weakened as time passed.
In contrast, the intervention was likely quite salient to the patients when they met the physician and resulted in sustained trust in physicians among patients in the common identity condition 4 and 16 weeks after their clinic visit, whereas trust declined among control-condition patients. Like physicians, there were no significant patient differences in team perceptions as a function of the intervention immediately after visits. One explanation is that medical interactions are already inherently team-oriented, creating a ceiling effect that suppresses differences by condition. Differences as a function of the intervention might be more apparent if it had focused more specifically on how patients and physicians experienced their relationship (e.g., feeling like members of one group versus different groups),17 than on the instrumental (team) aspect of the situation.
For patients, the difference in trust by condition also did not appear immediately after the interaction, probably because of the demands of the context in which post-interaction trust was initially assessed. Patients were alone when they completed the measures, and had been told that no one at the clinic would ever see their answers. Nonetheless, the situation may still have aroused patient expectations about what desirable answers would be. The research coordinator could easily have been perceived to be part of clinic staff. The patient satisfaction literature suggests a strong positive response bias in patients’ reports of satisfaction with physicians.32,33 Such a response bias probably served to artificially raise scores on some of the immediate post-interaction measures and mask effects of the intervention. During the mail follow-ups, however, contextual demands for positive answers were weaker, because patients completed questionnaires in their homes, names were not asked for, and the questionnaires were returned to a university address rather than the clinic.
Two, potentially related microprocesses may be responsible for the between-condition differences in patient trust. First, the intervention may have created better physician–patient rapport. Research in non-medical contexts demonstrates that sharing a common identity facilitates greater self-disclosure34 and promotes smoother and more effective intergroup interactions.18 Future research might use dyadic analyses to explore interrelationships between patient and physician trust during the interactions, and how these perceptions influence the quality (e.g., self-disclosing content) of patient participation in the exchange and subsequent adherence.
Second, patients in the two conditions may have differed in how they processed and interpreted the information they received during the interactions. Feelings of common ingroup identity lead people to process information more deeply,35 be more trusting of people conveying the information,36,37 and thus ultimately be more influenced by the information.38 Also, people give ingroup members greater “benefit of the doubt,”39 which would help to maintain patient trust in physicians and adherence over time.
One potential study limitation of the present study is that most of these interactions involved non-Black physicians from the Asian subcontinent. Despite this, we believe that our findings are likely generalizable to other racially discordant medical interactions involving Black patients. The large percentage of Asian physicians in our sample is quite typical for clinics that serve low-socioeconomic ethnic minority patient populations in the United States.40 We also did not find any systematic differences associated with physician race or ethnicity, but we note that our sample size of physicians was restricted and thus statistical power for these tests was quite low (< 0.50). In addition, the interactions fit the conditions that would lead to ingroup and outgroup categorization. Physicians in our sample occupied a professional role in the medical encounters that was quite distinct from the role held by patients. Furthermore, the non-Black physicians and Black patients could readily recognize from a number of physical features and accents that they did not share common racial/ethnic/social identities. It is true that the physicians in this sample showed less implicit bias than White physicians in general.41 However, there is no evidence that physician bias (or patient perceived discrimination) operated any differently in this study than in several other studies of racially discordant medical interactions.7–9,42–45 Nevertheless, it is possible that because this particular group of physicians had a slight pro-Black bias, had been trained in patient-centered communication skills, and/or had racial/ethic socialization experiences that differ from those of large portions of White Americans, it might have been easier to engender patient trust of them than it would be with a sample of White physicians displaying a stronger pro-White implicit bias. Thus the effectiveness of the intervention merits testing with other samples of physicians varying in attitudes, background, and prior training.
In conclusion, the current findings have practical implications for improving healthcare of Black patients. This relatively low-cost and effective intervention does not require substantial amounts of time from either physicians or patients. In addition, a common ingroup identity intervention can be used with both physicians and patients and may have mutually reinforcing effects on the dynamics of medical interactions and, ultimately (as we demonstrated) on patients’ longer-term responses to medical care. However, the sample size of physicians and patients in the present study was limited, and thus the effectiveness of the intervention should be further tested in different settings, with different populations of physicians and other health outcomes. Nevertheless, results are promising and offer initial evidence of an efficient and useful intervention to improve outcomes of racially discordant medical interactions and address the continuing pervasive racial disparities in the quality of healthcare.46
REFERENCES
Chen FM, Fryer GE, Phillips RL, Wilson E, Pathman DE. Patients’ beliefs about racism, preferences for physician race, and satisfaction with care. Ann Fam Med. 2005;3:139–143.
Cooper-Patrick L, Gallo JJ, Gonzales JJ, et al. Race, gender, and partnership in the patient–physician relationship. JAMA J Am Med Assoc. 1999;282(6):583–589.
Johnson RL, Roter D, Powe NR, Cooper LA. Patient race/ethnicity and quality of patient-physician communication during medical visits. Am J Public Health. 2004;94(12):2084–2090.
Oliver MN, Goodwin MA, Gotler RS, Gregory PM, Stange KC. Time use in clinical encounters: are African-American patients treated differently? J Natl Med Assoc. 2001;93(10):380–385.
Siminoff LA, Graham GC, Gordon NH. Cancer communication patterns and the influence of patient characteristics: disparities in information-giving and affective behaviors. Patient Educ Counsel. 2006;62(3):355–360.
Eggly S, Penner LA, Harper FW, et al. Perceptions of information provided by oncologists in clinical interactions with black and white patients/companions. Paper presented at: American Association for Cancer Research Science of Cancer Health Disparities in Racial/Ethnic Minorities and the Medically Underserved; October; 2010.
Cooper LA, Roter DL, Carson KA, et al. The associations of clinicians’ implicit attitudes about race with medical visit communication and patient ratings of interpersonal care. Am J Public Health. 2012;102(5):979–987.
Penner LA, Dovidio JF, Edmondson D, et al. The experience of discrimination and Black–White health disparities in medical care. J Black Psychol. 2009;35:180–203.
Penner LA, Dovidio JF, West TW, et al. Aversive racism and medical interactions with Black patients: a field study. J Exp Soc Psychol. 2010;46:436–440.
van Ryn M, Saha S. Exploring unconscious bias in disparities research and medical education. JAMA J Am Med Assoc. 2011;306(9):995–996.
Dovidio JF, Penner LA, Albrecht TL, Norton WE, Gaertner SL, Shelton JN. Disparities and distrust: the implications of psychological processes for understanding racial disparities in health and health care. Soc Sci Med. 2008;67:478–486.
Moskowitz D, Thom DH, Guzman D, Penko J, Miaskowski C, Kushel M. Is primary care providers’ trust in socially marginalized patients affected by race? J Gen Intern Med. 2011;26(8):846–851.
Doescher MP, Saver BG, Franks P, Fiscella K. Racial and ethnic disparities in perceptions of physician style and trust. Arch Fam Med. 2000;9(10):1156–1163.
Halbert CH, Armstrong K, Gandy OH, Shaker L. Racial differences in trust in health care providers. Arch Intern Med. 2006;166:896–901.
Johnson RL, Saha S, Arbelaez JJ, Beach MC, Cooper LA. Racial and ethnic differences in patient perceptions of bias and cultural competence in health care. J Gen Intern Med. 2004;19:101–110.
Gordon HS, Street RL Jr, Sharf BF, Kelly PA, Souchek J. Racial differences in trust and lung cancer patients’ perceptions of physician communication. J Clin Oncol Offic J Am Soc Clin Oncol. 2006;24(6):904–909.
Gaertner SL, Dovidio JF. Reducing intergroup bias: the common ingroup identity model. New York: Psychology Press; 2000.
Gaertner SL, Dovidio JF. A common ingroup identity: a categorization-based approach for reducing intergroup bias. In: Nelson TD, ed. Handbook of prejudice, stereotyping, and discrimination. New York: Psychology Press; 2009:489–505.
Crisp RJ, Turner RN, Hewstone M. Common ingroups and complex identities: routes to reducing bias in multiple category contexts. Group Dynam Theor Res Pract. 2010;14(1):32–46.
Guerra R, Rebelo M, Monteiro MB, et al. How should intergroup contact be structured to reduce bias among majority and minority group children? Group Process Intergroup Relat. 2010;13(4):445–460.
González R, Manzi J, Noor M. Intergroup forgiveness and reparation in Chile: the role of identity and intergroup emotions. In: Tropp LR, Mallett RK, eds. Moving beyond prejudice reduction: pathways to positive intergroup relations. Washington, DC: American Psychological Association; 2011:221–239.
Wohl MJA, Branscombe NR. Forgiveness and collective guilt assignment to historical perpetrator groups depend on level of social category inclusiveness. J Personal Soc Psychol. 2005;88(2):288–303.
Brigham JC. College students’ racial attitudes. J Appl Soc Psychol. 1993;23(23):1933–1967.
McConahay JB. Modern racism, ambivalence, and the modern racism scale. In: Dovidio JF, Gaertner SL, eds. Prejudice, discrimination, and racism. San Diego: Academic; 1986:91–125.
Greenwald AG, Poehlman TA, Uhlmann EL, Banaji MR. Understanding and using the implicit association test: III. Meta-analysis of predictive validity. J Personal Soc Psychol. 2009;97:17–41.
Hays RD, Kravitz RL, Mazel RM, Sherbourne CD. The impact of patient adherence on health outcomes for patients with chronic disease in the medical outcomes study. J Behav Med. 1994;17(4):347–360.
Brown TN. Measuring self-perceived racial and ethnic discrimination in social surveys. Sociol Spectr. 2001;21(3):377–392.
Dugan E, Trachtenberg F, Hall MA. Development of abbreviated measures to assess patient trust in a physician, a health insurer, and the medical profession. BMC Health Services Research. 2005;5.
Stewart MA, Brown JB, Donner A, et al. The impact of patient-centered care on outcomes. J Fam Pract. 2000;49:796–804.
PROCESS [computer program]. 2012.
Epstein RM, Street RL. Patient-centered communication in cancer care: promoting healing and reducing suffering. Bethesda, MD: National Cancer Institute; 2007.
Derby DC, Haan A, Wood K. Data quality assurance: an analysis of patient non-response. Int J Health Care Qual Assur. 2011;24(3):198–210.
Mazor KM, Clauser BE, Field T, Yood RA, Gurwitz JH. A demonstration of the impact of response bias on the results of patient satisfaction surveys. Heal Serv Res. 2002;37(5):1403–1417.
Dovidio JF, Gaertner SL, Validzic A, Matoka K, Johnson B, Frazier S. Extending the benefits of recategorization: evaluations, self-disclosure, and helping. J Exp Soc Psychol. 1997;33(4):401–420.
Park B, Rothbart M. Perception of out-group homogeneity and levels of social categorization: memory for the subordinate attributes of in-group and out-group members. J Personal Soc Psychol. 1982;42(6):1051–1068.
Foddy M, Platow MJ, Yamagishi H. Group-based trust in strangers: the role of stereotypes and expectations. Psychol Sci. 2009;20:419–422.
Vorauer JD. An information search model of evaluative concerns in intergroup interaction. Psychol Rev. 2006;113(4):862–886.
Mackie DM, Devos T, Smith ER. Intergroup emotions: explaining offensive action tendencies in an intergroup context. J Personal Soc Psychol. 2000;79:602–616.
Hewstone M. The ‘ultimate attribution error’? A review of the literature on intergroup causal attribution. Eur J Soc Psychol. 1990;20(4):311–335.
Hing E, Lin S. Role of international medical graduates providing office-based medical care: United States, 2005–2006. NCHS Data Brief. 2009;13:1–8.
Sabin JA, Rivara FP, Greenwald AG. Physician implicit attitudes and stereotypes about race and quality of medical care. Med Care. 2008;46:678–685.
Benkert R, Peters RM, Clark R, Keves-Foster K. Effects of perceived racism, cultural mistrust and trust in providers on satisfaction with care. J Natl Med Assoc. 2006;98:1532–1540.
Green AR, Carney DR, Pallin DJ, et al. Implicit bias among physicians and its predictions of thrombolysis decisions for Black and White patients. J Gen Intern Med. 2007;22:1231–1238.
Hagiwara N, Penner LA, Eggly S, Albrecht TL. Perceived discrimination, implicit bias, and adherence to physician recommendations. Paper presented at: The Science of Research on Discrimination and Health Conference, Bethesda, MD; 2011.
Blair IV. Doctor’s implicit bias predicts Black patients’ evaluations. Symposium on The Role of Stereotypes and Prejudice in Health. Aassociation for Psychological Science. Chicago Illinois; 2012.
Smedley BD, Stith AY, Nelson AR. Unequal treatment: Confronting racial and ethnic disparities in health care. In: Medicine Io, (ed). Washington DC: National Academies Press; 2003.
Acknowledgements
This research was supported by a grant to the first author from the National Institute of Child Health and Development (1R21HD050445001A1) and a SAGES Award from the Society for the Psychological Study of Social issues, grants to the last author from the National Cancer Institute (U01CA114583, 1U54CA154606-01), a grant from the National Science Foundation (BCS-0613218) to Samuel L. Gaertner and John F. Dovidio, and a NIH Grant RO1HL 0856331-0182 and a NIDA Grant 1R01DA029888-01 to John F. Dovidio. Prior Presentation: Society for Personality and Social Psychology, January 27, 2010, Tampa, Florida.
Conflict of Interest
The authors declare that they do not have a conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Penner, L.A., Gaertner, S., Dovidio, J.F. et al. A Social Psychological Approach to Improving the Outcomes of Racially Discordant Medical Interactions. J GEN INTERN MED 28, 1143–1149 (2013). https://doi.org/10.1007/s11606-013-2339-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-013-2339-y