
Abstract
Background
Head impacts and resulting head accelerations cause concussive injuries. There is no standard for reporting head impact data in sports to enable comparison between studies.
Objective
The aim was to outline methods for reporting head impact acceleration data in sport and the effect of the acceleration thresholds on the number of impacts reported.
Methods
A systematic review of accelerometer systems utilised to report head impact data in sport was conducted. The effect of using different thresholds on a set of impact data from 38 amateur senior rugby players in New Zealand over a competition season was calculated.
Results
Of the 52 studies identified, 42 % reported impacts using a >10-g threshold, where g is the acceleration of gravity. Studies reported descriptive statistics as mean ± standard deviation, median, 25th to 75th interquartile range, and 95th percentile. Application of the varied impact thresholds to the New Zealand data set resulted in 20,687 impacts of >10 g, 11,459 (45 % less) impacts of >15 g, and 4024 (81 % less) impacts of >30 g.
Discussion
Linear and angular raw data were most frequently reported. Metrics combining raw data may be more useful; however, validity of the metrics has not been adequately addressed for sport. Differing data collection methods and descriptive statistics for reporting head impacts in sports limit inter-study comparisons. Consensus on data analysis methods for sports impact assessment is needed, including thresholds. Based on the available data, the 10-g threshold is the most commonly reported impact threshold and should be reported as the median with 25th and 75th interquartile ranges as the data are non-normally distributed. Validation studies are required to determine the best threshold and metrics for impact acceleration data collection in sport.
Conclusion
Until in-field validation studies are completed, it is recommended that head impact data should be reported as median and interquartile ranges using the 10-g impact threshold.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
The validity of head impact metrics has not been adequately addressed for sports. |
Consensus on data analysis methods is required for reporting head impact biomechanics. |
As head impact data are not normally distributed, to allow for comparison between studies, it is recommended that these data be reported using median values and interquartile ranges. |
It is recommended that a 10-g linear threshold be utilised for the reporting of head impact biomechanics. |
1 Introduction
1.1 Head Impacts Cause Injury: Evidence
Known as the ‘silent injury’ [1], and often reported by the media and sporting circles as a ‘knock to the head’ [2], sport-related concussions (hereafter called ‘concussion’) are a subset of mild traumatic brain injuries (mTBIs) [3] and have become an increasingly serious concern for all sporting activities worldwide [4–6]. Research into concussions [7] has increased over the years, leading to greater insight into the causes and the effects of these injuries. Research [8–27] has sought to better determine the head linear and rotational accelerations involved in concussion injuries through the use of telemetry. By adapting radio-telemetry that was utilised for astronauts [28], a telemetry system was developed and has been in use since 1961 for the recording of impacts for football players and concussions [29] that have occurred.
1.2 A Cumulative Head Impact Threshold may be Related to Concussion
The immediate and long-term effects of multiple and repeated blows to the head that athletes receive in contact sporting environments are a growing concern in clinical practice [30, 31]. Concern has grown about the effects of subconcussive impacts to the head and how these impacts may adversely affect cerebral functions [30–32]. Subconcussive events are impacts that occur where there is an apparent brain insult with insufficient force to result in the hallmark signs and symptoms of a concussion [31, 33, 34]. Although subconcussive events do not result in observable signs and apparent behavioural alterations [35, 36], they can cause damage to the central nervous system and have the potential to transfer a high degree of linear and rotational acceleration forces to the brain [37]. Proposed decades previously [38, 39], exposure to repetitive subconcussive blows to the head may result in similar, if not greater damage than a single concussive event [33] and may have cumulative effects [40].
Participants can be exposed to a high number of impacts per season [32]. It has been suggested [41, 42] that brain injuries come from concussive events and also from the accumulation of subconcussive impacts that result in pathophysiological changes in the brain. As subconcussive impacts do not result in observable concussion-related signs and symptoms, these are often not medically diagnosed. The accumulation of subconcussive blows can result in neuropsychological changes [30, 31, 42–46]. However, similar to the literature focused on concussion and mTBI, the literature on subconcussive head trauma is limited [47]. What is not known is the number of head impacts and their intensity that might lead to concussion (i.e. a concussion cumulative threshold). The injury threshold is likely to be different for each person given the multifactorial nature of injuries, as per other thresholds for injuries to tendons, ligaments, muscle and bone. If a threshold could be determined, players could be monitored to reduce their potential risk for concussion injury—akin to cricket monitoring players’ loading to the body during bowling events via the number of overs in an attempt to reduce the risk of back stress fractures [48].
1.3 Impacts can be Measured with a Number of Technologies
Head impact dynamics have been analysed through the use of video analysis [8], in game measurements [20–25, 27, 49–52], numerical methods [9–12] and reconstructions using anthropometric test devices [13–19] in helmeted sports such as American football [20–23] and ice hockey [24, 25] and in un-helmeted sports such as soccer [26] and rugby union [27].
The on-field assessment of head impacts has been enabled with a head impact telemetry system (HITS) (Simbex, LLC, Lebanon, NH), using helmet-mounted accelerometers enabling determination of the head linear and rotational accelerations in American football [21, 23, 49, 53–55] and ice hockey [24, 25], and using a headband in youth soccer [26]. The data collected through the HITS has enabled analytical risk functions [16, 51, 56, 57], concussion risk curves [51], and risk weighted exposure metrics [58] to be developed, further assisting in the identification of sports participants at risk of concussive injuries. More recently, instrumented mouthguards known as XGuard (X2biosystems, Inc., Seattle, WA, USA) have documented head impacts in rugby union [27].
1.4 Thresholds have Differed for Reporting Impact Data in Contact and Collision Sports
Although there is an increasing amount of published literature reporting impact accelerations to the head in the sporting environment, there is less attention focussed on identifying what is a subconcussive impact and where this occurs. Studies [55, 59, 60] have been conducted reporting the impacts absorbed by the head during activities undertaken daily. Although impacts to the head and body under 10 g have been reported [55], these activities such as walking, jumping, running and sitting are considered to be non-contact events [21, 61]. However, impacts greater than 10 g occurring from contact events that do not result in acute signs or symptoms of concussion are identified as subconcussive impacts [43].
1.5 To Enable Comparison of Studies, a Consistent Threshold for Reporting is Needed
Head impact data are essential to understand the biomechanics of head injury to develop potential injury prevention strategies. Researchers have utilised different thresholds, with the most common being 9.6 and 14.4 g, depending on the accelerometer. The equipment utilised to record and report head impacts varies in sensitivity and the types of algorithms employed for the identification of impacts [62]. These differences may invariably influence the results of the published studies as, although some studies report the linear threshold as 14.4 g, they may actually be recording from 10 g, and if the researcher is unaware that this threshold is the default, the data may be included (personal correspondence, S. Broglio; September 2015). The collection of the impact data is based on one accelerometer and the unfiltered/unprocessed data, and the value obtained only loosely relates to the final measure being sought. The impact data are processed with a hard exclusion cut-off of 10 g, enabling data collection to become manageable as acceleration lower than 10 g without impacts occurring becomes more common (personal correspondence, S. Broglio; 22 September 2015). There is currently no standard for reporting head impact data to enable comparison between studies. Currently, the use of accelerometers may not necessarily provide the meaningful inter-study comparisons that are sought, because of data collection, processing and methodologies not being standardised [63]. Studies utilising different impact thresholds have proposed varying conclusions based on the methodological and reporting approaches undertaken.
1.6 Measurements Reporting Head Impact Biomechanics and Injury Causation
In 1966, Gadd [64] proposed the Gadd Severity Index (GSI) head injury severity index based on the Wayne State Tolerance Curve (WSTC). Developed from animal and cadaver impact data, the GSI simplified the WSTC by taking into consideration the shape of the linear acceleration time history, providing a weighting factor of 2.5, enabling the whole body acceleration data to be plotted on log-log coordinates along a straight line. The critical value of the GSI is 1000. If the GSI is less than 1000, the head impact is considered probabilistically safe. The GSI is used to quantify severe skull fractures and brain injury risk, but is not recommended for use to quantify a risk of concussion [65]. A concern with regard to the GSI is that it can give unrealistically high values for impacts that have a much longer pulse duration [66]. The mathematical expression for the GSI is:
where a is the ‘effective’ acceleration (thought to have been the average linear acceleration) of the head measured in terms of g, the acceleration of gravity, and t is the time in milliseconds from the start of the impact [67].
In 1971, a modification of the GSI, the Head Injury Criterion (HIC), was proposed [68] to focus the severity index on that part of the impact that was likely to be relevant to the risk of injury to the brain. This was done by averaging the integration of the resultant acceleration/time curve over whatever time interval yielded the maximum value of HIC. Because this varies from one impact to another, the expression for the modified index simply refers to times t 1 and t 2. The HIC is computed based on the following expression:
where t 2 and t 1 are any two arbitrary time points during the acceleration pulse. Acceleration is measured in multiples of g, and time is measured in seconds. The resultant acceleration is used for the calculation. The US National Highway Traffic Safety Administration (NHTSA) requires t 2 and t 1 to not be more than 36 ms apart (thus called HIC36) and the maximum HIC36 to not exceed 1000. In 1998 [69], the NHTSA introduced the HIC15, where t 2 and t 1 are not to be more than 15 ms apart and the maximum HIC15 is not to exceed 700. In a numerical study [70], it was estimated that an mTBI tolerance for the HIC15, where there is a 25, 50 and 75 % likelihood of an mTBI occurring, had HIC15 values of 136, 235 and 333, respectively.
In 2008 [71], the principal component score (PCS), a weighted sum of linear acceleration, rotational acceleration, HIC and GSI, with objectively defined weights, was published. It is now more commonly termed the Head Impact Telemetry Severity Profile (HITSP), and is a weighted composite score including linear and rotational accelerations, impact duration, as well as impact location. The resulting formula is:
where sX = (X-mean [X])/(SD [X]), LIN = linear acceleration, ROT = rotational acceleration, HIC = Head Injury Criterion, and GSI = Gadd Severity Index. The offset by 2 and scaling by 10 generates HITSP values greater than 0 and in the numerical range of the other classic measures studied. A HITSP score of 63 or greater is reported to be an indication there is a 75 % risk of a concussive injury occurring [71].
In 2013, a novel cumulative exposure metric, the Risk Weighted Cumulative Exposure (RWE) equation, was developed [58] with four previously published analytical risk functions. The four different analytical risk functions were the linear resultant acceleration [16, 56], rotational resultant acceleration [51] and combined probability (linear and rotational) resultant accelerations [57]. These risk functions were utilised to elucidate individual player and team-based exposure to head impacts. The RWE equations comprise of a L as the measured peak linear acceleration (PLA), a R as the measured peak rotational acceleration (PRA), and n hits as the number of head impacts in a season for a given player.
Risk function(s) | Equation |
|---|---|
RWELinear = \( \mathop \sum \nolimits_{i = 1}^{{n_{\text{hits}} }} R\left( {a_{\text{L}} } \right)i \) | |
Rotational [51] | RWERotational = \( \mathop \sum \nolimits_{i = 1}^{{n_{\text{hits}} }} R\left( {a_{\text{R}} } \right)i \) |
Combined probability [57] | RWECP = \( \mathop \sum \nolimits_{i = 1}^{{n_{\text{hits}} }} CP\left( {a_{\text{L}} ,a_{\text{R}} } \right)i \) |
In the logistic regression equations and regression coefficients of the injury risk functions utilised in the prediction of injury, α and β are the regression coefficients and x is the measured acceleration for the linear and rotational risk functions [58].
Logistic regression equation | Risk function | Regression coefficients |
|---|---|---|
\( R\left[ a \right] = \frac{1}{{1 + {\text{e}}^{ - \alpha + \beta x} }} \) | α = −9.805, β = 0.0510 | |
Rotational [51] | α = −12.531, β = 0.0020 | |
\( {\text{CP}} = \frac{1}{{1 + {\text{e}}^{{ - (\beta_{0} + \beta_{1} a + \beta_{2} \alpha + \beta_{3 } a\alpha }} }} \) | Combined probability (CP) [57] | β 0 = −10.2, β 1 = 0.0433, β 2 = 0.000873, β 3 = −9.2E−07 |
β 0, β 1, β 2 and β 3 are regression coefficients, a is the measured linear acceleration, and α is the measured rotational acceleration for the combined probability risk function. The three metrics provided as a result of these equations are for linear (RWELinear), rotational (RWERotational) and combined (linear and rotational) probability (RWECP).
In an attempt to delineate injury causation and to establish a meaningful injury criterion through the use of actual field data, Zhang et al. [12]. proposed tolerance levels for human head injury based on input kinematics scaled from animal data and non-injurious volunteer test results. Injury predictors and injury levels were analysed on the basis of resulting brain tissue responses, and these were correlated with the site and occurrence of a concussion. The calculated sheer stress around the brainstem region could be an injury predictor, and statistical analyses were performed to establish a brain injury tolerance level. As a result of the analyses undertaken, and based on linear logistic regression analyses, it was reported [12] that the maximum resultant translational acceleration at the centre of gravity of the head was estimated to be 66, 82 and 106 g for a 25, 50 and 80 % probability of sustaining an mTBI, respectively.
For resultant rotational acceleration at the centre of gravity of the head, this was estimated to be 4600 radians per second per second (rad/s2), 5900 rad/s2 and 7900 rad/s2 for a 25, 50 and 80 % probability of sustaining an mTBI, respectively. The estimated HIC15 thresholds were 151, 240 and 369 for a 25, 50 and 80 % probability of sustaining an mTBI, respectively. These thresholds are considerably less than the HIC15 limit of 1000 for sustaining a serious brain injury. If the head was exposed to a combined translational and rotational acceleration with an impact duration between 10 and 30 ms, the suggested tolerable reversible brain injury was 85 g translational acceleration, 6000 rad/s2 rotational acceleration and an HIC15 value of 240. These values may change as more human data become available, but to date no published updates of these values have been available. Although other variables have been proposed (Generalised Acceleration Model for Brain Injury Threshold [GAMBIT] [14, 72, 73], and Head Impact Power [HIP] [74]), these have not been utilised in any studies reporting head impacts in contact sport.
1.7 Aim of the Study
The rationale for this study is based on questions around the magnitude of a single impact that may result in concussion, the number of impacts needed to result in signs and symptoms of concussion, and individual player differences that might affect injury tolerance levels for concussion. Given head impacts are likely to cause concussive injury, and the number of head impacts may be related to a potential concussion threshold (i.e. a cumulative threshold), the number of head impacts should be monitored in players. However, given impacts can be measured with a number of technologies (e.g. instrumented behind-the-ear patches, mouthguards, and head gear) and thresholds have differed for reporting impact data in contact and collision sports, a threshold for reporting impact data in sport is needed to enable comparison of studies. Therefore, the aims of this study were to (a) summarise the methods for reporting head impact data in sport to date and (b) assess the impact of different acceleration thresholds on the likely identification of concussive injuries.
2 Methods
To outline methods for reporting head impact data, a systematic review of the literature was conducted. The guideline for reporting observational studies [Meta-analysis Of Observational Studies in Epidemiology (MOOSE)] [75] was followed for the empirical literature evidence included in this study. The MOOSE checklist contains specifications and guidelines for the conduct and review of the studies. To evaluate the effects of acceleration thresholds on the number of impacts reported, variable thresholds were applied to head impact data obtained from 38 senior amateur rugby union players during 19 matches in New Zealand [27].
2.1 Literature Review to Identify Thresholds for Reporting Head Impact Data in Contact and Collision Sport
2.1.1 Search Strategy for Identification of Publications
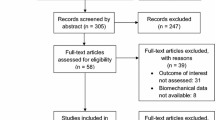
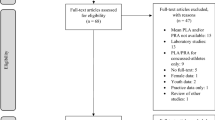
A total of 53,185 studies available online from January 1990 to June 2015, identified through the SCOPUS (n = 10,090), SportDiscus (n = 1187), OVID (n = 9729), Science Direct (n = 27,803) and Health Sciences (n = 4376) databases, were screened for eligibility (see Fig. 1). The keywords utilised for the search of relevant research studies included combinations of ‘head impact telemetry system*’, ‘HITS’, ‘concussion’, ‘impact*’, ‘traumatic brain injury’, ‘chronic traumatic encephalopathy’, ‘angular’, ‘linear’, ‘rotational’, ‘acceleration’, ‘biomechanics’, ‘head acceleration’ and ‘risk’. An example of the Health Sciences search strategy is provided in the Electronic Supplementary Material (ESM), Table S1. Searches were limited to ‘English language’ and ‘humans’ only. The references of all relevant articles were searched for further articles. All publications identified were initially screened by publication title and abstract to identify eligibility. In cases of discrepancies of eligibility, another author assessed the publication to screen for eligibility.

Flow of identification, screening, eligibility and study inclusion of previously published studies
To establish some control over heterogeneity of the studies [75], inclusion criteria were established. Any published study or book that did not meet the inclusion criteria was excluded from the study. Publications were included if they reported head impact biomechanics and met the following inclusion criteria:
-
1.
The study was published in a peer reviewed journal or book.
-
2.
The study reported the biomechanics of impacts to the head in a sporting environment.
-
3.
The study addressed one or more of the keywords used in the search strategy relating to this study.
Reviewed studies were excluded from this review if it was identified that the publication:
-
1.
Was unavailable in English.
-
2.
Did not provide additional information specifically addressing areas relating to this study.
-
3.
Was a case study.
-
4.
Reviewed head impact studies.
2.1.2 Assessment of Publication Quality
The 52 studies [10, 12, 16, 20–27, 32, 37, 42, 49, 51–54, 57, 58, 61, 71, 73, 76–103] meeting the inclusion criteria (see Table 1) were assessed for quality by two of the authors on the basis of the MOOSE [75] published checklist. Heterogeneity of the studies included in the literature review was expected as there might be differences in the study design, population and outcomes [75]. As a result of the MOOSE [75] checklist, the studies included had a median score of 4.8/6.0, with a range of 4.0–5.0.
2.2 Ethical Consent and Mouthguard Instrumentation
2.2.1 Participants and Ethical Consent
A prospective observational cohort study was conducted on a premier club level amateur rugby union team during the 2013 domestic competition season of matches in New Zealand. All thirty-eight male players [mean ± standard deviation (SD) age 22 ± 4 years] were amateurs receiving no remuneration for participating in rugby union activities. The matches were played under the laws of the New Zealand Rugby Football Union. All players involved in the team under study were invited to participate and were free to withdraw at any stage of the study. All participating players signed a consent form before being provided with the mouthguard. If players withdrew from the study, they were still eligible for participation in the match activities of the team under study. No players withdrew from the study. The researchers’ university ethics committee approved all procedures in the study (AUTEC 12/156), and all players gave informed consent prior to participating. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
2.2.2 Mouthguard Instrumentation
Players were fitted with a moulded X2Biosystems All-In-Mouth (AIM) instrumented mouthguard (X2Biosystems, Inc., Seattle, WA, USA), sampling at 1000 Hz, prior to the start of the season. The mouthguards contained a low-power, high-g tri-axial accelerometer (H3LIS331DL) with 200 g maximum per axis, and a tri-axial angular rate gyroscope (L3G4200D; ST Microelectronics, Geneva, Switzerland; http://www.st.com) [104]. The mouthguards utilised were similar to those utilised in a previous study [104]. The accelerometer and gyroscope calculated an acceleration and rotational time history of the head’s estimated centre of gravity for all impacts that occurred during match participation. The time history incorporated three axes (x, y, z) of acceleration and three axes of velocity. With the player standing upright, these planes described sideways (medio-lateral), forward–back (anterior–posterior) and vertical acceleration and deceleration. The mouthguards [104] have strong correlations for PLA (r 2 = 0.93), PRA (r 2 = 0.88) and peak rotational velocity (r 2 = 0.97) when compared with the head’s centre of gravity.
The moulded instrumented mouthguards have been reported [104, 105] to have normalised root-mean-square errors for impact time traces of 9.9 ± 4.4 % for linear acceleration, 9.7 ± 7.0 % for angular acceleration, and 10.4 ± 9.9 % for angular velocity, but miss, or misclassify, ~4 % of impacts [106]. The average error offset for impact location was 1.63° ± 3.74° azimuth and −1.57° ± 0.48° elevation [105]. The mouthguards recorded head linear and rotational acceleration, impact location and duration. For the impact to be recorded, a total of 100 ms of data were stored, including 25 ms prior to, and 75 ms following, the impact. Software provided by X2Biosystems calculated the PLA, PRA (x axis and y axis angular accelerations), impact location, HIC [68] and GSI [64], and these were date and time stamped for later download and analyses. All data were recorded on the X2Biosystem Injury Management Software (IMS) and transferred to an Excel spreadsheet for further analysis. All matches were videotaped (Sony HDR-PJ540 Camcorder) to enable verification of the impacts recorded.
The biomechanical measures of head impact severity consisted of impact duration in milliseconds (ms), linear acceleration (g), and rotational head acceleration (rad/s2). Resultant linear acceleration is the rate of change in velocity of the estimated centre of gravity of the head attributable to an impact and the associated direction of motion of the head [107]. Resultant rotational acceleration is the rate of change in rotational velocity of the head attributable to an impact and its direction in a coordinate system with the origin at the estimated centre of gravity of the head [107]. The rotational acceleration was calculated through the IMS utilising a 5-point stencil from the rotational velocity measured by the tri-axial angular rate gyroscope (L3G4200D; ST Microelectronics, Geneva, Switzerland; http://www.st.com).
Impacts were identified as any linear acceleration above 10 g measured at the mouthguard. These impacts could be a result of a direct blow to the head, face, neck or elsewhere on the body with an ‘impulsive’ acceleration transmitted to the head. Each recorded impact was categorised into four general locations (front, side, back and top) [53]. The direction of impact (azimuth θ) was defined from −180° to 180° with 0° at the x axis with positive θ on the right side of the player’s head. The height of impact (elevation α) was defined from 0° (horizontal plane that passes through the head’s centre of gravity) to 90° (crown of the head at the z axis). The xz plane represented the midsagittal plane, with positive x corresponding to the caudal direction. The xy plane represented the coronal plane, with positive y corresponding to the right side of the head. Impacts with an α of >65° were defined as top, while impacts with a θ of −45° to 45° were defined as back, ±45° to ±135° side and −135° to 135° front.
All impacts recorded were assessed for head movement or biting by the players when the mouthguard was worn. Impacts that were identified as having occurred through these activities were termed ‘clacks’. All impacts were assessed through the IMS utilising a ‘de-clacking algorithm’ that involved two methods. The first method utilised various parameters (time above 10-g data acquisition limit, ratio of PLA to area under curve, filtered/unfiltered PLA ratio, PLA vs. number of points above data acquisition limit) to assess waveform characteristics of the aggregate of the various features of the acceleration waveform to determine an impact versus a ‘clack’. The second method utilised a cross-correlation pattern matching (with configurable cross-correlation coefficient) by comparing the impact form to a Gaussian-like reference waveform, looking for a cross-correlation coefficient above a configurable data acquisition limit (0.90 is the default, i.e. 90 % match). This method assumed a ‘good’ shape for a head impact and matches recorded impacts against this reference waveform (personal correspondence, J. Thibado; 1 May 2014). All impacts identified as ‘clacks’ were removed from the data set prior to downloading for further analysis. All data collected were entered into a Microsoft Excel spreadsheet and analysed with SPSS V.22.0.0.
Over the course of the 2013 domestic rugby union season of matches, a total of 20,687 impacts exceeded our study data acquisition limit of 10 g for a head impact and were retained for data analyses. Impacts of <10 g of linear acceleration were considered negligible in regard to impact biomechanical features and to eliminate head accelerations from non-impact events such as jumping and running [55]. Their relationships to head trauma make it difficult to distinguish between head impacts and voluntary head movement [107]. Please see King et al. [27] for the full statistical analysis undertaken on the head impact biomechanics.
2.3 Application of Head Impact Thresholds Identified from the Literature to the Rugby Head Impact Data Set
The data set used for the application of the head impact thresholds identified from the literature review was from 38 amateur rugby union players who wore instrumented mouthguards over a season of matches [27]. The raw data set was filtered by linear acceleration thresholds at increments of 1 g to establish the percentage of impacts removed at each threshold from 10.0 to 30.0 g. This percentage was then used to calculate the possible number of impacts removed for the impact thresholds used in the different studies reviewed.
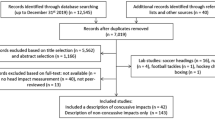
All data estimations were calculated on an Excel spreadsheet. The data were analysed using SPSS v22.0.0 (SPSS Inc.), and as the data were non-normally distributed (Shapiro–Wilk test p < 0.001), data were analysed using a Friedman repeated measures ANOVA on ranks. Post hoc analysis with Wilcoxon signed-rank tests was conducted with a Bonferroni correction applied. Statistical significance was set at p < 0.05. The estimated number of impacts was calculated by dividing the number of reported impacts by the estimated percentage of impacts removed at the different thresholds. The estimated total number of reported impacts was subtracted from the reported number of impacts to identify the possible number of impacts removed from the data set; for example, for a number of impacts reported of 161,732 [87, 88], an impact threshold of 14.4 g, and based on the New Zealand rugby union data set for 20,687 impacts recorded at 10.0 g, when reassessed at 14.4 g, there were 12,091 impacts. A total of 8569 impacts were removed or 42 % of the data set (see Fig. 2). Therefore, 161,732 (number of impacts reported) ÷ 42 % (percentage of impacts removed at 14.4 g) gave a possible total number of impacts at the 10-g threshold of 385,076. The possible total number of impacts removed from the data set was 223,344 (i.e. 385,076 − 161,732 impacts).

Percentage of impacts removed when applying different data impact threshold limits compared with original 10-g threshold limit for the New Zealand data set of head impacts to senior amateur rugby union players for one season
3 Findings
3.1 Literature Review
A total of 52 publications were identified that reported head impacts and met the inclusion criteria. Studies reported impacts to the head via technology in American football [12, 16, 20–23, 32, 37, 42, 49, 51–54, 57, 58, 61, 71, 73, 76–79, 81, 85–95, 97, 98, 100–102], ice hockey [24, 25, 80, 82–84, 96, 101, 103], soccer [26], rugby union [10, 27], Australian Football [10, 99] and mixed martial arts and boxing [73].
3.1.1 Impact Threshold
Studies utilised different data impact acceleration thresholds (see Table 1): 42 % of studies [21, 22, 24, 26, 27, 49, 52, 54, 61, 73, 76–86] used 10 g; 17 % of studies [20, 23, 42, 51, 53, 58, 87–90] used 14.4 g; 8 % of studies [37, 91–95] used 15 g; 4 % of studies [25, 96] used 20 g; 2 % of studies [97] used 30 g; and 4 % of studies [32, 98] reported impact data within 10–60 g and greater than 90 g. Four studies [10, 12, 16, 99] (8 %) were reconstruction studies from video analysis, but were included as they reported impact biomechanics. Six studies [57, 71, 100–103] (12 %) did not report the impact threshold, but did report head impact biomechanics. One study [73] (2 %) used a 7- and 10-g threshold with different sporting activities.
3.2 Acceleration Raw Data and Metrics
Apart from raw resultant linear accelerations [12, 16, 20–27, 32, 37, 49, 52, 54, 57, 58, 61, 71, 73, 76–103] (reported in 90 % of studies) and rotational acceleration data [10, 51] (reported in 73 % of studies) [10, 12, 16, 20–27, 37, 51, 54, 57, 58, 71, 73, 77, 78, 81–96, 99–101, 103], several head impact-derived variables were reported, such as the GSI [64] (4 % [26, 49]), the HIC [68] (21 % [10, 12, 16, 24, 26, 49, 71, 79, 87, 88]), HITSP [71] (28.8 % [21, 25, 37, 71, 78, 81, 83–86, 89, 93–96, 103]) and the RWE [58] (1.8 %) metrics.
Nearly all of the studies reviewed identified the number of impacts that were recorded; however, 4 % of studies reported impacts in matches only, 23 % recorded impacts for both match and practice activities, and 55 % combined both match and practice activity impacts. The remaining 15 % of studies reviewed reported on impacts above 90 g or were reconstruction of impacts from video analysis. The number of impacts ranged from 480 impacts from 22 players in Pop Warner American football [97] to 486,594 impacts from 450 players in collegiate American football and ice hockey [101] (see Table 1).
Over half (52 %) of the studies [10, 12, 16, 22, 23, 27, 37, 49, 58, 61, 76, 77, 80–86, 91, 93–98, 102, 103] reported the impact biomechanics data as mean ± SD. Some studies [20, 21, 23, 25, 54, 58, 73, 85, 90, 94, 100] (21 %) also reported the head impacts as median, but not all [20, 21, 23, 54, 85, 90, 100] (13 %) included the interquartile ranges for the data. Of the studies that reported the impact biomechanics by the median, only 8 % [25, 58, 73, 94] reported the interquartile range. Most of the studies reporting the median also reported the 95th percentile of the impacts. Other data reporting methodologies utilised within the data sets reviewed were the median of the 95th [21], 98th [71, 94], 99th [71, 94], and 99.5th [94] percentiles. Fourteen percent of studies also included lower and upper limits [61, 83, 84, 86] for the range of impacts [24, 101] and the mean range [97] of the impacts. Less than a quarter of studies (23 %) reported their impacts as x-, y-, z-axis data [22], +1 SD [52], cumulative distribution functions [54, 58], percentage of impacts [21, 53], and the impact duration (ms) [16, 87, 88, 92, 93]. In addition to the impact biomechanics being presented by various methodologies, 14 % of studies [12, 27, 37, 81, 86, 91, 102] also incorporated impact tolerances and impact severity levels.
3.3 Application of Head Impact Thresholds to the Rugby Head Impact Data Set
By utilising data from a previously published study [27] that used the 10-g impact threshold, data were re-extracted at differing impact thresholds from 10 g to 30 g. By adjusting the impact threshold (see Fig. 2), the number of impacts decreased as the impact threshold increased (see Table 2). There were significant differences observed (p < 0.05) for each of the different acceleration thresholds for the number of impacts reported, the mean, median and the 95th percentile when compared with the impacts at the 10-g linear acceleration threshold (see Table 2).
Based on the differences observed in the study reporting on impacts in amateur senior rugby union [27], at the 14.4-g threshold, there could have been as many as 42 % of the impacts recorded not being reported. As a result, studies [20, 23, 25, 32, 37, 42, 51, 53, 58, 87–98] using impact thresholds above 10 g may have removed 2100–206,573 impacts. At the 30-g impact threshold, it can be estimated that 80–85 % of impacts were not reported [97]. Again, based on the differences observed in this study through the analysis of different thresholds, it is possible that each player in the Pop Warner study [97] may have experienced a cumulative total of 1885 impacts above 10 g. Although the impacts may not have been recorded, the players may well have been exposed to this number of impacts between 10 and 30 g. The differences between impacts reported and the possible number of impacts (480 vs. 2365) may result in an underestimation of the exposure risk of these players to subconcussive impacts.
4 Discussion
This study undertook to review the methods for reporting head impact data in sport and to outline the effect of various acceleration thresholds on the number of impacts reported. A consensus on a threshold for reporting data is important given the variation in conclusions that may be drawn if the same data set is used with different thresholds, as identified by our application of the range of thresholds from prior literature applied to a New Zealand rugby union head impact data set. A standard threshold for head impact data is important given possible monitoring of player head impact acceleration data in the hope of identifying a cumulative threshold for concussion from subconcussive impacts.
The equipment utilised to record and report head impacts varies in sensitivity and the types of algorithms employed for the identification of impacts [62]. These differences may invariably influence the results of the published studies as, although some studies report the linear threshold as 14.4 g, they may actually be recording from 10 g and, if the researcher is unaware that this threshold is the default, the data may be included (personal correspondence, S. Broglio; September 2015). In the recording of data for the HITS, the data are based on the triggering of one accelerometer, and the unfiltered/unprocessed data only loosely relates to the final measurement of interest at the head’s centre of gravity.
The discussion surrounding subconcussive impacts has become popular [32, 41, 43, 95, 108, 109]. Initially the term subconcussive impact described an impact that did not result in severe, noticeable symptoms, especially loss of consciousness [108]. However, recently, subconcussive is a term used to describe an asymptomatic non-concussive impact to the head [32, 41, 43, 95, 109]. The issue relating to the effects of subconcussive impacts is controversial as researchers and clinicians are divided on the true effects [30–32, 42, 45, 110]. Some research [32, 110] has reported that these impacts have minimal effect on cognitive functions, while others [30, 31, 42, 45, 46] have reported these impacts to be detrimental to cerebral and cognitive functions. To date, there is a paucity of evidence to identify the impact acceleration that is adequate to produce a non-structural brain injury associated with the neuronal changes of concussion [30].
Animal models display metabolic changes associated with concussion, which may be similar in subconcussive impacts [111]. To research subconcussive impacts in isolation is challenging, and there are, to date, no reports on animal models or other reliable methodologies that have been successful at identifying these impacts [111]. Brain injury may occur from concussive events as well as from an accumulation of subconcussive impacts [41]. The effects of concussive events and multiple subconcussive impacts have been associated with long-term progressive neuropathologies and cognitive deficits [43, 112–114]. Longitudinal impact monitoring at the level where these subconcussive events are beginning to occur is important, and a standard threshold needs to be established.
4.1 What Threshold Should be Used to Monitor Head Impacts?
Impacts of <10 g of linear acceleration have been considered negligible in regards to impact biomechanical features. The <10-g impact threshold has been used in research to eliminate head accelerations from non-impact events such as jumping and running [21, 55, 61]. The inclusion of these non-impact events to head trauma make it difficult to distinguish between head impacts and voluntary head movement [107], and eliminating these will help identify the true extent of the number of impacts that do occur from sports participation. A suggestion for this may be to report the distribution of the impacts by the various resultant linear accelerations, using a frequency analysis and reporting quartile ranges, i.e. 25th and 75th interquartile range. This may assist in identifying where the most frequent resultant linear accelerations occur in the different sports. Consensus for the impact threshold will need to be established, and should be based on validation studies to determine the best impact threshold for various sports and injury outcomes. Biomechanical modelling of impact forces and brain movement would be needed to identify likely impact thresholds for injury, as well as in-field validation studies using prospective monitoring of players during tackles and impacts with the ground. As there is no established criterion for reporting head impact biomechanics, and the largest proportion (42 %) of studies [21, 22, 24, 26, 27, 49, 52, 54, 61, 72, 75–85] reported the resultant linear acceleration threshold at 10 g, future studies should report all impacts above the 10-g resultant linear acceleration threshold.
4.2 What Descriptive Statistics Should be Used to Report Head Impact Biomechanics?
There were a variety of descriptive statistics used in the reporting of head impact biomechanics in the reviewed studies which limits inter-study comparisons. Although more than half (52 %) of the studies reviewed [10, 12, 16, 22, 23, 27, 37, 49, 58, 61, 73, 76, 77, 81–87, 91, 94–98, 102, 103] reported their results by means and SDs, the use of these statistics may not accurately represent the true centre of the data. By reporting the mean value of the data set, this method is subject to extreme values (i.e. outliers) such as those in skewed data sets. The use of the mean is suitable if the data set has a symmetrical distribution. In non-normal distributed data, the median is the most useful for describing the centre of the data [127]. Of the studies [23, 25, 58, 85, 87, 94] reviewed (22 %) that reported the results by the median would more accurately have identified the centre of the data set. The New Zealand senior amateur head impact data were non-normally distributed (i.e. not symmetrical), therefore the use of descriptive statistics that can account for this skewness needed to be considered. To enable inter-study comparisons, and until a consensus is established for the reporting of head impact biomechanics, future studies should report the median [25th and 75th interquartile ranges] for all head impact biometrics.
4.3 What Acceleration Metrics Should be Used to Monitor Head Impacts?
It has been suggested that both resultant linear and rotational accelerations should be reported with head impact metrics [115], as there is an improved correlation between impact biomechanics and the occurrence of a concussion, compared with when linear accelerations are reported alone [12]. Research [18, 116–119] suggests that the brain is more sensitive to rotational than linear accelerations. Rotational accelerations are reported [12, 120] to be correlated to the strain response of the brain and the primary mechanism for diffuse brain injury including concussion, contusion, axonal injuries and loss of consciousness [116, 117, 121, 122]. Linear accelerations are reported to result in the intracranial pressure response of the brain and to be the primary mechanism for skull fractures and epidural haematomas [120, 123]. Reporting both linear and rotational accelerations should assist with identification of possible brain injury.
More recently [57, 58], resultant linear and rotational acceleration results have been combined into an RWE metric. This metric can be beneficial for fully capturing the linear (RWELinear), rotational (RWERotational) and combined probability (from linear and rotational) (RWECP) of the risk of a concussion as it accounts for the frequency and severity of each player’s impacts. The HIC and GSI are the most frequently utilised head injury assessment functions in helmet and traffic restraint safety standards [12, 124]; however, this was not reflected in the sport head impact studies reviewed. Based on the WSTC [68], the HIC and GSI criteria are considered plausible ways of determining relative risk of severe head injury [125], but they do not account for the complex motion of the brain, nor the contribution of resultant rotational acceleration to the head [12, 14, 74]. In particular, the HIC only deals with frontal impacts and was not designed to be used for lateral impacts that can be found in head impact biomechanics [124] and arbitrarily defines an ‘unsafe pulse’ within a ‘safe pulse’ by discounting any data outside the two time points chosen for the calculation of the HIC value [126].
The GSI and HIC may be beneficial for evaluating acute head trauma due to single impacts, but they are reportedly not beneficial for repeated impacts at lower acceleration magnitudes [124], such as those found in contact sports such as American football, rugby union and soccer. The inclusion of the HIC and GSI by studies reporting on head impact biomechanics may be more historical, thus providing the ability for inter-study comparisons with previous studies. However, as they are used to calculate multiple impacts and provide a nonsensical number, the value of these metrics is limited. The use of HIC and GSI in future studies, and the value that these metrics provide, needs to be standardised. Consensus is required on the incorporation of these and other biomechanical metrics into future research.
4.4 Limitations in the Use of Accelerometery
The use of accelerometers to record and assess movement is not new to the scientific community [127, 128]. There have been some inter-study and international comparability limitations reported for use of accelerometers to report physical activity [63]. The identified limitations for physical activity accelerometers may be identical to areas now being faced by studies reporting the biomechanics of impacts to the head. The largest proportion of studies reporting head impact biomechanics have utilised HITS [20–24, 32, 37, 42, 49, 51–54, 57, 58, 61, 71, 76–79, 81–95, 97, 98, 100–102], or a variant [26]. More recently, an electronic mouthguard has been used to assess head impacts in rugby union [27].
The issues identified with the use of accelerometers for physical activity [63] include affordability of the accelerometers [63], and the administration burden [63] to the participants and researcher(s) given post-data-collection analysis. The choice of accelerator brand [129], generation [130] and firmware version [131], wearing position [132] based on the sports code requirements (i.e. helmet mounted vs. headband mounted vs. mouthguard embedded vs. patch), specifics of the research being undertaken, such as the epoch length [133, 134] (match vs. training vs. combined), data imputation methods [135], dealing with spurious data [136] and the reintegration of smaller epochs into larger epochs [137] are all considerations for use of accelerometers. In addition to the issues identified, there are technological developments, emerging methodological questions and a lack of academic consensus that may also hinder the development of uniformity in the utilisation of accelerometers [63] for recording head impact biomechanics.
In comparing the New Zealand rugby union data with data collected with the use of the HITS, it must be noted that these are different impact telemetry systems. The mouthguard is reported to have a 10 % error for linear and rotation acceleration and for angular velocity with an average offset of 2° for azimuth and elevation impact location [104, 105]. Although the correlation of the AIM mouthguard with laboratory head forms is good, the impact measurements should be assumed to have some form of error that is dependent on impact conditions and the measure of interest and the variability tested [101, 138]. It is unlikely that the mouthguard was tested under all of the activities seen in rugby union matches, such as the rucks, mauls, lineouts and scrum situations. How these rugby activities correlate to the laboratory conditions is unknown. Although the majority of the impact biomechanics studies reported in this review are helmet-based telemetry systems, there is a paucity of studies reporting on head impact biomechanics with other systems such as the mouthguard and headband. In addition, there are no published studies comparing the HITS with other forms of impact telemetry systems, such as the X2Biosystems AIM mouthguard.
A final consideration to the use of accelerometers in recording impacts is the need for concurrent video analysis to enable comparison and verification of the impacts. This would enable the identification of non-impact activities where an impact has been recorded, such as post-try celebrations, dropping equipment onto the ground, or other activities where the equipment may record an impact. In the case of the New Zealand rugby union data, only impacts that occurred in the tackle with the player standing were able to be verified [27]. The percentage of impacts that were identified at the 10-g inclusion limit, that were able to be visualised by video review and analysis, varied from 65 to 85 % of the total impacts recorded per match [27].
4.5 What are the Long-Term Implications of Repeated Head Impacts?
The use of impact tolerance and impact severity level data may be important if a risk assessment is undertaken for possible long-term implications from repetitive head impacts (RHIs). Recently, in a small sample [77] of collegiate players with no reported concussions after a season of American football, there were white-matter changes that correlated with multiple head impact measures. Participants with more than 30–40 RHIs with PRAs of >4500 rad/s2 per season (r = 0.91; p < 0.001) and more than 10–15 RHIs with >6000 rad/s2 (r = 0.81; p < 0.001) were significantly correlated with post-season white-matter changes [77]. These changes post season imply a relationship between the number of RHIs that occur over a season of American football and white-matter injury, despite no clinically evident concussion being recorded [77].
The inclusion of impact tolerances and impact severity levels may assist with the identification of players at risk of possible long-term injuries. Impact tolerance may also act as an indicator of when to rest players if they are exposed to RHIs above >4500 and >6000 rad/s2. This type of information will assist in formulating a detailed understanding of the exposure and mechanism of injury of concussion [53, 139]. Further research is required to evaluate the injury tolerance of concussive type injuries, to develop interventions to reduce the likelihood of any concussive type injuries, and to develop exposure durations and standdown periods to establish a broader understanding of the potential role of subconcussive events and long-term health [53].
5 Conclusion
This study identified the methodological differences in the threshold limits of impacts to the head as a result of participation in contact sports. Of the 52 studies, 42 % reported impacts at the 10-g impact threshold, while 17 % of studies used the 14.4-g impact threshold. Resultant linear accelerations were most frequently reported (90 %), while 73 % reported resultant rotational accelerations. Over three-quarters (94 %) of studies reported both resultant linear and rotational accelerations. Impact data were most frequently (52 %) reported as mean ± SD. Some studies (21 %) reported the head impact data as median, but not all (13 %) included the interquartile ranges for these data.
The influence of head impact thresholds was shown using head impact data obtained from 38 senior amateur rugby union players during 19 matches in New Zealand. Application of the varied impact thresholds resulted in 20,687 impacts of >10 g, 11,459 (44.6 % less) impacts of >15 g, and 4024 (80.5 % less) impacts of >30 g.
Given head impacts are likely to cause concussive injury, and the number of head impacts may be related to a potential concussion threshold (i.e. a cumulative threshold), the number and severity of head impacts should be monitored in players. However, impacts can be measured with several technologies (e.g. instrumented behind-the-ear patches, mouthguards and head gear), and thresholds have differed for reporting impact data in contact and collision sports. Consensus is therefore required to identify the reporting modalities (e.g. linear threshold, descriptive calculations) to utilise in future impact studies to enable between-study comparisons. Until in-field validation studies are completed, it is recommended that data should be reported as mean ± SD and median and interquartile ranges, using the 10-g impact threshold.
References
Kirkwood M, Yeates K, Taylor H, et al. Management of pediatric mild traumatic brain injury: a neuropsychological review from injury through recovery. Clin Neuropsychol. 2008;22(5):769–800.
Khurana V, Kaye A. An overview of concussion in sport. J Clin Neurosci. 2012;19(1):1–11.
McCrory P, Meeuwisse W, Aubry M, et al. Consensus statement on concussion in sport: the 4th International conference on concussion in sport held in Zurich, November 2012. Br J Sports Med. 2013;47(5):250–8.
Covassin T, Elbin R III, Sarmiento K. Educating coaches about concussion in sports: evaluation of the CDC’s “Heads Up Concussion in Youth Sports” initiative. J School Health. 2012;82(5):233–8.
De Beaumont L, Brisson B, Lassonde M, et al. Long-term electrophysiological changes in athletes with a history of multiple concussions. Brain Inj. 2007;21(6):631–44.
McCrory P. Sports concussion and the risk of chronic neurological impairment. Clin J Sports Med. 2011;21(1):6–12.
King D, Brughelli M, Hume P, et al. Assessment, management and knowledge of sport-related concussion: systematic review. Sports Med. 2014;44(4):449–71.
McIntosh A, McCrory P, Comerford J. The dynamics of concussive head impacts in rugby and Australian rules football. Med Sci Sports Exerc. 2000;32(12):1980–4.
Baumgartner D, Willinger R, Shewchenko N, et al. Tolerance limits for mild traumatic brain injury derived from numerical head impact replication. In: Proceedings of the IRCOBI conference on the biomechanics of impact; 2001 Oct 10–12; Isle of Man (UK): IRCOBI; 2001 Oct 10–12. p. 353–5.
Fréchède B, McIntosh A. Numerical reconstruction of real-life concussive football impacts. Med Sci Sport Exerc. 2009;41(2):390–8.
Shewchenko N, Withnall C, Keown M, et al. Heading in football. Part 2: biomechanics of ball heading and head response. Br J Sports Med. 2005;39(Suppl 1):i26–32.
Zhang L, Yang J, King A. A proposed injury threshold for mild traumatic brain injury. J Biomed Eng. 2004;126(2):226–36.
Gilchrist A, Mills NJ. Protection of the side of the head. Accid Anal Prev. 1996;28(4):525–35.
Newman J, Barr C, Beusenberg M, et al. A new biomechanical assessment of mild traumatic brain injury. Part 2—results and conclusions. International IRCOBI conference on the biomechanics of impacts 2000; 2000; Montpellier (France); 2000. p. 223–33.
Pellman E, Viano D, Tucker A, et al. Concussion in professional football: location and direction of helmet impacts-part 2. Neurosurgery. 2003;53(6):1328–41.
Pellman E, Viano D, Tucker A, et al. Concussion in professional football: reconstruction of game impacts and injuries. Neurosurgery. 2003;53(4):799–814.
Viano D, Pellman E. Concussion in professional football: biomechanics of the striking player—part 8. Neurosurgery. 2005;56(2):266–80.
Viano DC, Casson IR, Pellman EJ. Concussion in professional football: biomechanics of the struck player - part 14. Neurosurgery. 2007;61(2):313-27; discussion 27-28.
Withnall C, Shewchenko N, Gittens R, et al. Biomechanical investigation of head impacts in football. Br J Sports Med. 2005;39(suppl 1):i49–57.
Cobb B, Urban J, Davenport E, et al. Head impact exposure in youth football: elementary school ages 9–12 years and the effect of practice structure. Ann Biomed Eng. 2013;21(12):2463–73.
Crisco J, Wilcox B, Beckwith J, et al. Head impact exposure in collegiate football players. J Biomech. 2011;44(15):2673–8.
Rowson S, Brolinson G, Goforth M, et al. Linear and angular head acceleration measurements in collegiate football. J Biomed Eng. 2009;131(061016):1–7.
Young T, Daniel R, Rowson S, et al. Head impact exposure in youth football: elementary school ages 7-8 years and the effect of returning players. Clin J Sport Med. 2014;24(5):416–21.
Reed N, Taha T, Keightley M, et al. Measurement of head impacts in youth ice hockey players. Int J Sports Med. 2010;31(11):826–33.
Wilcox B, Beckwith J, Greenwald R, et al. Head impact exposure in male and female collegiate ice hockey players. J Biomech. 2013;47(1):109–14.
Hanlon E, Bir C. Real-time head acceleration measurements in girls youth soccer. Med Sci Sports Exerc. 2012;44(6):1102–8.
King D, Hume P, Brughelli M, et al. Instrumented mouthguard acceleration analyses for head impacts in amateur rugby union players over a season of matches. Am J Sports Med. 2015;43(3):614–24.
Reid S, Epstein H, Louis M, et al. Physiologic response to impact. J Trauma. 1975;15(2):150–2.
Reid S, Tarkington J, Epstein H, et al. Brain tolerance to impact in football. Surg Gynecol Obstet. 1971;133(6):929–36.
Baugh C, Stamm J, Riley D, et al. Chronic traumatic encephalopathy: neurodegeneration following repetitive concussive and subconcussive brain trauma. Brain Imaging Behav. 2012;6(2):244–54.
Gavett B, Stern R, McKee A. Chronic traumatic encephalopathy: a potential late effect of sport-related concussive and subconcussive head trauma. Clin Sports Med. 2011;30(1):179–88.
Gysland S, Mihalik J, Register-Mihalik J, et al. The relationship between subconcussive impacts and concussion history on clinical measures of neurologic function in collegiate football players. Ann Biomed Eng. 2012;40(1):14–22.
Webbe F, Barth J. Short-term and long-term outcome of athletic closed head injuries. Clin Sports Med. 2003;22(3):577–92.
Witol A, Webbe F. Soccer heading frequency predicts neuropsychological deficits. Arch Clin Neuropsychol. 2003;18(4):397–417.
Bauer J, Thomas T, Cauraugh J, et al. Impacts forces and neck muscle activity in heading by collegiate female soccer players. J Sports Sci. 2001;19(3):171–9.
Dashnaw M, Petraglia A, Bailes J. An overview of the basic science of concussion and subconcussion: where we are and where we are going. Neurosurg Focus. 2012;33(6):E5.
Broglio SP, Eckner J, Martini D, et al. Cumulative head impact burden in high school football. J Neurotrauma. 2011;28(10):2069–78.
Tysvaer A, Løchen E. Soccer injuries to the brain: a neuropsychologic study of former soccer players. Am J Sports Med. 1991;19(1):56–60.
Unterharnscheidt F. About boxing: review of historical and medical aspects. Tex Rep Biol Med. 1970;28(4):421–95.
Shultz S, MacFabe D, Foley K, et al. Sub-concussive brain injury in the Long-Evans rat induces acute neuroinflammation in the absence of behavioral impairments. Behav Brain Res. 2012;229(1):145–52.
Spiotta A, Shin J, Bartsch A, et al. Subconcussive impact in sports: a new era of awareness. World Neurosurg. 2011;75(2):175–8.
Talavage T, Nauman E, Breedlove E, et al. Functionally-detected cognitive impairment in high school football players without clinically-diagnosed concussion. J Neurotrauma. 2014;31(4):327–38.
Bailes J, Petraglia A, Omalu B, et al. Role of subconcussion in repetitive mild traumatic brain injury. J Neurosurg. 2013;119(5):1235–45.
Erlander D, Kutner K, Barth J, et al. Neuropsychology of sports-related head injury: dementia pugilistica to post concussion syndrome. Clin Neurophysiol. 1999;13(2):193–209.
McKee A, Cantu R, Nowinski C, et al. Chronic traumatic encephalopathy in athletes: progressive tauopathy after repetitive head injury. J Neuropathol Exp Neurol. 2009;68(7):709–35.
Poole V, Abbas K, Shenk T, et al. MR spectroscopic evidence of brain injury in the non-diagnosed collision sport athlete. Dev Neuropsychol. 2014;39(6):459–73.
Rutherford A, Stephens R, Potter D. The neuropsychology of heading and head trauma in association football (soccer): a review. Neuropsychol Rev. 2003;13(3):153–79.
Johnson M, Ferreira M, Hush J. Lumbar vertebral stress injuries in fast bowlers: a review of prevalence and risk factors. Phys Ther Sport. 2012;13(1):45–52.
Duma S, Manoogian S, Bussone W, et al. Analysis of real-time head accelerations in collegiate football players. Clin J Sport Med. 2005;15(1):3–8.
Naunheim R, Standeven J, Richter C, et al. Comparison of impact data in hockey, football, and soccer. J Trauma. 2000;48(5):938–41.
Rowson S, Duma S, Beckwith J, et al. Rotational head kinematics in football impacts: an injury risk function for concussion. Ann Biomed Eng. 2012;40(1):1–13.
Schnebel B, Gwin J, Anderson S, et al. In vivo study of head impacts in football: a comparison of National Collegiate Athletic Association division I versus high school impacts. Neurosurgery. 2007;60(3):490–6.
Crisco J, Fiore R, Beckwith J, et al. Frequency and location of head impact exposures in individual collegiate football players. J Athl Train. 2010;45(6):459–559.
Daniel R, Rowson S, Duma S. Head impact exposure in youth football. Ann Biomed Eng. 2012;40(4):976–81.
Ng T, Bussone W, Duma S. The effect of gender and body size on linear accelerations of the head observed during daily activities. Biomed Sci Instrum. 2006;42:25–30.
Rowson S, Duma S. Development of the STAR evaluation system for football helmets: integrating player head impact exposure and risk of concussion. Ann Biomed Eng. 2011;39(8):2130–40.
Rowson S, Duma S. Brain injury prediction: Assessing the combined probability of concussion using linear and rotational head acceleration. Ann Biomed Eng. 2013;41(5):873–82.
Urban J, Davenport E, Golman A, et al. Head impact exposure in youth football: high school ages 14 to 18 years and cumulative impact analysis. Ann Biomed Eng. 2013;41(12):2474–87.
Allen M, Weir-Jones I, Eng P, et al. Acceleration perturbations of daily living: a comparison to ‘whiplash’. Spine (Phila Pa 1976). 1994;19(11):1285–90.
Kavanagh J, Barrett R, Morrison S. Upper body accelerations during walking in healthy young and elderly men. Gait Posture. 2004;20(3):291–8.
Mihalik J, Bell D, Marshall S, et al. Measurements of head impacts in collegiate football players: an investigation of positional and event type differences. Neurosurgery. 2007;61(6):1229–35.
Wu L, Nangia V, Bui K, et al. In vivo evaluation of wearable head impact sensors. Ann Biomed Eng. 2015. doi:10.1007/s10439-015-1423-3.
Pedišić Ž, Bauman A. Accelerometer-based measures in physical activity surveillance: current practices and issues. Br J Sports Med. 2014. doi:10.1136/bjsports-2013-093407.
Gadd C. Use of a weighted impulse criterion for establishing injury hazard. In: Proceedings of the 10th STAPP Car rash conference, Society of Automotive Engineers; New York; 1966. p. 164–74.
Bartsch A, Benzel E, Miele V, et al. Impact test comparisons of 20th and 21st century American football helmets. J Neurosurg. 2012;116(1):222–33.
Lewis E. Head injury and protection. In: Rainford D, Gradwell D, editors. Ernsting’s aviation medicine. Boca Ratoa: CRC Press; 2006. p. 179–88.
McLean A, Anderson W. Biomechanics of closed head injury. In: Reilly P, Bullock R, editors. Head injury. London: Chapman & Hall; 1997. p. 25–37.
Versace J. A review of the severity index. In: 15th Stapp Car Crash Conference, Society of Automotive Engineers; 1971:771–96.
Kleinberger M, Sun E, Eppinger R, et al. Development of improved injury criteria for the assessment of advanced automotive restraint systems: NHTSA; 1998.
King A, Yang K, Zhang L, et al. Is head injury caused by linear or angular acceleration? IRCOBI conference. Lisbon, Portugal; 2003. p. 1–12.
Greenwald R, Gwin J, Chu J, et al. Head impact severity measures for evaluating mild traumatic brain injury risk exposure. Neurosurgery. 2008;62(4):789–98.
Newman J. A generalized acceleration model for brain injury threshold (GAMBIT). International IRCOBI conference on the biomechanics of impacts 1986. Zurich (Switzerland); 1986. p. 121–31.
Hernandez F, Wu L, Yip M, et al. Six degree-of-freedom measurements of human mild traumatic brain injury. Ann Biomed Eng. 2015. doi:10.1007/s10439-014-1212-4.
Newman J, Shewchenko N, Welbourne E. A proposed new biomechanical head injury assessment function—the maximum power index. Stapp Car Crash J. 2000;44:215–47.
Stroup D, Berlin J, Morton S, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. J Am Med Assoc. 2000;283(15):2008–12.
Brolinson P, Manoogian S, McNeely D, et al. Analysis of linear head accelerations from collegiate football impacts. Curr Sports Med Rep. 2006;5(1):23–8.
Bazarian J, Zhu T, Zhong J, et al. Persistent, long-term cerebral white matter changes after sports-related repetitive head impacts. PLoS One. 2014;9(4):1–12.
Crisco J, Wilcox B, Machan J, et al. Magnitude of head impact exposures in individual collegiate football players. J Appl Biomech. 2012;28(2):174–83.
Funk J, Rowson S, Daniel R, et al. Validation of concussion risk curves for collegiate football players derived from HITS data. Ann Biomed Eng. 2011;40(1):79–89.
Gwin J, Chu J, McAllister T, et al. In situ measures of head impact acceleration in NCAA division I men’s Ice Hockey: implications for ASTM F1045 and other ice hockey helmet standards. J ATSM Int. 2009;6(6):101848.
Harpham J, Mihalik J, Littleton A, et al. The effect of visual and sensory performance on head impact biomechanics in college football players. Ann Biomed Eng. 2014;42(1):1–10.
Mihalik J, Guskiewicz K, Marshall S, et al. Does cervical muscle strength in youth ice hockey players affect head impact biomechanics? Clin J Sport Med. 2011;21(5):416–21.
Mihalik J, Guskiewicz K, Marshall S, et al. Head impact biomechanics in youth hockey: comparisons across playing position, event types, and impact locations. J Biomed Eng. 2012;40(1):141–9.
Mihalik J, Greenwald R, Blackburn J, et al. Effect of infraction type on head impact severity in youth ice hockey. Med Sci Sport Exerc. 2010;42(8):1431–8.
Munce T, Dorman J, Thompson P, et al. Head impact exposure and neurologic function of youth football players. Med Sci Sport Exerc. 2015. doi:10.1249/MSS.0000000000000591.
Ocwieja K, Mihalik J, Marshall S, et al. The effect of play type and collision closing distance on head impact biomechanics. Ann Biomed Eng. 2012;40(1):90–6.
Beckwith J, Greenwald R, Chu J, et al. Head impact exposure sustained by football players on days of diagnosed concussion. Med Sci Sport Exerc. 2013;45(4):737–46.
Beckwith J, Greenwald R, Chu J, et al. Timing of concussion diagnosis is related to head impact exposure prior to injury. Med Sci Sport Exerc. 2013;45(4):747–54.
Broglio S, Martini D, Kasper L, et al. Estimation of head impact exposure in high school football: Implications for regulating contact practices. Am J Sports Med. 2013;41(12):2877–84.
Daniel R, Rowson S, Duma S. Head impact exposure in youth football: middle school ages 12-14 years. J Biomech Eng. 2014;136(9):094501–6.
Broglio S, Schnebel B, Sosnoff J, et al. Biomechanical properties of concussions in high school football. Med Sci Sports Exerc. 2010;42(11):2064–71.
Broglio S, Sosnoff J, Shin S, et al. Head impacts during high school football: a biomechanical assessment. J Athl Train. 2009;44(4):342–9.
Broglio S, Eckner J, Surma T, et al. Post-concussion cognitive declines and symptomatology are not related to concussion biomechanics in high school football players. J Neurotrauma. 2011;28(10):2061–8.
Eckner J, Sabin M, Kutcher J, et al. No evidence for a cumulative impact effect on concussion injury threshold. J Neurotrauma. 2011;28(10):2079–90.
Martini D, Eckner J, Kutcher J, et al. Sub-concussive head impact biomechanics: comparing differing offensive schemes. Med Sci Sport Exerc. 2013;45(4):755–61.
Wilcox B, Machan J, Beckwith J, et al. Head-impact mechanisms in men’s and women’s collegiate ice hockey. J Athl Train. 2014;49(4):514–20.
Wong R, Wong A, Bailes J. Frequency, magnitude, and distribution of head impacts in Pop Warner football: The cumulative burden. Clin Neurol Neurosur. 2014;118:1–4.
McCaffrey M, Mihalik J, Crowell D, et al. Measurement of head impacts in collegiate football players: clinical measures of concussion after high- and low-magnitude impacts. Neurosurgery. 2007;61(6):1236–43.
McIntosh A, Patton D, Fréchède B, et al. The biomechanics of concussion in unhelmeted football players in Australia: a case–control study. BMJ Open. 2014;4(5):e005078.
Breedlove E, Robinson M, Talavage T, et al. Biomechanical correlates of symptomatic and asymptomatic neurophysiological impairment in high school football. J Biomech. 2012;45(7):1265–72.
Duhaime A-C, Beckwith J, Maerlender A, et al. Spectrum of acute clinical characteristics of diagnosed concussions in college athletes wearing instrumented helmets. J Neurosurg. 2012;117(6):1092–9.
Guskiewicz K, Mihalik J, Shankar V, et al. Measurement of head impacts in collegiate football players: relationship between head impact biomechanics and acute clinical outcome after concussion. Neurosurgery. 2007;61(6):1244–53.
Wilcox B, Beckwith J, Greenwald R, et al. Biomechanics of head impacts associated with diagnosed concussion in female collegiate ice hockey players. J Biomech. 2015;48(10):2201–4.
Camarillo D, Shull P, Mattson J, et al. An instrumented mouthguard for measuring linear and angular head impact kinematics in American football. Ann Biomed Eng. 2013;41(9):1939–49.
Mattson J, Schultz R, Goodman J, et al. Validation of a novel mouth guard for measurement of linear and rotational accelerations during head impacts. Clin J Sport Med. 2012;22(3):294.
Siegmund G, Guskeiwicz K, Marshall S, et al. Laboratory validation of two wearable sensor systems for measuring head impact severity in football players. Ann Biomed Eng. 2015. doi:10.1007/s10439-015-1420-6.
Mihalik J, Blackburn J, Greenwald B, et al. Collision type and player anticipation affect head impact severity among youth ice hockey players. Pediatrics. 2010;125(6):e1394–401.
Denny-Brown D, Russell W. Experimental cerebral concussion. Brain. 1940;64(2–3):93–164.
Broglio S, Eckner J, Paulson H, et al. Cognitive decline and aging: the role of concussive and subconcussive impacts. Exerc Sport Sci Rev. 2012;40(3):138–44.
Miller J, Adamson G, Pink M, et al. Comparison of preseason, midseason, and postseason neurocognitive scores in uninjured collegiate football players. Am J Sports Med. 2007, 2007; 35(8):1284–8.
Erlanger D. Exposure to sub-concussive head injury in boxing and other sports. Brain Inj. 2015;29(2):171–4.
Packard R. Chronic post-traumatic headache: associations with mild traumatic brain injury, concussion, and post-concussive disorder. Curr Pain Headache Rep. 2008;12(1):67–73.
Stern R, Daneshvar D, Baugh C, et al. Clinical presentation of chronic traumatic encephalopathy. Neurology. 2013;81(13):1122–9.
McKee A, Stein T, Nowinski C, et al. The spectrum of disease in chronic traumatic encephalopathy. Brain. 2012;136(1):43–64.
Ommaya A. Biomechanics of head injuries: experimental aspects. In: Nuham A, Melvin J, editors. Biomechanics of trauma. Norwalk: Appleton-Century-Crofts; 1985. p. 245–69.
Kleiven S. Why most traumatic brain injuries are not caused by linear acceleration but skull fractures are. Front Bioeng Biotechnol. 2013;1:15.
Kleiven S. Evaluation of head injury criteria using a finite element model validated against experiments on localized brain motion, intracerebral acceleration, and intracranial pressure. Int J Crashworthines. 2006;11(1):65–79.
Shreiber D, Bain A, Meaney D. In vivo thresholds for mechanical injury to the blood-brain barrier. In: Procedings of the 41st Stapp Car Crash Conference. Lake Buena Vista, Florida (USA); 1997. p. 227–91.
Cantu R. Head injuries in sport. Br J Sports Med. 1996;30(4):289–96.
Unterharnscheidt F. Translational versus rotational acceleration: animal experiments with measured inputs. Scand J Rehabil Med. 1972;4(1):24–6.
King A, Yang K, Zhang L, et al. Is rotational acceleration more injurious to the brain than linear acceleration? In: Hwang NC, Woo S-Y, editors. Frontiers in biomedical engineering. USA: Springer; 2004. p. 135–47.
Kleiven S. Influence of impact duration on the human head in prediction of subdural hemotoma. J Neurotrauma. 2003;20(4):365–79.
Kleiven S. Predictors for traumatic brain injuries evaluated through accident reconstructions. Stapp Car Crash J. 2007;51:81–117.
Mecham M, Greenwald R, Macintyre J, et al. Incidence and severity of head impact during freestyle aerial ski jumping. J App Biomech. 1999;15(1):27–35.
Lockett F. Biomechanics justification for emperical head impact tolerance criteria. J Biomech. 1985;18(3):217–24.
Fenner H, Thomas D, Gennarelli T, et al. Final report of workshop on criterion for head injury in helmet standards. Milwaukee Wisconsin: Medical College of Wisconsin/Snell Memorial Foundation; 2005.
World Health Organisation. Review of physical activity surveillance data sources in European Union Member States. Report No. 6. Copenhagen, Denmark: WHO Regional Office for Europe; 2010.
Colley R, Garriguet D, Janssen I, et al. Physical activity of Canadian adults: accelerometer results from the 2007 to 2009 Canadian Health Measures Survey. Health Rep. 2011;22(1):7–14.
Paul D, Kramer M, Moshfegh A, et al. Comparison of two different physical activity monitors. BMC Med Res Methodol. 2007;7:26.
Cain K, Conway T, Adams M, et al. Comparison of older and newer generations of ActiGraph accelerometers with the normal filter and the low frequency extension. Int J Behav Nutr Phys Act. 2013;10:51.
John D, Sasaki J, Hickey A, et al. ActiGraph™ activity monitors: “The firmware effect”. Med Sci Sport Exerc. 2014;46(4):834–9.
Yngve A, Nilsson A, Sjöström M, et al. Effect of monitor placement and of activity setting on the MTI accelerometer output. Med Sci Sport Exerc. 2003;35(2):320–6.
Edwardson C, Gorely T. Epoch length and its effect on physical activity intensity. Med Sci Sport Exerc. 2010;42(5):928–34.
Ojiambo R, Cuthill R, Budd H, et al. Impact of methodological decisions on accelerometer outcome variables in young children. Int J Obes. 2011;35(S1):S98–103.
Lee P. Data imputation for accelerometer-measured physical activity: the combined approach. Am J Clin Nutr. 2013;97(5):965–71.
Evenson K, Terry J. Assessment of differing definitions of accelerometer nonwear time. Res Q Exerc Sport. 2012;80(2):355–62.
Kim Y, Beets M, Pate R, et al. The effect of reintegrating Actigraph accelerometer counts in preschool children: comparison using different epoch lengths. J Sci Med Sport. 2013;16(2):129–34.
Beckwith J, Greenwald R, Chu J. Measuring head kinematics in football: correlation between the head impact telemetry system and hybrid III headform. Ann Biomed Eng. 2012;40(1):237–48.
Broglio S, Eckner J, Kutcher J. Field-based measures of head impacts in high school athletes. Curr Opin Pediatr. 2012;24(6):702–8.
Acknowledgments
The authors declare that there are no competing interests associated with the research contained within this manuscript. No sources of funding were utilised in conducting this study. According to the definition given by the International Committee of Medical Journal Editors (ICMJE), the authors listed above qualify for authorship on the basis of making one or more of the substantial contributions to the intellectual content of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
Doug King, Patria Hume, Conor Gissane, Matt Brughelli and Trevor Clark declare that they have no conflict of interest.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
King, D., Hume, P., Gissane, C. et al. The Influence of Head Impact Threshold for Reporting Data in Contact and Collision Sports: Systematic Review and Original Data Analysis. Sports Med 46, 151–169 (2016). https://doi.org/10.1007/s40279-015-0423-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-015-0423-7