
Abstract
For several years, Virginia Tech and other schools have measured the frequency and severity of head impacts sustained by collegiate American football players in real time using the Head Impact Telemetry (HIT) System of helmet-mounted accelerometers. In this study, data from 37,128 head impacts collected at Virginia Tech during games from 2006 to 2010 were analyzed. Peak head acceleration exceeded 100 g in 516 impacts, and the Head Injury Criterion (HIC) exceeded 200 in 468 impacts. Four instrumented players in the dataset sustained a concussion. These data were used to develop risk curves for concussion as a function of peak head acceleration and HIC. The validity of this biomechanical approach was assessed using epidemiological data on concussion incidence from other sources. Two specific aspects of concussion incidence were addressed: the variation by player position, and the frequency of repeat concussions. The HIT System data indicated that linemen sustained the highest overall number of head impacts, while skill positions sustained a higher number of more severe head impacts (peak acceleration > 100 g or HIC > 200). When weighted using injury risk curves, the HIT System data predicted a higher incidence of concussion in skill positions compared to linemen at rates that were in strong agreement with the epidemiological literature (Pearson’s r = 0.72–0.87). The predicted rates of repeat concussions (21–39% over one season and 33–50% over five seasons) were somewhat higher than the ranges reported in the epidemiological literature. These analyses demonstrate that simple biomechanical parameters that can be measured by the HIT System possess a high level of power for predicting concussion.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Mild traumatic brain injury (MTBI), or concussion, is by definition caused by biomechanical forces. The quantification of concussion risk in terms of biomechanical parameters, such as peak head acceleration and the Head Injury Criterion (HIC), provides valuable insight for helmet designers seeking to reduce the incidence of concussion and clinicians seeking to diagnose a concussion on the field. A full statistical description of concussion biomechanics in football requires an epidemiological characterization of head impact exposure and concussion incidence within the relevant population. Concussion risk can then be calculated by normalizing concussion incidence by head impact exposure. No single study design can capture all the required information in sufficient detail. Studies utilizing injury surveillance systems or questionnaires have been able to capture hundreds to thousands of concussions and quantify concussion incidence in great detail, including overall concussion rate per athlete exposure,1,7,14 concussion rate by player position,7,22 and the rate of repeat concussions.6,15,16,23,32 However, these types of studies do not provide any biomechanical data.
Biomechanical data associated with concussive head impacts in football were first generated by reconstructing NFL game impacts resulting in concussion using Hybrid III crash test dummies and detailed video analyses.21,24 The reconstructed concussive impacts were associated with peak head accelerations of 98 ± 28 g and HIC values of 381 ± 197.24 The development of the Head Impact Telemetry (HIT) System enabled direct, real-time measurement of biomechanical parameters in thousands of head impacts using helmet-mounted accelerometers.2,3,5,8,10,13,14,18,20,28–30 So far, the HIT System has been used at the collegiate and high school levels.9 Studies utilizing the HIT System have reported on head impact exposure in great detail, including variations in head impact exposure by player position.3,5,9,20 Studies utilizing the HIT System are also able to record biomechanical data for concussive impacts occurring in players who happen to be instrumented at the time of injury. Because concussion is a relatively rare event, the number of concussions captured by the HIT System is relatively low.
Risk curves for concussion were first proposed by Newman et al.21 using data from reconstructed NFL game impacts. Pellman et al.,24 using the complete dataset of reconstructed NFL game impacts, suggested nominal tolerance values of 80 g peak head acceleration and a HIC of 250. These tolerance values were thought to represent an approximately 50% risk of concussion. The NFL study was a landmark investigation in terms of characterizing concussion incidence, but no head impact exposure data were collected, apart from the 31 reconstructed impacts that were intentionally biased toward injury. Therefore, the NFL risk curves were fundamentally flawed because they did not rely on unbiased head impact exposure data. Numerous HIT System studies have shown the NFL risk curves to be grossly inaccurate, with fewer than 1% of head impacts having a peak head acceleration greater than 80 g resulting in concussion.2,10,20 Funk et al.10 presented a mathematically rigorous methodology for calculating concussion risk curves by combining epidemiological data on overall concussion incidence with HIT System data to define head impact exposure and concussion in terms of biomechanical parameters. According to the concussion risk curves proposed by Funk et al.,10 the nominal tolerance values proposed by Pellman et al.24 of 80 g and a HIC of 250 represented approximately a 1% risk of concussion, rather than a 50% risk. Rowson and Duma29 recently proposed a slightly more conservative concussion risk curve that accounts for the underreporting of concussions.19 The purpose of the present article is to evaluate how well the risk curves derived primarily from HIT System data predicted independent epidemiological features of concussion incidence. Two specific epidemiological features of concussion incidence were studied: the variations in concussion rate by player position, and the rate of first-time vs. repeat concussions.
Methods
Data Collection
Head impact data were collected from 98 collegiate football players at Virginia Tech over a 5-year period (2006–2010). Instrumented players gave written informed consent with Institutional Review Board approval from Virginia Tech and the Edward Via Virginia College of Osteopathic Medicine. The helmets of the subject players were instrumented with the HIT System (Simbex, Lebanon, NH), which consists of an array of accelerometers that records 40 ms of data at 1000 Hz for each head impact and transmits the data wirelessly to a laptop computer on the sideline. The accuracy of the HIT System has been validated with headform and dummy testing.4,8,10,17,26 Data collection was triggered when any one helmet-mounted accelerometer exceeded 10 g. Only impacts in which the calculated translational acceleration at the center of gravity of the player’s head exceeded 10 g were analyzed. Because most helmets were not designed to measure head accelerations in 6 degrees of freedom (6 DOF), rotational acceleration data were not analyzed in this study. All impacts greater than 150 g were verified using game video to confirm that the subject player had indeed experienced a head impact at the time of the recording. For each impact analyzed, the HIC value was calculated31:
where t 1 and t 2 are the initial and final times in seconds (15 ms maximum), which maximize the HIC value and a(t) is the resultant translational acceleration at the center of gravity of the head expressed in the dimensionless unit of gravities (g). Beginning in 2006, detailed team records were available to determine each player’s participation in each game in terms of the number of plays and the position played. HIT System data were collected during both practices and games, but because player participation data were not available for practices, only the HIT System data collected during games were analyzed.
Risk Curve Development
Although concussion risk curves have previously been developed by Funk et al.10 and Rowson and Duma,29 each of these analyses included assumptions that tended to make the risk curves more conservative. For example, Funk et al.10 adjusted for the fact that the HIT System tends to overestimate peak head acceleration by 8 ± 11% and HIC by 23 ± 28%, and Rowson and Duma29 assumed a relatively high concussion rate of 5.56 concussions per 1000 athlete exposures in games1 and inflated that rate by 53% to account for underreporting of concussions.19 For the purpose of this analysis, new concussion risk curves were developed solely from the Virginia Tech dataset described above without any conservative assumptions. Concussion incidence was assumed to follow a normal distribution that could be described by the average and standard deviation of the peak head acceleration and HIC values experienced by the concussed players during the injurious impacts, with the integral of the distribution equal to the total number of concussions captured in the dataset. Head impact exposure was the raw HIT System data normalized by the number of athlete exposures in games. Concussion risk at discrete levels of impact severity (peak acceleration increments of 1 g and HIC increments of 10) was calculated by dividing the concussion incidence by the head impact exposure. A “Virginia Tech-optimized” risk curve having a Weibull distribution was fit to the discrete risk data. Owing to anomalous results at the extreme high end of the severity spectrum, head impacts above 175 g or a HIC of 700 (about 30–35 data points) were ignored when fitting the risk curve. This risk curve was meant to provide a lower bound for concussion risk. In order to characterize how conservative the various risk curves were, peak head acceleration and HIC values associated with a 1, 5, and 10% risks of concussion were evaluated, as well as the overall concussion rate per 1000 athlete exposures (E inj) predicted by the risk curve, given the head impact exposure of the Virginia Tech HIT System dataset:
where n(x) is the number of head impacts at a given head impact severity level x, p(x inj < x) is the probability of concussion given by the chosen concussion risk curve, and AE is the number of instrumented athletic exposures (defined as one instrumented player playing in one game). Head impact severity (x) was defined either in terms of peak head acceleration or HIC.
Player Position Analysis
Two epidemiological studies were found, which reported concussion rates by player position. Pellman et al.22 reported the total number of concussions sustained over a 6-year period in the NFL games by player position and calculated concussion rates that were normalized by position weights corresponding to the number of players typically present at each position. Dick et al.7 investigated 16 years worth of NCAA injury data and expressed game concussion rates by weighted player position as a percentage of the total number of concussions among the seven positions studied (quarterback, running back, wide receiver, offensive line, defensive line, linebacker, and defensive back). For the purpose of this study, all concussion rates by player position were converted to percentages to facilitate comparison with the data from Dick et al.7
Two separate analyses of the Virginia Tech HIT System data were conducted: a threshold analysis, and a risk curve analysis. In the threshold analysis, the number of head impacts experienced by players at a given position during a game was calculated by dividing the number of head impacts above a given biomechanical threshold by the number of instrumented athlete exposures. The Virginia Tech HIT System data were normalized by instrumented athlete exposure rather than by assumed “position weights” because the proportion of players who were instrumented varied by position. Impacts below the threshold were assumed to pose no risk of concussion, while impacts above the threshold were assumed to provide a uniform risk of concussion. The proportion of concussions (P) for each of the seven positions studied was given by
where i is an index variable for player position, n(x > x threshold) is the number of head impacts above the chosen threshold level, and AE is the number of instrumented athlete exposures at each position.
In the risk curve analysis, the proportion of concussions expected at each position was obtained by weighting each impact recorded by the HIT System by its estimated risk of concussion:
The level of agreement between the predicted and actual concussion rates by weighted player position was assessed using the Pearson product–moment correlation coefficient (Pearson’s r).
Repeat Concussion Analysis
The risk of sustaining multiple concussions was calculated assuming that head impact tolerance varies among the population of players but remains fixed for each individual player. The probability that a player will suffer at least one concussion is therefore given by the risk of concussion for the player’s most severe head impact. The probability that a player will suffer exactly one concussion is given by the difference in concussion risk associated with the most severe and the second-most severe head impacts sustained by the player. This logic can be extended to determine a player’s risk of sustaining exactly k concussions (p k ):
where p(x inj < x) is the risk of concussion given by the chosen concussion risk curve, and x k is the head impact severity of rank k for the player (x 1 is the most severe head impact, x 2 is the second-most severe head impact, etc.). The overall number of players expected to sustain exactly k concussions (E k ) is simply the sum of each player’s probability of sustaining exactly k concussions:
where i is an index variable for player number. From this equation, the percentage of players expected to sustain exactly k concussions (P k ) can be calculated:
The analysis could also be performed in terms of the percentage of concussions that are expected to be one of exactly k concussions sustained by a player. If expressed in terms of concussions instead of players, the repeat concussion rate would be higher. It can be shown mathematically that the overall concussion rate E inj (expressed in terms of concussions per 1000 athlete exposures) calculated by summing the number of repeat concussions over all players is equivalent to summing the risk of concussion for each individual impact regardless of which player sustained the impact, as described in Eq. (2):
For this article, the predicted repeat concussion rate was expressed as the percentage of players expected to sustain more than one concussion over one season and over all five seasons. The repeat concussion rate predicted for a single season was calculated by averaging the predicted repeat concussion rate for each season weighted by the number of instrumented athlete exposures in games:
where i is an index variable for season year. The predicted rate of repeat concussions was based entirely on the head impact exposure data recorded by the HIT System, rather than on the data from actual concussions.
Results
Between 17 and 53 players were instrumented each season, with a total of 98 players (55% of all players) participating in the study over the course of five seasons. HIT System data were recorded for 1349 athletic exposures in games (39% of the whole team) and 49,417 player plays in games (46% of the whole team). A total of 37,128 head impacts above 10 g were recorded during games. The distribution of head impacts was heavily skewed toward lower severity impacts in a generally exponential fashion (Figs. 1 and 2). The number of head impacts above a given peak head acceleration decreased by roughly a factor of 2 with every 20 g increase in severity and by roughly a factor of 10 with every 60 g increase in severity. The number of more severe head impacts was considerably lower than the total number of impacts, with 516 impacts exceeding 100 g and 468 impacts exceeding a HIC of 200.

Head impact exposure in terms of peak head acceleration. Bars reflect the number of head impacts within a 10-g window (10–20 g, 20–30 g, etc.). The line reflects the cumulative number of impacts above a particular peak head acceleration

Head impact exposure in terms of HIC. Bars reflect the number of head impacts within a HIC window of 50 (HIC from 50–100, 100–150, etc.). The line reflects the cumulative number of impacts above a particular HIC level
Concussions were diagnosed in four instrumented players during games, yielding an overall game injury rate of 2.97 concussions per 1000 athletic exposures. The average head impact severity associated with concussion was 145 ± 35 g and a HIC of 615 ± 309 (Table 1). For three of the four concussed players, the concussive impact was the most severe impact they experienced that year and one of the two most severe impacts they experienced during the entire study period in terms of both peak head acceleration and HIC. The fourth player experienced eight impacts with higher peak head accelerations and three impacts with a higher HIC value. An additional four concussions were diagnosed in instrumented players during practices and scrimmages, but these data were not analyzed.
The concussion risk curves optimized to the Virginia Tech dataset were considerably less conservative than the concussion risk curves developed previously by Funk et al.10 and Rowson and Duma29 (Table 2). All of the concussion risk curves studied predicted relatively high overall concussion rates (E inj) given the Virginia Tech HIT System exposure data (Table 3). The risk curves optimized to the Virginia Tech dataset were the least conservative and predicted the lowest overall concussion rate, while the risk curves of Pellman et al.24 were excessively conservative and predicted that each player should sustain about two concussions per game.
Each player position was well sampled, with the number of recorded head impacts above 10 g ranging from 4771 in quarterbacks to 22,047 in offensive linemen. The number of more severe head impacts (>100 g or HIC > 200) ranged from 29 to 124 for each position. The overall number of head impacts above 10 g was not indicative of the number of more severe head impacts above 100 g or a HIC of 200 sustained at each player position. Quarterbacks and offensive linemen provide an illustrative comparison. Offensive linemen sustained 3.4 times more head impacts above 10 g than quarterbacks (55 vs. 16 per athlete exposure). However, this difference narrowed and eventually reversed at higher impact severities (Fig. 3). Quarterbacks actually sustained 1.3–1.5 times more impacts of higher severity (>100 g or HIC > 200) per athlete exposure than offensive linemen (Fig. 4).

Number of head impacts per athlete exposure for offensive linemen and quarterbacks as a function of the chosen peak head acceleration threshold

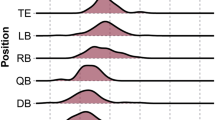
Number of head impacts per athlete exposure for various positions using head impact severity thresholds of G > 10 g and G > 100 g
The concussion rates by player position reported in the epidemiological studies of Dick et al.7 and Pellman et al.22 were very well correlated to each other (r = 0.89). When concussion rate by player position was predicted using a 10-g injury threshold, the results were in poor agreement with these studies7,24 (Fig. 5). The concussion rate was overpredicted in offensive linemen and underpredicted in quarterbacks and running backs. In fact, there was a strongly negative correlation between the predicted concussion rates and the actual concussion rates documented by Dick et al.7 (r = −0.71) and Pellman et al.22 (r = −0.88). As the injury threshold was increased, the correlation between the predicted and actual concussion rates by player position improved (Fig. 6). When only impacts over 100 g were considered, there was much better agreement between the predicted and actual concussion rates (r = 0.56 vs. Dick et al.7 and r = 0.34 vs. Pellman et al.22). The correlation was even higher when only impacts having a HIC over 200 were considered (r = 0.66 vs. Dick et al.7 and r = 0.47 vs. Pellman et al.22). Similar levels of correlation between predicted and actual concussion rates by player position were obtained using the concussion risk curves of Rowson and Duma29 and Funk et al.10 (r = 0.40–0.75) (Table 3). The correlation between actual and predicted concussion rates by player position was strongly negative using the concussion risk curves of Pellman et al.24 and strongly positive using the concussion risk curves optimized to the Virginia Tech dataset (r = 0.72–0.87). In general, the less conservative the concussion risk curves were, the better they predicted the actual variation in concussion rates by player position.

Concussion incidence by player position. The top two bars (Pellman et al.22 and Dick et al.7) are epidemiological data. The next three bars (G > 10 g, G > 100 g, and HIC > 200) are predicted values from the threshold analyses. The remaining bars are predicted values using various concussion risk curves

Degree of agreement between predicted and actual concussion rates by player position as a function of the chosen head impact severity threshold
All of the concussion risk curves studied predicted a high rate of repeat concussions over both a 1- and a 5-year period (Table 3). As expected, the repeat concussion rate was always predicted to be higher when analyzing 5 years of exposure data compared to analyzing only 1 year of exposure data. Being excessively conservative, the Pellman et al.24 risk curves predicted that over 90% of concussed players would sustain multiple concussions, with the majority of those players sustaining more than seven concussions (Fig. 7). Among the concussion risk curves derived primarily from HITS data, the predicted repeat concussion rate was generally higher in those curves using peak head acceleration as an injury metric (39–67%) compared to the curves using HIC as an injury metric (21–55%) (Table 3). The less conservative risk curves predicted a lower repeat concussion rate than the more conservative risk curves. All of the risk curves studies predicted a higher repeat concussion rate over a 5-year period than the epidemiological data of Pellman et al.,23 although the concussion risk curve optimized for the Virginia Tech dataset using HIC as an injury metric matched the Pellman et al.23 epidemiological data reasonably well (Fig. 7).

Repeat concussion rate over five seasons. The top bar (Pellman et al. 23) is epidemiological data. The remaining bars are predicted values using various concussion risk curves
Discussion
The purpose of this article was to validate the accuracy of the HIT System data and the concussion risk curves derived from it by attempting to predict more detailed features of the epidemiological data on concussion incidence, namely, variations in the rate of concussion by player position and the incidence of repeat concussions. The overall number of head impacts (>10 g) sustained at each player position as recorded by the HIT System did not correlate well with the player position concussion rates reported in epidemiological studies.7,22 Rather, positions sustaining higher frequencies of more severe head impacts (>100 g or HIC > 200) were also associated with higher concussion rates in epidemiological studies. Likewise, strong agreement between predicted and measured concussion rates by player position was achieved when the HIT System exposure data were weighted using concussion risk curves derived from HIT System data. In general, less conservative concussion risk curves yielded a better match to the epidemiological data in terms of both player position concussion rates and the rate of repeat concussions. The finding that the combination of HIT System exposure data with the appropriate risk curves accurately predicted epidemiological data from independent sources lends support to this biomechanical approach to understanding concussion.
One of the most notable features of the HITS data is that the distribution of head impacts is highly skewed toward the low end of the severity spectrum. This observation has several implications. First, any quantification of the number of head impacts sustained by a player must be qualified by the severity threshold used to define that number. Unfortunately, the criteria for counting a head impact have not always been consistent between HITS studies. Some studies (including this one) have used a 10-g threshold for any one of the helmet-mounted accelerometers,8,10,20,28,29,31 while others have used a 15-g threshold.2,3,5 Even when one helmet-mounted accelerometer records an acceleration greater than 10 or 15 g, it is possible for the calculated peak head acceleration at the center of gravity of the head to be less than 10 g. Some studies (including this one) have explicitly excluded head accelerations less than 10 g,14,20,28 whereas others have not.2,3,8,10,29,30 Although somewhat arbitrary, a threshold of 10–15 g, which is commonly used in HITS studies, is probably reasonable for separating actual head impacts from voluntary movement of the head. However, based on the observed distribution of head impact severities (Fig. 1), there may be almost as many head impacts below 15 g as there are above 15 g. Therefore, seemingly minor differences in inclusion criteria can make head impact exposure comparisons between studies problematic if exposure is defined by the number of head impacts5 or any derivative thereof, such as the average or log-transformed average head impact severity,8,20,30 or the percentage of head impacts above a given severity level.8,30 Counts of head impacts above a higher threshold can be meaningfully compared between studies if they are normalized by the number of athlete exposures.
A second implication of the skewness of the head impact distribution is that the great majority of head impacts pose essentially no risk of concussion. One aim of the present study was to determine what threshold levels should be applied to the HIT System data to provide a meaningful estimate of injury potential. The results of the study suggest that a good estimate of injury potential can be obtained by counting only impacts with peak accelerations greater than 100 g or HIC values greater than 200. Although many concussions occur at lower impact severities, these thresholds represent less than a 1% risk of concussion and seem to provide a good balance between including potentially injurious impacts and excluding impacts having only a negligible injury potential. Furthermore, these results are in good agreement with Broglio et al.,2 who found that 96 g was a useful cutoff value for separating potentially injurious impacts from benign ones. Obviously, there is no single threshold for concussion for all players, and the distribution of concussion risk among the population is better characterized by a curve rather than a step function. However, reporting head impact exposure requires that some threshold be chosen, and we have found that choosing a higher severity threshold provides a better reflection of injury potential.
A third implication of the finding that head impact exposure is highly skewed towards low severity impacts is that overestimation errors in the HITS data are magnified at the highest end of the impact severity spectrum. Although quite accurate, the HIT System does have some measurement error that is comparable to many other biomechanical measurement devices.27,28 Funk et al.10 analyzed over 100 dummy validation tests and calculated the coefficient of variation of the scatter error in HIT System measurements to be 11% for peak head acceleration and 28% for HIC. The effect of this scatter error is to flatten out the distribution of recorded head impacts, with the recorded impacts at the highest severities being much more likely to be the result of overestimation errors.10
This phenomenon largely explains two anomalous findings in the present study. First, in developing a concussion risk curve optimized to the Virginia Tech dataset, it was observed that the risk of concussion appeared to actually decrease at the highest severity levels, a finding that was also reported by Broglio et al.3 We found a notable decrease in predicted concussion risk beginning at peak head acceleration levels above 175 g and HIC values above 700. There were only about 30–35 head impacts at this extremely high end of severity spectrum, and so these data points were ignored when fitting the Weibull concussion risk curve. We hypothesize that these data points were by and large erroneously high. It is also possible that some of the high severity impacts may have actually resulted in concussions that were not diagnosed. The second anomalous finding was that all of the concussion risk curves tended to greatly overpredict the overall concussion incidence compared to epidemiological studies in spite of being optimized to predict lower concussion incidences1,7,14,22 (Table 3). Again, and likely for the same reasons, it was found that a small number of HITS data points at the highest end of the severity spectrum (peak head acceleration >175 g or HIC > 700) accounted for most of the overestimation in predicted concussion incidence in spite of the fact that few of those head impacts actually resulted in diagnosed concussions. These considerations reinforce the admonition that concussion risk curves derived from HITS data are the most accurate at low risk levels (generally 10% or less) where the data are most plentiful.
An issue that always complicates concussion research is the imprecise nature of the diagnosis, which relies on the medical judgment of the team physician or athletic trainer and on the reporting of subjective complaints by the patient. There is some evidence that the diagnostic criteria for concussion at Virginia Tech are more stringent than at other schools. For example, the average head impact severity associated with concussion was 145 ± 35 g and a HIC of 615 ± 309 in this study (Table 1), which is consistent with previous Virginia Tech data,10 but generally higher than reported elsewhere.2,14,24 On the other hand, the concussion rate in the Virginia Tech data is consistent with other studies. For example, 4 out of 1097 (0.36%) head impacts above 80 g resulted in concussions in the present study. This finding is in excellent agreement with Mihalik et al.,20 who reported that 7 out 1858 (0.38%) head impacts above 80 g resulted in concussions and Schnebel et al.,30 who reported that 3 out of 1083 (0.28%) head impacts above 80 g resulted in concussions. Furthermore, the Virginia Tech data yielded 2.97 concussions per 1000 athlete exposures, which is within the range of 2.34–5.51 concussions per 1000 athlete exposures reported in the epidemiological literature.1,7,14,22
The concussion risk curves optimized for the Virginia Tech dataset were meant to provide a lower bound for concussion risk. Their derivation did not rely on any conservative assumptions the way that the risk curves of Funk et al.10 and Rowson and Duma29 did. The risk curves optimized for the Virginia Tech data likely underestimate the true risk of concussion for three reasons. First, the HIT System systematically overestimates peak head acceleration by 8% and HIC by 23%.10 Second, the epidemiological data used in the validation analysis do necessarily rely on the reported concussion rates, and therefore do not account for the underreporting of concussions, which may occur at a rate as high as 53%.19 Third, the analysis was based on only four concussions, and these concussions involved higher peak head accelerations and HIC values than other studies of larger sample sizes have reported.2,14,24,29
However, the appropriateness of a risk curve depends on the setting in which it is applied. The fact that some proposed concussion risk curves are more or less conservative than others may not indicate problems in accuracy so much as differences in the diagnostic criteria used to define concussion, with more conservative risk curves reflecting a more liberal definition of concussion that includes more low-grade concussions. The concussion risk curves optimized for the Virginia Tech data were the best predictors of variations in concussion rates by player position and repeat concussion rates because the epidemiological studies used for validation utilized similar diagnostic criteria for concussion, as evidenced by the similar concussion incidence rates.7,22,23 However, the concussion risk curves of Rowson and Duma29 are more appropriate for evaluating helmet performance in testing because head accelerations in testing are measured by headform accelerometers rather than the HIT System and because it was desired to use a more liberal definition of concussion that would capture unreported concussions.
The concussion risk curves evaluated in this study used very simple biomechanical metrics to predict injury, namely, peak head acceleration and HIC. Other investigators have recommended more refined biomechanical metrics that take into account translational and rotational head kinematics as well as impact location.2,11,25 Adding variables will always improve the predictive power of a statistical model, but at the risk of introducing spurious results that reflect idiosyncrasies in the dataset rather than truly predictive findings. A remarkable result of the present study is just how well the simple metrics of peak head acceleration and HIC performed as injury predictors. These variables were able to predict variations in concussion incidence by player position with strong agreement (Pearson’s r = 0.72–0.87). Furthermore, peak head acceleration and HIC identified three out of the four concussive impacts in instrumented players as being either the most severe or the second-most severe impact sustained by the player.
The predicted rate of repeat concussions in the present study was somewhat higher than most of the epidemiological data. Most of the epidemiological studies have reported that 7–15% of concussed players sustained at least one additional concussion over a single season12,15 and 24–28% of concussed players experienced multiple concussions over 5–6 seasons.23,32 A few studies have reported much higher rates of both overall concussion incidence (47–70%) and repeat concussion incidence (74–85%) over a single season.6,16 However, these studies diagnosed concussions without a medical evaluation based only on a player’s retrospective report of concussive symptoms in a post-season survey.
It is notable that the repeat concussion analysis did not take into account the possibility of a concussion actually reducing the biomechanical tolerance of the injured individual in the future. Rather, the analysis reflected the fact that there is a continuum of biomechanical tolerance in the population, with those on the lowest end of the continuum being most likely to sustain multiple concussions. Therefore, a history of concussion may simply be a marker for a low biomechanical tolerance to concussion to begin with, rather than a factor that actively increases a player’s future risk of concussion. Of course, it may be both. There is evidence suggesting that the biomechanical tolerance of an individual to a second concussive injury may be reduced for a short period of time during the healing period following the initial concussion.12 If the repeat concussion analysis in this study had factored in a reduction in tolerance with each concussion, then the predicted rate of repeat concussions would have been even higher.
Although biomechanical metrics have proven effective in predicting concussion incidence in a population, some investigators have questioned whether they are useful as an on-field diagnostic tool, noting that some players remain uninjured after experiencing very high head accelerations while other players are concussed at relatively lower head accelerations.14,18 This is indeed the expected outcome predicted by biomechanical analysis. There is no single injury threshold above which all people are injured and below which none are injured. Concussion tolerance varies within the population, and the aim of a concussion risk curve is to characterize this variation. The HIT System data suggest that most concussed players have a concussion tolerance that is much lower than average, generally within the first to fifth percentile of the population (Tables 1 and 2). Unfortunately, it is difficult to determine beforehand which players are vulnerable to concussion, but one marker appears to be a history of concussion.12,31
The HIT System can alert a team physician or athletic trainer immediately when a player has sustained a potentially injurious head impact. However, with no established method to distinguish which players are at greater risk, the false positive and false negative rates are very high. For example, if the team physician or athletic trainer evaluates every player who experiences a head impact over 100 g, they will discover a concussion only a very small percentage of the time while still missing nearly half of all concussions. Lowering the threshold will catch more concussions, but may increase the number of required evaluations beyond what is feasible.
We believe the on-field diagnostic capability of the HIT System can be improved by defining player-specific thresholds for medical evaluation based on their specific head impact history. We propose that players should be evaluated each time they experience a head impact that is among the most severe they have ever previously experienced without injury, assuming that the impact is above a nominal threshold, such as 60 g. Players with a history of having sustained several more severe head impacts without concussion have demonstrated an elevated biomechanical tolerance. In our study, 38 out of 98 players had a history of at least five head impacts over 100 g without concussion, and so evaluating those players after a 100-g head impact would be unlikely to reveal a concussion. On the other hand, the concussion tolerance of players without a history of sustaining more severe head impacts is unknown, so they should be evaluated after experiencing a head impact less than 100 g if it is the most severe or among the most severe they have ever experienced. It may also be advisable to lower the evaluation threshold for players with a history of concussion. In this way, resources may be more efficiently utilized to discover the maximum possible number of concussed players as quickly as possible and remove them from play.
References
Booher, M. A., J. Wisniewski, B. W. Smith, and A. Sigurdsson. Comparison of reporting systems to determine concussion incidence in NCAA division I collegiate football. Clin. J. Sports Med. 13:93–95, 2003.
Broglio, S. P., B. Schnebel, J. J. Sosnoff, S. Shin, X. He, C. Alcaraz, and J. Zimmerman. Biomechanical properties of concussions in high school football. Med. Sci. Sports Exerc. 42(11):2064–2071, 2010.
Broglio, S. P., J. J. Sosnoff, S. Shin, X. He, C. Alcaraz, and J. Zimmerman. Head impacts during high school football: a biomechanical assessment. J. Athl. Train. 44(4):342–349, 2009.
Crisco, J. J., J. J. Chu, and R. M. Greenwald. An algorithm for estimating acceleration magnitude and impact location using multiple nonorthogonal single-axis accelerometers. J. Biomech. Eng. 26:849–854, 2004.
Crisco, J. J., R. Fiore, J. G. Beckwith, J. J. Chu, P. G. Brolinson, S. M. Duma, T. W. McAllister, A.-C. Duhaime, and R. M. Greenwald. Frequency and location of head impact exposures in individual collegiate football players. J. Athl. Train. 45(6):549–559, 2010.
Delaney, J. S., V. J. Lacroix, S. Leclerc, and K. M. Johnson. Concussions among university football and soccer players. Clin. J. Sports Med. 12:331–338, 2002.
Dick, R., M. S. Ferrara, J. Agel, R. Courson, S. W. Marshall, M. J. Hanley, and F. Reifsteck. Descriptive epidemiology of collegiate men’s football injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2003–2004. J. Athl. Train. 42(2):221–233, 2007.
Duma, S. M., S. J. Manoogian, W. R. Bussone, P. G. Brolinson, M. W. Goforth, J. J. Donnenworth, R. M. Greenwald, J. J. Chu, and J. J. Crisco. Analysis of real-time head accelerations in collegiate football players. Clin. J. Sports Med. 15(1):3–8, 2005.
Duma, S. M., and S. Rowson. Past, present, and future of head injury research. Exerc. Sport Sci. Rev. 39:2–3, 2011.
Funk, J. R., S. M. Duma, S. J. Manoogian, and S. Rowson. Biomechanical risk estimates for mild traumatic brain injury. Annu. Proc. Assoc. Adv. Automot. Med. 51:343–361, 2007.
Greenwald, R. M., J. T. Gwin, J. J. Chu, and J. J. Crisco. Head impact severity measures for evaluating mild traumatic brain injury risk exposure. Neurosurgery 62(4):789–798, 2008.
Guskiewicz, K. M., M. McCrea, S. W. Marshall, R. C. Cantu, C. Randolph, W. Barr, J. A. Onate, and J. P. Kelly. Cumulative effects associated with recurrent concussion in collegiate football players: the NCAA concussion study. JAMA 290(19):2549–2555, 2003.
Guskiewicz, K. M., and J. P. Mihalik. Biomechanics of sport concussion: quest for the elusive injury threshold. Exerc. Sport Sci. Rev. 39(1):4–11, 2011.
Guskiewicz, K. M., J. P. Mihalik, V. Shankar, S. W. Marshall, D. H. Crowell, S. M. Oliaro, M. F. Ciocca, and D. N. Hooker. Measurement of head impacts in collegiate football players: relationship between head impact biomechanics and acute clinical outcome after collision. Neurosurgery 61(6):1244–1253, 2007.
Guskiewicz, K. M., N. L. Weaver, D. A. Padua, and W. E. Garrett. Epidemiology of concussion in collegiate and high school football players. Am. J. Sports Med. 28(5):643–650, 2000.
Langburt, W., B. Cohen, N. Akhthar, K. O’Neill, and J. C. Lee. Incidence of concussion in high school football players of Ohio and Pennsylvania. J. Child Neurol. 16(2):83–85, 2001.
Manoogian, S., D. McNeely, S. Duma, G. Brolinson, and R. Greenwald. Head acceleration is less than 10% of helmet acceleration in football impacts. Biomed. Sci. Instrum. 42:383–388, 2006.
McCaffrey, M. A., J. P. Mihalik, D. H. Crowell, E. W. Shields, and K. M. Guskiewicz. Measurement of head impacts in collegiate football players: clinical measures of concussion after high- and low-magnitude impacts. Neurosurgery 61(6):1236–1243, 2007.
McCrea, M., T. Hammeke, G. Olson, P. Leo, and K. Guskiewicz. Unreported concussion in high school football players: implications for prevention. Clin. J. Sports Med. 14:13–17, 2004.
Mihalik, J. P., D. R. Bell, S. W. Marshall, and K. M. Guskiewicz. Measurement of head impacts in collegiate football players: an investigation of positional and event-type differences. Neurosurgery 61(6):1229–1235, 2007.
Newman, J., C. Barr, M. Beusenberg, E. Fournier, N. Schewchenko, E. Welbourne, and C. Withnall. A new biomechanical assessment of mild traumatic brain injury: part 2—results and conclusions. In: Proceedings of the IRCOBI Conference, 2000, pp. 223–233.
Pellman, E. J., J. W. Powell, D. C. Viano, I. R. Casson, A. M. Tucker, H. Feuer, M. Lovell, J. F. Waeckerle, and D. W. Robertson. Concussion in professional football: epidemiological features of game injuries and review of the literature—part 3. Neurosurgery 54(1):81–96, 2004.
Pellman, E. J., D. C. Viano, I. R. Casson, A. M. Tucker, J. F. Waeckerle, J. W. Powell, and H. Feuer. Concussion in professional football: repeat injuries—part 4. Neurosurgery 55(4):860–876, 2004.
Pellman, E. J., D. C. Viano, A. M. Tucker, I. R. Casson, and J. F. Waeckerle. Concussion in professional football: reconstruction of game impacts and injuries. Neurosurgery 53:799–814, 2003.
Putukian, M., R. J. Echemendia, and S. Mackin. The acute neuropsychological effects of heading in soccer: a pilot study. Clin. J. Sport Med. 10:104–109, 2000.
Ross, D. T., D. F. Meaney, M. K. Sabol, D. H. Smith, and T. A. Gennarelli. Distribution of forebrain diffuse axonal injury following inertial closed head injury in miniature swine. Exp. Neurol. 126:291–299, 1994.
Rowson, S., J. G. Beckwith, J. J. Chu, D. S. Leonard, R. M. Greenwald, and S. M. Duma. A six degree of freedom head acceleration measurement device for use in football. J. Appl. Biomech. 27:8–14, 2011.
Rowson, S., G. Brolinson, M. Goforth, D. Dietter, and S. Duma. Linear and angular head acceleration measurements in collegiate football. J. Biomech. Eng. 131:061016-1-7, 2009.
Rowson, S., and S. M. Duma. Development of the STAR evaluation system for football helmets: integrating player head impact exposure and risk of concussion. Ann. Biomed. Eng. 39(8):2130–2140, 2011.
Schnebel, B., J. T. Gwin, S. Anderson, and R. Gatlin. In vivo study of head impacts in football: a comparison of national collegiate athletic association division I versus high school impacts. Neurosurgery 60(3):490–496, 2007.
Versace, J. A review of the severity index. SAE Technical Paper Series. SAE 710881, 1971.
Zemper, E. D. A two-year prospective study of relative risk of a second cerebral concussion. Am. J. Phys. Med. Rehabil. 82(9):653–659, 2003.
Acknowledgment
The authors gratefully acknowledge the National Institutes of Health (National Institute for Child Health and Human Development) R01HD048638 for sponsoring this research.
Author information
Authors and Affiliations
Corresponding author
Additional information
Associate Editor Joel Stitzel oversaw the review of this article.
Rights and permissions
About this article
Cite this article
Funk, J.R., Rowson, S., Daniel, R.W. et al. Validation of Concussion Risk Curves for Collegiate Football Players Derived from HITS Data. Ann Biomed Eng 40, 79–89 (2012). https://doi.org/10.1007/s10439-011-0400-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10439-011-0400-8